Back to Journals » Drug Design, Development and Therapy » Volume 18
Comparison of Remimazolam and Propofol in Recovery of Elderly Outpatients Undergoing Gastrointestinal Endoscopy: A Randomized, Non-Inferiority Trial
Authors Lu L, Chen B ![]() , Zhao X, Zhai J, Zhang P, Hua Z
, Zhao X, Zhai J, Zhang P, Hua Z
Received 20 June 2024
Accepted for publication 11 September 2024
Published 28 September 2024 Volume 2024:18 Pages 4307—4318
DOI https://doi.org/10.2147/DDDT.S474275
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Anastasios Lymperopoulos
Lin Lu,1,* Bing Chen,1,* Xueli Zhao,1 Jie Zhai,1 Pan Zhang,2 Zhen Hua1
1Department of Anesthesiology, Beijing Hospital, National Center of Gerontology, Institute of Geriatric Medicine, Chinese Academy of Medical Sciences, Beijing, People’s Republic of China; 2Department of Gastroenterology, Beijing Hospital, National Center of Gerontology, Institute of Geriatric Medicine, Chinese Academy of Medical Sciences, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Bing Chen, Department of Anesthesiology, Beijing Hospital, National Center of Gerontology, Institute of Geriatric Medicine, Chinese Academy of Medical Sciences, No. 1 Dahua Road, DongDan, Beijing, 100730, People’s Republic of China, Tel +8613811295927, Email [email protected]
Purpose: We designed this trial to compare the recovery time of remimazolam and propofol in elderly patients undergoing painless gastrointestinal endoscopy.
Patients and Methods: In this randomized, non-Inferiority trial, 360 patients aged 65 years or older, scheduled for elective outpatient gastrointestinal endoscopy, were randomly assigned to the remimazolam combined with fentanyl (RF) group or the propofol combined with fentanyl (PF) group. The primary outcome was the post-anesthesia care unit (PACU) stay time, defined as the time from the end of the examination to scoring 9 points using the Modified Post-Anesthetic Discharge Scoring System (MPADSS) criteria. Secondary outcomes included sedation-related adverse events, recall, injection pain, as well as postoperative Quality of Recovery-15 (QoR-15) scores and Pittsburgh Sleep Quality Index (PSQI) scores at 1 day, 1 week, and 1 month postoperatively.
Results: A total of 351 patients completed the study, with 174 receiving remimazolam and 177 receiving propofol. The PACU stay time in RF group was non-inferior to that in PF group [14 (11, 18) vs 13 (10, 17), mean difference 1 (95% confidence interval 0, 2), P=0.084 for noninferiority]. However, remimazolam was associated with lower rate of hypoxemia [4.7% (8/180) vs 12.4% (22/180), P=0.011], reduced use of vasoactive drugs [1 (0, 1) vs 1 (1, 2), P< 0.001], less injection pain [2 (1.2%) vs 35 (21.3%), P< 0.001], and lower recall [20 (11.8%) vs 36 (20.3%), P=0.034]. There were no differences in the QoR-15 scores and PSQI scores at postoperative 1 day, 1 week, and 1 month between groups.
Conclusion: This non-inferiority study revealed that in elderly outpatients undergoing gastrointestinal endoscopy, remimazolam achieved recovery times comparable to propofol, with fewer associated complications.
Keywords: remimazolam, postoperative recovery, older patients, gastrointestinal endoscopy
Introduction
As life expectancy continues to rise globally, the incidence of gastrointestinal diseases is concurrently increasing due to the aging demographic. Endoscopy serves as a prevalent diagnostic and therapeutic tool for gastrointestinal disorders and is commonly performed with sedation.1 The elderly population faces an elevated risk of adverse events, including hypoxemia, hypotension, arrhythmias, and esophageal reflux, during these procedures.2,3 Advanced age (70–99 years) is also considered to increase the risk of cardio-cerebrovascular adverse events during gastrointestinal endoscopy.4 Clinicians should exercise heightened caution and diligence in administering medications to elderly patients.5
Propofol is presently acknowledged as the “gold standard” for short-term sedation requirements during gastrointestinal endoscopy.6 While numerous studies underscore the overall superiority of propofol over other analgesics/sedatives utilized, propofol still presents certain drawbacks. These include dose-dependent cardiovascular and respiratory depression, particularly in frail and elderly patients, as well as pain at the administration site and the potential risk of infection due to the lipid formulation of the drug.7 Remimazolam Besylate (remimazolam) is a novel benzodiazepine-class drug, characterized by its ultra-short duration of action. It has obtained approval for induction and maintenance of general anesthesia, as well as procedural sedation.8 Current research has demonstrated the safe and effective application of remimazolam in patients aged 65–75 undergoing colonoscopy.9 In comparison to propofol, remimazolam exhibits a lower incidence of sedation-related adverse reactions, particularly in terms of hemodynamic events and respiratory depression.10 Notably, it can be safely and effectively employed for sedation management in outpatient colonoscopy patients classified as American Society of Anesthesiologists (ASA) III/IV.11 However, the assessment of whether remimazolam could emerge as a more favorable sedative for gastrointestinal endoscopy than propofol requires further evaluation beyond safety and efficacy. Consideration should also be given to patient outcomes, patient safety, quality of patient experience, or health economics.12
A nationwide survey in China revealed that there were 10 million cases of gastroscopy in 2016. With the anticipated growth in aging population, it is projected that this figure will reach 35 million by 2030.13 Achieving higher quality and faster recovery can effectively reduce the manpower and resources required in endoscopy centers with significant outpatient volumes. Therefore, it is imperative to enhance the quality and efficiency of sedation while ensuring safety. Currently, research has found comparable recovery times between the two drugs during endoscopic examinations,14 but there is a lack of evidence specific to elderly patients. Additionally, remimazolam demonstrates significant advantages in alleviating respiratory and circulatory depression, stress responses, and cognitive dysfunction due to its pharmacological characteristics.15–17 These advantages position it favorably for anesthesia in elderly patients. Therefore, we designed this randomized controlled non-inferiority study to compare the effects of remimazolam and propofol sedation on recovery time in elderly patients undergoing gastrointestinal endoscopy. We hypothesize that the recovery time with remimazolam sedation is not inferior to that with propofol sedation.
