")
Back to Journals » Drug Design, Development and Therapy » Volume 18
Comparison of Remimazolam versus Sevoflurane on the Postoperative Quality of Recovery in Cervical Spine Surgery: A Prospective Randomized Controlled Double-Blind Trial
Authors Lee J , Han DW, Kim NY , Kim KS, Yang Y, Yang J, Lee HS , Kim MH
Received 27 September 2023
Accepted for publication 18 January 2024
Published 23 January 2024 Volume 2024:18 Pages 121—132
DOI https://doi.org/10.2147/DDDT.S441622
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Georgios Panos
Jiwon Lee,1 Dong Woo Han,1 Na Young Kim,2 Keun-Su Kim,3 Yunil Yang,1 Juyeon Yang,4 Hye Sun Lee,4 Myoung Hwa Kim1
1Department of Anesthesiology and Pain Medicine, Anesthesia and Pain Research Institute, Yonsei University College of Medicine, Gangnam Severance Hospital, Seoul, Republic of Korea; 2Department of Anesthesiology and Pain Medicine, Anesthesia and Pain Research Institute, Yonsei University College of Medicine, Seoul, Republic of Korea; 3Department of Neurosurgery, Spine and Spinal Cord Institute, Gangnam Severance Spine Hospital, Yonsei University College of Medicine, Seoul, Republic of Korea; 4Department of Research Affairs, Biostatistics Collaboration Unit, Yonsei University College of Medicine, Seoul, Republic of Korea
Correspondence: Myoung Hwa Kim, Department of Anesthesiology and Pain Medicine, Anesthesia and Pain Research Institute, Yonsei University College of Medicine, Gangnam Severance Hospital, Seoul, Republic of Korea, Fax +82-2-3463-0940, Email [email protected]
Purpose: Remimazolam is a newly developed ultra-short-acting benzodiazepine. We compared overall functional recovery, including the postoperative Quality of Recovery-15 (QoR-15) questionnaire scores, between balanced inhalational anesthesia using sevoflurane and total intravenous anesthesia (TIVA) with remimazolam in patients undergoing anterior cervical discectomy and fusion (ACDF).
Patients and Methods: Seventy-two patients were randomized to the remimazolam (group R) or sevoflurane (group S) group. The primary outcome was the total QoR-15 score on postoperative day (POD) 1. We also assessed the total QoR-15 score on POD2, sub-scores of the QoR-15, perioperative parameters, and postoperative recovery profiles. Group-time interaction effects on the QoR-15 and its sub-scores were analyzed using a linear mixed model.
Results: The total QoR-15 score on POD1 (120.2 in group R vs 114.3 in group S, P=0.189) was not statistically different between the groups. There were no significant group-time interaction effects on total QoR-15 scores. Instead, patients in group R showed significantly better sub-scores in psychological and postoperative nausea and vomiting (PONV) items on POD1, as well as a lower degree of PONV, than those in group S. Among the five dimensions of the QoR-15, a significant group-time interaction effect was observed for psychological support. Group R showed significantly less changeability in blood pressure and heart rate with a lower dose of intraoperatively administered vasopressor than group S.
Conclusion: Considering QoR-15, including PONV reduction, and intraoperative hemodynamic stability, remimazolam can be used as the novel and safe anesthetic agent for maintaining general anesthesia instead of sevoflurane in patients undergoing ACDF.
Plain Language Summary: Compared with balanced anesthesia using sevoflurane, total intravenous anesthesia with remimazolam showed better aspects for psychological support and postoperative nausea/vomiting in the quality of recovery and hemodynamic stability.
Despite comparable total Quality of Recovery-15 scores, remimazolam-based total intravenous anesthesia could be a secure and suitable choice for patients undergoing cervical spine surgery.
Keywords: cervical spine surgery, quality of recovery, remimazolam, sevoflurane, total intravenous anesthesia
Introduction
Remimazolam is a sedative of the benzodiazepine class‒an ester-based gamma-aminobutyric acid type A (GABAA) receptor agonist. It has several distinct advantages over existing benzodiazepines, including rapid onset, a short context-sensitive half-time, being metabolized by tissue esterase independent of hepatic or renal function, producing an inactive metabolite, existence of an antidote (antagonized by flumazenil), and hemodynamic stability.1–7 Remimazolam was recently developed and is safe even with continuous intravenous infusion; as a result, it has been gradually used as an anesthetic for sedation or general anesthesia.5,8 However, there is a lack of studies clarifying the postoperative functional recovery of patients after remimazolam administration, especially compared with that of balanced inhalational anesthesia.
Moreover, if the quality of postoperative recovery is low, the actual length of stay in hospital or the medical cost increases, further affecting the long-term prognosis as well as lowering patient satisfaction.9–11 Accordingly, anesthesiologists must consider hypnotic agents and anesthetic methods that provide fast and high-quality recovery, minimizing perioperative morbidities and the time taken to resume daily activities. The Quality of Recovery (QoR)-15 questionnaire, which was created by simplifying the existing QoR-40 questionnaire, is a well-known, useful, and valuable self-rated and self-completed postoperative questionnaire to assess the condition of patients in the postoperative phase.12,13
When anesthesia or surgery is administered, even if there are no complications, patients often complain of inconvenience during the recovery period, which can inevitably negatively impact the quality of life of patients. While balanced inhalational anesthesia is the most used and conventional method of general anesthesia, the prevailing opinion is that volatile agents, including sevoflurane, have a higher frequency of postoperative nausea and vomiting (PONV) and lead to greater neuroendocrine stress hormone secretion than does total intravenous anesthesia (TIVA).14,15 However, propofol is also associated with vascular pain on injection, risk of awakening during anesthesia, and the possibility of adverse effects, such as metabolic acidosis, lipidemia, and platelet dysfunction. Above all, it has the disadvantage of not having an antidote.6 Consequently, it is necessary to develop a method of TIVA through a combination of new intravenous anesthetics, such as remimazolam.
In this study, we compared postoperative functional recovery between remimazolam-based TIVA and balanced inhalational anesthesia with sevoflurane in patients undergoing anterior cervical discectomy and fusion (ACDF) using the QoR-15 questionnaire.
