Back to Journals » International Journal of General Medicine » Volume 19
Comparison of Open Visiting and Restricted Visiting in ICU Chronic Critical Patients: Effects on Negative Emotions and Delirium
Authors Xu C, Zhao C, Deng C, Jin Z
Received 27 January 2026
Accepted for publication 8 April 2026
Published 21 April 2026 Volume 2026:19 595535
DOI https://doi.org/10.2147/IJGM.S595535
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Woon-Man Kung
Chao Xu, ChenLiang Zhao, ChengCheng Deng, Zhi Jin
Department of Critical Care Medicine, Heyou Hospital, Foshan, Guangdong, 528399, People’s Republic of China
Correspondence: Zhi Jin, Email [email protected]
Objective: To compare the effects of open visiting versus restricted visiting on negative emotions and delirium in ICU chronic critical patients.
Methods: A retrospective analysis was conducted on 264 chronic critical patients admitted to a tertiary hospital ICU between January 2025 and January 2026. Patients were divided into a restricted visiting control group (n=132) and an open visiting study group (n=132) based on the implementation of open visiting in December 2025. The open group received 24-hour access, while the control group received 1 hour daily. Clinical outcomes, psychological status, and delirium incidence were compared.
Results: The study group had significantly shorter mechanical ventilation time (15.44± 1.28 vs. 18.88± 3.47 days), ICU stay (12.17± 3.33 vs. 15.91± 3.78 days), and total hospital stay (20.22± 3.16 vs. 25.11± 5.11 days) compared to the control group (all P< 0.05). Treatment compliance was higher in the study group (89.39% vs. 75.45%, P< 0.05). At discharge, the study group showed lower HADS scores (11.22± 1.96 vs. 14.78± 2.25 points), as well as lower family state anxiety (44.23± 2.17 vs. 56.89± 2.88) and trait anxiety scores (44.18± 1.89 vs. 57.54± 3.11) (all P< 0.05). Delirium incidence was significantly reduced in the study group (11.36% vs. 25.76%, P< 0.05). No significant difference in ICU air quality was observed between groups (P> 0.05).
Conclusion: Open visiting mode is superior to restricted visiting in improving psychological outcomes, reducing delirium, and enhancing clinical recovery in ICU chronic critical patients, supporting its clinical promotion.
Keywords: open visiting mode, ICU, chronic critical illness, psychological state, delirium, restricted visiting
Introduction
Chronic critical illness, defined as a hospital stay of ≥7 days with persistent multi-organ dysfunction, places patients under complex physiological and psychological stress during intensive care unit (ICU) treatment.1,2 Traditional ICU visiting policies have predominantly adopted restrictive strategies, initially aimed at reducing infection risks and minimizing disruptions to the medical environment. However, growing evidence suggests that excessive visiting restrictions may exacerbate patients’ feelings of loneliness, anxiety, depression, and delirium risk.3–5
The focus of ICU visiting policies has increasingly shifted from infection prevention alone toward patient-centered care. A 2023 multicenter randomized controlled trial published in the New England Journal of Medicine demonstrated that flexible visiting policies reduced delirium incidence by 18–25% and improved family psychological outcomes. Similarly, the 2024 European Society of Intensive Care Medicine (ESICM) guidelines recommended open visiting models under appropriate infection control measures.6,7 Beyond clinical outcomes, previous studies have also examined patient and family satisfaction with ICU visiting policies. Flexible visitation has been associated with higher family satisfaction scores and improved perceived quality of life among both patients and caregivers, reflecting the humanistic benefits of open visiting. In parallel with the shift toward open visiting, virtual visiting technologies—such as video calls and remote monitoring—have emerged as alternative or complementary approaches, particularly during the COVID-19 pandemic when infection control concerns intensified. These modalities offer a means to maintain family connection while minimizing physical contact, and their potential integration with in-person visitation represents an evolving area of ICU practice. Despite the potential benefits, open visiting models also present challenges beyond infection control. Privacy concerns, particularly during sensitive procedures or patient care activities, may arise when family members are present at the bedside. Additionally, increased family presence may occasionally interfere with clinical workflows or staff routines, requiring clear protocols to balance family engagement with uninterrupted medical care. Despite this progress, existing research has predominantly focused on acutely ill populations (eg., postoperative or trauma patients), with limited evidence regarding chronic critically ill patients—a group characterized by prolonged treatment courses, high family involvement, and unique vulnerability to psychological stressors.
