Back to Journals » Advances in Medical Education and Practice » Volume 16
Comparison of Online-to-Offline Teaching Rounds and Bedside Teaching Rounds in Nephrology Residency Training
Authors Han B, Yang F, Yang M, Yang Q, Xiong Y, Ma K
Received 18 June 2025
Accepted for publication 24 October 2025
Published 19 November 2025 Volume 2025:16 Pages 2115—2122
DOI https://doi.org/10.2147/AMEP.S548103
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Bin Han,1 Fuye Yang,1 Muying Yang,2 Qiongying Yang,1 Yabing Xiong,1 Kunling Ma1
1Department of Nephrology, The Second Affiliated Hospital of Zhejiang University School of Medicine, Hangzhou, Zhejiang, People’s Republic of China; 2Department of Nursing, The Second Affiliated Hospital of Zhejiang University School of Medicine, Hangzhou, Zhejiang, People’s Republic of China
Correspondence: Kunling Ma, Department of Nephrology, The Second Affiliated Hospital of Zhejiang University School of Medicine, No. 88 Jiefang Road, Hangzhou, Zhejiang, 310009, People’s Republic of China, Email [email protected]; [email protected]
Background: Most surveys today show a marked decline in traditional beside teaching rounds (BTR) in medical education. The online-to-offline (O2O) teaching mode has been associated with improvement of academic performance of learners. This study aimed to compare the O2O teaching rounds (O2OTR) with BTR on a nephrology inpatient service and assess efficiency and satisfaction among residents.
Methods: A total of 79 trainees who participated in the nephrology residency training, were randomized either to the O2OTR group or the BTR group (control). Theoretical knowledge tests, clinical case scenarios, and questionnaires were integrated to systematically assess the teaching efficacy.
Results: Thirty-eight residents were assigned to the O2OTR group, while the other 41 were assigned to the BTR group. Baseline demographics and performance were comparable between groups. Residents in the O2OTR group demonstrated superior performance in clinical case scenarios compared to those in the BTR group (P < 0.001) at 2 months after teaching. Moreover, O2OTR residents expressed more positive attitudes toward their clinical thinking proficiency (P < 0.001), and exhibited higher satisfaction with their teaching rounding style (P = 0.004) than their BTR counterparts.
Conclusion: This study suggests that the O2OTR mode serves as an effective and alternative approach in the nephrology residency training.
Keywords: online-to-offline, teaching rounds, bedside, residency training, nephrology
Introduction
Standardized residency training (SRT) program, as an important component of postgraduate medical education, is the first mandatory stage of training highly competent physicians.1,2 Since the first residency training program under the supervision of William Osler, bedside teaching rounds (BTR), the process where care review and medical plan among healthcare providers take place in the presence of the patient, has been viewed as a comprehensive practical teaching activity.3 The practice of BTR may provide opportunities for exercising residents’ clinical thinking abilities and professionalism.4,5
Despite its rhetorical and theoretical benefits, a substantial number of factors have led to a decline in the bedside teaching.6–9 Technological advancements have shifted the diagnostic process away from the bedside and towards laboratory testing and imaging,9 which has led some healthcare providers to question the utility of bedside diagnosis.10 The electronic medical record (EMR) has enhanced information accessibility, thus leading physicians to now often spend more time caring for digital representations of the patient than the actual person.11,12 Studies demonstrated that internal medicine residents spend as little as 12% of their learning time in direct contact with patients.13,14 Recently, a prospective and observational survey revealed that only 17% of teaching time for internal medicine residents involved interaction with patients at the bedside.7 Boyle et al found that only 30% of trainees examined the patients with the attending at the bedside in the Department of Nephrology.15 Other barriers to the bedside teaching included pressure to reduce length of stay, concern for patient discomfort, and insufficient time to teach, particularly in the context of duty-hour constraints of residents.16,17 As a result, these challenges mentioned above have prompted educators and trainees to seek more efficient and innovative patterns of teaching rounds.
