Back to Journals » Open Access Emergency Medicine » Volume 14
Comparison of Sustained Return of Spontaneous Circulation Rate Between Manual and Mechanical Chest Compression in Adult Cardiac Arrest
Authors Tantarattanapong S ![]() , Chantaramanee K
, Chantaramanee K
Received 6 May 2022
Accepted for publication 19 October 2022
Published 2 November 2022 Volume 2022:14 Pages 599—608
DOI https://doi.org/10.2147/OAEM.S373669
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Hans-Christoph Pape
Siriwimon Tantarattanapong, Kwanchanok Chantaramanee
Department of Emergency Medicine, Songklanagarind Hospital, Faculty of Medicine, Prince of Songkla University, Hat Yai, Songkhla, Thailand
Correspondence: Siriwimon Tantarattanapong, Department of Emergency Medicine, Songklanagarind Hospital, Faculty of Medicine, Prince of Songkla University, Hat Yai, Songkhla, 90110, Thailand, Tel +66 74-451705, Fax +66 74-451704, Email [email protected]
Objective: This study aimed to compare the rates of sustained return of spontaneous circulation (ROSC) between manual and mechanical chest compression in adult non-traumatic cardiac arrest.
Methods: A retrospective cohort study was conducted from 2017 to 2019. The medical records were reviewed in 227 cardiac arrest patients aged ≥ 18 years who experienced out-of-hospital cardiac arrest or cardiac arrest while visiting the emergency department (ED). The patients were divided into manual chest compression and mechanical chest compression groups. The two groups were compared in terms of baseline characteristics, time to arrive at the ED, time to basic life support, initial rhythm, time to defibrillation in the shockable group, time to the first dose of adrenaline, and possible cause of arrest. A multivariate logistic regression model was used to determine the factors associated with ROSC.
Results: A total of 227 patients met the inclusion criteria:193 patients in the manual chest compression group and 34 patients in the mechanical chest compression group. The rate of sustained ROSC in the manual chest compression group was higher (43% vs 8.8%; P < 0.001). The significant factors associated with ROSC were witnessed cardiac arrest (odds ratio (OR) = 3.41; 95% confidence interval (CI) 0.94– 12.4), ED arrival by basic ambulance service (OR = 1.93; 95% CI 0.86– 4.35), cardiac arrest at the ED (OR = 3.69; 95% CI 1.73– 7.88), and cardiac arrest from hypoxia (OR = 2.01; 95% CI 1.02– 3.97).
Conclusion: Mechanical chest compression was not associated with sustained ROSC and tended to be selectively used in patients with a prolonged duration of cardiac arrest.
Keywords: mechanical chest compression, sustained return of spontaneous circulation, cardiac arrest
Plain Language Summary
What is already known on this topic.
The use of mechanical piston devices may be considered in specific settings where the delivery of high-quality manual compressions may be challenging for the provider (eg, limited availability of rescuers, prolonged CPR, in a moving ambulance, and in the angiography suite).
What this study adds.
The CPR outcome of mechanical chest compression may be associated with the cause of cardiac arrest and duration to apply the system.
Introduction
Cardiac arrest is a national and global health problem. Worldwide cardiac arrest was reported to be more than 3.7 million cases a year.1 Cardiac arrest patients need immediate emergency care and high-quality cardiopulmonary resuscitation (CPR) for an increased chance of survival. The American Heart Association (AHA) has indicated that high quality CPR consists of chest compression that is 5–6 cm in depth at a rate of 100–120 times/min that allows for full recoil of the chest wall with assisted ventilation at 10 times/min and minimal interruption.2
Fatigue of the rescuers can occur, which causes inadequate high-quality chest compression.3 A suboptimal rate of chest compression is associated with a poor return of spontaneous circulation (ROSC).4 In an attempt to improve perfusion during resuscitation, mechanical chest compression systems have been developed.5 The devices are designed to perform at a continuous specified rate and depth of chest compression.
The AHA 2019 guideline recommends that manual chest compression continue to be the standard but a mechanical chest compression system is a reasonable alternative when used by personnel who have been properly trained.5 The LINC randomized trial and the PARAMEDIC trial were two randomized trials that compared mechanical chest compression in out-of-hospital cardiac arrest (OHCA) with manual chest compression.6,7 The results of these trials showed that the survival rate in mechanical chest compression was not superior to manual chest compression. A systematic review and meta-analysis of mechanical chest compression systems was conducted in in-hospital cardiac arrest settings. The results showed an increased rate of ROSC and survival.8 There were no differences in life-threatening complications such as rib fracture, lung contusion, and pneumothorax between manual and mechanical chest compression. However, the rate of chest wall abrasion was higher in the application of mechanical chest compression systems.9–12
The emergency department (ED) at Songklanagarind Hospital has used the LUCAS-3 mechanical chest compression system since August 2018. This study aimed to determine the sustained ROSC rate between manual chest compression and mechanical chest compression in both OHCA patients and patients who experienced in-hospital cardiac arrest at the ED.
Materials and Methods
Study Design and Setting
A retrospective chart review was conducted at the ED of Songklanagarind Hospital, which is a university hospital and regional referral center in southern Thailand.
