Back to Journals » International Journal of General Medicine » Volume 15
Comparison of Percutaneous Endoscopic Cervical Keyhole Foraminotomy versus Microscopic Anterior Cervical Discectomy and Fusion for Single Level Unilateral Cervical Radiculopathy
Authors Ma W, Peng Y, Zhang S ![]() , Wang Y, Gan K
, Wang Y, Gan K ![]() , Zhao X, Xu D
, Zhao X, Xu D ![]()
Received 27 June 2022
Accepted for publication 22 August 2022
Published 29 August 2022 Volume 2022:15 Pages 6897—6907
DOI https://doi.org/10.2147/IJGM.S378837
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Weihu Ma,1 Yujie Peng,2 Song Zhang,2 Yulong Wang,2 Kaifeng Gan,3 Xuchen Zhao,2 Dingli Xu2
1Orthopedic Department, Ningbo No.6 Hospital, Zhejiang, Ningbo, People’s Republic of China; 2Clinical Medical Department, Medical School of Ningbo University Zhejiang, Ningbo, People’s Republic of China; 3Orthopedic Department, The Affiliated Lihuili Hospital of Ningbo University, Ningbo, People’s Republic of China
Correspondence: Dingli Xu, Email [email protected]
Objective: To compare the clinical and radiological outcomes between microscopic anterior cervical discectomy and fusion (ACDF) and percutaneous endoscopic cervical keyhole foraminotomy (PECF) for single level unilateral cervical radiculopathy.
Methods: A total of 127 patients (59 in PECF VS 68 in ACDF) were enrolled in this study from April 2016 to May 2018 with a minimum follow-up of 2 years. Clinical data including baseline data, Neck Disability Index (NDI), and Visual Analogue Scale for neck and arm (VAS-n, VAS-a) were collected and compared. Radiological evaluation such as disc height, ROM of cervical, Cobb’s angle of cervical and Cobb’s angle of operated segment was measured by two experienced radiologists in twice.
Results: There was no significant difference between the two groups in the baseline data, and hospital stay was significantly decreased in PECF group than ACDF group (P < 0.001). PECF group did not yield superior better outcomes in NDI, VAS-a and VAS-n than ACDF group except at 1-month follow-up. As for radiological outcomes, PECF group has significantly better cervical motion, cervical angle and segmental angle than ADCF group at 12- and 24-month follow-up visit (P < 0.05); however, ACDF had shown better disc height restoration and maintenance than PECF (P < 0.05). More complications including surface hematoma and swallowing difficulty were occurred in ADCF group.
Conclusion: Percutaneous endoscopic cervical keyhole foraminotomy could be the alternative method for anterior cervical discectomy and fusion in selective cases. However, the indication should be fulfilled, more studies need to be conducted to further testify the efficacy of PECF.
Keywords: unilateral cervical radiculopathy, percutaneous endoscope cervical keyhole foraminotomy, microscopic anterior cervical discectomy and fusion
Introduction
Cervical radiculopathy has become a common clinical scenario and it increases the burden on healthcare centers.1 Intervertebral foramen stenosis caused by cervical degenerative changes such as lateral disc herniation and osteophyte will incur neurothlipsis. As a consequence, the sensory and motion function and muscle reflection will degrade in the upper extremity. Surgical treatments are needed to reduce the neurothlipsis and relieve the pain. Conservative treatments including pharmacotherapy (nonsteroidal anti-inflammatory drugs, muscle relaxants and steroid injections), traction therapy, physical therapy and manipulative therapy are useful for pain relief but may not impede degenerative changes. Surgical treatments can achieve complete decompression and maintain cervical alignment and are superior to conservative treatments. Anterior cervical discectomy and fusion (ACDF) was firstly proposed by Smith and Robinson in 1958 and was regarded as an effective operation by many researchers.2–4
Although ACDF is one of the safest and most commonly performed spine operations, its defects and complications have been extensively reported in the last decades. Morishita et al found that respiratory difficulty, pneumonia and dysphagia occurred in patients treated with ACDF.5 Hironen et al reported that young adults who underwent ACDF are susceptible to accelerated degeneration in the adjacent cervical disc, leading to adjacent segment diseases.6 Pseudoarthrosis, hardware failure and anterior approach-related complications were also reported.7 Microscope-assisted ACDF was proposed to decrease the intraoperative complications, including esophagus and tracheal and dural injuries. Yao et al reported that 48 patients treated with microscope-assisted ACDF achieved satisfactory improvement in JOA and VAS with complications occurring in 11.11% of them.8
However, the optimal surgical method for unilateral cervical radiculopathy is still controversial. Kato et al reported that both anterior and posterior approaches show similar neurological recovery and quality of life improvement, whereas, anterior surgery is associated with a higher rate of reoperation.9 Adamson et al reported that among the 100 cases of cervical radiculopathy treated with percutaneous endoscopic cervical foraminotomy (PECF), 97 obtained satisfactory recovery and can return to their daily life.10 Thus, this minimally invasive method attracted increasing interest and was regarded as a feasible procedure. Some researchers reckon that PECF can achieve pain relief while avoiding neck anatomical injury and complications. Shu et al reported that 32 patients undergoing PECF showed satisfying clinical outcomes and concluded that PECF could enable nerve root decompression better than ACDF.11 In the aspect of cost, Mansfield et al reported that the average cost of ACDF is significantly higher than that of minimally invasive posterior cervical foraminotomy ($8192 ± 3155 VS $4230 ± 1719, P < 0.001).12
Studies on the comparison between clinical and radiological outcomes of PECF and microscope-assisted ACDF are rare, and whether PECF can improve clinical recovery and diminish complications has not been deeply analyzed. This paper aims to analyze the therapy efficacy of these two methods and verify (1) whether PECF can provide a better pain-relieving effect and larger cervical range of motion (ROM) for patients with cervical radiculopathy; (2) whether PECF leads to fewer complications; (3) whether patients treated with PECF show better outcomes during follow-up.