Driven by rapid advancements in information technology and educational innovation, the mixed online-to-offline (O2O) teaching model has demonstrated increasingly prominent advantages.18 The O2O pattern initially emerged in the field of e-commerce, defined as a business paradigm using digital platforms to drive offline transactions and consumption.19 The O2O teaching pattern was a combination of the online teaching and traditional offline teaching, leveraging network technology and digital platforms.20,21 Emerging studies have shown that using the O2O teaching pattern in teaching of English,22 computer science23 and medical educaition24–26 have yielded significant outcomes, such as improvement of participants’ learning enthusiasm and academic performance. However, studies on application of the O2O model in teaching rounds are lacking. To fill the gap in nephrology education research, we performed a prospective interventional study that compared the O2O teaching rounds (O2OTR) with traditional BTR in the Department of Nephrology, with the aim of ascertaining which rounding practice is associated with superior teaching efficiency and higher trainee satisfaction.
Methods
Participants
A total of 79 internal medicine trainees were consecutively enrolled from the Department of Nephrology of the Second Affiliated Hospital of Zhejiang University School of Medicine in Hangzhou, China. These residents underwent a two-months Standardized Internal Medicine Training Program in the nephrology department between Jun 1, 2023, to July 30, 2024. Eligibility criteria were as follows: (i) attended the hospital for standardized internal medicine training program; (ii) first time to attend the clinical rotation in the nephrology department, and (iii) having a presence of 90% or more during the rotation period. Exclusion criteria included (i) an absence rate of over 10% during the rotation period; (ii) refusing participation, and (iii) dropping out for other reasons.
Study Design
We conducted a single-center prospective randomized study of O2OTR vs BTR in a two-months nephrology residency training. Before the initiation of the study, we educated attending physicians, nephrology residents, and nurses about traditional BTR and O2OTR through voluntary conference presentations. All residents were required to take examinations containing the theoretical knowledge test and clinical case scenarios related to nephrology. The baseline performance of residents was evaluated according to the results of the examinations. All residents were randomly assigned either to the BTR group or the O2OTR group (Figure 1), each with 1 attending physician and 2–3 residents. The participants in this study included nephrology residents, attending physicians, nurses, and newly admitted nephrology patients. The attending physicians were experienced teachers in clinical teaching and were trained before teaching. The BTR team p Please describe the timing of online pre-learning relative to roundsresented medical history, performed physical examination, and discussed summarized results and subsequent medical plans at the bedside with encouragement of patient’s participation. The O2OTR team published the patient history through the Chinese university Massive Open Online Courses (MOOC) platform,27 and residents were expected to take about 30 min to use flexible intelligent devices to complete independent learning and then enter offline process with thinking and problems. The O2OTR team performed physical examination in the room, followed by discussion of medical plans through Ding Talk, a widely used online office platform in China.28 DingTalk live broadcast was initiated and hosted by the attending physician, with a total duration of approximately 1 hour. Theoretical knowledge tests, clinical case scenarios, and questionnaires were used to assess teaching efficacy and trainee satisfaction.
 |
Figure 1 Study design. Abbreviations: BTR, bedside teaching rounds; O2OTR, online-to-offline teaching rounds. |
The study protocol was approved by the Institutional Review Board and Ethics Committee of the Second Affiliated Hospital of Zhejiang University School of Medicine (2023–0989). We provided participating residents, attending physicians, nurses, and patients with a study handout and information sheet. All participants involved in the present study signed informed consent forms.
