Back to Journals » Journal of Pain Research » Volume 15
Comparison of Percutaneous Endoscopic Interlaminar Discectomy and Open Fenestration Discectomy for Single-Segment Huge Lumbar Disc Herniation: A Two-year Follow-up Retrospective Study
Authors Ma C ![]() , Li H, Zhang T, Wei Y, Zhang H, Yu F, Lv Y, Ren Y
, Li H, Zhang T, Wei Y, Zhang H, Yu F, Lv Y, Ren Y ![]()
Received 5 December 2021
Accepted for publication 6 April 2022
Published 13 April 2022 Volume 2022:15 Pages 1061—1070
DOI https://doi.org/10.2147/JPR.S352595
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Krishnan Chakravarthy
Cheng Ma,1,* He Li,1,* Teng Zhang,1 Yifan Wei,1 Helong Zhang,1 Fenglei Yu,1 You Lv,2 Yongxin Ren1
1Department of Orthopaedics, The First Affiliated Hospital of Nanjing Medical University, Nanjing, 210029, Jiangsu, People’s Republic of China; 2Department of Orthopaedics, Lianyungang Clinical College of Nanjing Medical University, The First People’s Hospital of Lianyungang, Lianyungang, 222061, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yongxin Ren, Tel +86 13585162283, Email [email protected]
Purpose: Both percutaneous endoscopic lumbar discectomy (PELD) and open fenestration discectomy (OFD) are effective and safe surgical procedures for the treatment of LDH. The purpose of this retrospective study was to compare the surgical outcomes of percutaneous endoscopic interlaminar discectomy (PEID) and OFD for single-segment huge lumbar disc herniation (HLDH).
Patients and Methods: We retrospectively analyzed 91 patients diagnosed with single-segment HLDH and treated with OFD or PEID. Visual analog scale (VAS), modified Japanese orthopedic association (mJOA) and Oswestry disability index (ODI) were used to assess clinical outcomes at preoperation and postoperatively at 3, 6, 12, and 24months. Modified Macnab criteria were applied to evaluate clinically satisfaction at the final follow-up.
Results: In both groups, the VAS and ODI scores at 3, 6, 12, and 24months postoperatively showed a significant decrease and the mJOA score at 3, 6, 12, and 24months postoperatively was significantly increased compared to preoperative results (P< 0.001). According to Macnab criteria at the final follow-up, the overall clinically satisfactory rate was 86.67% in the OFD group and 86.96% in the PEID group. There were no significant differences in VAS, ODI, and mJOA scores between the two groups at preoperation and postoperative 3, 6, 12, and 24months, respectively. In the PEID group, the length of hospitalization and the length of incision were significantly shorter than that in the OFD group (P< 0.0001). However, there was no significant difference in operative time between groups (P=0.81).
Conclusion: Collectively, postoperative clinical results were equally favorable for both procedures, with no statistically significant difference between PEID and OFD at the two-year of follow-up. No serious complication was observed in two groups. Compared with the traditional surgery, PEID has the following benefits: less trauma, less bleeding, speedy recovery, and shorter hospitalization. Therefore, PEID may be a promising alternative to traditional surgery.
Keywords: percutaneous endoscopic lumbar discectomy, percutaneous endoscopic interlaminar discectomy, open fenestration discectomy, single-segment, huge lumbar disc herniation
Introduction
Lumbar disc herniation (LDH) is one of the most common orthopedic disorders for society, which is the cause of lower back pain and sciatica.1 A herniation that occupies more than fifty percent of the canal cross-sectional area on computed tomography (CT) scans and magnetic resonance images (MRI) is defined as a huge, large, massive, or giant disc herniation.2 According to statistics, the incidence of huge lumbar disc herniation (HLDH) accounts for 8 to 22% of all cases of LDH.3 As a special type of lumbar disc herniation, HLDH usually results in more severe back and leg pain, as well as often associated with neurological deficits, compared to general LDH.4,5 The long-term clinical outcomes of Spine Patient Outcomes Research Trial (SPORT) suggested significantly greater improvement in pain, function and satisfaction in operative group compared to nonoperative group.6–8 Several observational studies have shown that surgical treatment provides more effective and rapid pain relief for patients who are diagnosed with HLDH.2,9–12
The traditional surgical approach, open fenestration discectomy (OFD), has been considered as a standard surgical treatment for LDH for many years.13 Currently, percutaneous endoscopic lumbar discectomy (PELD), with the development of endoscopes and instruments, the increased experience of surgeons, and the great demands by patients for minimally invasive procedure, is commonly used worldwide and is considered to be the gold standard surgical procedure for the treatment of LDH.14,15 PEID adopts a posterior approach, passing through the lamina and ligamentum flavum, entering the spinal canal and finally reaching the intervertebral disc, especially suitable for for the treatment of L5/S1 intervertebral disc herniation. Since Ruetten introduced PEID in 2006, this technique has been widely accepted by spinal surgeons for its more familiar anatomical approach and more direct intraspinal decompression.15
Previously, several observational studies have also tried to compare the efficacy and safety of these two procedures.16,17 It has been reported that both PELD and OFD are effective and safe surgical procedures for the treatment of LDH and no significant difference was found in pain and other functional scores. However, to date, few data are available on comparison of the clinical effectiveness between percutaneous endoscopic interlaminar discectomy (PEID) and OFD for HLDH. The purpose of this retrospective study was to compare the surgical outcomes of PEID and OFD for single-segment HLDH.
