Back to Journals » Patient Preference and Adherence » Volume 17
Comparison of SARS-CoV-2 Vaccination Skepticism, Reasons, and Concerns Between Mass Vaccination Centers and General Practices in Germany 2021
Authors Schrimpf A, Jentzsch A, Geier AK, Bleckwenn M
Received 4 September 2023
Accepted for publication 24 October 2023
Published 7 November 2023 Volume 2023:17 Pages 2855—2870
DOI https://doi.org/10.2147/PPA.S433331
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Anne Schrimpf, Anne Jentzsch, Anne-Kathrin Geier, Markus Bleckwenn
Institute for General Practice, Faculty of Medicine, Leipzig University, Leipzig, Germany
Correspondence: Anne Schrimpf, Leipzig University, Institute for General Practice, Philipp-Rosenthal-Str. 55, Leipzig, 04103, Germany, Email [email protected]
Introduction: The reluctance to be vaccinated against COVID-19 has significantly curbed vaccine uptake. Unlike mass vaccination centers, general practitioners (GPs) might be able to address some of the patients’ concerns through their long-term doctor-patient relationship. This study compared vaccination reasons, concerns and skepticism about vaccination, and perceived importance of the vaccine and its hypothetical value between vaccination centers and GP practices.
Methods: A survey was distributed (07/2021-10/2021) among newly vaccinated individuals in ten GP practices (n = 364) and two vaccine centers (n = 474).
Results: Participants in vaccine centers stated more prosocial and benefit-oriented reasons for vaccination, whereas participants in GP practices more often stated the GP’s recommendation as the reason. Perceived importance of the vaccine in combating the pandemic was rated higher among individuals at vaccine centers and with higher health awareness and self-efficacy. Participants at both types of sites who preferred a GP for vaccination expressed more vaccination skepticism, which was also related to older age, more health risk concerns related to COVID-19 vaccines, and lower perceived importance of the vaccine.
Conclusion: Our results indicate opportunities for framing future vaccination campaigns that include vaccination centers. Additionally, a rapid GP involvement in future mass vaccinations might be crucial for overcoming attitudinal barriers and achieving higher vaccine uptake.
Keywords: COVID-19, vaccines, immunization programs, mass vaccination, vaccination hesitancy, attitude to health
Introduction
After an accelerated authorization procedure, the first SARS-CoV-2 vaccine was approved in December 2020 in the European Union, followed by two more in January 2021.1 At the beginning of the European COVID-19 vaccination campaign, vaccines were administered according to prioritization groups, such as age, occupation, and co-morbidities, due to initial shortages in vaccine doses and logistical challenges.2,3 In Germany, mass vaccination centers were implemented starting in December 2020 to manage the initial high vaccine demands and were joined by general practitioners (GPs) across Germany in April 2021.4 GPs received a limited portion of the vaccine doses to vaccinate their patients in their community-based practices and also had to adhere to the allocation according to prioritization groups. The prioritization groups were suspended in June 2021, however, vaccine uptake stagnated considerably, which has been discussed as a result of an emerging vaccination hesitancy.5,6 The German government intended to vaccinate 85% of the population under 60 years of age and 90% of the population over 60 years of age against COVID-19 to reach herd immunity.7 These targets have never been achieved, despite evidence that COVID-19 vaccinations reduced total global deaths by 63% in the first year of vaccination8 and showed protective properties against subsequent variants of the virus.9 At the time of the present study, less than half of the German population had been vaccinated.5
The reluctance to get a vaccination in general and against COVID-19 specifically has been found to have multiple and complex reasons. With respect to COVID-19, socio-demographic factors, such as female gender or younger age,10–14 were strong predictors for reduced vaccine uptake. Education, however, showed mixed interactions.14 Further, vaccine types gained differing levels of trust, with the mRNA vaccines receiving higher levels compared to the vector vaccine, potentially influenced by the varying immunological efficacy, safety concerns, and media coverage.15 Other factors such as attitudes and beliefs have also been identified to be associated with vaccination hesitancy, particularly vaccination skepticism, social pressure, perceived vaccine safety, skepticism due to rapid clinical approval procedures, past vaccination refusal, healthcare system and authority distrust, media usage, and political affiliation.6,14,16–20 Some of these concerns were based on safety reports of rare but serious adverse events caused by COVID-19 vaccines, such as myopericarditis or thrombosis. While myopericarditis did not occur more frequently than after other types of vaccination,21 the risk for thrombosis was higher after COVID-19 vaccines compared to influenza.22 Minor systemic reactions, such as chills or headache, were also more common after COVID-19 vaccinations compared to influenza,23,24 indicating at least partly justified concerns.
In contrast to other medical specializations, GPs might be able to overcome some of the above-mentioned concerns in patients treated previously by using the trust gained in their long-term doctor-patient relationship.25–28 Particularly, the length of the relationship might enhance trust in the health care provider29 and trust in the provider has been found to be a factor influencing the willingness to get vaccinated.30 The underlying mechanism might be effective patient-centered communication strategies,31–33 especially regarding vaccine safety and necessity.34 For example, it has been shown that the provision of a verbal health education for influenza vaccinations substantially increased the vaccine uptake especially in individuals whose initial vaccination intention was uncertain.35 Further, repeated exposure to information about vaccination benefits might increase vaccine uptake,36 indicating that GPs might be especially able to target vaccine hesitant individuals through their repeated face-to-face meetings. In contrast, mass vaccination centers might be less suited to attract vaccination hesitant individuals.27,37–39
For future vaccination campaigns and to increase SARS-CoV-2 vaccine uptake, it is important to understand which vaccine sites are best suited to address factors such as attitudes and motivations. To our knowledge, no study directly investigated if previous COVID-19 vaccination hesitancy varied between individuals receiving their vaccine in a GP practice and those receiving their vaccine in a mass vaccination center. This study was conducted more than six months following the initial SARS-CoV-2 vaccine approval in Germany in mid-2021. During this period, prioritization groups had already been suspended, and the incidence of COVID-19 cases was relatively low, enabling widespread access to vaccination. Consequently, the demographics of the vaccinated population shifted towards a younger, less comorbid, and non-high-risk group. Moreover, this particular time period offered a unique opportunity for comparing the motivation for vaccination across different vaccination sites, as vaccination centers were subsequently closed. By distributing a paper-based survey among newly vaccinated individuals in both types of vaccine sites, this study aimed to examine participants’ reasons for vaccination, their concerns regarding the vaccination, perceived importance, and potential differences between sites. In addition, participants’ hypothetical willingness to pay for the vaccination, used as an indicator for the value attributed to the vaccine, was assessed and compared between sites. We also examined whether vaccination skepticism and concerns differed in participants who preferred a particular vaccine site, regardless of where they received the vaccine. Finally, sociodemographic characteristics were considered in all analyses to identify population groups that were more likely to express concerns or certain attitudes.
Methods
Procedure
The data were collected between July 2021 and October 2021 in the Free State of Saxony, Germany by using a cross-sectional questionnaire study design. We calculated a required sample size for surveys of at least 601 completed questionnaires based on the overall population in Saxony (4,043,002 in 2021), a percentage of occurrence of 50%, confidence level of 95%, and a 4% margin of error. Vaccination centers and GP practices in both city and rural areas of Saxony were invited on a convenience basis to voluntarily participate in the study and distribute a self-developed questionnaire among vaccinated individuals over 18 years of age who had received their first or second SARS-CoV-2 vaccine. Participants completed the survey immediately after receiving their vaccine within their recommended 15 min observation time.
In total, we recruited two vaccine centers and ten GP practices. The two vaccination centers received in total n = 650 questionnaires to distribute: n = 350 in Leipzig-Messe (city area) and n = 300 in Belgern (rural area). Ten GP practices received in total n = 450 questionnaires, of which five GP practices were located in the city area of Leipzig (n = 195 questionnaires) and five practices were located in a rural area, Leipziger Land/Nordsachsen (n = 255 questionnaires). A part of this study was reported elsewhere with the same sample and procedure.40 The recruitment process is depicted in Figure 1.
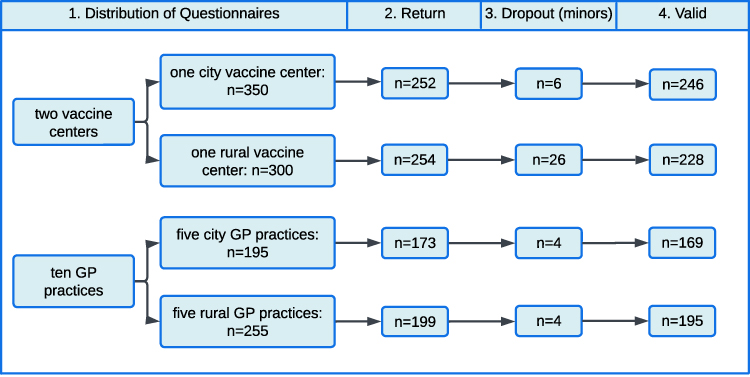 |
Figure 1 Flowchart of recruitment process. |
Questionnaire
The patient questionnaire was self-developed in the Institute for General Practice of the Leipzig University by an interdisciplinary research team (medical scientists and GPs) in a multi-stage revision process. In addition, an extensive literature search aimed at identifying relevant factors for the reasons for receiving vaccines and potential concerns complemented the questionnaire development.18–20,25,29,30 The questionnaire was adjusted for the respective vaccination site and varied in terms of wording. It contained the following topics: 1) socio-demographics (eg, age, gender, education, occupation, influenza vaccine status), 2) reasons for obtaining vaccination, and 3) attitudes towards and perceived importance of SARS-CoV-2 vaccinations and vaccine site preference.
