Back to Journals » Neuropsychiatric Disease and Treatment » Volume 16
Comparison of Relapse Prevention with 3 Different Paliperidone Formulations in Patients with Schizophrenia Continuing versus Discontinuing Active Antipsychotic Treatment: A Post-Hoc Analysis of 3 Similarly Designed Randomized Studies
Authors Mathews M, Gopal S ![]() , Singh A
, Singh A ![]() , Nuamah I, Pungor K
, Nuamah I, Pungor K ![]() , Tan W
, Tan W ![]() , Soares B, Kim E
, Soares B, Kim E ![]() , Savitz AJ
, Savitz AJ
Received 28 June 2019
Accepted for publication 17 December 2019
Published 19 June 2020 Volume 2020:16 Pages 1533—1542
DOI https://doi.org/10.2147/NDT.S221242
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Maju Mathews,1 Srihari Gopal,2 Arun Singh,3 Isaac Nuamah,4 Katalin Pungor,5 Wilson Tan,6 Bernardo Soares,7 Edward Kim,8 Adam J Savitz2
1Global Medical Affairs, Janssen Research & Development, LLC, Titusville, NJ, USA; 2Department of Neuroscience, Janssen Research & Development, LLC, Titusville, NJ, USA; 3Department of Neuroscience, Janssen Research & Development, LLC, Pennington, PA, USA; 4Clinical Biostatistics, Janssen Research & Development, LLC, Titusville, NJ, USA; 5Medical Affairs, Janssen-Cilag GmbH, Neuss, North Rhine-Westphalia, Germany; 6Regional Medical Affairs, Janssen Pharmaceutical Companies of Johnson and Johnson, Singapore; 7Medical Affairs, Jan-Cil, High Wycombe, Buckinghamshire, UK; 8Janssen Scientific Affairs, Janssen Scientific Affairs, LLC, Titusville, NJ, USA
Correspondence: Maju Mathews
Global Medical Affairs, Janssen Research & Development, LLC, 1125 Trenton-Harbourton Road, Titusville, NJ, USA
Tel +1 609 433-9257
Email [email protected]
Background: Sudden discontinuation from antipsychotic treatment is a common occurrence in patients with schizophrenia. Lower rates of relapse could be expected for patients discontinuing treatment from longer-acting formulations vs their shorter-acting equivalents.
Objective: To compare relapse rates and time-to-relapse between the active (analogous to adherent patients) and placebo (analogous to non-adherent patients in the real-world) arms of three different formulations of paliperidone (oral paliperidone extended release [paliperidone ER], paliperidone palmitate once monthly [PP1M], and paliperidone palmitate three monthly [PP3M] long-acting injectables).
Methods: Data from three similarly designed, randomized relapse prevention studies in adult patients with schizophrenia were analyzed.
Results: In total, 922 patients were included (active treatment: 473, placebo: 449). Lowest percentage of patients experienced relapse with PP3M PP1M (172 days [134– 222 days])> paliperidone ER (58 days [42– 114 days]) and was “not-estimable” in the active treatment group due to low relapse rates. Hazard ratios (HR) of the three paliperidone formulations relative to their respective placebos were PP3M ([HR: 3.81; 95% CI: 2.08, 6.99; P< 0.0001]> PP1M [HR: 3.60; 95% CI: 2.45, 5.28; P< 0.0001]> paliperidone ER [HR: 2.83; 95% CI: 1.73, 4.63; P< 0.001]).
Conclusion: The lower percentage of relapse during active treatment and longer time to relapse after discontinuing active treatment with longer-duration antipsychotic formulations suggests the benefit of longer-acting over shorter-acting formulations, especially in patients susceptible to poor adherence.
Clinical trial registration: paliperidone ER (NCT00086320), PP1M (NCT00111189), and PP3M (NCT01529515).
Keywords: relapse prevention, schizophrenia, oral paliperidone extended release, paliperidone palmitate once monthly, paliperidone palmitate three monthly
Introduction
Schizophrenia is a chronic illness often associated with a decline in social, occupational and cognitive functioning.1 Pharmacological interventions for the management of schizophrenia are aligned at alleviating symptoms, maximizing quality of life and maintaining recovery to prevent disease worsening.2 Although multiple treatment options are available for the management of schizophrenia, patients frequently experience relapses due to poor or partial adherence to antipsychotics.2 Longitudinal studies have demonstrated microglia abnormalities and grey matter atrophy resulting in loss of brain tissue in multiple regions of the brain and suggest these aberrations are associated with incidences of acute relapses.3–6 Therefore, long-term, continued pharmacological treatment is the mainstay in schizophrenia management with a primary goal of relapse prevention.7
A large percentage of patients with schizophrenia discontinue their medications, often without notifying anyone.8 Antipsychotic formulations with longer half-lives and slow release profiles help maintain therapeutic plasma levels for longer durations, enabling longer dosing intervals, thereby improving prospects for medication adherence and treatment continuity vs their shorter-acting equivalent.7,9–11 Consequently, longer time-to-relapse can be expected in patients discontinuing long-acting injectables (LAIs) during its remaining duration of drug exposure vs the shorter-acting oral antipsychotics.