Patients and Methods
Patients
The study conforms to the principles outlined in the Declaration of Helsinki. Ethical committee approval was obtained from the Institutional Review Board of the First Affiliated Hospital of Nanjing Medical University, and the written informed consent was received from all patients. A total of 91 patients with HLDH admitted in our hospital from March 2014 to December 2019 were enrolled in this study. Forty-six patients were treated with PEID and 45 patients were treated with OFD at the orthopedics department, the First Affiliated Hospital of Nanjing Medical University, Nanjing, China. The inclusion criteria were: (1) a herniation that occupy more than fifty percent of the canal cross-sectional area on CT scans and MRI in singlesegment; (2) patients complaining of low back and lower limb pain or numbness and motor weakness due to HLDH; (3) symptoms associated with preoperative MRI and CT scans; (4) invalid conservative treatment for six-weeks; (5) imagological examination showing single-segmental LDH without accompanying thickening and calcification of posterior longitudinal ligament and ligamentum flavum. The exclusion criteria were: (1) patients with surgical contraindication; (2) multiple segments of disc herniation, vertebral infection or tumor; (3) lumbar spondylolisthesis, obvious degenerative deformities, instability, and scoliosis; (4) substantial diseases of important organs (5) patients who were lost to follow-up.
Percutaneous Endoscopic Interlaminar Discectomy (PEID)
PEID was performed under general anesthesia with the patient in the prone position, lying on a C-arm fluoroscopic table to make abdomen suspense freely. A pillow was placed between the lower abdomen and chest. The hip and knee joints are flexed to allow the interlaminar window to widen. The skin entry point was confirmed with the assistance of anterior-posterior fluoroscopy. A puncture needle was inserted to the lateral margin of the interlaminar window, subsequently replaced by an 18G guide wire. A 0.7cm incision at puncture needle entrance was made, then the tapered trocar obturator is passed through the guidewire until its tip reaches the upper border of the inferior vertebral body. By using fluoroscopic guidance, the position of obturator and guide wire were identified properly. After removal of obturator and guide wire, the working cannula, through which the endoscope with the working channel and irrigation systems was inserted. Firstly, by using trephine and Kerrison rongeur, the part of lamina and the medial edge of the facet joint usually were removed to achieve bone decompression. Then, the ligamentum flavum was resected to expose the edge of the dural sac and the nerve root. Up until this point, the dorsal decompression of the dural sac was basically completed, which could allow enough space to avoid further damage to the dural sac as the working trocar entered the spinal canal. Nucleus pulposus forceps were used for removal of disc fragments through the nerve root shoulder or nerve root axillary. The dural sac and lumbar-exiting nerve root being freely movable were observed, indicating complete decompression. Finally, the working cannula was carefully removed, and skin incision was sutured with a single suture.
Open Fenestration Discectomy (OFD)
OFD was performed under general anesthesia with the patient in the prone position. After regular disinfection and spreading towels, a 4 cm longitudinal median skin incision was made, then sacrospinal muscles were split to fully expose vertebral plate and zygapophyseal joint on surgical site. By using Kerrison rongeur, vertebral plate and inferior articular process were partially removed to fully expose herniated disc and nerve roots. After herniated intervertebral disc tissues were exposed, herniated nucleus pulposus and residual diseased tissues in intervertebral disc were removed. Confirming that the nerve root was completely loosened and nerve root canal stenosis was not observed, a drainage tube was indwelled and the incision was sutured layer by layer to conclude the surgery.
Postoperative Care
The patients were monitored for six hours, during which they were encouraged to perform ankle pumps exercises in bed. Then, patients in PEID group were allowed to ambulate under a flexible back brace protection, while the OFD group required bed rest until the drainage tube was removed. After discharge, the brace supported the patient for four weeks. During the period, sitting for a long time and bending to lift heavy objects were not recommended, while resuming their daily routine was encouraged.
Evaluation Metrics
All patients were followed-up by telephone or outpatient interviews for at least 24 months. Clinical data included age, gender, operation level, and clinical manifestation, while perioperative parameters such as operative time and length of hospital stay were collected. All patients had an MRI at three months postoperatively to evaluate the resection completeness of disc pulposus fragments (Figures 1 and 2). The complications including recurrent disc herniation were documented and managed during hospital stay and the follow-up period. Visual analogu scale (VAS), modified Japanese Orthopedic Association (mJOA) score, and ODI (Oswestry disability index questionnaire) were applied to evaluate the preoperative condition as well as the curative effectiveness at 3, 6, 12, and 24months postoperatively. Modified Macnab criteria were applied at the final follow-up. The Macnab criteria were categorized as follows: excellent—being able to do all activities, with no pain or restriction; good—occasional pain with relief of symptoms and return to work with some modification; fair—improved function but intermittency of pain influenced the patients’ daily life and work; and poor—no relief or aggravation of symptoms, unable to return to work.18 The excellent and good rates were defined as clinically satisfactory.