Materials and Methods
Study Population and Design
A single-center, prospective, randomized, non-inferiority, partly blinded study was conducted with 360 consecutive patients referred for gastrointestinal endoscopy from February 2023 to August 2023. The study was approved by the Institutional Ethics Committee of Beijing Hospital (2022BJYYEC-416-02) and registered in the Chinese Clinical Trial Registry (www.chictr.org.cn; ChiCTR2300071635; Date of registration: 19/5/2023). The entire study adhered strictly to the principles outlined in the Helsinki Declaration. All eligible patients provided written informed consent.
The inclusion criteria were as follows: (1) patients aged ≥65 years, (2) ASA I–II patients, (3) Body mass index (BMI) 18.0~30.0 kg/m2, (4) scheduled to undergo a gastrointestinal endoscopy under sedation. The exclusion criteria were: (1) patients allergic to the anesthetic drugs or with a history of anesthesia-related complications, (2) patients with alcohol abuse (defined as an average daily consumption of more than 2 units of alcohol, where 1 unit equals 360 mL of beer, 45 mL of 40% liquor, or 150 mL of wine), drug abuse, long-term use of psychotropic drugs, (3) history of cognitive impairment or psychiatric illness prior to examination (including Anxiety Self-rating Scale scores > 50, schizophrenia, mania, bipolar disorder, mental disorders, etc), (4) patients with an upper respiratory tract infection within 2 weeks before examination, challenging airway conditions or severe respiratory diseases (such as obstructive sleep apnea syndrome, inability to open the mouth wider than 3 cm, restricted neck or jaw movement, severe obesity, acute exacerbation of chronic obstructive pulmonary disease, and uncontrolled asthma), (5) Severe cardiovascular conditions (such as acute heart failure, unstable angina pectoris, recent myocardial infarction within the last 6 months, resting electrocardiogram (ECG) heart rate below 50 beats per minute, third-degree atrioventricular block, severe arrhythmias, moderate to severe heart valve diseases, QTc interval ≥ 450 ms for males, ≥ 470 ms for females), (6) complex endoscopic procedures (such as endoscopic ultrasonography, endoscopic mucosal resection, endoscopic submucosal dissection, transoral endoscopic myotomy, etc)., (7) participation in other studies within the previous 30 days or unwillingness/inability to cooperate.
Randomization and Blinding
All enrolled patients were randomly assigned in a 1:1 ratio to either remimazolam combined with fentanyl (RF) group or propofol combined with fentanyl (PF) group using a simple random number sequence generated by Microsoft Excel. The randomization process was conducted by individuals not involved in this study, and the group assignments were securely sealed in opaque envelopes. This envelope was then delivered to the anesthesiologist responsible for sedation just before the examination. The sedative drugs were placed in opaque syringes, thus concealing the randomization from the patients, the anesthesia nurses responsible for data recording, and the endoscopists, but not from the anesthesiologists.
Study Procedures and Drug Administration
Prior to the examination, all patients fasted for eight hours for food and two hours for water. Standard anesthesia monitoring, including a five-lead electrocardiogram, blood pressure cuff, pulse oximetry and end-expiratory carbon dioxide, was administered to all participants. Supplemental oxygen (4 L/min) was provided to patients via a standard face mask throughout the procedure. Additionally, a peripheral intravenous line was established before entering the examination room.
After anesthesia induction, all patients were initially administered a single dose of 1 µg/kg fentanyl. Subsequently, based on their assigned groups, patients received intravenous injections of either 0.15 mg/kg remimazolam or 1 mg/kg propofol. The injection duration for both remimazolam and propofol was longer than 1 minute, and modified Observer’s Assessment of Alertness/Sedation (MOAA/S) scores18 were assessed every 30 seconds. If the score was ≤1, endoscopy could proceed. If the score was >1, an additional 0.05 mg/kg of remimazolam or 0.5 mg/kg of propofol was administered 2 minutes after the last injection. The injection time for each additional dose was 10 seconds. If the number of additional doses administered within any 15-minute period was five or more, the researcher decided on sedation rescue measures based on clinical experience. The targeted depth of sedation level during painless gastrointestinal endoscopy was MOAA/S≤1. MOAA/S was shown in Appendix 1. All endoscopies were performed by experienced gastroenterologists.
After examination, all patients were transferred to PACU. If the Modified Post-Anesthetic Discharge Scoring System (MPADSS)19 reached 9 points or higher, patients were eligible for discharge. If not reach 9 points 1h after examination, patients should be transferred to the emergency observation room for observation and treatment. The MPADSS criteria shown in Appendix 2.
Outcome Measurements and Definitions
The primary outcome assessed was the PACU stay time, defined as the time from the end of the examination to scoring 9 points using the MPADSS criteria (assessments were performed every 2 min in PACU).
