Back to Journals » Nature and Science of Sleep » Volume 18

Comparison of Intraoperative Noise Isolation and White Noise on Postoperative Sleep in Patients Undergoing Flexible Ureteroscopic Holmium: YAG Laser Lithotripsy: A Randomized Clinical Trial
Authors Dai W, Wang XY ![]() , Yang R
, Yang R ![]()
Received 7 October 2025
Accepted for publication 9 January 2026
Published 24 January 2026 Volume 2026:18 571531
DOI https://doi.org/10.2147/NSS.S571531
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 6
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Wei Dai,* Xin-yue Wang,* Rui Yang
Department of Anesthesiology, The First Affiliated Hospital of Anhui Medical University, Hefei, Anhui, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Rui Yang, Department of Anesthesiology, The First Affiliated Hospital, Anhui Medical University, 218 Jixi Road, Hefei, Anhui, 230022, People’s Republic of China, Tel +86-0551-62922344, Fax +86 0551 62923704, Email [email protected]
Background: The constantly rising noise level in the operating theatre is not only a heavy burden for healthcare providers but also a threat to patients undergoing general anesthesia. Noise isolation and white noise are two distinct methods for mitigating noise during surgery. Improved sleep quality has a positive effect on patients’ postoperative recovery and comfort. This study aimed to compare the effects of the two methods mentioned above on postoperative sleep quality in patients undergoing flexible ureteroscopic Holmium: YAG laser lithotripsy.
Methods: A total of 90 patients who were scheduled to undergo flexible ureteroscopic Holmium: YAG laser lithotripsy were included in the study. All patients were randomly assigned to Group N (noise isolation) and Group W (white noise). The primary outcome was the sleep quality scores of patients in both groups on the first postoperative night, which were measured using the Richard Campbell Sleep Scale. Secondary outcomes included pain scores at rest and during activity 24 hours after surgery, intraoperative propofol consumption, and length of postoperative hospital stay in both groups.
Results: On the first postoperative night, the sleep quality scores reported by patients in Group N were higher than those of patients in Group W (P=0.009). There was no difference in pain scores at rest and during activity between the two groups 24 hours after surgery (P=0.234, P=0.753). The consumption of propofol during surgery in Group N was lower than that in Group W (P=0.005). The postoperative hospital stay of patients in Group N was shorter than that of patients in Group W(P=0.022).
Conclusion: For patients undergoing flexible ureteroscopic Holmium: YAG laser lithotripsy under general anesthesia, noise isolation has potential advantages in reducing the consumption of propofol during surgery and improving the quality of sleep on the first night after surgery compared to playing white noise in noise-cancelling headphones.
Clinical Trial Registration: This study has also been registered with the Chinese Clinical Trial Registry (ChiCTR2500097807). Date of registration: February 26, 2025.
Keywords: noise isolation, white noise, flexible ureteroscopic holmium: YAG laser lithotripsy, sleep, pain
Introduction
Due to the introduction of various new types of medical instruments into surgical procedures, the noise level in the operating theatre has far exceeded our previous understanding. A study on the commonly used instruments in the operating theatre confirmed that the average noise level during surgery was greater than 85 decibels (dB).1 Different types of surgeries result in different levels of noise. For instance, the noise range reported in total knee arthroplasty was 92–104 dB (sound of motorcycle),2 while the noise intensity generated by the instruments used in otolaryngology theatres could reach up to 131dB (sound of aircraft engine).3 Exposure to a noisy environment can lead to the activation of the sympathetic nervous system and an increase in stress hormone levels.4 This further shortens sleep duration and reduces sleep quality.5
Flexible ureteroscopic Holmium: YAG (Ho: YAG) laser lithotripsy, considered the gold standard, is the most commonly employed surgical technique for kidney stone patients. The noise generated by the device includes baseline noise during idle use and additional noise during device activation. As reported by Moore et al, the holmium laser device produced sound that varied widely in level, with peak levels intermittently reaching 91.2 dB.6 During this surgery, the surgeons, anesthesiologists, and nurses all struggled due to exposure to high-level noise, which was a significant occupational health and safety risk.7 Strategies for managing noise in operating rooms involve stopping noise from being produced and blocking it from reaching the ears.8 Several studies have focused on how to reduce the noise level in the operating room to improve communication among the operating room staff and reduce occupational exposure.9,10 Nonetheless, the measures to address noise exposure for patients during surgery remain inadequate.
Previous Studies have confirmed that the auditory cortex of patients undergoing general anesthesia remains active during this period.11,12 A systematic review has confirmed that even with adequate general anesthesia in clinical practice, intraoperative auditory stimuli can be perceived and processed by patients, leading to the formation of implicit memory without explicit consciousness.13 Thus, patients undergoing flexible ureteroscopic Holmium: YAG laser lithotripsy may experience the same noisy environment as the healthcare providers. The noise isolation during the surgery might have a potential positive role in such patients. Nonetheless, there are always two approaches to counteract noise interference: blocking the noise or amplifying the background music to overshadow it. Intraoperative auditory stimuli has been reintroduced in recent years. Fu et al concluded that intraoperative music has a positive effect on patients’ postoperative pain and the demand for analgesics.13
Intraoperative music, white noise, and therapeutic suggestions have been used as auditory stimuli in patients undergoing general anesthesia.14–16 The researchers concluded that the auditory stimuli mentioned above had a positive effect on postoperative pain in patients receiving general anesthesia. However, the effect of intraoperative auditory stimuli on the postoperative sleep quality of patients receiving general anesthesia remains unclear. In daily life, white noise has been increasingly used to improve sleep based on its auditory masking effect.17 Ebben et al have confirmed that white noise can significantly improve the sleep of subjects who complain of sleep difficulties due to high levels of environmental noise.18 We speculated that intraoperative white noise might achieve a similar effect on postoperative sleep quality in patients undergoing general anesthesia. Although intraoperative noise isolation and intraoperative white noise have both been studied separately, conducting a head-to-head comparison in the urological surgical population we studied holds unique value.
In this study, we investigated the differences in sleep quality on the night after surgery between intraoperative noise isolation and intraoperative white noise in general anesthesia patients receiving flexible ureteroscopic Holmium: YAG laser lithotripsy. We hypothesized that intraoperative noise isolation was superior to intraoperative white noise in improving sleep on the first night after surgery.
