Back to Journals » International Journal of General Medicine » Volume 19
Comparison of Postoperative Visual Acuity and Visual Quality Among Vision Enhancing Bifocal Intraocular Lenses (AM4UH), Bifocal IOLs, and Monofocal IOLs
Authors Xu Z, Ma X, Gao J, Liu F, Han D
Received 27 August 2025
Accepted for publication 21 January 2026
Published 3 February 2026 Volume 2026:19 563632
DOI https://doi.org/10.2147/IJGM.S563632
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Brian C. Gilger
Ziwei Xu, Xinli Ma, Jiayue Gao, Fa Liu, Dan Han
Department of Ophthalmology, Harbin 242 Hospital, Harbin City, People’s Republic of China
Correspondence: Dan Han, Email [email protected]
Objective: To compare visual acuity and visual quality after implantation of Vision Enhancing bifocal intraocular lens (IOL), bifocal IOL or monofocal IOL in patients with age-related cataract.
Methods: Retrospective study. Group A was implanted with Vision Enhancing bifocal (bifocal combined extended depth of focus (EDOF)) IOL (Eyebright Medical Technology (Beijing) Co. Ltd. China: AM4UH, 21 eyes), group B was implanted with bifocal IOL (Johnson & Johnson, USA: ZMB00, 21 eyes), and group C was implanted with monofocal IOL (Eyebright Medical Technology (Beijing) Co. Ltd. China: A1UL22, 21 eyes). At 3 months postoperatively, uncorrected distance visual acuity (UDVA) was compared among 3 groups, while uncorrected near visual acuity (UNVA) and uncorrected intermediate visual acuity (UIVA), defocus curves, and visual quality questionnaire results were compared between Group A and B.
Results: There was no statistically significant difference in UDVA among three groups postoperatively (P > 0.05); in terms of UIVA and UNVA, group A was better than group B (P < 0.05); the defocus curves showed that group A was close to bimodal but tended to be flat, while group B was bimodal; groups A and B became spectacle-independent postoperatively, and 40% of patients in group B reported the halo phenomenon, especially when driving at night.
Conclusion: Vision Enhancing bifocal IOL (AM4UH) exhibited a better UIVA and UNVA, indicating a continuous visual range. And patients implanted with AM4UH achieved postoperative spectacle independence, with less visual disturbance.
Keywords: age-related cataract, intraocular lens, extended depth of field
Introduction
Cataract remains the first or second leading cause of visual impairment worldwide,1 primarily characterized by lens opacity affecting visual acuity. Refractive cataract surgery has been the most fundamental and effective approach to treating cataracts and restoring vision, with phacoemulsification combined with intraocular lens (IOL) implantation being one of the primary procedures. As patients’ demands for postoperative visual and quality of life increase, the kinds and design of IOL have evolved continuously. Monofocal IOLs provide satisfactory distance visual acuity but are associated with a high dependence on spectacles for near vision.2 Bifocal IOLs effectively improve both distance and near vision; however, intermediate vision often remains suboptimal, and discontinuous vision may cause discomfort.3 To address these limitations, EDOF IOLs offer continuous vision, leading manufacturers to integrate EDOF optical designs with bifocal configurations to overcome the inherent drawbacks of conventional bifocal IOLs.4,5 The Tecnis Synergy ZFR00 IOL (Johnson & Johnson, USA) is a representative model of this category.6,7 As a new vision enhancing bifocal IOL, the AM4UH IOL (Eyebright Medical Technology (Beijing) Co., Ltd., China) adopts a similar design, featuring a high-order aspheric EDOF profile on the anterior surface combined with a diffractive bifocal (0D and +3.2D) structure on the posterior surface, aiming to improve intermediate vision acuity. While laboratory studies have objectively measured optical quality and demonstrated that the AM2UH (which differs from the AM4UH only in its near addition of +2.8D) exhibits extended depth of focus characteristics comparable to those of the AT LARA EDOF IOL (Zeiss, Germany),8 clinical reports on the effectiveness of bifocal-EDOF hybrid IOLs predominantly focus on other products, such as the Tecnis Synergy ZFR00,9 rather than China-made AM4UH. Therefore, it is necessary to conduct clinical research to evaluate the efficacy of the Vision Enhancing IOL AM4UH.