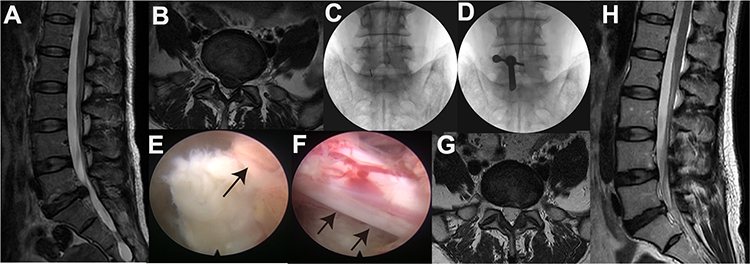 |
Figure 1 A 47-year-old woman suffering from radiating pain in the left leg treated with PEID. Preoperative sagittal (A) and axial (B) MRI showing huge disc herniation at the L5/S1 level. (C and D) the placement of the puncture needle and the working cannula in intraoperative AP fluoroscopic image. (E) fully exposure of herniated disc under endoscope. Black arrow indicated herniated disc. (F) nerve root being freely movable after herniated disc fragments resected under endoscope. Black arrows indicated nerve root. Postoperative three-month sagittal (G) and axial (H) MRI showing no obvious compression of dural sac and nerve root. Preoperation vs postoperative three months, ODI: 62.2 vs 24.44 VAS: 8 vs 3; mJOA: 8 vs 15. |
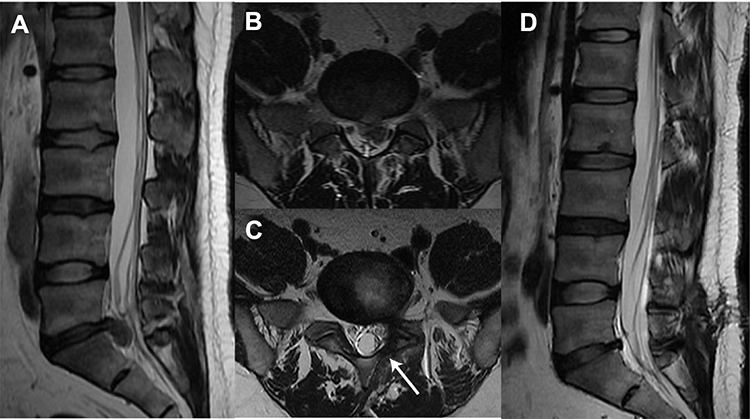 |
Figure 2 A 30-year-old man suffering from radiating pain in the left leg treated with OFD. Preoperative sagittal (A) and axial (B) MRI showing huge disc herniation at the L5/S1 level. Postoperative three-month sagittal (C) and axial (D) MRI showing no obvious compression of dural sac and nerve root. Preoperation vs postoperative three months; white arrow indicates partially removal of lamina; ODI: 62.22 vs 17.78; VAS: 8 vs 2; mJOA: 7 vs 16. |
Statistical Analysis
The measurement data distribution fitted with a Gaussian representation were evaluated using a Shapiro–Wilk Normality test. The data obeyed normal distribution were presented as mean ±standard deviation (SD) and those not obeyed normal distribution were presented as median and range. Enumeration data were expressed as number of cases or percentages. Paired t-test was used for comparison of the VAS, mJOA and ODI score between different periods in the same group when the difference between the two groups is normally distributed. Wilcoxon matched-pairs signed rank test was used for comparison of the VAS score and ODI score between different periods in the same group when the difference between the two groups is normally distributed. Enumeration data were analyzed between two groups by using the chi-squared test or Fisher’s exact probability method. Student’s t-test was used for comparison of the VAS, mJOA and ODI score between two groups in the same period when the data of the two groups is normally distributed. Mann–Whitney U-test was used for comparison of the VAS, mJOA and ODI score between two groups in the same period when at least the data of the one group is not normally distributed. GraphPad Prism Software (version 8.0.0, USA) was used for presenting all graphs and statistical analysis; P<0.05 was considered to indicate a statistically significant difference.
Results
Sociodemographic and Clinical Characteristics of the Patients
A total of 91 patients were included in the study, of which 45 were in the OFD group and 46 in the PEID group. As shown in Table 1, no statistical differences were observed in sociodemographic and clinical characteristics including age, gender, BMI and herniated segment between the two groups.