The secondary outcomes included (1) sedation success rate (defined as achieving the target sedation depth, completing the endoscopic examination, and not exceeding five additional doses of medication within any 15-minute period, without the use of rescue medications). (2) sedation-associated adverse events during procedure, including severe adverse events (need for intensive-care unit admission, intubation, resuscitation and/or death) and minor adverse events (respiratory depression or hemodynamic fluctuations which could be corrected rapidly).20 Respiratory depression was categorized into hypoxemia (85% < SpO2 < 90%), which could be corrected by mask oxygen inhalation and jaw thrusting, and severe hypoxemia (SpO2 ≤ 85%), which could be corrected by assisted ventilation. Hypotension was defined as a reduction in mean arterial pressure of at least 20% from baseline. Bradycardia was characterized by a heart rate of less than 50 beats per minute, while tachycardia was characterized by a heart rate of more than 100 beats per minute. (3) Outcome measures during the examination included mean blood pressure, heart rate, blood oxygen saturation (SpO2), respiratory rate, and bispectral index (BIS). Body movements during the procedure were also assessed, categorized as follows: 0 - no movement; 1 - minor movements of hands or feet that do not interfere with the examination; 2 - significant movements of legs or hips that disrupt the examination. Additionally, injection pain was recorded. (4) The satisfaction levels of both the endoscopist and the patient were measured using an 11-point numerical rating scale (NRS), where 0 indicated complete dissatisfaction and 10 indicated complete satisfaction. (5) Incidence of recall. (6) QoR-15 scores21 and PSQI scores22 for patients at 1 day, 1 week, and 1 month after the examination.
Patients will be withdrawn from the study under the following circumstances: occurrence of severe sedation-related complications (transfer to ICU, intubation, cardiopulmonary resuscitation, and/or death); withdrawal deemed necessary by the investigator for participant safety reasons (severe arrhythmias, suspected cerebrovascular accidents); changes in endoscopic examination procedure (eg, termination due to inadequate bowel preparation, cessation of sedation due to difficult insertion requiring patient cooperation, major bleeding, or perforation requiring surgical intervention); participant withdrawal of informed consent for any reason.
Sample Size Estimation
In this trial, propofol was used as the active control, and a non-inferiority test was conducted for the primary outcome (PACU stay time) between the two groups. Based on the preliminary results from our center, the average discharge time in the propofol group was 18.85±9.56 minutes. A prospective randomized non-inferiority study comparing post-procedural discharge times for non-elderly patients undergoing colonoscopy indicated an average recovery time of 21 minutes for the remimazolam group, which was 2 minutes shorter than the propofol group.14 Based on conclusions from our anesthesia and endoscopy expert panel not involved in this study, we considered a minimum clinically relevant significant difference in recovery time to be 5 minutes and set it as our non-inferiority margin. With a one-sided α of 0.025, assuming a β of 0.2, a 1:1 ratio, a non-inferiority margin of 5 minutes, an inter-group difference of 2 minutes, and a standard deviation of 9.56 minutes, the calculated sample size for each group was 161 using PASS (version 15.0.5, Kaysville, Utah, USA, Non-Inferiority Tests for the Difference Between Two Means). Considering a 10% dropout rate, the sample size for each group was increased to 180 individuals, resulting in a total sample size of 360 individuals.
Statistical Analysis
Statistical analysis for both primary and secondary outcomes adhered to the modified intention-to-treat (m-ITT) principle. Baseline characteristics and intraoperative data were summarized using descriptive analysis. Distribution of continuous variables was examined using the Kolmogorov–Smirnov method. Categorical variables were presented as numbers (proportion), while continuous variables were reported as mean±SD and median (q1, q3) to accommodate normal and non-normal distributions, respectively.
As for the primary outcome, non-inferiority was evaluated by examining the upper bound of the 95% confidence interval (CI) of the median difference, employing the Hodges-Lehmann method. Non-inferiority was established if the upper bound was smaller than the predefined margin of 5. A one-sided non-inferiority p<0.025 (Wilcoxon rank sum test) was considered statistically significant for the primary outcome (SAS 9.4, Institute Incv Cary, NC, USA).
The strategy for analyzing secondary outcomes was as follows: Continuous data underwent the Student’s t-test when normally distributed, or the Mann–Whitney U-test when non-normally distributed. Categorical data were analyzed using a χ2 test or Fisher’s exact test. For repeated measurement data, including QoR-15 scores, PSQI scores, and hemodynamic variables, a generalized linear mixed model was employed to analyze interactions between different groups, different time periods, and the interaction of group and time. All tests were two-tailed, and statistical significance was defined as a P-value <0.05. SPSS Statistics [version 29.0.1.0 (171), IBM Corp., Armonk, New York, USA] was employed for all analyses.