Materials and Methods
Participant Enrollment and Assignment
Patients aged ≥20 and ≤70 years with an American Society of Anesthesiologists physical status of I−III who were scheduled for elective ACDF surgery in the Neurosurgery Department at our institution between September 2021 and August 2022 were included. Patients with a tolerance or hypersensitivity to benzodiazepines, dependence on or addiction to psychotropic drugs or alcohol, and body mass index (BMI) >30 kg/m2 and those who refused to provide consent were excluded. After obtaining informed consent, the patients were randomly allocated to the sevoflurane (group S) or remimazolam (group R) group in a 1:1 ratio. The randomization sequence was produced by a researcher who did not participate in this study using computer-generated block randomization. Each generated letter was concealed in a sequentially numbered opaque envelope. On the day of the operation, another researcher opened the envelope, and each patient was assigned to a study group according to the letter in the envelope. All patients, surgeons, and outcome assessors were blinded to the group allocation of patients.
Anesthesia and Intervention
Patients were admitted to the operating theatre without premedication and monitored using electrocardiography, pulse oximetry, and non-invasive blood pressure measurements. A SedLine® sensor (Masimo Corp, Irvine, CA, USA) was attached to the forehead to monitor the depth of anesthesia via the patient state index (PSI) value. In group S, anesthesia was induced with 0.1 mg glycopyrrolate, 40 mg lidocaine, 1–2 mg kg−1 propofol, and 3.0 ng mL−1 target-controlled infusion (TCI) of remifentanil by applying the Minto model. In group R, anesthesia was induced with 0.1 mg glycopyrrolate, initiation of 6–12 mg kg−1 h−1 remimazolam infusion, and 3.0 ng mL−1 TCI of remifentanil by applying the Minto model. After confirmation that the patient did not respond to verbal commands or have an eyelash reflex, 0.8–1.0 mg kg−1 rocuronium was administered for neuromuscular blockade (NMB) before airway intubation with an endotracheal tube sized 8.0 mm (for men) or 7.0 mm (for women). Anesthesia was maintained by sevoflurane inhalation at 1.5–2 vol% and an infusion of remifentanil in group S, while remimazolam was infused at 1.0–2.0 mg kg−1 h−1 with an infusion of remifentanil in group R. The depth of anesthesia was adjusted with a mean arterial pressure (MAP) within 20% of the baseline value and a PSI value of 25–50 points. Rocuronium was continuously infused to maintain a train‐of‐four (TOF) count of 1–2 with moderate NMB in both groups. To reduce postoperative pain, 20 mg of nefopam and 1 g of acetaminophen were slowly injected intraoperatively, and 75 µg of palonosetron was also intravenously administered to prevent PONV. Patient-controlled analgesia (PCA) was also prepared with 10 µg kg−1 of fentanyl, 2 mg kg−1 of nefopam, and 0.3 mg of ramosetron and administered via the intravenous route. At the end of the operation, the anesthetic agent and remifentanil administration was terminated; further, NMB was evaluated by a TOF test using a nerve stimulator and reversed using 0.07 mg kg−1 of neostigmine with 0.05 mg kg−1 of glycopyrrolate. Extubation was performed after spontaneous breathing and recovery of consciousness were confirmed. Subsequently, patients were transferred to the post-anesthetic care unit (PACU). Pain intensity while moving and resting was evaluated using a 10-point numeric rating scale (NRS). Additionally, the requested rescue analgesics and their consumption (as morphine equivalent dose) were recorded. We also assessed complaints of nausea or vomiting as well as the requested antiemetics. In the ward, we collected data on postoperative pain intensity and degree of PONV using an NRS, as well as those on administered rescue analgesics and antiemetics within 6, 24, and 48 h postoperatively.
Outcome Assessment
The Korean version of the QoR-15 questionnaire, which is as efficient and reliable as the original English version,12 was used to measure the overall functional recovery after surgery of patients. It comprises five dimensions that address questions concerning the overall status of postoperative functional recovery, including physical comfort (five items), emotional state (four items), psychological support (two items), physical independence (two items), and pain (two items). Each item was rated on an 11-point scale, with higher scores for positive items, lower scores for negative items, and a total score ranging from a minimum of 0 (worst recovery quality) to a maximum of 150 (best recovery quality) points. We visited the patients a total of three times for this survey on the day before surgery after consent was obtained, as well as on postoperative days 1 and 2 (POD1 and POD2, respectively). The questionnaire was administered by a researcher who was not involved in anesthesia administration and was blinded to the assigned groups.
The total QoR-15 score on POD1 was the primary endpoint. The following outcomes were also assessed: total amount of remimazolam and remifentanil administered during surgery; PSI values and hemodynamic data, including MAP; heart rate (HR); and peripheral oxygen saturation before induction (baseline), immediately after tracheal intubation, at surgical incision, at 1 h after surgical incision, at the end of surgery, immediately after extubation, and on arrival and discharge from the PACU; duration of loss of consciousness, a PSI value of <50 points, and intubation after anesthesia commencement; and recovery of consciousness, a PSI value of >50 points, and extubation after anesthesia completion. In addition, recovery profiles, such as the NRS of pain intensity and PONV; administration of rescue analgesics or antiemetics at the PACU and ward; duration of PACU stay; length of hospital stay after surgery; and postoperative complications were evaluated.
Statistical Analyses
The sample size was obtained based on a previous study.16 The absolute mean change in the total QoR-15 value was >13 points; the perceived postoperative recovery health status of patients was improved. Additionally, the average (standard deviation) value of the total QoR-15 score on POD1 was 114 (18) points in intermediate surgeries, which included ACDF surgery. Therefore, we estimated that 34 patients would be required in each group, with 90% power at a significance level (alpha) of 0.05. Factoring in a 5% drop-out rate, we enrolled a total of 72 patients with 36 patients in each group.
The Shapiro–Wilk test was used to confirm a normal distribution of the patient characteristics, including patient age, height, weight, and all variables related to the perioperative phase. For continuous variables, we presented the mean (standard deviation, SD) or median (interquartile range) with comparisons using an independent two-sample t-test or Wilcoxon rank-sum test, as appropriate, according to normality distribution. For categorical variables, we listed a percentage in the total number of patients with comparisons using the chi-square test of Fisher’s exact test, as appropriate. We applied linear mixed models and generalized estimating equations with an unstructured covariance matrix for continuous and binary outcomes with repeated measures. We examined the effect of the intervention on each outcome between the groups at each time point in terms of between-group differences (group effects), within-group changes from baseline (time effects), and between-group differences in changes from baseline (group-by-time interaction effects). Statistical analyses were performed using SAS (version 9.4; SAS Institute, Cary, NC, USA). Two-sided P-values of <0.05 indicated statistical significance.
