Back to Journals » Clinical Ophthalmology » Volume 20
Comparison of Reproducibility and Repeatability of Corneal Topography Measured by ATLAS 500 and ATLAS 9000 in Average Patient Population
Authors Tañá-Rivero P, Orts-Vila P, Tañá-Sanz P, Tañá-Sanz S, Ramos M, Tello-Elordi C
Received 3 December 2025
Accepted for publication 9 March 2026
Published 20 March 2026 Volume 2026:20 581736
DOI https://doi.org/10.2147/OPTH.S581736
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Sotiria Palioura
Pedro Tañá-Rivero, Paz Orts-Vila, Pedro Tañá-Sanz, Santiago Tañá-Sanz, Maria Ramos, Cristina Tello-Elordi
Department of Ophthalmology, Oftalvist, Alicante, Spain
Correspondence: Pedro Tañá-Rivero, Department of Ophthalmology, Oftalvist, C/Angel Lozano 11, Alicante, 03001, Spain, Tel +34 965 14 15 00, Email [email protected]
Purpose: To compare repeatability, reproducibility, and agreement of the Placido-based ATLAS 500 topographer (straight and swivel-out positions) with its predecessor, ATLAS 9000.
Design: Prospective, single-center, post-market observational study.
Methods: In this prospective, single-center post-market study involving 100 eyes with various corneal profiles, two operators obtained randomized, repeated measurements using the ATLAS 500 and ATLAS 9000 topographers. Parameters included corneal power, astigmatism, white-to-white distance, meridian powers, aberrations, and Placido coverage. Primary outcomes were repeatability and reproducibility; secondary analyses assessed coefficient of variation (CV), inter-device agreement, and keratoconus classification (Cohen’s κ).
Results: The ATLAS 500 showed equal or superior repeatability and reproducibility compared to ATLAS 9000 across most parameters, with lower standard deviations (SDs) for central power (K1: 0.025 vs. 0.062 D; K2: 0.023 vs. 0.058 D) and astigmatism (0.015 vs. 0.018 D). The only exception was white-to-white distance, where ATLAS 9000 had lower variability (SD 0.032 mm vs. 0.066 mm), albeit with more missing data (41 vs. 10). The ATLAS 500 yielded lower coefficients of variation for corneal power and astigmatism (e.g. CV 0.058% vs. 0.146% for K1). Bland–Altman analysis showed minimal bias for K1/K2, with narrower limits in intra-device comparisons. Inter-device variability was greater for astigmatism and WTW, with ATLAS 500 measuring smaller WTW values. The swivel-out configuration increased Placido coverage by approximately 4%. Keratoconus classification showed moderate agreement (κ = 0.50) between devices.
Conclusion: ATLAS 500 showed measurement precision comparable to or better than ATLAS 9000, with strong intra-device repeatability and broader corneal coverage in the swivel-out mode, confirming its suitability for routine corneal topography and refractive assessment.
Keywords: corneal topography, placido disk, repeatability, reproducibility, bland–altman agreement, keratoconus, ATLAS 500, ATLAS 9000
Introduction
The cornea is the primary refractive element of the eye, contributing approximately 70% of its optical power.1,2 Consequently, accurate assessment of corneal shape and curvature (corneal topography) is fundamental for clinical practice and research.
Corneal topography is a core component of modern anterior segment assessment and is routinely used to screen for ectatic disease, guide contact lens fitting, and support refractive and cataract surgery planning, particularly where accurate keratometry and astigmatism characterization affect intraocular lens selection and refractive predictability. However, measurements from different corneal imaging devices are not always interchangeable, and clinically relevant discrepancies, especially in astigmatism magnitude and axis, have been reported across platforms, underscoring the need for device-specific validation when new technology is introduced or when practices transition between systems.3,4
Placido-based corneal topography maps anterior corneal curvature by projecting concentric rings (mires) onto the tear film and analyzing their reflected spacing and distortion, yielding a high-resolution, non-contact assessment of surface shape and optical power. In clinical practice, Placido-based corneal topography plays a central role in refractive and cataract surgery planning, providing precise corneal power and astigmatism data to optimize refractive outcomes, while also enabling longitudinal monitoring of corneal disease and postoperative stability.5 Despite its strengths, Placido-derived measurements are sensitive to acquisition conditions and corneal surface quality (eg, tear film irregularity), and precision may degrade in challenging eyes or when peripheral ring capture is incomplete. Accordingly, repeatability and reproducibility studies have become essential for quantifying within-device precision, while Bland–Altman methods are commonly applied to evaluate agreement and potential bias between devices when assessing clinical comparability.6,7
Among commercially available Placido-based corneal topography systems, the ATLAS 9000 (Carl Zeiss Meditec AG, Jena, Germany) is a well-established platform that employs a 22-ring Placido disk, Cone-of-Focus™ alignment, Arc-Step™ reconstruction algorithms, and SmartCapture™ image selection to enhance repeatability and anterior corneal surface accuracy in both routine and complex cases.8 The ATLAS 500, representing the next generation of this technology, builds upon the same Placido-based measurement principles while introducing workflow and ergonomic enhancements, most notably a swivel-out measurement head designed to improve patient alignment and extend peripheral corneal coverage during data acquisition.
Despite the clinical relevance of such workflow and acquisition differences, peer-reviewed head-to-head comparative data between ATLAS 500 and ATLAS 9000 remain limited, and the degree to which measurements are comparable across devices and configurations in routine practice warrants evaluation. The purpose of this study was therefore to compare the repeatability, reproducibility, and agreement of corneal topography measurements obtained with the ATLAS 500 and ATLAS 9000 under routine clinical conditions.
Methods
Study Design and Patient Selection
This was a prospective, single-center, observational, post-market clinical investigation. All participants were enrolled at Oftalvist Alicante, Spain, within the EMEA region. The study spanned approximately three months, involved a single study visit, and included 100 eyes of 100 adult participants.
This study was conducted in accordance with ISO 14155:2020, the Declaration of Helsinki, and applicable local regulations. Ethical approval was obtained from the Comité Ético de Investigación con Medicamentos (CEIm) of the Health Department of the Hospital General Universitario de Alicante (Ref. CEIm: 2024–062; Ref. ISABIAL: 2024–0159). All participants provided written informed consent before enrollment. The risk-benefit evaluation confirmed that the study involved minimal risk and was ethically justified by its anticipated value for future patients.
In addition to healthy eyes, the study population included patients with post-laser vision correction (PVC), keratoconus, subclinical keratoconus, pellucid marginal corneal degeneration, and irregular astigmatism.
Patients were excluded if they had any ocular condition that could interfere with accurate image acquisition, including a history of ocular trauma, corneal disease, or other pathologies compromising measurement quality. Additional exclusion criteria included soft contact lens wear within two weeks or rigid gas-permeable (RGP) lens wear within four weeks prior to measurement, inability to maintain fixation or follow instructions, or poorly reflective corneal surfaces resulting from scarring or an unstable tear film. Eyes that were partially or completely obscured by anatomical limitations such as small palpebral fissures were also excluded. Furthermore, participants taking systemic medications known to affect corneal wound healing or hormonal balance, as well as pregnant or lactating women, were not eligible for inclusion.
Sample Size
This study included 100 eyes from 100 subjects. Two operators, each acquired three repeated measurements per eye, yielding 600 measurements for analysis. Sample size adequacy was assessed using the approach of McAlinden et al;9 based on six repeated measurements per eye, the estimated precision for repeatability was approximately 6%. As all measurements were obtained during a single visit, drop-outs were not expected. The sample size also exceeds ISO 19980 recommendations, which specify a minimum of 20 independent eyes for repeatability analysis.