Results
From February 2023 to August 2023, 360 patients scheduled for outpatient gastrointestinal endoscopy were included, 174 in RF group and 177 in PF group received sedation according to the study protocol. Thirteen patients in RF group and three patients in PF group did not complete sedation and withdrew. The reasons included changes in the examination procedure, patient safety considerations (such as pre-procedure hypertension, full stomach, and supraventricular tachycardia following medication administration), sedation administered by other anesthetists, patient withdrawal and sedation failure. A flowchart summarizing the patients enrolled in the study is shown in Figure 1.
 |
Figure 1 CONSORT diagram of patient flow through the study. CONSORT indicates Consolidated Standards of Reporting Trials. Abbreviations: RF, remimazolam combined with fentanyl; PF, propofol combined with fentanyl. Notes: Pos1d: one day after the examination, Pos1w: one week after the examination, Pos1m: one month after the examination. |
Table 1 offers an overview of the baseline characteristics of the enrolled participants. Generally, there was a balanced distribution of patient and clinical data across both groups. The sedation success rates were 163 (95.9%) in RF group and 174 (98.3%) in PF group, with a P-value of 0.212. In RF group, the remimazolam dosage was 16 (14, 18) mg, and the fentanyl dosage was 65 (60, 70) ug. In PF group, the propofol dosage was 145 (120, 175) mg, and the fentanyl dosage was 55 (65, 75) μg.
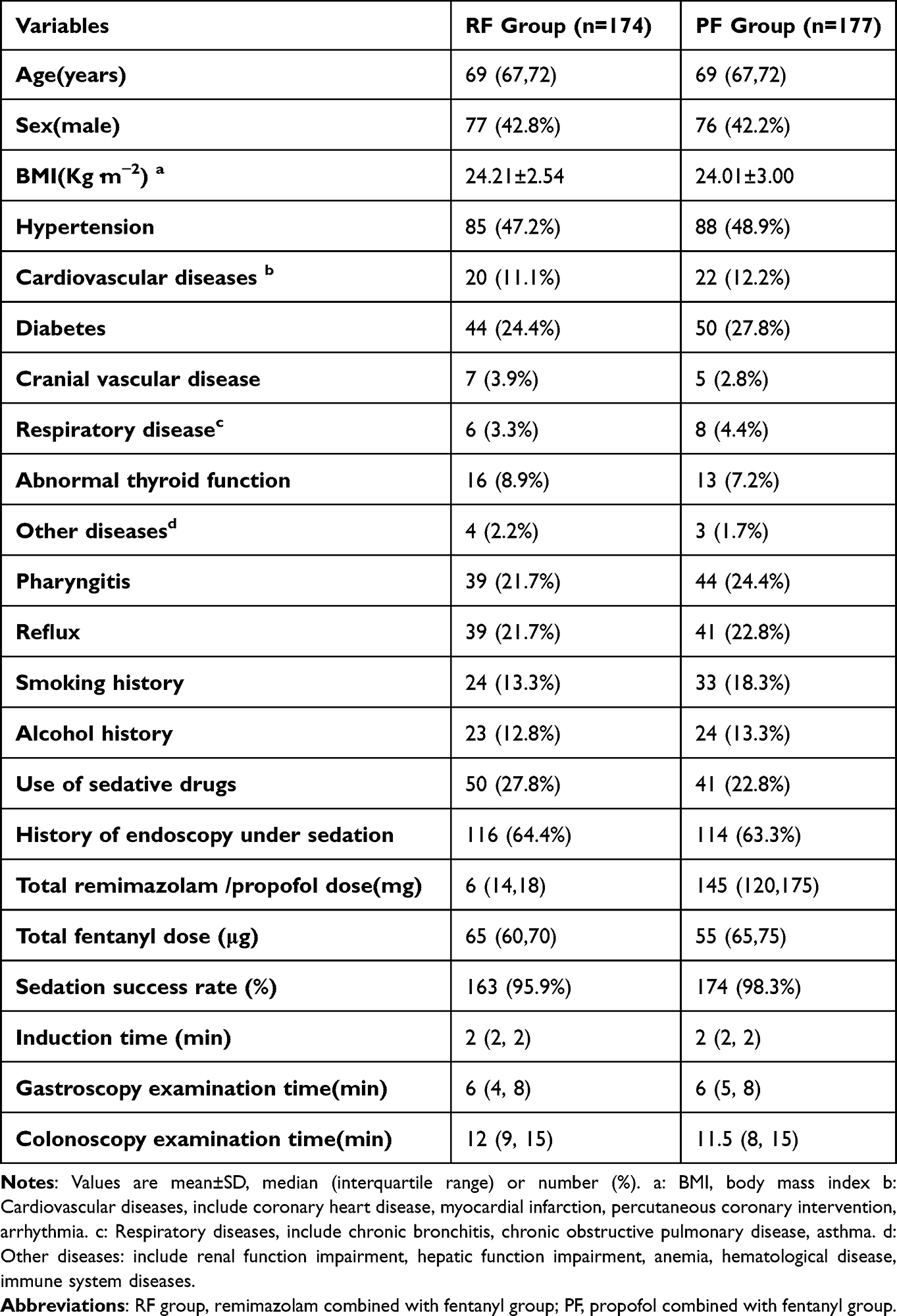 |
Table 1 Basic Characteristics |
Primary Outcome
The primary outcome, PACU stay time, was 14 (11, 18) minutes in RF group, which was longer than PF group with a recovery time of 13 (10, 17) minutes [median difference of 1 (95% confidence interval 0 to 2)]. As the upper limit of the 95% confidence interval of the difference is 2, which is below the predefined non-inferiority margin of 5 minutes, it is concluded that RF group’s recovery time is non-inferior to that of the propofol group (P=0.084). The recovery of vital signs, ambulation, pain, and surgical bleeding did not differ between the two groups. However, the recovery time for nausea and vomiting was longer in RF group (P<0.05), as indicated in Table 2.