Methods
Before enrolling patients, we registered this experiment with the Chinese Clinical Trial Registry and obtained approval (ChiCTR2500097807). Ethical approval was obtained from our hospital’s Ethical Committee (PJ2024-12-34). Written consent was obtained from all patients for participation in this study.
During the visit one day before surgery, demographic data for all subjects were recorded. The Richards Campbell Sleep Questionnaire (RCSQ) was employed to assess the preoperative sleep quality of all subjects.19 Using a 0–100 mm visual analog scale, the RCSQ is a six-domain questionnaire designed to measure subjective sleep quality, covering sleep depth, sleep latency, awakenings, sleep efficiency, sleep quality, and noise perception. For the first five domains, the higher the score, the higher the quality. The patient’s sleep quality score is the average score of the first five domains. For the sixth domain, a higher score indicates a quieter environment. Screening was conducted on 123 patients older than 40 years with American Society of Anesthesiologists (ASA) grade I-III, all of whom were scheduled for flexible ureteroscopic Holmium: YAG laser lithotripsy. Ninety patients finally participated in our study. The Consolidated Standards of Reporting Trials (CONSORT) diagram is shown (Figure 1).20 The exclusion criteria included severe sleep disturbances before surgery, alcohol or drug abuse, hearing impairment, taking medication that may interfere with sleep, and any factors that might hinder the completion of the study. Enrolled subjects were randomly assigned to Group N (noise isolation group) and Group W (white noise group) using random number sequence. The randomization sequence was generated by an assistant who was remote to the procedure using a computer. The group allocation was sealed in an opaque envelope by the chief resident. Only the postoperative follow-up staff were blinded to the group allocation.
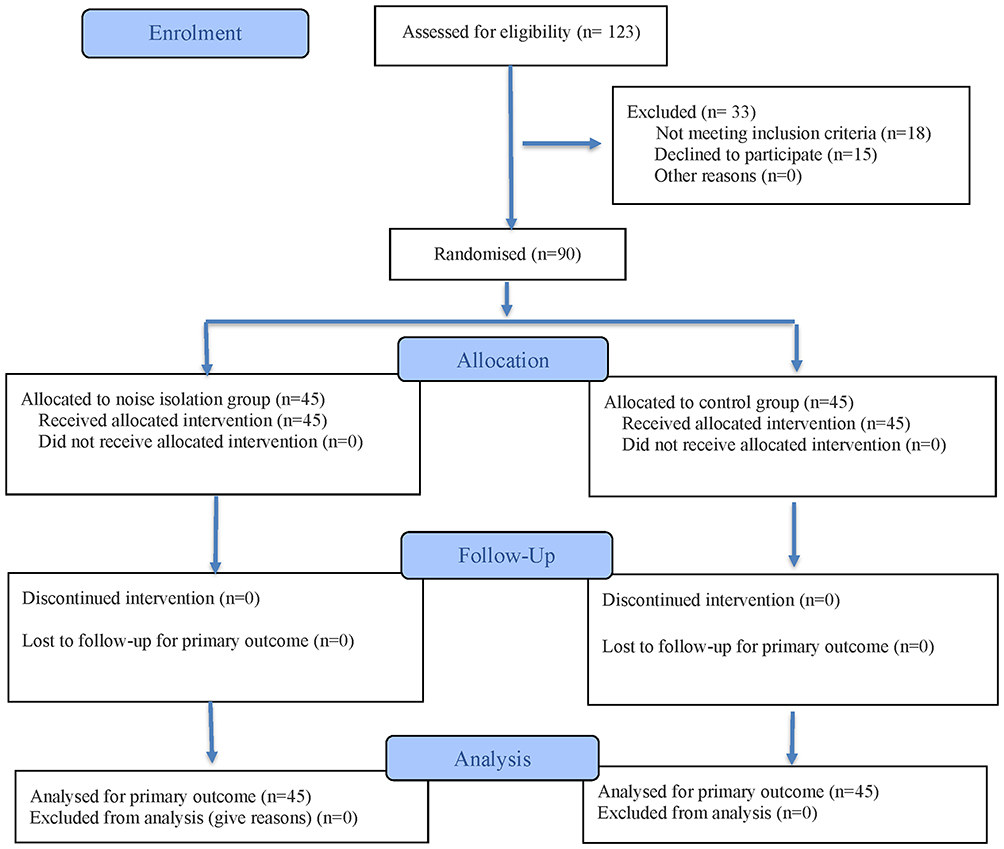 |
Figure 1 CONSORT 2025 Flow Diagram. Notes: CONSORT figure adapted from Hopewell S, Chan AW, Collins GS et al. CONSORT 2025 statement: updated guideline for reporting randomised trials. BMJ. 2025;389:e08112320. |
Study Protocol
Intravenous access was established after the subject arrived in the operating theatre. Standard monitoring comprised heart rate, oxygen saturation, noninvasive blood pressure, electrocardiogram, capnography, and bispectral index (BIS) measurement. Before general anesthesia induction, subjects in Group N wore earplugs (3M™E-A-Rsoft™ Yellow Neons™ 312–1250, USA, signal noise reduction of 33 dB) and confirmed satisfactory noise isolation effect. Subjects in Group W wore noise-cancelling headphones (WH-1000XM3; Sony, Tokyo, Japan) before general anesthesia induction and connected them to a smartphone (Xiaomi 14, Android 15, Xiaomi Inc., China) via Bluetooth. The equipment used for the intervention received by the two groups of subjects were shown in Figure 2. White noise was generated by Audacity software (Audacity Team) and presented as a stereo signal. The audio was recorded at a sampling rate of 48000 Hz, digitized to 16 bits, and saved in an uncompressed.wav file format. The UNI-T UT351 sound level meter was used to set the noise level to 50dB. The experimental assistant played the white noise at the set noise level via the smartphone and ensured that all subjects could hear it through noise-cancelling headphones. The smartphone was placed at the head of all subjects’ operating beds. Then, general anesthesia was initiated using midazolam (0.02–0.05mg/kg), etomidate (0.2–0.3 mg/kg), sufentanil (0.3–0.5 μg/kg), and cis-atracurium (0.2–0.3 mg/kg). Subsequently laryngeal mask airway was inserted. Maintenance of anesthesia was achieved through the infusion of propofol and remifentanil. The initial infusion rate of propofol was 5mg/kg/h. The infusion rate of propofol was titrated appropriately according to the increase or decrease of the BIS value (1–2mg/kg/h per time). The sedation depth was maintained at a BIS value between 40 and 60 by titrating the infusion rate of propofol. All subjects received flurbiprofen axetil 50mg before the end of surgery. After the surgery was completed, the earplugs of subjects in Group N and the noise-cancelling headphones of subjects in Group W were removed. All subjects were then transferred to the post-anesthesia care unit (PACU). All subjects were discharged from the PACU when their Aldrete scores were ≥ 9. After the subjects were transferred to the ward, each subject was only allowed to be accompanied by one escort. After dark, the room light was adjusted to soft light, and after 9 pm, the room light was turned off, and only the bedside lamp was left. When the subject intended to fall asleep, the bedside lamp was turned off and the bed curtain was closed. The volume of the electronic devices of the subject and the escort was turned down after dark. After 9 pm, the electronic devices for the subject and the escort were turned to mute. Subjects might take medication to help them sleep if they reported being unable to fall asleep.
