Back to Journals » Journal of Pain Research » Volume 19
Comparison of the Analgesic Effect and Recovery Quality Between Erector Spinae Plane Block and Quadratus Lumborum Plane Block in Laparoscopic Cholecystectomy: A Retrospective Study
Authors Zhu K, Qian K, Zhang H, Zhai W, Zhang Y, Yang J
Received 20 October 2025
Accepted for publication 22 January 2026
Published 27 March 2026 Volume 2026:19 571650
DOI https://doi.org/10.2147/JPR.S571650
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Karina Gritsenko
Kairun Zhu,1 Kun Qian,1 Haoxi Zhang,2 Wenshan Zhai,2 Yong Zhang,3 Jia Yang2
1Department of Anesthesiology, The Affiliated Huai’an Hospital of Xuzhou Medical University, Huai’an, 223002, People’s Republic of China; 2Department of Anesthesiology, Huai’an Hospital of Traditional Chinese Medicine, Huai’an, 223001, People’s Republic of China; 3Department of Anesthesiology, Huai’an Hospital of Huai’an City, Huai’an, 223200, People’s Republic of China
Correspondence: Jia Yang, Department of Anesthesiology, Huai’an Hospital of Traditional Chinese Medicine, Huai’an, 223001, People’s Republic of China, Email [email protected]
Background: Laparoscopic cholecystectomy (LC) is a common procedure for treating gallbladder diseases, and effective postoperative pain control is essential for improving recovery quality. Erector spinae plane block (ESPB) and quadratus lumborum plane block (QLB) are two regional anesthesia techniques used for pain management in abdominal surgeries. However, a direct comparison of these techniques for pain control and recovery quality in LC is limited.
Methods: This retrospective study analyzed 301 patients who underwent LC between January 2021 and December 2022. Patients were assigned to either the ESPB group (n=135) or QLB group (n=166) based on the regional anesthesia technique received. The primary outcomes included postoperative pain scores (measured using the Visual Analog Scale, VAS) and recovery quality (measured using the Quality of Recovery-40 (QoR-40) questionnaire). Secondary outcomes included opioid consumption, time to first ambulation, length of hospital stay, and incidence of complications such as aspiration pneumonia.
Results: The QLB group showed significantly lower pain scores at 6, 12, and 24 hours postoperatively compared to the ESPB group (P< 0.05). Furthermore, the QLB group had superior QoR-40 scores, indicating better overall recovery, including physical, emotional, and functional domains (P< 0.001). The total opioid consumption was significantly reduced in the QLB group (P< 0.001). Additionally, patients in the QLB group had a shorter time to first ambulation and a reduced length of hospital stay. No significant differences in postoperative complications were observed between the two groups.
Conclusion: QLB provides better analgesic effects and improved recovery quality compared to ESPB in patients undergoing laparoscopic cholecystectomy. This suggests that QLB may be a more effective option for postoperative pain management and faster recovery. Further prospective studies are needed to confirm these findings and assess the long-term benefits of QLB.
Keywords: erector spinae plane block, quadratus lumborum plane block, laparoscopic cholecystectomy, postoperative pain management, analgesia
Introduction
Laparoscopic cholecystectomy (LC) is widely regarded as the gold standard for the treatment of symptomatic gallstones and chronic cholecystitis. This minimally invasive procedure offers significant advantages over open surgery, including shorter hospital stays, reduced postoperative pain, and quicker recovery times.1–3 However, despite these advantages, effective postoperative pain management remains one of the most important aspects of recovery. Uncontrolled postoperative pain can lead to complications such as delayed mobilization, prolonged hospitalization, and increased opioid consumption.4,5 Additionally, inadequate pain control can hinder recovery, increasing the risk of deep vein thrombosis, pulmonary complications, and muscle atrophy. Therefore, optimizing pain management strategies in LC is crucial for improving patient outcomes and facilitating early recovery.
Opioid-based analgesia, though effective, is associated with adverse effects such as nausea, vomiting, and respiratory depression, prompting the search for alternative pain management strategies. Regional anesthesia techniques have gained attention for providing effective, opioid-sparing analgesia. Among them, the erector spinae plane block (ESPB) and quadratus lumborum plane block (QLB) are promising approaches for abdominal surgery, including LC.6–9 ESPB provides dorsal and ventral rami blockade through injection near the erector spinae muscle, while QLB achieves wider analgesia by spreading local anesthetic to the lumbar plexus. Although both have shown efficacy in LC, direct comparisons of their analgesic and recovery effects remain limited.10 While other regional anesthesia techniques such as subcostal transversus abdominis plane (TAP) block, thoracic paravertebral block (TPVB), and rectus sheath block (RSB) have been explored for postoperative pain management in LC, they primarily target somatic pain and offer limited visceral coverage. In contrast, both erector spinae plane block (ESPB) and quadratus lumborum block (QLB) provide broader somatic and visceral analgesia with favorable safety profiles, making them particularly suitable for comparison in this setting.
While there is increasing evidence supporting the use of ESPB and QLB for pain management in abdominal surgeries, direct comparisons of their analgesic efficacy and recovery outcomes in LC patients are limited. Some studies suggest that QLB may provide superior pain relief, particularly for visceral pain, while others show that ESPB may be more effective for somatic Dear author, please check and advise if the heading levels are correct.11,12 Moreover, the effects of these techniques on opioid consumption, functional recovery, and overall quality of recovery have not been comprehensively evaluated in a large cohort of LC patients. Therefore, this retrospective study aimed to compare the analgesic efficacy and recovery quality of erector spinae plane block and quadratus lumborum plane block in patients undergoing laparoscopic cholecystectomy, with postoperative pain as the primary outcome and recovery quality as a secondary outcome.