Methods and Materials
Patients
All data were collected from medical records. Inclusion criteria: (1) patients over 25 with single-level unilateral cervical radiculopathy (paracentral type); (2) patients that had undergone failed palliative therapy for at least 3 months; (3) patients with minimal 2 years of follow-up visit after the PECF or ADCF treatment. Exclusive criteria: (1) patients with cervical spine surgical history; (2) patients with cervical abnormalities including hemivertebrae, block vertebrae and butterfly vertebrae; (3) patients with other comorbidities such as tumor, rheumatic arthritis and tuberculosis; (4) patients with prolapse or calcification of lumbar intervertebral disc. All cases were regarded as good candidates for these two procedures after two senior spinal surgeons uninvolved in the care of these subjects reviewed their radiology report, medical history and physical examination report. The result of the interrater reliability score was tested by Spearman correlation before collection (rs = 0.829).
All procedures involving human participants were performed in accordance with the ethical standards of the institution and the 1964 Helsinki Declaration, and its later amendments or comparable ethical standards. This study was approved by the Research and Ethics Committee of Ningbo No.6 Hospital. The informed consent was waived, because of retrospective study, and all participants’ information would be stored and used for research anonymously.
Surgical Method
Surgeries in all patients were performed by the chief spine surgeon. The details about surgical procedures were shown as follows:
ACDF Group
The procedure of microscope-assisted ACDF was mainly the same as that described by Schroeder et al.13 Patients took a supine position after general anesthesia, and the incision of the pathological segment has a 2- or 3-finger breadth above the clavicle. Then, pathological segment was confirmed by C-arm after exposure, and the relative anatomical structure was distracted. The osteophytes around the vertebrae, if any, were removed. The intervertebral disc and cartilaginous endplate were completely removed with a microscope. Herniated disc and nerve root were completely decompressed without causing dura injury. Next, intervertebral cages (VENTURE, Medtronic, Minnesota, USA), plates and screws (VENTURE, Medtronic, Minnesota, USA) were inserted for fixation and fusion. A drain was placed, and it was removed after 24 h.
PECF Group
The procedure of PECF was similar to that in papers.10,14 Firstly, patients took a prone position with a mattress under their forehead, chest and abdomen after general anesthesia. The entry point was marked by intraoperative C-arm, which is located on the superior border of the inferior lamina of the pathologic segment near the medial of the facet joint on the herniated side. All of the instruments were included in the cervical foraminal system (Joimax, Germany). An 18-gauge puncture needle was inserted and was pushed through the marked point until reaching the inferior lamina with the assistance of the C-arm. An incision around 8 mm was made above the V-point (the medial junction of the inferior and superior facet joint), then the guidewire was placed, and the needle was withdrawn. The 6.9-mm obturator, 8.0-mm oblique working channel and 4.1-mm endoscope were set sequentially with continuous saline solution irrigation. After the identification of the V-point, the overlying soft tissue was removed with endoscopic forceps. After the bone structure was exposed, the lower margin of the superior lamina was drilled laterally toward the facet joint and caudally to the pedicle. Then, the intersection of the ascending facet with the inferior laminae was drilled with a radius around half of the facet length.15 The ligamentum flavum and foraminal ligament were removed so that the probe could be easily inserted into the foramen and the dural sac and outgoing nerve were visible. The protruding nucleus pulposus, which is usually beneath the nerve root, was located, and it was resected by tissue forceps. Before removing the working channel, it was confirmed that the nerve root was completely decompressed (Figure 1).
 |
Figure 1 A 46-year-old female who suffered from C6/7 unilateral cervical radiculopathy and treated with percutaneous endoscopic cervical foraminotomy. (A) Preoperative MRI showed C6/7 disc herniation (Left site). (B) and (C) The CT and MRI of three days after operation, showing completely decompression of dura and nerve root. (D) The 3D reconstruction image shown keyhole technique. |
Rehabilitation Principle
Postoperative rehabilitation was the same in the two groups. Three days after the operation, limb exercise was started with the assistance of a neck collar (maintaining cervical stability), and the neck collar was used for 4 weeks. All patients were asked to go back to hospital 1, 6, 12 and 24 months after the operation for clinical and radiographic outcome assessment. Drugs such as neurotrophic drugs and pain killers were used according to patients’ symptoms.