Education was assessed by using the CASMIN educational classification.41 Attitudes were assessed by means of either 5-point or 10-point rating scales. Participants were asked on a 5-point scale if they agreed or disagreed with a given statement (eg, “I am generally skeptical about COVID-19 vaccines”, 1 = Strongly disagree, 5 = Strongly agree). Item-specific response options were given on 10-point rating scales (eg, “How important was it for you to be vaccinated against COVID-19 as soon as possible?”, 1 = Not at all important, 10 = Very important). All survey questions were assigned abbreviated labels. For instance, the term “vaccination skepticism”, as employed in the analyses, corresponds to the survey question “I am generally skeptical about COVID-19 vaccines”. All items analyzed in this study and their abbreviated labels can be found in the results section.
The questionnaire underwent a think-aloud pre-testing42 aimed at identifying problems or misunderstandings related to each item. The provisional questionnaire was filled out by five patients from the targeted group who were instructed to think aloud while answering each item and report every spontaneous thought. All patients were subsequently interviewed, leading to additional revisions and simplifications of some items. These five pre-testing questionnaires were not included in the final sample. The final version of the questionnaires can be found in Supplementary Material S1a, b.
Ethics Statement
The study was carried out in accordance with the Declaration of Helsinki and the study protocol was approved by the research ethics committee of the Leipzig University (reference number 314/21-ek). Participants agreed to participate by voluntary returning the anonymous questionnaire. No personal data besides age and sex were assessed.
Statistical Analyses
All statistical analyses were carried out using IBM SPSS Statistics 27 (Armonk, NY, USA) with a two-sided α-level of 0.05. For descriptive statistics, missing values in single variables were considered by presenting frequencies as % (n/nvalid). Continuous variables were presented as mean ± standard deviation (SD). Differences between groups (“vaccine center city”, “vaccine center rural”, “GP practices city”, “GP practices rural”) were analyzed with the following tests: Group differences in categorical variables were analyzed using chi-square or Fisher’s exact tests. Estimated effect sizes were reported using Cramer’s V. Group differences in non-normally distributed continuous variables (age and rating scales) were analyzed using Kruskal‐Wallis tests and subsequent post-hoc tests with Bonferroni corrections. Estimated effect sizes are reported using Cohen’s d. Two-sided bivariate correlations were calculated to analyze the association of attitudes towards vaccination with vaccine site preference.
Further, multiple linear regression analyses using Entry method were conducted. 1) The predictive ability of demographic variables, reasons for vaccination, health risk concerns, perceived importance of the vaccine, and perceived own influence on the infection risk (independent variables) in explaining vaccination skepticism (dependent variable) was calculated. 2) The predictive ability of demographic variables, reasons for vaccination, health risk concerns, and perceived own influence on the infection risk (independent variables) in explaining the perceived importance of vaccination for combating the pandemic (dependent variable) was calculated. Lastly, a multiple logistic regression analysis using Entry method was conducted to calculate 3) the predictive ability of demographic variables, reasons for vaccination, vaccination skepticism, health risk concerns, and perceived importance of the vaccine (independent variables) in explaining the willingness to pay for vaccination (dependent variable, only “yes” and “no” were included, participants answering “not sure” were excluded from analysis). For all models, assumption checks for multiple linear or logistic regressions were performed before interpretation. Results of these checks can be found in supplementary material S2.
Results
Sample Characteristics
In total, 1100 questionnaires were distributed in two vaccine centers and ten GP practices (see Figure 1), of which 838 were filled out and were eligible for analyses (response rate of 76.2%). Percentages, means, and standard deviations for sample characteristics can be found in Table 1 and in Jentzsch et al 2022.40
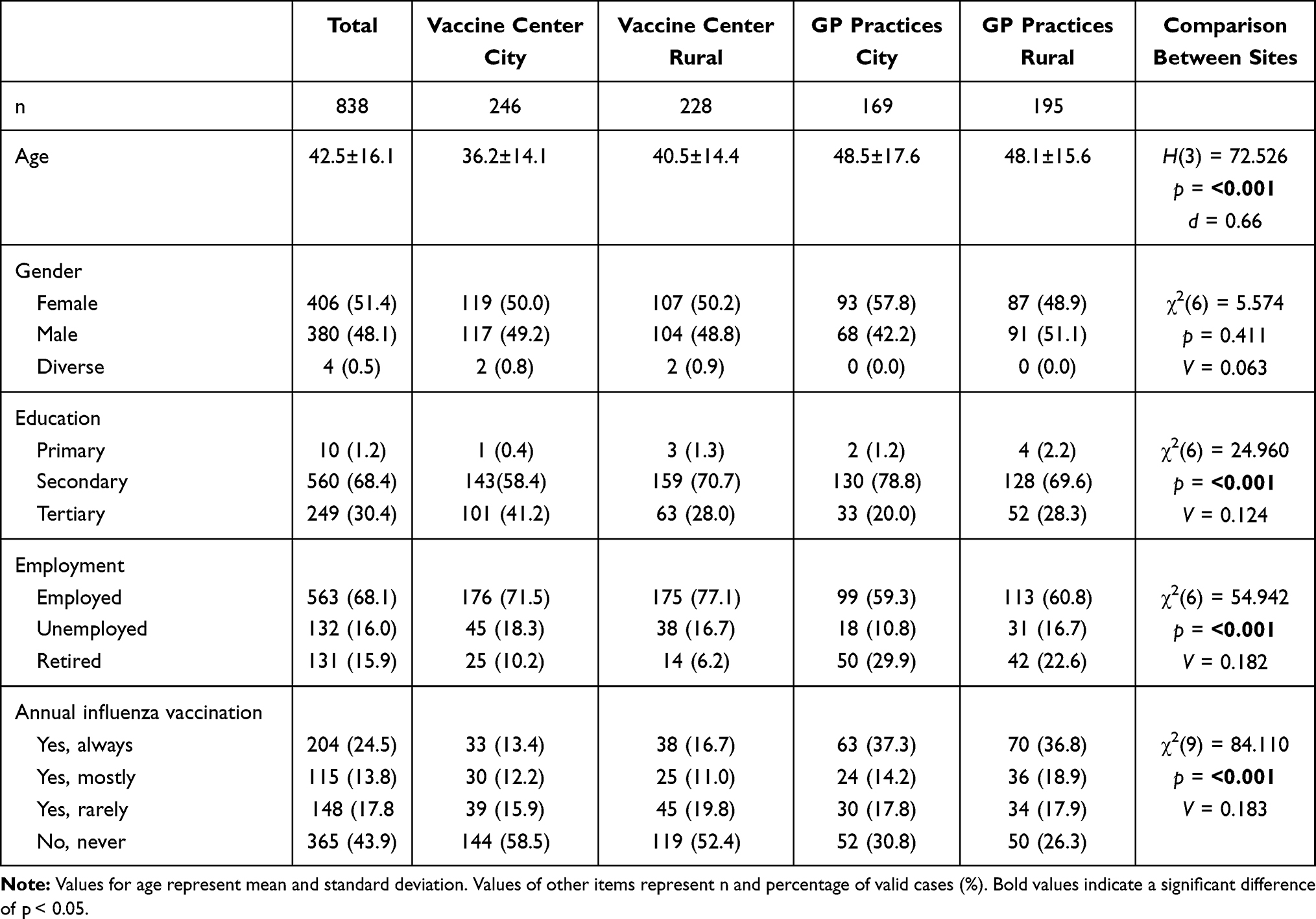 |
Table 1 Sociodemographic Sample Characteristics and Comparison Between Vaccine Sites |
Participants’ Reasons, Concerns, and Willingness to Get the SARS-CoV-2 Vaccine
We examined participants’ reasons for getting vaccinated, concerns regarding the vaccination, perceived importance of getting vaccinated, and willingness to pay for the vaccination (WTP, as an indicator for the value attributed to the vaccine). Percentages and differences between vaccination sites can be found in Table 2. Whereas benefits through the vaccination and protection of others were more likely reasons for vaccinations in individuals in vaccine centers, individuals in GP practices were more likely to state that their GP’s recommendation was a reason for vaccination. Participants in GP practices reported being slightly more skeptical towards the vaccine compared to participants in vaccine centers (Figure 2). Being vaccinated as soon as possible was more important to participants in rural GP practices compared to the other sites. In addition, participants in vaccine centers, especially in the city, were more likely to be willing to pay for the vaccination.