Materials and Methods
Study and Patients
This was a retrospective study. Clinical and follow-up data of 63 cases (63 eyes) of senile cataract patients who underwent phacoemulsification combined with IOL implantation in Department of Ophthalmology of Harbin 242 Hospital from May to July 2024 were collected. This study strictly complied with the principles of the Helsinki Declaration and clinical norms, and the research protocol was approved by the Ethics Committee of Harbin 242 Hospital (Approval No. lw-2024002). All participants signed informed consent before enrollment, agreeing to the use of their clinical data for research. Patients were divided into three groups based on the type of IOL implanted: Group A (Vision Enhancing bifocal IOL [AM4UH]), Group B (bifocal IOL [ZMB00]), and Group C (monofocal IOL [A1UL22]), with 21 cases (21 eyes) in each group.
Inclusion criteria: (1) Diagnosed with age-related cataract without a history of major ocular or systemic diseases; (2) Regular astigmatism, with preoperative and postoperative corneal astigmatism <1 D, kappa angle <0.3 mm, and 6 mm corneal spherical aberration >0.2 μm; (3) Pupil diameter of 3.5–5.5 mm in bright environment and 4–6 mm in dark environment.
Exclusion criteria: (1) Any other ocular diseases significantly affecting vision, such as corneal diseases, glaucoma, uveitis, severe fundus lesions; (2) History of previous intraocular surgery or trauma; (3) Intraoperative or postoperative complications, such as posterior capsule rupture, IOL dislocation, severe posterior capsule opacification; (4) Incomplete clinical data.
Preoperative Examinations
All three groups underwent preoperative electrocardiogram, chest X-ray, uncorrected visual acuity, intraocular pressure, slit-lamp examination, ocular color Doppler ultrasound, fundus photography, optical coherence tomography, visual evoked potential, corneal endothelial microscopy, and IOL calculation. The refractive powers for the three IOL models were calculated using their respective manufacturers’ online calculators. Although the computational principles of these calculators differ, they all aimed for emmetropia (0 D) as the target refraction.
Surgical Procedure
After thorough posterior capsule polishing, the IOL was implanted into the capsular bag. The viscoelastic material was completely aspirated from the anterior chamber, and the incisions were hydrated to ensure watertight closure.
Outcome Measurements
Slit-lamp examination was performed to evaluate anterior segment structures and assess IOL position. Non-contact tonometry was used to measure intraocular pressure (IOP). Fundus examination was conducted using a fundus lens. Standard logarithmic visual acuity charts were used to examine the uncorrected distant visual acuity (UDVA, 5 m), uncorrected intermediate visual acuity (UIVA, 66 cm), and uncorrected near visual acuity (UNVA, 40 cm) of the tested eyes. Using a comprehensive optometer, the lens refraction was adjusted in 0.5 D increments (range: −4.5 D to +1.5 D) in front of the patient’s eye, and the best corrected visual acuity corresponding to each lens degree was measured and recorded. The defocus curve was plotted with lens refraction as the horizontal axis and logMAR visual acuity as the vertical axis. Additionally, the incidence of adverse visual phenomena was investigated by inquiring whether patients experienced glare or halos. And the postoperative spectacle independence rate was investigated by having patients report whether they needed to wear glasses for distance, intermediate, and near vision tasks.