Outcome Evaluation
The clinical evaluations include hospital stay, perioperative bleeding, complications, neck disability index (NDI), VAS-arm and VAS-neck.16 All data were collected from medical records. Radiological outcomes were measured by two experienced radiologists, and the details were shown as follows: Disc height (DH): the average distance between the adjacent endplate and the pathological segment at anterior, middle, and posterior parts. Segment angle (SA) of the pathological segment was defined as the Cobb angle between the superior endplate of the upper vertebrae and the inferior endplate of the lower vertebrae. Cervical angle (CA) representing the cervical curvature was defined as Cobb angle between C2 and C7 measured using the tangential method17 (Figure 2). ROM of cervical was calculated based on the angles between the parallel lines of C2 and C7 trailing edge in both the extension and flexion lateral radiographs (Figure 3). The complications were also recorded and compared in this study.
 |
Figure 2 The measurement of Segment angle and cervical angel. (A). Segment angle (SA): the Cobb’s angle between inferior endplate of lower vertebrae and superior endplate of upper vertebrae (For example: pathologic segment is C6/7, the SA is the Cobb’s angle between superior endplate of C6 and inferior endplate of C7). (B). Cervical angel (CA): the angle between lines which parallel to the trailing edge of C2 and C7. |
 |
Figure 3 The calculation of ROM of cervical is the sum of angles in extension and flexion lateral X-ray. (A). Angle between the parallel line of C2 and C7 trailing edge in the extension lateral radiograph. (B). Angle between the parallel line of C2 and C7 trailing edge in the flexion lateral radiograph. |
Statistics
All data were expressed as mean ± standard deviations. The statistical analysis was performed by SPSS 24.0 (IBM Corp., Armonk, New York, USA). Shapiro–Wilk (SW) test was used to assess the normality of continuous data. The independent t-test was applied to compare measurement data such as hospital stay, operation time, NDI, VAS-arm and VAS-neck of the two groups. Categorical data including gender, operation level and herniation site were analyzed by χ2 test. The P value smaller than 0.05 was considered to indicate statistical significance. Line charts were designed to intuitively show the difference between the two groups.
Results
Baseline Data
The data of 127 patients with unilateral cervical radiculopathy who were treated with PECF or microscope-assisted ADCF were collected from April 2016 to May 2018. In the present study, 68 patients were treated with ACDF (ACDF group) and 59 patients underwent PECF (PECF group). As shown in Table 1, there were no significant differences in gender, age, BMI, duration time, operation segment and pain site between the two groups (P > 0.05). The hospital stay of the PECF group is shorter than that of the ACDF group (3.7 ± 1.3 d VS 6.8 ± 1.5 d, P < 0.001). However, significantly longer operation time was observed in the PECF group (66.8 ± 6.8 mins VS 59.4 ± 9.1mins, P < 0.001).
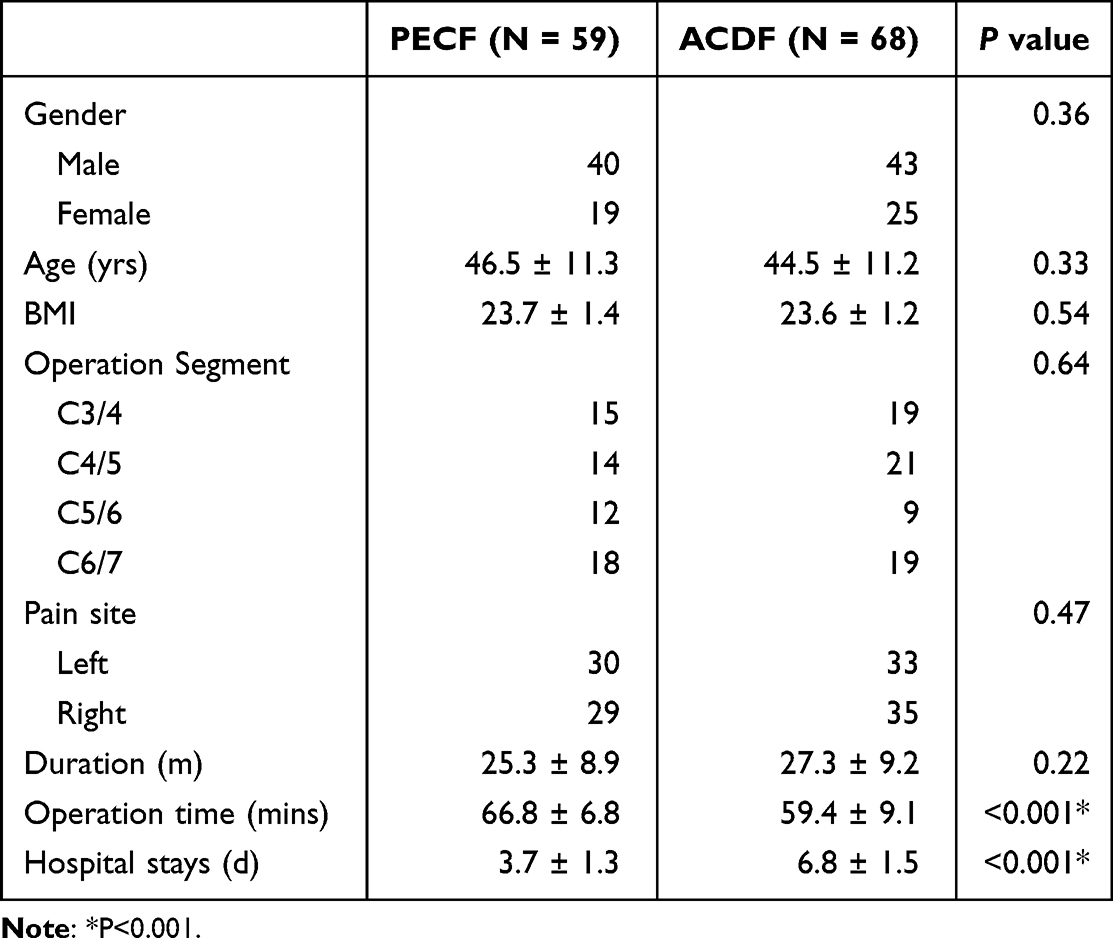 |
Table 1 The Comparison of Baseline Data Between Two Groups |
The Clinical Outcomes
After the operation, the two groups showed satisfactory recovery in clinical outcomes, including NDI, VAS-arm and VAS-neck (P < 0.05). There was no significant difference in these clinical outcomes between the two groups in the 6-, 12- and 24-month follow-up visits, and in the 1-month follow-up visit, the improvement of these outcomes in the PECF group was more significant than that in the ACDF group (P < 0.05). These results reveal that symptoms of cervical radiculopathy were effectively alleviated and the function of patients was improved after the surgery with the two surgical methods, and PECF could achieve better improvement at an early stage (Table 2).