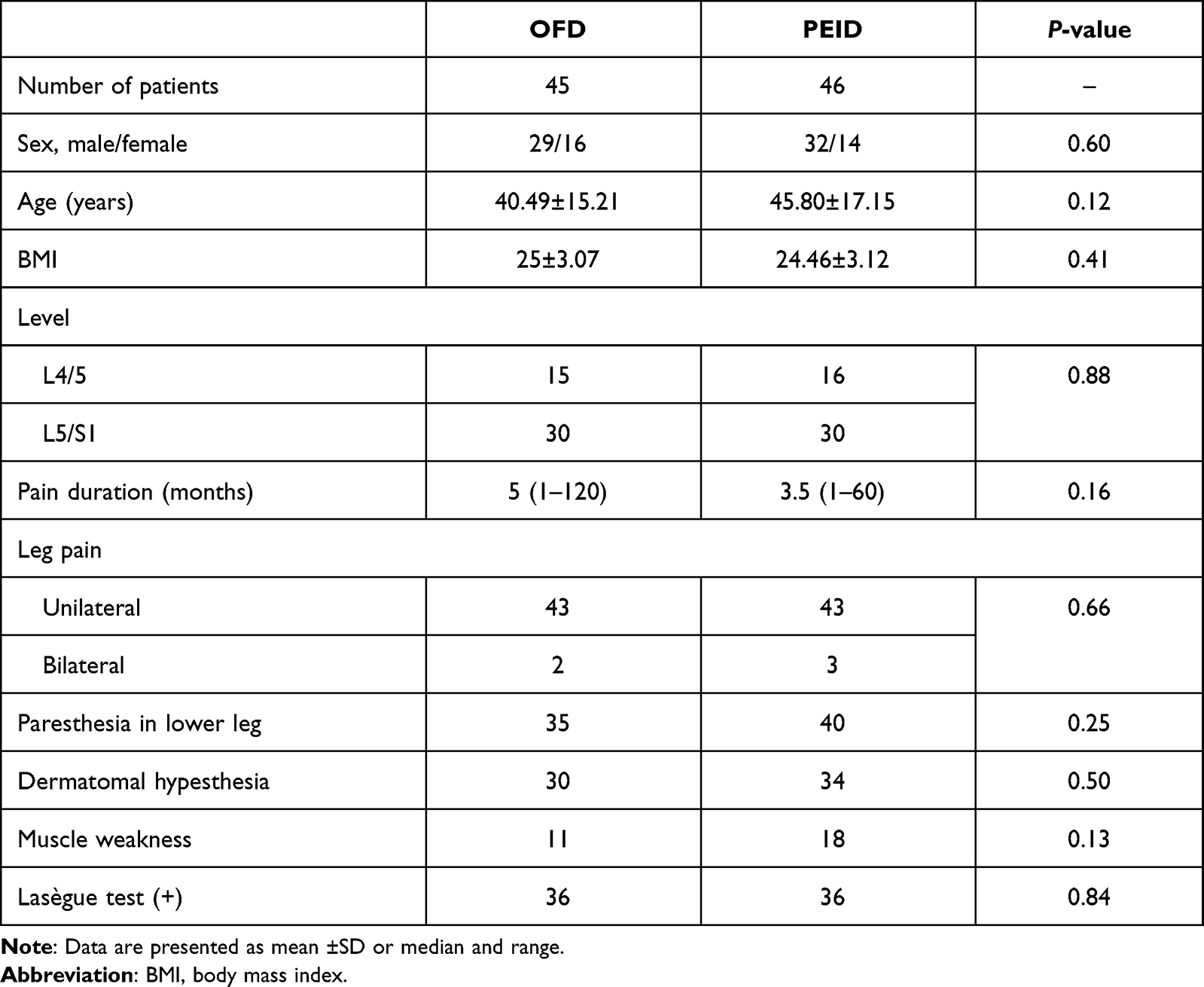 |
Table 1 Comparison of Sociodemographic and Clinical Characteristics Between OFD and PEID Groups |
Clinical Outcomes
As shown in Figure 3, In the OFD group, the median value of VAS for back and leg pain at preoperation and postoperative 3, 6, 12, and 24months was 7 (range: 6–9), 3 (range: 1–5), 2 (range: 1–4), 2 (range: 1–5), and 2 (range: 1–5), respectively. The median value of mJOA score at preoperation and postoperative 3, 6, 12, and 24-months were 9 (range: 6–13), 15 (range: 11–20), 16 (range: 12–20), 17 (range: 11–20), and 16 (range: 10–20), respectively. The median value of ODI score at preoperation and postoperative 3, 6, 12, and 24months were 60 (range: 40–71.11), 17.78 (range: 11.11–37.78), 17.78 (range: 11.11–37.78), 15.56 (range: 11.11–51.11), and 17.78 (range: 11.11–28.89), respectively. The VAS and ODI scores at 3, 6, 12, and 24months postoperatively showed a significant decrease and the mJOA score at 3, 6, 12, and 24months postoperatively showed a significant increase compared to preoperative results (P<0.001). Macnab criteria at the final follow-up were excellent in 32 patients (71.11%), good in seven (15.56%), fair in four (8.89%) and poor in two (4.44%). The overall clinically satisfactory rate was 86.67%.
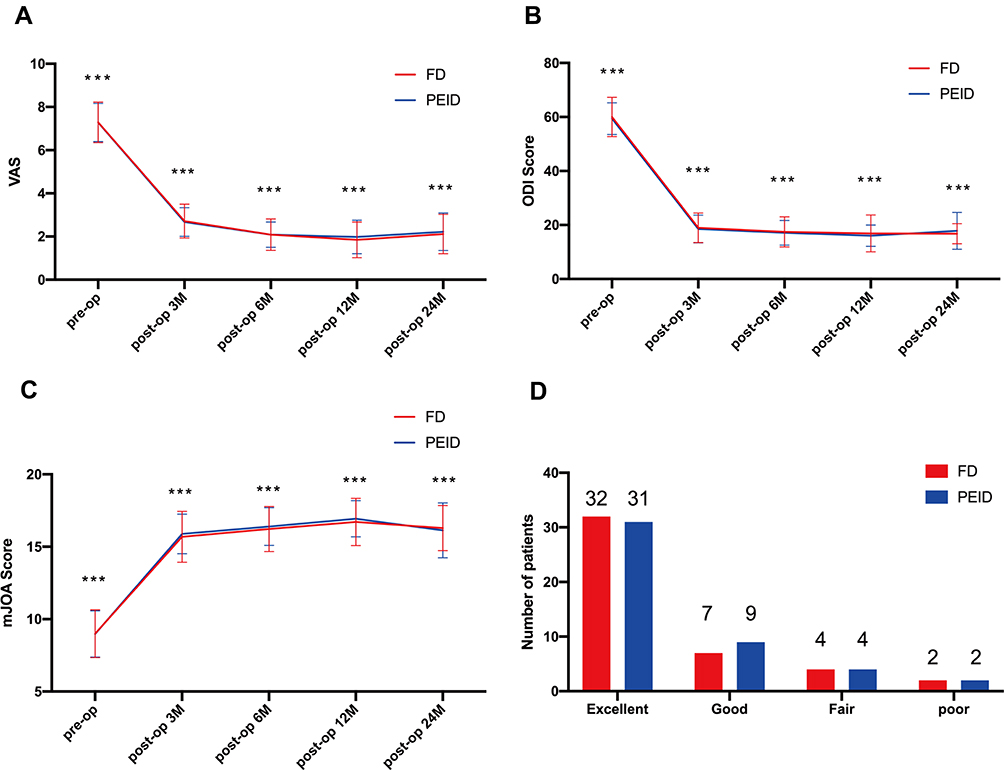 |
Figure 3 Comparison of pre- and postoperative clinical outcomes in OFD and PEID group. (A) Visual analog scale, (B) modified Japanese Orthopedic Association Score, and (C) Oswestry disability index were evaluated in the OFD and PEID group preoperation and postoperatively at 3, 6, 12, and 24 months. (D) At the final follow-up visit (at least postoperatively 24-month), the modified Macnab criteria were utilized to assess clinical effects. *P<0.001, compared with preoperation results in OFD group; #P<0.001, compared with preoperation results in PEID group. |
In the PEID group, the median value of VAS for back and leg pain at preoperation and postoperative 3, 6, 12, and 24 months was 7 (range: 6–9), 3 (range: 2–4), 2 (range: 1–3), 2 (range: 1–4), and 2 (range: 1–5), respectively. The median value of mJOA score at preoperation and postoperative 3, 6, 12, and 24 months were 9 (range: 6–13), 16 (range: 12–18), 17 (range: 12–19), 17 (range: 13–20), and 16 (range: 9–20), respectively. The median value of ODI score at preoperation and postoperative 3, 6, 12, and 24 months were 60 (range: 44.44–71.11), 17.78 (range: 11.11–35.56), 15.56 (range: 11.11–35.56), 15.56 (range: 11.11–35.56), and 15.56 (range: 11.11–44.44), respectively. The VAS and ODI scores at 3, 6, 12, and 24 months postoperatively showed a significant decrease and the mJOA score at 3, 6, 12, and 24 months postoperatively showed a significant increase compared to preoperative results (P<0.001). Macnab criteria at the final follow-up were excellent in 31 patients (67.39%), good in nine (19.57%), fair in four (8.7%) and poor in two (4.35%). The overall clinically satisfactory rate was 86.96%.