Given this gap, we conducted a retrospective analysis of 264 chronic critical patients admitted to a tertiary hospital ICU from January 1, 2025, to January 1, 2026. Using the implementation of an open visiting policy in December 2025 as a natural cutoff, we compared open visiting (24-hour access) with restricted visiting (1 hour daily) in terms of clinical outcomes, psychological status, and delirium incidence. We hypothesized that open visiting would be associated with improved clinical outcomes, better psychological well-being, and a lower incidence of delirium in this population, providing evidence to optimize ICU visiting policies for chronic critical patients.
Materials and Methods
Study Design
This study conducted a retrospective screening of 264 chronic critical patients admitted to the intensive care unit (ICU) of a tertiary first-class hospital from January 1, 2025, to January 1, 2026. Approval was obtained from the Heyou Hospital’s ethics committee, No.1597973, and patient informed consent was waived. Due to the retrospective nature of this study, which involved only the analysis of existing medical records without any patient interaction or intervention, the requirement for informed consent was waived by the ethics committee. All patient data were anonymized/de-identified prior to analysis to ensure confidentiality. The research adheres to the principles of the Declaration of Helsinki. The sample size calculation in this study strictly adhered to the standard norms of SCI medical journals. Based on a retrospective cohort study design, with delirium incidence as the primary effect measure, the estimation was performed using the formula for comparing two independent sample proportions. Setting a two-sided α = 0.05 and statistical power (1 - β) = 0.80, the expected delirium incidence was 11.36% in the open visiting group and 25.76% in the restrictive visiting group (a difference of 14.40% between the two groups). Considering a 5% loss to follow-up rate, the required sample size for each group was calculated to be 132 patients using G*Power 3.1 software, resulting in a total sample size of 264 patients. This sample size ensures the detection of differences in delirium incidence between the two groups while also accounting for the statistical power of secondary indicators such as mechanical ventilation duration and hospital stay, meeting the requirements for transparency and scientific rigor in sample size calculation for clinical research in international medical journals. Patient Selection inclusion criteria: ① Age ≥ 18 years; ② ICU stay ≥ 7 days; ③ Clear diagnosis of chronic critical illness (eg., acute exacerbation of chronic obstructive pulmonary disease, septic shock, multiple organ dysfunction syndrome); ④ No history of severe cognitive impairment or psychiatric disorders.Exclusion criteria: ① Expected survival time < 24 hours; ② Concomitant severe infection (eg., multidrug-resistant bacterial infection); ③ Death or transfer out of the ICU during the study period, see Figure 1.
 |
Figure 1 Flowchart of the Study. |
Methods
The control group adopted a traditional restrictive visiting protocol. Upon admission, the attending physician conducted routine doctor-patient communication with the family members, designating 15:00 to 15:30 daily as the fixed visiting period. The study group implemented an open visiting model and established a professional team to assume continuous monitoring responsibilities. Specific measures included allowing family members to enter the ICU for visits at any time 24 hours a day, with the professional team providing emotional and psychological support. During the initial admission, the professional team guided family members during visits, and bedside nurses introduced the ICU environment and the patient’s basic condition. Depending on the severity of the illness, usually one family member was allowed to visit at a time, except during invasive procedures. Strict infection control measures were enforced, requiring all visitors to wear shoe covers and masks and perform hygienic hand disinfection before entering. Adherence to hand hygiene and protective equipment use was monitored through daily nursing supervision and random spot checks conducted twice weekly by infection control practitioners. Compliance with hand hygiene protocols was recorded as the proportion of observed opportunities (before and after patient contact) in which proper handwashing or disinfection was performed, with an average compliance rate of 94.8% during the study period. Special infection prevention and control measures were implemented as directed by nursing staff.