Intraocular Lenses
The AM4UH IOL (Eyebright Medical Technology (Beijing) Co., Ltd., China) is an aspheric diffractive IOL, made of hydrophobic acrylic material. It combines diffractive design and extended depth of focus high-order aspheric technology, with an additional dioptric power of +3.2D.10
The Tecnis Synergy ZMB00 IOL (Johnson & Johnson Surgical Vision, Inc., Santa Ana, CA, USA) is a one-piece full-optical diffractive bifocal IOL (+4.0D). It features low chromatic aberration and pupil independence, improving visual quality under different lighting conditions and significantly enhancing patients’ postoperative distant and near vision.11
The A1UL22 IOL (Eyebright Medical Technology (Beijing) Co., Ltd., China) is a one-piece monofocal aspheric IOL, made of hydrophobic acrylic material, effectively correcting postoperative distant vision in cataract patients. The characteristics of three types of IOLs were shown in Table 1.
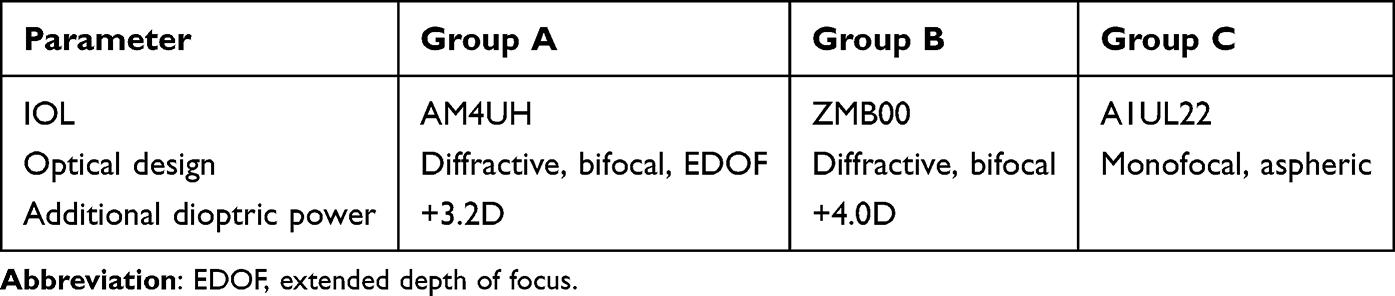 |
Table 1 Characteristics of IOLs in Groups A, B, and C |
Statistical Analysis
Data were analyzed using IBM SPSS 22.0 statistical software. Categorical variables (such as sex) were expressed as frequency and percentage (%), and intergroup comparisons were performed using the chi-square test. Continuous variables were expressed as mean ± standard deviation. The normality of data samples was tested using the Shapiro–Wilk test, and intergroup comparisons were conducted using independent t-test or Mann–Whitney U-test based on normality. All statistical tests were two-sided, and P < 0.05 was considered statistically significant.
Results
Baseline Data
A total of 63 cases (63 eyes) successfully received IOL implantation, with 21 cases (21 eyes) in each of Groups A, B, and C. The baseline characteristics of the three groups, including age, gender distribution, and axial length, were balanced and comparable (P > 0.05) (Table 2). All patients’ operative eyes recovered well postoperatively, with normal anterior segments, centered IOL position, and normal fundus and intraocular pressure.
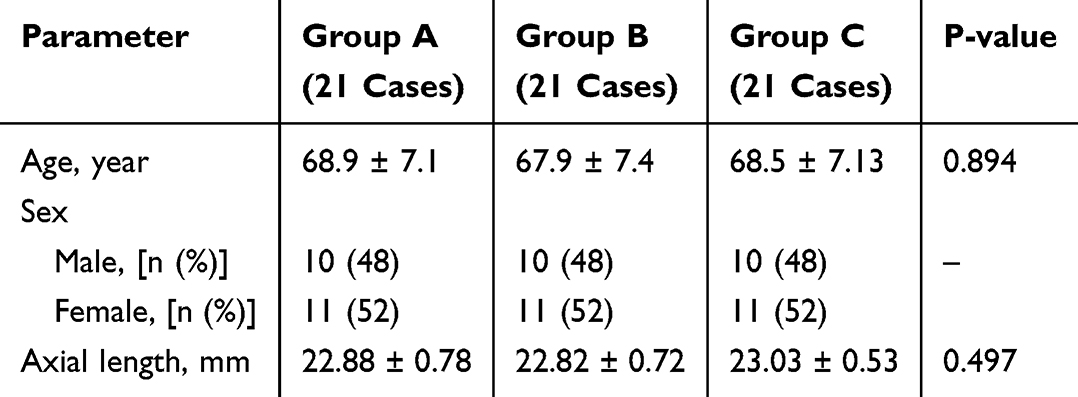 |
Table 2 Comparison of Preoperative Baseline Characteristics in Groups A, B, and C |
Postoperative Visual Acuity
Groups A, B, and C demonstrated comparable distance visual acuity (P > 0.05). Compared with Group B (ZMB00), Group A (AM4UH) showed significantly improved intermediate and near visual acuity (all P < 0.05) (Table 3).