Pre-Implementation of the Mechanical Chest Compression Phase
When OHCA occurs, the dispatch center coordinates with the nearest available response team, such as a basic ambulance. Usually, an advanced ambulance is immediately dispatched. If there is evidence of death, such as rigor mortis, or the patient has a “do not attempt resuscitation” order and the relatives understand and consent with the order, the ambulance staff are authorized to recognize death and to stop CPR. Otherwise, the patients are transported to the appropriate nearby hospital with prehospital notification. When the patients arrive at the ED, the CPR team, which consists of an anesthesiologist, surgeons, and internists, promptly performs CPR. In patients who experience cardiac arrest at the ED, the emergency physicians (EP) perform CPR immediately and activate the CPR team. The hospital CPR guideline follows AHA 2015 and the members of the CPR team are qualified. These patients were analyzed in the manual chest compression group. Data were collected from June 2017 to July 2018.
Implementation the Mechanical Chest Compression Phase
The LUCAS-3 mechanical chest compression system has been used since August 2018. Before the chest compression system is implemented on patients, the paramedics and EPs are trained. Training is based on the manufacturer’s guidelines. Training includes protocols and procedures for proper use of the system to obtain high-quality CPR. Training is performed by hands-on mechanical chest compression practice with a CPR manikin with emphasis on rapid application and minimal interruption of CPR. Indications to implement the mechanical chest compression system consist of (1) adult non-traumatic cardiac arrest and (2) ability of the patient to fit the system. Contraindications are traumatized cardiac arrest, pediatric patient, pregnancy, and chest wall diameter or width not suitable for the system. The timing to apply mechanical chest compression is not strict in the implementation protocol. The important concept is to never delay chest compression and defibrillation with minimal interruption of chest compressions. All patients begin with manual chest compression and change to mechanical chest compression based on the team’s decision.
In the case OHCA patients, mechanical chest compression is used at the scene by an advanced ambulance and during transfer to the appropriate hospital. Patients who experience OHCA and arrive at the ED by relatives or a basic ambulance may start with manual CPR and continue with manual CPR or switch to mechanical chest compressions at the ED. Both types of these patients with OHCA were analyzed in the mechanical chest compression group.
In the case of cardiac arrest at the ED, basic life support is started immediately and early advanced life support is given by the CPR team. The application of mechanical chest compression is done by the team. The data for the mechanical chest compression group were collected from August 2018 to July 2019.
Post-Cardiac Arrest Care
After ROSC, post-cardiac arrest cases are managed and the patients are intensively monitored by the CPR team and post-cardiac arrest team.
Ethics Approval
Ethics approval was obtained from the Institutional Ethics Committee Board of the Faculty of Medicine at Prince of Songkla University (EC 62–254-20-4). This study was conducted in accordance with the declaration of Helsinki. According to our institutional review board protocol, the requirement for informed consent was waived because the research presented no more than minimal risk to participants and involved no procedures for which written consent is normally required outside the research context. All research information was kept confidential in an encrypted file with a password with limited access to the data by only the researcher and assistant.
Study Population
The inclusion criteria were: (1) adult non-traumatic cardiac arrest patients aged ≥18 years; (2) received CPR in the ED of Songklanagarind Hospital; and (3) OHCA and in-hospital cardiac arrest patients in the ED. The exclusion criteria were: (1) traumatic cardiac arrest patients; (2) pregnant patients; (3) patients who had a “do not attempt resuscitation” order; (4) incomplete medical records; and (5) patients referred to other hospitals.
Data Collection
The data collected from the medical records included age, sex, comorbidity, location of cardiac arrest, type of ED arrival, bystander CPR, time of cardiac arrest to basic life support (BLS), time of cardiac arrest to advanced cardiac life support (ACLS), initial rhythm, time of first dose of adrenaline, and causes of cardiac arrest. The outcome of CPR consisted of sustained ROSC (defined as 20 consecutive minutes with palpable pulse),13 survival to hospital admission, survival to hospital discharge, and survival to hospital discharge with good neurological outcome. Good neurological outcome was defined as a Cerebral Performance Category score of 1 or 2.14 Mechanical chest compression device complications were recorded.
Outcome Measurements
The primary outcome was the rate of sustained ROSC between manual chest compression and mechanical chest compression. The secondary outcomes were factors associated with sustained ROSC.
Statistical Analysis
The statistical analysis was conducted using R software version 3.6.1. Continuous variables were analyzed and are reported as median, while discrete variables are reported as percentage. All data were based on non-parametric frequency distributions. A univariate model analyzed the baseline characteristics, type of transport, location of arrest, ED time of arrival, initial rhythm, possible cause of arrest, and CPR outcome. The data were compared in subjects who had either manual or mechanical chest compression. Continuous variables were compared using the Mann–Whitney U-test. Categorical variables were compared using the χ2 or Fisher’s exact test as indicated. Selected variables with P-values <0.2 were introduced into a multivariate logistic regression model for secondary outcomes. The odds ratio (OR) for the outcomes and the 95% confidence interval (CI) were used to identify significant factors associated with sustained ROSC. Results are shown as two-tailed and a P-value <0.05 was selected as the level of statistical significance.
Results
A total of 308 patients during the study period had cardiac arrest and received CPR at the ED. The number of patients who met the inclusion criteria was 227 (Figure 1).