There were no significant differences in VAS, ODI and mJOA scores between the two groups at preoperation and postoperatively at 3, 6, 12 and 24 months, respectively.
As shown in Table 2, complications such as nerve root damage, dural tear and cerebrospinal fluid leakage, intraoperative vascular injury were not observed. Four patients (8.89%) in the OFD group and five patients (6.52%) in the PEID group underwent transient lower limb numbness. The symptoms relieved within three months postoperatively after conservative treatment. One patient (10.87%) in the OFD group underwent intervertebral infection at six days postoperatively, subsequently treated with antibiotics and was healing well at 23 days postoperatively. In addition, two patients (4.44%) in the OFD group had a recurrence at 14 months postoperatively, which obtained relief after conservative treatment. Three patients (6.52%) in the PEID group had been diagnosed with recurrent disc herniation at the final follow-up. One patient had received conservative treatment; one patient had been treated with PEID and one patient had been treated with lumbar decompression and fusion with internal fixation. Therefore, there was no significant difference in the total complications between groups (P=0.81).
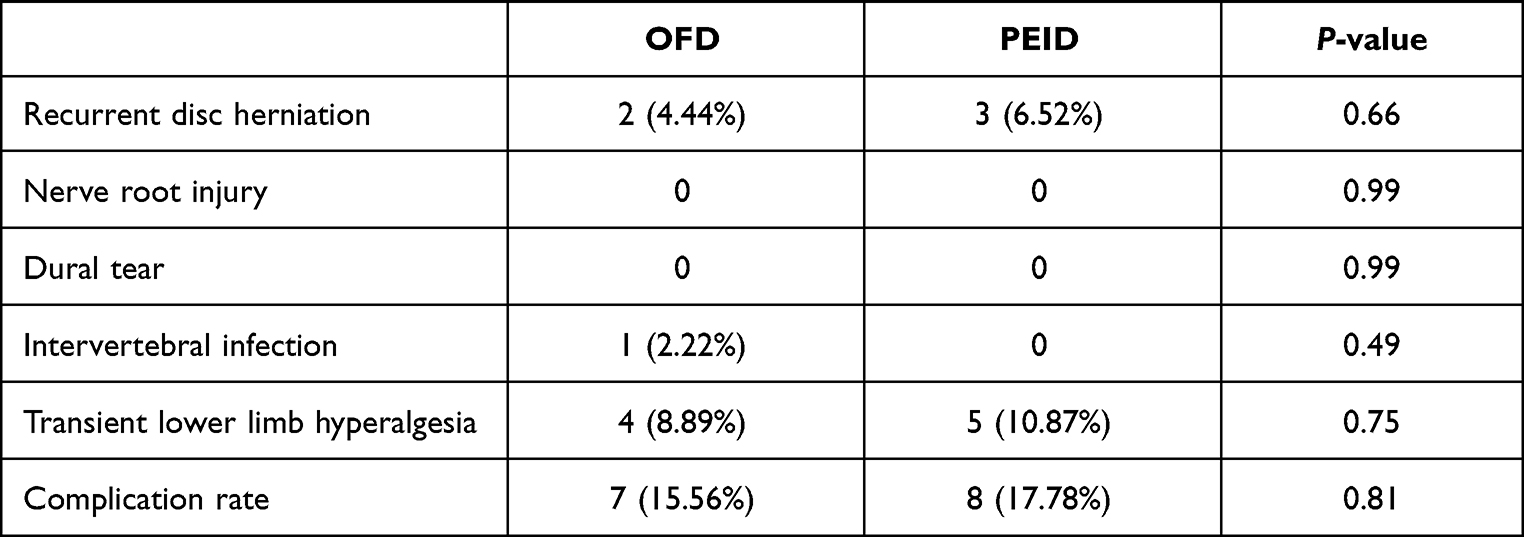 |
Table 2 Complications Collected from OFD and PEID Groups |
As shown in Table 3, In the PEID group, the length of hospitalization and the length of incision was significantly shorter than that in the OFD group (P<0.0001). However, there was no significant difference in operative time between groups (P=0.81).