 |
Table 2 The Comparison of Clinical Outcomes Between Two Groups |
The Radiological Outcomes
As shown in Table 3, there was no significant difference in preoperative DH, SA, CA and ROM between the two groups. However, the PECF group shows a better recovery in SA, CA and ROM than the ACDF group in the 12- and 24-month follow-up visits (P < 0.05). The ADCF group shows a larger increase in DH than the PECF group in the 12- and 24-month follow-up visits (P < 0.05). The comparison of these radiological outcomes during the follow-up visit was shown in Figure 4.
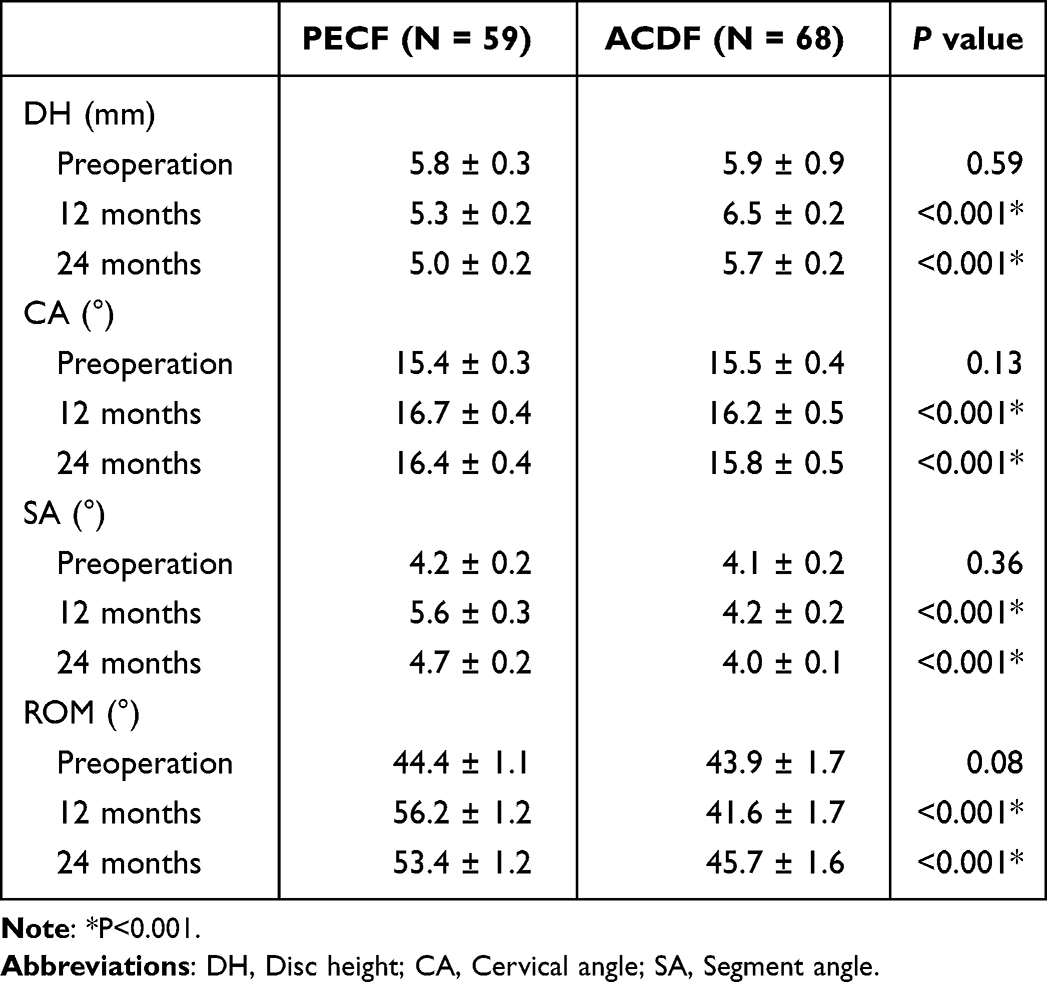 |
Table 3 The Comparison About Radiological Outcomes Between Two Groups |
 |
Figure 4 The radiological outcomes comparison with time between two group. *P<0.05. |
Complications
In the ADCF group, four patients showed superficial surgical site infection and three patients suffered paresthesia. These symptoms were successfully managed by conservative treatment. Adjacent segment degeneration without any symptoms was observed based on radiological data in two patients, and they preferred nonsurgical treatment. One patient had mild motor weakness but was recovered after rehabilitation exercise. MRI showed that one patient had asymptomatic cervical disc herniation recurrence, which was successfully managed with conservative treatment. In the PECF group, one patient had surgical site hematoma and one had asymptomatic dural tear immediately after the operation, and they adopted conservative treatment.
In summary, there were significant differences in the complications between the two groups (P < 0.05).
Discussion
Cervical radiculopathy is a common disease with 85 cases per 100,000 population, and the compression of the nerve root usually results from a sequential degenerative change of intervertebral disc, vertebral body, facet joint and ligaments during the aging process of adults who had cigarette smoking habits and excessive axial load bearing.18,19 Radicular pain and paresthesia in the neck, shoulder and even chest are the most complained symptoms, depending on the involved nerve root and disease duration. In addition, radicular pain will be accentuated if the compressed nerve root is stretched by some cervical motions like sneezing and coughing. The treatment objectives of cervical radiculopathy are immediate pain relief, complete decompression of nerve root and function improvement. ACDF is a widely used operation for cervical radiculopathy. Previous studies reported that after ACDF treatment, patients with cervical radiculopathy achieved gratified neurologic function improvement and pain alleviation. Burkhardt et al conducted a study in which 80 patients with cervical disc herniation who underwent ACDF complained about radicular pain and sensory disturbance, 70 (87.5%) patients were free of radicular pain and 78 patients achieved neurologic function improvement.20 Jenkins reported that 51 patients with Patient Health Questionnaire (PHQ) score <5 who underwent ACDF all showed significant improvement in Short Form-12 Physical Component Score (SF-12 PCS) and NDI during 1-year follow-up (46.5 ± 8.3 and 20 ± 18.4 VS 39.1 ± 9.3 and 25.8 ± 15.8, P < 0.05).21