Results
Of the 76 patients assessed for eligibility, four were excluded because they refused to provide consent. Ultimately, 72 patients were included and randomized to either group S or group R for the final analyses (Figure 1). The preoperative characteristics of patients did not differ between the groups (Table 1).
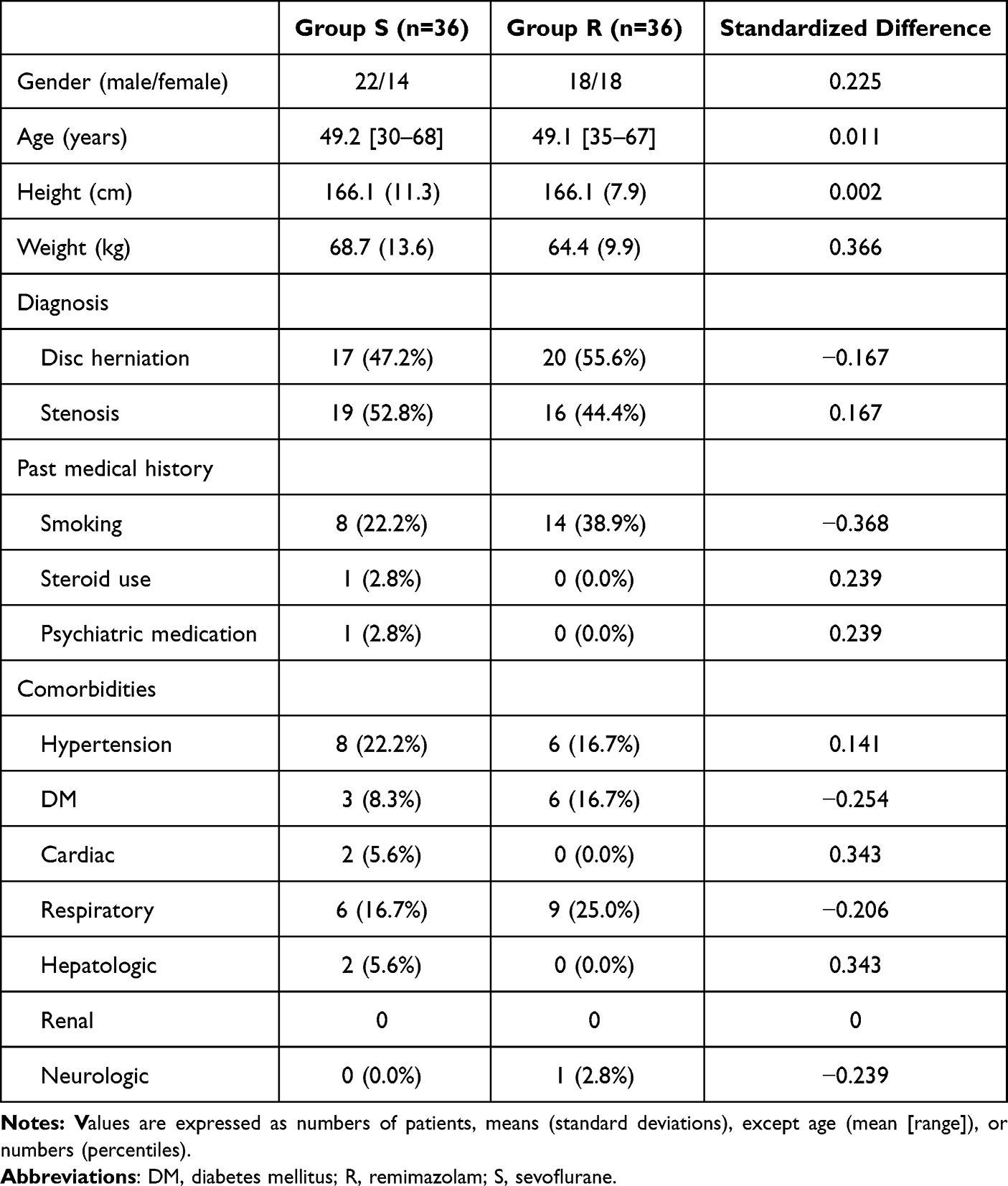 |
Table 1 Patients’ Characteristics |
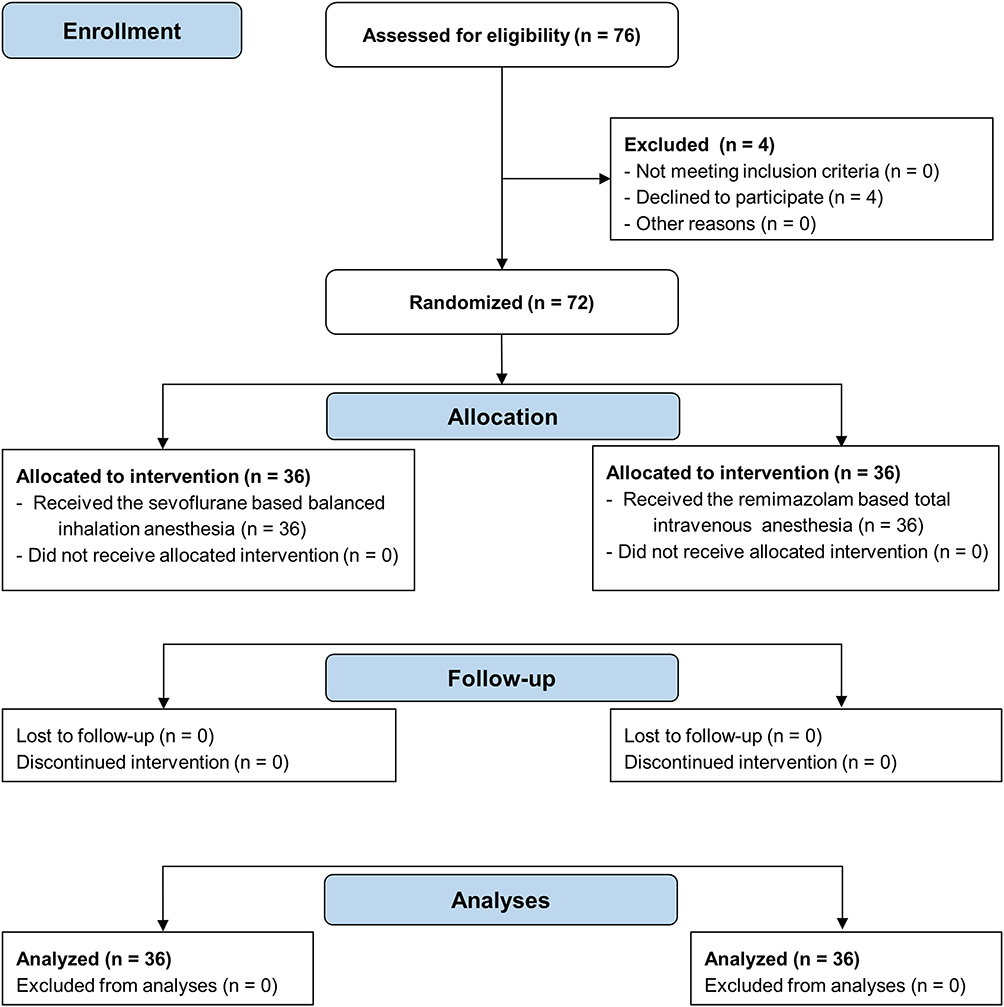 |
Figure 1 CONSORT flow diagram. Adapted from Schulz KF, Altman DG, Moher D. CONSORT 2010 Statement: Updated Guidelines for Reporting Parallel Group Randomised Trials. PLoS Med. 2010;7(3): e1000251. Copyright: © 2010 Schulz et al. Creative Commons Attribution License. |
The total QoR-15 scores and their sub-scores at the preoperative, POD1, and POD2 time points are presented in Figures 2 and 3, as well as in Supplementary Table 1, Supplementary Figure 1 and 2. There were no statistical differences between the two groups in terms of the total QoR-15 scores measured at POD1 (114.3 [18.9] vs 120.2 [18.8] points, P=0.189). However, the total QoR-15 scores at POD1 of both groups significantly decreased compared with those from the preoperative questionnaire (P<0.05 for each), and the total QoR-15 scores at POD 2 significantly increased in both groups compared with those from POD1 (P<0.001 for each). Patients in group R showed significantly higher scores than those in group S on POD1 for 6 psychological items (8.1 vs 9.4, P<0.001) and for 13 nausea and vomiting items (7.0 vs 8.8, P=0.009) among 15 questions. Among the five dimensions of the QoR-15, there was a significant group-time interaction effect on psychological support consisting of six and seven items (P=0.015, Figure 3).