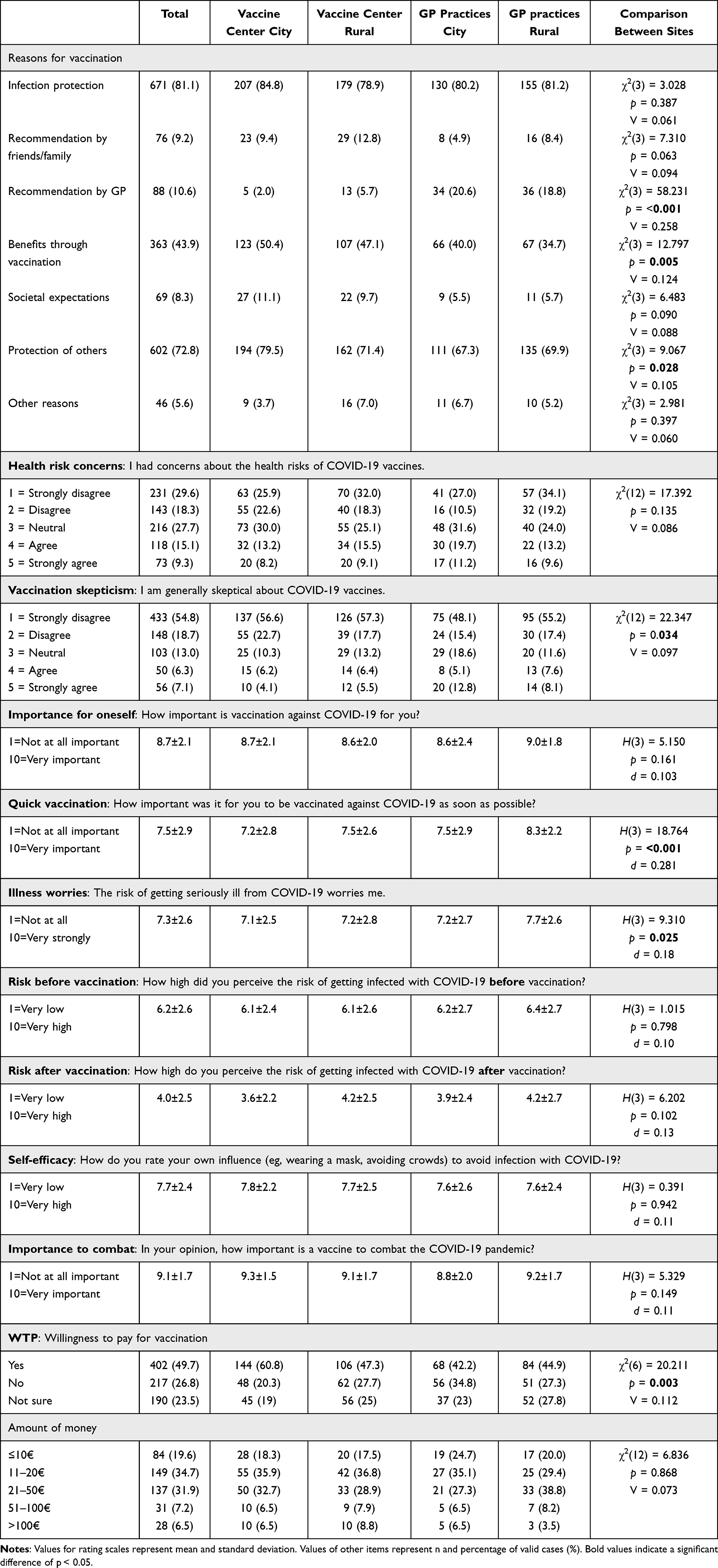 |
Table 2 Reasons, Concerns, and Willingness to Pay for Vaccination and Comparison Between Sites |
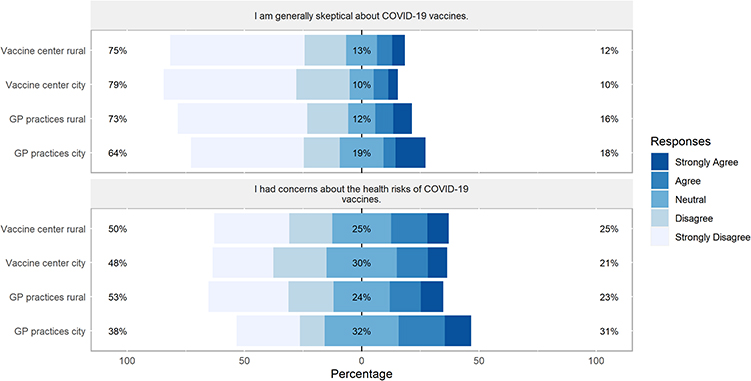 |
Figure 2 Differences between sites in participants’ vaccination skepticism and health risk concerns. Percentages on the left and right side of the graph represent a summary of Strongly Agree and Agree on the right and Disagree and Strongly Disagree on the left side. |
Vaccine Site Preference and Its Relation to Participants’ Concerns and Perceived Importance to Get the SARS-CoV-2 Vaccine
We further assessed participants’ preference for a specific vaccine site in vaccine centers and GP practices. In GP practices, participants were asked to rate the importance to be vaccinated by their GP and how willing they were to also get vaccinated in a vaccine center. In vaccine centers, participants were asked if they would have preferred being vaccinated by a GP and if they would go to a vaccine center again for immunization (for more information see).40 These items were correlated with participants’ concerns regarding the vaccination and perceived importance. Results of the correlations are in Table 3.
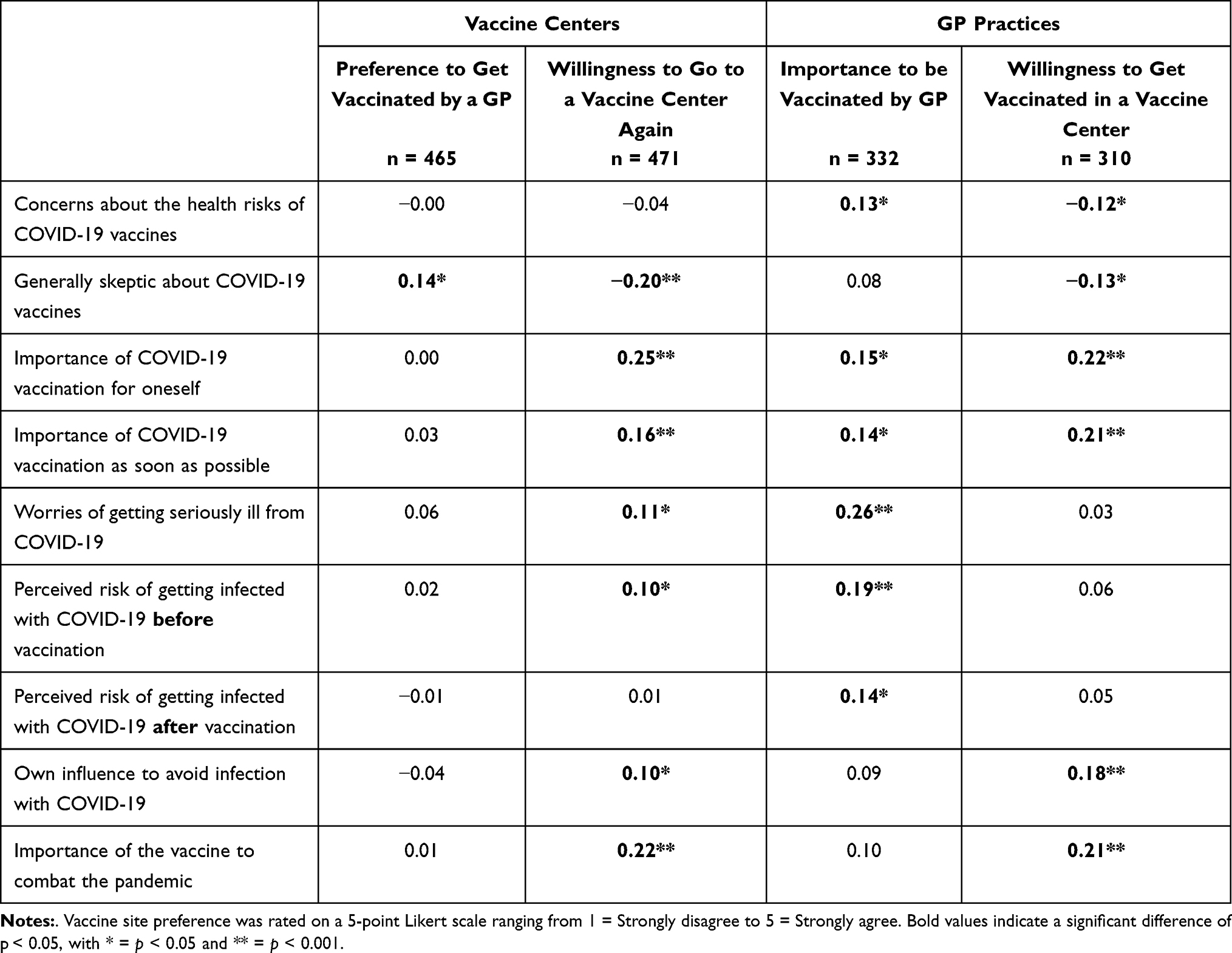 |
Table 3 Correlations Between Vaccine Site Preference and Participants’ Concerns and Willingness to Get the SARS-CoV-2 Vaccine |
Predicting Vaccination Skepticism
A multiple linear regression was calculated to predict vaccination skepticism based on reasons for vaccination, health risk concerns, perceived importance of the vaccine, self-efficacy, and demographic variables. We further calculated a new variable “GP preference” by merging “Preference to get vaccinated by a GP” (vaccine center participants) and “Importance to be vaccinated by GP” (GP practice participants) and included this variable in the model. The model explained 39.9% of the variation in vaccination skepticism (F(12,646) = 35.708, p < 0.001; Table 4).