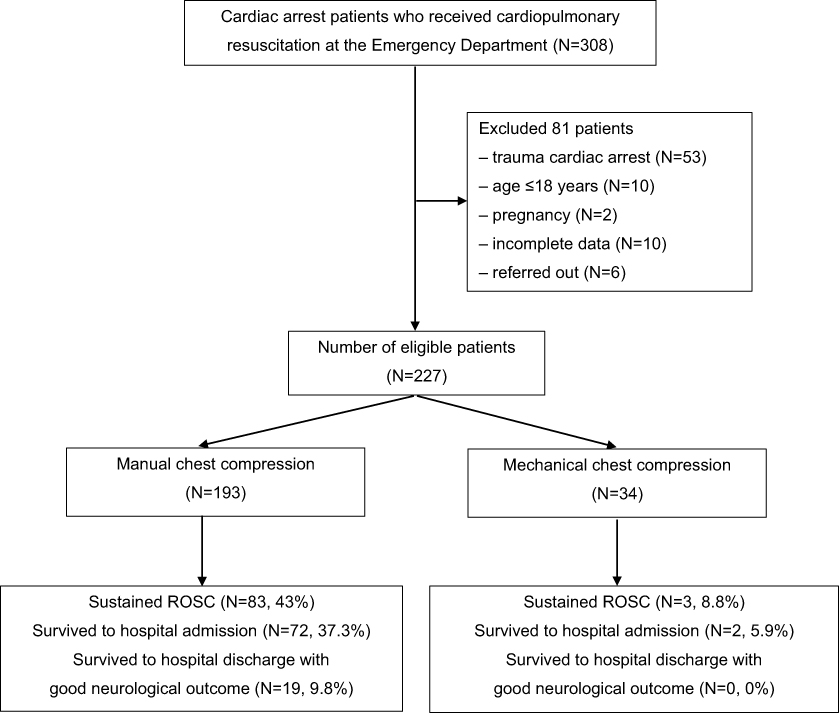 |
Figure 1 Patient flow chart. |
The baseline characteristics, initial management, and causes of cardiac arrest are shown in Table 1. The manual chest compression patients were older than the mechanical chest compression patients (68 vs 59 years; P = 0.010). There was no statistically significant difference of comorbidities between the two groups. However, the mechanical chest compression group had a higher percentage of patients with underlying heart disease than the manual chest compression group (38.2% vs 29.5%; P = 0.417). OHCA was greater in the mechanical chest compression (94.1% vs 70.5%; P = 0.007). Most of the patients in the mechanical CPR group arrived at the ED by advanced ambulance, whereas a smaller percentage of patients in the manual chest compression group arrived by advanced ambulance (76.5% vs 43.5%; P = 0.001). The manual chest compression patients had more bystander CPR than the mechanical chest compression patients (50.3% vs 23.5%; P = 0.007). The time from onset of cardiac arrest to providing advanced cardiac life support (ALCS) in the manual chest compression group was less than in the mechanical chest compression group (8 vs 26 min; P < 0.001). Also, the time from cardiac arrest to the first dose