The LAI formulations of paliperidone (paliperidone palmitate once monthly [PP1M] and paliperidone palmitate three monthly [PP3M]) can be expected to increase time-to-relapse as well as reduce the risk of relapse vs their shorter-acting oral equivalent (paliperidone ER).12 The time-to-relapse estimated for oral paliperidone ER formulation was 83 days and not estimable for PP1M and PP3M in their respective primary studies, which could be attributed to the low water solubility and differences in the pharmacokinetic profile of the LAI formulations vs oral paliperidone ER.13–15 Further, in a post-hoc analysis of three similarly designed relapse prevention studies of paliperidone formulations, an increase in time to first relapse and reduction in number of patients experiencing relapse was observed with the LAI formulations of paliperidone vs oral paliperidone ER in clinically stable patients who later discontinued their active treatment (placebo, analogous to non-adherent).16 These observations were in agreement with the hypothesis that longer half-lives (PP1M: 25 to 49 days [dose range: 39 mg to 234 mg]; PP3M: 84 to 95 days [deltoid injection], 118 to 139 days [gluteal injection], [dose range: 273 mg to 819 mg] vs paliperidone ER: ~23 hrs) confer more sustained relapse prevention after treatment discontinuation.9–11,16
In the current post-hoc analysis, we further analyzed the three studies to compare the time-to-relapse and related change in efficacy scales, in patients suddenly discontinuing antipsychotics (patients randomized to placebo groups) vs patients who continue treatment (patients randomized to active treatment groups).13–15 The placebo groups from the three studies represent an appropriate model to simulate what might happen to patients in the real world on suddenly discontinuing ongoing antipsychotic therapy (non-adherent patients); whereas, the active arms represent adherent patients who continue treatment.13–15
Methods
Study Design
This post-hoc analysis used data from three similarly designed, randomized, double-blind (DB), placebo-controlled, relapse-prevention studies of paliperidone ER (NCT00086320; 2004 to 2005), PP1M (NCT00111189; 2005 to 2007), and PP3M (NCT01529515; 2012 to 2014) conducted over a period of 10 years.13–15 These studies conducted to evaluate the impact of long-term use of different paliperidone formulations had a two-stage group sequential design and could be terminated early based on the results of an interim analysis that assessed efficacy based on a pre-specified number of relapses.
All three studies had a variable open-label phase (paliperidone ER, 14 weeks; PP1M, 33 weeks; and PP3M, 29 weeks) during which eligible patients in each study received either paliperidone ER, PP1M or PP3M during the run-in/transition phase (paliperidone ER, 8 weeks; PP1M, 9 weeks; PP3M, 17 weeks). Patients in the OL phase were considered symptomatically stable if they had a Positive and Negative Syndrome Scale (PANSS) total score below a predetermined value (≤70; paliperidone ER; ≤75, PP1M; <70, PP3M) and PANSS scores of ≤4 (moderate or less) on selected individual items (P1, delusion; P2, conceptual disorganization; P3, hallucinatory behavior; P6, suspiciousness/persecution; P7, hostility; G8, uncooperativeness), in addition to ≤4 PANSS G14 score (poor impulse control) for PP1M and PP3M only and Clinical Global Impression-Severity (CGI-S) score of ≤4 (moderately ill or better) for paliperidone ER only.
The stabilized patients from the OL run-in/transition phase entered the variable maintenance phase (paliperidone ER, 6 weeks; PP1M, 24 weeks; PP3M, 12 weeks) prior to entering the DB treatment phase where they were randomized to receive either paliperidone (paliperidone ER, daily; PP1M, monthly; PP3M every three months) at the same dose administered at end of the stabilization/maintenance phase or placebo. Administration of matching placebo in the DB phase after the last dose of paliperidone was initiated either on the next day (paliperidone ER), after a month (PP1M) or after 3 months (PP3M) depending on the formulation type. Until relapse or withdrawal from the study or termination from the study, all patients remained in the DB phase. The details of the overall study design, similarities and differences are shown in Figure 1.
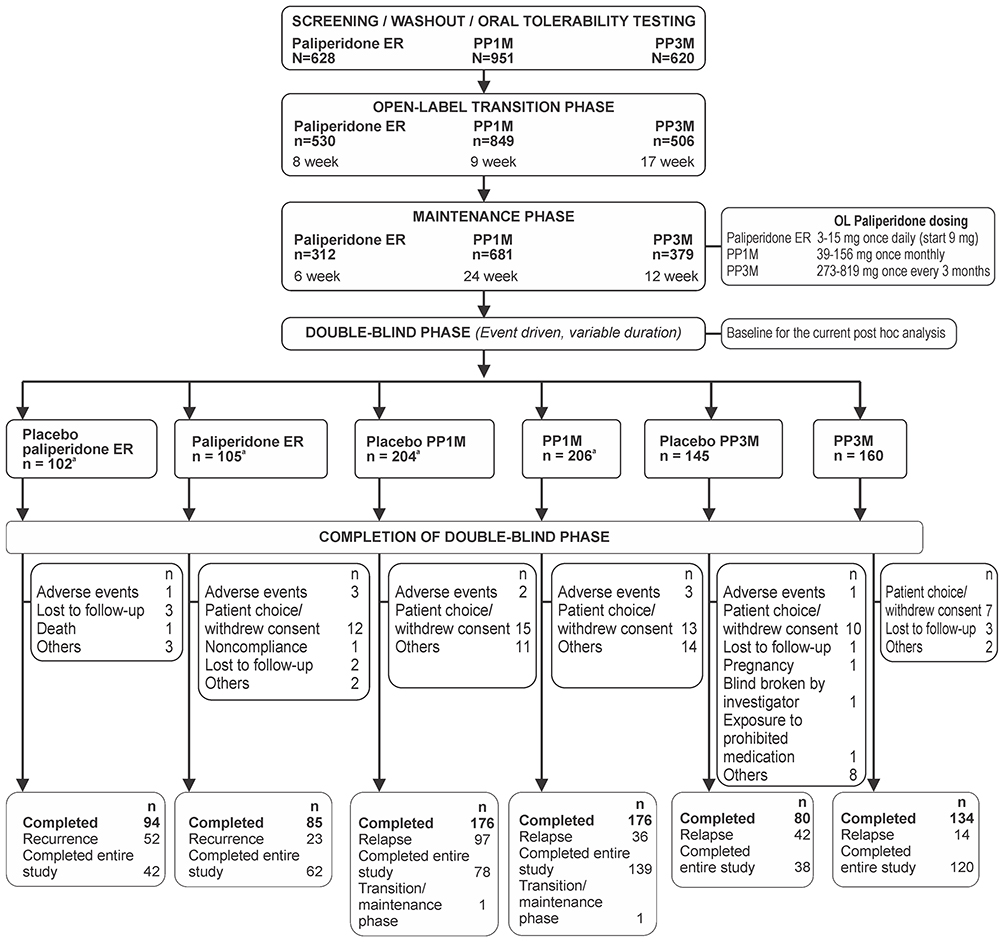 |
Figure 1 Flowchart of overall study design, highlighting major similarities and differences. aOne patient in each treatment group was randomized but was in the transition/maintenance phase when the study was stopped and did not receive any double-blind injections. Abbreviations: ER, extended release; LAI, long-acting injectable; PP1M, paliperidone palmitate once monthly LAI; PP3M, paliperidone palmitate three monthly LAI. |
An Independent Ethics Committee or Institutional Review Board (listed in Supplementary material) approved the study protocols and all three studies were conducted in accordance with the Declaration of Helsinki, Good Clinical Practices, and applicable regulatory requirements. All patients provided written informed consent before participating in the study.