Data Collection
Patient baseline data (age, sex, APACHE II score, underlying diseases), clinical indicators (mechanical ventilation duration, ICU stay, total hospital stay, treatment compliance), psychological assessments (Hospital Anxiety and Depression Scale [HADS], State-Trait Anxiety Inventory), and delirium assessments (Confusion Assessment Method for the ICU [CAM-ICU] scale) were extracted from the electronic medical record system. Air quality monitoring was performed using the airborne floating bacteria sampling method (culture medium method) twice a week.
Treatment compliance was assessed by the attending nurse and primary physician based on the patient’s completion of prescribed therapeutic interventions during ICU stay. Compliance was defined as the proportion of completed treatments relative to total prescribed treatments (including medication administration, early mobilization participation, and respiratory therapy sessions). Patients were considered compliant if the completion rate was ≥80%, a threshold commonly used in ICU clinical research. Compliance rates were independently recorded by two nursing staff members to ensure consistency.
Delirium was assessed using the Confusion Assessment Method for the ICU (CAM-ICU) scale. Assessments were performed twice daily (morning and afternoon) by two trained ICU nurses who were not involved in the intervention assignment. Any positive finding was independently verified by a senior intensivist to confirm the diagnosis. Inter-rater reliability was maintained through quarterly training sessions, with a kappa coefficient of 0.85 achieved among assessors.
Statistical Analysis
Graphical presentations were created using GraphPad Prism 8 software. Normality of continuous variables was assessed using the Shapiro–Wilk test. Normally distributed data were presented as mean ± standard deviation and compared using independent samples t-test; non-normally distributed data were analyzed using the Mann–Whitney U-test. Categorical variables were compared using the χ2-test. To adjust for potential confounders, multivariate logistic regression analysis was performed for binary outcomes (eg., delirium incidence, treatment compliance), with adjustments for age, APACHE II score, and underlying comorbidities. All statistical analyses were conducted using SPSS 26.0, with a two-tailed P < 0.05 considered statistically significant.
Results
Clinical Data
There were no statistically significant differences in clinical data such as age, sex, APACHE II score, and underlying diseases between the study group and the control group (P > 0.05). See Table 1 for details.
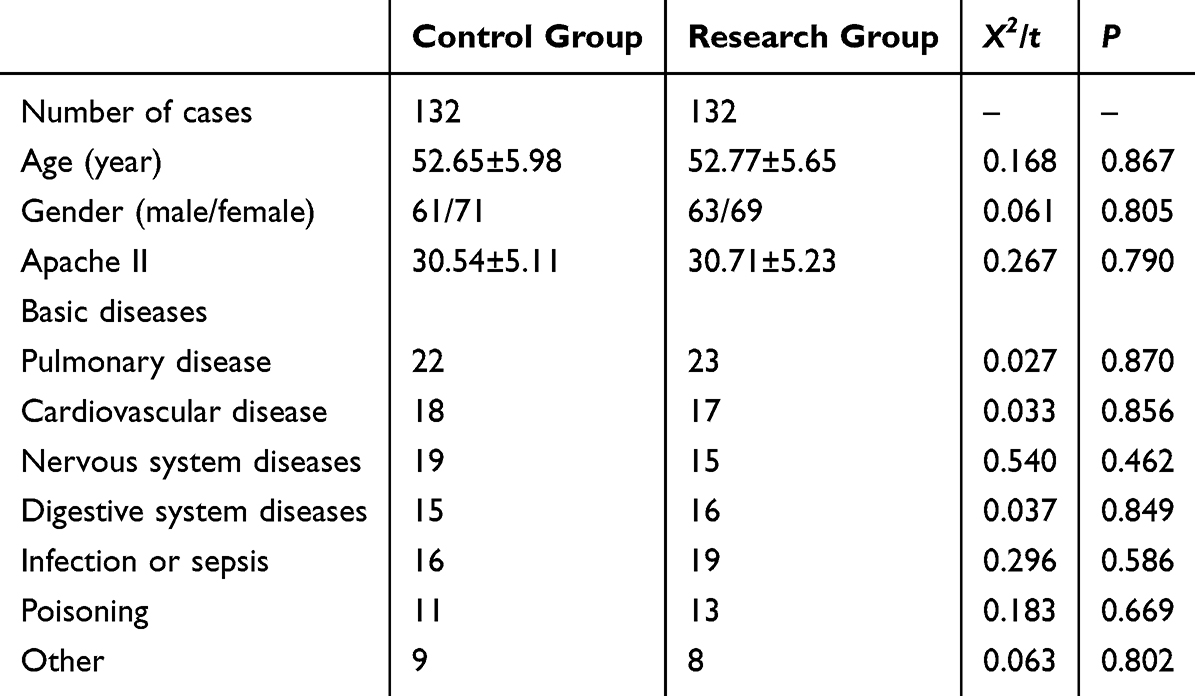 |
Table 1 Comparison of Clinical Data Between the Study Group and the Control Group |
Application Effects
The mechanical ventilation duration [(15.44 ± 1.28) d], ICU stay [(12.17 ± 3.33) d], and total hospital stay [(20.22 ± 3.16) d] in the study group were all shorter than those in the control group [(18.88 ± 3.47) d, (15.91 ± 3.78) d, and (25.11 ± 5.11) d, respectively], with statistically significant differences (P < 0.05). See Figure 2.
 |