Measurement Protocol
All measurements were performed during a single study visit following completion of screening procedures, with no follow-up visits planned.
To minimize bias, block randomization was applied to ensure balanced allocation of the study eye (right or left), operator order (operator 1 or 2), and device sequence (ATLAS 500 [straight], ATLAS 500 [swivel-out], or ATLAS 9000). Operators were not masked to prior measurement outputs during repeated acquisitions. At baseline, demographic and medical history data were collected, followed by a slit-lamp examination and routine diagnostic assessments. For the designated study eye, uncorrected and best-corrected visual acuity were recorded, and pachymetry (CIRRUS OCT, Carl Zeiss Meditec AG, Jena, Germany) was performed to measure corneal thickness, particularly relevant for detecting corneal thinning in keratoconus.
Each participant underwent topography with both the ATLAS 500 and ATLAS 9000 devices. Two certified operators performed the measurements in randomized order. Each operator obtained three consecutive scans per configuration, allowing brief intervals between captures for blinking and tear-film stabilization. For the ATLAS 500, measurements were acquired in both the straight and swivel-out head positions to evaluate potential differences in corneal coverage.
This design yielded six measurements per configuration (2 operators × 3 repeats), enabling assessment of intra-observer repeatability and inter-observer reproducibility.
For each acquisition, a comprehensive set of quantitative and qualitative corneal parameters was recorded. These included corneal power, astigmatism magnitude, WTW distance, corneal aberrations, and the Placido coverage area. Placido coverage represents the proportion of the Placido disk area successfully utilized for topographic reconstruction. Coverage quality is classified by the device as green (good acquisition) or yellow/red (reduced area utilization), with reduced coverage typically resulting from shadowing caused by anatomical factors such as brows, nose, ptosis, or deep-set eyes.10
During image acquisition, the device software automatically applied manufacturer-defined quality-control criteria. Scans that did not meet these criteria generated on-screen warning messages (eg., fixation errors, pupil detection failure, inadequate Placido coverage, or image decentration) were excluded from analysis. Only scans meeting the predefined quality indicators were retained.
All measurements were performed using the manufacturer’s software (version 1.0). Device settings were applied consistently across all acquisitions in accordance with routine clinical use and manufacturer specifications. Standard calibration and laterality checks were performed at device start-up and after any change in device conditions, as recommended by the manufacturer.
All acquisitions were performed in a semi-darkened room without pharmacologic mydriasis.
Study Devices
This clinical investigation involved two Placido-based corneal topography systems manufactured by Carl Zeiss Meditec AG: ATLAS 9000 and ATLAS 500. Both instruments utilize Placido-disk reflection technology, which projects a series of concentric illuminated rings onto the anterior corneal surface. The reflected pattern is captured by an integrated camera, and specialized software reconstructs a high-resolution topographic map based on the spacing and distortion of the rings. This non-contact method enables assessment of anterior corneal curvature, shape irregularities, and optical power distribution.
ATLAS 9000 projects 22 concentric Placido rings onto the anterior corneal surface, each containing 180 data points reflected back to the analysis system. The instrument reconstructs corneal curvature using Arc-Step™ and Cone-of-Focus™ algorithms, ensuring precise surface alignment and accurate topographic mapping. Its integrated SmartCapture™ system automatically selects the most sharply focused frames, improving measurement precision and repeatability across both regular and irregular corneas. ATLAS 500 represents the next generation of ATLAS 9000 while incorporating several workflow and ergonomic advancements. It features a swivel-out measurement head, enabling improved patient alignment and extended corneal coverage, particularly useful in eyes with deep-set anatomy or limited palpebral fissures. The system also includes updated software algorithms for automated ring analysis and real-time quality feedback.
Study Endpoints – Primary Endpoints
The primary efficacy endpoints were the overall repeatability (agreement between repeated measurements under identical conditions by the same operator) and overall reproducibility (agreement between measurements obtained under varying conditions, such as different operators) for both ATLAS 500 and ATLAS 9000.
Secondary Endpoints
- The coefficient of variation (CV%) for both repeatability and reproducibility of ATLAS 500 and ATLAS 9000.
- The agreement between both devices for corresponding topographic parameters.
- The maximum absolute mean difference among the three repeated measurements per patient and operator.
- The difference in mapped corneal area between the straight and swivel-out head positions of ATLAS 500, assessing the impact of measurement geometry on Placido coverage.
Study Endpoints – Exploratory Endpoint
An exploratory endpoint assessed the agreement in dichotomized keratoconus classification (normal/abnormal) between ATLAS 500 and ATLAS 9000.
Safety
Adverse events (AEs) and device deficiencies were recorded observationally.
Statistical Analysis
All statistical analyses were conducted using SAS® software, Version 9.4 or higher (SAS Institute Inc., Cary, NC, USA). Analyses included both descriptive and inferential statistics. Precision analysis was performed for eyes with at least two valid measurements. For each device (ATLAS 500 and ATLAS 9000), repeatability and reproducibility were estimated using a random-effects analysis of variance (ANOVA) model, allowing separation of intra- and inter-operator variability. The ANOVA model included the operator as a random factor to account for inter-operator variability in the precision estimates. Agreement analysis between ATLAS 500 (straight and swivel-out) and ATLAS 9000 was evaluated using Bland–Altman plots for repeated measures across key topographic parameters: corneal power, astigmatism, WTW distance, meridians, and corneal aberrations. Repeated measurements (2 operators × 3 acquisitions per eye) were consolidated at the eye level prior to analysis. Specifically, measurements obtained from both operators were averaged per eye to generate a single representative value for each parameter before Bland-Altman agreement and reliability calculations were performed. For the exploratory endpoint, the dichotomized keratoconus classification derived from ATLAS 500 was compared with ATLAS 9000. For keratoconus categorisation, each eye was classified based on all six measurements (2 operators × 3 repeats); an eye was considered abnormal if at least two measurements were labelled abnormal. Cohen’s κ was calculated using one final classification per eye per device.
Results
Patient Demographics
A total of 100 adult participants were enrolled in the study. The mean age was 51.6±17 years. Demographic characteristics are summarized in Table 1.