Assessment
To evaluate the teaching efficacy, residents of both groups were required to take examinations containing theoretical knowledge test and clinical case scenario, each with a full score of 100 points, according to the outline of residency training of nephrology. The examinations were performed on the last day of the rotation in the Department of Nephrology. The results of the examinations were employed as objective indicators of evaluation. The theoretical knowledge test utilized a multiple-choice question format, with each question assigned equal weighting. The residents were required to engage in clinical practice as nephrology physicians do in the clinical case scenarios, encompassing medical history collection, physical examination, record writing, clinical thinking, and patient care. The scenarios used for examination were never displayed in the teaching process for residents in the two groups. Moreover, the clinical case scenarios were the same between groups. Ultimately, the residents were scored based on their performance. All residents were required to complete an anonymous questionnaire online, which aimed to examine their perspectives and experiences regarding the teaching rounding patterns using a five-point Likert scale. The questionnaire items covered aspects about medical history collection, physical examination, record writing, clinical thinking, and care for patients, as well as time spent for the class, and satisfaction with the teaching method. The questionnaire was adapted from Paul Ramsden’s Course Experience Questionnaire and Biggs’ Study Process questionnaire, both of which have been verified for reliability and validity.29 The whole examination process was under the supervision of the residency training secretary of the Department of Nephrology and the Supervisory Committee of the Medical Residency Training Program, ensuring compliance with the established standards. Independent observers tabulated data into a spreadsheet. Data collected from both independent observers was aggregated for ease of analysis.
Statistical Analyses