 |
Table 2 Primary Outcomes |
Second Outcomes
No severe sedation-related adverse events occurred in either group. Hypoxemia was noted in 8 patients (4.7%) in RF group compared to 22 patients (12.4%) in PF group (P=0.011). Severe hypoxemia was observed in one patient (0.3%) in PF group, with none occurring in RF group (P=0.328). The use of vasopressors was higher in PF group compared to RF group. There were no differences in the incidence rates of adverse events and the rates of emergency observation between the two groups. The results are summarized in Table 3. Significant decreases of MAP, HR, SpO2 and BIS were observed after induction in PF group compared to RF group (P<0.001, <0.001, 0.048, <0.001, respectively). The results are illustrated in Figure 2.
 |
Table 3 Secondary Outcomes |
 |
Figure 2 Perioperative hemodynamic variables, encompassing (A) HR, (B) MAP, (C) SpO2, (D)BIS. Significant reductions in MAP, HR, SpO2, and BIS were observed post-induction in PF group compared to RF group (P<0.001, <0.001,0.048, <0.001, respectively). Abbreviations: RF, remimazolam combined with fentanyl; PF, propofol combined with fentanyl; HR, heart rate; MAP, mean blood pressure; SpO2, blood oxygen saturation; BIS, bispectral index. Notes: T1: basal values, T2: immediately before gastroscope insertion, T3: 5 min after insertion, T4: 10 min after insertion, T5: 15 min after insertion, T6: 20 min after insertion, T7: 25 min after insertion, T8: 30 min after insertion, T9: time of withdrawal, T10: time of discharge. |
The incidence of general body movements was higher in RF group compared to PF group, while the incidence of severe physical movements was similar between the two groups and did not affect endoscopist satisfaction. The incidence of recall was higher in PF group, and the occurrence of injection pain was also more frequent in PF group. However, there was no difference in patient satisfaction between the two groups. The results are shown in Table 3.
There was no significant difference in the trend of changes in perioperative QoR-15 scores between the two groups and the interaction of group and time (P=0.060, 0.772, respectively). The QoR-15 scores at 1 day and 1 week post-examination were higher than the preoperative levels (P=0.001, 0.035, respectively), and by 1 month post-examination, they had returned to preoperative levels. There was no significant difference in the trend of changes in perioperative PSQI scores between the two groups and the interaction of group and time (P=0.322, 0.548, respectively). The PSQI scores at 1 day and 1 week post-examination were lower than the preoperative levels (P<0,001), and by 1 month post-examination, they had returned to preoperative levels. The above results are presented in Figure 3.
 |
Figure 3 Perioperative QoR-15 scores(A) and PSQI scores (B). There were no noteworthy differences in the trends of changes in perioperative QoR-15 scores and PSQI scores between the two groups (P=0.060, 0.322, respectively). Abbreviations: RF, remimazolam combined with fentanyl; PF, propofol combined with fentanyl. Notes: QoR-15: Quality of Recovery-15, PSQI: Pittsburgh Sleep Quality Index, Pre: prior to the examination, Pos1d: one day after the examination, Pos1w: one week after the examination, Pos1m: one month after the examination. |
Discussion
Our research results indicated that remimazolam could be safely and effectively used for painless gastrointestinal endoscopy in the elderly, and the recovery time was non-inferior to the traditional agent propofol, with fewer associated complications. To date, there are several reviews and meta-analyses that have compared the use of remimazolam and propofol in painless gastrointestinal endoscopy from four major aspects: efficacy (sedation success rate, induction time, or time to loss of consciousness), safety (respiratory depression, hypoxemia, hypotension, bradycardia), side effects (injection pain, nausea, vomiting, dizziness), and postoperative recovery (discharge time, recovery time).23–26 These reviews generally conclude that remimazolam is not inferior to propofol in terms of efficacy, has higher safety, and fewer or comparable side effects. Postoperative recovery time was mentioned in three meta-analyses. One of these included 21 clinical studies,25 while the other two,23,26 which specifically targeted elderly patients, included 4 and 6 clinical studies, respectively. Although the analyses suggested similar recovery times between the two drugs, the high heterogeneity of the studies and publication bias limit the reliability of these conclusions. On the other hand, the number of painless gastrointestinal endoscopy procedures in elderly individuals is increasing annually. Some authors have also suggested that the advantages of remimazolam might be more pronounced in elderly patients.23,26 Therefore, studies comparing remimazolam and propofol with recovery time as the primary endpoint in the elderly population remain clinically valuable.
Based on prior literature and clinical expertise,16,27–31 our study employed individualized medication based on weight, with an initial dose of 0.15 mg/kg remimazolam and 1.0 mg/kg propofol, aligning more closely with the standard of personalized medication. Recent study has recommended a dose of 0.2 mg/kg remimazolam for sedation during upper gastrointestinal endoscopy, but the sedation success rates reported were lower than those in our study.32 The reasons for this may be twofold: first, the target population in the referenced study was non-elderly, while our target population was elderly; second, the referenced study combined 5 μg of sufentanil, whereas we used 1 µg/kg fentanyl, resulting in a relatively higher opioid dosage in our study. In our study, all patients underwent gastrointestinal endoscopy, with sedation success rates of 95.9% in RF group and 98.3% in PF group, respectively. This is consistent with the findings of Chen SH et al, who confirmed that the sedation success rate of remimazolam was 97.35%.33 These rates are higher than those reported by Dou et al in a review encompassing four randomized controlled trials (RCTs), where the sedation success rate of remimazolam was 90.3%. We believe that this difference is attributed to the fact that the sedation success rate data in this review were derived from two RCTs, in which remimazolam was administered at a fixed dosage of 5mg loading dose and 2.5mg supplemental dose.34 Therefore, remimazolam at a dose of 0.15 mg/kg may be more suitable for sedation in painless gastrointestinal endoscopy in elderly patients.