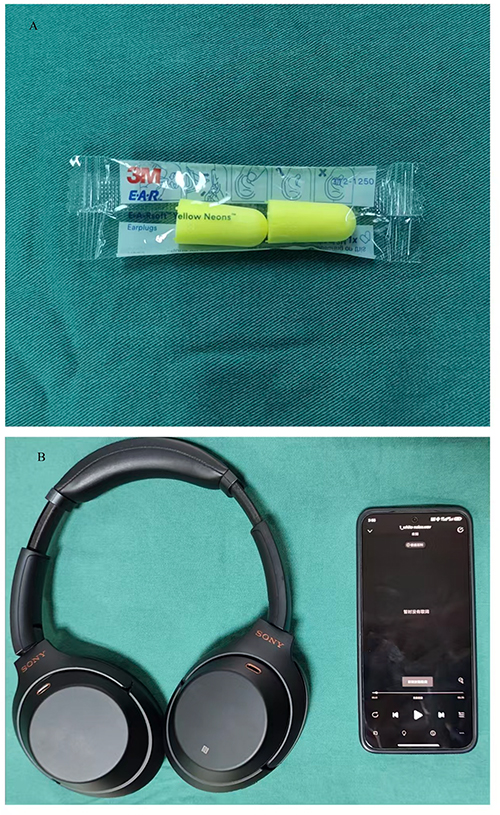 |
Figure 2 The equipment needed to perform interventions on two groups of subjects. Notes: (A) Earplugs required by the subjects receiving noise isolation intervention; (B) Noise-cancelling headphone and smartphone required by the subjects receiving white noise intervention. |
Outcome Measures
Our primary outcome was the difference in the sleep quality on the first postoperative night, as assessed by RCSQ. Secondary outcomes were differences in the pain scores at rest and during activity by rating on an 11-point Likert-type scale 24 hours after surgery, the consumption of propofol and remifentanil infused intraoperatively, the duration of surgery and anesthesia, and the length of postoperative hospital stay.
Statistical Analysis
Since there are no results from previous studies as a reference. Sample size calculations were based on the results of pre-experiments. In the pre-experiment, twenty subjects were randomly assigned to Group N and Group W. On the first postoperative night, patients in Group N reported a mean sleep quality score of 48.4 with a standard deviation of 10.3, while patients in Group W reported a mean score of 40.8. Eighty subjects would provide 90% power to detect a significant difference in the sleep quality scores in patients who received noise isolation vs patients who received white noise using an independent-samples T test with a two-sided α of 0.05. Forty-five subjects per group were considered adequate based on potential loss to follow-up. PASS 2021 was used to determine the sample size.
For continuous variables, the choice of representation and testing methods should vary according to whether the data adheres to a normal distribution. Normality of distribution was assessed using the Kolmogorov–Smirnov normality test. Continuous data of normal distribution was expressed using mean and standard deviation and analyzed by an independent-samples T test. Non normally distributed continuous data was represented by median and quartiles and analyzed by Mann–Whitney U-tests. Categorical variables were expressed as frequencies with percentages and analyzed using Pearson’s Chi-square tests. The primary outcome, sleep quality score on the first postoperative night, was a normally distributed continuous variable, and an independent-samples T test was used as the primary analysis to compare differences between the two groups. To control the potential impact of baseline imbalance on sleep quality scores, an exploratory analysis of covariance (ANCOVA) was used to analyze the differences between groups. Secondary outcomes include the pain scores at rest and during activity 24 hours after surgery, the consumption of propofol and remifentanil infused intraoperatively, the duration of surgery and anesthesia, and the length of postoperative hospital stay were continuous variables that did not conform to the normal distribution. Mann–Whitney U-tests were used to compare the differences between the two groups of the secondary outcomes mentioned above. Due to conducting seven Mann–Whitney U-tests on the same dataset, Bonferroni correction (0.05/7=0.007) was used to adjust the alpha level.
The significance level for all statistical tests was set at P < 0.05. The statistical analysis was conducted using SPSS version 16.
Results
From March 2025 to September 2025, a total of 123 patients who underwent elective flexible ureteroscopic Holmium: YAG laser lithotripsy were screened for study eligibility. Among them, 15 patients refused to participate, 18 patients did not meet the inclusion criteria, and the remaining 90 patients were randomly assigned to Group N and Group W. A total of 90 patients were included in the final analysis. There was no difference in the demographic data between the two groups of patients (Table 1).