All data were presented as mean ± standard deviation of mean (SD) or umber (percentage). All analyses were performed using SPSS for windows (SPSS Inc., Chicago, IL, USA) version 22. Differences in variables by teaching round styles were performed using independent sample t-test or Mann–Whitney U-test for continuous data and Pearson’s Chi-squared test for categorical data. Independent sample t test was used for the variables with normal distributions and homogeneity, while Mann–Whitney U-test was performed for parametric variables with non-normal distributions or non-homogeneity. In the present study, a P-value of <0.05 was considered statistically significant.
Results
Characteristics of Participants
Of 90 nephrology residents at baseline, 11 were excluded from this analysis: 7 refusing to participate in this study, 3 with absence rate of >10% during the rotation period, and 1 dropping out for other reasons. Finally, the study cohort in this study contained 79 nephrology residents (49 female, 30 male) with a mean age of 30.68 years. There were no significant differences in gender and age between our cohort and those excluded. Thirty-eight residents were randomly assigned to the O2OTR group, while the other 41 were randomly assigned to the BTR group. There were no significant differences between the two groups in gender, age, marital status, education, and household income (Table 1).
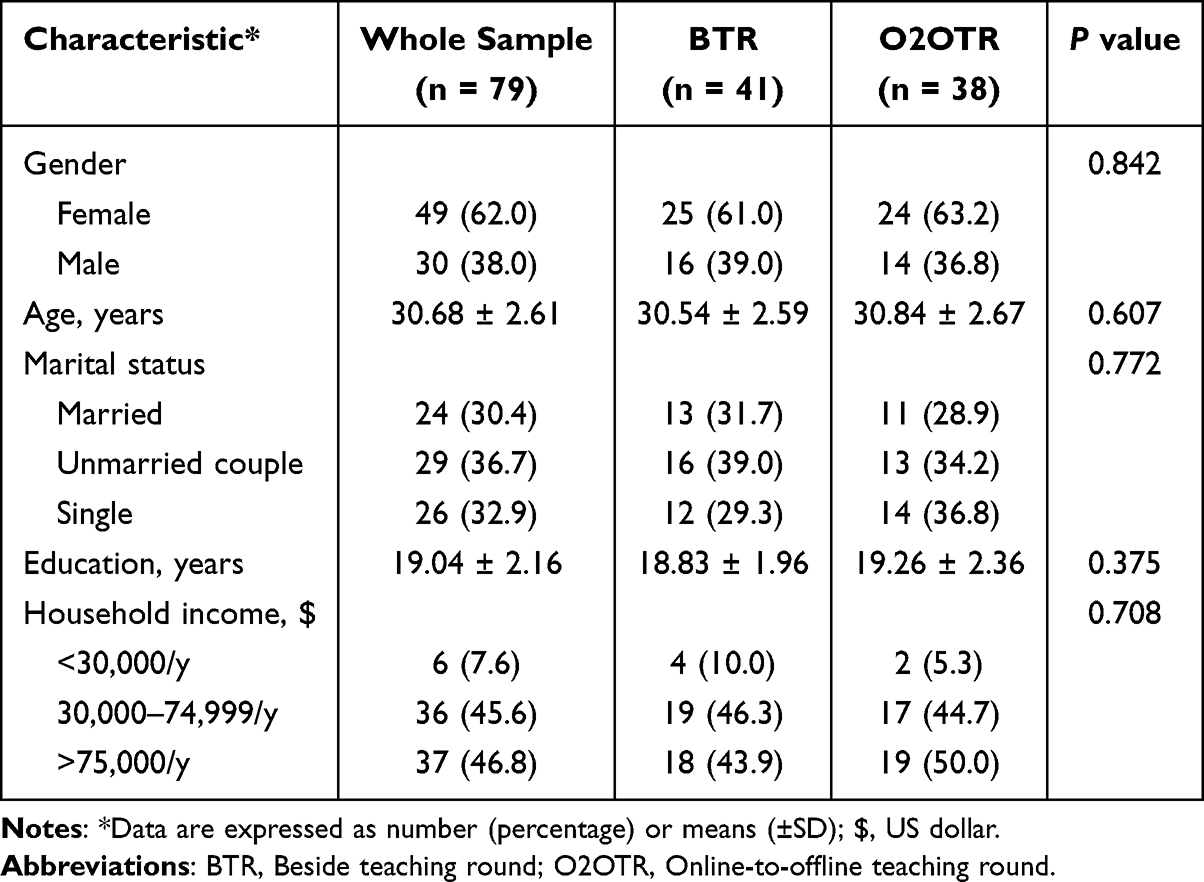 |
Table 1 Characteristics of Participants in the Present Study |
Performance of Participants
We assessed baseline performance of residents through the examinations consisting of theoretical knowledge and clinical case scenarios. The scores of the examinations were analyzed and the results revealed no significant differences between the O2OTR group and the BTR group (Figure 2A and B). At 2 months after the teaching, the average score of the theoretical knowledge test in the O2OTR group was 80.12 ± 4.23, while the average score was 79.46 ± 3.28 in the BTR group, revealing a similar performance in the two groups (P = 0.415, Figure 3A). However, residents in the O2OTR group shown a superior performance to those in the BTR group in terms of the clinical case scenarios (71.87 ± 3.22 vs 67.80 ± 3.65, P < 0.001), as displayed in Figure 3B.
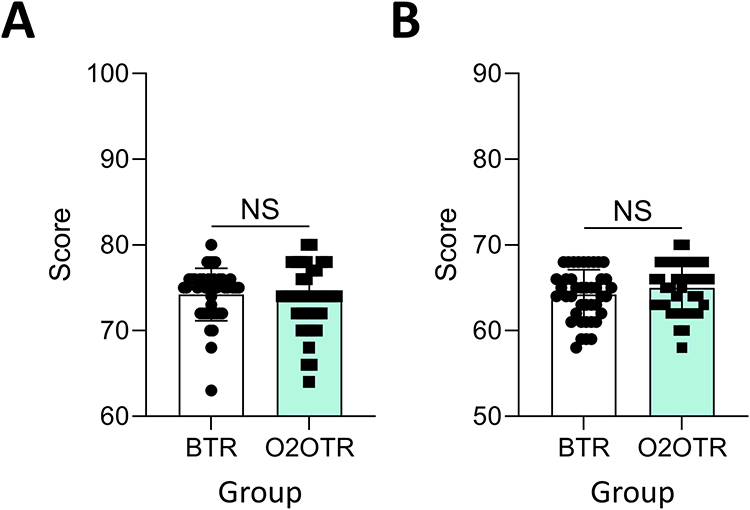 |
Figure 2 Performance of residents at baseline. (A) Theoretical knowledge test between groups; (B) Examination of clinical case scenarios between groups. Abbreviations: NS, no statistical significance, BTR, bedside teaching rounds; O2OTR, online-to-offline teaching rounds. |