Key Inclusion/Exclusion Criteria
Detailed inclusion/exclusion criteria are described in the individual study publications.13–15 Briefly, the three studies included patients (men and women aged 18 to 65 years [PP3M: ≤70 years]) with schizophrenia (Diagnostic and Statistical Manual of Mental Disorders Fourth edition [DSM-IV] diagnosis) and PANSS total score between 70 to 120 (for paliperidone ER and PP1M studies) and <120 (for PP3M study).
Patients with major DSM-IV diagnosis other than schizophrenia ≤6 months or other medical or psychiatric conditions, history of depot antipsychotic use ≤28 days (PP1M study) or ≤120 days (PP3M study) before screening were excluded from the studies.
In the PP1M study, patients on paliperidone ER could enter the OL phase and in the PP3M study, symptomatically-stable patients on other LAI antipsychotic could switch to PP1M and then transition to PP3M, if the transitions were clinically validated.13
Study Endpoints
The primary endpoint measure was the time-to-relapse of schizophrenia symptoms during the DB phase. Relapse was defined based on the Csernansky et al17 criteria. Patients fulfilling ≥1 of the following criteria were considered to have relapsed (1) hospitalization for symptoms of schizophrenia (involuntary or voluntary admission), (2) 25% increase in PANSS total score for two consecutive assessments for patients who scored >40 at randomization, or a 10-point increase for patients who scored ≤40 at randomization, (3) deliberate self-injury or aggressive behavior, or suicidal or homicidal ideation and aggressive behavior that was clinically significant, (4) increase for two consecutive assessments in pre-specified individual PANSS item scores (P1, P2, P3, P6, P7 and G8) to ≥5 for patients whose score was ≤3 at randomization, or to ≥6 for patients whose score was 4 at randomization. The secondary endpoints included change from DB baseline to endpoint in PANSS total score, CGI-S and Personal and Social Performance (PSP) scale scores. Safety was reported previously for each of the individual studies so it was not included in the current analysis.13–15 Safety assessments included treatment-emergent adverse events (TEAEs), extrapyramidal symptom (EPS), clinical laboratory tests, vital sign measurements, 12-lead electrocardiograms, physical examination findings, and injection-site evaluations.
A pre-planned interim analysis was performed in all three studies by an independent data-monitoring committee following a pre-defined number of relapse events (paliperidone ER, 43; PP1M, 68; and PP3M, 42). The studies were terminated early at the interim analysis stage when the efficacy was established based on pre-specified relapse events and level of significance (paliperidone ER, P value: 0.01; PP1M, P value: 0.0106; PP3M, P value: 0.0101). Following the termination of studies, all data after the interim analyses were collected and included in the final analysis. The results of final analysis were included in the individual studies and subsequently in this post-hoc analysis.
Statistical Analysis
The current or final analysis included all patients who were included up to the interim cut-off date and subsequently until the completion of the study. All final efficacy analyses from the DB phase were reported for the intent-to-treat (ITT) analysis set, which included randomized patients who received ≥1 dose of treatment in the DB phase. Demographics and baseline characteristics (DB phase) were summarized descriptively. Kaplan–Meier method was used to analyze time-to-relapse and estimate its cumulative distribution function. Hazard ratios (HRs) and 95% confidence intervals (CIs) were estimated using a Cox proportional hazards regression model. HR >1 denotes longer time-to-relapse for each paliperidone formulation vs its respective placebo arm. Reasons for relapse were summarized. In all three studies, secondary efficacy endpoints were analyzed at a 2-sided significance level of α =0 0.05 across treatment groups and adjustments were not made for multiplicity.