However, there were multiple complications reported after ACDF. According to the study of Epstein in 2019, anatomical complications including immediate postoperative dysphagia, laryngeal nerve palsy, and even esophagus and tracheal injuries are the most frequently reported complications. Surgery-related complications include surgery site infection, new radicular symptoms, hematoma, adjacent segment degeneration, cerebrospinal fluid leakage and internal fixation failure.22 They are also common, with an occurrence rate of around 6–13.8%. The rare but severe complications are internal jugular venous thrombosis, pseudarthrosis and epidural hematoma.22–24 Wichmann et al conducted a study with 410 patients with cervical radiculopathy and undergoing ACDF treatment. Clinical outcomes such as VAS, NDI and patient-reported outcome measures (PROMs) were significantly improved, the complication rates were 2.4% intraoperatively and 1.2% postoperatively.25 Microscope-assisted ACDF can diminish the rate of esophagus injury and dural injury. However, in the research of Adogwa et al, where 59 patients were treated with microscope-assisted ACDF and 81 underwent ACDF without the use of a microscope, no significant difference in the rate of complication was found.26 In addition, Omidi-Kashani et al reported that patients younger than 45 who underwent microscope-assisted ACDF showed better recovery in NDI than patients older than 45 (10.1 ± 9.5 VS 15.8 ± 4.6, P < 0.05). This result indicates that patients older than 45 benefit more from microscope-assisted ADCF than younger patients.27 As a consequence, PECF was proposed by Roh et al. They performed posterior cervical foraminotomy under an endoscope in four cadavers. After CT scan evaluation, significantly better decompression diameter and facet joint removal percentage were achieved when compared with the traditional open technique.28 Subsequent studies reported gratified outcomes after PECF. Zheng et al reported that among 249 patients with single-level cervical disc herniation treated with PECF, 216 (86.7%) had no or minimal pain, and 33 had occasional pain; in addition, no patient presented adjacent segment degeneration during follow-up.29
In this study, we retrospectively collected and compared the clinical and radiological outcomes of 127 patients (68 in ACDF, 59 in PECF). Significantly longer operation time and shorter hospital stay were found in PECF group (3.7 ± 1.3 d and 66.8 ± 6.8 mins VS 6.8 ± 1.5 d and 59.4 ± 9.1mins, P < 0.001). The reasons could be that the location of the surgical site and installation of the endoscope take time. PECF is a microinvasive, minimally invasive technique which is regarded as one of the ERAS techniques in spine surgery, so the hospital stay was significantly shorter than ACDF.30 As for the clinical outcomes, the two surgical methods both contribute to significant improvement. The PECF group showed significantly better pain relief and a higher NDI score than the ACDF group in 1-month follow-up, but no significant difference was found in other follow-up periods. Some studies showed similar results of neurological function recovery. Lee et al reported that among 76 patients with motor weakness and undergoing PECF, 72 showed significantly recovered neurological function and 65 had a normal neurological function at the end of follow-up.31 Terai et al reported that grip strength on the lesion site was significantly improved (from 30kg to 35kg) in patients after PECF.32 These results indicate that PECF exerts little influence on neck muscle and can verify whether the nerve root is completely decompressed visually. It was reported that the protection of the neck muscle of the cervical spine could better maintain the cervical ROM and reduce axial symptoms,33 which could be a convincible explanation why the PRCF group had significantly better improvement in VAS and NDI.