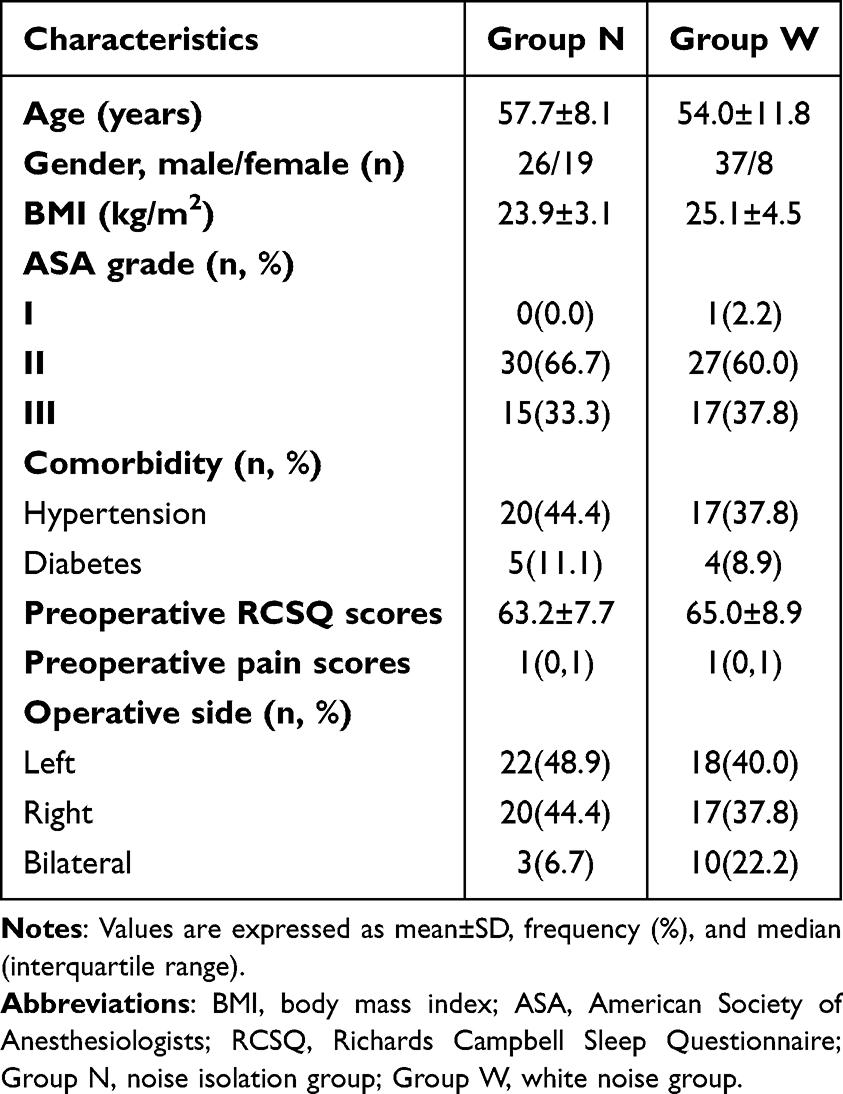 |
Table 1 Baseline Data of Two Groups of Patients |
The mean preoperative RCSQ scores of patients in Group N were 63.2 with a standard deviation of 7.7, and those of patients in Group W were 65.0 with a standard deviation of 8.9. The primary outcome of our study was the RCSQ scores on the first night after surgery. As shown in Table 2, on the first night after surgery, patients in Group N reported higher RCSQ scores than those in Group W (P=0.009). After adjusting for gender and baseline RCSQ scores as potential confounding factors in analysis of covariance, there was still a statistically significant difference in RCSQ scores between patients in Group N and Group W [F(1,85)=4.17, P=0.044]. After adjustment, the RCSQ scores of Group N were 49.60 (95% confidence interval: 45.33, 53.86), while those of Group W were 42.41 (95% confidence interval: 36.90, 47.93). On the first night after surgery, the decrease in RCSQ scores in Group N was lower than that in Group W compared with that before surgery (13.9 vs 23.6, P=0.007). The effect size of the decrease in RCSQ scores between groups was 0.58 (95% confidence interval: 0.16 to 1.00). There was no difference in the noise intensity scores at night reported by the two groups of patients (P=0.359). There was no difference in pain scores between the two groups of patients 24 hours after surgery, both at rest and during activity (P=0.234, P=0.753). The intraoperative propofol consumption of Group N patients was lower than that of Group W(P=0.005). There was no difference in the intraoperative consumption of remifentanil between the two groups of patients (P=0.290). There was no difference in the duration of surgery and anesthesia between the two groups of patients (P=0.211, P=0.103). There was no difference in the recovery time, extubation time, and duration of postoperative PACU stay between the two groups of patients (all P>0.05). The postoperative hospital stay of patients in Group N was shorter than that of patients in Group W (P=0.022). After Bonferroni correction, there was no longer a difference in postoperative hospital stay between the two groups of patients.