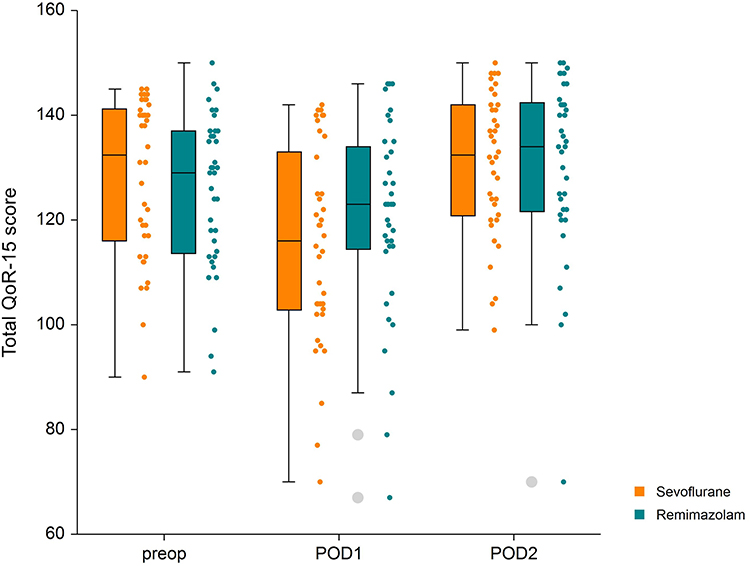 |
Figure 2 Total QoR-15 score. Boxplots represent the median, as well as the 25% and 75% interquartile range. Dot plots show the distribution of QoR-15 scores. Abbreviations: POD, postoperative day; preop, preoperative; QoR, quality of recovery. |
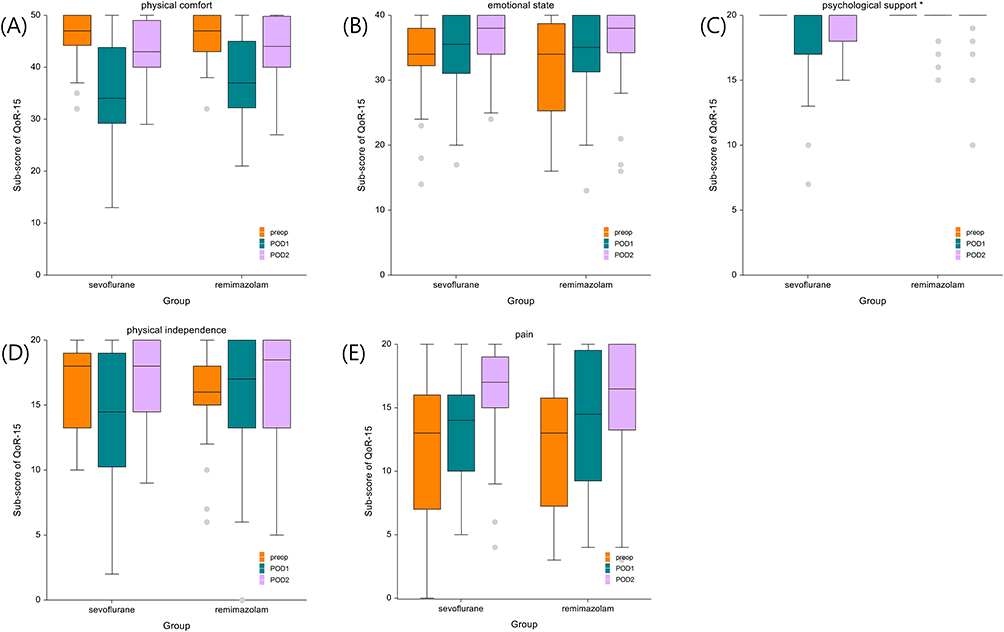 |
Figure 3 Sub-scores of the five dimensions of the QoR-15. Boxplots display the median, as well as the 25% and 75% interquartile range. (A) Physical comfort, (B) emotional state, (C) psychological support, (D) physical Independence, and (E) pain. Asterisk represents a significant interaction between the group and time is shown in the psychological aspect. Abbreviations: POD, postoperative day; preop, preoperative; QoR, quality of recovery. |
The intraoperative parameters are listed in Table 2. The time to loss of consciousness and decrease in the PSI score <50 points were significantly lower in group S than in group R (52.3 vs 90.6 s, 97.5 vs 170.0 s, P<0.001 for each). While total remifentanil consumption was higher (774.5 [212.9] µg vs 1569.5 [760.6] µg, P<0.001), total consumption of phenylephrine, a vasoactive agent, was significantly lower (1580 [940, 2890] µg vs 60 [0, 335] µg, P<0.001) in group R than in group S. Perioperative hemodynamic status and intraoperative PSI values are described in Supplementary Figure 3. In terms of both HR and blood pressure, group R showed significantly less changeability over time than group S (P=0.002 and P<0.001, respectively). In addition, the PSI values were significantly higher in group R than in group S immediately after endotracheal intubation and surgical incision, at 1 h after surgery, and immediately after extubation (P<0.001).
