Back to Journals » Journal of Pain Research » Volume 18
Comparison of Opioid Consumption During Target Controlled Infusion (TCI) Guided By Nociception Level Index (NOL) or Standard Care Undergoing Intracranial Tumor Surgery
Authors Demirel ME, Bilgin H, Akesen S
Received 19 May 2025
Accepted for publication 27 September 2025
Published 11 October 2025 Volume 2025:18 Pages 5347—5355
DOI https://doi.org/10.2147/JPR.S531931
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Timothy Atkinson
Muhammet Esat Demirel,1,* Hulya Bilgin,2,* Selcan Akesen2
1Department of Anesthesiology, Bursa City Hospital, Bursa, Türkiye; 2Department of Anesthesiology, Bursa Uludağ University Faculty of Medicine, Bursa, Türkiye
*These authors contributed equally to this work
Correspondence: Muhammet Esat Demirel, Email [email protected]
Purpose: This prospective, randomized controlled study aims to compare opioid doses in patients undergoing intracranial tumor surgery managed with Total Intravenous Anesthesia using Target Controlled Infusion (TIVA-TCI) combined with Nociception Level (NOL) monitoring. The NOL index, an artificial intelligence–driven multiparameter index, integrates physiological signals such as heart rate, skin conductance, and photoplethysmography to provide an objective measure of nociception and guide personalized opioid administration. Additionally, the study evaluates the consumption of hypnotic drugs, hemodynamic parameters, variability in the NOL index, and changes in Heart Rate (HR) in the study group patients who received NOL monitoring following severe noxious stimuli.
Patients and Methods: The study involved 50 ASA II–III patients undergoing intracranial tumor surgery, with 25 in the standard care guided group and 25 in the NOL guided group. The control group received standard monitoring while NOL monitoring added in the study group. Propofol and remifentanil were titrated to maintain hemodynamic parameters or NOL values. Hemodynamic parameters, propofol and remifentanil doses were recorded and compared between groups. NOL index changes before and after noxious stimuli were compared with HR changes.
Results: No significant differences were found in demographic data between the two groups. The remifentanil dose administered was similar in both groups. The study group received a higher dose of propofol. However, the control group had a longer duration of operation. The NOL index showed a significantly higher change after severe noxious stimuli compared to Heart Rate, indicating greater sensitivity.
Conclusion: This study compares NOL index monitoring to standard monitoring during intracranial tumor surgery. The results indicate that NOL monitoring is reliable in detecting and monitoring nociception events compared to heart rate changes. However, it does not lead to a significant reduction in opioid dose administration.
Keywords: target controlled infusion, intracranial tumor surgery, intraoperative nociception monitoring, NOL index monitoring, opioid
Introduction
In neurosurgery, the priority is preserving or restoring brain function, so anesthesiologists aim for agents like propofol for quick, smooth induction, and rapid emergence, and an analgesic such as remifentanil that has a rapid onset and offset feature.1,2 Anesthesiologists often deduce the nociceptive level by observing clinical signs like elevated blood pressure and increased heart rate, which are indicators of autonomic nervous system activation.3 While these indicators may be adequate for identifying intense nociceptive stimuli, they frequently fail to detect or identify mild-to-moderate stimuli promptly or at all.4 Monitoring of nociception remains a major intraoperative challenge.
Target Controlled Infusion (TCI) is a method for intravenous anesthetic delivery that targets a specific drug concentration in the body. It uses a computer-controlled pump to adjust dosages based on patient factors like height, weight, and age, aiming for a desired plasma level or a specific site, such as the brain. TCI is a routine anesthetic practice.
A recently published review recommends the use of nociception monitors instead of relying solely on vital sign changes for more accurate intraoperative pain management under anesthesia.5 The nociception level monitor amalgamates data from diverse sources: finger photoplethysmogram amplitude, skin conductance, skin conductance fluctuation, heart rate, heart rate variability, and their temporal shifts. This amalgamation results in a singular index spanning from 0 (indicating an absence of noxious stimulation) to 100 (indicating intense noxious stimulation).4 Among the plethora of monitors on the market, the NOL index has consistently demonstrated its proficiency in monitoring nociception and evaluating a patient’s reaction to antinociceptive treatments.3,6–10
In this prospective, randomized controlled study, we hypothesized that nociception level index monitoring reduced opioid administration during surgery. The secondary goals are to compare the total dose hypnotic drugs, as well as hemodynamic parameters, and to investigate the relationship between changes in the NOL index and HR change following severe noxious stimuli during effect site TCI of propofol and remifentanil in patients undergoing intracranial tumor surgery who are monitored using either standard monitors or the NOL monitor additionally.
Materials and Methods
The prospective, randomized controlled study, in compliance with the principles outlined in the Declaration of Helsinki, was conducted following the approval granted by the Bursa Uludag University Medical Trials Ethics Committee on September 8, 2020 (Approval Number: 2020–15/15), and after obtaining written informed consent from the patients. This study was supported by Uludag University Scientific Research Project Unit and registered in Clinical Trials (NCT05732896).
Fifty patients scheduled for intracranial tumor surgery aged 18–65 years with American Society of Anaesthesiologists (ASA) Physical status class II–III were included in the study. Patients who were suspected to be pregnant, were receiving antiarrhythmic therapy, or had autonomic nervous system disease were excluded from the study. Additionally, patients who were ASA IV, pregnant or lactating, had a body mass index over 35 kg/m, had perceived difficult intubation, were receiving chronic pain treatment, or were undergoing emergency surgery were also excluded.