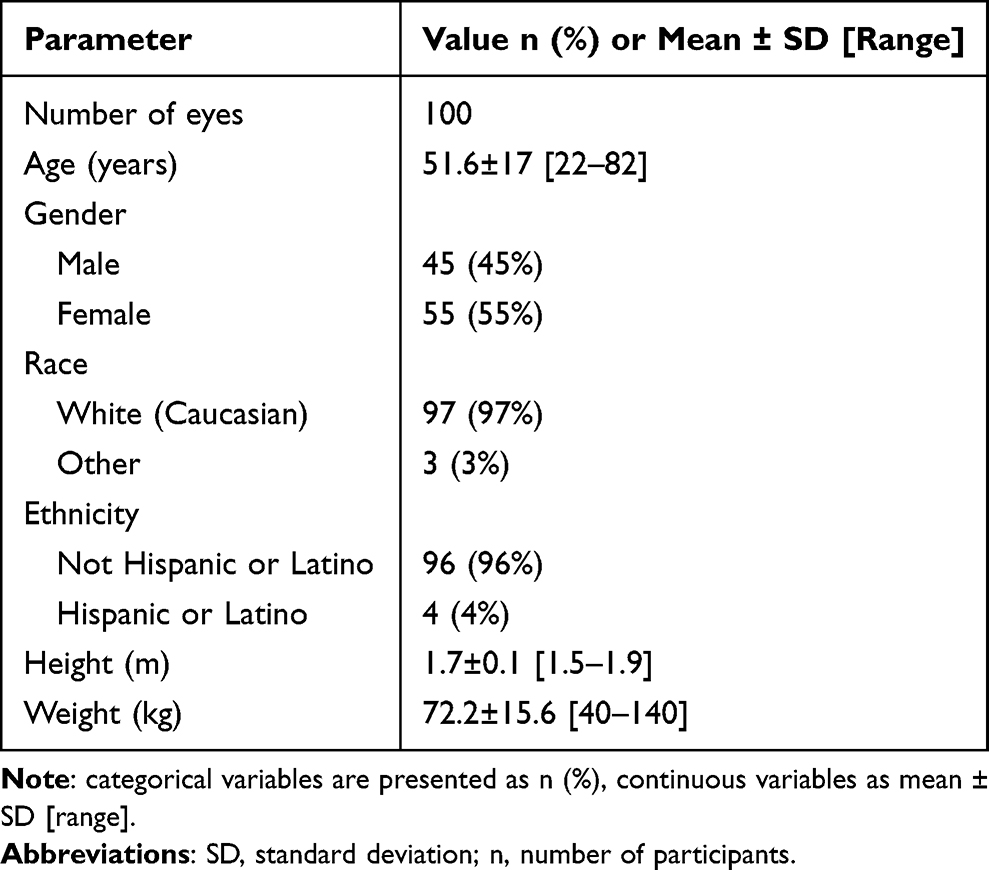 |
Table 1 Patient Demographics |
Repeatability and Reproducibility
The repeatability results are summarized in Table 2. For corneal power measurements, ATLAS 500 demonstrated lower repeatability standard deviations (SDs) than ATLAS 9000 for both K1 (0.025 vs. 0.062) and K2 (0.023 vs. 0.058). Astigmatism repeatability was also slightly better with ATLAS 500 (SD 0.015) compared to ATLAS 9000 (SD 0.018). For peripheral hemi-meridian zones (0–3 mm), repeatability SDs for ATLAS 500 ranged from 0.066 to 0.125, substantially lower than those for ATLAS 9000 (0.225–0.833). Zernike-based aberration analysis showed comparable or improved repeatability with ATLAS 500. The only parameter favoring ATLAS 9000 was the WTW measurement (SD 0.032 vs. 0.066), though ATLAS 9000 had a higher rate of missing data (41 vs. 10).
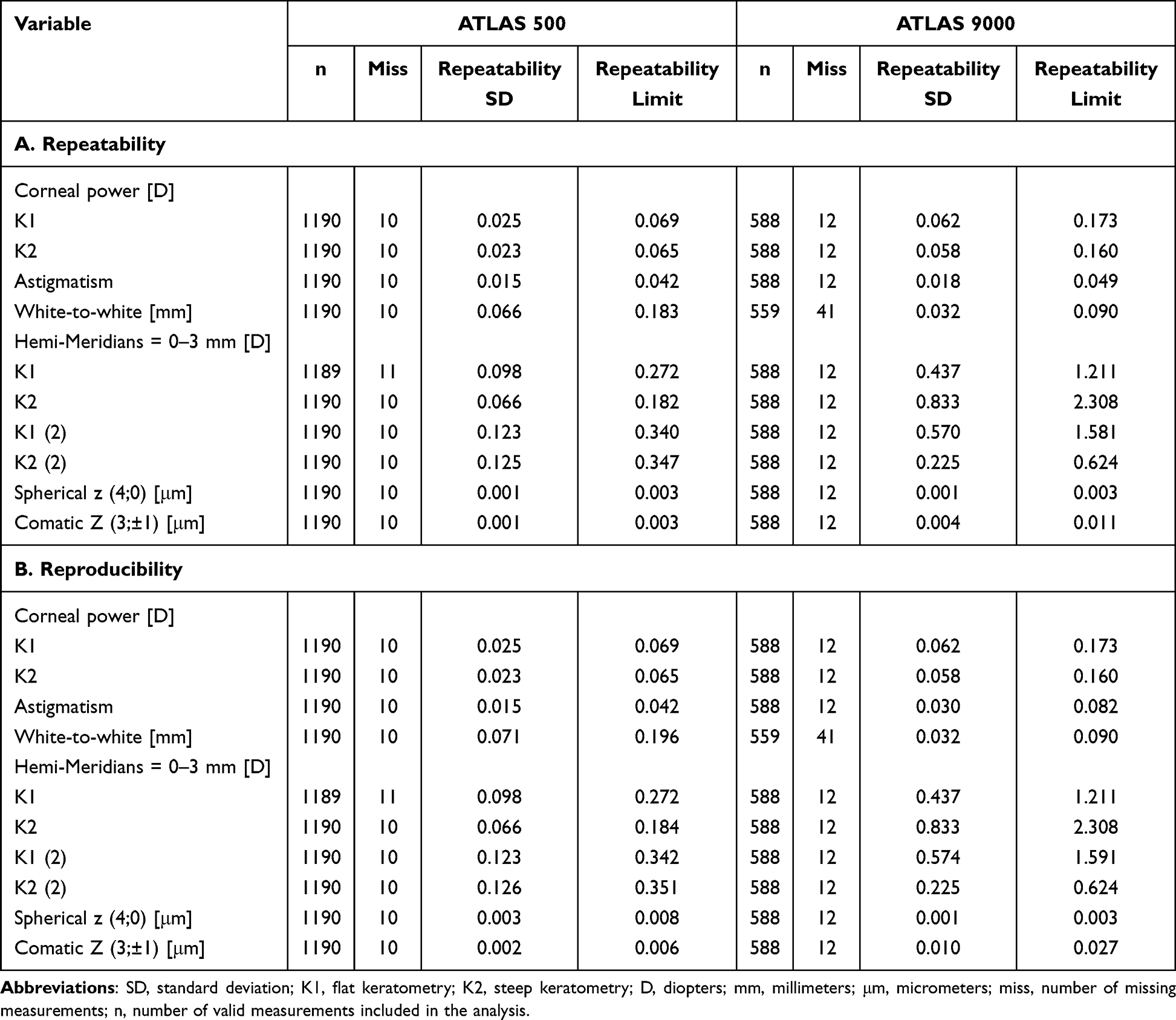 |
Table 2 Repeatability and Reproducibility for ATLAS 500 (Straight and Swivel-Out) and ATLAS 9000 |
The reproducibility results are summarized in Table 2. ATLAS 500 demonstrated lower reproducibility SDs for corneal power (K1: 0.025 vs. 0.062; K2: 0.023 vs. 0.058) and astigmatism (0.015 vs. 0.030) compared to ATLAS 9000. Peripheral hemi-meridian measurements again favored ATLAS 500, with reproducibility SDs between 0.066 and 0.126, versus 0.225–0.833 for ATLAS 9000. Spherical aberration reproducibility was comparable for both devices (0.003 μm vs. 0.001 μm), while coma measurements were more consistent with ATLAS 500 (0.002 μm vs. 0.010 μm). As for repeatability, ATLAS 9000 showed slightly better performance for WTW distance but with more missing data (41 vs. 10).
Coefficient of Variation (CV)
For central corneal power, ATLAS 500 exhibited substantially lower CVs than ATLAS 9000, with both repeatability and reproducibility CVs of 0.058% for K1 and 0.054% for K2, compared with 0.146% and 0.132%, respectively, for ATLAS 9000. Astigmatism measurements also demonstrated lower variability with ATLAS 500 (1.525%) versus 1.837–3.083% for ATLAS 9000.