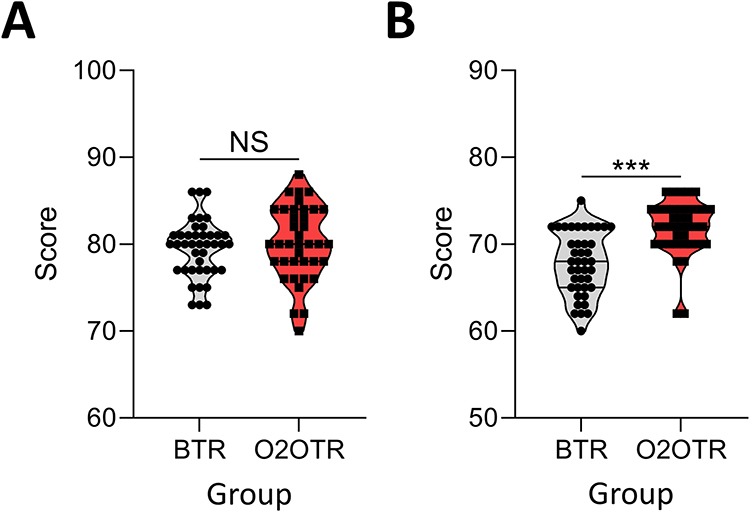 |
Figure 3 Comparison of residents’ performance between groups at 2 months. (A) Theoretical knowledge test between groups; (B) Examination of clinical case scenarios between groups. *** P < 0.001. Abbreviations: NS, no statistical significance; BTR, bedside teaching rounds; O2OTR, online-to-offline teaching rounds. |
Experience Survey of Participants
Residents’ perceptions and experiences were assessed using an anonymous questionnaire. In the present study, a total of 79 questionnaires were distributed and all 79 were received. The Cronbach’s alpha value for the positive-oriented items of the questionnaire was determined to be 0.84, suggesting that the questionnaire exhibited satisfactory internal consistency and reliability. There were no significant differences in medical history collection, physical examination, record writing, care for patients, and time spent for the class between the two groups (all P > 0.05, Figure 4). However, residents in the O2OTR group provided a more positive perception of improving the clinical thinking abilities of (4.73 ± 0.45 vs 4.24±0.70, P < 0.001) when compared to those in the BTR group. Of important, the O2OTR residents exhibited higher satisfaction with their teaching rounding styles (4.08 ± 0.43 vs 3.76 ± 0.54, P = 0.004) than their BTR counterparts, as shown in Figure 4.
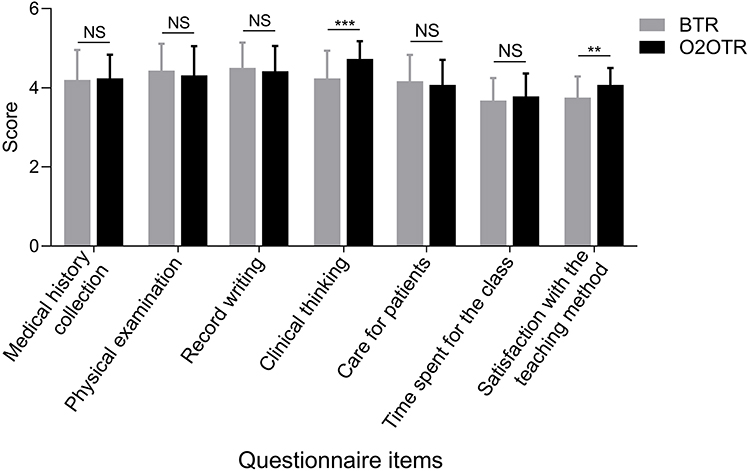 |
Figure 4 Residents’ perspectives on the teaching rounding pattern. ** P < 0.01; *** P < 0.001. Abbreviations: NS, no statistical significance; BTR, bedside teaching rounds; O2OTR, online-to-offline teaching rounds. |
Discussion
Nephrology is a comprehensive and highly practical discipline that is a crucial component of standardized residency training in internal medicine. Despite amounts of changes in medical education, teaching rounds remain a core part of experiences of trainees.30,31 However, studies have shown a marked decline in teaching rounds, BTR in particular, resulting from barriers such as dependence of diagnosis on technology, insufficient time to teach, introduction of the electronic medical record, and pressure to reduce length of stay.9,11,12,32 Therefore, novelty teaching rounding mode should be explored to enhance teaching quality and strengthen residents’ clinical thinking abilities and problem-solving competencies.