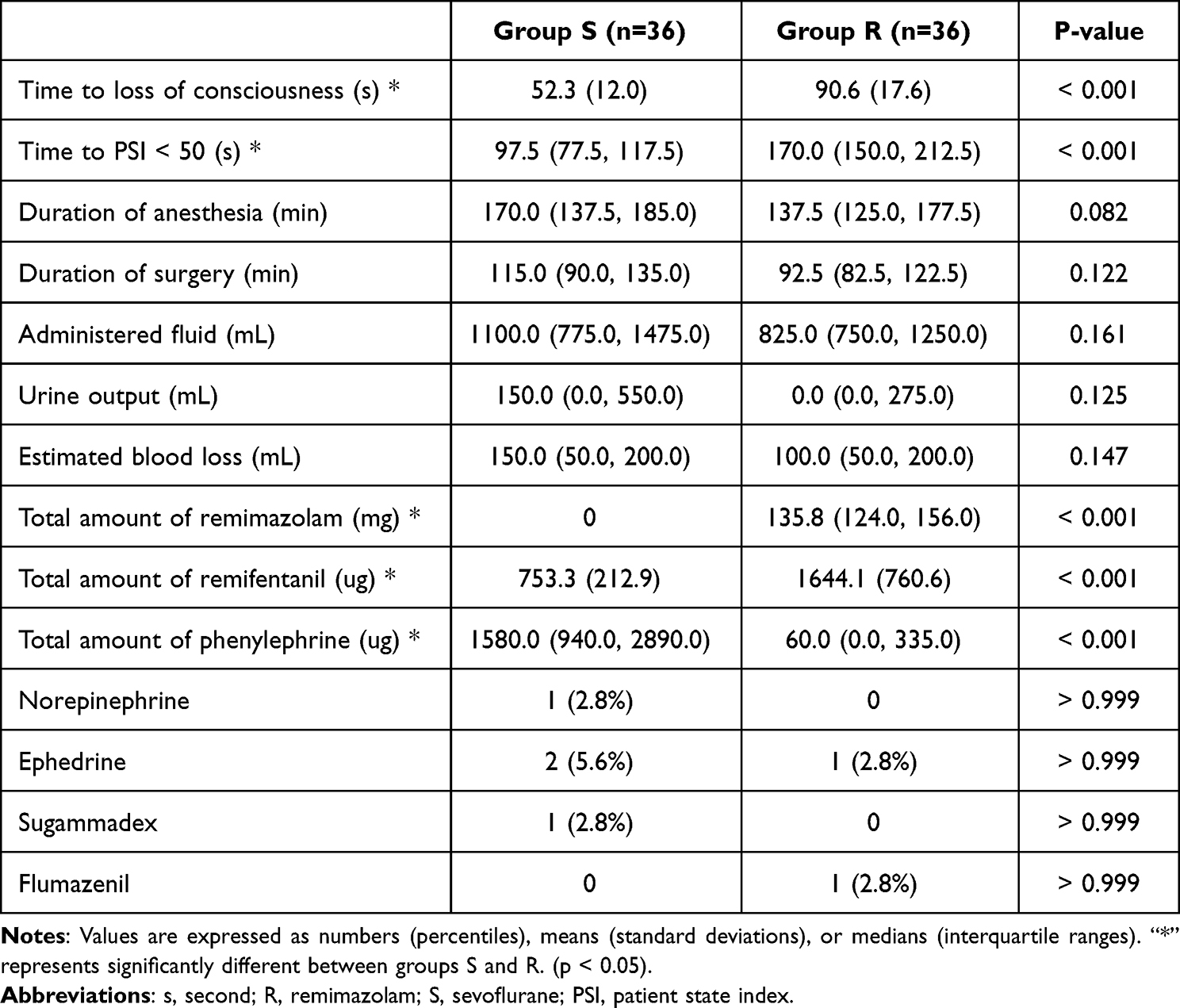 |
Table 2 Parameters Related to Anesthesia and Surgery |
Table 3 presents the postoperative recovery profiles. The time to reach a PSI score of >50 points was not significantly different between two groups (275 vs 290 s, P=0.964). Four patients (three with tachycardia and one with hypertension) experienced adverse events related to extubation in group S, whereas one had hypertension in group R. The incidence of adverse events related to extubation did not significantly differ between the groups. In the ward, patients in group R requested significantly more rescue analgesics, including their morphine equivalent doses, than those in group S within postoperative 6 h. In contrast, the NRS score indicating the degree of PONV within 6 and 24 h after surgery was statistically significantly higher in patients in group S. Four patients (voiding difficulties, n=2; QT prolongation, n=1; unilateral ptosis, n=1) in group S and two (voiding difficulties) in group R experienced postoperative adverse events. However, there were no residual complications until hospital discharge, as well as no significant differences in postoperative adverse events and length of hospital stay, between the two groups.