In the peripheral hemi-meridian zone (0–3 mm), ATLAS 500 again showed superior performance, with repeatability and reproducibility CVs below 0.3%, compared with values mostly exceeding 1% (except for K2=0.5%) for ATLAS 9000 (Table 3).
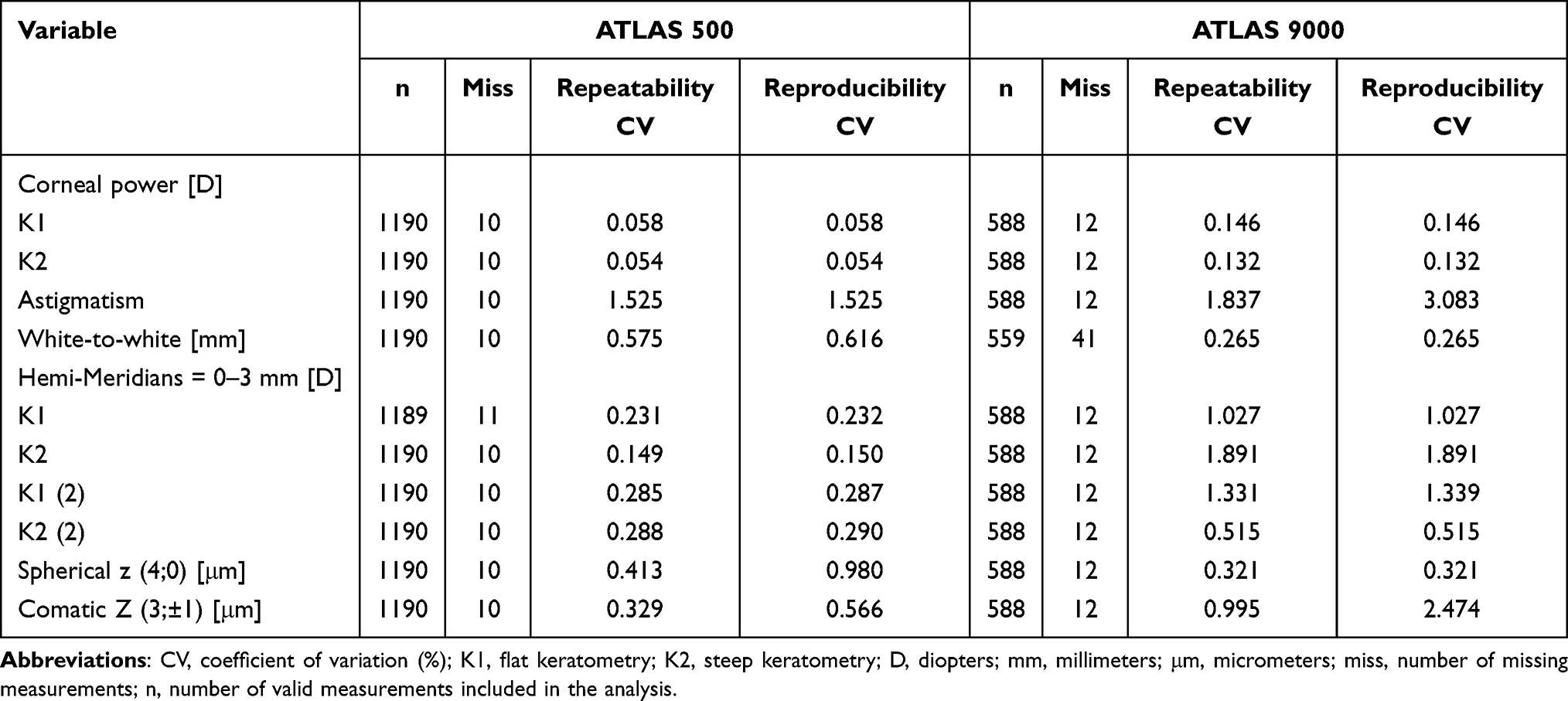 |
Table 3 Overall Coefficient of Variation for ATLAS 500 (Straight and Swivel-Out) and ATLAS 9000 |
Regarding corneal aberrations, both devices demonstrated high measurement precision. ATLAS 500 showed lower variability for comatic aberrations, with repeatability and reproducibility coefficients of variation (CV) of 0.329% and 0.566%, respectively, compared to 0.995% and 2.474% for ATLAS 9000. Conversely, ATLAS 9000 exhibited slightly better consistency for spherical aberration, with repeatability and reproducibility CVs of 0.321%, compared to 0.413% and 0.980% for ATLAS 500.
Agreement Between ATLAS 500 and ATLAS 9000
Corneal Power: Agreement between ATLAS 500 and ATLAS 9000 showed minimal bias for K1 (−0.011 D; 95% LoA −0.777 to 0.754 D) and K2 (0.021 D; 95% LoA −0.682 to 0.724 D). Comparison of ATLAS 500 straight and swivel-out configurations demonstrated similarly small mean differences for K1 (−0.011 D; 95% LoA −0.239 to 0.216 D) and K2 (−0.007 D; 95% LoA −0.240 to 0.225 D), with no evident proportional bias across the measurement range (Figure 1A).