of adrenaline was faster in the manual chest compression group than in the mechanical chest compression group (11 vs 30 min; P < 0.001). The possible causes of arrest in both groups were not much different except for hypoxia and hyperkalemia. In the manual chest compression patients, hypoxia was more than in the mechanical chest compression patients (38.9% vs 11.8%; P = 0.004) and hyperkalemia was less than in the mechanical chest compression patients (11.9% vs 26.5%; P = 0.033).
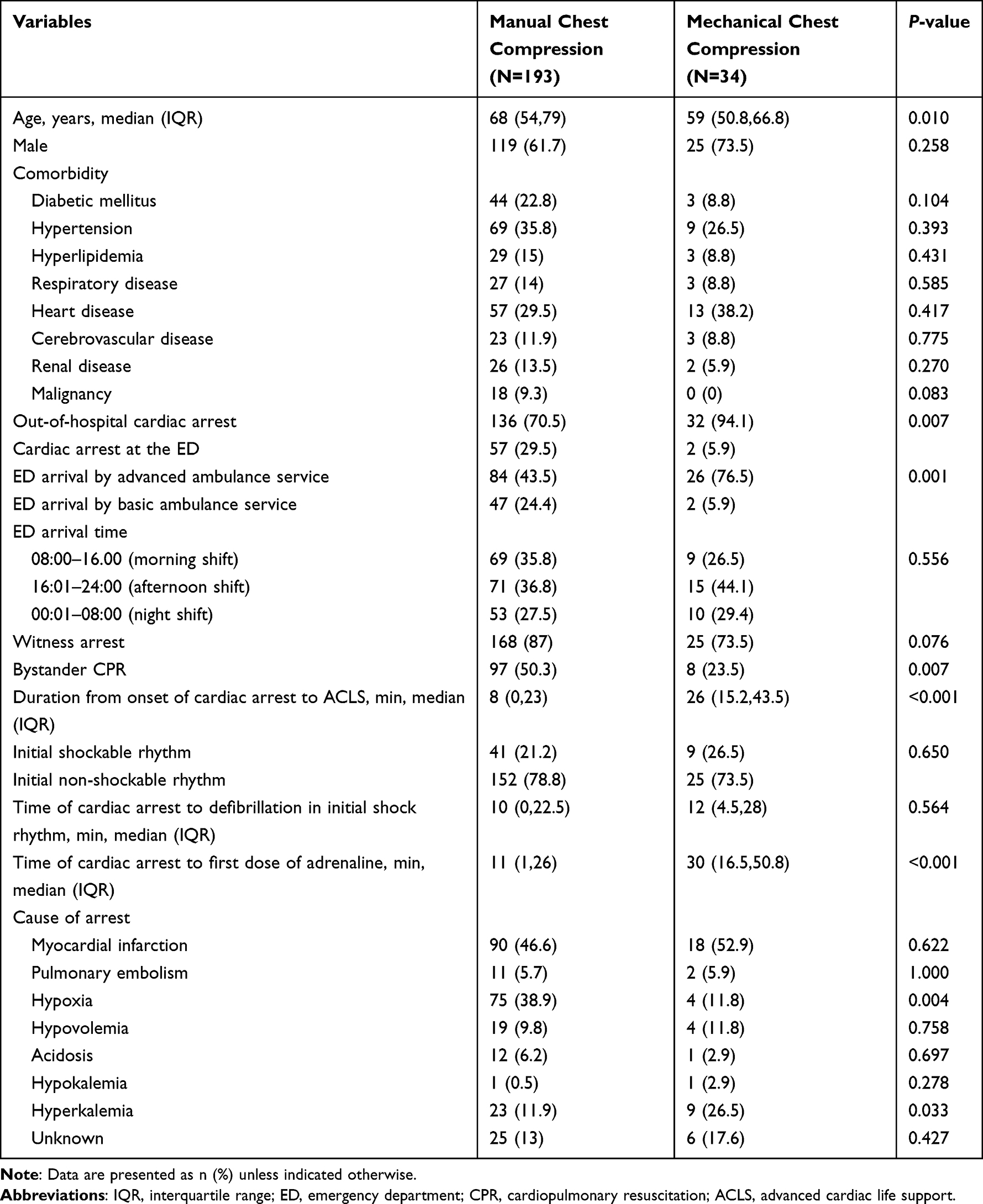 |
Table 1 Baseline Characteristics, Initial Management and Causes of Cardiac Arrest |
A comparison of the outcomes of the manual chest compression and mechanical chest compression groups are shown in Table 2. The rate of sustained ROSC in the manual chest compression group was higher (43% vs 8.8%; P < 0.001).
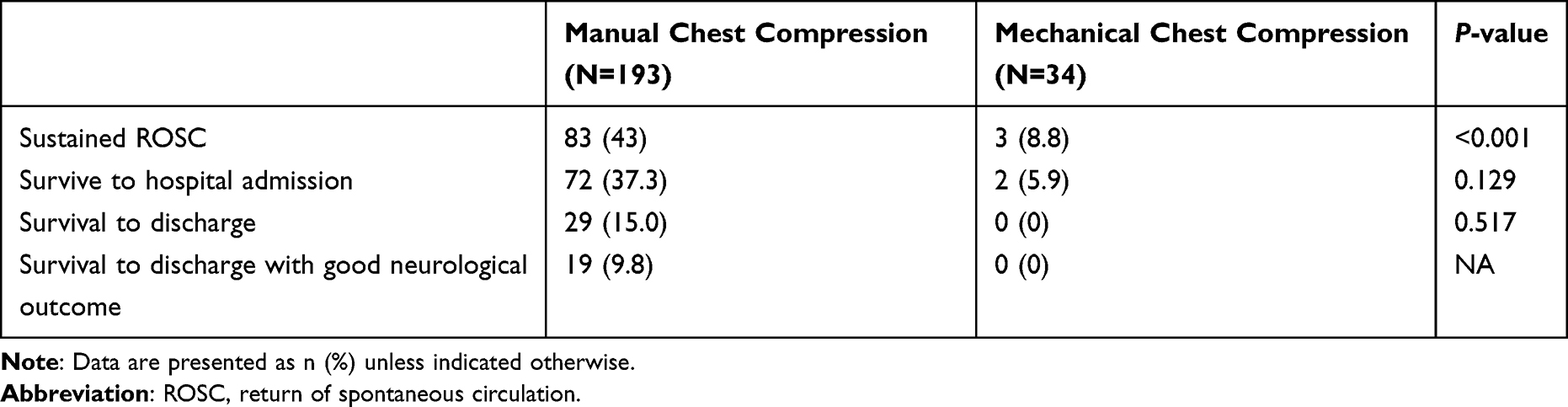 |
Table 2 Outcomes of Cardiopulmonary Resuscitation |
In this study, mechanical chest compression was performed more often by third-year residents (Table 3). The median time from cardiac arrest to mechanical chest compression was 37.5 min. Complications of mechanical chest compression, which included chest wall abrasion, contusion, and a circle mark on the chest wall, occurred in 17.6% of patients.