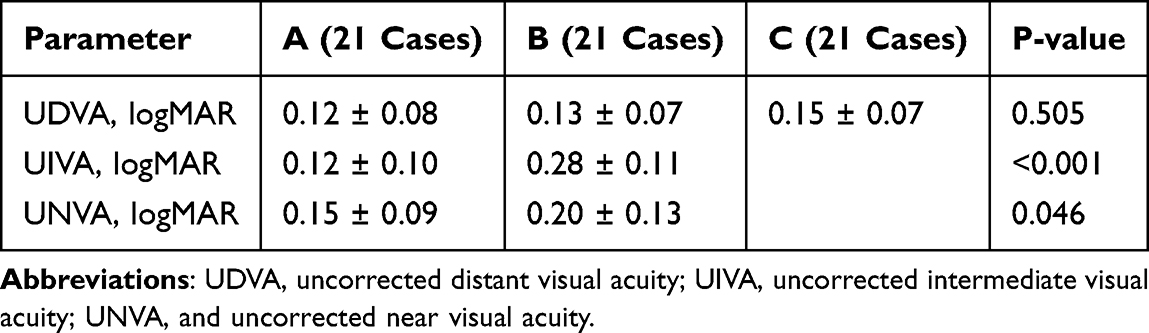 |
Table 3 Comparison of Postoperative UDVA, UIVA, and UNVA Among Groups A, B, and C |
Defocus Curve
The postoperative defocus curves of Groups A and B at 3 months were shown in Figure 1. The defocus curve of Group A was smooth, while that of Group B showed two peaks (at 0 D and −2.5 D), suggesting differential adaptation to defocus. Compared with Group B, Group A maintained a higher visual acuity from −1.5D to −2.5D, showing a plateau (vision value > 0.3 logMAR) within the −1.0 D to −2.5 D defocus range, indicating that IOL in Group A improved intermediate visual acuity and provided a more continuous range of vision postoperatively. From −3.0 D to −4.5D, Group B had better postoperative visual acuity than Group A (P < 0.05), indicating that IOL in Group B provided more favorable near visual acuity at the shorter distance (≤33 cm). These results were consistent with the results of UDVA, UIVA and UNVA.
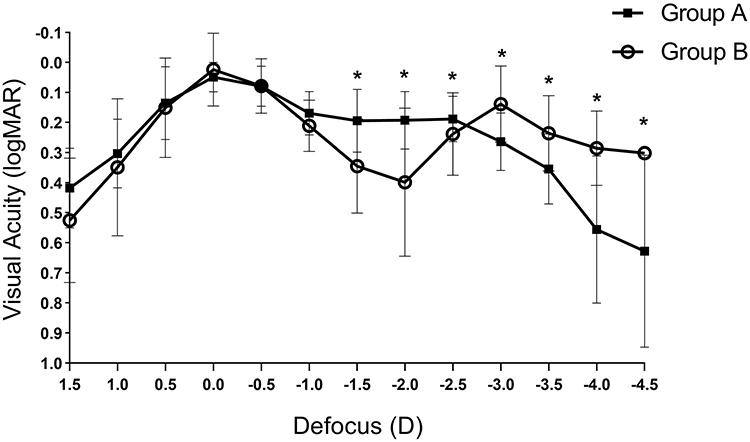 |
Figure 1 Defocus curve at 3 months after intraocular lens implantation. *, statistically significant difference between Group A and group B, P < 0.05. |
Postoperative Visual Quality
Postoperatively, 20 valid cases were obtained in each of Groups A and B for questionnaire surveys. Both groups achieved 100% spectacle independence for distant and near vision without discomfort (Table 4). However, 8 patients (40%) in Group B complained of nighttime halos, especially during night driving, which did not affect daily life.