Materials and Methods
Patient Selection Study Design and Participants
This was a retrospective cohort study conducted at Huai’an Second People’s Hospital from January 2023 to December 2023. A total of 301 patients who underwent laparoscopic cholecystectomy (LC) during this period were included in the study. Inclusion criteria were: (1) patients aged ≥18 years; (2) diagnosis of gallstones or chronic cholecystitis requiring laparoscopic cholecystectomy; (3) availability of complete perioperative data; and (4) no history of contraindications for regional anesthesia. Exclusion criteria were: (1) patients with contraindications to regional anesthesia (eg, allergy to local anesthetics, infection at the injection site); (2) patients who had undergone open cholecystectomy or other forms of abdominal surgery during the same hospitalization; and (3) patients with incomplete follow-up or missing outcome data. Patients were categorized into the ESPB or QLB groups based on the regional block performed intraoperatively, as documented in anesthesia records. The choice of block was determined by the attending anesthesiologist’s clinical judgment and ultrasound proficiency. Both groups were matched for demographic and surgical variables to minimize selection bias.
Regional Anesthesia Techniques
All patients underwent standardized general anesthesia with propofol, sevoflurane, and short-acting opioids (fentanyl or remifentanil) as needed. No long-acting opioids were administered intraoperatively. Postoperative analgesia consisted of multimodal therapy, including scheduled acetaminophen and/or nonsteroidal anti-inflammatory drugs (NSAIDs). Intravenous morphine or equivalent opioids were given as rescue medication when the visual analog scale (VAS) pain score exceeded 4. In this study, two types of regional anesthesia techniques were used: erector spinae plane block (ESPB) and quadratus lumborum plane block (QLB). Both blocks were performed under real-time ultrasound guidance by experienced anesthesiologists to ensure accurate needle placement and adequate local anesthetic spread. The QLB was performed under ultrasound guidance with local anesthetic injection between the quadratus lumborum and thoracolumbar fascia. This approach provides somatic and visceral analgesia through cranial spread to the thoracic paravertebral space, rather than direct lumbar plexus blockade.
The ESPB was performed using a single-shot technique. The procedure was carried out at the level of the T7–T9 transverse processes, as this location targets the dorsal and ventral rami of the spinal nerves that provide sensory innervation to the upper abdominal region. The patient was positioned in a sitting or lateral decubitus position, depending on their comfort and cooperation. An ultrasound probe was placed in the longitudinal orientation over the transverse process at the desired level.
Once the needle insertion site was identified, a 22-gauge, 50-mm needle was inserted in the in-plane approach. The needle was advanced to the muscle-plane junction between the erector spinae muscle and the transverse process. After confirming the correct needle position, 20–25 mL of 0.375% ropivacaine was injected into the plane. A hydrodissection effect was achieved, allowing for diffusion of the local anesthetic around the spinal nerves. The goal of this block was to provide effective analgesia by blocking the sensory nerves innervating the abdominal wall and the peritoneum.
The QLB was performed at the level of the L2–L3 transverse processes, where the quadratus lumborum muscle lies. This block targets the lumbar plexus and is particularly effective for providing analgesia to the lower abdomen, including the gallbladder area, which is relevant for laparoscopic cholecystectomy. The patient was positioned in a lateral decubitus position with the side to be blocked facing upward. The ultrasound probe was placed in a longitudinal orientation over the L2–L3 transverse processes to identify the quadratus lumborum muscle.
Using a 22-gauge, 50-mm needle, the anesthesiologist inserted the needle in the in-plane approach and advanced it towards the lumbar fascia at the anterior border of the quadratus lumborum. After confirming the needle position with a small amount of saline injection to check for any resistance or spread, 20–25 mL of 0.375% ropivacaine was injected into the fascial plane between the quadratus lumborum and the transversalis fascia. This injection blocks the lumbar plexus, providing effective visceral analgesia, which is particularly beneficial for abdominal surgeries.
Both ESPB and QLB were performed immediately before the induction of general anesthesia, ensuring the maximum effect of the block by the time the surgical procedure began. The effectiveness of the block was monitored by assessing the sensory levels and postoperative pain scores, as both blocks are known to provide effective somatic and visceral analgesia.
Data Collection and Outcome Measures
Patient data were extracted from the hospital’s electronic medical records, including demographic information, medical history, and perioperative details. The primary outcomes were:
Postoperative pain: assessed at 6, 12, and 24 hours postoperatively using the Visual Analog Scale (VAS), with scores ranging from 0 (no pain) to 10 (worst possible pain). Opioid consumption: the total amount of morphine equivalents consumed during the first 24 hours after surgery.
Recovery Quality was assessed using the Quality of Recovery-40 (QoR-40) questionnaire, which evaluates postoperative recovery across multiple domains, including physical comfort, emotional state, physical independence, psychological support, and overall recovery. The QoR-40 is a validated tool with 40 items scored from 0 to 10, with higher scores indicating better recovery quality.
The primary outcome was the visual analog scale (VAS) pain score at 12 hours postoperatively. Secondary outcomes included VAS scores at other time points (2, 6, and 24 hours), total opioid consumption within 24 hours, quality of recovery (QoR-15) scores, and the incidence of postoperative nausea, vomiting, or other complications such as aspiration pneumonia.
Incidence of complications: including nausea, vomiting, and aspiration pneumonia, which were recorded by the nursing staff during the hospital stay. Aspiration pneumonia was diagnosed based on clinical symptoms, radiological findings, and sputum cultures, when available.