Upon admission to the operating room, patients were randomly assigned to either the standard care guided group (n=25) or the NOL guided group (n=25) using the closed-envelope method. No premedication was given to any of the patients. In both groups, patients received an intravenous line, five-lead ECG, blood pressure cuff, and bispectral index (BIS) for measurement of depth of anesthesia. In the NOL guided group, a properly prepared NOL index probe (PMD-200, Medasense Biometrics Ltd., Israel) was placed on the 4th finger of the hand on the contralateral side of the blood pressure cuff before induction.
Anesthesia was delivered using TCI with a preset effect side concentration (Ce) of propofol and remifentanil. The Schnider model was used for propofol, and the Minto model was used for remifentanil. Before induction, 1.5 mg/kg of lidocaine i.v. was administered. Induction was administered with propofol Ce of 3.5–6 ng/mL and remifentanil Ce of 2–6 ng/mL. After consciousness was lost (as detected by BIS values below 60, absence of eyelash reflex, and no response to loud and repeated verbal commands), rocuronium 0.6 mg/kg i.v. was administered, and the patient’s trachea was intubated after two minutes later. A radial artery catheter was then inserted to continuously monitor the patient’s arterial blood pressure.
The target propofol concentration was adjusted in steps of 0.1–0.5 μg/mL to maintain a steady state in the value of the BIS at 50±5. The target remifentanil concentration was adjusted in steps of 0.1–0.5 ng/mL to maintain the NOL index between 10 and 25. The maximum concentration dose of remifentanil was set at 7 ng/mL. Higher doses were avoided due to the risk of significant side effects, such as severe bradycardia. The same maximum dose of 7 ng/mL was applied to both groups. Although remifentanil was increased up to 7 ng/mL, additional analgesic (morphine 0.1 mg/kg i.v. bolus or dexmedetomidine 1 μg/kg/h loading for 10 minutes followed by 0.1–0.8 μg/kg/h maintenance i.v. infusion) was administered if the systolic arterial blood pressure (SAP) was above 140 mmHg and the NOL index was above 25. Clinicians in the NOL-guided group titrated the remifentanil concentration based solely on the NOL index monitor’s guidance. A vasodilator (nitroglycerin 0.1 mg i.v. bolus) was administered when the NOL index was in the range of 10–25 and SAP was above 140 mmHg. In the standard care group, the target remifentanil concentration was increased or decreased by 0.1–0.5 ng/mL in a single step to maintain mean arterial pressure (MAP) above 60 mmHg and SAP below 140 mmHg. If the patient was hypotensive (mean arterial pressure < 55 mmHg), ephedrine 5–10 mg i.v. bolus was administered, and when the heart rate was below 40 beats per minute, atropine 0.01 mg/kg i.v. was administered.
In both groups, fluid administration was standardized to 5 to 6 mL/min. It was decided jointly with the surgical team whether the patient should be extubated or not. Before the end of the operation, patients to be extubated were administered pethidine 1 mg/kg i.m., acetominophen 1 g i.v., tenoxicam 20 mg i.v. and metoclopramide 10 mg i.v.
Patients demographic data (age, gender, body weight, height, body mass index, lean body mass index, ASA score) was recorded. Systolic, Diastolic and Mean Arterial Pressure (SAP, DAP, MAP), Heart Rate (HR), BIS values were recorded. In addition, NOL index in the NOL-guided group were recorded before induction (T0), intubation (T1), head holder pinning (T2), skin incision (T3), muscle and periosteal dissection (T4), craniotomy (T5), dural incision (T6), tumor excision (T7), dural suturation (T8), muscle and periosteum suturation (T9), skin suturation (T10), and interruption of infusions (T11).
The study recorded and compared changes in NOL index and HR before and after severe noxious stimuli, including intubation, pin placement, skin incision, and craniotomy. In addition, the duration of the operation and the doses of propofol and remifentanil administered were recorded.
The sample size calculation primarily focused on remifentanil consumption. Based on findings from Meijer et al,8 it was anticipated that the NOL-guided group would exhibit a significant 30% decrease in remifentanil consumption. We needed a minimum of 24 patients in each group for 90% power and α < 0.05, resulting in a total of 50 patients. PASS version 08.0.5 determined statistical power and effect size.
Descriptive stats included mean, SD, range, frequency, and ratio values. We assessed variable distribution with the Kolmogorov–Smirnov test. For quantitative independent data, we used t-tests and Mann–Whitney U-tests. The chi-square test analyzed independent categorical data, and the Fisher’s exact test when the chi-square conditions were not met. SPSS 26.0 conducted our analyses, and significance was P < 0.05.
Results
A total of 50 patients were included in the study. Demographic characteristics and ASA scores of the patients are shown in Table 1. There was no significant difference in demographic data between the two groups (p > 0.05).