Results
Patient Disposition and Demographics
All 922 (placebo, n = 449; paliperidone, n = 473) patients from the three studies who entered the DB treatment phase and received at least one study dose were included in this post-hoc analysis. A total of 801 patients (86.9%; placebo, n = 392; paliperidone, n = 409) completed the study as defined by having a relapse or being enrolled in the study when it completed. Baseline characteristics and demographics were generally well-balanced across all studies except for a few differences such as predominance of men (>53%) and white (>60%) patients across both treatment arms for all three studies (Table 1) which was also observed in patients entering the DB phase.16
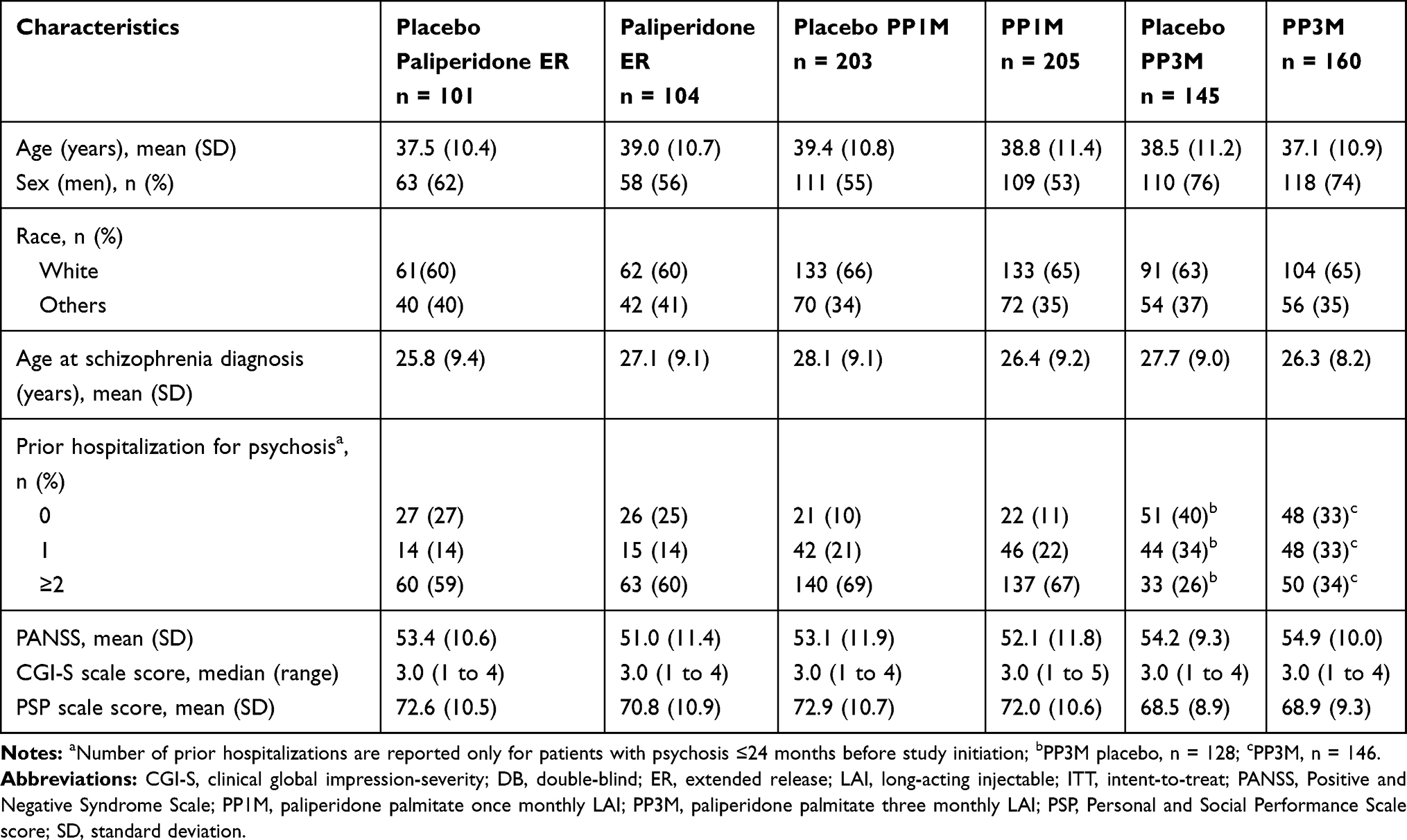 |
Table 1 Demographics and Baseline Characteristics (ITT Population) |
Time-to-Relapse and Associated Change in Key Secondary Parameters
In the placebo group, median time-to-relapse was significantly longer with PP3M, 395 days (274 days to “not reached”) > PP1M, 172 days (134 to 222 days) > paliperidone ER, 58 days (42 to 114 days); (Figure 2) for the final analysis. The HR and 95% CI of the various formulations relative to their respective placebos were PP3M (HR: 3.81; 95% CI: 2.08, 6.99; P <0.0001); PP1M (HR: 3.60; 95% CI: 2.45, 5.28; P <0.0001) and paliperidone ER (HR: 2.83; 95% CI: 1.73, 4.63; P <0.001); (Figure 3). Thus, post discontinuation of PP3M and PP1M, a delay in relapse was observed vs the paliperidone ER group. In the active treatment group, the median time-to-relapse could not be estimated. The percentage of patients who experienced relapse was lowest with PP3M vs PP1M and paliperidone ER in both the active (PP3M, 9% < PP1M, 18% < paliperidone ER, 22%) and placebo group patients (PP3M, 29% < PP1M, 48% < paliperidone ER, 52%) (Table 2).