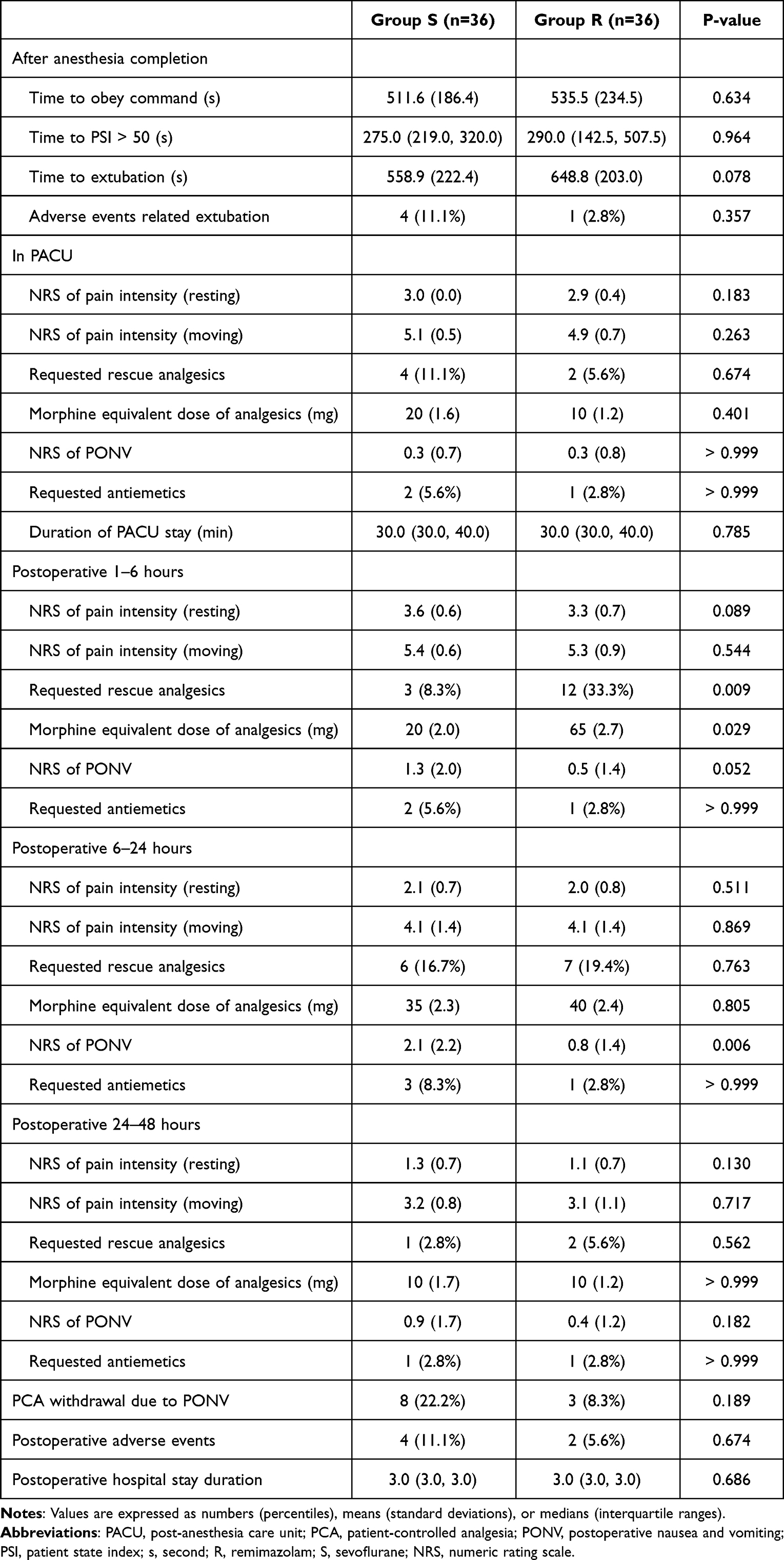 |
Table 3 Postoperative Recovery Profiles |
Discussion
In this study, we compared overall functional recovery between balanced inhalational anesthesia using sevoflurane and TIVA using remimazolam in patients undergoing ACDF. To the best of our knowledge, there are currently no studies on the QoR of patients after intermediate or major surgery with remimazolam vs sevoflurane use for general anesthesia. Herein, we compared the postoperative QoR-15 scores between remimazolam-based TIVA and balanced inhalational anesthesia with sevoflurane in patients undergoing ACDF belonging to the intermediate surgery group. Although the total QoR-15 score of group R was 120.2 points and that of group S was 114.3 points on POD 1, there was no statistical difference between the groups and no significant group-time interaction effect. However, in patients who received remimazolam, the sub-scores of the QoR-15 were significantly superior in the dimensions of psychological support as well as in those of nausea and vomiting than those in patients who received sevoflurane.
According to previous studies related to QoR after remimazolam use in general anesthesia, TIVA with remimazolam provided better postoperative global QoR-40 scores in laparoscopic cholecystectomy and robotic gynecological minor surgeries than inhalational anesthesia using desflurane.17 Compared with propofol-based TIVA, remimazolam-based TIVA in thyroidectomy showed comparable postoperative global QoR-15 scores and more stable hemodynamic changes.18 Conversely, another study showed that the postoperative total QoR-15 scores were significantly lower in remimazolam-based than in propofol-based TIVA in urologic minor surgery.19 The divergence in outcomes between this study and others, where remimazolam showcased superiority over inhalation concerning QoR, may due to the extent of surgery and operative time. Stark et al described the clear differentiation between patient groups using the QoR-15, noting significantly reduced scores in the cohort undergoing more extensive surgery.20 Given that ACDF in our study represents an intermediate risk surgery, the observed decrease in QoR compared to minor surgeries in other studies might account for the variance in statistical outcomes.
The QoR-15 is a validated multidimensional patient-reported outcome measurement-based questionnaire that is used to measure postoperative QoR.20–22 The QoR-15 has fine internal consistency, as well as split–half and test–retest reliability. This scale for postoperative recovery status can provide us with reproducible results. The ability to detect and measure clinically significant changes is a key feature of any tool for health conditions used to predict patient prognosis. The QoR-15 has also been validated in a variety of linguistic and cultural contexts, including Korean-speaking patients.12 The acceptable symptom status describes the minimum absolute score on the health scale that the patient perceives to be indicative of good health or good condition.18,23 A QoR-15 score of ≥118 points can be considered to indicate good recovery after surgery.22 Moreover, the large clinical studies identified in a previous review found that patients with and without serious complications had mean QoR-15 scores of 101 and 113 points, respectively.22 In the present study, the mean total QoR-15 score on POD1 of group R was 120.2, which was >118, indicating good recovery after surgery even though the difference between the two groups was not statistically significant. Myles et al24 suggested that variations exceeding 6 points in the QoR-15 scale, as seen in the present study, could be considered minimal clinically important differences (MCIDs).