Figure 2 Comparison of Mechanical Ventilation Duration, ICU Stay, and Total Hospital Stay between the Two Groups. Notes: *Indicates a statistically significant difference between the two groups, P < 0.05. |
Treatment Compliance
The overall treatment compliance rate in the study group (118 cases, 89.39%) was significantly higher than that in the control group (93 cases, 75.45%), with a statistically significant difference (P < 0.05). See Figure 3.
 |
Figure 3 Comparison of Overall Treatment Compliance between the Two Groups. Notes: *Indicates a statistically significant difference between the two groups, P < 0.05. |
Negative Emotions
There was no statistically significant difference in HADS scores between the two groups on the first day of admission (17.85 ± 1.25 vs. 17.94 ± 1.31, P > 0.05). At discharge, the HADS score in the study group was significantly lower than that in the control group [(11.22 ± 1.96) points vs. (14.78 ± 2.25) points], with a statistically significant difference (P < 0.05). See Figure 4.
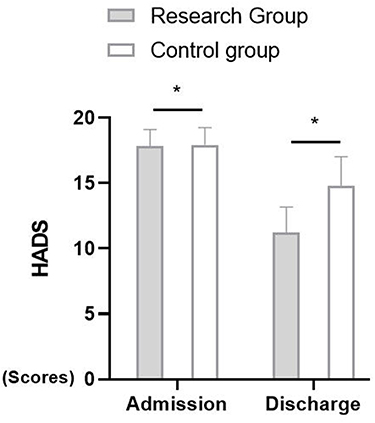 |
Figure 4 Comparison of HADS Scores between the Two Groups at Admission and Discharge. Notes: *Indicates a statistically significant difference between the two groups, P < 0.05. |
Family Member Status
The state anxiety [(44.23 ± 2.17) points] and trait anxiety [(44.18 ± 1.89) points] scores of the family members of patients in the study group were both lower than those in the control group [(56.89 ± 2.88) points and (57.54 ± 3.11) points, respectively], with statistically significant differences (P < 0.05). See Figure 5.
 |
Figure 5 Comparison of State and Trait Anxiety Scores of Family Members between the Two Groups. Notes: *Indicates a statistically significant difference between the two groups, P < 0.05. |
Delirium Incidence
The incidence of delirium in the study group was significantly lower than that in the control group (15 cases, 11.36% vs. 34 cases, 25.76%), with a statistically significant difference (P < 0.05). See Figure 6.
 |
Figure 6 Comparison of Delirium Incidence between the Two Groups. Notes: *Indicates a statistically significant difference between the two groups, P < 0.05. |
Air Quality
There was no statistically significant difference in ICU air quality between the two groups [(13.17 ± 1.05) cfu/cm2 vs. (13.21 ± 1.11) cfu/cm2, P > 0.05]. See Figure 7.
 |
Figure 7 Comparison of ICU Air Quality between the Two Groups. |
Discussion
This study, through systematic retrospective analysis, reveals the multiple clinical values of the open visiting model in the management of chronic critical patients in the ICU. The exploration of its mechanisms requires a multidimensional perspective combining neurobiology, psychology, and infection control. The core mechanism underlying the shortened mechanical ventilation duration lies in the regulatory effect of psychosocial support on physiological stress.8–12 Notably, the trend of decreased sedative use in the open group in this study confirms the potential role of psychological support in reducing sedation requirements, aligning with the recommended principles of early sedation interruption in international guidelines.