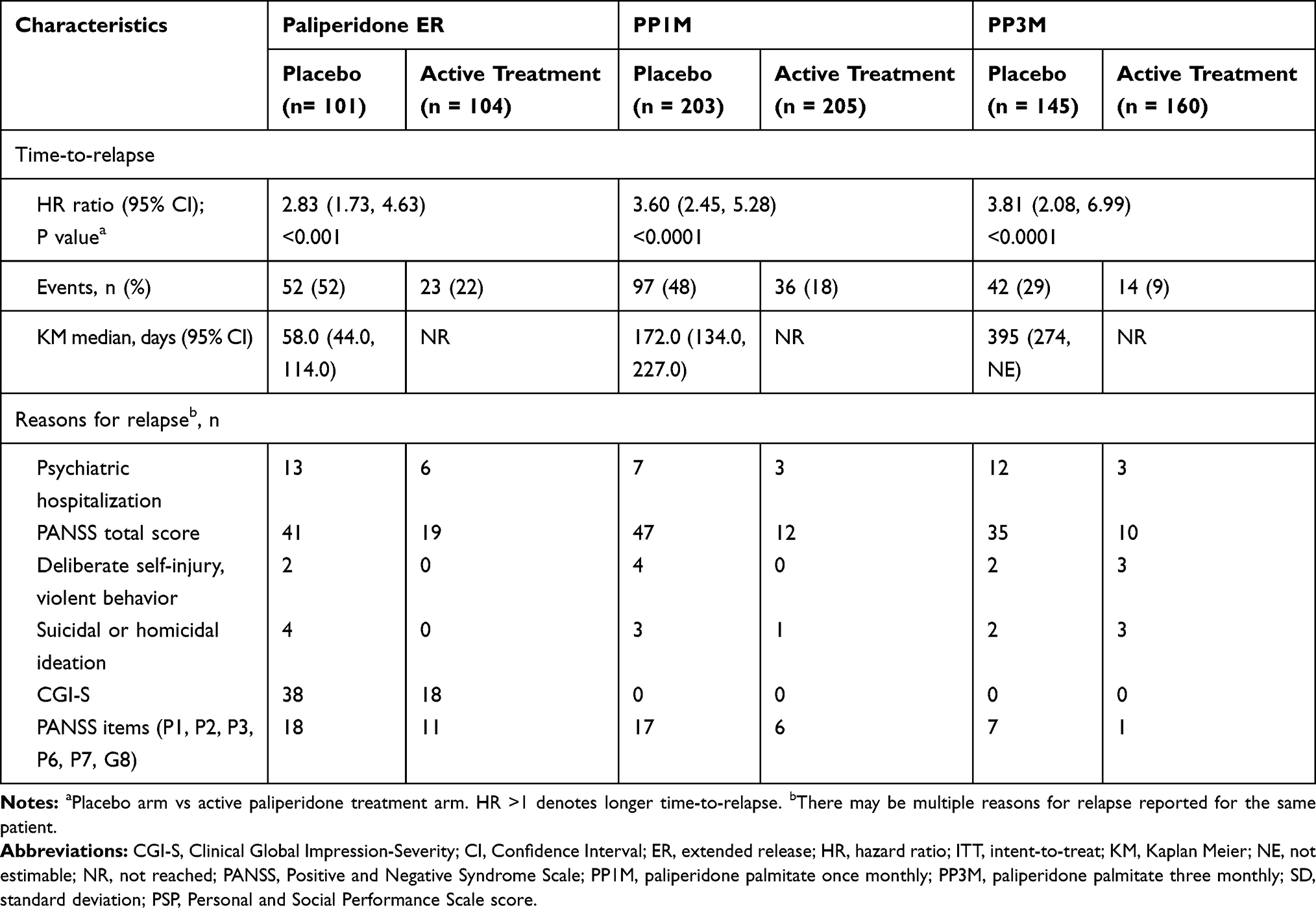 |
Table 2 Time-to-Relapse and Reasons for Relapse (ITT) Final Analysis Set |
 |
Figure 2 Kaplan-Meier plots of three paliperidone formulations vs placebo. (A) Paliperidone ER. (B) PP1M. (C) PP3M. Abbreviations: ER, extended release; LAI, long-acting injectable; PP1M, paliperidone palmitate once monthly LAI; PP3M, paliperidone palmitate three monthly LAI; |
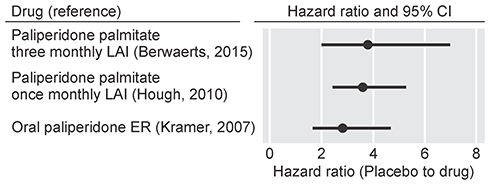 |
Figure 3 Forest plot of the hazard ratios from paliperidone ER and paliperidone palmitate studies with placebo. Abbreviations: CI, confidence interval; ER, extended release; LAI, long-acting injectable. |
Symptom exacerbations as reflected by an increase in PANSS total score were the most common reasons for relapse. Relatively fewer patients in the active vs placebo groups experienced relapse due to increase in PANSS total score and increase in PANSS items P1, P2, P3, P6, P7, and G8 (Table 2).
Secondary Efficacy Endpoints
PANSS total scores either remained stable or decreased (improved) with active paliperidone treatment; mean (SD) changes from DB baseline to endpoint of DB phase were significant vs patients who discontinued treatment (placebo group). Active vs placebo values were: paliperidone ER: 6.0 (13.6) vs 15.1 (19.1), P ≤0.003; PP1M: 2.5 (12.2) vs 11.1 (16.6), P ≤0.0001 and PP3M: −0.5 (8.4) vs 6.7 (14.4), P≤0.001 (Table 3; Figure 4). The median [range] CGI-S scores remained unchanged (paliperidone ER, 0 [‒2 to 3], P ≤0.003; PP1M, 0 [‒1 to 3], P ≤0.0001; PP3M, 0 [‒2 to 3], P ≤0.001) while a significant increase (indicating improvement) in mean (SD) PSP score (paliperidone ER, ‒3.0 [10.4], P ≤0.003; PP1M, ‒1.5 [11.5], P ≤0.0001; PP3M, ‒0.5 [6.6], P ≤0.001) from DB baseline to the end of DB phase in patients continuing active treatment was also observed. Numerical increases in CGI-S and PSP score were observed in patients discontinuing respective paliperidone formulation.