In the post-COVID-19 pandemic era, the single online or offline teaching mode fails to satisfy the needs of medical education. The O2O teaching refers to an innovative pattern that integrates the online teaching with traditional offline teaching, which both have advantages of accessibility and efficiency of the online teaching and environmental experience of the offline teaching. It has been proven that the O2O teaching mode was associated with learners’ increased learning enthusiasm and enhanced academic performance.22–26 Ding Talk, an online office platform widely used in the Second Affiliated Hospital of Zhejiang University School of Medicine, make it convenient to start a live stream for teaching, meeting, and remote consultation.28 The platform supports live playback of the teaching rounds, enabling repeated viewing to consolidate learning outcomes. In the present study, we applied the O2O mode in the teaching rounds of the residency training of nephrology, publishing the patient history through the Chinese university MOOC platform, performing physical examination and care review at the bedside, and finally discussing diagnosis and medical plans through Ding Talk network platform.
We found that residents in the O2OTR group scored higher than their counterparts in the BTR group for examinations of the clinical case scenarios at 2 months post-teaching. The residents from both groups exhibited comparable performance in the theoretical knowledge test. Notably, the baseline performances between the two groups were similar. Collectively, the O2OTR mode enhanced residents’ capacity for translating textbook knowledge to real-world clinical scenarios. Subsequently, feedback was collected from residents regarding the O2OTR mode in nephrology teaching rounds. The residents felt that the O2OTR mode helped them to enhance their clinical thinking abilities. Notably, residents enrolled in the O2OTR group showed higher satisfaction with the teaching method, while reporting no significant increase in learning time commitment. This phenomenon may be partly attributed to the teaching mode having advantages of the accessibility and efficiency of online teaching and the environmental experience of offline teaching. The time and space for learning of trainees were greatly expanded in the O2OTR teaching mode.33 Moreover, attending physicians and trainees can communicate and interact online, which will be conducive to establishing a harmonious teacher-student relationship.
This study had several limitations. First, we failed to blind the research participants, who were able to identify the pattern being used during the teaching rounding. But we ensured those who assessed the tests were unaware of the grouping. Second, this study was conducted exclusively within a single institutional setting, involving a relatively small sample of residents. Further research is warranted within larger sample cohorts across multiple centers. Third, the training time in the Department of Nephrology is relatively short, which did not allow for a crossover study, and might potentially yield bias in this study. Finally, we focused specifically on the teaching rounds with physician trainees in the hospital setting. Therefore, the findings of this study may not be generalized to other clinical settings (eg, the outpatient) or different trainee populations (eg, surgery or pharmacy learners).
Conclusion
The O2OTR mode offers a superior, evidence-based alternative to traditional BTR in the nephrology residency training. This approach motivates residents’ learning initiative and enhances their clinical thinking abilities. Future multi-center studies are warranted to validate its effectiveness across diverse institutions and trainee populations.
Acknowledgments
We are grateful to all residents enrolled in this study for their cooperation.