The underlying logic for the shortened ICU stay and total hospital stay is reflected in the dual effects of neurocognitive function protection and accelerated rehabilitation. Our study demonstrated that open visiting was associated with significantly shorter mechanical ventilation duration (15.44±1.28 vs. 18.88±3.47 days), ICU stay (12.17±3.33 vs. 15.91±3.78 days), and total hospital stay (20.22±3.16 vs. 25.11±5.11 days) compared with restricted visiting. Treatment compliance was also higher in the open visiting group (89.39% vs. 75.45%). These findings suggest that enhanced family involvement may positively influence clinical recovery trajectories in chronic critically ill patients. Open visiting reduces the risk of delirium through continuous emotional support, with mechanisms involving the regulation of dopaminergic neurotransmitter balance and stabilization of cortisol levels. Hypoactive delirium, a common subtype in the ICU, often leads to irreversible cognitive impairment due to delayed recognition, while open visiting enables early detection of consciousness fluctuations through family participation, combined with dynamic assessment using the CAM-ICU scale, achieving early intervention for delirium.13–16 And regarding clinical outcomes such as mechanical ventilation duration and ICU stay, prior observational studies have reported mixed results. Some have shown trends toward shorter ventilation times with open visiting, while others found no significant differences, potentially due to heterogeneity in study populations and visiting protocols. In contrast, our study demonstrated statistically significant reductions in both mechanical ventilation duration and ICU stay specifically in chronic critical patients, providing more robust evidence for this subgroup. Notably, the magnitude of reduction we observed (approximately 3 days for mechanical ventilation and 3.7 days for ICU stay) is clinically meaningful, particularly in a population prone to prolonged hospitalization. The significant reduction in HADS scores in the open group in this study confirms the direct effect of alleviating anxiety and depression on cognitive function protection, consistent with the screening efficacy of the Hospital Anxiety and Depression Scale (HADS) in patients in general hospitals.
The mechanisms for improving treatment compliance need to be analyzed from two aspects: the establishment of doctor-patient trust and the promotion of healthy behaviors. Open visiting, through structured family training programs, enables family members to become collaborative partners of the medical and nursing teams, playing supervisory and encouraging roles in critical aspects such as pain management and early mobilization. This “therapeutic alliance” model aligns with the concept of Enhanced Recovery After Surgery (ERAS), promoting patients’ active participation in rehabilitation training by reducing pain catastrophizing cognition and sleep disorders.17–20 The decrease in state anxiety scores of family members in the open group in this study reflects the positive impact of improved family psychological states on the quality of doctor-patient communication, consistent with the practice principles of Family-Centered Care (FCC).
Importantly, open visiting did not compromise ICU air quality, with no significant difference between groups (13.17±1.05 vs. 13.21±1.11 cfu/cm2, P > 0.05). This finding supports the feasibility of implementing open visiting under structured infection control measures, consistent with the 2024 ESICM guidelines. The mechanisms for reducing the incidence of delirium involve multi-dimensional interventions including infection control, sleep management, and neural stimulation. Open visiting, while strictly adhering to hand hygiene protocols and the use of protective equipment, has demonstrated controllable infection risks through air quality monitoring. Disruption of the sleep-wake cycle is an important predisposing factor for delirium.21–24 Our findings are broadly consistent with the landmark ICU Visits randomized controlled trial by Rosa et al, which demonstrated that flexible family visitation reduced delirium incidence and improved psychological outcomes in a mixed ICU population. However, that study primarily included acutely ill patients with relatively shorter ICU stays, whereas our cohort comprised exclusively chronic critically ill patients (ICU stay ≥7 days), a group characterized by prolonged treatment courses, higher dependency, and greater susceptibility to psychological stressors. By replicating the benefits of open visiting in this distinct subgroup, our study extends previous evidence and suggests that the advantages of flexible visitation are generalizable to more vulnerable ICU populations.