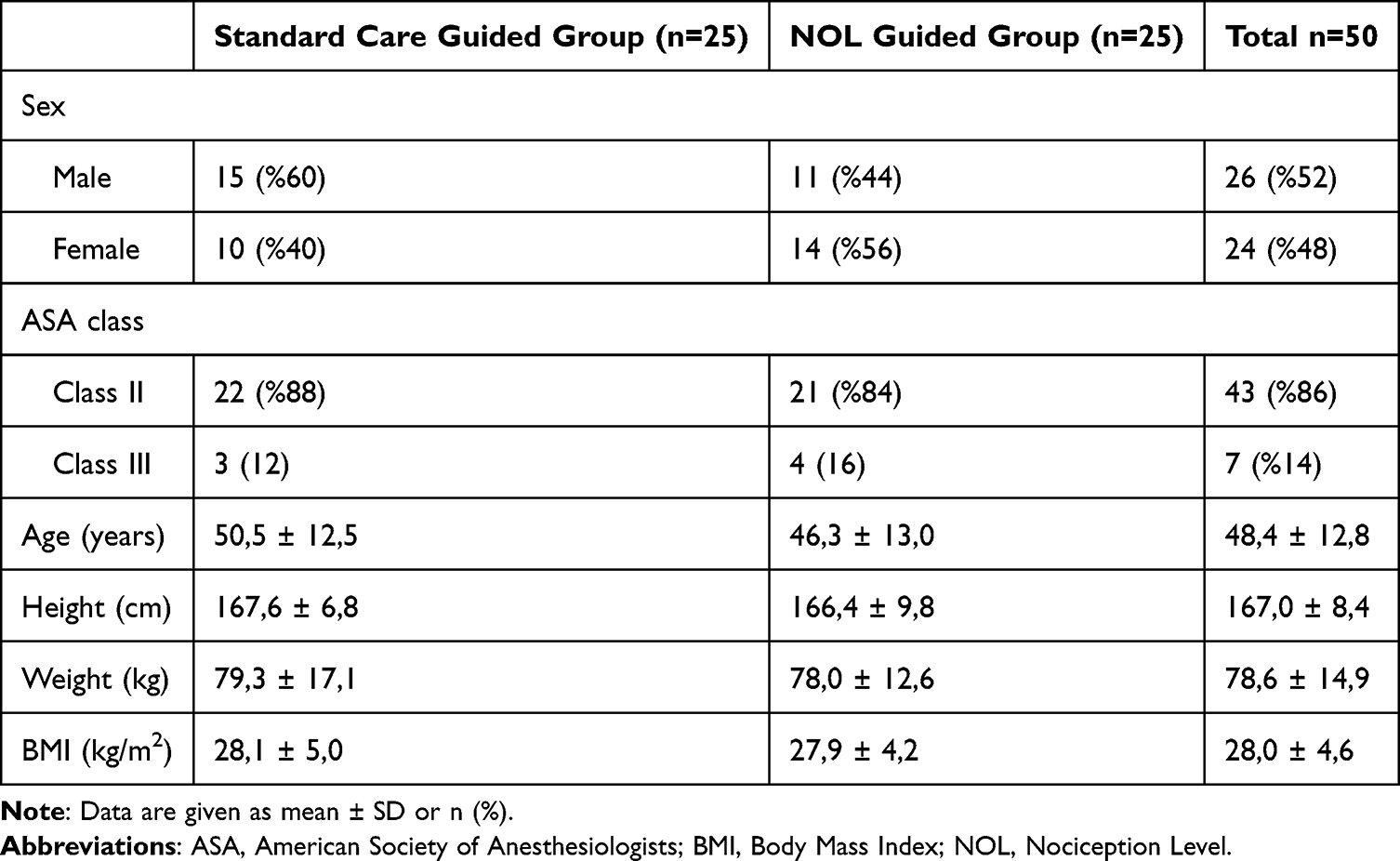 |
Table 1 Demographic Characteristics and ASA Scores |
The duration of operation, propofol and remifentanil dose consumed, propofol and remifentanil Ce values, propofol and remifentanil dose adjustment requirement, distribution of extubated and non-extubated patients are shown in Table 2.