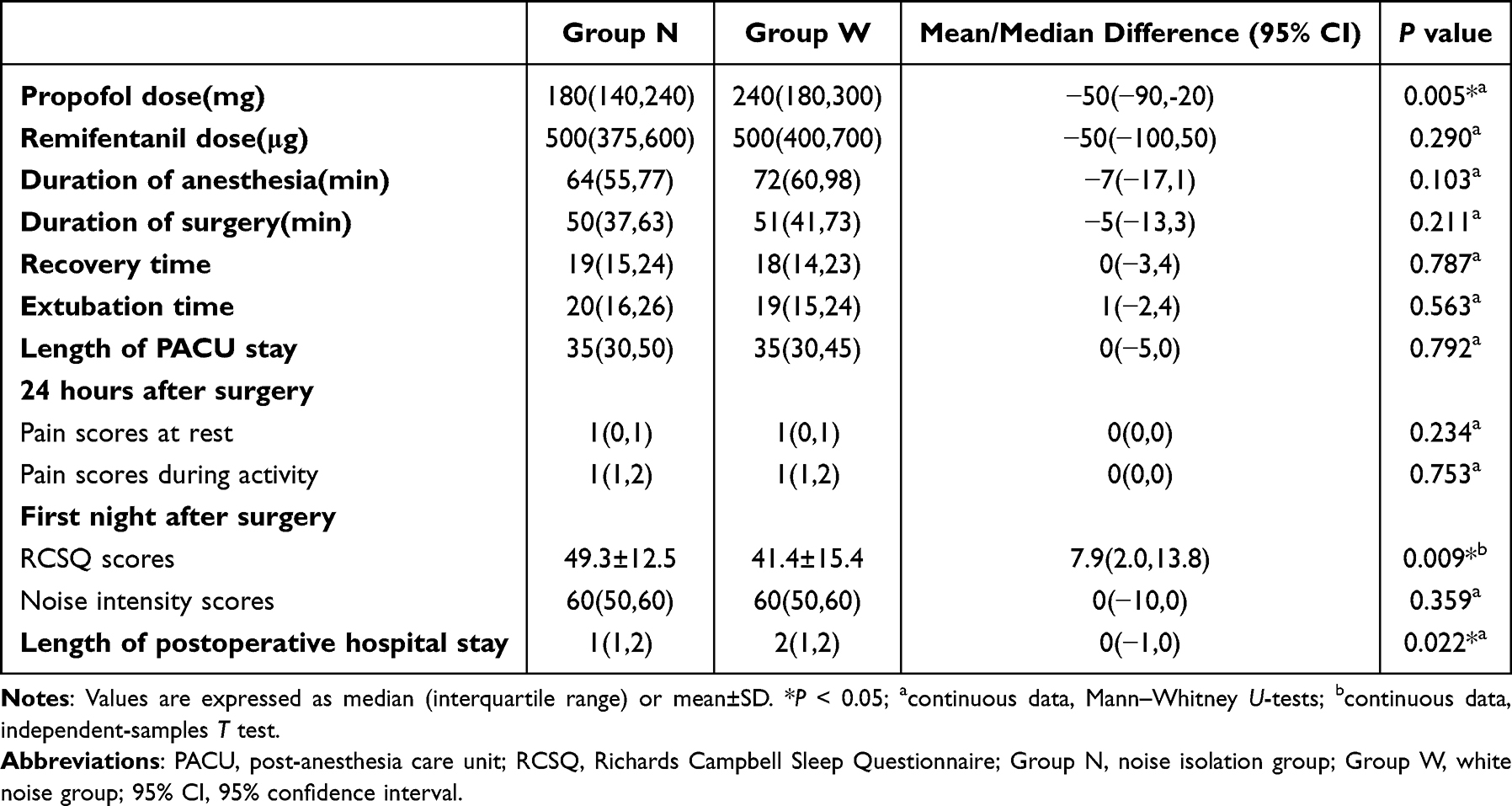 |
Table 2 Postoperative Data of Two Groups of Patients |
Discussion
In our study, the sleep quality score on the first night after surgery was higher in Group N than in Group W. There was no difference in pain scores between the two groups of patients at rest and during activity 24 hours after surgery. The intraoperative propofol consumption of Group N patients was lower than that of Group W patients.
The operating theatre is an unavoidable medical facility for patients undergoing surgical procedures. The noise issue in the operating theatre is a long-standing challenge that urgently needs to be addressed. At present, various new types of instruments have been introduced to assist in the completion of surgeries, but along with them comes the noise related to the instruments. The sound level generated by the instruments for average-length surgical cases in the operating room may exceed the National Institute for Occupational Safety and Health’s recommendations for hearing safety.3 A survey on the widespread noise in operating rooms revealed that anesthesiologists could be distracted by the noise levels in operating rooms, especially during general anesthesia induction and emergency. Noise in the operating room can harm communication, reduce attention to the patient’s condition, and lower the ability to hear alarms.21 Active noise management is beneficial for improving surgical performance and postoperative outcomes.22
The adverse effects of noise on healthcare providers are widely known, and certain measures have been taken to improve the situation. However, patients anesthetized but still physiologically responsive to auditory stimuli are rarely noticed. In our institution, the usual care for patients undergoing flexible ureteroscopic Holmium: YAG laser lithotripsy under general anesthesia does not include active intervention for intraoperative noise either. Noise isolation is a strategy used to avoid exposure to high-noise environments. Obviously, noise isolation can prevent the increase in sympathetic activation and stress hormone levels caused by noisy environments,4 thereby improving sleep.5 In Group N, all subjects received noise isolation intervention and reported higher sleep quality scores compared to patients in Group W. The decrease in sleep quality scores on the first night after surgery and before surgery between the two groups was also compared, and the effect sizes were calculated (0.58). The larger the effect size value, the greater the degree of difference. An effect size value greater than 0.5 is considered a moderate effect.23 Nevertheless, due to the lack of a validated minimal clinically important difference in RCSQ scores, we cannot determine that the difference between the two groups represents a clinical difference. A prior study has investigated the impact of intraoperative noise isolation on postoperative outcomes in patients receiving regional anesthesia. Tran et al found that in total knee arthroplasty patients receiving spinal epidural combined anesthesia, playing additional music in noise-cancelling headphones did not reduce intraoperative propofol consumption, postoperative pain scores, and postoperative analgesic consumption compared to simple noise isolation.24 The potential role of intraoperative noise isolation has also been noted in patients undergoing laparoscopic surgery under general anesthesia.25 You et al found that intraoperative noise isolation could reduce postoperative pain scores and the consumption of analgesic drugs in patients.25 In another basic and clinical combined study, it was found that the duration of intraoperative exposure to noise levels greater than 70dB was an independent risk factor for postoperative pain in patients. The results of the mouse model confirmed that noise exposure under general anesthesia could aggravate noxious stimulation-induced hyperpathia.26
Adequate depth of general anesthesia is usually considered to induce complete loss of consciousness in patients. Even under the condition that the depth of general anesthesia is adequate, the sensory cortex function of the patient is still active.11 The primary auditory cortex remains receptive and reactive to auditory stimuli.27,28 This contributed to the formation of the concept of implicit memory. Implicit memory refers to unconscious perception during surgery without explicit recall. It was also found in anesthetized monkeys that propofol disrupted the detection of higher-order auditory novelty by partially inhibiting the frontal-parietal network while preserving the complete response to auditory cortex input.29 The mechanisms mentioned above are also the basis for the potential role of music therapy during general anesthesia in patients.13 A meta-analysis involving 53 studies summarized that intraoperative auditory stimuli can be unconsciously perceived and positively affect patient outcomes during the immediate postoperative period.13 White noise includes a variety of continuous, monotonous sounds from the environment, each with different frequencies. In daily life, white noise is often used to mask unwanted sounds to improve nighttime sleep. The white noise is recommended as a method for masking environmental noises, improving sleep, and maintaining sleep in the coronary care unit.30 However, it is still unclear whether white noise has a potential role in patients undergoing general anesthesia. Can intraoperative white noise promote postoperative sleep at night as it does in daily life? Unfortunately, in the current study, intraoperative white noise did not demonstrate an advantage over intraoperative noise isolation in improving sleep quality on the first night after surgery. For patients in Group W, the active noise cancellation technology of the noise-cancelling headphones isolated the noise during surgery. The noise received by the two groups of patients during surgery may have been treated with similar isolation. This might be the reason why there was no difference in the pain score between the two groups of patients 24 hours after surgery. Adding white noise to the noise-cancelling headphones for Group W patients might have a negative effect. Up to date, the impact of white noise on postoperative sleep quality in patients undergoing general anesthesia revealed a paucity of literature. Intraoperative music has been proven to alleviate postoperative pain in patients undergoing general anesthesia.14 The potential mechanism is that music reduces autonomic nervous system activity, such as a decrease in pulse and respiratory rate, as well as a decrease in blood pressure. However, music and white noise are two different forms of auditory stimuli that affect completely different regions of the cerebral cortex. Music operates through a complex brain network centered around the temporal lobe but widely connected to multiple cortical and subcortical regions.31 White noise has been shown to reduce cortical connectivity between primary auditory and motor regions and very distant cortical regions, demonstrating a decrease in right-sided connectivity for the primary motor cortex.32 Therefore, the effect of intraoperative white noise cannot be equated with intraoperative music. Pinardi et al opposed the unrestricted use of white noise to mask environmental noise which is vastly different from our daily life and clinical practice.32