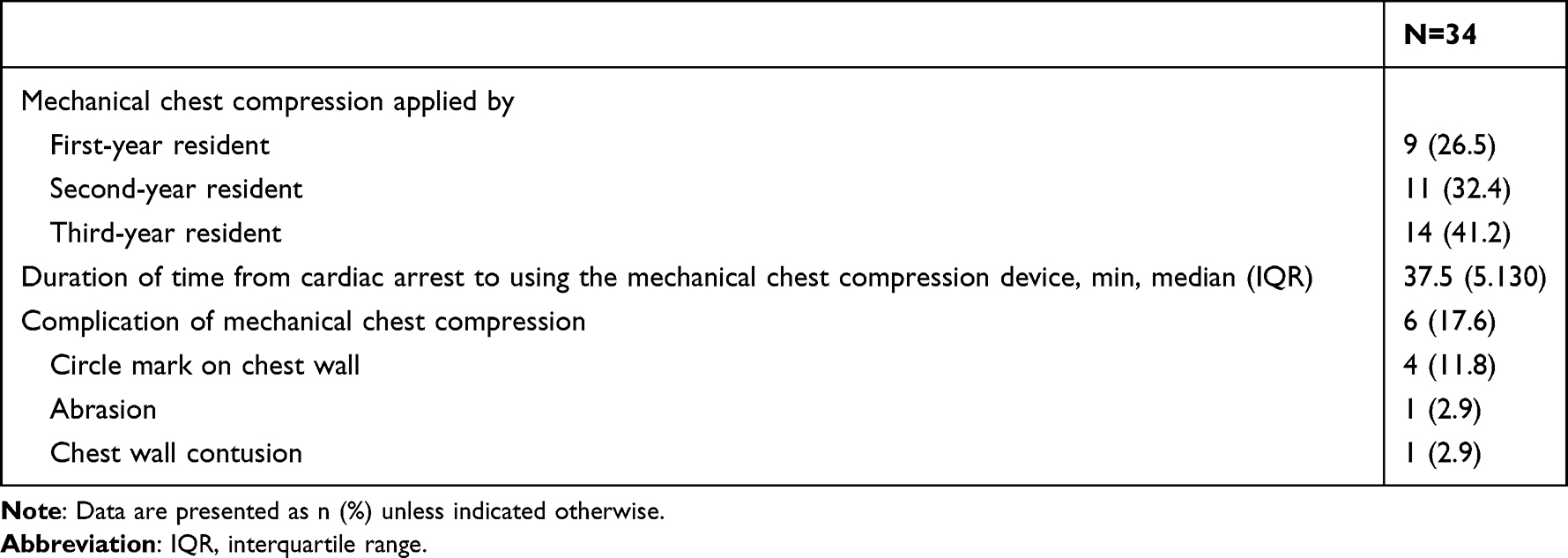 |
Table 3 Application and Complications of Mechanical Chest Compression |
In a subgroup analysis of patients with OHCA, the baseline characteristics, initial management, and causes of cardiac arrest are shown in Table 4. There was a statistical difference in the manual chest compression and mechanical chest compression groups in patients with underlying diabetes mellitus (27.9% vs 9.4%; P = 0.049, respectively). Patients in the manual chest compression group arrived earlier at the ED than patients in the mechanical chest compression group (24 vs 44 min; P < 0.001), while a greater percentage in the mechanical chest compression group arrived by advanced ambulance service (78.1% vs 55.1%; P = 0.029). The times from the onset of cardiac arrest to the times of BLS and ALCS in the manual chest compression patients were less than in the mechanical chest compression patients (5 vs 10 min; P < 0.001 and 16 vs 28 min; P = 0.002, respectively). Also, the time from cardiac arrest to the first dose of adrenaline was faster in the manual chest compression patients than in the mechanical chest compression patients (18 vs 30 min; P = 0.001). The possible causes of arrest in both groups were not much different except hypoxia was higher in the manual chest compression patients (40.4% vs 12.5%; P = 0.006). Sustained ROSC was higher in the manual chest compression patients (30.1% vs 9.4%; P = 0.029).
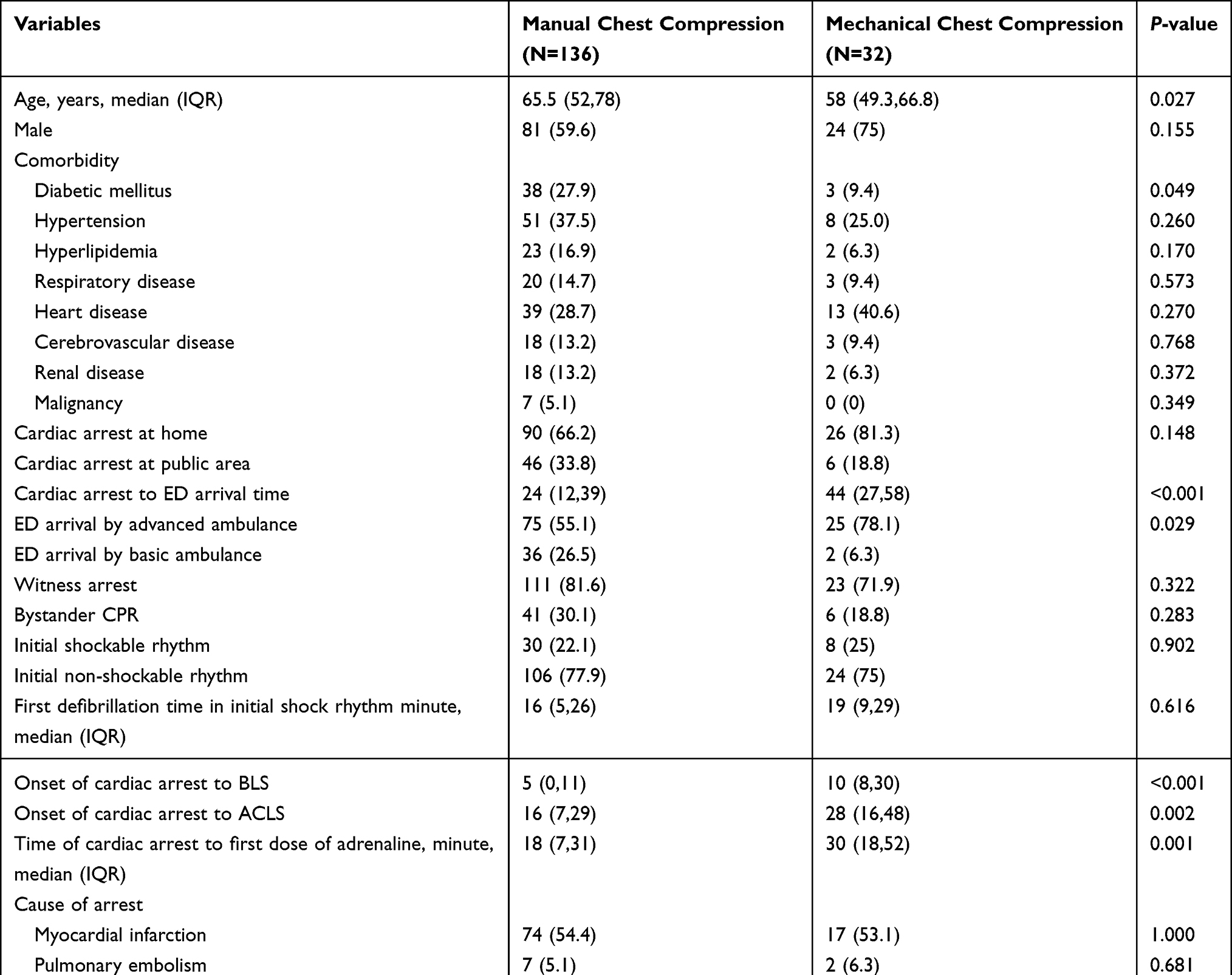 |
Table 4 Out-of-Hospital Cardiac Arrest |