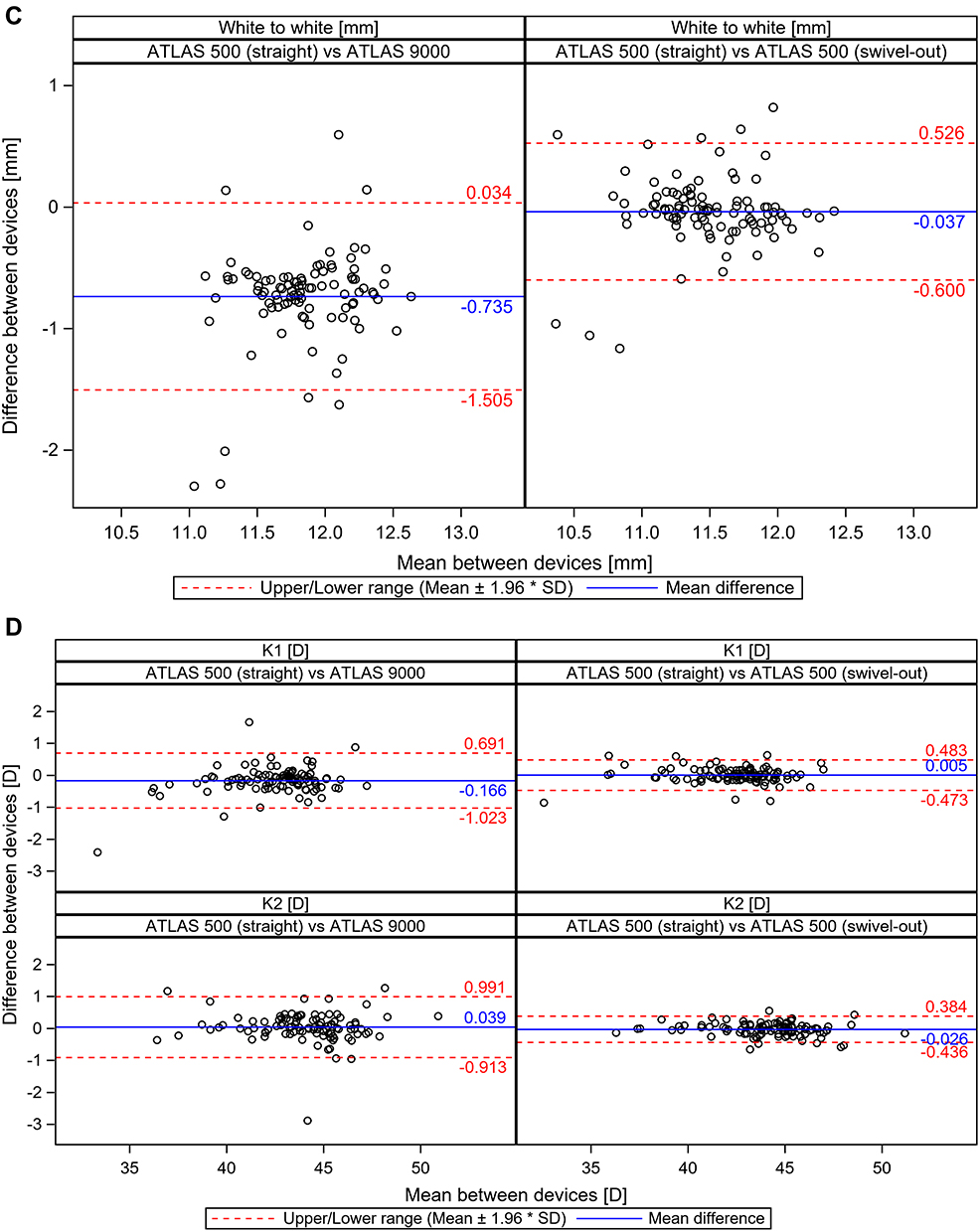
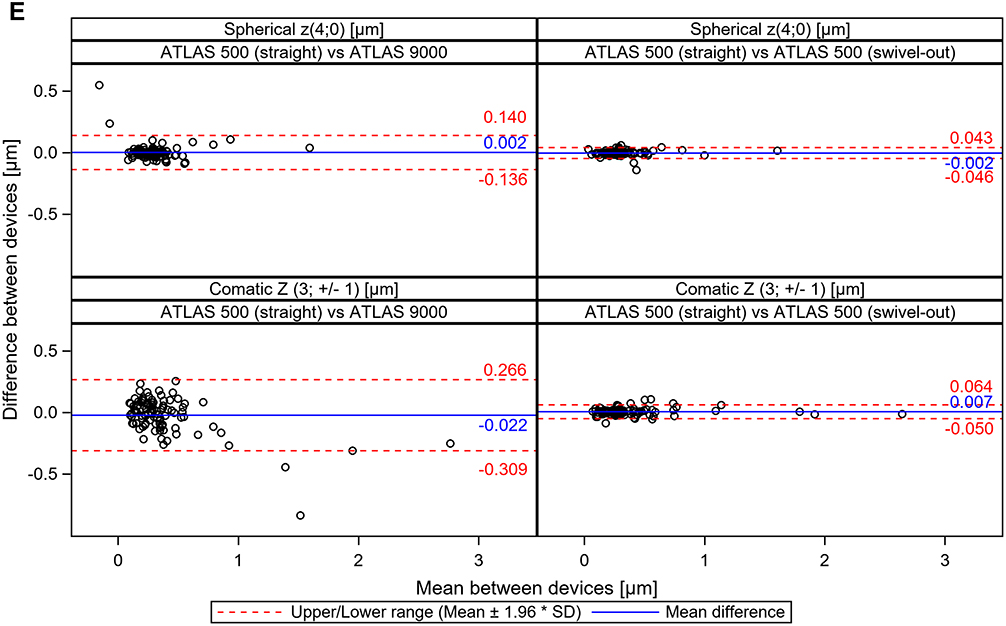
Figure 1 continued. Figure 1 continued. Figure 1 (A) Agreement of corneal power (K1 and K2) for ATLAS 500 (straight and swivel-out) and ATLAS 9000. (B) Agreement of astigmatism for ATLAS 500 (straight and swivel-out) and ATLAS 9000. (C). Agreement of white-to-white for ATLAS 500 (straight and swivel-out) and ATLAS 9000. (D) Agreement of hemi-meridians (0–3 mm) for ATLAS 500 (straight and swivel-out) and ATLAS 9000. (E) Agreement of corneal aberrations for ATLAS 500 (straight and swivel-out) and ATLAS 9000.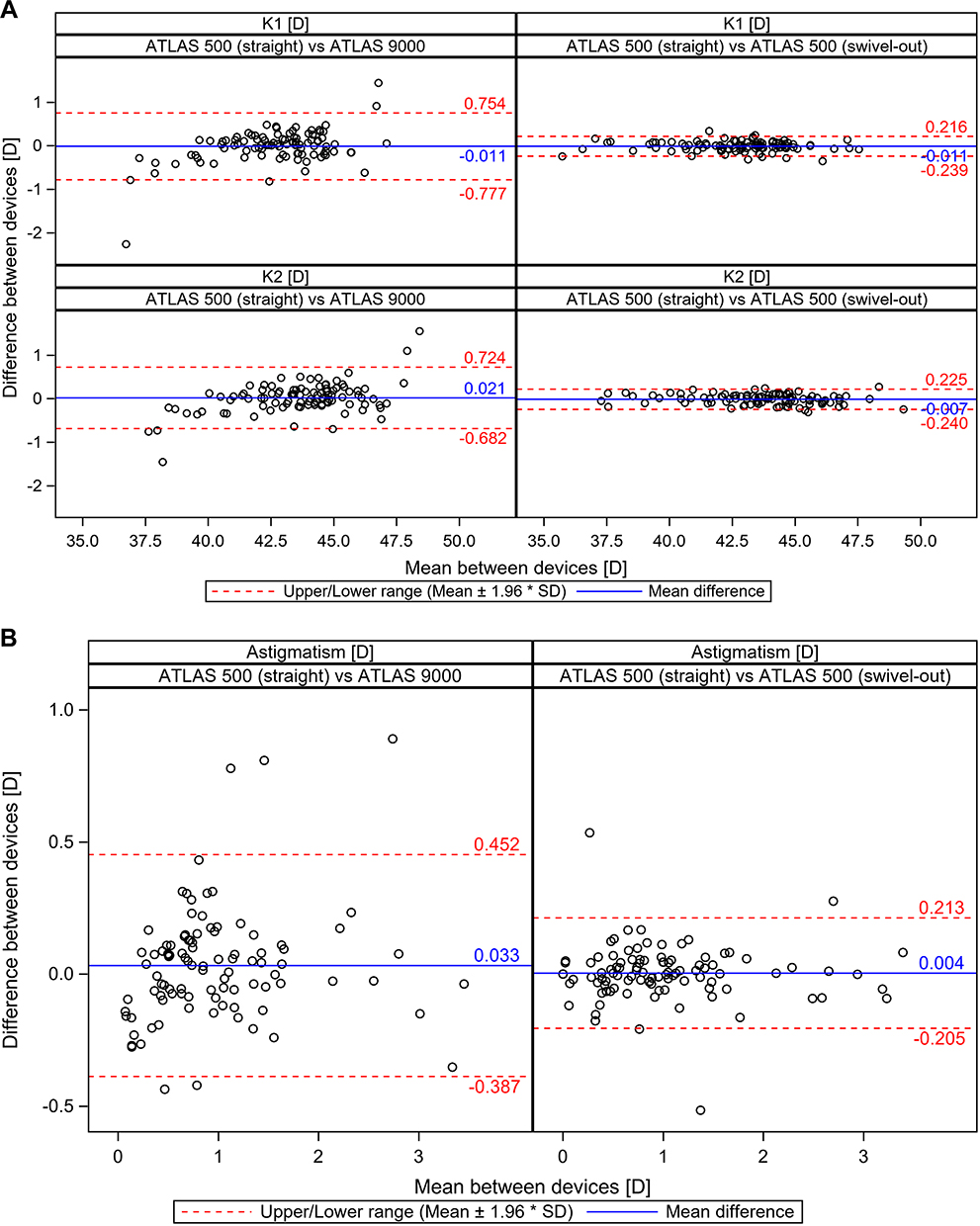
Astigmatism: The ATLAS 500 (straight configuration) measured slightly higher astigmatism values than the ATLAS 9000, as reflected by a small positive mean difference (0.033 D) and relatively wider limits of agreement (−0.387 to 0.452 D), with a few points approaching the ±2 SD boundaries. In contrast, comparison between ATLAS 500 straight and swivel-out configurations demonstrated negligible bias (0.004 D) and narrower limits of agreement (−0.205 to 0.213 D), with tighter clustering of measurements around the mean difference (Figure 1B).