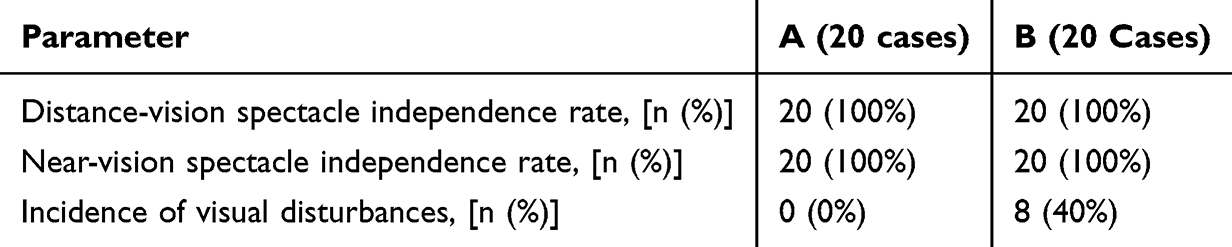 |
Table 4 Results of Visual Quality Questionnaire in Groups A and B |
Discussion
With the continuous development of IOLs, modern cataract surgery is no longer limited to enabling patients to “see”, but aims to meet their requirements for clearer and more comfortable visual quality. Moreover, patients, influenced by the digital lifestyle, have an increasing need for near-vision tasks, making the selection of IOLs to achieve optimal intermediate and near visual quality a common focus for surgeons, patients, and IOL manufacturers.12
Monofocal IOLs provide a single focal point, primarily improving distance vision postoperatively, so patients require spectacle correction beyond the preset focal range, which may compromise lifestyle convenience.13 Bifocal IOLs provide two optical focal points, addressing near vision needs and reducing dependence on spectacle lenses,9,10 but intermediate visual acuity remains low, and reports of nighttime halos and discomfort after implantation are common.14 Vision Enhancing bifocal IOL AM4UH combines EDOF technology with diffractive bifocal design. The posterior surface of the AM4UH adopts a bifocal design, distributing light to two focal points (0D and +3.2D) for distance and near vision. Simultaneously, its anterior surface utilizes a high-order aspheric EDOF design to diffract light at the focal points, extending it on an extended longitudinal plane between the two focal points to improve intermediate vision. This study demonstrated the effectiveness and safety of a novel bifocal and EDOF hybrid IOL (AM4UH) and provided a new selection for cataract patients.
This study evaluated postoperative uncorrected visual acuity of the three IOLs. All three IOLs provided excellent distance vision with no statistically significant intergroup differences (P > 0.05). The Vision Enhancing bifocal IOL AM4UH achieved superior intermediate visual acuity (0.12 ± 0.10 vs 0.28 ± 0.11 logMAR, P < 0.001) due to its EDOF design, which distributes more light between the distance and near focal points—a feature the ZMB00 lacks. It is consistent with previous findings.7,15 Moreover, AM4UH demonstrated better near visual acuity (0.15 ± 0.09 vs 0.20 ± 0.13 logMAR, P < 0.05), because its +3.2D add power is lower than the +4.0D of ZMB00, resulting in a longer optimal near working distance. Previous studies have indicated that ZMB00 IOL’s optimal near working distance is 33 cm.16 Consequently, when measured at the standard 40 cm distance in this study, the AM4UH exhibited better near visual acuity.