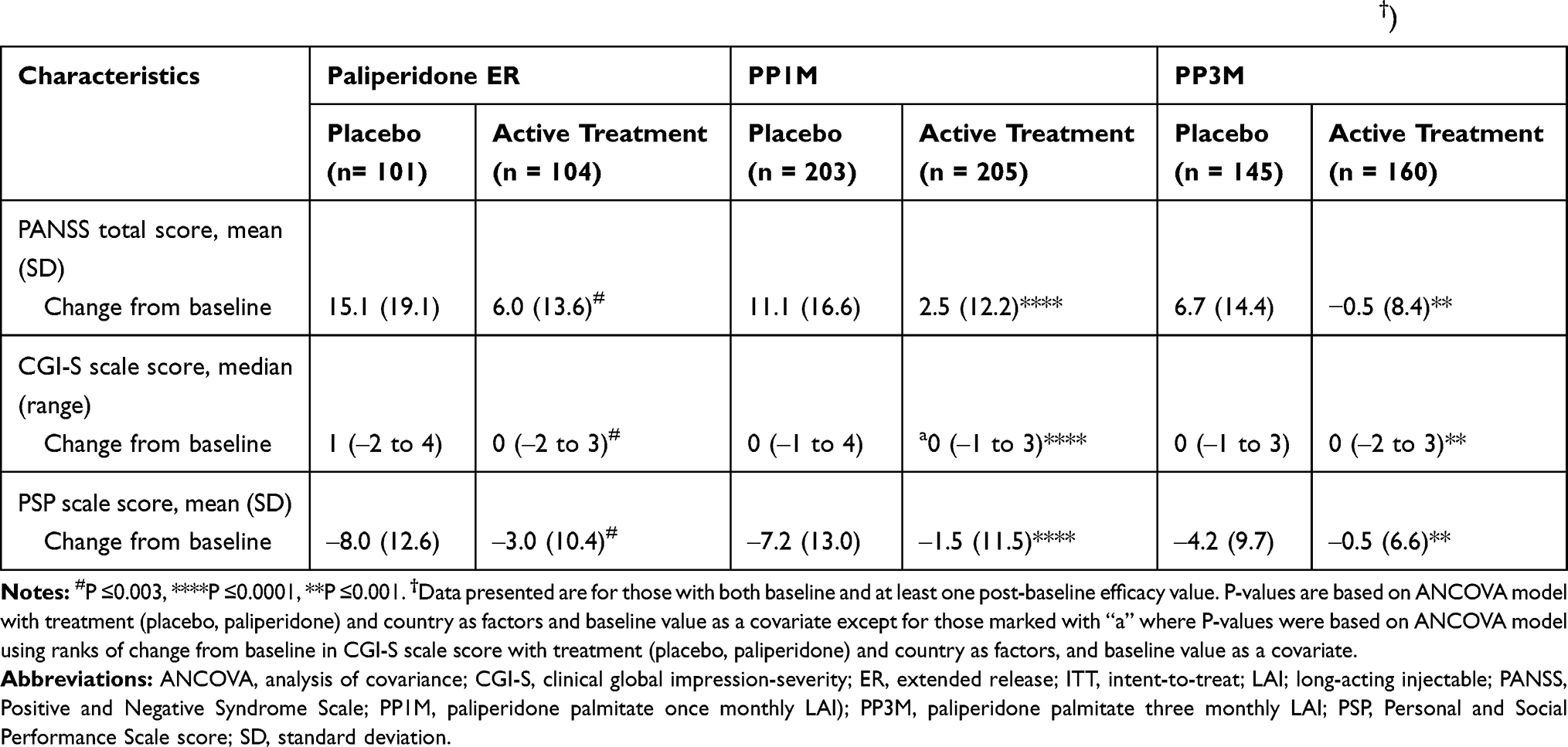 |
Table 3 Change in Secondary Efficacy Measures from Double-Blind Baseline to End of the Double-Blind Phase (ITT†) |
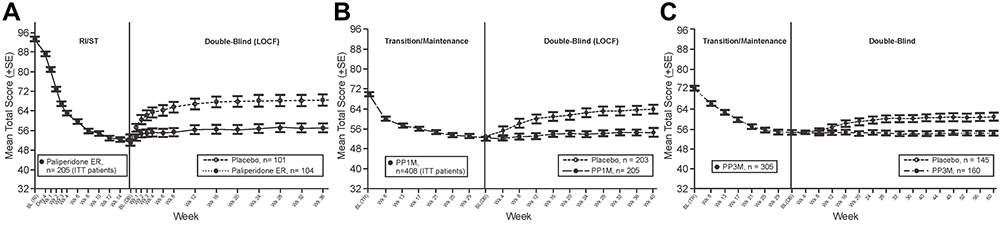 |
Figure 4 Positive and Negative Syndrome Scale (PANSS) total scores over time for three different formulations of Paliperidone. (A) Paliperidone ER. (B) PP1M. (C) PP3M. Abbreviations: ER, extended release; LAI, long-acting injectable; PP1M, paliperidone palmitate once monthly LAI; PP3M, paliperidone palmitate three monthly ; RI/ST, run-in and stabilization phases |
Safety
Apart from events related to the injection site, the safety profile was similar across all 3 formulations of paliperidone (Table 4). Two deaths occurred during the three studies (placebo in paliperidone ER group: 1 suicide; 1 patient being shot) and none were reported in any of the paliperidone formulation groups.