In our study, the intraoperative consumption of propofol in Group N was lower than that in Group W. In our study, only two researchers were responsible for the intraoperative anesthesia management of all subjects. Based on randomization, we believed that the variability of clinicians could be ignored. For the two researchers who adhered to the intraoperative propofol infusion protocol, other potential influences on the consumption of propofol during surgery could be negligible. The increase in noise intensity is accompanied by an increase in the BIS value for patients under propofol sedation.33 Studies have confirmed that in patients undergoing knee replacement, blocking noise rather than playing music is more effective in reducing the BIS value.34 This might explain the difference in propofol consumption between the two groups of patients. Propofol has a very short drug half-life of about 15 minutes and no cumulative effect.35 Propofol has been proven to repay the sleep debt of sleep-deprived rats by reducing neuroinflammation and regulating the activation state of microglia phenotypes from M1 to M2.36 However, in critically ill patients receiving assisted ventilation, the use of propofol only inhibits the rapid eye movement sleep stage and further deteriorates the sleep quality of such patients.37 In patients receiving propofol anesthesia, the short-term sleep quality of the patients after surgery was also disrupted.38 The potential causes of the negative effect of propofol on the postoperative sleep quality of patients have been deeply studied. The potential mechanisms include the inhibition of melatonin secretion and the locus coeruleus norepinephrine system, as well as the impact on inflammatory mediators.39–41 The higher intraoperative consumption of propofol in Group W might be one of the potential factors for the lower sleep quality on the first night after surgery compared to patients in Group N. The potential link between propofol consumption and postoperative sleep, as well as noise isolation, may require in-depth investigation in future research.
For patients undergoing surgery, sleep directly impacts immune function and wound healing.42,43 Poor sleep quality raises the risk of complications after surgery and prolongs hospital stays.44 This may be a potential factor for the shorter postoperative hospital stay in Group N compared to Group W. Although this difference was not statistically significant after Bonferroni correction, it may still hold value in healthcare cost considerations. In clinical practice, the noise in the operating room is unbearable, and the auditory management of patients under general anesthesia during the operation has never been given due attention. Noise isolation and auditory stimulation are both strategies for intraoperative auditory management. Earplugs, as a non-invasive, inexpensive, and easy-to-implement tool, were used in our research for noise isolation. This represents a new approach to intraoperative auditory management for patients, achieving better sleep quality and potential reduction in healthcare costs at a lower cost. It is hoped that our research results can provide a simple and effective approach for intraoperative auditory management in a wider range of clinical practice applications.
Several limitations should be mentioned in our research. Firstly, the underlying mechanism of the impact of intervention measures on sleep may have to rely on the results of preclinical studies. No underlying deep mechanism can be derived from our research results alone. Secondly, the noise levels generated by different types of surgeries vary. The lack of intraoperative noise intensity measurement may have introduced potential confounding factors. These two noise processing strategies we studied may exhibit different characteristics, and caution should be exercised when externalizing our research conclusions. Thirdly, in light of our research objective, the strategy that might truly improve patients’ sleep lies in how to create a quiet resting environment. Fourthly, in our study, we only compared the differences in the effects of noise isolation and white noise on postoperative sleep in patients. The lack of a control group prevents us from confirming that these two intervention measures are superior to usual care, and caution should be exercised in externalizing the results. Fifthly, in our study, only the postoperative follow-up staff were blinded to the group allocation, which might have introduced bias regarding the subjective sleep evaluation scores of all subjects. In our research, white noise was based on the active noise cancellation technology of noise-cancelling headphones, which is essentially different from earplugs. This design limitation prevents definitive attribution of effects to noise isolation, white noise, or device features. Future research can separate the impact of white noise from device-based noise reduction to evaluate clinical thresholds for meaningful change.
Conclusions
In our study, for patients undergoing flexible ureteroscopic Holmium: YAG laser lithotripsy under general anesthesia, noise isolation has potential advantages in reducing the consumption of propofol during surgery and improving the quality of sleep on the first night after surgery compared to playing white noise in noise-cancelling headphones. Larger, multicenter studies using objective sleep monitoring (eg, polysomnography or actigraphy) are needed to confirm these subjective findings before they can be broadly adopted in clinical settings to assess the possible reduction in healthcare expenses. When comparing the impact of earplugs and white noise on sleep, it is necessary to isolate device-based noise cancellation to reduce device-related confounding.
Data Sharing Statement
Within five years after the publication of the research, the corresponding author can be contacted via Email to obtain research data.