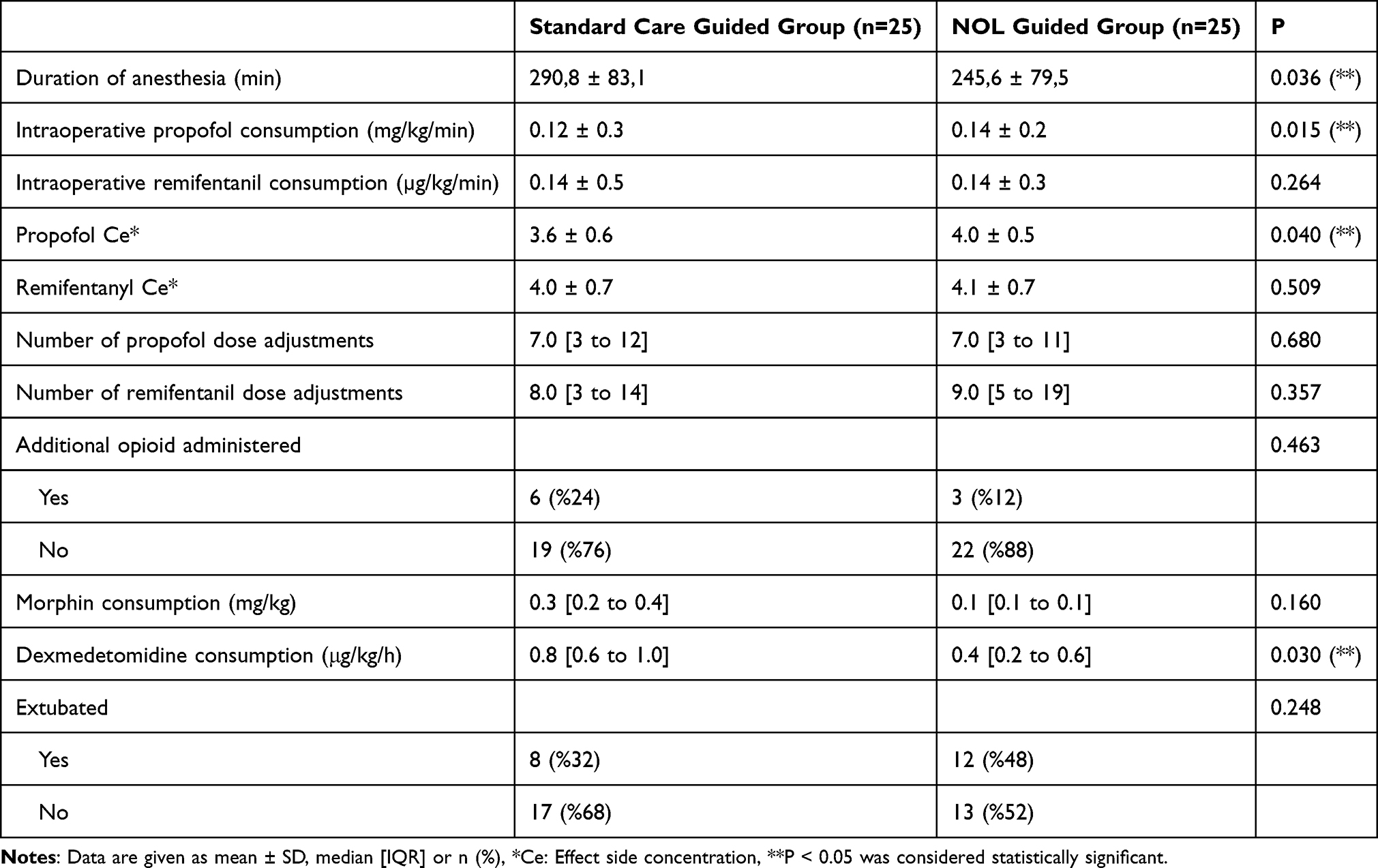 |
Table 2 Intraoperative Data |
We calculate anesthesia drug doses as dose/kg/min of anesthesia time to adjust for patient weight and anesthesia duration. There was no significant difference in the dose of remifentanil consumed between the two groups (0.14 μg/kg/min, p:0.264). The dose of propofol administered in the NOL guided group was significantly higher compared to the standard care guided group (0.14 mg/kg/min vs 0.12 mg/kg/min, p:0.015). The mean Ce values of propofol and remifentanil in the standard care guided group and NOL guided group were 3.6 μg/mL, 4.0 μg/mL and 4.0 ng/mL, 4.1 ng/mL, respectively. The mean Ce value of propofol significantly higher in the NOL guided group (p:0.040).
There was no significant difference in the number of patients requiring additional opioids. However, when comparing the patients who needed additional opioids, although there was no significant difference in the morphine dose, the dose of dexmedetomidine used was significantly higher in the standard care group (p: 0.030).
The total duration of the operation was significantly longer in the standard care guided group compared to the NOL guided group (p:0.036). There was no difference in the number of patients extubated or not and additional opioid administered between the groups.
When comparing the groups based on MAP and HR values during the intraoperative period, no significant difference was found at any time and the average values are presented in Figure 1. In the NOL-guided group, 7 out of 25 patients (28%) encountered a singular hypotensive episode with MAP dropping below 55 mm Hg, while in the standard care-guided group, at least one such event was observed in 10 out of 25 patients (40%). In the NOL guided group, 12 of 25 patients (48%) experienced episodes of systolic blood pressure greater than 140 mmHg, as did 12 of 25 patients (48%) in the standard care guided group. Two patients in the NOL-guided analgesia group had HR below 45 bpm, compared to five in the standard care group out of 25 patients. Eight patients in both groups had an HR greater than 100 bpm. Ephedrine was administered to 4 patients in the standard care guided group, it was administered to 2 patients in the NOL guided group. Nitroglycerine was administered to 3 patients in both groups. Blood product replacement was performed in 1 patient in the NOL guided group and 8 patients in the standard care guided group. The two groups did not exhibit any statistically significant differences in terms of the incidence of hypertension, hypotension, tachycardia, bradycardia, or the need for ephedrine or nitroglycerin administration among patients. However, the number of patients who received blood product replacement was significantly higher in the standard care guided group (n=8) compared to the NOL guided group (n=1) (p=0.023).