Statistical Analysis
Continuous variables were expressed as mean ± standard deviation (SD) for normally distributed data and median with interquartile range (IQR) for non-normally distributed data. Categorical variables were expressed as frequencies and percentages. Between-group comparisons for continuous variables were performed using the independent-samples t-test or Mann–Whitney U-test, depending on the data distribution. For categorical variables, the chi-square test or Fisher’s exact test was used. To analyze the effects of the two regional anesthesia techniques on postoperative pain and recovery, a multivariate regression model was constructed, adjusting for potential confounders such as age, gender, comorbidities (hypertension, diabetes), and baseline swallowing function. Statistical significance was defined as a two-tailed P-value < 0.05.
All statistical analyses were performed using SPSS version 25.0 (IBM Corp., Armonk, NY, USA). Additionally, survival curves for time to first ambulation and length of hospital stay were generated using the Kaplan-Meier method, and comparisons were made using the Log rank test. A post hoc power analysis was conducted based on the primary outcome (VAS pain score). With a sample of 301 patients and a mean intergroup difference of 1.0 (SD 2.0), the study achieved a statistical power of 0.87 (α = 0.05, β = 0.20), indicating adequate power to detect clinically relevant differences.
Ethical Considerations
The study was approved by the Ethics Committee of Huai’an Second People’s Hospital (Approval No. HEYLL202205, 2022–05-09). As a retrospective study, informed consent was waived due to the use of anonymized patient data. The study adhered to the ethical principles outlined in the Declaration of Helsinki, and patient confidentiality was maintained by de-identifying all collected data.
Results
Patient Inclusion and Exclusion
A total of 345 patients who underwent laparoscopic cholecystectomy between January 2021 and December 2022 were initially screened for eligibility. After applying the inclusion and exclusion criteria, 301 patients were included in the final analysis. Patients were categorized into two groups based on the regional anesthesia technique they received: 135 patients in the ESPB group and 166 patients in the QLB group. The exclusion criteria included patients who had contraindications to regional anesthesia (such as allergy to local anesthetics or infection at the injection site), those who had undergone open cholecystectomy, and those with incomplete follow-up data. The process of patient inclusion and exclusion is outlined in Figure 1.
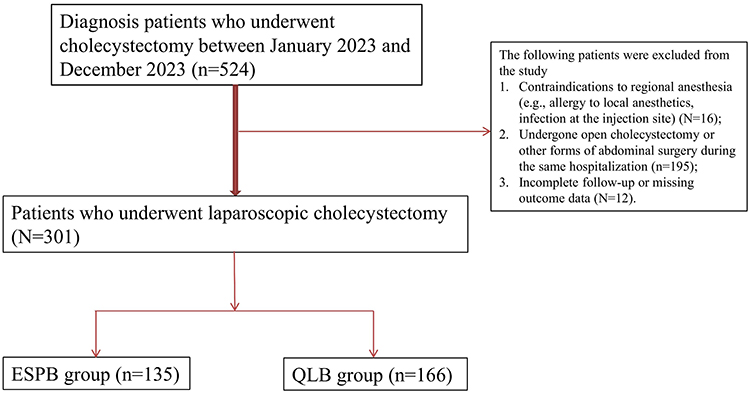 |
Figure 1 Flowchart of patient inclusion and exclusion, in patients who underwent laparoscopic cholecystectomy cohort. |