WTW Distance: ATLAS 500 (straight vs ATLAS 9000) demonstrated a clear negative bias (−0.735 mm) with relatively wide limits of agreement (−1.505 to 0.034 mm), indicating systematically smaller WTW measurements compared with ATLAS 9000 and greater inter-device variability. In contrast, comparison between ATLAS 500 straight and swivel-out configurations showed minimal bias (−0.037 mm) and narrower limits of agreement (−0.600 to 0.526 mm), reflecting improved intra-device consistency (Figure 1C).
Hemi-Meridian Measurements: For K1 (0–3 mm hemi-meridian), ATLAS 500 (straight vs ATLAS 9000) showed a slight negative bias (−0.166 D) with wider limits of agreement (−1.023 to 0.691 D), whereas the straight vs swivel-out comparison demonstrated negligible bias (0.005 D) and narrower limits (−0.473 to 0.483 D).
For K2, inter-device comparison showed minimal bias (0.039 D) but broader limits (−0.913 to 0.991 D), while intra-device comparison revealed smaller bias (−0.026 D) and tighter limits (−0.436 to 0.384 D), indicating improved consistency within ATLAS 500 (Figure 1D).
Corneal Aberrations: For spherical aberration (Z(4;0)), both devices demonstrated strong agreement with negligible bias (0.002 μm) and relatively narrow limits of agreement (−0.136 to 0.140 μm), while intra-device ATLAS 500 comparison showed the narrowest limits (−0.046 to 0.043 μm), indicating excellent consistency. For comatic aberration (Z(3;±1)), ATLAS 500 exhibited a slight negative bias relative to ATLAS 9000 (−0.022 μm) with broader limits (−0.309 to 0.266 μm), whereas intra-device comparison demonstrated minimal bias (0.007 μm) and tighter limits (−0.050 to 0.064 μm) (Figure 1E).
Maximum Absolute Mean Difference
The maximum absolute mean difference was calculated for each operator and patient across all parameters. Overall, ATLAS 500 showed smaller within-patient variations and greater inter-operator consistency than ATLAS 9000.
For both operators using ATLAS 500, mean differences in corneal power (K1/K2) were below 0.2 D, and astigmatism differences averaged around 0.10 D. Peripheral and hemi-meridian zones showed slightly higher variability but remained within clinically acceptable limits. Differences in WTW and corneal aberrations were minimal.
In contrast, ATLAS 9000 exhibited larger mean differences and greater dispersion, particularly for peripheral and hemi-meridian parameters, with occasional high outliers exceeding 10 D in some cases. Inter-operator variability was also more pronounced, confirming lower reproducibility compared with ATLAS 500.
Placido Coverage Area
The comparison of Placido coverage between measurement head positions demonstrated consistently higher corneal coverage in the swivel-out position for both operators. For Operator 1, the mean coverage increased from 85.6±4.6% in the straight position to 89.8±4.6% in the swivel-out position, with a mean within-patient difference of –4.18±2.69%, favoring the swivel-out configuration. Similarly, Operator 2 recorded mean coverage values of 85.4±4.7% (straight) and 89.5±4.8% (swivel-out), with a mean difference of –4±2.7%, again favoring the swivel-out position. Overall, both operators showed greater and more uniform Placido disk coverage with the swivel-out configuration (Table 4).
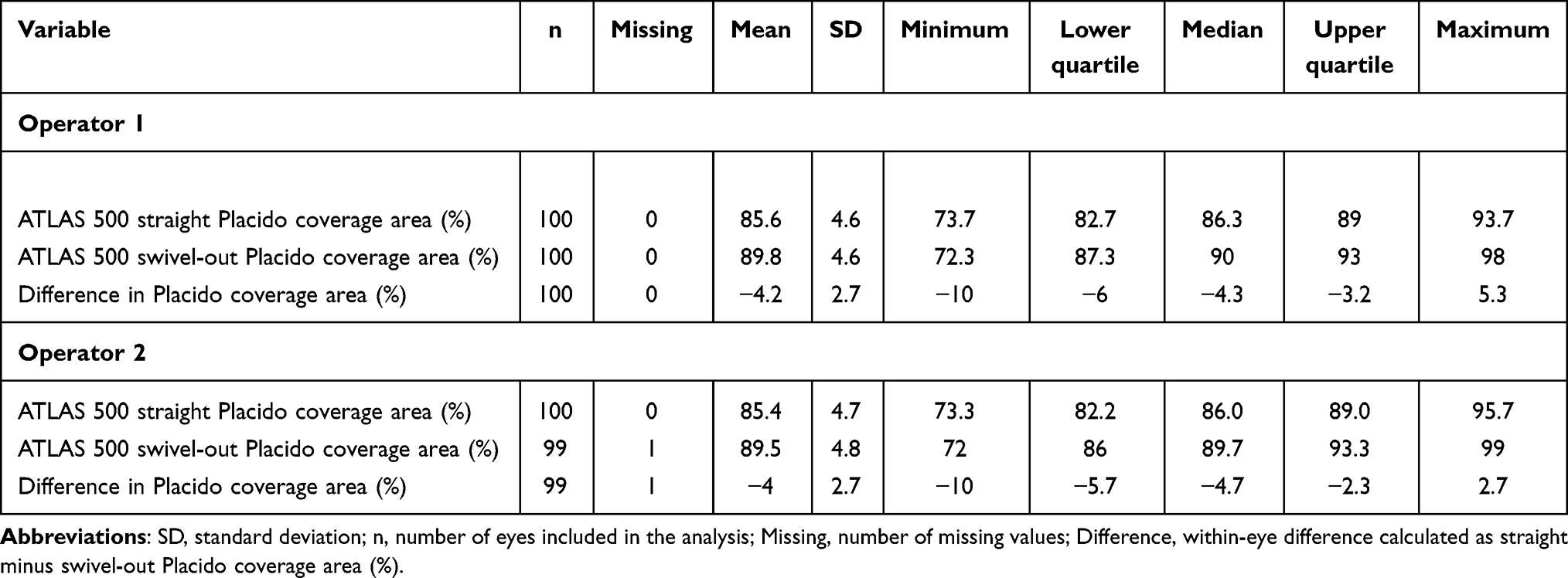 |
Table 4 Difference in Placido Coverage Area by Position (Straight vs Swivel-Out) for ATLAS 500 |
Agreement of Dichotomized Keratoconus Categorization
The agreement between ATLAS 500 (straight and swivel-out positions) and ATLAS 9000 in classifying eyes as normal or abnormal for keratoconus was assessed using Cohen’s kappa (κ).
Agreement between ATLAS 500 and ATLAS 9000 for keratoconus classification (normal vs abnormal) was moderate. For the straight configuration, 57 eyes (58.2%) were classified as normal by both devices and 20 eyes (20.4%) as abnormal by both devices, while 8 eyes (8.2%) were classified as normal by ATLAS 500 but abnormal by ATLAS 9000, and 13 eyes (13.3%) were classified as abnormal by ATLAS 500 but normal by ATLAS 9000. Cohen’s κ was 0.50, indicating moderate agreement. Similar results were observed for the swivel-out configuration, with κ = 0.50. (Table 5).