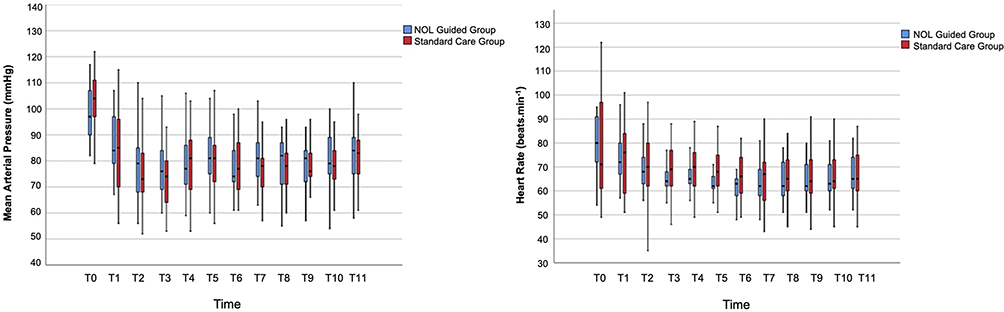 |
Figure 1 Intraoperative Mean Arterial Pressure and Heart Rate. T0: before induction, T1: intubation, T2: head holder pinning, T3: skin incision, T4: muscle and periosteal dissection, T5: craniotomy, T6: dural incision, T7: tumor excision, T8: dural suturation, T9: muscle and periosteum suturation, T10: skin suturation, T11: interruption of infusions. |
NOL index averages are shown in Figure 2. The averages for dural incision (T6), tumor excision (T7), dural suturation (T8), muscle and periosteum suturation (T9), skin suturation (T10) were below the target value of 10.
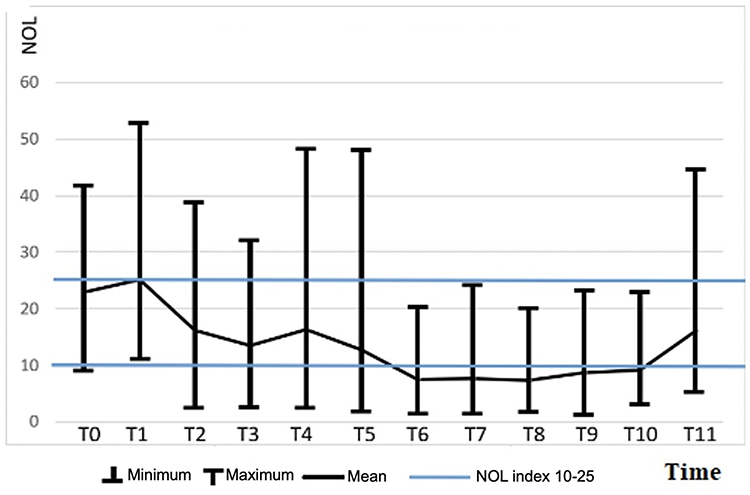 |
Figure 2 Intraoperative NOL index. |
The changes in NOL index and HR before and after intubation, head holder pinning, skin incision and craniotomy, which were determined as severe noxious stimuli, are shown in Figure 3. There was a significant difference between NOL index and HR changes in these stimuli (p<0.05). Following intubation, NOL index increased by 16.2 points, representing a 95% increase from baseline, while HR increased by 9.9 bpm, which was a 14% increase from baseline. Head holder pinning resulted in an increase of 11.7 points in NOL index and 2.8 bpm in HR, corresponding to increased rates of 113% and 4%, respectively. Skin incision led to an increase of 12.0 points in NOL index and 2.2 bpm in HR, which represented an increase rate of 181% and 3%, respectively. Finally, after craniotomy, the NOL index increased by 9.9 points and the HR increased by 2.2 bpm, representing increase rates of 133% and 2%, respectively.
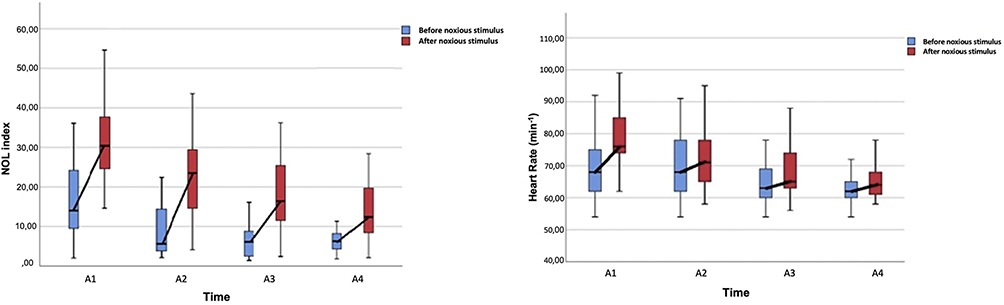 |
Figure 3 Change in NOL index and Heart Rate before and after the severe noxious stimulus. A1: intubation, A2: pin placement, A3: skin incision, A4: craniotomy. |
Regarding intracranial tumor localizations, we identified 15 supratentorial and 10 infratentorial lesions in the standard care guided group, and 19 supratentorial and 6 infratentorial lesions in the NOL guided group. There was no significant difference in lesion localization, midline shift, edema, or tumor size between the two groups. The number of patients who received pre-operative antiedema and antiepileptic treatment was significantly higher in the NOL guided group (p=0.02, p=0.034), whereas the number of patients who received intraoperative antiedema treatment was significantly higher in the standard care guided group (p=0.005). There was no significant difference in the number of patients receiving intraoperative antiepileptic therapy (p=0.48).
Subgroup analyses were performed according to tumor localizations for both groups. The propofol dose was higher in patients with supratentorial tumors in the NOL guided group. Additionally, the number of patients who received ephedrine and/or atropine was higher in patients with infratentorial tumors compared to those with supratentorial tumors in the NOL guided group (p=0.05 and p=0.05, respectively). In the standard care guided group, the number of patients who received atropine was higher in those with supratentorial tumors (p=0.029).