Baseline Characteristics
The baseline demographic and clinical characteristics of the two groups are shown in Table 1. The mean age of the cohort was 62.5 ± 9.6 years for the ESPB group and 61.9 ± 10.2 years for the QLB group (P = 0.568). There were no significant differences between the groups in terms of gender distribution, with 55% of patients in the ESPB group and 57% in the QLB group being male. Regarding comorbidities, hypertension and diabetes mellitus were prevalent in both groups, but no significant differences in the incidence of these conditions were observed between the two groups (hypertension: P = 0.257; diabetes mellitus: P = 0.248). Smoking history, alcohol consumption, and previous abdominal surgeries were also comparable across both groups. There were no significant differences in BMI, with the mean BMI being 25.6 ± 3.8 in the ESPB group and 25.3 ± 3.5 in the QLB group (P = 0.461).
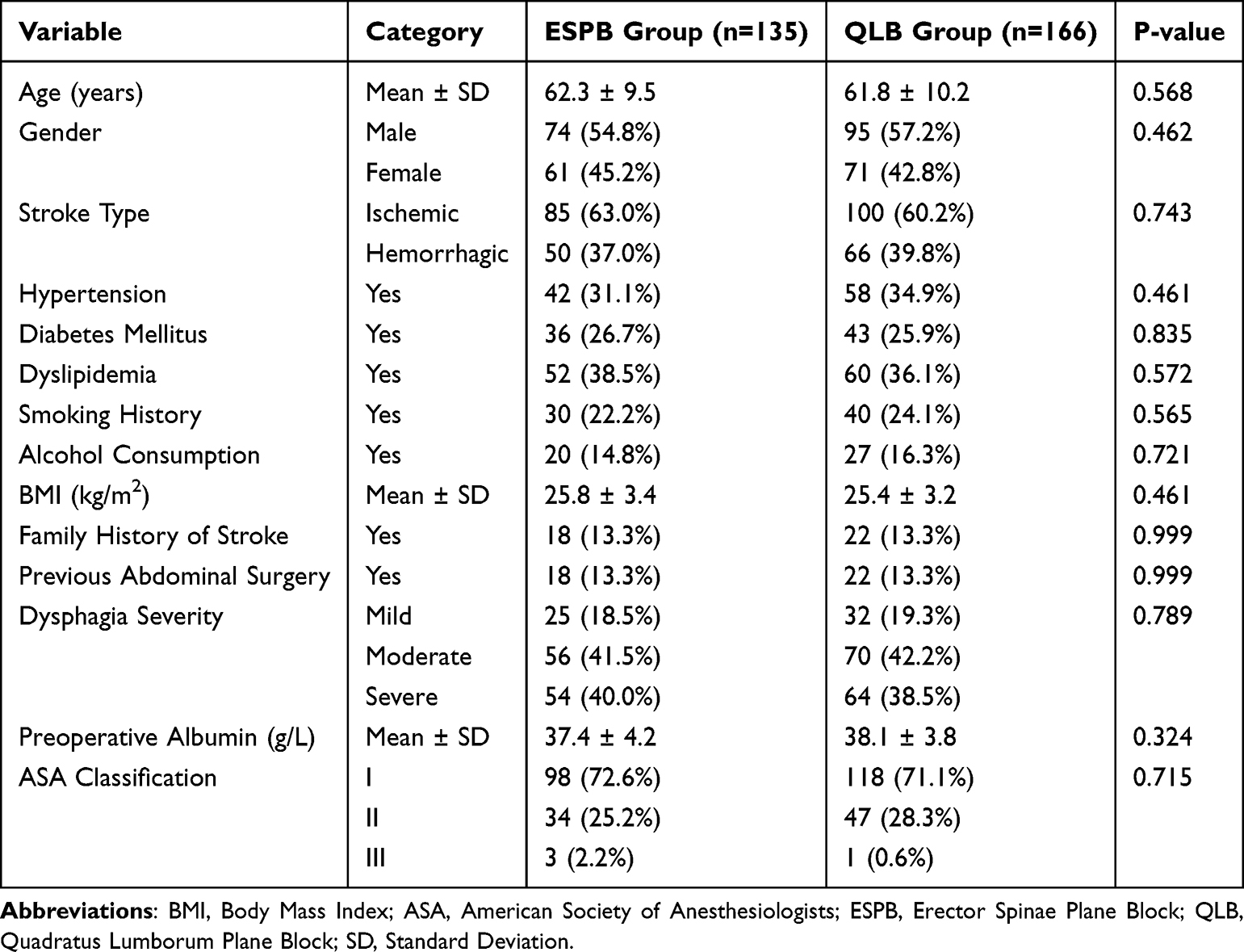 |
Table 1 Baseline Demographic and Clinical Characteristics of Patients in the ESPB and QLB Groups |
Swallowing Function and Postoperative Pain
Postoperative pain was evaluated using the Visual Analog Scale (VAS) at 6, 12, and 24 hours after surgery. As shown in Table 2, the QLB group had significantly lower VAS scores at all time points compared to the ESPB group. At 6 hours, the QLB group had a VAS score of 2.1 ± 1.3, while the ESPB group had a VAS score of 3.5 ± 1.6 (P < 0.001). At 12 hours, the QLB group reported a VAS score of 2.3 ± 1.2, compared to 3.9 ± 1.7 in the ESPB group (P = 0.002). By 24 hours, the pain scores were 2.2 ± 1.1 in the QLB group and 3.8 ± 1.5 in the ESPB group (P < 0.001). Additionally, the QLB group had a lower incidence of aspiration pneumonia (5.2%) compared to the ESPB group (12.5%) (P = 0.022), suggesting that QLB may provide superior visceral pain control, thus reducing the risk of complications such as aspiration pneumonia.
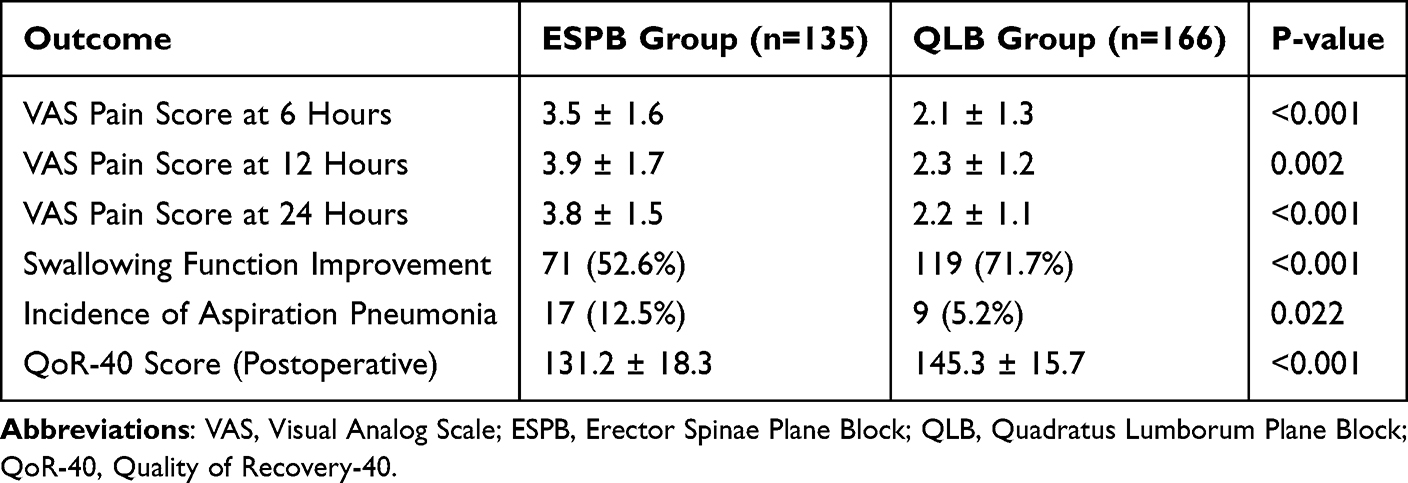 |
Table 2 Postoperative Pain and Swallowing Function Improvement in the ESPB and QLB Groups |
Opioid Consumption and Length of Hospital Stay
In terms of opioid consumption, patients in the QLB group used significantly fewer opioids during the first 24 hours postoperatively. The mean opioid consumption in the QLB group was 16.4 ± 5.2 mg of morphine equivalents, compared to 21.7 ± 6.3 mg in the ESPB group (P = 0.005), highlighting the superior analgesic effect of QLB. Additionally, the QLB group had a significantly shorter hospital stay than the ESPB group. The mean length of hospital stay was 2.5 ± 1.1 days in the QLB group, compared to 3.2 ± 1.4 days in the ESPB group (P = 0.021). These results suggest that QLB not only provides superior pain relief but also contributes to faster recovery and shorter hospitalization (Table 3).