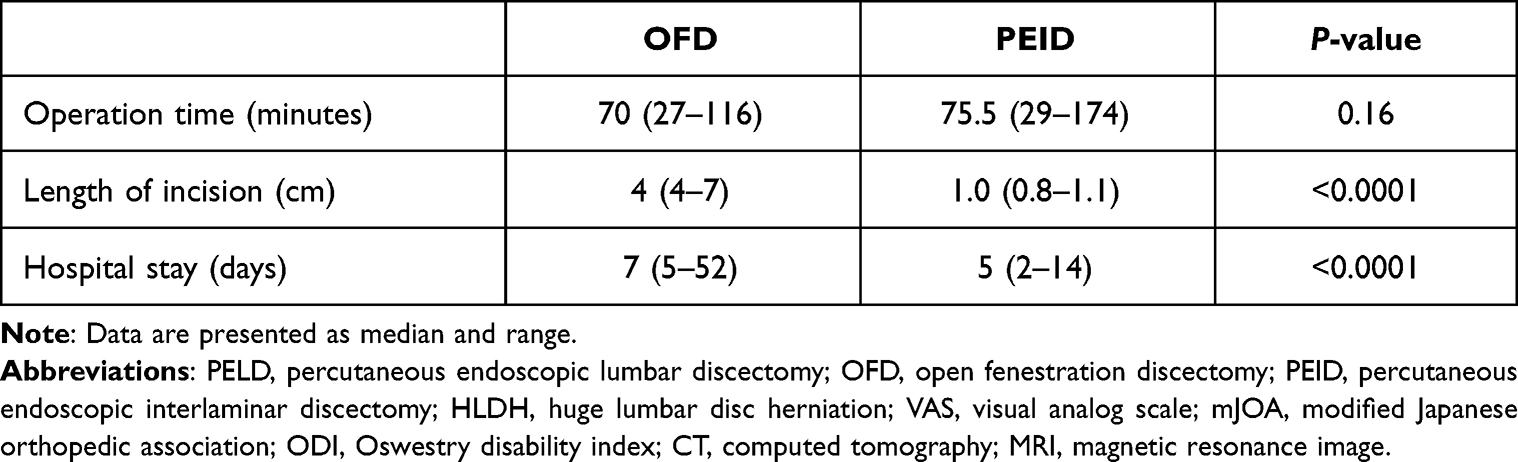 |
Table 3 Comparison of Perioperative Data Between OFD and PEID Groups |
Discussion
LDH is the most common cause of low back and leg pain. Compared with general LDH, more severe low back and leg pain was found in HLDH. However, previous study reported that HLDH might not contribute higher incidence to cauda equina syndrome.4 Existing clinical studies believe that the size and free degree of protruding nucleus pulposus and its contact area with blood circulation are related to the incidence of intervertebral disc resorption.19,20 Although there is a possibility of spontaneous resorption in lumbar disc herniation, its mechanisms remain incompletely understood. Currently, dehydration and inflammation-related resorption are thought to be the possible mechanisms for this event.21 Due to the low incidence of spontaneous resorption in lumbar disc herniation, there are no statistically significant reports, but it is undeniable that spontaneous resorption may occur in huge LDH. As with general LDH, if it is not accompanied by neurological deficits or cauda equina injury manifestations, surgical treatment is not necessary. Patients with huge LDH can also be managed conservatively in the first instance, such as medication, physiotherapy, and other methods.21,22 If conservative treatment is ineffective and accompanied by neurological deficits or manifestations of cauda equina syndrome, surgical treatment is recommended. Surgical approaches include traditional open fenestration discectomy with or without fusion and internal fixation, and the increasingly popular microscopic and endoscopic techniques.
The surgical treatment of HLDH remains controversial, with the main debate being over whether to perform intervertebral fusion and internal fixation. Zhao et al concluded that transforaminal lumbar interbody fusion (TLIF) is an effective treatment option for HLDH.12 Satoh et al noted that posterior lumbar interbody fusion (PLIF) can be used as a surgical treatment for HLDH or segmental instability.23 Moreover, Wang et al and Sharma et al considered PELD to be an effective alternative to nucleus pulposus removal or fusion for HLDH.2,11 The main disadvantages of fusion surgery are the increased incidence of adjacent segment degeneration (ASD), the relatively large trauma and the high-cost burden. In contrast, simple nucleus pulposus removal has the potential for postoperative lumbar instability and recurrence. In previous studies, the criteria for additional fusion internal fixation depended on the presence or absence of concomitant lumbar instability. Due to lumbar instability being a major risk predictor of adverse clinical outcomes in lumbar disc herniation, it was included as one of our exclusion criteria for this study.24 Traditionally, open fenestration discectomy is the gold standard procedure for lumbar disc herniation. In recent years, as the minimally invasive concept is accepted by most doctors and patients and the rapid development of minimally invasive techniques, PELD has gradually become an effective alternative to traditional surgery.