Totally, 40% of the patients could be extubated (n=12, 48%) in the standard care guided group (n=8, 32% in the NOL-guided group). Other patients were taken to the intensive care unit as intubated for surgical reasons.
Discussion
This prospective, randomized, controlled study investigates whether monitoring with the NOL index has an effect on opioid consumption compared to standard monitoring during effect site TCI of propofol and remifentanil in patients undergoing elective intracranial tumor surgery. Additionally, the study examined the consumption of hypnotic drugs, hemodynamic parameters, NOL index variability, and changes in HR following severe noxious stimuli in the study group patients who underwent NOL monitoring. This study was performed on patients with similar intracranial tumor locations and demographic characteristics.
In our study, the intraoperative remifentanil dose administered in both groups was 0.14 μg/kg/min, and no significant difference was found. However, the remifentanil dose was increased up to a maximum of 7 ng/mL. If additional analgesia was needed, morphine or dexmedetomidine was added. Although there was no significant difference in the number of patients requiring additional analgesia, a higher number of patients in the standard care guided group (6/25 vs 3/25) received additional analgesia. Furthermore, the dose of dexmedetomidine used was higher in the standard care guided group. Different results were found for the administered remifentanil dose, such as 0.11 μg/kg/min.11,12 In Meijer et al’s study, the administered remifentanil dose was found to be 0.119 μg/kg/min in the standard care group and 0.086 μg/kg/min in the NOL-guided group, which was significantly different.8 In a meta-analysis, it was found that when opioids were administered with NOL guided anesthesia, intraoperative opioid consumption was significantly lower.13 Funcke et al showed that the NOL-guided group exhibited a substantial 32% reduction in intraoperative sufentanil consumption.6 Furthermore, a more recent study conducted by the same research group, this time focusing on remifentanil, also showcased a noteworthy decrease in intraoperative remifentanil consumption.14 In studies of intra-abdominal, colorectal, laparoscopic gynecological, and “da Vinci” prostatectomy surgeries, no significant difference was found in opioid consumption with anesthesia guided by NOL index.15–18
In the NOL-guided group, both the dose of propofol (mg/kg/min) and the mean Ce value of propofol were significantly higher. In studies that used TCI pumps for anesthesia during intracranial tumor surgeries, the propofol dose was found to be between 0.21 mg/kg/min and 0.09 mg/kg/min.11,12,19,20 However, only two studies utilized effect site TCI for propofol. In one of these studies, propofol was found to be 0.10 mg/kg/min for the non-functioning tumor surgery group and 0.12 mg/kg/min for the growth hormone-secreting tumor surgery group that was performed through the transsphenoidal approach.11 Nunes et al12 used effect-site TCI, and they found the administered propofol dose of 0.12 mg/kg/min in their study of neurosurgical procedures. In this study, which was performed on patients with similar intracranial tumor locations and demographic characteristics, the administered propofol dose was 0.12 ± 0.3 mg/kg/min in the standard care group and 0.14 ± 0.2 mg/kg/min in the NOL guided group, which was significantly different.
Since there is no other study comparing the effectiveness of standard care and NOL monitoring in patients who underwent general anesthesia with effect site TCI during intracranial tumor surgery, we examined the drug consumption in patients who underwent different surgeries. Meijer et al8 found the administered propofol dose to be 0.107 mg/kg/min in the standard care group and 0.105 mg/kg/min in the NOL-guided group in their study on patients undergoing intraabdominal surgery.
Another study, focusing on the influence of intraoperative pupillometry monitoring on perioperative opioid usage during major gynecologic surgery with effect site TCI, revealed that propofol consumption remained consistent at 0.14 mg/kg/min in both study groups.21
In an another study, which evaluated the impact of intraoperative pupillometry monitoring on perioperative opioid consumption in major gynecologic surgery during effect site TCI, it was found that propofol consumption was similar in both groups.
Sahinovic et al reported that brain tumours might alter the pharmacokinetics of propofol and drew attention to the need for caution when using propofol TCI in patients with frontal brain tumours due to higher clearance.22 Moreover, indices generated by electroencephalogram-based systems such as BIS do not directly correlate with the neurophysiology of how a specific anesthetic drug affects the brain; therefore, they cannot provide an accurate representation of the brain’s response to drugs. In patients undergoing intracranial tumor surgery, this situation can be even more complex and uncertain. In this study, there was no significant difference in brain tumor localization, midline shift, edema, or tumor size between the two groups.
The number of patients who received pre-operative antiedema and antiepileptic treatment was significantly higher in the NOL guided group. All patients treated with anticonvulsant medication in our study were using levetiracetam. Due to their patients being on chronic medication with one or more traditional anticonvulsants (phenobarbitone, phenytoin, or carbamazepine), Huggins et al19 reported a high target plasma concentration, as these medications induce hepatic microsomal enzymes. Sahinovic et al reported that propofol clerence was higher in subjects with a brain tumour compared to the control group.22 Their suggestion leads to the consideration that to achieve the same target propofol concentration, infusion rates should be higher for patients with brain tumors in comparison to those undergoing spinal surgery. They also reported that neither antiepileptic drugs in general nor enzyme-inducing antiepileptic drugs were helpful in explaining the higher clerence in the tumour group. Therefore, thus they postulated that other factors are responsible for the observed difference in pharmacokinetics.