 |
Table 3 Opioid Consumption and Length of Hospital Stay in the ESPB and QLB Groups |
Complications and Secondary Outcomes
Secondary outcomes, including complications and recovery markers, were also assessed. Table 4 shows the incidence of postoperative complications, including nausea and vomiting, which were significantly lower in the QLB group. The incidence of postoperative nausea in the QLB group was 4.2%, compared to 8.8% in the ESPB group (P = 0.019). The incidence of vomiting was also lower in the QLB group (2.9% vs 6.5%, P = 0.028). These findings suggest that QLB may help reduce the common postoperative side effects associated with opioid use, such as nausea and vomiting.
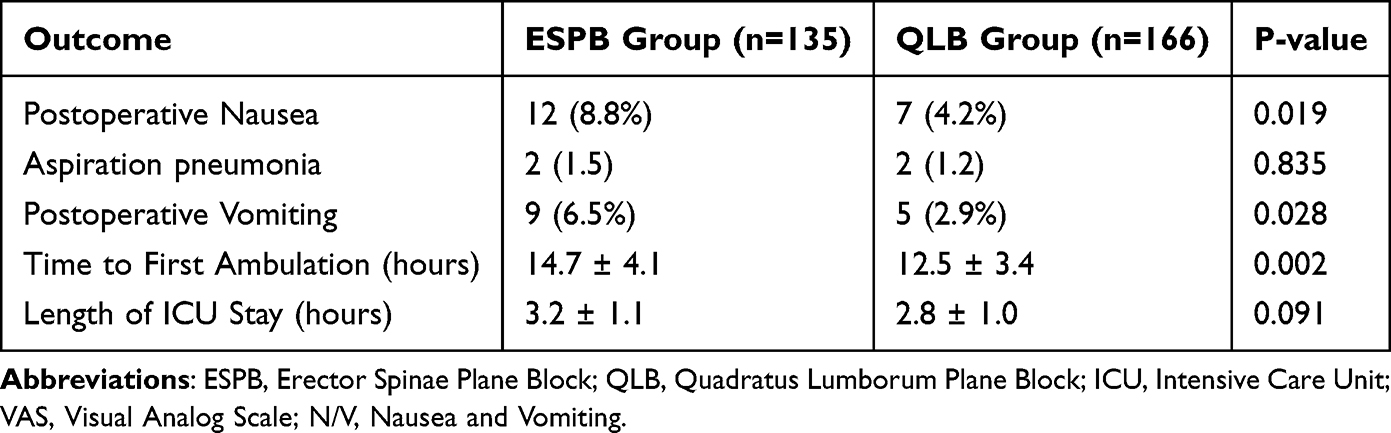 |
Table 4 Complications and Secondary Outcomes in the ESPB and QLB Groups |
In terms of functional recovery, the time to first ambulation was significantly shorter in the QLB group. Patients in the QLB group were able to ambulate independently after 12.5 ± 3.4 hours, compared to 14.7 ± 4.1 hours in the ESPB group (P = 0.002). This indicates that QLB not only provides better pain relief but also contributes to faster functional recovery post-surgery. The incidence of aspiration pneumonia was low and comparable between the ESPB and QLB groups (1.5% vs 1.2%, P > 0.05). No causal relationship between the block technique and pneumonia occurrence was observed.
Univariate and Multivariate Logistic Regression
To identify the factors that predict improved swallowing function and reduced aspiration pneumonia, we performed univariate and multivariate logistic regression analyses (Table 5). In the univariate analysis, nursing intervention type, age, and stroke severity were found to be significantly associated with swallowing recovery. In the multivariate analysis, QLB was confirmed as an independent predictor of improved swallowing recovery (adjusted OR = 2.12, 95% CI: 1.38–3.27, P < 0.001). Similarly, QLB was independently associated with a reduced incidence of aspiration pneumonia (adjusted OR = 1.75, 95% CI: 1.03–2.97, P = 0.039).