Funding
This study was funded by the Teaching Reform and Cultivation Project of the Second Clinical Medical College of Zhejiang University (20220222-01).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lio J, Dong H, Ye Y, Cooper B, Reddy S, Sherer R. Standardized residency programs in China: perspectives on training quality. Int J Med Educ. 2016;7:220–221. doi:10.5116/ijme.5780.9b85
2. Johnson GJ, Kilpatrick CC, Zaritsky E, et al. Training the next generation of obstetrics and gynecology leaders, a multi-institutional needs assessment. J Surg Educ. 2021;78(6):1965–1972. doi:10.1016/j.jsurg.2021.06.010
3. Peters M, Ten Cate O. Bedside teaching in medical education: a literature review. Perspect Med Educ. 2014;3(2):76–88. doi:10.1007/S40037-013-0083-Y
4. Gonzalo JD, Heist BS, Duffy BL, et al. The value of bedside rounds: a multicenter qualitative study. Teach Learn Med. 2013;25(4):326–333. doi:10.1080/10401334.2013.830514
5. Narayanan V, Nair BR. The value of bedside teaching in undergraduate medical education: a literature review. MedEdPublish. 2020;9:149. doi:10.15694/mep.2020.000149.1
6. Ahmed H, King AB, Mohamed N, Mokaya E, Chapman K, Leonard R. Perception versus reality: analysis of time spent on bedside rounds in an academic ICU (Intensive care unit). BMC Med Educ. 2023;23(1):274. doi:10.1186/s12909-023-04243-y
7. Crumlish CM, Yialamas MA, McMahon GT. Quantification of bedside teaching by an academic hospitalist group. J Hosp Med. 2009;4(5):304–307. doi:10.1002/jhm.540
8. Garibaldi BT, Russell SW. Strategies to improve bedside clinical skills teaching. Chest. 2021;160(6):2187–2195. doi:10.1016/j.chest.2021.06.055
9. Garout M, Nuqali A, Alhazmi A, Almoallim H. Bedside teaching: an underutilized tool in medical education. Int J Med Educ. 2016;7:261–262. doi:10.5116/ijme.5780.bdba
10. Bergl P, Farnan JM, Chan E. Moving toward cost-effectiveness in physical examination. Am J Med. 2015;128(2):109–110. doi:10.1016/j.amjmed.2014.10.003
11. Chi J, Verghese A. Clinical education and the electronic health record: the flipped patient. JAMA. 2014;312(22):2331–2332. doi:10.1001/jama.2014.12820
12. Verghese A. Culture shock--patient as icon, icon as patient. N Engl J Med. 2008;359(26):2748–2751. doi:10.1056/NEJMp0807461
13. Block L, Habicht R, Wu AW, et al. In the wake of the 2003 and 2011 duty hours regulations, how do internal medicine interns spend their time? J Gen Intern Med. 2013;28(8):1042–1047. doi:10.1007/s11606-013-2376-6
14. Desai SV, Asch DA, Bellini LM, et al. Education outcomes in a duty-hour flexibility trial in internal medicine. N Engl J Med. 2018;378(16):1494–1508. doi:10.1056/NEJMoa1800965
15. Boyle SM, Subedi K, Pivert KA, et al. Nephrology fellows’ and program directors’ perceptions of hospital rounds in the United States. Clin J Am Soc Nephrol. 2020;15(4):474–483. doi:10.2215/CJN.10190819
16. Gonzalo JD, Heist BS, Duffy BL, et al. Identifying and overcoming the barriers to bedside rounds: a multicenter qualitative study. Acad Med. 2014;89(2):326–334. doi:10.1097/ACM.0000000000000100
17. Khan MA, Rajendram R, Al-Jahdali H, et al. Do ward rounds offer effective teaching and training? Obstacles to learning and what makes good teaching in a large tertiary care hospital from trainee doctor’s perspective. GMS J Med Educ. 2021;38(6):Doc106. doi:10.3205/zma001502