Importantly, open visiting did not compromise ICU air quality, with no significant difference between groups (13.17±1.05 vs. 13.21±1.11 cfu/cm2, P > 0.05). This finding supports the feasibility of implementing open visiting under structured infection control measures, consistent with the 2024 ESICM guidelines and control strategies. This study, using the airborne bacteria sampling method combined with the culture medium method, validated the controllability of infection risks in open visiting under the conditions of standardized hand hygiene, protective equipment use, and special infection prevention and control measures.25–27 This is consistent with the evolving trend of ICU visiting policies after the COVID-19 pandemic, which emphasizes the development of standardized operating procedures through interdisciplinary collaboration to achieve an ethical balance between ensuring patient safety and realizing visiting rights.
Although this study is based on a retrospective cohort design, it ensures the scientific rigor of the research methodology by strictly matching baseline characteristics (such as core confounding factors including age, gender, and APACHE II score) and adjusting for potential confounding variables using a multivariate logistic regression model, meeting the quality control requirements for observational studies in international medical journals. However, the inherent limitations of the retrospective design still require careful consideration: Firstly, the data are sourced from the electronic medical record system of a single center, which may be subject to information bias (such as unrecorded latent confounding factors) and selection bias (such as population heterogeneity due to non-random time cutoff points). Furthermore, the findings of this single-center study may not be directly generalizable to other healthcare settings. Variations in ICU structure (eg., open vs. closed ICU models), resource availability (eg., nursing staffing ratios, infection control infrastructure), and cultural norms (eg., family involvement expectations) may influence the feasibility and outcomes of open visiting policies. The high level of family engagement observed in our study reflects the cultural context of Chinese tertiary hospitals, where family participation in patient care is deeply valued. Future multicenter studies across diverse settings are needed to assess the external validity of these findings. Secondly, this study did not include long-term outcome indicators (such as 1-year survival rate, quality of life score, readmission rate) and patient-reported outcome (PRO) indicators (such as health-related quality of life, treatment satisfaction), limiting a comprehensive assessment of the long-term clinical value of the open visiting model. Thirdly, the potential value of virtual visiting technologies (such as video calls and remote monitoring) as supplementary visiting methods was not included in the comparative analysis. Although baseline characteristics were comparable between groups and multivariate logistic regression was used to adjust for potential confounders, the time-based group allocation (before vs. after implementation of the open visiting policy) inherently carries the risk of temporal confounding. Unmeasured changes in clinical practice, staff expertise, or patient case mix over the study period may have influenced outcomes independent of the visiting policy. We attempted to mitigate this by ensuring consistent ICU care protocols throughout the study period, but this limitation should be considered when interpreting the findings. Additionally, although the ICU’s clinical management protocols (including sedation strategies, mechanical ventilation weaning protocols, and infection control measures) remained unchanged during the study period, the retrospective time-based design cannot entirely exclude the possibility that other unmeasured temporal changes in clinical practice or staff experience may have contributed to the observed differences. Future prospective studies with concurrent control groups would help address this limitation. Future research should explore integrated visiting models combining online and offline approaches in line with digital healthcare trends. It is worth emphasizing that this study, through air quality monitoring data, confirms that open visiting does not significantly increase infection risks, providing empirical evidence for balancing infection prevention and humanistic care, consistent with the ethical framework for ICU visiting policy formulation in the 2024 ESICM guidelines. Future studies should adopt a multi-center prospective randomized controlled trial design, include long-term outcome indicators and PROs, conduct crossover controlled studies incorporating virtual visiting technologies, and use mixed methodologies integrating quantitative data with qualitative interviews to comprehensively verify the comprehensive benefits of the open visiting model in improving patients’ clinical outcomes, psychological states, and family members’ psychological stress. This will provide higher-level evidence-based medical evidence for optimizing global ICU visiting systems. As a representative of Chinese local data, this study not only fills the gap in research on the effects of visiting models in chronic critical patients but also contributes key evidence to the reform of “patient-centered” visiting policies in the international field of critical care medicine through methodological innovation and mechanism exploration, with significant clinical promotion value and academic leading significance.