 |
Table 4 Treatment-Emergent Adverse Events During Double-Blind Phase (Safety Analysis Set) |
Discussion
In this post-hoc analysis, patients continuing active paliperidone treatment (analogous to “adherent” patients in the real world) had a significantly lower risk of relapse as compared to those who discontinued treatment and received placebo after stabilization (analogous to “non-adherent” patients in the real world). Further, the risk of relapse was numerically lower with longer-acting formulations of paliperidone (PP3M<PP1M<paliperidone ER). Post-discontinuation median time-to-relapse was also longer with paliperidone LAI treatments (PP1M: 172 days; PP3M: 395 days) as compared with oral paliperidone ER (58 days). Consistent with these observations, patients who were switched to placebo post-stabilization phase had greater relapse rates vs patients who continued on active treatment (paliperidone ER: 52% vs 22%; PP1M: 48% vs 18%; PP3M: 29% vs 9%).
The relative relapse rates between patients who continued on any of the three different active paliperidone treatments could not be determined in this analysis, as <50% of patients experienced a relapse. A recent post-hoc comparison of the same studies demonstrated that the relative relapse rates were 2.27 fold higher for patients discontinuing paliperidone ER vs PP1M, 4.47 fold higher for patients discontinuing paliperidone ER vs PP3M and 2.08 fold higher for patients discontinuing PP1M vs PP3M.16
Long-term treatment goals in schizophrenia require that patients not only remain in symptom control, but also maintain the ability to function in the community, socially as well as vocationally.18 The three studies included in this analysis used validated tools to assess symptom severity (PANSS), functional status (PSP) and clinical response (CGI-S).19–21 Supporting the results of relapse assessment and consistent with earlier reports, changes in secondary endpoints suggested improvements in symptomatic and functional parameters in patients continuing their active paliperidone treatment.22,23 As anticipated, an increase in PANSS total score and CGI-S and reduction in PSP scores suggesting worsening were observed in patients who discontinued treatment and switched to placebo.
In clinical practice, the majority of patients with schizophrenia respond well to pharmacological interventions; however, patients may eventually experience worsening of symptoms and recurrent relapse due to non-adherence to dosing regimens, especially with daily oral medication. Further, every recurrent or longer episode of relapse may have a negative impact on neurodevelopment and brain integrity; it is therefore important for treatments to offer relapse prevention that is sustained.3,4 Longer-acting formulations of paliperidone provide an extended relapse-free window for non-adherent patients, wherein they can be encouraged to become adherent, and for adherent patients, fewer and delayed relapses over the course of a lifetime of schizophrenia may provide protection against aberrant brain changes and help preserve functioning.3,4,24 The present findings support the recent National Institute for Health and Care Excellence (NICE) recommendations of using a longer-acting formulation of paliperidone for improving adherence, reducing relapse and rehospitalizations.25
The randomized withdrawal design used in all three studies is applicable to clinical practice, as it mimics the real-life sudden discontinuation of antipsychotics observed in patients with schizophrenia. However, there were some limitations: the data included in the current analysis were combined from 3 separate studies in a post-hoc manner. The studies were not designed to assess differences across different formulations and there were differences in the lengths of paliperidone exposure (OL phase), stabilization period, and follow-up (DB phase) across studies. The differences in time-to-relapse and relapse rates were based on numerical comparison of HRs and tests to determine the statistical significance of differences were not used.
Conclusions
Active treatment with paliperidone formulations was associated with significantly longer time-to-relapse and reduced relapse rates as compared with discontinuation of these treatments (simulated by placebo groups in the DB phase). Time-to-relapse after treatment discontinuation was longer with longer-duration formulations, so that PP3M > PP1M > oral paliperidone. The enduring effect of longer-acting formulations in reducing relapses was seen both in patients who continued active antipsychotic treatment and those who discontinued medications (placebo group). These effects can most likely be associated with the longer durations of sustained therapeutic plasma levels with PP3M and PP1M as compared with oral paliperidone ER. Fewer and delayed relapses over the course of a lifetime of schizophrenia may provide protection against progressive brain damage and help preserve functioning.
Acknowledgments
Rohit Bhandari, PhD, and Priya Ganpathy, MPharm, CMPP™ (SIRO Clinpharm Pvt. Ltd., India) provided writing assistance and Ellen Baum, PhD (Janssen Research & Development, LLC) provided editorial support for this article. Data from this study were presented as a poster at the APA2018, SIRS2018, RCP2018, CPA2018, ECNP2018 and RCP2018.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
This study was funded by Janssen Research & Development, LLC, USA. The sponsor provided a formal review for this article.
Disclosure
SG, MM, AS, AJS and IN are employees of Janssen Research & Development, LLC, United States. AJS, SG, KP, EK and MM hold stocks of Johnson & Johnson. KP is an employee of Janssen-Cilag GmbH, Neuss, Germany, WT is an employee of Janssen Pharmaceutical Companies of Johnson and Johnson, Singapore and BS is an employee of Jan-Cilag UK and EK is an employee of Janssen Scientific Affairs, LLC, Titusville, New Jersey, United States. The authors report no other conflicts of interest in this work.
References
1. WHO. The World Health Report: mental health: new understanding, new hope; 2001. Available from: http://www.who.int/whr/2001/en/whr01_en.pdf?ua=1.
2. Lehman AF, Lieberman JA, Dixon LB, et al. Practice guideline for the treatment of patients with schizophrenia, second edition. Am J Psychiatry. 2004;161(2 Suppl):1–56.