In this study, both groups had similar MAP and HR, and there was no significant difference in the numbers of patients experiencing hypotension, hypertension, tachycardia, bradycardia, and receiving vasoactive agents. In the study conducted by Meijer et al,8 the standard care group had a higher number of patients experiencing hypotensive events and receiving vasopressor agents compared to the NOL-guided group. Additionally, the standard care group had a higher number of patients with bradycardia. Renaud-Roy et al16 studied colorectal surgery patients and compared BIS and NOL guidance with standard care. They found no significant difference in hemodynamic stability. In another study, Espitalier et al17 also found no significant differences in hemodynamic parameters during laparoscopic gynecological surgeries between the NOL group and standard care.
In neuroanesthesia, intense stimulation occurs during procedures like laryngoscopy, intubation, head holder pinning, scalp incision, and craniotomy. These are followed by periods of minimal stimulation during surgical site preparation. These quiet moments can lead to decreased sympathetic activity, causing bradycardia and hypotension. To manage this, quick-acting drugs like remifentanil are valuable in neurosurgery.
Many studies in the literature highlight the reliability of NOL index monitoring in assessing nociception and detecting noxious stimuli. Martini et al found NOL index to be superior to HR and MAP in distinguishing nociceptive and nonnociceptive conditions during surgery with propofol-remifentanil anesthesia.23 Treister et al discovered that while individual NOL components could not differentiate between levels of noxious intensity, the combined NOL index effectively distinguished between pain and no pain, as well as different pain intensities in awake volunteers.24 Bollag et al noted NOL index’s higher sensitivity in detecting noxious stimuli like intubation, incisions, and trocar placement compared to HR changes.7 In our study, the changes in the NOL index before and after intubation, head holder pinning, skin incision and craniotomy, which were determined as severe noxious stimuli, are significantly higher than the changes in HR. NOL index increased by 95%, 113%, 181%, 133% after intubation, head holder pinning, skin incision and craniotomy, whereas HR increased by only 14%, 4%, 3%, and 2% for the same stimulus, respectively. NOL index was found to be more sensitive during these periods. These findings are consistent with earlier reports suggesting that the NOL index may exhibit enhanced sensitivity in identifying noxious stimuli, such as intubation.7,23,25
The study has limitations. Firstly, the maximum dose of Remifentanil was set at 7 ng/mL, and additional different analgesic drugs were used when necessary. This could be a reason for the lack of significant differences in the consumed doses of Remifentanil. Secondly, it was single-blinded, potentially introducing implementation or performance bias. Thirdly, NOL monitoring could not be applied to the Standard Care group due to limited probes, preventing NOL value comparisons.
Conclusion
This study compares NOL index monitoring with standard monitoring during propofol and remifentanil infusion in intracranial tumor surgery. Results suggest that NOL monitoring is reliable for detecting noxious stimuli but does not significantly reduce remifentanil dose. Limited literature exists on effect site concentration, elimination, distribution volume, and clearance of these drugs in targeted infusion systems. Future trials are needed for more conclusive results.
Data Sharing Statement
De-identified participant data will not be available as an online accessible source. The study protocol can be accessed via the clinical trial number on clinicaltrials.gov.
Acknowledgments
I would like to thank Uludag University Scientific Research Project Unit for their financial support.
Disclosure
The abstract of this paper was presented at the 57th National Congress of the Turkish Society of Anesthesiology and Reanimation as an oral presentation.
Muhammet Esat Demirel reports grants from Uludag University Scientific Research Project Unit during the conduct of the study. The authors declare no other conflicts of interest.
References
1. Costa AM, Lobo F. TIVA for neurosurgery. In: Challenging Topics in Neuroanesthesia and Neurocritical Care. 2017;155–166. doi:10.1007/978-3-319-41445-4_13
2. Erickson KM, Cole DJ. Anesthetic considerations for awake craniotomy for epilepsy and functional neurosurgery. Anesthesiol Clin. 2012;30(2):241–268. doi:10.1016/j.anclin.2012.05.002
3. Renaud-Roy E, Stöckle PA, Maximos S, et al. [Correlation between incremental remifentanil doses and the Nociception Level (NOL) index response after intraoperative noxious stimuli]. Corrélation entre des doses croissantes de rémifentanil et la réponse de l’indice de nociception NOL après des stimuli peropératoires douloureux. Can J Anaesth. 2019;66(9):1049–1061. doi:10.1007/s12630-019-01372-1
4. Ben-Israel N, Kliger M, Zuckerman G, Katz Y, Edry R. Monitoring the nociception level: a multi-parameter approach. J Clin Monit Comput. 2013;27(6):659–668. doi:10.1007/s10877-013-9487-9