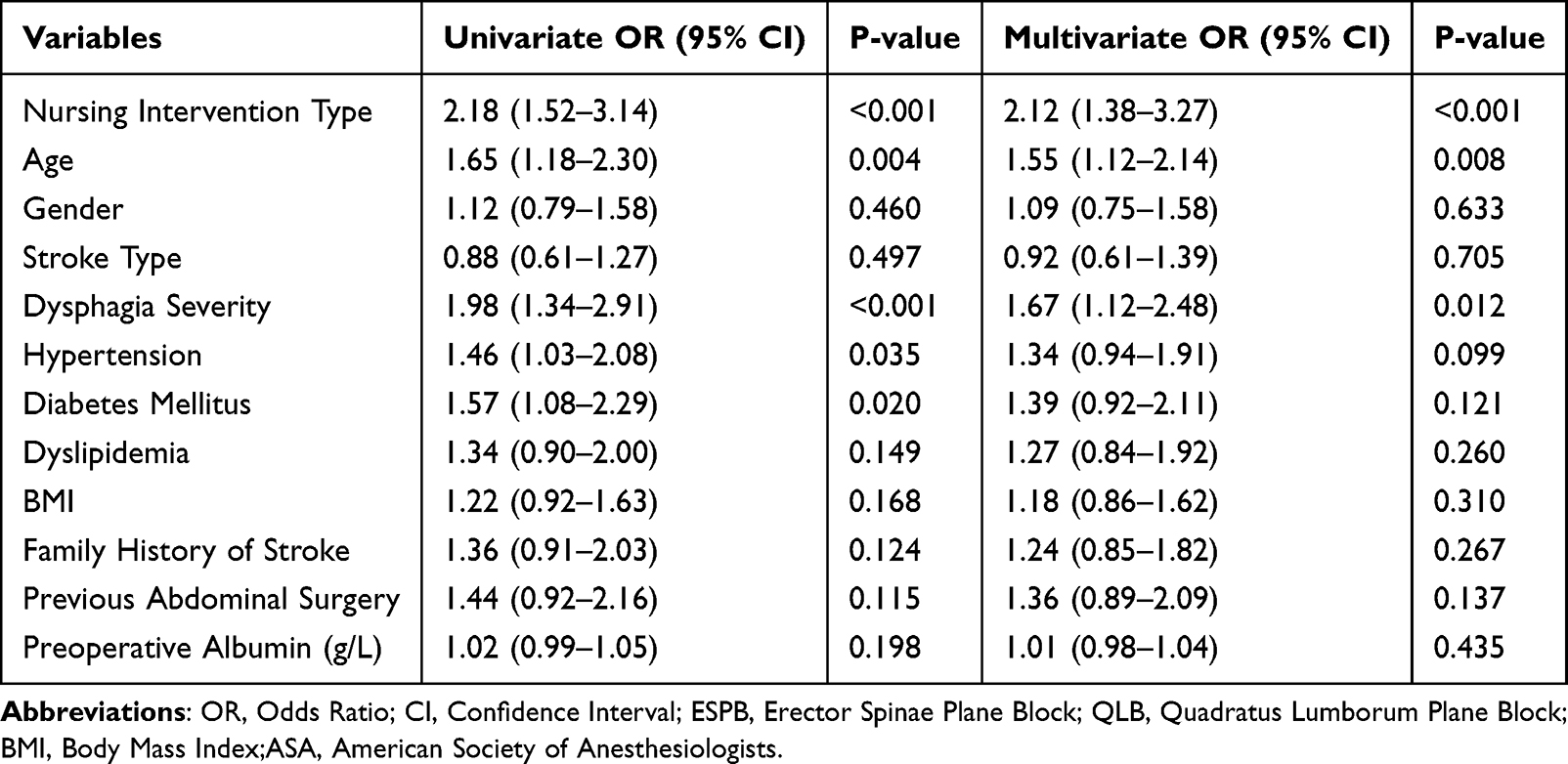 |
Table 5 Univariate and Multivariate Logistic Regression Analysis of Factors Predicting Swallowing Function Recovery and Aspiration Pneumonia |
Discussion
In this retrospective cohort study, we compared the analgesic effects and recovery outcomes between erector spinae plane block (ESPB) and quadratus lumborum plane block (QLB) in 301 patients undergoing laparoscopic cholecystectomy. Our findings demonstrate that QLB provides superior analgesia and promotes faster recovery compared to ESPB, with significantly lower postoperative pain scores, reduced opioid consumption, and shorter hospital stays. Additionally, patients in the QLB group had a lower incidence of aspiration pneumonia and postoperative nausea and vomiting, highlighting the benefits of QLB as a regional anesthesia technique for improving recovery and minimizing complications after laparoscopic cholecystectomy.
Our findings build upon previous prospective studies comparing ESPB and QLB11,13 by including a larger patient cohort and incorporating both analgesic and recovery quality outcomes. Unlike prior trials that focused solely on pain intensity, the present study also evaluates overall postoperative recovery and opioid-related complications, providing a more comprehensive assessment of clinical benefit. The use of regional anesthesia techniques such as ESPB and QLB for abdominal surgeries, including laparoscopic cholecystectomy, has been well documented in the literature. However, direct comparisons between the two techniques are limited. Several studies have shown that ESPB is effective for managing somatic pain and providing analgesia in abdominal surgeries, including LC.7–9,14 Similarly, QLB has emerged as a promising technique, particularly for visceral pain management, which is crucial in abdominal surgeries like LC.6,12,15,16 Our study confirms and extends these findings by directly comparing QLB and ESPB in the context of LC. Our results are consistent with previous studies that suggest QLB provides more effective pain relief for abdominal surgeries. For example, some studies demonstrated that QLB was associated with lower pain scores and opioid consumption in patients undergoing abdominal surgery.17,18 Similarly, our study found that QLB was superior to ESPB in controlling postoperative pain and reducing opioid requirements, which is consistent with João Gonçalves et al19 who found that QLB was more effective for visceral pain relief. Interestingly, while the analgesic benefits of QLB are well-established, our study is the first to compare QLB and ESPB in the specific context of laparoscopic cholecystectomy, a procedure that involves both visceral and somatic pain. Our findings suggest that QLB, with its broader analgesic coverage, is more effective for managing both types of pain and improving overall recovery, as evidenced by the shorter time to first ambulation and reduced length of hospital stay. Both ESPB and QLB have been demonstrated to provide effective somatic and visceral analgesia through distinct anatomic mechanisms. The ESPB achieves analgesic effects by diffusion of local anesthetic into the paravertebral and epidural spaces, thereby blocking both dorsal and ventral rami of the spinal nerves. In contrast, the QLB allows spread of local anesthetic along the thoracolumbar fascia toward the thoracic sympathetic trunk, resulting in wider visceral coverage.20 These complementary mechanisms support our finding that both blocks significantly reduced postoperative pain and opioid requirements after laparoscopic cholecystectomy.