Significant factors associated with sustained ROSC were witnessed cardiac arrest (OR = 3.41; 95% CI 0.94–12.4), ED arrival by basic ambulance service (OR = 1.93; 95% CI 0.86–4.35), cardiac arrest at the ED (OR = 3.69; 95% CI 1.73–7.88), and cardiac arrest from hypoxia (OR = 2.01; 95% CI 1.02–3.97) (Table 5).
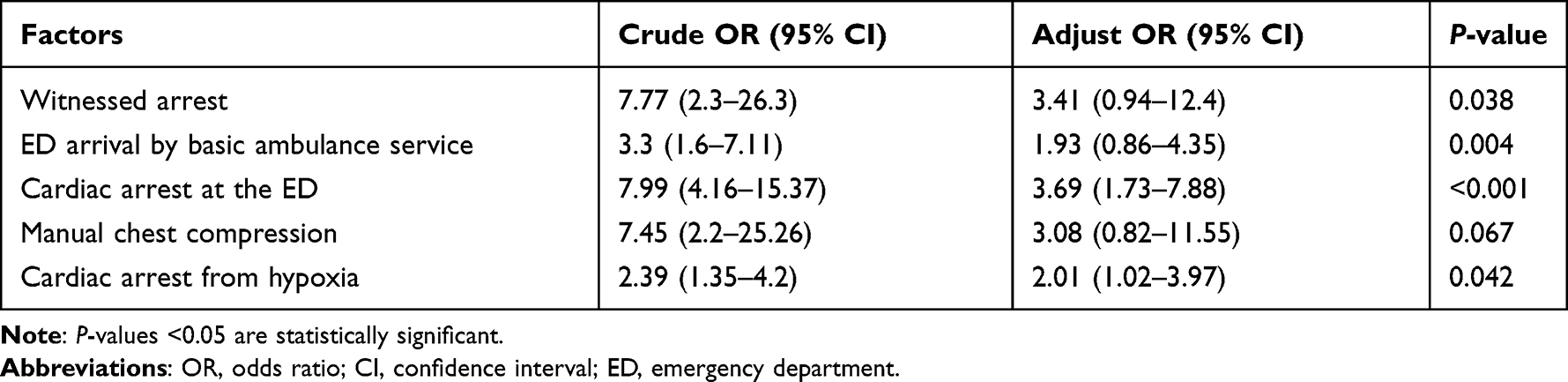 |
Table 5 Multivariate Logistic Regression Model for the Associated Factors with the Return of Spontaneous Circulation of Non-Traumatic Cardiac Arrest |
Discussion
This study found that the sustained ROSC rate from mechanical chest compression was lower than manual chest compression (8.8% vs 43.0%; P < 0.001). In the mechanical chest compression group, most patients had (1) cardiac arrest outside of the hospital, (2) less bystander CPR, and (3) prolonged times of cardiac arrest to ACLS and adrenaline. These factors influenced the poor outcomes. This reflects the results of several studies that demonstrated that early CPR and the presence of bystanders rose the rate of survival.15–17 In contrast to a study by Marcus, the ROSC rate was higher in mechanical chest compression (mechanical 35.3% vs manual 22.4%; adjusted OR = 1.89; 95% CI 1.43–2.50), which possibly resulted from the difference in baseline characteristics.14 That study had a significantly higher number of initial shockable rhythm in patients in the mechanical chest compression group (initial rhythm ventricular fibrillation 5.0% vs 7.3% and ventricular tachycardia 0% vs 1.8%; P < 0.001).