And there were 10 patients suffered from complication after ACDF and 2 patients in PECF (P < 0.05). Fountas et al reported that overall complication rate was 19.3% (196 of 1015 patients). The most common complication was dysphagia in 9.5% and postoperative hematoma occurred in 5.6%.7 And Zhang et al reported a meta analysis and concluded that complications of patients with PECF were lower than ACDF (P < 0.05).34
Radiological outcomes were also compared in this study. The PECF group achieves more significant recovery in SA, CA and ROM in 12- and 24-month follow-up visits than the ACDF group (P < 0.05). Whereas the ADCF group shows a more significant recovery in DH than the PECF group in 12- and 24-month follow-up visits (P < 0.05). The ROM-related result in this study is consistent with that in the research of Kim et al, who measured the instantaneous axis of rotation (IAR) via extension and flexion cervical X-ray of 11 patients treated with PECF and found that the IAR was significantly improved at the surgical segment, especially at C5/6 and C6/7 (P = 0.02).35 Ke et al found that the range of motion (ROM) of operation level was significantly improved (7.27 ± 1.75° VS 8.48 ± 2.67°, P = 0.02) and the ROM of C2-7 was better, but there was no statistical significance.36 Chen et al performed a finite element study and found that ACDF exerts a remarkable impact on intervertebral disc pressure and ROM of the surgical segment, whereas there was no significant difference in intervertebral disc pressure and ROM after posterior cervical foraminotomy.37
As for DH, Lin reported that DH of the surgical segment of 55 patients treated with ACDF was more significantly increased than that of patients treated with posterior cervical foraminotomy.38 Disc height of surgical segment increases after ACDF mainly because ACDF can provide stronger support on anterior column by hardware fixation. The possible reason why PECF shows better improvements in ROM, CA and SA is that ACDF immobilized the vertebral body by plate and cage, while PECF only removed herniated disc.
Limitations
This study has some limitations. First, this is a study with small sample size and single center, and further prospective study should be conducted for enhancing the credibility of study. Second, the follow-up period of this study was short, and some complications such as reoperation and implementation failure may be observed with longer follow-up visit. Lastly, some life habits, such as smoking and physical exercise which could have an influence on outcomes, cannot be obtained due to retrospective study.
Conclusion
Cervical radiculopathy was always treated with ACDF, but patients may experience a lot of complications and accelerate adjacent segment degeneration. PECF could be an effective alternative method which can achieve better pain relief, neurologic function recovery and ROM of cervical, decreasing hospital stay and complications. However, the disc herniation type needs to pay more attention before operation because PECF is unsuitable for central cervical disc herniation.
Data Sharing Statement
The data that support this study are available within supplement file (raw data.xlsx) and available from the corresponding authors upon request.
Ethical Approval
This study was approved by the Research and Ethics Committee of Ningbo No.6 Hospital. The informed consent was waived, because of retrospective study, and all participants’ information would be stored and used for research anonymously.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Acknowledgment
The study was supported by the Nature Science Foundation of Zhejiang (LY19H060002), National Nature Foundation of China (81572217) and Social Welfare Research Key Project of Ningbo (2021S105). The authors declare no conflicts of interest.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no conflict of interest.