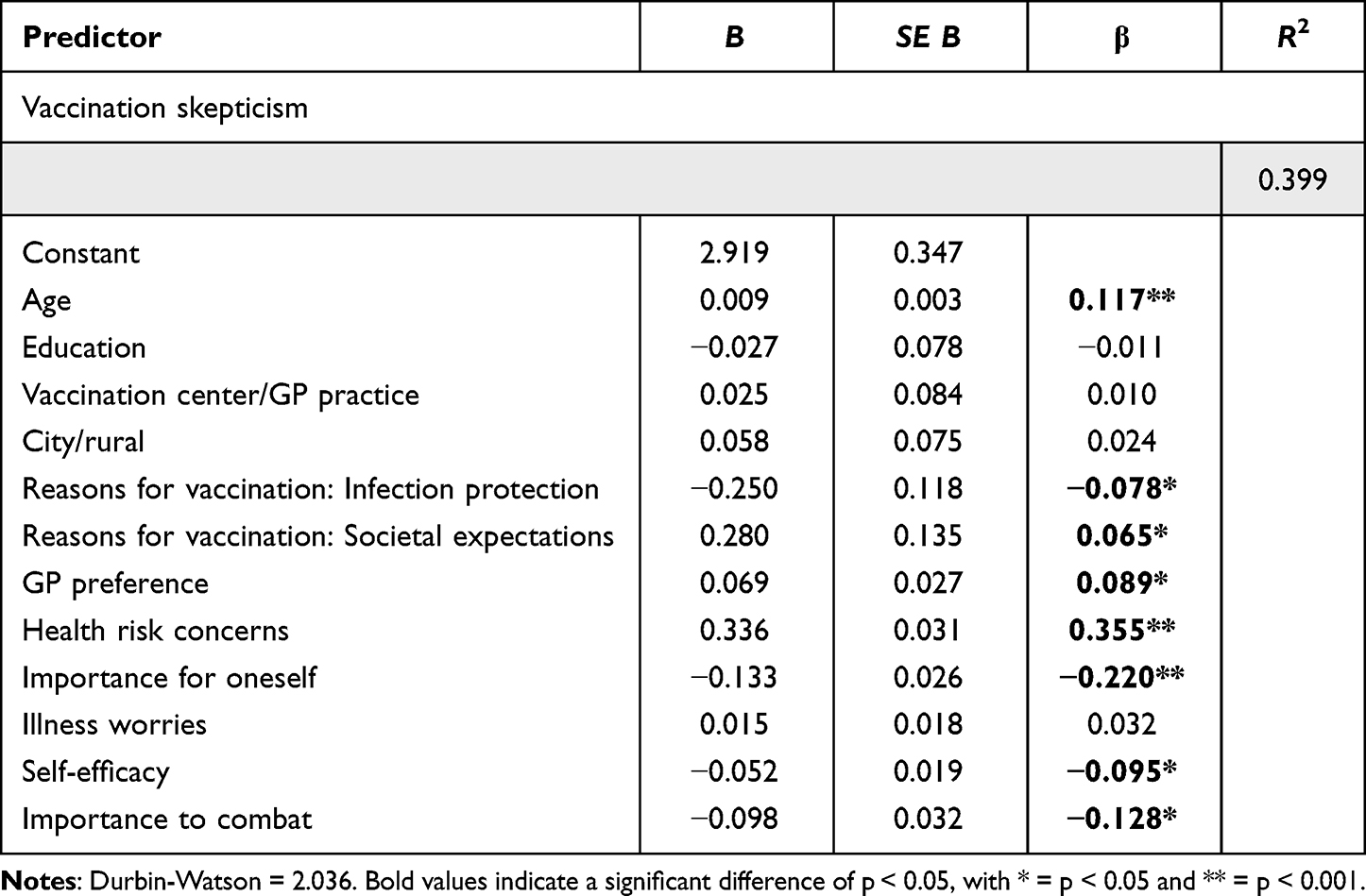 |
Table 4 Multiple Regression Analysis Predicting Vaccination Skepticism |
Predicting Perceived Importance of Vaccination for Combating the Pandemic
A multiple linear regression was calculated to predict perceived importance of the COVID-19 vaccine for combating the pandemic, including demographic variables, reasons for vaccination, health risk concerns, and self-efficacy. The model explained 37.1% of the variation in the perceived importance (F(8,685) = 50.534, p < 0.001; Table 5).
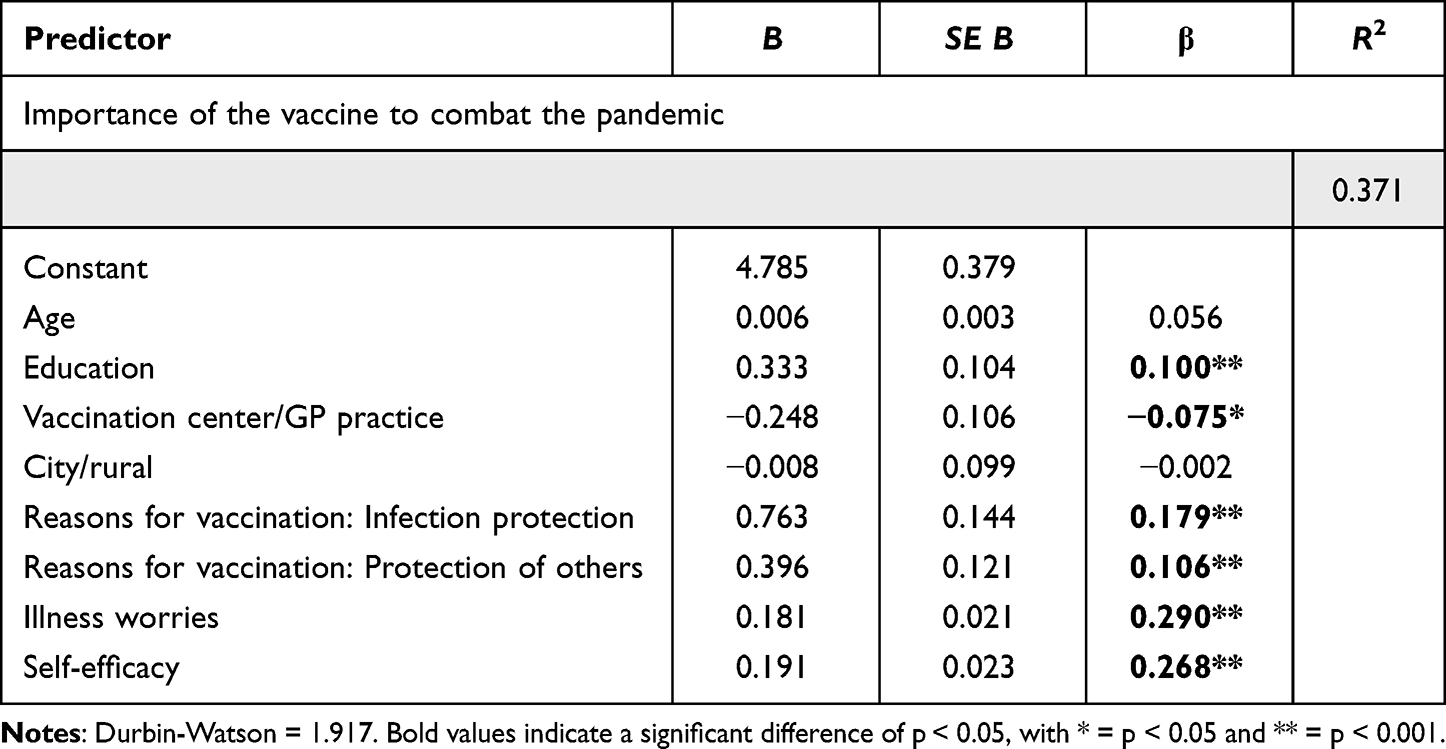 |
Table 5 Multiple Regression Analysis Predicting Perceived Importance of the Vaccine to Combat the Pandemic |
Predicting the Willingness to Pay for Vaccination
A multiple logistic regression was calculated to predict participants’ WTP for the vaccination (yes, no) based on reasons for vaccination, vaccination skepticism, importance of a vaccination, perceived risk of getting infected with COVID-19, and demographic variables. The model explained 30.7% (Nagelkerke's R2) of the WTP for vaccination (Wald χ2 (1) = 48.439, p < 0.001; Table 6).