A study by Smekel in OHCA patients reported no statistical difference of ROSC between the manual chest compression and mechanical chest compression groups (41% vs 32%; P = 0.30).18 Wik showed equivalent survival to hospital discharge and the sustained ROSC rate was 32.3% vs 28.6% (covariate adjusted OR = 0.84; 95% CI 0.73–0.96).19 Studies by Perkins reported a similar outcome of 30-day survival (mechanical 6% vs manual 7%; adjusted OR = 0.86; 95% CI 0.64–1.15).7 However, in this current study, the sustained ROSC and survival to admission rates differed between the two groups. The sustained ROSC and survival to admission rates of mechanical chest compression in the OHCA patients was lower (9.4% vs 30.1%; P = 0.029 and 6.3% vs 23.5%; P = 0.052, respectively). The differences between this current study and the other studies were the significant differences in baseline characteristics. The mechanical chest compression group had a longer time to start BLS (10 vs 5 min; P < 0.001), time to ACLS (28 vs 16 min; P = 0.002), time to the first dose of adrenaline (30 vs 18 min; P = 0.001), and time to ED arrival (44 vs 24 min; P < 0.001). It is compatible with the evidence that every minute without CPR reduces the chances of patient survival by 10–15%.20 In our local setting, neither basic nor advanced life support terminates prolonged CPR at the scene. CPR is continuous during transport of the patients to the hospital. Therefore, this influences the prolonged CPR time and adverse outcome.
The duration from cardiac arrest to starting the mechanical compression system varied from a minimum of 5 min to a maximum of 130 min. No study has indicated an appropriate time to apply a mechanical chest compression system. However, this study showed that mechanical CPR tends to be selectively used in OHCA patients and in patients with a prolonged duration of CPR.
The four significant factors associated with sustained ROSC in this study were witnessed cardiac arrest (OR = 3.41; 95% CI 0.94–12.4), ED arrival by basic ambulance service (OR = 1.93; 95% CI 0.86–4.35), cardiac arrest at the ED (OR = 3.69; 95% CI 1.73–7.88), and cardiac arrest from hypoxia (OR = 2.01; 95% CI 1.02–3.97). Neither manual nor mechanical chest compression were associated with sustained ROSC.
The limitations of this study need to be mentioned. The sample size of the mechanical chest compression system group was small. This was a retrospective cohort study; therefore, limitations are inherent in this type of study design. We noticed that the baseline characteristics were significantly different between the manual and mechanical chest compression groups. For example, the mechanical chest compression group had a prolonged duration of cardiac arrest to ACLS and the first dose of adrenaline. These factors influenced the outcomes.
We noted from this study that the time to apply mechanical chest compression did not have a strict guideline. Furthermore, we did not investigate the time the team decided to apply mechanical chest compression, whether or not it was a successful application of the system, and whether or not the system was unavailable or failed to function properly. In this study, the time to apply mechanical chest compression varied. This study found that mechanical chest compression is commonly used during prolonged CPR. In real life practice, mechanical chest compression was applied when required to prolong CPR. This confounding factor affected the unfavorable CPR outcome. This study did not investigate the quality of CPR during mechanical chest compression, especially any interruption of CPR during the application and removal of the system.
Therefore, a further study should be designed to obtain more complete data. The strength of this study is that this is the first study in our regional hospital. The current patient baseline characteristics can lead to a future study design to improve the protocol.
Conclusions
In conclusion, this study showed that a resuscitation strategy using a mechanical chest compression system in an ED environment was not associated with improved sustained ROSC. Mechanical CPR tends to be selectively used in patients with OHCA and prolonged duration of cardiac arrest rather than in patients who responded immediately to initial defibrillation or CPR.
Acknowledgments
The authors thank Kingkarn Waiyanak for searching articles and retrieval, Glenn K. Shingledecker for his help in editing the manuscript, Asst. Prof. Prasit Wuthisuthimethawee and Asst. Prof. Dr. Rassamee Sangthong for giving advice, and the Faculty of Medicine for funding this research.