Conclusion
This retrospective analysis of 264 chronic critically ill ICU patients found that open visiting, compared with restricted visiting, was associated with shorter mechanical ventilation duration, reduced ICU and hospital stays, higher treatment compliance, improved psychological outcomes (lower HADS scores and family anxiety levels), and a lower incidence of delirium, without compromising ICU air quality. These findings suggest that open visiting may offer clinical and psychological benefits in this patient population.
However, several limitations should be considered. The single-center, retrospective design with time-based group allocation introduces the risk of temporal confounding and selection bias. Although baseline characteristics were comparable and multivariate regression was used to adjust for potential confounders, unmeasured factors may have influenced the results. Additionally, the absence of long-term outcome measures (eg., 1-year survival, quality of life) limits the assessment of sustained benefits.
Given these limitations, our findings should be considered preliminary. Future prospective, multicenter randomized controlled trials are needed to validate the efficacy of open visiting in chronic critically ill patients and to further evaluate its long-term impact on clinical outcomes, patient-reported outcomes, and the potential integration of virtual visiting technologies. Despite its limitations, this study provides a foundation for further investigation and contributes local data from China to the ongoing discourse on optimizing ICU visiting policies.
Acknowledgments
We thank the ICU medical and nursing team for their support in data collection.
Funding
This study was funded by Foshan City Medical Research Project, No. 20250217.
Disclosure
All authors declare no conflict of interest.
References
1. Wang L, Chen R, Dong J, et al. Nutrition support in the chronic critically ill patients. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2021;33(3):381–11. doi:10.3760/cma.j.cn121430-20201010-00665
2. Lan W, Liu E, Sun D, et al. Red cell distribution in critically ill patients with chronic obstructive pulmonary disease. Pulmonology. 2024;30(1):34–42. doi:10.1016/j.pulmoe.2022.04.001
3. Khanna P, Chandralekha C, Pandey RK, et al. Pain assessment in the critically ill mechanically ventilated adult patients: comparison between skin conductance algesimeter index and physiologic indicators. Saudi J Anaesth. 2018;12(2):204–208. doi:10.4103/sja.SJA_489_17
4. Khanna P, Chandralekha C, Pandey RK, et al. Comparison between Critical-Care Pain Observation Tool and physiologic indicators for pain assessment in the critically ill, mechanically ventilated adult patients. Saudi J Anaesth. 2018;12(3):384–388.
5. Minton C, Batten L, Huntington A. The impact of a prolonged stay in the ICU on patients’ fundamental care needs. J Clin Nurs. 2018;27(11–12):2300–2310. doi:10.1111/jocn.14184
6. Sahawneh F, Boss L. Non-pharmacologic interventions for the prevention of delirium in the intensive care unit: an integrative review. Nurs Crit Care. 2021;26(3):166–175. doi:10.1111/nicc.12594
7. Edward H. Family visitation restrictions. Am J Nurs. 2022;122(6):13. doi:10.1097/01.NAJ.0000833868.34163.3f
8. Khandelwal N, Downey L, May P, et al. Risk factors and consequences of financial hardship among family of critically ill patients. Ann Am Thorac Soc. 2025;22(8):1217–1226. doi:10.1513/AnnalsATS.202408-865OC
9. Grau-Carmona T, Bonet-Saris A, García-de-lorenzo A, et al. Influence of n-3 polyunsaturated fatty acids enriched lipid emulsions on nosocomial infections and clinical outcomes in critically ill patients: ICU lipids study. Crit Care Med. 2015;43(1):31–39. doi:10.1097/CCM.0000000000000612