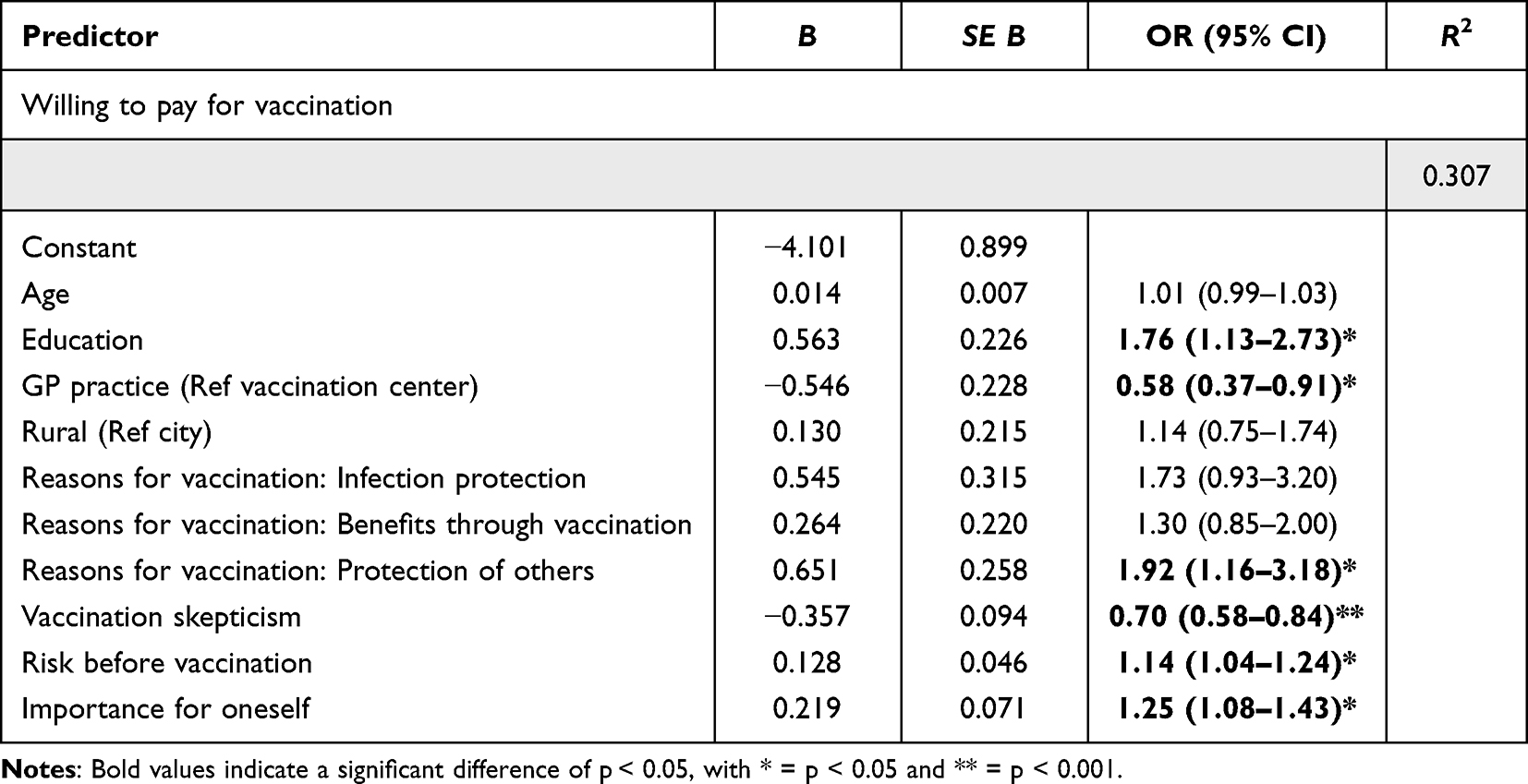 |
Table 6 Multiple Regression Analysis Predicting the Willingness to Pay for the Vaccination |
Discussion
Using a questionnaire, vaccinated individuals in German GP practices (n = 364) and mass vaccination centers (n = 474) were compared with regard to vaccine skepticism, concerns, and reasons for receiving a SARS-CoV-2 vaccine. In vaccine centers, the benefits of vaccination and protection of others were more likely to be reasons for vaccination, whereas individuals in the GP practices were more likely to state that the GP’s recommendation was a reason for vaccination. Participants in both sites preferring a GP for vaccination were more skeptical about the vaccine and more worried about getting seriously ill from COVID-19. In addition, vaccination skepticism was higher in older participants who also expressed more concerns about health risks of COVID-19 vaccines and lower perceived importance of the vaccine. However, no differences in vaccination skepticism between sites were independently found. The importance of the vaccine for combating the pandemic was rated higher by participants at vaccination centers, with a higher educational level, more self-efficacy, and an increasing need to protect others and themselves from serious illness. Participants in vaccine centers and who had attained a higher level of education were also hypothetically more willing to pay for a vaccine, especially when they were less skeptical and had a higher need to protect others and themselves. Our results indicate that GPs might indeed be better able to reach individuals with stronger vaccination hesitancy and, conversely, that individuals with higher vaccine skepticism might prefer to be vaccinated by a GP rather than at a vaccine center.
Reasons for Vaccination
We examined participants’ reasons for vaccination and potential differences between mass vaccination centers and GP practices. We found that participants at vaccine centers were more likely to state benefits through the vaccination and protection of others as reasons for vaccinations. Individuals in GP practices, in contrast, were more likely to state their GP’s recommendation as a reason for vaccination. Previous studies have shown that protecting others is a strong motivator for receiving SARS-CoV-2 vaccines,43–46 even among hesitant individuals.47 In addition, at the time of the survey, a full immunization offered everyday benefits, such as easier access to leisure and travel. Our results suggest that individuals in vaccine centers were more motivated to be vaccinated by anticipating more social benefits. As vaccinations in vaccine centers in our study required longer travel times compared to GP practices,40 we can assume that individuals with a high level of motivation to protect others and to receive benefits would be more likely to seek a vaccination on their own initiative and would be willing to travel a further distance to a vaccine center. In contrast, GPs’ long-term doctor-patient relationships, including with individuals who are less willing to receive a SARS-CoV-2 vaccine, might enable them to overcome some vaccination concerns. Provider recommendation has been shown to be an effective intervention to increase vaccine uptake,48 a mechanism potentially influenced by trust30 and effective patient-centered communication and education strategies.34,35
Vaccination Skepticism and Vaccine Site Preference
As vaccination skepticism has been found to indirectly influence vaccination readiness6 and GPs might be better able to overcome these attitudes,25,27 we examined whether vaccination skepticism and concerns differed among participants who preferred a particular vaccine site. Although participants in GP practices were slightly more skeptical about the vaccine compared to participants in vaccine centers in a univariate analysis, we could not find general differences in vaccination skepticism between sites in a multivariate analysis, indicating additional interacting variables. Indeed, we found that regardless of site, vaccination skepticism was higher in older participants, who also expressed lower perceived importance of the vaccine and more health risk concerns of COVID-19 vaccines. The latter is in line with the findings of a systematic review, showing that vaccine safety concerns are a strong global predictor of vaccine hesitancy.49 Importantly, GP preference was an additional predictor of higher vaccination skepticism in both vaccine sites. Our results might suggest that the vaccine site was not per se selecting vaccinees with more or less vaccine skepticism. Instead, it is conceivable that other factors might influence the decision to be vaccinated at a mass vaccination center, despite preference for a specific site or vaccination skepticism. For instance, our data were collected in summer of 2021, and touristic traveling required immunization in most cases. At the same time, GPs could order vaccines according to their needs, but only in limited quantities, resulting in low capacity for high demand. Therefore, it is likely that even vaccine-hesitant individuals with a preference for a GP would register at the vaccination centers to prepare for the upcoming holidays in time, which is supported by studies showing that travel intentions might encourage even vaccine-hesitant individuals to receive a vaccine.47,50 In addition, social pressure from relatives or friends has been found to be a strong motivator for vaccination, even among hesitant individuals.47 The fact that more skeptical individuals would prefer to be vaccinated by a GP, however, indicates that the established relationship between patient and GP might be beneficial in reaching vaccine-hesitant individuals, as has been suggested elsewhere.25,27,51,52 Consistent with this, studies found that the SARS-CoV-2 vaccination coverage was positively associated with provider recommendation53 and with the number of GPs per capita, even in regions with higher vaccination hesitancy.28
The association between older age and increased vaccination skepticism contrasts with the findings of other studies (see reviews,12,14) which mainly report higher vaccination hesitancy in younger individuals. However, a global systematic review also showed contradictory results with respect to age and vaccination hesitancy.49 In our study, this effect might be due to the timing of the survey, as the data were collected when prioritization of more vulnerable groups, such as older people with co-morbidities, had already been suspended. At the time of our survey, the remaining older individuals might have been more reluctant to receive the vaccine in the earlier phases, while those more willing to receive the vaccine had already gone through the process and could not be captured in our study. A potential explanation for our finding might therefore be the known association between older age and increasing conservatism.54,55 Conservatism, conversely, has been found to be associated with lower vaccine uptake and more vaccination hesitancy or skepticism.49,56,57 However, future studies should examine the relationship between older age, conservatism, and vaccination skepticism in more detail.