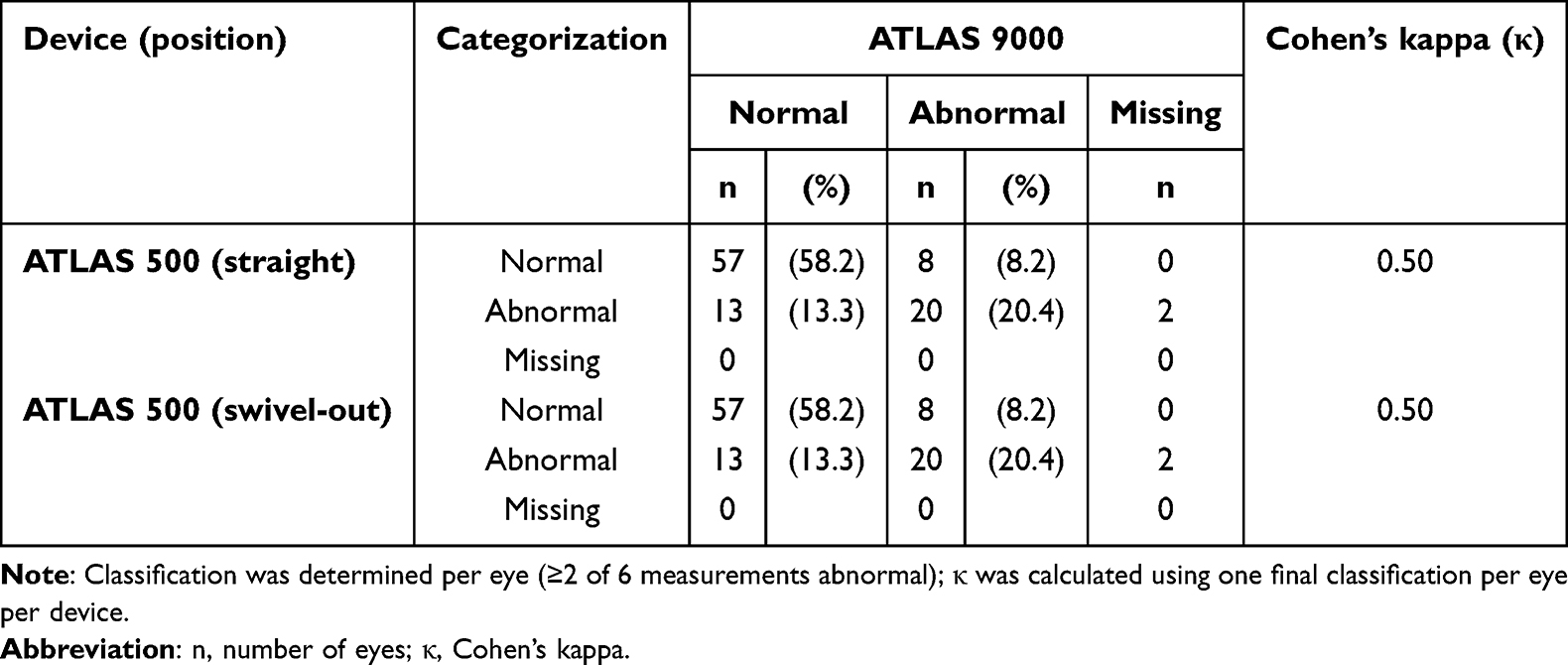 |
Table 5 Agreement of Keratoconus Categorization |
Safety Analysis
Safety was evaluated in an observational manner only by assessment and documentation of AEs. There were no (zero) AEs reported.
Discussion
Several studies have highlighted that corneal measurements obtained from different topography or keratometric devices should not be considered interchangeable.11,12 Variations in optical design, calibration methods, and computational algorithms can produce small but systematic discrepancies, even when both systems demonstrate strong internal precision. In this context, evaluating the performance of new-generation topographers against established devices is essential to confirm measurement reliability and clinical comparability. The present clinical investigation compared the repeatability and reproducibility of ATLAS 500 (straight and swivel-out positions) and ATLAS 9000 topographers.
Both devices demonstrated excellent repeatability and reproducibility, confirming their suitability for clinical use. Previous studies on Placido-based and hybrid systems, including ATLAS 9000, have similarly reported strong within-device precision for corneal curvature and astigmatism measurements, although inter-device agreement can vary due to differences in design and algorithms.13 ATLAS 500 in our study exhibited lower SDs for corneal power, astigmatism, and peripheral parameters compared with ATLAS 9000. The only exception was the WTW distance, where ATLAS 9000 showed slightly lower SDs (0.032 mm vs. 0.066 mm). However, this apparent advantage was offset by a higher proportion of missing data with ATLAS 9000 (41 vs. 10), limiting the robustness of this comparison. The CV further supported these findings. For central corneal power, ATLAS 500 demonstrated markedly lower CVs (0.058% and 0.054% for K1 and K2, respectively) compared with ATLAS 9000 (0.146% and 0.132%). Similarly, astigmatism reproducibility was substantially better with ATLAS 500 (1.525% vs. 3.083%), indicating greater inter-operator consistency. Conversely, ATLAS 9000 yielded lower CVs for WTW (0.265%) and spherical aberration (0.321%), although comatic aberration showed less variability with ATLAS 500 (repeatability CV 0.329% vs. 0.995% for ATLAS 9000).
These differences are clinically meaningful, as lower variability directly enhances confidence in applications such as toric IOL calculation and postoperative corneal stability assessments.14
The Bland–Altman method was used to evaluate agreement between ATLAS 500 and ATLAS 9000 at the eye level. Given the inherent biological variability of in vivo corneal measurements, comparison with an established device is essential to determine whether observed differences remain clinically acceptable and whether devices may be used interchangeably.9 To ensure independence of observations, repeated measurements (2 operators × 3 acquisitions) were consolidated at the eye level prior to agreement and reliability analyses, thereby avoiding pseudo-replication and strengthening statistical validity.
For central corneal power (K1 and K2), bias between devices was minimal, suggesting that differences are unlikely to influence routine clinical decision-making. Astigmatism showed a small positive bias with broader variability between devices, indicating that caution may be warranted when comparing measurements across platforms, particularly in borderline cases.
WTW measurements demonstrated a systematic negative bias of ATLAS 500 relative to ATLAS 9000, with relatively wide limits of agreement, suggesting limited interchangeability for this parameter. In contrast, intra-device comparisons (straight vs swivel-out) consistently showed negligible bias and narrower limits across parameters, supporting strong internal consistency of the ATLAS 500 platform.
For higher-order aberrations, spherical aberration showed excellent inter-device agreement, while comatic aberration demonstrated slightly wider inter-device variability but stable intra-device performance. Overall, the ATLAS 500 exhibited robust internal reproducibility, with most inter-device differences remaining small and likely clinically acceptable for routine corneal assessment. Interchangeability between the straight and swivel-out configurations should be interpreted in the context of the magnitude of observed bias and limits of agreement for individual parameters. For central keratometry (K1 and K2), Bland–Altman analysis demonstrated mean differences close to zero with narrow limits of agreement, supporting practical interchangeability for routine corneal power assessment. Similar patterns were observed for selected higher-order aberrations, where intra-device agreement was strong and variability was limited.
Across both operators, the ATLAS 500 yielded lower within-patient mean differences for corneal power, astigmatism, and peripheral meridian values compared to the ATLAS 9000. The only exception was WTW, which demonstrated smaller variability with ATLAS 9000. These findings highlight the superior measurement stability of the ATLAS 500 across users and sessions.