Ethical Adherence
Ethical approval was provided by the Ethical Committee of the First Affiliated Hospital of Anhui Medical University, Hefei, Anhui, China. All patients provided informed consent, and all procedures were conducted according to the Declaration of Helsinki.
Author Contributions
Wei Dai: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Software, and Writing–original draft.
Xin-yue Wang: Funding acquisition, Project administration, Resources, Supervision, Validation, and Writing–original draft.
Rui Yang: Conceptualization, Supervision, Visualization, Writing–review & editing.
All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study did not receive any funding support.
Disclosure
The authors declare no competing interests.
References
1. Au J, Hamilton S, Webb A. Decibels in the operating theatre: a study of noise levels during surgical procedures. ANZ J Surg. 2024;94(10):1841–11. doi:10.1111/ans.19001
2. Nott MR, West PD. Orthopaedic theatre noise: a potential hazard to patients. Anaesthesia. 2003;58(8):784–787. doi:10.1046/j.1365-2044.2003.03257.x
3. Fritsch MH, Chacko CE, Patterson EB. Operating room sound level hazards for patients and physicians. Otol Neurotol. 2010;31(5):715–721. doi:10.1097/MAO.0b013e3181d8d717
4. Daiber A, Kröller-Schön S, Frenis K, et al. Environmental noise induces the release of stress hormones and inflammatory signaling molecules leading to oxidative stress and vascular dysfunction-Signatures of the internal exposome. Biofactors. 2019;45(4):495–506. doi:10.1002/biof.1506
5. Tai BWS, Dawood T, Macefield VG, et al. The association between sleep duration and muscle sympathetic nerve activity. Clin Auton Res. 2023;33(6):647–657. doi:10.1007/s10286-023-00965-7
6. Moore J, Chavez A, Narang G, et al. Operating room noise hazards during laser lithotripsy: a comparison between the thulium fiber and holmium laser platforms. World J Urol. 2022;40(3):801–805. doi:10.1007/s00345-021-03897-x
7. Obeid DA, Assiri H, AlShalawi J, et al. Hearing loss among otolaryngologist and healthcare workers: case control study. Am J Otolaryngol. 2025;46(4):104635. doi:10.1016/j.amjoto.2025.104635
8. Katz JD. Noise in the operating room. Anesthesiology. 2014;121(4):894–898. doi:10.1097/ALN.0000000000000319
9. Leitsmann C, Uhlig A, Popeneciu IV, et al. The Silent Operation Theatre Optimisation System (SOTOS©) to reduce noise pollution during da vinci robot-assisted laparoscopic radical prostatectomy. J Robot Surg. 2021;15(4):519–527. doi:10.1007/s11701-020-01135-x
10. Hall AC, Silver BH, Ellis W, et al. The impact of personal protective equipment on speech discrimination and verbal communication in the operating room and the role of audio communication devices. Simul Healthc. 2023;18(1):64–70. doi:10.1097/SIH.0000000000000646
11. Madler C, Keller I, Schwender D, et al. Sensory information processing during general anaesthesia: effect of isoflurane on auditory evoked neuronal oscillations. Br J Anaesth. 1991;66(1):81–87. doi:10.1093/bja/66.1.81
12. Capezuti E, Pain K, Alamag E, et al. Systematic review: auditory stimulation and sleep. J Clin Sleep Med. 2022;18(6):1697–1709. doi:10.5664/jcsm.9860
13. Fu VX, Sleurink KJ, Janssen JC, Wijnhoven BPL, Jeekel J, Klimek M. Perception of auditory stimuli during general anesthesia and its effects on patient outcomes: a systematic review and meta-analysis. Perception de stimuli auditifs pendant l’anesthésie générale et ses effets sur les devenirs des patients: revue systématique et méta-analyse. Can J Anaesth. 2021;68(8):1231–1253. doi:10.1007/s12630-021-02015-0
14. Hole J, Hirsch M, Ball E, et al. Music as an aid for postoperative recovery in adults: a systematic review and meta-analysis. Lancet. 2015;386(10004):1659–1671. doi:10.1016/S0140-6736(15)60169-6
15. Nowak H, Zech N, Asmussen S, et al. Effect of therapeutic suggestions during general anaesthesia on postoperative pain and opioid use: multicentre randomised controlled trial. BMJ. 2020;371:m4284.