References
1. Thoomes EJ, van Geest S, van der Windt DA, et al. Value of physical tests in diagnosing cervical radiculopathy: a systematic review. Spine J. 2018;18:179–189. doi:10.1016/j.spinee.2017.08.241
2. Smith GW, Robinson RA. The treatment of certain cervical-spine disorders by anterior removal of the intervertebral disc and interbody fusion. J Bone Joint Surg Am. 1958;40-a:607–624. doi:10.2106/00004623-195840030-00009
3. Safaee MM, Nichols NM, Yerneni K, Zhang Y, Riew KD, Tan LA. Safety and efficacy of direct nerve root decompression via anterior cervical discectomy and fusion with uncinectomy for cervical radiculopathy. J Spine Surg. 2020;6:205–209. doi:10.21037/jss.2019.12.04
4. Engquist M, Löfgren H, Öberg B, et al. A 5- to 8-year randomized study on the treatment of cervical radiculopathy: anterior cervical decompression and fusion plus physiotherapy versus physiotherapy alone. J Neurosurg Spine. 2017;26:19–27. doi:10.3171/2016.6.SPINE151427
5. Morishita S, Yoshii T, Inose H, et al. Comparison of perioperative complications in anterior decompression with fusion and posterior decompression with fusion for cervical spondylotic myelopathy: propensity score matching analysis using a nationwide inpatient database. Clin Spine Surg. 2021;34:E425–e31. doi:10.1097/BSD.0000000000001209
6. Hirvonen T, Marjamaa J, Siironen J, Koskinen S, Niemelä M, Koski-Palkén A. Young adults undergoing ACDF surgery exhibit decreased health-related quality of life in the long term in comparison to the general population. Spine J. 2021;21:924–936. doi:10.1016/j.spinee.2021.01.021
7. Fountas KN, Kapsalaki EZ, Nikolakakos LG, et al. Anterior cervical discectomy and fusion associated complications. Spine. 2007;32:2310–2317. doi:10.1097/BRS.0b013e318154c57e
8. Yao Y, Xiong C, Wei T, Yao Z, Zhu F, Xu F. Three-dimensional high-definition exoscope (Kestrel View II) in anterior cervical discectomy and fusion: a valid alternative to operative microscope-assisted surgery. Acta Neurochir. 2021;163:3287–3296. doi:10.1007/s00701-021-04997-8
9. Kato S, Ganau M, Fehlings MG. Surgical decision-making in degenerative cervical myelopathy – anterior versus posterior approach. J Clin Neurosci. 2018;58:7–12. doi:10.1016/j.jocn.2018.08.046
10. Adamson TE. Microendoscopic posterior cervical laminoforaminotomy for unilateral radiculopathy: results of a new technique in 100 cases. J Neurosurg. 2001;95:51–57. doi:10.3171/spi.2001.95.1.0051
11. Shu W, Zhu H, Liu R, et al. Posterior percutaneous endoscopic cervical foraminotomy and discectomy for degenerative cervical radiculopathy using intraoperative O-arm imaging. Wideochirurgia I Inne Techniki Maloinwazyjne. 2019;14:551–559. doi:10.5114/wiitm.2019.88660
12. Mansfield HE, Canar WJ, Gerard CS, O’Toole JE. Single-level anterior cervical discectomy and fusion versus minimally invasive posterior cervical foraminotomy for patients with cervical radiculopathy: a cost analysis. Neurosurg Focus. 2014;37:E9. doi:10.3171/2014.8.FOCUS14373
13. Schroeder GD, Kurd MF, Millhouse PW, Vaccaro AR, Hilibrand AS. Performing an anterior cervical discectomy and fusion. Clin Spine Surg. 2016;29:186–190. doi:10.1097/BSD.0000000000000383
14. Quillo-Olvera J, Lin GX, Kim JS. Percutaneous endoscopic cervical discectomy: a technical review. Ann Transl Med. 2018;6:100. doi:10.21037/atm.2018.02.09
15. Luo RJ, Song Y, Liao ZW, et al. Keyhole foraminotomy via a percutaneous posterior full-endoscopic approach for cervical radiculopathy: an advanced procedure and clinical study. Curr Med Sci. 2020;40:1170–1176. doi:10.1007/s11596-020-2299-5
16. Owen RJ, Khan AZ, McAnany SJ, Peters C, Zebala LP. PROMIS correlation with NDI and VAS measurements of physical function and pain in surgical patients with cervical disc herniations and radiculopathy. J Neurosurg Spine. 2019;1–6. doi:10.3171/2019.4.SPINE18422
17. Li C, Tang X, Chen S, Meng Y, Zhang W. Clinical application of large channel endoscopic decompression in posterior cervical spine disorders. BMC Musculoskelet Disord. 2019;20:548. doi:10.1186/s12891-019-2920-6
18. Roth D, Mukai A, Thomas P, Hudgins TH, Alleva JT. Cervical radiculopathy. DM. 2009;55:737–756. doi:10.1016/j.disamonth.2009.06.004
19. Abbed KM, Coumans JV. Cervical radiculopathy: pathophysiology, presentation, and clinical evaluation. Neurosurgery. 2007;60:S28–34. doi:10.1227/01.NEU.0000249223.51871.C2