Defocus curve measurement involves adding lenses with different refractions in front of the eye, altering retinal imaging through the lenses’ light convergence/divergence, and simulating ocular accommodation at a fixed target distance.17 The defocus curve showed that the Vision Enhancing bifocal IOL (AM4UH) had a smoother overall trend and a significant advantage in intermediate vision over bifocal IOLs (ZMB00), with a higher visual acuity plateau, indicating a more continuous visual range and smoother vision transition, consistent with previous studies.18,19 However, at its shorter optimal working distance of 33 cm, the bifocal IOL ZMB00 demonstrated better near visual acuity (0.14 logMAR) compared to the AM4UH (0.19 logMAR at 40 cm). This difference is attributable to its higher add power (ZMB00: +4.0D vs AM4UH: +3.2D), which reflects the inherent trade-off between near vision optimization and intermediate vision continuity inherent in their optical designs. The result of defocus curve was consistent with the result of uncorrected visual acuity.
Previous studies have shown that EDOF technology improves near visual comfort.20 Both AM4UH and ZMB00 showed high spectacle independence, but 8 (40%) patients with the bifocal IOL (ZMB00) complained of nighttime halos, especially during night driving, without obvious discomfort or impact on daily life. The higher incidence of halos in the bifocal IOL group may relate to its higher additional dioptric power. Previous studies have shown that bifocal IOLs with +3.75D additional dioptric power have a higher frequency of halos than those with +2.50D.21
This study has several limitations: a small sample size, the absence of defocus curve for the monofocal IOL group; a short follow-up period of only 3 months; and a lack of objective assessments of visual quality or reading speed under mesopic conditions. Future studies with follow-up extended to one year or longer may demonstrate the long-term stability of AM4UH in visual and safety outcomes.
Conclusion
In conclusion, Vision Enhancing bifocal IOL AM4UH exhibited a better intermediate and near visual acuity than bifocal IOL, indicating a continuous visual range. Future follow-up could be extended with measurements of optical performance data to enhance credibility.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
All authors declare no conflicts of interest in this work.
References
1. Flaxman SR, Bourne RRA, Resnikoff S, et al. Global causes of blindness and distance vision impairment 1990-2020: a systematic review and meta-analysis. Lancet Glob Health. 2017;5(12):e1221–7. doi:10.1016/S2214-109X(17)30393-5
2. Nijkamp MD, Dolders MG, de Brabander J, et al. Effectiveness of multifocal intraocular lenses to correct presbyopia after cataract surgery: a randomized controlled trial. Ophthalmol. 2004;111(10):1832–1839. doi:doi: 10.1016/j.ophtha.2004.05.023