16. Kühlmann AYR, de Rooij A, Kroese LF, et al. Meta-analysis evaluating music interventions for anxiety and pain in surgery. Br J Surg. 2018;105(7):773–783. doi:10.1002/bjs.10853
17. Hawkins JE, Stevens SS. The masking of pure tones and of speech by white noise. J Acoust Soc Am. 1950;22(1):6–13. doi:10.1121/1.1906581
18. Ebben MR, Yan P, Krieger AC. The effects of white noise on sleep and duration in individuals living in a high noise environment in New York City. Sleep Med. 2021;83:256–259. doi:10.1016/j.sleep.2021.03.031
19. Chen LX, Ji DH, Zhang F, et al. Richards-Campbell sleep questionnaire: psychometric properties of Chinese critically ill patients. Nurs Crit Care. 2019;24(6):362–368. doi:10.1111/nicc.12357
20. Hopewell S, Chan AW, Collins GS, et al. CONSORT 2025 statement: updated guideline for reporting randomised trials. BMJ. 2025;389:e081123. doi:10.1136/bmj-2024-081123
21. Crockett CJ, Dalal PG, Tjia I, et al. A loud call for silence: anaesthesiologists’ perceptions of noise in the operating room. Br J Anaesth. 2024;132(2):444–447. doi:10.1016/j.bja.2023.11.035
22. Baltin CT, Wilhelm H, Wittland M, et al. Noise patterns in visceral surgical procedures: analysis of second-by-second dBA data of 599 procedures over the course of one year. Sci Rep. 2020;10(1):3030. doi:10.1038/s41598-020-59816-4
23. Kazis LE, Anderson JJ, Meenan RF. Effect sizes for interpreting changes in health status. Med Care. 1989;27(3 Suppl):S178–S89. doi:10.1097/00005650-198903001-00015
24. Tran BW, Nowrouz MY, Dhillon SK, et al. The impact of music and noise-cancellation on sedation requirements during total knee replacement: a randomized controlled trial. Geriatr Orthop Surg Rehabil. 2020;11:2151459320910844. doi:10.1177/2151459320910844
25. You S, Xu F, Wu Y, et al. Effect of noise isolation using noise-cancelling headphones during laparoscopic surgery for postoperative pain reduction: a randomized clinical trial. J Clin Anesth. 2024;92:111286. doi:10.1016/j.jclinane.2023.111286
26. You S, Xu F, Zhu X, et al. Effect of intraoperative noise on postoperative pain in surgery patients under general anesthesia: evidence from a prospective study and mouse model. Int J Surg. 2023;109(12):3872–3882. doi:10.1097/JS9.0000000000000672
27. Gross WL, Lauer KK, Liu X, et al. Propofol sedation alters perceptual and cognitive functions in healthy volunteers as revealed by functional magnetic resonance imaging. Anesthesiology. 2019;131(2):254–265. doi:10.1097/ALN.0000000000002669
28. Dueck MH, Petzke F, Gerbershagen HJ, et al. Propofol attenuates responses of the auditory cortex to acoustic stimulation in a dose-dependent manner: a FMRI study. Acta Anaesthesiol Scand. 2005;49(6):784–791. doi:10.1111/j.1399-6576.2005.00703.x
29. Uhrig L, Janssen D, Dehaene S, et al. Cerebral responses to local and global auditory novelty under general anesthesia. Neuroimage. 2016;141:326–340. doi:10.1016/j.neuroimage.2016.08.004
30. Farokhnezhad Afshar P, Bahramnezhad F, Asgari P, et al. Effect of white noise on sleep in patients admitted to a coronary care. J Caring Sci. 2016;5(2):103–109. doi:10.15171/jcs.2016.011
31. Sihvonen AJ, Särkämö T. Music processing and amusia. Handb Clin Neurol. 2022;187:55–67.
32. Pinardi M, Schuler AL, Arcara G, et al. Reduced connectivity of primary auditory and motor cortices during exposure to auditory white noise. Neurosci Lett. 2023;804:137212. doi:10.1016/j.neulet.2023.137212
33. Kim DW, Kil HY, White PF. The effect of noise on the bispectral index during propofol sedation. Anesth Analg. 2001;93(5):1170–1173. doi:10.1097/00000539-200111000-00022
34. Kang JG, Lee JJ, Kim DM, et al. Blocking noise but not music lowers bispectral index scores during sedation in noisy operating rooms. J Clin Anesth. 2008;20(1):12–16. doi:10.1016/j.jclinane.2007.06.005
35. Ozone M, Itoh H, Yamadera W, et al. Changes in subjective sleepiness, subjective fatigue and nocturnal sleep after anaesthesia with propofol. Psychiatry Clin Neurosci. 2000;54(3):317–318. doi:10.1046/j.1440-1819.2000.00694.x
36. Liu H, Yang C, Wang X, et al. Propofol improves sleep deprivation-induced sleep structural and cognitive deficits via upregulating the BMAL1 expression and suppressing microglial M1 polarization. CNS Neurosci Ther. 2024;30(7):e14798. doi:10.1111/cns.14798
37. Kondili E, Alexopoulou C, Xirouchaki N, et al. Effects of propofol on sleep quality in mechanically ventilated critically ill patients: a physiological study. Intensive Care Med. 2012;38(10):1640–1646. doi:10.1007/s00134-012-2623-z
38. Wu X, Deng J, Li X, et al. Effects of propofol on perioperative sleep quality in patients undergoing gastrointestinal endoscopy: a prospective cohort study. J Perianesth Nurs. 2023;38(5):787–791. doi:10.1016/j.jopan.2023.02.001
39. Kushikata T, Sawada M, Niwa H, et al. Ketamine and propofol have opposite effects on postanesthetic sleep architecture in rats: relevance to the endogenous sleep-wakefulness substances orexin and melanin-concentrating hormone. J Anesth. 2016;30(3):437–443. doi:10.1007/s00540-016-2161-x
40. Du WJ, Zhang RW, Li J, et al. The locus coeruleus modulates intravenous general anesthesia of zebrafish via a cooperative mechanism. Cell Rep. 2018;24(12):3146–55.e3. doi:10.1016/j.celrep.2018.08.046
41. Sayed S, Idriss NK, Sayyedf HG, et al. Effects of propofol and isoflurane on haemodynamics and the inflammatory response in cardiopulmonary bypass surgery. Br J Biomed Sci. 2015;72(3):93–101. doi:10.1080/09674845.2015.11666803
42. Kamdar BB, Needham DM, Collop NA. Sleep deprivation in critical illness: its role in physical and psychological recovery. J Intensive Care Med. 2012;27(2):97–111. doi:10.1177/0885066610394322
43. Hoyle NP, Seinkmane E, Putker M, et al. Circadian actin dynamics drive rhythmic fibroblast mobilization during wound healing. Sci Transl Med. 2017;9(415):eaal2774. doi:10.1126/scitranslmed.aal2774
44. Su X, Wang DX. Improve postoperative sleep: what can we do? Curr Opin Anaesthesiol. 2018;31(1):83–88. doi:10.1097/ACO.0000000000000538
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Association Between Pain and Frailty in Middle-Aged and Older Patients: The Mediating Roles of Sleep and Mood
Wang HP, Wang T, Ye HT, Dong YY, Zhao SJ, Liu QR, Hu XY, Ji MH, Yang JJ
Clinical Interventions in Aging 2025, 20:777-789
Published Date: 4 June 2025
Development of the Sleeping Pills Receptivity and Involuntariness Scale-6 (SPRIS-6) to Assess Acceptance of Hypnotics Use
Chung S, Shahrier MA
Nature and Science of Sleep 2025, 17:2309-2319
Published Date: 26 September 2025
Recent Trends in Cannabis Use in Adults Ages 60 Years and Older
Thayer RE, Anquillare E, Coromac-Medrano J, Hardin EE, Hatcher K, Hermann GE
Substance Abuse and Rehabilitation 2026, 17:560360
Published Date: 13 February 2026