Among the five dimensions of the QoR, group R had significantly superior scores compared with group S in the psychological support dimension. Remimazolam acts on GABAA receptors and shows pharmacological effects similar to those of midazolam.1,25,26 It produces the antegrade amnesia effect that benzodiazepines usually produce.27 Lack of awareness in recognizing the trauma or pain caused by surgery owing to antegrade amnesia may indicate a psychological prevention effect. In addition, the use of benzodiazepines as anxiolytic agents for premedication also seems to support the findings of this study showing stable psychological results after surgery in group R. The score for nausea and vomiting was significantly better in group R than in group S. Moreover, the NRS score of PONV severity measured in the ward within 6 and 24 h after surgery was also statistically significantly lower in patients in group R, which is in line with the results of previous studies showing that PONV reduction is significantly greater in propofol-based TIVA than in inhalation anesthesia.28,29 This is because benzodiazepine-like drugs have antiemetic properties and inhalational anesthetics stimulate the vagal nerve and affect the vestibular system, thus causing nausea.25,30 Another specific finding is that although postoperative 1–6 h rescue analgesia was higher in group R, there was no difference in the QoR-15 pain score on POD 1. This can be attributed to the fact that the remifentanil use during surgery was significantly higher in group R, and the resulting pain due to opioid-induced hyperalgesia appeared immediate after surgery and disappeared the next day, as in the study by Hood et al.31
As revealed in previous studies, remimazolam has a notable advantage in maintaining hemodynamic stability during surgery.2 In various types of surgeries, intraoperative vasopressor requirements were significantly low with remimazolam.16,18,30,32 Similarly, the phenylephrine consumption in group R was significantly lower than that in group S. Urabe et al published a study showing that remimazolam increased the intracellular calcium level in a dose-dependent manner above a certain concentration.33 They explained that the increase in intracellular calcium level was caused by the action of remimazolam on the G-protein coupled receptor–inositol 1,4,5-triphosphate pathway.
This study has some limitations. First, the sample size was relatively small, and it might be difficult to generalize our results, especially for sub-score comparisons. Most values of MCIDs described in several studies were below 13 points of the total QoR-15 score.18,19 However, a 13-point difference in the total QoR-15 score in our study could indicate clinical improvement in functional recovery and not just MCID.16 In addition, our study population was controlled with minimal bias, including the type of surgery and surgeon. Second, as the timing and conditions for the approval of new drugs differ across countries, remimazolam has not been approved for general anesthesia in some cases. Additionally, depending on the scope of insurance coverage and permission in the country of use, remimazolam may be more expensive than inhalation agents.
Conclusion
In conclusion, we examined the difference in the QoR between conventional balanced inhalational anesthesia using sevoflurane and remimazolam-based TIVA in the present study. Remimazolam did not show statistical superiority in total postoperative QoR-15 scores but did demonstrate a good recovery score of >118 points on POD1 compared with sevoflurane. In addition, patients in group R also had better results with regard to the degree of PONV and psychological support than those in group S. Further studies with a larger sample size and a wider variety of surgeries are required to establish whether remimazolam can improve postoperative functional recovery as the main anesthetic for general anesthesia.
Abbreviations
ACDF, anterior cervical discectomy and fusion; BMI, body mass index; GABAA, gamma-aminobutyric acid type A; HR, heart rate; MAP, mean arterial pressure; MCID, minimal clinically important difference; NMB, neuromuscular blockade; NRS, numeric rating scale; PONV, postoperative nausea and vomiting; PACU, post-anesthetic care unit; PCA, Patient-controlled analgesia; POD, postoperative day; PSI, patient state index; QoR, Quality of Recovery; SD, standard deviation; TCI, target-controlled infusion; TIVA, total intravenous anesthesia; TOF, train‐of‐four.
Ethics Approval and Informed Consent
This prospective double-blind randomized controlled trial was conducted at a tertiary hospital in accordance with the Declaration of Helsinki 2013. The protocol was approved by the Institutional Review Board (IRB) of Gangnam Severance Hospital (IRB No. 3-2021-0257), Yonsei University Health System (Seoul, Republic of Korea), and registered before patient enrolment at clinicaltrials.gov (Trial Registration Number: NCT05019222).
Data availability
The datasets used or analyzed during the current study are available from the corresponding author upon reasonable request.
Acknowledgments
We thank the Biostatistics Collaboration Unit and Electronic Medical Record Team at Severance Hospital Yonsei University College of Medicine for their contribution to this study.
Funding
This research received no financial support.
Disclosure
The authors declare that they have no conflict of interest.
References
1. Kim S-H, Fechner J. Remimazolam – current knowledge on a new intravenous benzodiazepine anesthetic agent. Korean Journal of Anesthesiology. 2022;75(4):307–315. doi:10.4097/kja.22297
2. Kim KM. Remimazolam: pharmacological characteristics and clinical applications in anesthesiology. Anesth Pain Med. 2022;17(1):1–11. doi:10.17085/apm.21115
3. Cardia L. Remimazolam: an ultrashort-acting intravenous anesthetic suitable for general anesthesia. Minerva Anestesiol. 2021;87(10):1059–1063. doi:10.23736/s0375-9393.21.16006-7
4. Sneyd JR, Rigby-Jones AE. Remimazolam for anaesthesia or sedation. Curr Opin Anaesthesiol. 2020;33(4):506–511. doi:10.1097/aco.0000000000000877
5. Schüttler J, Eisenried A, Lerch M, Fechner J, Jeleazcov C, Ihmsen H. Pharmacokinetics and Pharmacodynamics of Remimazolam (CNS 7056) after Continuous Infusion in Healthy Male Volunteers: part I. Pharmacokinetics Clin Pharmacodynamics Anesthesiol. 2020;132(4):636–651. doi:10.1097/aln.0000000000003103