Gastrointestinal endoscopy, characterized by prolonged fasting and bowel preparation, is particularly susceptible to hypotension.7,33 Concurrently, hypoxemia caused by sedative drugs is also the most common complication during gastrointestinal endoscopy sedation. The probability of sedation-related adverse events significantly increases in elderly patients compared to non-elderly individuals.3 Remimazolam is a novel benzodiazepine-class drug, characterized as an ultra-short-acting agent that acts on gamma-aminobutyric acid subtype A (GABAA) receptors. Pharmacological analysis reveals that remimazolam exhibits a clear dose-dependent sedative effect, with a short duration of action and no apparent cardiovascular or respiratory depression.35 The data from this study also support the above conclusions. Due to the non-uniform definition of hypoxemia and the influence of multiple factors such as sedation application, type of endoscopy, dosage administration methods, and the patient’s condition, the reported incidence of hypoxemia under remimazolam sedation currently fluctuates between 2.7% and 15.38% (2.7%36,4.5%,37 9.3%,2 14.2%,38 15.38%10). In our study, the incidence of 85%<SpO2≤90% was 4.7%. Consistent with earlier studies,24,39 our investigation revealed a markedly reduced utilization of cardiovascular active drugs in the remimazolam group as compared to the propofol group. In the prevention of hypotension and hypoxemia, remimazolam appears to be superior to propofol.
Nausea and vomiting are common complications following gastrointestinal endoscopy, and two recent meta-analyses have found no increase in postoperative nausea and vomiting rates with remimazolam compared to propofol.25,26 Interestingly, our research findings indicate that the recovery time for nausea and vomiting was longer in the RF group. And we observed that in RF group, three patients experienced prolonged MPADSS recovery times exceeding 1 hour without reaching a score of 9, necessitating transfer to the emergency department for further observation and treatment, unlike PF group. These individuals all exhibited symptoms such as dizziness, nausea, fatigue and profuse sweating approximately 15–20 minutes postoperatively, with improvement later in the day. Although we did not observe this phenomenon to have statistically significant differences between the two groups, possibly due to insufficient sample size, this observation warrants further investigation.
Most current studies comparing the use of remimazolam in gastrointestinal endoscopy are short-term studies that observe until discharge. Therefore, we extended the follow-up period to better explore and evaluate post-procedure quality of life and sleep quality. Postoperatively, we employed the QoR-15 scale for long-term follow-up observations on the quality of recovery. At 1 day, 1 week, and 1 month postoperatively, there were no differences in recovery between the two groups. Similarly, Choi et al also found that the quality of recovery after remimazolam-based total intravenous anesthesia (TIVA) was non-inferior to that after propofol-based TIVA in female patients undergoing thyroidectomy.17 Considering that remimazolam belongs to the benzodiazepine class of drugs, which may potentially affect sleep,40 and there is limited existing research on the relationship between intraoperative remimazolam infusion and postoperative sleep quality, we concurrently followed up on the sleep status of both groups at 1 day, 1 week, and 1 month postoperatively. No clinically significant differences between groups were observed. From our research findings, it appears that there were changes in both QoR-15 scale and PSQI scores at 1 day and 1 week post-examination compared to preoperative levels, which require one month to return to pre-examination levels, and this trend of change was not related to the choice of sedative drugs.
Limitations
This study had several limitations. First, it was a single-center study, and the number of patients was too small to accurately assess rare adverse events. However, a follow-up at one month postoperatively revealed no observed adverse events. Second, our findings may be applicable primarily to gastroscopies in ASA I–II older patients, with the majority falling within the age range of 65–70 years and a lower proportion of very elderly patients. The generalization of these findings to the broader population or very elderly patients requires further investigation. Third, despite initially incorporating BIS monitoring in the trial design, the ultimate assessment of sedation depth relied on the MOAA/S scale. However, our observations indicated that BIS values in RF group were relatively higher than those in PF group, consistent with the study by Yang et al,41 suggesting that BIS monitoring may not be ideal for assessing remimazolam sedation. However, the above viewpoint still requires further research and validation.
Conclusion
The findings from this trial indicated that the duration of PACU stay when using remimazolam for painless gastrointestinal endoscopy in the elderly was comparable to that of propofol. The quality of postoperative recovery at 1 day, 1 week, and 1 month showed no significant differences. Remimazolam achieved an equivalent sedation success rate while minimizing injection pain and recall, as well as reducing the incidences of hypoxemia and hemodynamic fluctuations. Consequently, remimazolam emerges as a potentially more suitable sedative agent for painless gastrointestinal endoscopy in the elderly.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request. Interested researchers can contact the corresponding author via email. Access to the data will be provided upon agreement and approval by the author.