Perceived Importance of the Vaccine
We further found that the perceived importance of the vaccine in combating the pandemic was higher among individuals with higher education and in vaccine centers. Individuals who stated that the vaccine is important to overcome the pandemic also more often expressed their own and others’ infection protection as the main reasons for vaccination, worries of getting seriously ill from COVID-19, and higher own influence over avoiding infection with COVID-19 (self-efficacy). Our results suggest that especially individuals with a high health awareness (indicated by wanting to protect against infection and worrying about getting ill) and health self-efficacy were more likely to consider the vaccine as important for ending the pandemic. This resonates with pre-pandemic findings showing that a health-promoting behavior was predicted by health self-efficacy and health values.58 Self-efficacy, but also risk perception and outcome expectancies, have also been found to be associated with influenza vaccination intentions.59,60 With respect to COVID-19, perceived benefits and severity of the novel disease were found to be positively associated with higher vaccine acceptance.61–63 Another study found that individuals with higher risk perception of COVID-19 also expressed higher self-efficacy,64 suggesting that higher perceived risk might modulate behavioral adaptations. As all individuals included in our study received a vaccine, we could not directly measure vaccination intention in this population, but only the importance attributed to the vaccine to combat the pandemic. However, it has been shown that the perceived importance of the SARS-CoV-2 vaccine increased vaccination intentions and acceptance.65–67 Thus, supported by our results, both parameters (risk perception and self-efficacy) might promote protective measures, and, in turn, the importance attributed to vaccination, as it can be seen as an opportunity for action.
Willingness to Pay
Lastly, we examined participants’ hypothetical WTP for the vaccination as a measure of the perceived value attributed to COVID-19 vaccines. We found that participants with a higher level of education and in vaccine centers were more willing to pay for the vaccine. Further, protecting others as a reason for vaccination, perceived risk of getting infected with COVID-19, and perceived importance of the vaccine for oneself increased the WTP, whereas vaccination skepticism markedly decreased the WTP. A recent review identified, among others, sociodemographic characteristics, perceived threat, and perceived benefit as determinants of the WTP for health care services.68 With respect to COVID-19, a higher educational level69,70 and the perceived threat of the pandemic71 have been found to increase the amount of money people are willing to pay for SARS-CoV-2 vaccines. In contrast, lower trust in the government was associated with a decrease in the amount of money people were willing to pay for SARS-CoV-2 vaccines.69 However, apart from the specific individual determinants of the WTP replicated in our study, we also found that these individuals were more likely to get vaccinated at a vaccine center. Consistent with the results discussed above regarding the perceived importance of the vaccine in combating the pandemic, individuals who would spend money on a vaccine, and, thus, might place a higher value on it, were more likely to accept a potentially longer travel time to the vaccine center.40 Conversely, individuals who placed a lower value on the vaccine were more likely to be vaccinated in a GP practice, strengthening our argument that GPs may be better able to reach individuals with lower motivation to get vaccinated against COVID-19. This might also be due to the fact that vaccinations were offered at the GP practice during consultations for other reasons, whereas vaccination at the vaccine center required additional time and effort.
Limitations
Our study has limitations. Although we measured vaccination skepticism, we cannot fully account for vaccination skepticism in the general population, as all individuals who completed the questionnaire were vaccinated, indicating potentially lower skepticism in this group. In addition, the data were assessed when the prioritization of specific groups had already been suspended, which implies that the results might have differed at the beginning of the immunization campaign. In particular, the survey period coincided with the 2021 summer holiday season, which may have led to a shift in motivation to vaccinate to comply with travel regulations at both types of vaccination sites. Further, participants did not fill in the questionnaire at the same timepoint, instead ranging from July 2021 to October 2021. Temporary differences, such as case incidences of COVID-19, subjective perception of the pandemic’s progression, or holiday seasons, might have influenced participants’ reports over time. In addition, all answers were self-reports and might be imprecise due to subjective perceptions. Importantly, our questionnaire is not a validated scale as we did not develop and assess several items measuring a construct related to motivation, vaccine skepticism, or perceived importance, but rather investigated single item responses.
Lastly, the study was conducted in one federal state in Germany. Socio-demographic differences between federal states in Germany as well as between European countries limit the generalizability of our findings. Further, the varying access to mass vaccination centers/GPs, availability of vaccines, case incidences, and vaccination willingness in Europe and other parts of the world might impede comparability.
Implications
Our study contributes to a better understanding of vaccination preferences and reasons in individuals with varying degrees of vaccination skepticism. The present results indicate that GPs might be both able to convince more vaccination hesitant and less motivated individuals and, conversely, be the preferred option for more skeptical individuals. We argue, in line with previous research,25–27,30,53 that especially the trust gained in a long-term doctor-patient relationship might significantly increase vaccine uptake in more hesitant individuals. In contrast, mass vaccination centers might be more likely to attract individuals with stronger intrinsic motivations, such as risk perception, higher health values, protection of others and self, and with higher self-efficacy. Considering the national vaccination campaign in Germany 2021, GPs were included in the vaccination strategy at a later stage after implementing mass vaccination sites. Our results therefore suggest the following opportunities for future vaccination campaigns: 1) In a future mass vaccination event, the rapid involvement of GPs in parallel with mass vaccination sites might enhance the vaccine uptake across broad socio-demographic groups. 2) As self-efficacy and risk perception might promote protective behaviors, framing vaccination as an opportunity to act to protect others and oneself might be beneficial in future vaccination campaigns to overcome attitudinal barriers. In turn, the provision of sufficient health-related information could increase self-efficacy and, thus, confidence in making informed choices. Through their long-term relationship with patients, we suggest that especially the provision of health information by GPs can play a crucial role in influencing patients’ vaccination decisions. These framings need not be restricted to vaccination behavior, and could potentially be used to promote other favorable health behaviors as well. 3) Our results also suggest that social and leisure benefits might increase vaccine uptake. In future vaccination campaigns, these benefits could be explicitly emphasized. 4) Lastly, vaccination skepticism is not restricted to COVID-19 vaccines and other infectious diseases have recently been on the rise (eg, polio and measles). GPs might be able to reduce vaccination hesitancy for various infections through effective but time-consuming patient-centered communication strategies.31–33,35 To fulfill this role, better support and recognition for the important role they play in immunizing their communities is urgently needed (eg, financial improvements of the billings and more time to discuss potential concerns during appointments).
Conclusion
Attitudes towards SARS-CoV-2 vaccination have significantly curbed vaccine uptake worldwide. In this study, we examined whether participants’ reasons for vaccination, concerns and skepticism about vaccination, and perceived importance of the vaccine and its hypothetical value would differ between mass vaccination sites and GP practices. We found that reasons for vaccination were more prosocial and benefit-oriented among those who attended vaccine centers. In the same line, both the perceived importance of the vaccine for combating the pandemic and its hypothetical value were rated higher among individuals at vaccine centers, indicating opportunities for framing future vaccination campaigns that include large-scale uptake at mass vaccination centers. We also confirm that individuals with more vaccination skepticism and concerns more often preferred a GP to administer the vaccine, suggesting that a rapid involvement of GPs in future mass vaccination events might be crucial for overcoming attitudinal barriers. Our findings provide insights into how future vaccination campaigns could be designed to achieve higher vaccine uptake and to optimally meet individual attitudes in all population groups.
Acknowledgments
We thank participating GPs, vaccine centers, and vaccinated individuals for their support. For assistance and help during the preparation of the study, we thank Britt Häusler and Nathalie Mähl. We thank André Jentzsch for support with the graphical representation of the results. For proofreading we thank Dawn M. Bielawski.
Disclosure
All authors would like to disclose that data from the same cohort of participants were previously published in the journal Vaccines (https://www.mdpi.com/2076-393X/10/11/1823). In this previous study, other variables from the same sample were reported. The present study is based on the same cohort of participants (n = 838), but consists of new variables related to vaccine attitudes that have not been reported before.
The authors acknowledge support from the German Research Foundation (DFG) and Leipzig University within the program of Open Access Publishing. The authors have no relevant financial or non-financial interests to disclose.
References
1. European Medicines Agency. COVID-19 Vaccines Authorized in the European Union (EU) to Prevent COVID-19, Following Evaluation by the European Medicines Agency (EMA); European Medicines Agency: Amsterdam, The Netherlands; 2022. Available from: https://www.ema.europa.eu/en/human-regulatory/overview/public-health-threats/coronavirus-disease-covid-19/treatments-vaccines/vaccines-covid-19/covid-19-vaccines-authorised.