6. Masui K. Remimazolam besilate, a benzodiazepine, has been approved for general anesthesia!! J Anesth. 2020;34(4):479–482. doi:10.1007/s00540-020-02755-1
7. Keam SJ. Remimazolam: first Approval. Drugs. 2020;80(6):625–633. doi:10.1007/s40265-020-01299-8
8. Eisenried A, Schuttler J, Lerch M, Ihmsen H, Jeleazcov C. Pharmacokinetics and Pharmacodynamics of Remimazolam (CNS 7056) after Continuous Infusion in Healthy Male Volunteers: part II. Pharmacodynamics of Electroencephalogram Effects. Anesthesiology. 2020;132(4):652–666. doi:10.1097/ALN.0000000000003102
9. Poitras S, Beaule PE, Dervin GF. Validity of a short-term quality of life questionnaire in patients undergoing joint replacement: the Quality of Recovery-40. J Arthroplasty. 2012;27(9):1604–1608 e1. doi:10.1016/j.arth.2012.03.015
10. Murphy GS, Szokol JW, Greenberg SB, et al. Preoperative dexamethasone enhances quality of recovery after laparoscopic cholecystectomy: effect on in-hospital and postdischarge recovery outcomes. Anesthesiology. 2011;114(4):882–890. doi:10.1097/ALN.0b013e3181ec642e
11. Kluivers KB, Riphagen I, Vierhout ME, Brolmann HA, de Vet HC. Systematic review on recovery specific quality-of-life instruments. Surgery. 2008;143(2):206–215. doi:10.1016/j.surg.2007.08.017
12. Lee JH, Ki M, Choi S, et al. Validity and reliability of the Korean version of the Quality of Recovery-15 questionnaire. Korean J Anesthesiol Apr. 2021;74(2):142–149. doi:10.4097/kja.20435
13. Yoon S, Joo H, Oh YM, Lee J, Bahk JH, Lee HJ. Validation and clinical utility of the Korean version of the Quality of Recovery-15 with enhanced recovery after surgery: a prospective observational cohort study. Br J Anaesth. 2020;125(4):614–621. doi:10.1016/j.bja.2020.06.040
14. Kim SH, Ju HM, Choi CH, Park HR, Shin S. Inhalational versus intravenous maintenance of anesthesia for quality of recovery in patients undergoing corrective lower limb osteotomy: a randomized controlled trial. PLoS One. 2021;16(2):e0247089. doi:10.1371/journal.pone.0247089
15. Lee WK, Kim MS, Kang SW, Kim S, Lee JR. Type of anaesthesia and patient quality of recovery: a randomized trial comparing propofol-remifentanil total i.v. anaesthesia with desflurane anaesthesia. Br J Anaesth Apr. 2015;114(4):663–668. doi:10.1093/bja/aeu405
16. Myles PS, Myles DB, Galagher W, Chew C, MacDonald N, Dennis A. Minimal Clinically Important Difference for Three Quality of Recovery Scales. Anesthesiology. 2016;125(1):39–45. doi:10.1097/ALN.0000000000001158
17. Song SW, Jang YN, Yoon MW, Jeon YG. Quality of recovery in patients administered remimazolam versus those administered an inhalant agent for the maintenance of general anesthesia: a randomized control trial. BMC Anesthesiol. 2022;22(1):226. doi:10.1186/s12871-022-01770-x
18. Choi JY, Lee HS, Kim JY, et al. Comparison of remimazolam-based and propofol-based total intravenous anesthesia on postoperative quality of recovery: a randomized non-inferiority trial. J Clin Anesth. 2022;82:110955. doi:10.1016/j.jclinane.2022.110955
19. Mao Y, Guo J, Yuan J, Zhao E, Yang J. Quality of Recovery After General Anesthesia with Remimazolam in Patients’ Undergoing Urologic Surgery: a Randomized Controlled Trial Comparing Remimazolam with Propofol. Drug Des Devel Ther. 2022;16:1199–1209. doi:10.2147/dddt.S359496
20. Stark PA, Myles PS, Burke JA. Development and psychometric evaluation of a postoperative quality of recovery score: the QoR-15. Anesthesiology. 2013;118(6):1332–1340. doi:10.1097/ALN.0b013e318289b84b
21. Myles PS. Measuring quality of recovery in perioperative clinical trials. Curr Opin Anaesthesiol. 2018;31(4):396–401. doi:10.1097/ACO.0000000000000612
22. Kleif J, Waage J, Christensen KB, Gogenur I. Systematic review of the QoR-15 score, a patient- reported outcome measure measuring quality of recovery after surgery and anaesthesia. Br J Anaesth. 2018;120(1):28–36. doi:10.1016/j.bja.2017.11.013
23. Lee JH, Kim D, Seo D, Son JS, Kim DC. Validity and reliability of the Korean version of the Quality of Recovery-40 questionnaire. Korean J Anesthesiol. 2018;71(6):467–475. doi:10.4097/kja.d.18.27188
24. Myles PS, Myles DB. An Updated Minimal Clinically Important Difference for the QoR-15 Scale. Anesthesiology. 2021;135(5):934–935. doi:10.1097/ALN.0000000000003977
25. Noor N, Legendre R, Cloutet A, Chitneni A, Varrassi G, Kaye AD. A comprehensive review of remimazolam for sedation. Health Psychol Res. 2021;9(1):24514. doi:10.52965/001c.24514
26. Kilpatrick GJ. Remimazolam: non-Clinical and Clinical Profile of a New Sedative/Anesthetic Agent. Front Pharmacol. 2021;12:690875. doi:10.3389/fphar.2021.690875
27. Wittenborn JR. Effects of benzodiazepines on psychomotor performance. Br J Clin Pharmacol. 1979;7 Suppl 1(Suppl 1):61S–67S. doi:10.1111/j.1365-2125.1979.tb04667.x
28. Yang L, Xu YJ, Shen J, Lou FF, Zhang J, Wu J. Propofol-based total intravenous anesthesia decreases the incidence of postoperative nausea and vomiting without affecting flap survival in free flap breast reconstruction. Gland Surg. 2020;9(5):1406–1414. doi:10.21037/gs-20-225
29. Yoo YC, Bai SJ, Lee KY, Shin S, Choi EK, Lee JW. Total intravenous anesthesia with propofol reduces postoperative nausea and vomiting in patients undergoing robot-assisted laparoscopic radical prostatectomy: a prospective randomized trial. Yonsei Med J. 2012;53(6):1197–1202. doi:10.3349/ymj.2012.53.6.1197
30. Lee B, Kim MH, Kong HJ, et al. Effects of Remimazolam vs. Sevoflurane Anesthesia on Intraoperative Hemodynamics in Patients with Gastric Cancer Undergoing Robotic Gastrectomy: a Propensity Score-Matched Analysis. J Clin Med. 2022;11(9). doi:10.3390/jcm11092643
31. Hood DD, Curry R, Eisenach JC. Intravenous remifentanil produces withdrawal hyperalgesia in volunteers with capsaicin-induced hyperalgesia. Anesth Analg. 2003;97(3):810–815. doi:10.1213/01.ANE.0000078811.80093.88
32. Qiu Y, Gu W, Zhao M, Zhang Y, Wu J. The hemodynamic stability of remimazolam compared with propofol in patients undergoing endoscopic submucosal dissection: a randomized trial. Front Med Lausanne. 2022;9:938940. doi:10.3389/fmed.2022.938940
33. Urabe T, Miyoshi H, Narasaki S, et al. Characterization of intracellular calcium mobilization induced by remimazolam, a newly approved intravenous anesthetic. PLoS One. 2022;17(2):e0263395. doi:10.1371/journal.pone.0263395
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.