Sharma et al reported good clinical outcomes in 18 patients with HLDH treated with PELD,2 which is consistent with the results in this study. Patients with HLDH who underwent either PEID or OFD could observe a significant reduction in VAS and ODI scores and a significant increase in mJOA scores after surgery, implying good clinical outcomes for both surgical approaches. According to the Macnab criteria, the satisfaction rate for the PEID group was 86.96% and for the OFD group 86.67%. There was no statistical difference between the two groups (P=0.75). In terms of postoperative complications, there were no serious complications such as nerve root injury or dural sac tears in either group. However, five patients in the PEID group and four in the OFD group experienced transient postoperative symptoms of pain or numbness in the lower limbs, which may be related to intraoperative nerve root irritation, and these improved with conservative treatment such as medication and without residual long-term symptoms. In addition, there were three recurrent patients in the PEID group and two recurrences in the OFD group at the subsequent two-year follow-up. The recurrence rates in both groups were lower than those previously reported in the literature for general lumbar disc herniation surgery, which is in line with Akhaddar et al’s findings.5 One patient in the OFD group was readmitted for postoperative infection, whereas no patient in the PEID group developed postoperative lumbar spine infection, probably because the incision of PEID was smaller and the entire operation was done under continuous flushing of saline. In addition, we observed that the length of incision and hospitalization in the PEID group were significant decreased compared with the OFD group. Unlike OFD, the PEID group avoids the extensive dissection of the paravertebral muscles, resulting in less trauma and less intraoperative bleeding. Previously reported literature suggests that the PELD operation time is shorter than open surgery.25,26 Interestingly, in our study, there was no difference in operative time between the two groups. We consider that one possible reason is that PEID requires an additional decompression of the dorsal side of the dural sac, which could effectively avoid further damage to the dural sac by a huge herniated disc. These findings indicate that both PEID and OFD can achieve good clinical outcomes and high patient satisfaction without serious complication, however, compared with OFD, PEID has the following benefits: less trauma, less postoperative pain, shorter hospitalization, and lower postoperative infection rates.
Actually, HLDH poses challenges for surgical operations. It should be noted that the dorsal side of the dural sac needs to be decompressed before the working cannula enters into the spinal canal. If this procedure is omitted, the compression on the dural sac would be more intensified when the working cannula is inserted from the dorsal to ventral side of the dural sac, due to the huge disc herniation located on the ventral side of the dural sac with compression on the dural sac. This may lead to severe nerve root or cauda equina damage. In addition, some patients may have low back pain after PEID. One of the reasons is that incision of the ligamentum flavum may cause epidural adhesion or inflammation.27 Kim pointed out that muscle damage and fibrosis behind the lumbar are the main causes of pain after spinal surgery.28 However, using the posterior approach, PEID inevitably caused damage to the multifidus muscles, which could lead to muscle fibrosis and adhesions. Other possible causes include the loss of intervertebral height, disc degeneration, and destruction of the facet joint.29,30
Some limitations in the current study were identified. Firstly, this was a retrospective study; therefore, there may be confounding factors that could have affected the results. In addition, the follow-up duration of our study was relatively short and the sample size was small. Future prospective studies with large sample sizes and long-term follow-up are needed to confirm our findings. Finally, it is important to note that PEID for HLDH is a difficult procedure and needs to be performed by an experienced surgeon to avoid additional damage from incorrect surgical procedures.
Conclusion
Collectively, postoperative clinical results were equally favorable for both procedures, with no statistically significant difference between PEID and OFD at the two-year of follow up. No serious complication was observed in two groups. Compared with the traditional surgery, PEID has the following benefits: less trauma, less bleeding, speedy recovery, and shorter hospitalization. Therefore, PEID may be a promising alternative to traditional surgery.
Acknowledgments
Special thanks to Dr Qirui Ding, Dr Qi Chen, Dr Zhi Li, Dr Hui Che, Dr You Li, Dr Huan Liu, and Dr Yimin Li for all their help. These authors contributed equally to this work and should be considered co-first authors: Cheng Ma and He Li.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chen Z, Zhang L, Dong J, et al. Percutaneous transforaminal endoscopic discectomy versus microendoscopic discectomy for lumbar disc herniation: two-year results of a randomized controlled trial. Spine. 2020;45(8):493–503. doi:10.1097/BRS.0000000000003314
2. Sharma SB, Lin GX, Jabri H, et al. Radiographic and clinical outcomes of huge lumbar disc herniations treated by transforaminal endoscopic discectomy. Clin Neurol Neurosurg. 2019;185:105485. doi:10.1016/j.clineuro.2019.105485
3. Gao X, Tang K, Xia Y, et al. Efficacy analysis of percutaneous endoscopic lumbar discectomy combined with PEEK rods for giant lumbar disc herniation: a randomized controlled study. Pain Res Manag. 2020;2020:3401605. doi:10.1155/2020/3401605
4. Jeon CH, Chung NS, Son KH, Lee HS. Massive lumbar disc herniation with complete dural sac stenosis. Indian J Orthop. 2013;47(3):244–249. doi:10.4103/0019-5413.111505
5. Akhaddar A, Belfquih H, Salami M, Boucetta M. Surgical management of giant lumbar disc herniation: analysis of 154 patients over a decade. Neurochirurgie. 2014;60(5):244–248. doi:10.1016/j.neuchi.2014.02.012
6. Lurie JD, Tosteson TD, Tosteson AN, et al. Surgical versus nonoperative treatment for lumbar disc herniation: eight-year results for the spine patient outcomes research trial. Spine. 2014;39(1):3–16. doi:10.1097/BRS.0000000000000088
7. Weinstein JN, Tosteson TD, Lurie JD, et al. Surgical vs nonoperative treatment for lumbar disk herniation: the Spine Patient Outcomes Research Trial (SPORT): a randomized trial. JAMA. 2006;296(20):2441–2450. doi:10.1001/jama.296.20.2441
8. Weinstein JN, Lurie JD, Tosteson TD, et al. Surgical versus nonoperative treatment for lumbar disc herniation: four-year results for the Spine Patient Outcomes Research Trial (SPORT). Spine. 2008;33(25):2789–2800. doi:10.1097/BRS.0b013e31818ed8f4
9. Liu C, Zhou Y. Percutaneous endoscopic lumbar discectomy and minimally invasive transforaminal lumbar interbody fusion for massive lumbar disc herniation. Clin Neurol Neurosurg. 2019;176:19–24. doi:10.1016/j.clineuro.2018.10.017
10. Shetty A, Craig PRS, Chitgopkar SD, Chitgopkar SD. An observation of massive lumbar disc prolapse. J Spine Surg. 2018;4(3):583–587. doi:10.21037/jss.2018.07.12
11. Wang Y, Yan Y, Yang J, et al. Outcomes of percutaneous endoscopic trans-articular discectomy for huge central or paracentral lumbar disc herniation. Int Orthop. 2019;43(4):939–945. doi:10.1007/s00264-018-4210-6
12. Zhao CQ, Ding W, Zhang K, Zhao J. Transforaminal lumbar interbody fusion using one diagonal fusion cage with unilateral pedicle screw fixation for treatment of massive lumbar disc herniation. Indian J Orthop. 2016;50(5):473–478. doi:10.4103/0019-5413.189595
13. Schoenfeld AJ. Historical contributions from the Harvard system to adult spine surgery. Spine. 2011;36(22):E1477–84. doi:10.1097/BRS.0b013e3181f2d52c
14. Xu Z, Liu Y, Chen J. Percutaneous endoscopic interlaminar discectomy for L5-S1 adolescent lumbar disc herniation. Turk Neurosurg. 2018;28(6):923–928. doi:10.5137/1019-5149.JTN.21579-17.3
15. Pan M, Li Q, Li S, et al. Percutaneous endoscopic lumbar discectomy: indications and complications. Pain Physician. 2020;23(1):49–56.