2. Cylus J, Panteli D, van Ginneken E. Who should be vaccinated first? Comparing vaccine prioritization strategies in Israel and European countries using the Covid-19 health system response monitor. Israel J Health Policy Res. 2021;10:16. doi:10.1186/s13584-021-00453-1
3. Pfeiffer-Ruiz M, Schroder V. COVID-19 vaccination strategy in Germany. Clin Soc Work Health Intervention. 2021;12:31–34. doi:10.22359/cswhi_12_2_05
4. Steiger E, Rass S, Seidel A, Kroll L, Czihal T. COVID-19 vaccination in medical practices in Germany. Deutsches Aerzteblatt International. 2021;118:756–757. doi:10.3238/arztebl.m2021.0354
5. Desson Z, Kauer L, Otten T, Peters JW, Paolucci F. Finding the way forward: COVID-19 vaccination progress in Germany, Austria and Switzerland. Health Policy Technol. 2022;11:100584. doi:10.1016/J.HLPT.2021.100584
6. Seddig D, Maskileyson D, Davidov E, Ajzen I, Schmidt P. Correlates of COVID-19 vaccination intentions: attitudes, institutional trust, fear, conspiracy beliefs, and vaccine skepticism. Soc Sci Med. 2022;302:114981. doi:10.1016/j.socscimed.2022.114981
7. Wichmann O, Scholz S, Waize M, et al. Welche Impfquote ist notwendig, um COVID-19 zu kontrollieren? Epidemiologisches Bulletin. 2021;27:3–13. doi:10.25646/8742
8. Watson OJ, Barnsley G, Toor J, Hogan AB, Winskill P, Ghani AC. Global impact of the first year of COVID-19 vaccination: a mathematical modelling study. Lancet Infect Dis. 2022;22(9):1293–1302. doi:10.1016/S1473-3099(22)
9. Cuadros DF, Moreno CM, Musuka G, Miller FD, Coule P, MacKinnon NJ. Association Between Vaccination Coverage Disparity and the Dynamics of the COVID-19 Delta and Omicron Waves in the US. Front Med. 2022;9:898101. doi:10.3389/fmed.2022.898101
10. Fobiwe JP, Martus P, Poole BD, Jensen JL, Joos S. Influences on Attitudes Regarding COVID-19 Vaccination in Germany. Vaccines. 2022;10(5):658. doi:10.3390/vaccines10050658
11. Morales DX, Beltran TF, Morales SA. Gender, socioeconomic status, and COVID-19 vaccine hesitancy in the US: an intersectionality approach. Sociol Health Illn. 2022;44(6):953–971. doi:10.1111/1467-9566.13474
12. Nehal KR, Steendam LM, Campos Ponce M, van der Hoeven M, Smit GSA. Worldwide Vaccination Willingness for COVID-19: a Systematic Review and Meta-Analysis. Vaccines. 2021;9(10):1071. doi:10.3390/vaccines9101071
13. Raciborski F, Samel-Kowalik P, Gujski M, Pinkas J, Arcimowicz M, Jankowski M. Factors Associated with a Lack of Willingness to Vaccinate against COVID-19 in Poland: a 2021 Nationwide Cross-Sectional Survey. Vaccines. 2021;9(9):1000. doi:10.3390/vaccines9091000
14. Aw J, Seng JJB, Seah SSY, Low LL. COVID-19 Vaccine Hesitancy—A Scoping Review of Literature in High-Income Countries. Vaccines. 2021;9(8):900. doi:10.3390/vaccines9080900
15. Rzymski P, Zeyland J, Poniedziałek B, Malecka I, Wysocki J. The Perception and Attitudes toward COVID-19 Vaccines: a Cross-Sectional Study in Poland. Vaccines. 2021;9(4):382. doi:10.3390/vaccines9040382
16. Price D, Bonsaksen T, Ruffolo MC, et al. Willingness to Take the COVID-19 Vaccine as Reported Nine Months after the Pandemic Outbreak: a Cross-National Study. Soc Sci. 2021;10(11):442. doi:10.3390/socsci10110442
17. Morales GI, Lee S, Bradford A, De Camp A, Tandoc EC. Exploring vaccine hesitancy determinants during the COVID-19 pandemic: an in-depth interview study. Qualitative Res Health. 2022;2:100045. doi:10.1016/j.ssmqr.2022.100045
18. Soares P, Rocha J, Moniz M, et al. Factors Associated with COVID-19 Vaccine Hesitancy. Vaccines. 2021;9(3):300. doi:10.3390/vaccines9030300
19. Ruiz JB, Bell RA. Predictors of intention to vaccinate against COVID-19: results of a nationwide survey. Vaccine. 2021;39(7):1080–1086. doi:10.1016/j.vaccine.2021.01.010
20. Reno C, Maietti E, Fantini MP, et al. Enhancing COVID-19 Vaccines Acceptance: results from a Survey on Vaccine Hesitancy in Northern Italy. Vaccines. 2021;9(4):378. doi:10.3390/vaccines9040378
21. Ling RR, Ramanathan K, Tan FL, et al. Myopericarditis following COVID-19 vaccination and non-COVID-19 vaccination: a systematic review and meta-analysis. Lancet Respir Med. 2022;10(7):679–688. doi:10.1016/S2213-2600(22)
22. Vallone MG, Falcón AL, Castro HM, et al. Thrombotic events following Covid-19 vaccines compared to Influenza vaccines. Eur J Intern Med. 2022;99:82–88. doi:10.1016/j.ejim.2022.03.002
23. Kim MS, Jung SY, Ahn JG, et al. Comparative safety of mRNA COVID-19 vaccines to influenza vaccines: a pharmacovigilance analysis using WHO international database. J Med Virol. 2022;94(3):1085–1095. doi:10.1002/jmv.27424
24. Cohen SE, Gao DY, Kahn JS, Rosmarin DH. Comparison of constitutional and dermatologic side effects between COVID-19 and non–COVID-19 vaccines: review of a publicly available database of vaccine side effects. J Am Acad Dermatol. 2021;86(1):248–249. doi:10.1016/j.jaad.2021.09.044
25. Katzman JG, Katzman JW. Primary Care Clinicians as COVID-19 Vaccine Ambassadors. J Prim Care Community Health. 2021;12:215013272110070. doi:10.1177/21501327211007026
26. Walsh JC, Comar M, Folan J, Williams S, Kola-Palmer S. The psychological and behavioural correlates of COVID-19 vaccine hesitancy and resistance in Ireland and the UK. Acta Psychologica. 2022;225:103550. doi:10.1016/j.actpsy.2022.103550
27. Ratzan S, Schneider EC, Hatch H, Cacchione J. Missing the Point - How Primary Care Can Overcome Covid-19 Vaccine “Hesitancy.”. N Engl J Med. 2021;384(25):e100. doi:10.1056/NEJMP2106137
28. Lo C, Chiu L, Qian A, et al. Association of Primary Care Physicians Per Capita With COVID-19 Vaccination Rates Among US Counties. JAMA network open. 2022;5(2):e2147920. doi:10.1001/jamanetworkopen.2021.47920
29. Fiscella K, Meldrum S, Franks P, et al. Patient Trust: is it related to patient-centered behavior of primary care physicians? Med Care. 2004;42(11):1049–1055. doi:10.1097/00005650-200411000-00003
30. Benin AL, Wisler-Scher DJ, Colson E, Shapiro ED, Holmboe ES. Qualitative Analysis of Mothers’ Decision-Making About Vaccines for Infants: the Importance of Trust. Pediatrics. 2006;117(5):1532–1541. doi:10.1542/peds.2005-1728
31. Thom DH. Physician behaviors that predict patient trust. J Fam Pract. 2001;50(4):323–328.
32. Jacobson RM, St. Sauver JL, Griffin JM, MacLaughlin KL, Finney Rutten LJ. How health care providers should address vaccine hesitancy in the clinical setting: evidence for presumptive language in making a strong recommendation. Hum Vaccin Immunother. 2020;16(9):2131–2135. doi:10.1080/21645515.2020.1735226
33. Breckenridge LA, Burns D, Nye C. The use of motivational interviewing to overcome COVID-19 vaccine hesitancy in primary care settings. Public Health Nurs. 2022;39(3):618–623. doi:10.1111/phn.13003
34. Day P, Strenth C, Kale N, Schneider FD, Arnold EM. Perspectives of primary care physicians on acceptance and barriers to COVID-19 vaccination. Family Med Commun Health. 2021;9(4):e001228. doi:10.1136/fmch-2021-001228
35. Leung KC, Mui C, Chiu WY, et al. Impact of patient education on influenza vaccine uptake among community-dwelling elderly: a randomized controlled trial. Health Educ Res. 2017;32(5):455–464. doi:10.1093/her/cyx05336
36. Burger MN, Mayer M, Steimanis I. Repeated information of benefits reduces COVID-19 vaccination hesitancy: experimental evidence from Germany. PLoS One. 2022;17(6):e0270666. doi:10.1371/journal.pone.0270666
37. Bone A, Guthmann J-P, Nicolau J, Lévy-Bruhl D. Population and risk group uptake of H1N1 influenza vaccine in mainland France 2009–2010: results of a national vaccination campaign. Vaccine. 2010;28(51):8157–8161. doi:10.1016/j.vaccine.2010.09.096
38. Cambon L, Schwarzinger M, Alla F. Increasing acceptance of a vaccination program for coronavirus disease 2019 in France: a challenge for one of the world’s most vaccine-hesitant countries. Vaccine. 2022;40(2):178–182. doi:10.1016/j.vaccine.2021.11.023
39. Fisher KA, Nguyen N, Crawford S, Fouayzi H, Singh S, Mazor KM. Preferences for COVID-19 vaccination information and location: associations with vaccine hesitancy, race and ethnicity. Vaccine. 2021;39(45):6591–6594. doi:10.1016/j.vaccine.2021.09.058
40. Jentzsch A, Geier A, Bleckwenn M, Schrimpf A. Differences in Demographics of Vaccinees, Access to, and Satisfaction with SARS-CoV-2 Vaccination Procedures between German General Practices and Mass Vaccination Centers. Vaccines. 2022;10(11):1823. doi:10.3390/vaccines10111823
41. Brauns H, Scherer S, Steinmann S. The CASMIN educational classification in international comparative research. In: Hoffmeyer-Zlotnik JHP, Wolf C, editors. Advances in Cross-National Comparison: A European Working Book for Demographic and Socio-Economic Variables (221–244). New York, NY, USA: Springer Science+Business Media; 2003. doi:10.1007/978-1-4419-9186-7_11.