The swivel-out head position of ATLAS 500 consistently achieved broader Placido disk coverage than the straight position (mean difference −4.175±2.686% for operator 1 and −3.992±2.673% for operator 2). Conventional Placido-based topography systems are known to experience nasal shadowing and incomplete peripheral data capture, particularly in eyes with prominent nasal bridges, deep-set anatomy, or steep corneal curvature. Large-cone Placido designs may produce “data gaps” where reflected rings are partially blocked or truncated by anatomical structures, and missing data are sometimes interpolated.15
The swivel-out configuration of ATLAS 500 is designed to minimize these limitations by modifying the projection geometry, thereby reducing nasal obstruction and enabling more complete reflection from the peripheral cornea. The resulting improvement in Placido coverage enhances visualization of the anterior surface and supports more reliable topographic assessment in anatomically challenging eyes.
Agreement between ATLAS 500 and ATLAS 9000 in dichotomized keratoconus classification (normal/abnormal) was moderate for both ATLAS 500 configurations (Cohen’s κ = 0.50). Concordant classification was observed in the majority of eyes. The keratoconus categorization analysis was intended to evaluate the consistency of device outputs across configurations rather than diagnostic accuracy.
The high repeatability and reproducibility demonstrated by ATLAS 500 supports its reliability for routine clinical use and longitudinal corneal monitoring. This is particularly relevant for screening and follow-up of conditions such as keratoconus, post-laser vision correction, and irregular astigmatism, where consistent measurements are essential for timely referral and management decisions.
The observed operator-independent performance enhances applicability in high-volume and multi-clinician settings, reducing measurement variability between visits. The increased Placido coverage achieved with the swivel-out configuration improves corneal assessment in anatomically challenging eyes, further supporting accurate evaluation across diverse patient populations.
The single-visit design supports conclusions related to short-term repeatability, inter-operator reproducibility, and configuration agreement, but does not address between-day repeatability, longer-term measurement drift, or thresholds relevant to longitudinal disease monitoring. Accordingly, implications should be limited to short-term clinical use and workflow considerations.
Strengths
This study provides one of the first independent clinical evaluations of the ATLAS 500, a next-generation Placido-based corneal topographer, under real-world clinical conditions. The prospective, randomized, and operator-balanced design minimized measurement bias and enabled robust assessment of both intra- and inter-operator variability. Inclusion of eyes with a broad range of corneal conditions (healthy, post-refractive, and ectatic) enhanced the clinical relevance of the findings.
Furthermore, the use of standardized calibration protocols, high-frequency repeated measurements, and adherence to ISO 14155:2020 and ICH-GCP standards ensured methodological rigor. The study also introduced analysis of swivel-out geometry performance, providing novel insights into the impact of measurement head design on Placido coverage and precision.
Limitations
This investigation was designed primarily to assess measurement precision rather than clinical outcomes. The evaluation was conducted in a controlled, single-center setting under standardized acquisition conditions, which may not fully reflect routine clinical variability such as tear-film instability, fixation fluctuations, or suboptimal patient alignment. Only short-term repeatability and inter-operator reproducibility were assessed during a single visit; therefore, long-term stability and instrument drift over time were not evaluated. The comparison was limited to another Placido-based system (Atlas 9000); expanding the evaluation to include tomographic or Scheimpflug-based platforms could offer complementary validation. Additionally, the study population included eyes with a range of corneal conditions, reflecting real-world clinical use; however, the study was not powered to perform disease-specific subgroup analyses. Future studies focusing on homogeneous subgroups (eg, normal eyes or ectatic corneas) may further elucidate potential differences in device performance across specific clinical states.
Conclusion
In summary, this study demonstrates that ATLAS 500 shows high repeatability and inter-operator reproducibility across a broad range of corneal parameters within a single study visit. Agreement between the straight and swivel-out configurations was strong for selected clinically relevant outputs, particularly central keratometry and selected higher-order aberrations, supporting practical configuration comparability under controlled conditions.
Acknowledgments
Editorial and writing support was provided by GP Communications and funded by Carl Zeiss Meditec AG.
Funding
Study sponsored by Carl Zeiss Meditec AG, Jena, Germany.
Disclosure
PTR reports grants from Alcon Laboratories, BVI, Carl Zeiss Meditec, Hoya Surgical AG, HumanOptics AG, Johnson & Johnson, and Vialase Inc, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Patel S, Tutchenko L. The refractive index of the human cornea: a review. Contact Lens Anterior Eye. 2019;42(5):575–14. doi:10.1016/j.clae.2019.04.018
2. Meek KM, Knupp C, Lewis PN, et al. Structural control of corneal transparency, refractive power and dynamics. Eye. 2024;39(4):644–650. doi:10.1038/s41433-024-02969-7
3. Martin R. Cornea and anterior eye assessment with placido-disc keratoscopy, slit scanning evaluation topography and scheimpflug imaging tomography. Indian J Ophthalmol. 2018;66(3):360–366. doi:10.4103/ijo.IJO_850_17
4. Holladay JT, Koch DD. Total keratometric power vs total corneal power. J Cataract Refract Surg. 2022;48(7):858. doi:10.1097/j.jcrs.0000000000000890
5. Carl Zeiss Meditec AG. Superior performance designed for how you practice the new ATLAS® Take YOUR practice to the next level.
6. Wylȩgała A, Mazur R, Bolek B, et al. Reproducibility, and repeatability of corneal topography measured by Revo NX, Galilei G6 and Casia 2 in normal eyes. PLoS One. 2020;15(4):e0230589. doi:10.1371/journal.pone.0230589
7. Ventura BV, Al-Mohtaseb Z, Wang L, et al. Repeatability and comparability of corneal power and corneal astigmatism obtained from a point-source color light–emitting diode topographer, a Placido-based corneal topographer, and a low-coherence reflectometer. J Cataract Refract Surg. 2015;41(10):2242–2250. doi:10.1016/j.jcrs.2015.11.003
8. Zeiss Atlas 9000 - Jody Myers Eye Equipment. Available from: https://jodymyerseye.com/product/zeiss-atlas-9000.
9. McAlinden C, Khadka J, Pesudovs K. Precision (repeatability and reproducibility) studies and sample-size calculation. J Cataract Refract Surg. 2015;41(12):2598–2604. doi:10.1016/j.jcrs.2015.06.029
10. Arbelaez MC, Versaci F, Vestri G, et al. Use of a support vector machine for keratoconus and subclinical keratoconus detection by topographic and tomographic data. Ophthalmology. 2012;119(11):2231–2238. doi:10.1016/j.ophtha.2012.06.005
11. Bland JM, Altman DG. Measuring agreement in method comparison studies. Stat Methods Med Res. 1999;8(2):135–160. doi:10.1177/096228029900800204
12. Giavarina D. Understanding Bland Altman analysis. Biochem Med. 2015;25(2):141. doi:10.11613/BM.2015.015
13. Cavas-Martínez F, De la Cruz Sánchez E, Nieto Martínez J, et al. Corneal topography in keratoconus: state of the art. Eye and Vision. 2016;3(1):5. doi:10.1186/s40662-016-0036-8
14. Dharwadkar S, Nayak B. Corneal topography and tomography. J Clin Ophthalmol Res. 2015;3(1):45. doi:10.4103/2320-3897.149379
15. Kanclerz P, Khoramnia R, Wang X. Current developments in corneal topography and tomography. Diagnostics. 2021;11(8):1466. doi:10.3390/diagnostics11081466
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.