Funding
The Faculty of Medicine, Prince of Songkla University funded this research.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hayashida K, Tagami T, Fukuda T., et al. Mechanical Cardiopulmonary Resuscitation and Hospital Survival Among Adult Patients With Nontraumatic Out-of-Hospital Cardiac Arrest Attending the Emergency Department: a Prospective, Multicenter, Observational Study in Japan (SOS-KANTO [Survey of Survivors after Out-of-Hospital Cardiac Arrest in Kanto Area] 2012 Study). J Am Heart Assoc. 2017;6(11):
2. Kleinman ME, Brennan EE, Goldberger ZD, et al. Part 5: adult Basic Life Support and Cardiopulmonary Resuscitation Quality: 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2015;132(18 Suppl 2):S414–35. doi:10.1161/CIR.0000000000000259
3. Ochoa FJ, Ramalle-Gómara E, Lisa V, Saralegui I. The effect of rescuer fatigue on the quality of chest compressions. Resuscitation. 1998;37(3):149–152. doi:10.1016/S0300-9572(98)00057-4
4. Stiell IG, Brown SP, Christenson J, et al. What is the role of chest compression depth during out-of-hospital cardiac arrest resuscitation? Crit Care Med. 2012;40(4):1192–1198. doi:10.1097/CCM.0b013e31823bc8bb
5. American Heart Association. Part 6: alternative Techniques and Ancillary Devices for Cardiopulmonary Resuscitation; 2019. Available from: https://eccguidelines.heart.org/circulation/cpr-ecc-guidelines/part-6-alternative-techniques-and-ancillary-devices-for-cardiopulmonary-resuscitation/.
6. Rubertsson S, Lindgren E, Smekal D, et al. Mechanical chest compressions and simultaneous defibrillation vs conventional cardiopulmonary resuscitation in out-of-hospital cardiac arrest: the LINC randomized trial. JAMA. 2014;311(1):53–61. doi:10.1001/jama.2013.282538
7. Perkins GD, Lall R, Quinn T, et al. Mechanical versus manual chest compression for out-of-hospital cardiac arrest (PARAMEDIC): a pragmatic, cluster randomised controlled trial. Lancet. 2015;385(9972):947–955. doi:10.1016/S0140-6736(14)61886-9
8. Couper K, Yeung J, Nicholson T, Quinn T, Lall R, Perkins GD. Mechanical chest compression devices at in-hospital cardiac arrest: a systematic review and meta-analysis. Resuscitation. 2016;103:24–31. doi:10.1016/j.resuscitation.2016.03.004
9. Koster RW, Beenen LF, van der Boom EB, et al. Safety of mechanical chest compression devices AutoPulse and LUCAS in cardiac arrest: a randomized clinical trial for non-inferiority. Eur Heart J. 2017;38(40):3006–3013. doi:10.1093/eurheartj/ehx318
10. Smekal D, Johansson J, Huzevka T, Rubertsson S. No difference in autopsy detected injuries in cardiac arrest patients treated with manual chest compressions compared with mechanical compressions with the LUCAS device--a pilot study. Resuscitation. 2009;80(10):1104–1107. doi:10.1016/j.resuscitation.2009.06.010
11. Smekal D, Lindgren E, Sandler H, Johansson J, Rubertsson S. CPR-related injuries after manual or mechanical chest compressions with the LUCAS™ device: a multicentre study of victims after unsuccessful resuscitation. Resuscitation. 2014;85(12):1708–1712. doi:10.1016/j.resuscitation.2014.09.017
12. Lardi C, Egger C, Larribau R, Niquille M, Mangin P, Fracasso T. Traumatic injuries after mechanical cardiopulmonary resuscitation (LUCAS2): a forensic autopsy study. Int J Legal Med. 2015;129(5):1035–1042. doi:10.1007/s00414-015-1146-x
13. Jacobs I, Nadkarni V, Bahr J, et al. Cardiac arrest and cardiopulmonary resuscitation outcome reports: update and simplification of the Utstein templates for resuscitation registries: a statement for healthcare professionals from a task force of the International Liaison Committee on Resuscitation (American Heart Association, European Resuscitation Council, Australian Resuscitation Council, New Zealand Resuscitation Council, Heart and Stroke Foundation of Canada, InterAmerican Heart Foundation, Resuscitation Councils of Southern Africa). Circulation. 2004;110:3385–3397. doi:10.1161/01.CIR.0000147236.85306.15
14. Hock Ong ME, Fook-Chong S, Annathurai A, et al. Improved neurologically intact survival with the use of an automated, load-distributing band chest compression device for cardiac arrest presenting to the emergency department. Crit Care. 2012;16(4):R144. doi:10.1186/cc11456
15. Porzer M, Mrazkova E, Homza M, Janout V. Out-of-hospital cardiac arrest. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2017;161(4):348–353. doi:10.5507/bp.2017.054
16. Piryani RM, Piryani S. Out-of-Hospital Cardiac Arrest (OHCA): a Critical Healthcare Problem. ECEC. 2019;3(4):197–204.
17. Myat A, Song KJ, Rea T. Out-of-hospital cardiac arrest: current concepts. Lancet. 2018;391(10124):970–979. doi:10.1016/S0140-6736(18)30472-0
18. Smekal D, Johansson J, Huzevka T, Rubertsson S. A pilot study of mechanical chest compressions with the LUCAS™ device in cardiopulmonary resuscitation. Resuscitation. 2011;82(6):702–706. doi:10.1016/j.resuscitation.2011.01.032
19. Wik L, Olsen JA, Persse D, et al. Manual vs. integrated automatic load-distributing band CPR with equal survival after out of hospital cardiac arrest. The randomized CIRC trial. Resuscitation. 2014;85(6):741–748. doi:10.1016/j.resuscitation.2014.03.005
20. Janota T. Kardiopulmonalni resuscitace. In: Vojacek J, Kettner J, editors. Klinická kardiologie. Hradec Kralove: Nucleus HK; 2012:871–879.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.