20. Burkhardt BW, Brielmaier M, Schwerdtfeger K, Oertel JM. Clinical outcome following anterior cervical discectomy and fusion with and without anterior cervical plating for the treatment of cervical disc herniation – a 25-year follow-up study. Neurosurg Rev. 2018;41:473–482. doi:10.1007/s10143-017-0872-6
21. Jenkins NW, Parrish JM, Yoo JS, et al. Are preoperative PHQ-9 scores predictive of postoperative outcomes following anterior cervical discectomy and fusion? Clin Spine Surg. 2020;33:E486–e92. doi:10.1097/BSD.0000000000000985
22. Epstein NE. A review of complication rates for anterior cervical diskectomy and fusion (ACDF). Surg Neurol Int. 2019;10:100. doi:10.25259/SNI-191-2019
23. Tasiou A, Giannis T, Brotis AG, et al. Anterior cervical spine surgery-associated complications in a retrospective case-control study. J Spine Surg. 2017;3:444–459. doi:10.21037/jss.2017.08.03
24. Wilson LA, Fiasconaro M, Liu J, et al. Trends in comorbidities and complications among patients undergoing inpatient spine surgery. Spine. 2020;45:1299–1308. doi:10.1097/BRS.0000000000003280
25. Wichmann TO, Bech-Azeddine R, Norling AL, Einarsson HB, Rasmussen MM. Comparison of outcomes and complications between one- and two-level anterior cervical discectomy and fusion: a population-based study of 410 patients. Br J Neurosurg. 2021;1–6. doi:10.1080/02688697.2021.2005778
26. Adogwa O, Elsamadicy A, Reiser E, et al. Comparison of surgical outcomes after anterior cervical discectomy and fusion: does the intra-operative use of a microscope improve surgical outcomes. J Spine Surg. 2016;2:25–30. doi:10.21037/jss.2016.01.04
27. Omidi-Kashani F, Ghayem Hasankhani E, Ghandehari R. Impact of age and duration of symptoms on surgical outcome of single-level microscopic anterior cervical discectomy and fusion in the patients with cervical spondylotic radiculopathy. Neurosci J. 2014;2014:808596. doi:10.1155/2014/808596
28. Roh SW, Kim DH, Cardoso AC, Fessler RG. Endoscopic foraminotomy using MED system in cadaveric specimens. Spine. 2000;25:260–264. doi:10.1097/00007632-200001150-00019
29. Zheng C, Huang X, Yu J, Ye X. Posterior percutaneous endoscopic cervical diskectomy: a single-center experience of 252 cases. World Neurosurg. 2018;120:e63–e7. doi:10.1016/j.wneu.2018.07.141
30. Zaed I, Bossi B, Ganau M, Tinterri B, Giordano M, Chibbaro S. Current state of benefits of enhanced recovery after surgery (ERAS) in spinal surgeries: a systematic review of the literature. Neurochirurgie. 2022;68:61–68. doi:10.1016/j.neuchi.2021.04.007
31. Lee U, Kim CH, Chung CK, et al. The recovery of motor strength after posterior percutaneous endoscopic cervical foraminotomy and discectomy. World Neurosurg. 2018;115:e532–e8. doi:10.1016/j.wneu.2018.04.090
32. Terai H, Suzuki A, Toyoda H, et al. Tandem keyhole foraminotomy in the treatment of cervical radiculopathy: retrospective review of 35 cases. J Orthop Surg Res. 2014;9:38. doi:10.1186/1749-799X-9-38
33. Xu D, Gan K, Wang Y, Wang Y, Ma W. Comparison of C2-3 pedicle screw fixation with C2 spinous muscle complex and iliac bone graft for instable hangman fracture. Front Surg. 2021;8:723078. doi:10.3389/fsurg.2021.723078
34. Zhang Y, Ouyang Z, Wang W. Percutaneous endoscopic cervical foraminotomy as a new treatment for cervical radiculopathy: a systematic review and meta-analysis. Medicine. 2020;99:e22744. doi:10.1097/MD.0000000000022744
35. Kim CH, Park TH, Chung CK, Kim KT, Choi YH, Chung SW. Changes in cervical motion after cervical spinal motion preservation surgery. Acta Neurochir. 2018;160:397–404. doi:10.1007/s00701-017-3375-x
36. Ke W, Zhi J, Hua W, et al. Percutaneous posterior full-endoscopic cervical foraminotomy and discectomy: a finite element analysis and radiological assessment. Comput Methods Biomech Biomed Engin. 2020;23:805–814. doi:10.1080/10255842.2020.1765162
37. Chen C, Yuchi CX, Gao Z, et al. Comparative analysis of the biomechanics of the adjacent segments after minimally invasive cervical surgeries versus anterior cervical discectomy and fusion: a finite element study. J Orthop Translat. 2020;23:107–112. doi:10.1016/j.jot.2020.03.006
38. Lin GX, Rui G, Sharma S, Kotheeranurak V, Suen TK, Kim JS. Does the neck pain, function, or range of motion differ after anterior cervical fusion, cervical disc replacement, and posterior cervical foraminotomy? World Neurosurg. 2019;129:e485–e93. doi:10.1016/j.wneu.2019.05.188
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.