3. Andreasen NC, Liu D, Ziebell S, Vora A, Ho BC. Relapse duration, treatment intensity, and brain tissue loss in schizophrenia: a prospective longitudinal MRI study. Am J Psychiatry. 2013;170(6):609–615. doi:10.1176/appi.ajp.2013.12050674
4. Laskaris LE, Di Biase MA, Everall I, et al. Microglial activation and progressive brain changes in schizophrenia. Br J Pharmacol. 2016;173(4):666–680. doi:10.1111/bph.v173.4
5. Wang M, Zhang L, Gage FH. Microglia, complement and schizophrenia. Nat Neurosci. 2019;22(3):333–334. doi:10.1038/s41593-019-0343-1
6. Whitford TJ, Grieve SM, Farrow TF, et al. Progressive grey matter atrophy over the first 2-3 years of illness in first-episode schizophrenia: a tensor-based morphometry study. Neuroimage. 2006;32(2):511–519. doi:10.1016/j.neuroimage.2006.03.041
7. Kane JM. Strategies for improving compliance in treatment of schizophrenia by using a long-acting formulation of an antipsychotic: clinical studies. J Clin Psychiatry. 2003;64 Suppl 16(Suppl 16):34–40.
8. Tiihonen J, Haukka J, Taylor M, Haddad PM, Patel MX, Korhonen P. A nationwide cohort study of oral and depot antipsychotics after first hospitalization for schizophrenia. Am J Psychiatry. 2011;168(6):603–609. doi:10.1176/appi.ajp.2011.10081224
9. Invega Sustenna® Prescribing Information. The official Invega Sustenna® website; June 2017. Available from: https://www.invegasustenna.com/revised.
10. Invega Trinza® Prescribing Information. The official Invega Trinza® website; Revised June 2016. Available from: https://www.invegatrinzahcp.com.
11. Invega® Prescribing Information. The official Invega® (paliperidone) extended---release tablets website; Revised June 2018. Available from: http://www.invega.com/prescribing-information.
12. Schreiner A, Aadamsoo K, Altamura AC, et al. Paliperidone palmitate versus oral antipsychotics in recently diagnosed schizophrenia. Schizophr Res. 2015;169(1–3):393–399. doi:10.1016/j.schres.2015.08.015
13. Berwaerts J, Liu Y, Gopal S, et al. Efficacy and safety of the 3-month formulation of paliperidone palmitate vs placebo for relapse prevention of schizophrenia: a randomized clinical trial. JAMA Psychiatry. 2015;72(8):830–839. doi:10.1001/jamapsychiatry.2015.0241
14. Hough D, Gopal S, Vijapurkar U, Lim P, Morozova M, Eerdekens M. Paliperidone palmitate maintenance treatment in delaying the time-to-relapse in patients with schizophrenia: a randomized, double-blind, placebo-controlled study. Schizophr Res. 2010;116(2–3):107–117. doi:10.1016/j.schres.2009.10.026
15. Kramer M, Simpson G, Maciulis V, et al. Paliperidone extended-release tablets for prevention of symptom recurrence in patients with schizophrenia: a randomized, double-blind, placebo-controlled study. J Clin Psychopharmacol. 2007;27(1):6–14. doi:10.1097/JCP.0b013e31802dda4a
16. Weiden PJ, Kim E, Bermak J, Turkoz I, Gopal S, Berwaerts J. Does half-life matter after antipsychotic discontinuation? A relapse comparison in schizophrenia with 3 different formulations of paliperidone. J Clin Psychiatry. 2017;78(7):e813–e820. doi:10.4088/JCP.16m11308
17. Csernansky JG, Mahmoud R, Brenner R, Risperidone USASG. A comparison of risperidone and haloperidol for the prevention of relapse in patients with schizophrenia. N Engl J Med. 2002;346(1):16–22. doi:10.1056/NEJMoa002028
18. Osborne RH, Dalton A, Hertel J, Schrover R, Smith DK. Health-related quality of life advantage of long-acting injectable antipsychotic treatment for schizophrenia: a time trade-off study. Health Qual Life Outcomes. 2012;10:35. doi:10.1186/1477-7525-10-35
19. Morosini PL, Magliano L, Brambilla L, Ugolini S, Pioli R. Development, reliability and acceptability of a new version of the DSM-IV Social and Occupational Functioning Assessment Scale (SOFAS) to assess routine social functioning. Acta Psychiatr Scand. 2000;101(4):323–329.
20. Kay SR, Fiszbein A, Opler LA. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr Bull. 1987;13(2):261–276. doi:10.1093/schbul/13.2.261
21. Busner J, Targum SD. The clinical global impressions scale: applying a research tool in clinical practice. Psychiatry (Edgmont). 2007;4(7):28–37.
22. Emsley R, Oosthuizen PP, Kidd M, Koen L, Niehaus DJ, Turner HJ. Remission in first-episode psychosis: predictor variables and symptom improvement patterns. J Clin Psychiatry. 2006;67(11):1707–1712. doi:10.4088/JCP.v67n1106
23. Emsley R, Oosthuizen PP, Koen L, Niehaus DJ, Martinez G. Symptom recurrence following intermittent treatment in first-episode schizophrenia successfully treated for 2 years: a 3-year open-label clinical study. J Clin Psychiatry. 2012;73(4):e541–547. doi:10.4088/JCP.11m07138
24. Bartzokis G, Lu PH, Amar CP, et al. Long acting injection versus oral risperidone in first-episode schizophrenia: differential impact on white matter myelination trajectory. Schizophr Res. 2011;132(1):35–41. doi:10.1016/j.schres.2011.06.029
25. NICE guidelines. Antipsychotic guidelines (version 7); 2018. Available from: https://www.guidelines.co.uk/mental-health/nice-dementia-guideline/454244.article.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.