5. Ledowski T. Objective monitoring of nociception: a review of current commercial solutions. Br J Anaesth. 2019;123(2):e312–e321. doi:10.1016/j.bja.2019.03.024
6. Funcke S, Pinnschmidt HO, Wesseler S, et al. Guiding opioid administration by 3 different analgesia nociception monitoring indices during general anesthesia alters intraoperative sufentanil consumption and stress hormone release: a randomized controlled pilot study. Anesth Analg. 2020;130(5):1264–1273. doi:10.1213/ANE.0000000000004388
7. Bollag L, Jelacic S, Delgado Upegui C, Wu C, Richebe P. The nociception level index (NOL) response to intubation and incision in patients undergoing video-assisted thoracoscopic surgery (VATS) with and without thoracic epidural analgesia. A pilot study. F1000Res. 2018;7:875. doi:10.12688/f1000research.15279.1
8. Meijer FS, Martini CH, Broens S, et al. Nociception-guided versus standard care during remifentanil-propofol anesthesia: a randomized controlled trial. Anesthesiology. 2019;130(5):745–755. doi:10.1097/ALN.0000000000002634
9. Ogata H, Nakamoto S, Miyawaki H, et al. Association between intraoperative nociception and postoperative complications in patients undergoing laparoscopic gastrointestinal surgery. J Clin Monit Comput. 2020;34(3):575–581. doi:10.1007/s10877-019-00347-3
10. Meijer FS, Niesters M, van Velzen M, et al. Does nociception monitor-guided anesthesia affect opioid consumption? A systematic review of randomized controlled trials. J Clin Monit Comput. 2020;34(4):629–641. doi:10.1007/s10877-019-00362-4
11. Kim SH, Kim N, Kim EH, Suh S, Choi SH. Propofol requirement in patients with growth hormone-secreting pituitary tumors undergoing transsphenoidal surgery. J Clin Med. 2019;8(5):571. doi:10.3390/jcm8050571
12. Nunes CS, Ferreira DA, Antunes L, Amorim P. Clinical variables related to propofol effect-site concentrations at recovery of consciousness after neurosurgical procedures. J Neurosurg Anesthesiol. 2005;17(2):110–114. doi:10.1097/01.ana.0000163198.02742.9d
13. Ma D, Ma J, Chen H, Mu D, Kong H, Yu L. Nociception monitors vs. standard practice for titration of opioid administration in general anesthesia: a meta-analysis of randomized controlled trials. Front Med. 2022;9:963185. doi:10.3389/fmed.2022.963185
14. Funcke S, Pinnschmidt HO, Brinkmann C, et al. Nociception level-guided opioid administration in radical retropubic prostatectomy: a randomised controlled trial. Br J Anaesth. 2021;126(2):516–524. doi:10.1016/j.bja.2020.09.051
15. Meijer F, Honing M, Roor T, et al. Reduced postoperative pain using Nociception Level-guided fentanyl dosing during sevoflurane anaesthesia: a randomised controlled trial. Br J Anaesth. 2020;125(6):1070–1078. doi:10.1016/j.bja.2020.07.057
16. Renaud-Roy E, Morisson L, Brulotte V, et al. Effect of combined intraoperative use of the Nociception Level (NOL) and bispectral (BIS) indexes on desflurane administration. Anaesth Crit Care Pain Med. 2022;41(3):101081. doi:10.1016/j.accpm.2022.101081
17. Espitalier F, Idrissi M, Fortier A, et al. “Impact of Nociception Level (NOL) index intraoperative guidance of fentanyl administration on opioid consumption, postoperative pain scores and recovery in patients undergoing gynecological laparoscopic surgery. A randomized controlled trial”. J Clin Anesth. 2021;75:110497. doi:10.1016/j.jclinane.2021.110497
18. Niebhagen F, Golde C, Koch T, Hübler M. [Does NoL monitoring affect opioid consumption during da Vinci prostatectomy?] Beeinflusst NoL-Monitoring den Opioidbedarf bei Da-Vinci-Prostatektomien?. Anaesthesiologie. 2022;71(9):683–688. doi:10.1007/s00101-022-01126-7
19. Huggins NJ. ‘Diprifusor’ for neurosurgical procedures. Anaesthesia. 1998;53(Suppl 1):53–55. doi:10.1111/j.1365-2044.1998.53s105.x
20. Sneyd JR, Andrews CJ, Tsubokawa T. Comparison of propofol/remifentanil and sevoflurane/remifentanil for maintenance of anaesthesia for elective intracranial surgery. Br J Anaesth. 2005;94(6):778–783. doi:10.1093/bja/aei141
21. Sabourdin N, Barrois J, Louvet N, et al. Pupillometry-guided intraoperative remifentanil administration versus standard practice influences opioid use: a randomized study. Anesthesiology. 2017;127(2):284–292. doi:10.1097/ALN.0000000000001705
22. Sahinovic MM, Eleveld DJ, Miyabe-Nishiwaki T, Struys MMRF, Absalom AR. Pharmacokinetics and pharmacodynamics of propofol: changes in patients with frontal brain tumours. Br J Anaesth. 2017;118(6):901–909. doi:10.1093/bja/aex134
23. Martini CH, Boon M, Broens SJ, et al. Ability of the nociception level, a multiparameter composite of autonomic signals, to detect noxious stimuli during propofol-remifentanil anesthesia. Anesthesiology. 2015;123(3):524–534. doi:10.1097/ALN.0000000000000757
24. Treister R, Kliger M, Zuckerman G, Aryeh IG, Eisenberg E. Differentiating between heat pain intensities: the combined effect of multiple autonomic parameters. Pain. 2012;153(9):1807–1814. doi:10.1016/j.pain.2012.04.008
25. Edry R, Recea V, Dikust Y, Sessler DI. Preliminary intraoperative validation of the nociception level index: a noninvasive nociception monitor. Anesthesiology. 2016;125(1):193–203. doi:10.1097/ALN.0000000000001130
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.