42. Drennan J. Cognitive interviewing: verbal data in the design and pretesting of questionnaires. J Adv Nurs. 2003;42(1):57–63. doi:10.1046/j.1365-2648.2003.02579.x
43. Štěpánek L, Janošíková M, Nakládalová M, Štěpánek L, Boriková A, Vildová H. Motivation to COVID-19 Vaccination and Reasons for Hesitancy in Employees of a Czech Tertiary Care Hospital: a Cross-Sectional Survey. Vaccines. 2021;9(8):863. doi:10.3390/vaccines9080863
44. Dodd RH, Pickles K, Nickel B, et al. Concerns and motivations about COVID-19 vaccination. Lancet Infect Dis. 2021;21(2):161–163. doi:10.1016/S1473-3099(20)
45. Wentzell E, Racila A-M. The social experience of participation in a COVID-19 vaccine trial: subjects’ motivations, others’ concerns, and insights for vaccine promotion. Vaccine. 2021;39(17):2445–2451. doi:10.1016/j.vaccine.2021.03.036
46. Benis A, Seidmann A, Ashkenazi S. Reasons for Taking the COVID-19 Vaccine by US Social Media Users. Vaccines. 2021;9(4):315. doi:10.3390/vaccines9040315
47. Moore R, Purvis RS, Hallgren E, et al. Motivations to Vaccinate Among Hesitant Adopters of the COVID-19 Vaccine. J Community Health. 2022;47(2):237–245. doi:10.1007/s10900-021-01037-5
48. Newman PA, Logie CH, Lacombe-Duncan A, et al. Parents’ uptake of human papillomavirus vaccines for their children: a systematic review and meta-analysis of observational studies. BMJ Open. 2018;8(4):e019206. doi:10.1136/bmjopen-2017-019206
49. Pires CAA. Global Predictors of COVID-19 Vaccine Hesitancy: a Systematic Review. Vaccines. 2022;10(8):1349. doi:10.3390/vaccines1008134950
50. Ekinci Y, Gursoy D, Can AS, Williams NL. Does travel desire influence COVID-19 vaccination intentions? J Hospitality Marketing Manage. 2022;31(4):413–430. doi:10.1080/19368623.2022.2020701
51. Tharmaratnam T, D’Urzo A, Cazzola M. Medical knowledge about COVID-19 is travelling at the speed of mistrust: why this is relevant to primary care. Fam Pract. 2022;39(5):988–991. doi:10.1093/fampra/cmac001
52. Schwarzinger M, Watson V, Arwidson P, Alla F, Luchini S. COVID-19 vaccine hesitancy in a representative working-age population in France: a survey experiment based on vaccine characteristics. Lancet Public Health. 2021;6(4):e210–e221. doi:10.1016/S2468-2667(21)
53. Nguyen KH, Yankey D, Lu P-J, et al. Report of Health Care Provider Recommendation for COVID-19 Vaccination Among Adults, by Recipient COVID-19 Vaccination Status and Attitudes - United States, April-September 2021. Morbidity Mortality Weekly Rep. 2021;70(50):1723–1730. doi:10.15585/mmwr.mm7050a1
54. Robinson OC. Values and adult age: findings from two cohorts of the European Social Survey. Eur J Ageing. 2013;10(1):11–23. doi:10.1007/s10433-012-0247-3
55. Cornelis I, Van Hiel A, Roets A, Kossowska M. Age Differences in Conservatism: evidence on the Mediating Effects of Personality and Cognitive Style. J Pers. 2009;77(1):51–88. doi:10.1111/j.1467-6494.2008.00538.x
56. Latkin CA, Dayton L, Moran M, Strickland JC, Collins K. Behavioral and psychosocial factors associated with COVID-19 skepticism in the United States. Curr Psychol. 2022;41(11):7918–7926. doi:10.1007/s12144-020-01211-3
57. Levin J, Bradshaw M. Determinants of COVID-19 skepticism and SARS-CoV-2 vaccine hesitancy: findings from a national population survey of U.S. adults. BMC Public Health. 2022;22(1):1047. doi:10.1186/s12889-022-13477-2
58. Jackson ES, Tucker CM, Herman KC. Health Value, Perceived Social Support, and Health Self-Efficacy as Factors in a Health-Promoting Lifestyle. J Am Coll Health. 2007;56(1):69–74. doi:10.3200/JACH.56.1.69-74
59. Fall E, Izaute M, Chakroun-Baggioni N. How can the health belief model and self-determination theory predict both influenza vaccination and vaccination intention? A longitudinal study among university students. Psychol Health. 2018;33(6):746–764. doi:10.1080/08870446.2017.1401623
60. Ernsting A, Gellert P, Schneider M, Lippke S. A mediator model to predict workplace influenza vaccination behaviour – an application of the health action process approach. Psychol Health. 2013;28(5):579–592. doi:10.1080/08870446.2012.753072
61. Qiao S, Tam CC, Li X. Risk Exposures, Risk Perceptions, Negative Attitudes Toward General Vaccination, and COVID-19 Vaccine Acceptance Among College Students in South Carolina. Am J Health Promotion. 2021;36(1):175–179. doi:10.1177/08901171211028407
62. Coe AB, Elliott MH, Gatewood SBS, Goode J-VR, Moczygemba LR. Perceptions and predictors of intention to receive the COVID-19 vaccine. Res Social Adm Pharm. 2022;18(4):2593–2599. doi:10.1016/j.sapharm.2021.04.023
63. Husted M, Gibbons A, Cheung W, Keating S. COVID-19 vaccination hesitancy in adults in the United Kingdom: barriers and facilitators to uptake. Health Psychol. 2023. doi:10.1037/hea0001256
64. Hassan MS, Al Halbusi H, Razali A, Ariffin RNR, Williams KA. The Swedish gamble: trust in the government and self-efficacy in the battle to combat COVID-19. Curr Psychol. 2022;1–16. doi:10.1007/s12144-022-02947-w
65. Wang J, Zhu H, Lai X, et al. From COVID-19 Vaccination Intention to Actual Vaccine Uptake: a Longitudinal Study Among Chinese Adults After Six Months of a National Vaccination Campaign. Expert Rev Vaccines. 2022;21(3):385–395. doi:10.1080/14760584.2022.2021076
66. Graupensperger S, Abdallah DA, Lee CM. Social norms and vaccine uptake: college students’ COVID vaccination intentions, attitudes, and estimated peer norms and comparisons with influenza vaccine. Vaccine. 2021;39(15):2060–2067. doi:10.1016/j.vaccine.2021.03.018
67. Skjefte M, Ngirbabul M, Akeju O, et al. COVID-19 vaccine acceptance among pregnant women and mothers of young children: results of a survey in 16 countries. Eur J Epidemiol. 2021;36(2):197–211. doi:10.1007/s10654-021-00728-6
68. Steigenberger C, Flatscher-Thoeni M, Siebert U, Leiter AM. Determinants of willingness to pay for health services: a systematic review of contingent valuation studies. Eur J Health Eco. 2022;23(9):1455–1482. doi:10.1007/s10198-022-01437-x
69. Costa-Font J, Rudisill C, Harrison SE, Salmasi L. The Social Value of a SARS-CoV-2 Vaccine: willingness to Pay Estimates from Four Western Countries. Soc Sci Res Network. 2021. doi:10.2139/ssrn.3870207
70. Cerda AA, García LY. Willingness to Pay for a COVID-19 Vaccine. Appl Health Econ Health Policy. 2021;19(3):343–351. doi:10.1007/s40258-021-00644-6
71. Catma S, Varol S. Willingness to Pay for a Hypothetical COVID-19 Vaccine in the United States: a Contingent Valuation Approach. Vaccines. 2021;9(4):318. doi:10.3390/vaccines9040318
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
COVID-19 Vaccination Breakthrough Infections in a Real-World Setting: Using Community Reporters to Evaluate Vaccine Effectiveness
Reynolds MW, Xie Y, Knuth KB, Mack CD, Brinkley E, Toovey S, Dreyer NA
Infection and Drug Resistance 2022, 15:5167-5182
Published Date: 3 September 2022
Distinct Features of Vascular Diseases in COVID-19
Ceasovschih A, Sorodoc V, Shor A, Haliga RE, Roth L, Lionte C, Onofrei Aursulesei V, Sirbu O, Culis N, Shapieva A, Tahir Khokhar MA, Statescu C, Sascau RA, Coman AE, Stoica A, Grigorescu ED, Banach M, Thomopoulos C, Sorodoc L
Journal of Inflammation Research 2023, 16:2783-2800
Published Date: 6 July 2023
Dietary Supplement Consumption and Mental Health in Indonesian Adults During Second Wave of COVID-19 Pandemic
Yusof J, d'Arqom A, Andriani AP, Nasution MZ, Fatimah N, Mustika A, Handayani S, Syed Abdul Kadir SZ
Patient Preference and Adherence 2023, 17:1799-1811
Published Date: 24 July 2023
Retinal Vein Occlusion Amongst People Vaccinated by mRNA- and Viral Vector- COVID-19 Vaccines: A Systematic Review
Rachman MJ, Kalanjati VP, Rimbun R, Khadijah F
Clinical Ophthalmology 2023, 17:2825-2842
Published Date: 28 September 2023
The Pandemics of Mass Destruction: A Comparative Analysis of HIV/AIDS and Coronavirus (COVID-19)
Kajiita RM, Kang'ethe SM
Journal of Multidisciplinary Healthcare 2024, 17:889-899
Published Date: 1 March 2024