Acknowledgments
The authors thank the Gastrointestinal Endoscopy Center and the Department of Anesthesiology for their help and support (Beijing Hospital).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Dossa F, Megetto O, Yakubu M, Zhang DDQ, Baxter NN. Sedation practices for routine gastrointestinal endoscopy: A systematic review of recommendations. BMC Gastroenterol. 2021;21(1):22. doi:10.1186/s12876-020-01561-z
2. Liu F, Cheng X, Wang Y, et al. Effect of remimazolam tosilate on the incidence of hypoxemia in elderly patients undergoing gastrointestinal endoscopy: A bi-center, prospective, randomized controlled study. Front Pharmacol. 2023;14:1131391. doi:10.3389/fphar.2023.1131391
3. Shimizu H, Homma Y, Norii T. Incidence of adverse events among elderly vs non-elderly patients during procedural sedation and analgesia with propofol. Am J Emerg Med. 2021;44:411–414. doi:10.1016/j.ajem.2020.04.094
4. Kim SY, Moon CM, Kim MH, et al. Impacts of age and sedation on cardiocerebrovascular adverse events after diagnostic GI endoscopy: A nationwide population-based study. Gastrointest Endosc. 2020;92(3):591–602. doi:10.1016/j.gie.2020.03.3864
5. Chandrasekhara V, Early DS, Acosta RD, et al. Modifications in endoscopic practice for the elderly. Gastrointest Endosc. 2013;78(1):1–7. doi:10.1016/j.gie.2013.04.161
6. Skiljic S, Budrovac D, Cicvaric A, Neskovic N, Kvolik S. Advances in analgosedation and periprocedural care for gastrointestinal endoscopy. Life. 2023;13(2):473. doi:10.3390/life13020473
7. Sneyd JR, Absalom AR, Barends CRM, Jones JB. Hypotension during propofol sedation for colonoscopy: A retrospective exploratory analysis and meta-analysis. Br J Anaesth. 2022;128(4):610–622. doi:10.1016/j.bja.2021.10.044
8. Kilpatrick GJ, McIntyre MS, Cox RF, et al. CNS 7056: A novel ultra-short-acting benzodiazepine. Anesthesiol. 2007;107(1):60–66. doi:10.1097/01.anes.0000267503.85085.c0
9. Liu X, Ding B, Shi F, et al. The efficacy and safety of remimazolam tosilate versus etomidate-propofol in elderly outpatients undergoing colonoscopy: A prospective, randomized, single-blind, non-inferiority trial. Drug Des Devel Ther. 2021;15:4675–4685. doi:10.2147/dddt.s339535
10. Guo J, Qian Y, Zhang X, Han S, Shi Q, Xu J. Remimazolam tosilate compared with propofol for gastrointestinal endoscopy in elderly patients: A prospective, randomized and controlled study. BMC Anesthesiol. 2022;22(1):180. doi:10.1186/s12871-022-01713-6
11. Rex DK, Bhandari R, Lorch DG, Meyers M, Schippers F, Bernstein D. Safety and efficacy of remimazolam in high risk colonoscopy: A randomized trial. Dig Liver Dis. 2021;53(1):94–101. doi:10.1016/j.dld.2020.10.039
12. Sneyd JR, Gambus PL, Rigby-Jones AE. Current status of perioperative hypnotics, role of benzodiazepines, and the case for remimazolam: A narrative review. Br J Anaesth. 2021;127(1):41–55. doi:10.1016/j.bja.2021.03.028
13. Zhou S, Zhu Z, Dai W, et al. National survey on sedation for gastrointestinal endoscopy in 2758 Chinese hospitals. Br J Anaesth. 2021;127(1):56–64. doi:10.1016/j.bja.2021.01.028
14. Yao Y, Guan J, Liu L, Fu B, Chen L, Zheng X. Discharge readiness after remimazolam versus propofol for colonoscopy: A randomised, double-blind trial. Eur J Anaesthesiol. 2022;39(12):911–917. doi:10.1097/eja.0000000000001715
15. Zhang J, Wang X, Zhang Q, Wang Z, Zhu S. Application effects of remimazolam and propofol on elderly patients undergoing Hip replacement. BMC Anesthesiol. 2022;22(1):118. doi:10.1186/s12871-022-01641-5
16. Tan Y, Ouyang W, Tang Y, Fang N, Fang C, Quan C. Effect of remimazolam tosilate on early cognitive function in elderly patients undergoing upper gastrointestinal endoscopy. J Gastroenterol Hepatol. 2022;37(3):576–583. doi:10.1111/jgh.15761
17. Choi JY, Lee HS, Kim JY, et al. Comparison of remimazolam-based and propofol-based total intravenous anesthesia on postoperative quality of recovery: A randomized non-inferiority trial. J Clin Anesth. 2022;82:110955. doi:10.1016/j.jclinane.2022.110955
18. Chernik DA, Gillings D, Laine H, et al. Validity and Reliability of the Observer’s: Assessment of Alertness/Sedation Scale: Study with: Intravenous Midazolam. J Clin Psychopharmacol. 1990;10(4):244–251.