10. Lee A, Cheung YSL, Joynt GM, et al. Are high nurse workload/staffing ratios associated with decreased survival in critically ill patients? A cohort study. Ann Intensive Care. 2017;7(1):46. doi:10.1186/s13613-017-0269-2
11. Hua M, Gong MN, Brady J, et al. Early and late unplanned rehospitalizations for survivors of critical illness*. Crit Care Med. 2015;43(2):430–438. doi:10.1097/CCM.0000000000000717
12. Rosa RG, Falavigna M, da Silva DB, et al. Effect of flexible family visitation on delirium among patients in the intensive care unit: the ICU visits randomized clinical trial. JAMA. 2019;322(3):216–228. doi:10.1001/jama.2019.8766
13. Adrion C, Weiss B, Paul N, et al. Enhanced Recovery after Intensive Care (ERIC): study protocol for a German stepped wedge cluster randomised controlled trial to evaluate the effectiveness of a critical care telehealth program on process quality and functional outcomes. BMJ Open. 2020;10(9):e036096. doi:10.1136/bmjopen-2019-036096
14. Mart MF, Williams Roberson S, Salas B, et al. Prevention and management of delirium in the intensive care unit. Semin Respir Crit Care Med. 2021;42(1):112–126. doi:10.1055/s-0040-1710572
15. Northam KA, Phillips KM. Sedation in the ICU. NEJM Evid. 2024;3(11):EVIDra2300347. doi:10.1056/EVIDra2300347
16. Kotfis K, van Diem-Zaal I, Williams Roberson S, et al. The future of intensive care: delirium should no longer be an issue. Crit Care. 2022;26(1):200. doi:10.1186/s13054-022-04077-y
17. Kang J, Cho YS, Lee M, et al. Effects of nonpharmacological interventions on sleep improvement and delirium prevention in critically ill patients: a systematic review and meta-analysis. Aust Crit Care. 2023;36(4):640–649. doi:10.1016/j.aucc.2022.04.006
18. Moraes FDS, Marengo LL, Moura MDG, et al. ABCDE and ABCDEF care bundles: a systematic review of the implementation process in intensive care units. Medicine. 2022;101(25):e29499. doi:10.1097/MD.0000000000029499
19. Klimasiński MW. Spiritual care in the intensive care unit. Anaesthesiol Intensive Ther. 2021;53(4):350–357.
20. de Souza JMB, Miozzo AP, Da rosa Minho Dos Santos R, et al. Long-term effects of flexible visitation in the intensive care unit on family members’ mental health: 12-month results from a randomized clinical trial. Intensive Care Med. 2024;50(10):1614–1621. doi:10.1007/s00134-024-07577-3
21. Sakusic A, Rabinstein AA. ICU Delirium. Neurol Clin. 2025;43(1):1–13. doi:10.1016/j.ncl.2024.07.001
22. Liu SB, Wu HY, Duan ML, et al. Delirium in the ICU: how much do we know? A narrative review. Ann Med. 2024;56(1):2405072. doi:10.1080/07853890.2024.2405072
23. Kotfis K, Marra A, Ely EW. ICU delirium - a diagnostic and therapeutic challenge in the intensive care unit. Anaesthesiol Intensive Ther. 2018;50(2):160–167. doi:10.5603/AIT.a2018.0011
24. Gómez Tovar LO, Henao Castaño AM. Dynamic delirium - Nursing intervention to reduce delirium in patients critically Ill, a randomized control trial. Intensive Crit Care Nurs. 2024;83:103691. doi:10.1016/j.iccn.2024.103691
25. Bakhru RN, Flores L, Cain JM, et al. A randomized controlled trial of a Post-ICU telehealth care model (WFIT). Am J Respir Crit Care Med. 2025;211(9):1662–1670. doi:10.1164/rccm.202411-2167OC
26. Beerens S, Van Steenkiste L, Egerod I, et al. Expert consensus on research priorities for the prevention of delirium in adult ICU patients. Intensive Crit Care Nurs. 2025;91:104124. doi:10.1016/j.iccn.2025.104124
27. Dos Santos SS, Nassar Junior AP. An outbreak of restrictive intensive care unit visiting policies. Intensive Crit Care Nurs. 2022;68:103140. doi:10.1016/j.iccn.2021.103140
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.