3. Anshel JR. Visual ergonomics in the workplace. Aaohn J. 2007;55(10):414–420.
4. Rampat R, Gatinel D. Multifocal and extended depth-of-focus intraocular lenses in 2020[J]. Ophthalmology. 2021;128(11):e164–185. doi:10.1016/j.ophtha.2020.09.026
5. Webers VSC, Bauer NJC, Saelens IEY, et al. Comparison of the intermediate distance of a trifocal IOL with an extended depth-of-focus IOL: results of a prospective randomized trial. J Cataract Refract Surg. 2020;46(2):193–203. doi:10.1097/j.jcrs.0000000000000012
6. Ozturkmen C, Kesim C, Karadeniz PG, et al. Visual acuity, defocus curve and patient satisfaction of a new hybrid EDOF-multifocal diffractive intraocular lens. Eur J Ophthalmol. 2022;32(5):2988–2993. doi:10.1177/11206721211057338
7. Dick HB, Ang RE, Corbett D, et al. Comparison of 3-month visual outcomes of a new multifocal intraocular lens vs a trifocal intraocular lens. J Cataract Refract Surg. 2022;48(11):1270–1276. doi:10.1097/j.jcrs.0000000000000971
8. Son HS, Łabuz G, Khoramnia R, et al. Laboratory analysis and ray visualization of diffractive optics with enhanced intermediate vision. BMC Ophthalmol. 2021;21(1):197. doi:10.1186/s12886-021-01958-8
9. Shin DE, Lee H, Koh K. Comparative analysis of a presbyopia-correcting intraocular lens that combines extended depth-of-focus and bifocal profiles with a standard monofocal intraocular lens. BMC Ophthalmol. 2022;22(1):302. doi:10.1186/s12886-022-02516-6
10. Farvardin M, Johari M, Attarzade A, et al. Comparison between bilateral im-plantation of a trifocal intraocular lens (Alcon Acrysof IQ®PanOptix) and extended depth of focus lens (Tecnis® Symfony® ZXR00 lens)[J]. Int Ophthalmol. 2021;41:567–573. doi:10.1007/s10792-020-01608-w
11. Du QX, Liu XM, Ma WH, et al. Evaluation of optical performance of different non-diffractive extended depth-of-focus intraocular lenses in vitro. Chin J Ophthalmol. 2024;60(6):494–502. doi:10.3760/cma.j.cn112142-20240226-00082
12. Zhu X, He W, Zhang S, et al. Dome-shaped macula: A potential protective factor for visual acuity after cataract surgery in patients with high myopia. Br J Ophthalmol. 2019;103(11):1566–1570. doi:10.1136/bjophthalmol-2018-313279
13. Qin Q, Liu J, Chen H, et al. Comparison of visual quality between trifocal and monofocal intraocular lenses one year after implantation. Zhonghua Shi Yan Yan Ke Za Zhi. 2022;40(5):454–460. doi:10.3760/cma.j.cn115989-20200211-00060
14. Leyland M, Zinicola E. Multifocal versus monofocal intraocular lenses in cataract surgery: a systematic review. Ophthalmology. 2003;110(9):1789–1798. doi:10.1016/S0161-6420(03)00722-X
15. Chang DH, Hu JG, Lehmann RP, et al. Clinical performance of a hybrid presbyopia-correcting intraocular lens in patients undergoing cataract surgery in a multicenter trial. J Cataract Refract Surg. 2023;49(8):840–847. doi:10.1097/j.jcrs.0000000000001205
16. Dell SJ. Evaluation of visual and subjective outcomes with mix-and-match of three one-piece Tecnis Multifocal IOLs of varying add powers. Clin Ophthalmol. 2020;14:2903–2911. doi:10.2147/OPTH.S266120
17. Plaza-Puche AB, Aliój L, Macrae S, et al. Correlating optical bench performance with clinical defocus curves in varifocal and trifocal intraocular lenses. Refract Surg. 2015;31(5):300–307. doi:10.3928/1081597X-20150423-03
18. Wang JM, Che JB, Yuan XW, et al. Effects of different types of intraocular lens implantation on patient’s visual quality and function after phacoemulsification. Zhonghua Yi Xue Za Zhi. 2024;104(16):1391–1396. doi:10.3760/cma.j.cn112137-20231125-01198
19. de Medeiros AL, de Araújo Rolim AG, Motta AFP, et al. Comparison of visual outcomes after bilateral implantation of a diffractive trifocal intraocular lens and blended implantation of an extended depth of focus intraocular lens with a diffractive bifocal intraocular lens. Clin Ophthalmol. 2017;11:1911–1916. doi:10.2147/OPTH.S145945
20. Wang J, Luo J, Yang W, et al. Efficacy and comfort following the implantation of extended depth of focus, multifocal, and monofocal intraocular lenses in cataract patients. BMC Ophthalmol. 2024;24(1):423. doi:10.1186/s12886-024-03685-2
21. Altinkurt E, Muftuoglu O. Comparison of three different diffractıve multifocal intraocular lenses with a +2.5, +3.0, and +3.75 diopter additıon power. Saudi J Ophthalmol. 2019;33(4):353–362. doi:10.1016/j.sjopt.2019.09.007
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.