18. Vallee A, Blacher J, Cariou A, Sorbets E. Blended learning compared to traditional learning in medical education: systematic review and meta-analysis. J Med Internet Res. 2020;22(8):e16504. doi:10.2196/16504
19. He B, Mirchandani P, Shen Q, Yang G. How should local brick-and-mortar retailers offer delivery service in a pandemic world? Self-building vs. O2O platform. Transp Res E Logist Transp Rev. 2021;154:102457. doi:10.1016/j.tre.2021.102457
20. Cheng X, Mo W, Duan Y. Factors contributing to learning satisfaction with blended learning teaching mode among higher education students in China. Front Psychol. 2023;14:1193675. doi:10.3389/fpsyg.2023.1193675
21. Xu Y, Wang L, Li P, et al. Exploring the impact of online and offline teaching methods on the cognitive abilities of medical students: a comparative study. BMC Med Educ. 2023;23(1):557. doi:10.1186/s12909-023-04549-x
22. Zhang Y. Analysis of O2O teaching assistant mode of college english in MOOC environment. J Environ Public Health. 2022;2022:8164934. doi:10.1155/2022/8164934
23. Zhang X, Zhang B, Zhang F. Student-centered case-based teaching and online-offline case discussion in postgraduate courses of computer science. Int J Educ Technol High Educ. 2023;20(1):6. doi:10.1186/s41239-022-00374-2
24. Wu J, Ke Y, Chen Z, Alhendi MA, Zhu L, Ma K. Online-to-offline combined with problem-based learning is an effective teaching modality in the standardized residency training of nephrology. BMC Med Educ. 2024;24(1):712. doi:10.1186/s12909-024-05675-w
25. Zhao YY, Zhang TT, Li LH, et al. Application of online to offline teaching mode in the training of non-anesthesiology residents in the department of anesthesiology: a randomized, controlled trial. Front Med (Lausanne). 2024;11:1329538. doi:10.3389/fmed.2024.1329538
26. Peng W, Wang S. Online-offline teaching for bio-pharmaceutical students during the COVID-19 pandemic: the case study of advanced mathematics in application-oriented universities of China. Front Public Health. 2022;10:911117. doi:10.3389/fpubh.2022.911117
27. Dong L, Yang L, Li Z, Wang X. Application of PBL mode in a resident-focused perioperative transesophageal echocardiography training program: a perspective of MOOC environment. Adv Med Educ Pract. 2020;11:1023–1028. doi:10.2147/AMEP.S282320
28. Xu T, Gao Q, Ge X, Lu J. The relationship between social media and professional learning from the perspective of pre-service teachers: a survey. Educ Inf Technol. 2023;2023:1–26.
29. Broomfield D, Bligh J. An evaluation of the ‘short form’ course experience questionnaire with medical students. Med Educ. 1998;32(4):367–369. doi:10.1046/j.1365-2923.1998.00232.x
30. Shoeb M, Khanna R, Fang M, et al. Internal medicine rounding practices and the accreditation council for graduate medical education core competencies. J Hosp Med. 2014;9(4):239–243. doi:10.1002/jhm.2164
31. Wang S, Chen W, Ma J, Zhan J. Thoughts on teaching ward round in the standardized training of anesthesiology residents. Asian J Surg. 2024;47(6):2788–2789. doi:10.1016/j.asjsur.2024.02.068
32. Laskaratos FM, Wallace D, Gkotsi D, Burns A, Epstein O. The educational value of ward rounds for junior trainees. Med Educ Online. 2015;20(1):27559. doi:10.3402/meo.v20.27559
33. Yu H, Wang S, Li J, Shi G, Yang J. Influence of online merging offline method on university students’ active learning through learning satisfaction. Front Psychol. 2022;13:842322. doi:10.3389/fpsyg.2022.842322
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.