19. Trevisani L, Cifalà V, Gilli G, Matarese V, Zelante A, Sartori S. Post-anaesthetic discharge scoring system to assess patient recovery and discharge after colonoscopy. World J Gastrointest Endosc. 2013;5(10):502–507. doi:10.4253/wjge.v5.i10.502
20. Behrens A, Kreuzmayr A, Manner H, et al. Acute sedation-associated complications in GI endoscopy (ProSed 2 study): Results from the prospective multicentre electronic registry of sedation-associated complications. Gut. 2019;68(3):445–452. doi:10.1136/gutjnl-2015-311037
21. Stark PA, Myles PS, Burke JA. Development and psychometric evaluation of a postoperative quality of recovery score: The QoR-15. Anesthesiol. 2013;118(6):1332–1340. doi:10.1097/ALN.0b013e318289b84b
22. Buysse DJ, Reynolds CF 3rd, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213. doi:10.1016/0165-1781(89)90047-4
23. Lee M, Lee C, Choi GJ, Kang H. Remimazolam for procedural sedation in older patients: A systematic review and meta-analysis with trial sequential analysis. J Pers Med. 2024;14(3):276. doi:10.3390/jpm14030276
24. Barbosa EC, Espírito Santo PA, Baraldo S, Meine GC. Remimazolam versus propofol for sedation in gastrointestinal endoscopic procedures: A systematic review and meta-analysis. Br J Anaesth. 2024;132(6):1219–1229. doi:10.1016/j.bja.2024.02.005
25. An X, Shen T, Yin X, Xu J, Zhang Y, Wang T. The safety of remimazolam versus propofol in gastroscopic sedation: A meta-analysis. BMC Anesthesiol. 2024;24(1):40. doi:10.1186/s12871-024-02422-y
26. Ahmer W, Imtiaz S, Alam DM, et al. Remimazolam versus propofol for sedation in gastrointestinal endoscopy and colonoscopy within elderly patients: A meta-analysis of randomized controlled trials. Eur J Clin Pharmacol. 2024;80(4):493–503. doi:10.1007/s00228-024-03624-6
27. Chen B, Lu L, Zhai J, Hua Z. Effect of moderate versus deep sedation on recovery following outpatient gastroscopy in older patients: A randomized controlled trial. Surg Endosc. 2023;38(3):1273–1282. doi:10.1007/s00464-023-10642-5
28. Ichijima R, Ikehara H, Maeda T, et al. First dose-ranging study of remimazolam in Japanese patients undergoing gastrointestinal endoscopy: Phase II investigator-initiated clinical trial. Digest Endosc. 2022;34(7):1403–1412. doi:10.1111/den.14365
29. Chae D, Kim HC, Song Y, Choi YS, Han DW. Pharmacodynamic analysis of intravenous bolus remimazolam for loss of consciousness in patients undergoing general anaesthesia: A randomised, prospective, double-blind study. Br J Anaesth. 2022;129(1):49–57. doi:10.1016/j.bja.2022.02.040
30. Dai G, Pei L, Duan F, et al. Safety and efficacy of remimazolam compared with propofol in induction of general anesthesia. Minerva Anestesiol. 2021;87(10):1073–1079. doi:10.23736/s0375-9393.21.15517-8
31. Phillips AT, Deiner S, Mo Lin H, Andreopoulos E, Silverstein J, Levin MA. Propofol use in the elderly population: Prevalence of overdose and association with 30-day mortality. Clin Ther. 2015;37(12):2676–2685. doi:10.1016/j.clinthera.2015.10.005
32. Zhu H, Su Z, Zhou H, et al. Remimazolam dosing for gastroscopy: A randomized noninferiority trial. Anesthesiol. 2024;140(3):409–416. doi:10.1097/aln.0000000000004851
33. Chen SH, Yuan TM, Zhang J, et al. Remimazolam tosilate in upper gastrointestinal endoscopy: A multicenter, randomized, non-inferiority, Phase III trial. J Gastroenterol Hepatol. 2021;36(2):474–481. doi:10.1111/jgh.15188
34. Dou D, Feng Y, Jiang L. Efficiency and safety of remimazolam and midazolam in digestive endoscopic sedation: Systematic review and meta-analysis. Digest Endosc. 2022;34(3):653. doi:10.1111/den.14219
35. Upton R, Martinez A, Grant C. A dose escalation study in sheep of the effects of the benzodiazepine CNS 7056 on sedation, the EEG and the respiratory and cardiovascular systems. Br J Pharmacol. 2008;155(1):52–61. doi:10.1038/bjp.2008.228
36. Cao Y, Chi P, Zhou C, Lv W, Quan Z, Xue FS. Remimazolam tosilate sedation with adjuvant sufentanil in chinese patients with liver cirrhosis undergoing gastroscopy: A randomized controlled study. Med Sci Monit. 2022;28:e936580. doi:10.12659/msm.936580
37. Lu K, Wei S, Ling W, et al. Remimazolam versus propofol for deep sedation/anaesthesia in upper gastrointestinal endoscopy in elderly patients: A multicenter, randomized controlled trial. J Clin Pharm Ther. 2022;47(12):2230–2236. doi:10.1111/jcpt.13797
38. Zhang K, Bao Y, Han X, et al. Effects of opioid-free propofol or remimazolam balanced anesthesia on hypoxemia incidence in patients with obesity during gastrointestinal endoscopy: A prospective, randomized clinical trial. Front Med. 2023;10:1124743. doi:10.3389/fmed.2023.1124743
39. Wei A, Ma S, Dou Y, et al. The safety and efficacy of remimazolam tosylate combined with propofol in upper gastrointestinal endoscopy: A multicenter, randomized clinical trial. PLoS One. 2023;18(8):e0282930. doi:10.1371/journal.pone.0282930
40. Tan WF, Miao EY, Jin F, Ma H, Lu HW. Changes in first postoperative night bispectral index after daytime sedation induced by dexmedetomidine or midazolam under regional anesthesia: A randomized controlled trial. Reg Anesth Pain Med. 2016;41(3):380–386. doi:10.1097/aap.0000000000000370
41. Yang C, Jiao J, Nie Y, Shao W, Zhang H, Huang S. Comparison of the bispectral indices of patients receiving remimazolam and propofol for general anesthesia: A randomized crossover trial. Anaesth Crit Care Pain Med. 2024;43(3):101377. doi:10.1016/j.accpm.2024.101377
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.