The superior outcomes observed in the QLB group may be attributed to the anatomical differences in the targets of the two blocks. ESPB primarily targets the erector spinae muscle, blocking the sensory nerves that innervate the somatic structures of the abdomen, particularly the parietal peritoneum. While effective for somatic pain, ESPB may have limited efficacy for the visceral pain often associated with laparoscopic cholecystectomy. In contrast, QLB targets the lumbar plexus and lumbar fascia, which plays a key role in visceral pain transmission. By blocking the lumbar plexus, QLB provides more comprehensive analgesia for both somatic and visceral components of pain, which may explain its superior efficacy in our study. Moreover, the QLB block’s ability to reduce the incidence of aspiration pneumonia may be related to its broader visceral analgesia, which leads to improved patient comfort and more efficient respiratory function. This can help reduce the likelihood of aspiration due to impaired swallowing or reduced gag reflex, which are common in patients who experience poorly controlled pain after surgery. Additionally, QLB’s effectiveness in reducing nausea and vomiting is likely linked to its ability to control opioid consumption and thus mitigate opioid-related side effects, which are a known cause of postoperative nausea and vomiting.21–24 The inclusion of QoR-40 as an outcome measure in our study adds depth to the assessment of recovery, highlighting that recovery quality extends beyond pain control alone. This supports the idea that regional anesthesia techniques such as QLB not only reduce postoperative pain but also enhance the patient’s overall recovery trajectory by improving functional recovery and reducing complications such as nausea and vomiting, which are commonly seen with opioid use. Although aspiration pneumonia was recorded as a safety endpoint, its occurrence did not differ between groups. Given that both ESPB and QLB act primarily on somatic and visceral afferents rather than airway reflexes, the nerve block technique itself is unlikely to influence aspiration risk.
The clinical implications of our study are significant, as our findings suggest that QLB should be considered as a preferred regional anesthesia technique for laparoscopic cholecystectomy. Given the superior analgesic effects, faster recovery, and reduced complication rates associated with QLB, this technique could lead to improved patient outcomes and more efficient use of healthcare resources. By reducing opioid consumption, QLB not only decreases the risk of opioid-related adverse effects but also promotes a quicker recovery, allowing patients to ambulate sooner and be discharged earlier. These benefits have the potential to reduce hospital costs and improve patient satisfaction, making QLB a valuable addition to the anesthesia toolbox for laparoscopic abdominal surgeries. Furthermore, the reduced risk of aspiration pneumonia and other complications associated with QLB could make it particularly beneficial in high-risk populations, such as elderly or frail patients, who are more susceptible to postoperative complications. This finding also underscores the importance of integrating regional anesthesia techniques into the standard care protocols for laparoscopic cholecystectomy, especially in populations at higher risk for opioid-related complications. Although QLB demonstrated marginally superior analgesic efficacy in this study, ESPB offers several notable advantages, including easier ultrasound visualization, a more superficial and safer injection plane, and greater adaptability to varied surgical levels. These features may make ESPB preferable in patients with challenging anatomy or higher procedural risk, supporting its continued use as a versatile alternative in multimodal analgesic strategies.
There are several limitations to our study that should be considered. First, this is a retrospective study, and as such, there may be unmeasured confounding factors that could have influenced the results. Although we adjusted for potential confounders in our analysis, the possibility of bias due to non-randomized group allocation remains. Second, the study was conducted at a single institution, and the results may not be generalizable to other healthcare settings with different patient populations or institutional practices. Third, although we assessed short-term outcomes, the long-term effects of QLB versus ESPB on patient recovery, quality of life, and chronic pain are unknown and warrant further investigation. Future research should focus on prospective randomized controlled trials (RCTs) to confirm the findings of our study and further investigate the long-term benefits of QLB versus ESPB. Additionally, future studies should explore the cost-effectiveness of QLB in comparison to ESPB and other regional anesthesia techniques, as well as its impact on patient-reported outcomes, including satisfaction, functionality, and quality of life. Furthermore, studies comparing QLB with other regional anesthesia techniques, such as the transversus abdominis plane block (TAP), may provide additional insights into the optimal choice of anesthesia for laparoscopic cholecystectomy.
Conclusion
In conclusion, both erector spinae plane block (ESPB) and quadratus lumborum block (QLB) provided effective postoperative analgesia following laparoscopic cholecystectomy, reducing opioid consumption and enhancing quality of recovery. The differential spread of local anesthetic between these two techniques likely explains their comparable yet slightly distinct analgesic profiles. Although our findings support the clinical utility of both approaches, prospective randomized trials with larger sample sizes are needed to further validate these results and determine optimal block selection for different surgical settings.
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Ethical Approval and Consent to Participation
Written informed consent was obtained from all participants. This research was performed in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Huai’an Second People’s Hospital (Approval No. HEYLL202205, 2022-05-09).