16. Li Q, Zhou Y. Comparison of conventional fenestration discectomy with Transforaminal endoscopic lumbar discectomy for treating lumbar disc herniation:minimum 2-year long-term follow-up in 1100 patients. BMC Musculoskelet Disord. 2020;21(1):628. doi:10.1186/s12891-020-03652-0
17. Yan TZ, Lyu CL, Wei YC, Niu SZ, Sun GQ. [Comparision of surgical outcomes between percutaneous endoscopic interlaminar discectomy and fenestration discectomy for L(5)S(1) lumbar disc herniation]. Zhongguo Gu Shang. 2019;32(10):933–936. Chinese. doi:10.3969/j.issn.1003-0034.2019.10.012
18. Macnab I. Negative disc exploration. An analysis of the causes of nerve-root involvement in sixty-eight patients. J Bone Joint Surg Am. 1971;53(5):891–903. doi:10.2106/00004623-197153050-00004
19. Autio RA, Karppinen J, Niinimaki J, et al. Determinants of spontaneous resorption of intervertebral disc herniations. Spine. 2006;31(11):1247–1252. doi:10.1097/01.brs.0000217681.83524.4a
20. Ahn SH, Ahn MW, Byun WM. Effect of the transligamentous extension of lumbar disc herniations on their regression and the clinical outcome of sciatica. Spine. 2000;25(4):475–480. doi:10.1097/00007632-200002150-00014
21. Orief T, Orz Y, Attia W, Almusrea K. Spontaneous resorption of sequestrated intervertebral disc herniation. World Neurosurg. 2012;77(1):146–152. doi:10.1016/j.wneu.2011.04.021
22. Oktay K, Ozsoy KM, Dere UA, et al. Spontaneous regression of lumbar disc herniations: a retrospective analysis of 5 patients. Niger J Clin Pract. 2019;22(12):1785–1789. doi:10.4103/njcp.njcp_437_18
23. Satoh I, Yonenobu K, Hosono N, Ohwada T, Fuji T, Yoshikawa H. Indication of posterior lumbar interbody fusion for lumbar disc herniation. J Spinal Disord Tech. 2006;19(2):104–108. doi:10.1097/01.bsd.0000180991.98751.95
24. Brooks M, Dower A, Abdul Jalil MF, Kohan S. Radiological predictors of recurrent lumbar disc herniation: a systematic review and meta-analysis. J Neurosurg Spine. 2020;1–11. doi:10.3171/2020.6.SPINE20598
25. Kim M, Lee S, Kim HS, Park S, Shim SY, Lim DJ. A comparison of percutaneous endoscopic lumbar discectomy and open lumbar microdiscectomy for lumbar disc herniation in the Korean: a meta-analysis. Biomed Res Int. 2018;2018:9073460. doi:10.1155/2018/9073460
26. Yu H, Zhu B, Liu X. Comparison of percutaneous endoscopic lumbar discectomy and open lumbar discectomy in the treatment of adolescent lumbar disc herniation: a retrospective analysis. World Neurosurg. 2021;151:e911–e7. doi:10.1016/j.wneu.2021.05.007
27. Yan Y, Zhu M, Cao X, et al. Different approaches to percutaneous endoscopic lumbar discectomy for L5/S1 lumbar disc herniation: a retrospective study. Br J Neurosurg. 2020;1–7. doi:10.1080/02688697.2020.1861218
28. Kim CW. Scientific basis of minimally invasive spine surgery: prevention of multifidus muscle injury during posterior lumbar surgery. Spine. 2010;35(26 Suppl):S281–6. doi:10.1097/BRS.0b013e3182022d32
29. Barth M, Diepers M, Weiss C, Thome C. Two-year outcome after lumbar microdiscectomy versus microscopic sequestrectomy: part 2: radiographic evaluation and correlation with clinical outcome. Spine. 2008;33(3):273–279. doi:10.1097/BRS.0b013e31816201a6
30. Yorimitsu E, Chiba K, Toyama Y, Hirabayashi K. Long-term outcomes of standard discectomy for lumbar disc herniation: a follow-up study of more than 10 years. Spine. 2001;26(6):652–657. doi:10.1097/00007632-200103150-00019
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.