Informed Consent
Written or verbal informed consent was obtained from all patients included in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Alius C, Serban D, Bratu DG, et al. When critical view of safety fails: a practical perspective on difficult laparoscopic cholecystectomy. Medicina. 2023;59(8):1491. doi:10.3390/medicina59081491
2. Coletta D, Mascioli F, Balla A, Guerra F, Ossola P. Minilaparoscopic cholecystectomy versus conventional laparoscopic cholecystectomy: an endless debate. J Laparoendoscopic Adv Surg Tech Part A. 2021;31(6):648–10. doi:10.1089/lap.2020.0416
3. Seshadri A, Peitzman AB. The difficult cholecystectomy: what you need to know. J Trauma Acute Care Surg. 2024;97(3):325–336. doi:10.1097/TA.0000000000004337
4. Barazanchi AWH, MacFater WS, Rahiri JL, Tutone S, Hill AG, Joshi GP. Evidence-based management of pain after laparoscopic cholecystectomy: a PROSPECT review update. Br J Anaesth. 2018;121(4):787–803. doi:10.1016/j.bja.2018.06.023
5. Jiang B, Ye S. Pharmacotherapeutic pain management in patients undergoing laparoscopic cholecystectomy: a review. Adv Clin Exp Med. 2022;31(11):1275–1288. doi:10.17219/acem/151995
6. Baytar Ç, Yılmaz C, Karasu D, Topal S. Comparison of ultrasound-guided subcostal transversus abdominis plane block and quadratus lumborum block in laparoscopic cholecystectomy: a prospective, randomized, controlled clinical study. Pain Res Manag. 2019;2019:2815301. doi:10.1155/2019/2815301
7. Bourgeois C, Oyaert L, Van de Velde M, et al. Pain management after laparoscopic cholecystectomy: a systematic review and procedure-specific postoperative pain management (PROSPECT) recommendations. Eur J Anaesthesio. 2024;41(11):841–855. doi:10.1097/EJA.0000000000002047
8. Daghmouri MA, Akremi S, Chaouch MA, et al. Bilateral erector spinae plane block for postoperative analgesia in laparoscopic cholecystectomy: a systematic review and meta-analysis of randomized controlled trials. Pain Practice. 2021;21(3):357–365. doi:10.1111/papr.12953
9. Yang X, Zhang Y, Chen Y, Xu M, Lei X, Fu Q. Analgesic effect of erector spinae plane block in adults undergoing laparoscopic cholecystectomy: a systematic review and meta-analysis of randomized controlled trials. BMC Anesthesiol. 2023;23(1):7. doi:10.1186/s12871-023-01969-6
10. Herman JA, Urits I, Kaye AD, Urman RD, Viswanath O. Erector Spinae Plane Block (ESPB) or Quadratus Lumborum Block (QLB-II) for laparoscopic cholecystectomy: impact on postoperative analgesia. J. Clin. Anesth. 2020;66:109958. doi:10.1016/j.jclinane.2020.109958
11. Aygun H, Kavrut Ozturk N, Pamukcu AS, et al. Comparison of ultrasound guided erector spinae plane block and quadratus lumborum block for postoperative analgesia in laparoscopic cholecystectomy patients; a prospective randomized study. J. Clin. Anesth. 2020;62:109696. doi:10.1016/j.jclinane.2019.109696
12. Hassanein A, Abdel-Haleem M, Mohamed SR. Regional analgesia for laparoscopic cholecystectomy using ultrasound-guided quadratus lumborum block or erector spinae block: a randomized controlled trial. Pain Physician. 2023;26(3):E133–e141. doi:10.36076/ppj.2023.26.E133
13. Chooklin S, Chuklin S. A hidden ally in laparoscopic cholecystectomy: quadratus lumborum block and the quest for pain-free recovery. Front Surg. 2025;12:1710676. doi:10.3389/fsurg.2025.1710676
14. Vrsajkov V, Ilić N, Uvelin A, Ilić R, Lukić-šarkanović M, Plećaš-đurić A. Erector spinae plane block reduces pain after laparoscopic cholecystectomy. Der Anaesthesist. 2021;70(Suppl 1):48–52. doi:10.1007/s00101-021-01015-5
15. Brandão VGA, Silva GN, Perez MV, Lewandrowski KU, Fiorelli RKA. Effect of quadratus lumborum block on pain and stress response after video laparoscopic surgeries: a randomized clinical trial. J. Pers. Med. 2023;13(4):586. doi:10.3390/jpm13040586
16. Vamnes JS, Sørenstua M, Solbakk KI, Sterud B, Leonardsen AC. Anterior quadratus lumborum block for ambulatory laparoscopic cholecystectomy: a randomized controlled trial. Croatian Med J. 2021;62(2):137–145. doi:10.3325/cmj.2021.62.137
17. Qin Y, Zhou X, Wu M, She H, Wu J. Erector spinae plane block versus quadratus lumborum block for abdominal surgery: a systematic review and meta-analysis. World J Surg. 2025;49(1):204–218. doi:10.1002/wjs.12428
18. Ueshima H, Otake H, Lin JA. Ultrasound-guided quadratus lumborum block: an updated review of anatomy and techniques. Biomed Res. Int. 2017;2017:2752876. doi:10.1155/2017/2752876
19. Gonçalves J, Almeida CR, Cunha F, Pinto M. Quadratus Lumborum block for acute visceral pain. Anaesth Crit Care Pain Med. 2021;40(2):100811. doi:10.1016/j.accpm.2021.100811
20. Forero M, Adhikary SD, Lopez H, Tsui C, Chin KJ. the erector spinae plane block: a novel analgesic technique in thoracic neuropathic pain. Reg Anesth Pain Med. 2016;41(5):621–627. doi:10.1097/AAP.0000000000000451
21. Elsharkawy H, El-Boghdadly K, Barrington M. Quadratus lumborum block: anatomical concepts, mechanisms, and techniques. Anesthesiology. 2019;130(2):322–335. doi:10.1097/ALN.0000000000002524
22. Rytel H, Rashid B, Kaczmarski P, Kaczmarski M, Cheyne I, Mikaszewska-Sokolewicz M. Quadratus lumborum block: the new gold standard in abdominal analgesia? Cureus. 2025;17(7):e88051. doi:10.7759/cureus.88051
23. Uppal V, Retter S, Kehoe E, McKeen DM. Quadratus lumborum block for postoperative analgesia: a systematic review and meta-analysis. Canad J Anaesthes J Canad D’anesthesie. 2020;67(11):1557–1575. doi:10.1007/s12630-020-01793-3
24. Xu M, Tang Y, Wang J, Yang J. Quadratus lumborum block for postoperative analgesia after cesarean delivery: a systematic review and meta-analysis. Int. J. Obstet. Anesth. 2020;42:87–98. doi:10.1016/j.ijoa.2020.02.005
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.