")
Back to Journals » Clinical Ophthalmology » Volume 10
Comparison of intraocular pressure adjusted by central corneal thickness or corneal biomechanical properties as measured in glaucomatous eyes using noncontact tonometers and the Goldmann applanation tonometer
Authors Yaoeda K, Fukushima A, Shirakashi M, Fukuchi T
Received 20 February 2016
Accepted for publication 15 March 2016
Published 11 May 2016 Volume 2016:10 Pages 829—834
DOI https://doi.org/10.2147/OPTH.S106836
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Kiyoshi Yaoeda,1,2 Atsushi Fukushima,1 Motohiro Shirakashi,3 Takeo Fukuchi2
1Yaoeda Eye Clinic, Nagaoka, 2Division of Ophthalmology and Visual Sciences, Niigata University Graduate School of Medical and Dental Sciences, 3Kido Eye Clinic, Niigata, Japan
Purpose: To investigate the correlation coefficients between intraocular pressure (IOP) before and after adjusting for central corneal thickness (CCT) and corneal biomechanical properties.
Patients and methods: A total of 218 eyes of 218 patients with primary open-angle glaucoma (mean age =71.5 years; mean spherical equivalent =-0.51 D; mean deviation determined by Humphrey visual field analyzer =-3.22 dB) were included in this study. The tIOP and tIOPCCT, which were adjusted by the CCT (with tIOP meaning IOP not adjusted by CCT, as determined using the CT-1P; and tIOPCCT meaning IOP adjusted by CCT, as determined using the CT-1P), were determined using a noncontact tonometer. The IOPg and IOPCCT, which were adjusted by CCT, and IOPcc adjusted by corneal biomechanical properties were determined using a Reichert 7CR (with IOPg meaning IOP not adjusted by CCT or corneal biomechanical properties, as determined using the Reichert 7CR; IOPCCT meaning IOP adjusted by CCT, as determined using the Reichert 7CR; and IOPcc meaning IOP adjusted by corneal biomechanical properties, as determined using the Reichert 7CR). The GT and GTCCT adjusted by CCT were determined using a Goldmann applanation tonometer (with GT meaning IOP not adjusted by CCT, as determined using the Goldmann applanation tonometer; and with GTCCT meaning IOP adjusted by CCT, as determined using the GAT). Pearson’s correlation coefficients among the IOPs were calculated and compared. P-values <0.05 were considered as statistically significant.
Results: The tIOP, tIOPCCT, IOPg, IOPCCT, IOPcc, GT, and GTCCT were 14.8±2.5, 15.0±2.4, 13.1±3.2, 13.3±3.1, 13.7±2.9, 13.2±2.4, and 13.4±2.3 mmHg (mean ± standard deviation), respectively. The correlation coefficient between tIOPCCT and tIOP (r=0.979) was significantly higher than that between tIOPCCT and the other IOPs (r=0.668–0.852; P<0.001, respectively). The correlation coefficient between IOPCCT and IOPg (r=0.994) or IOPcc and IOPg (r=0.892) was significantly higher than that between IOPCCT or IOPcc and the other IOPs (r=0.669–0.740; P<0.001, respectively). The correlation coefficient between GTCCT and GT (r=0.989) was significantly higher than that between GTCCT and the other IOPs (r=0.669–0.740; P<0.001, respectively).
Conclusion: The IOP adjusted by CCT or corneal biomechanical properties depends on the measurement instrument itself, rather than the adjustment methods, for eyes of patients with primary open-angle glaucoma.
Keywords: ocular response analyzer, corneal biomechanical property, corneal hysteresis, glaucoma, intraocular pressure
Introduction
Glaucoma is characterized by a glaucomatous optic neuropathy accompanied by progressive loss of retinal ganglion cells and the deterioration of the corresponding visual field.1 At present, based on available evidence, the only reliable treatment for glaucoma is to decrease intraocular pressure (IOP).1 Therefore, measurement of IOP is essential for diagnosis and treatment of glaucoma. The Goldmann applanation tonometer (GAT), developed by Goldmann and Schmidt,2 is still considered to be the gold standard in tonometry. However, IOP measurements by GAT have been shown to be affected by the central corneal thickness (CCT), irrespective of the tonometer used.3,4 Although it is considered necessary to adjust IOP by CCT for proper evaluation of IOP, Herndon5 has suggested that the results vary, even when using various algorisms. Liu and Roberts6 identified the factors affecting IOP; besides CCT, whole corneal biochemical properties also influenced IOP.
Corneal hysteresis (CH), which is an indication of corneal biomechanical properties, was first proposed by Luce.7 The ocular response analyzer (ORA) is a new noncontact tonometer (NCT) that allows evaluation of corneal biomechanical properties, such as CH and the corneal response factor (CRF). The ORA calculates IOPg, which has shown good correction of the IOP measurement for GAT (GT), and IOPcc (corneal-compensated IOP), which is adjusted by corneal biomechanical properties.8 IOPcc measurements were not associated with any of the variables such as CCT, corneal curvature, axial length, and age.9
Clinical assessment of corneal biomechanical properties and IOPcc determined by the ORA are considered to be effective for the diagnosis and treatment of glaucoma. In a study by Touboul et al,10 CH values were found to be lower in eyes with glaucoma than in normal eyes. Congdon et al11 reported that a lower CH value, but not CCT, was associated with progression of visual field deterioration in glaucoma. Ehrlich et al12 reported that, among eyes of patients with normal tension glaucoma, the IOPcc was greater than the GT, and the difference between the IOPcc and the GT was greatest for eyes of patients with normal tension glaucoma, as compared with high-tension glaucoma or normal eyes. Additionally, the area under the receiver operating characteristic curve for the detection of glaucomatous optic neuropathy was significantly greater for the IOPcc than for the GT, which suggested that IOPcc may be superior as a test for the evaluation of glaucoma.
In general, the NCT is used as a screening device of GAT.13 The IOPcc, in which the IOP is adjusted by corneal biomechanical properties and is useful for the evaluation of glaucoma, is thought to be affected by the properties of the NCT because the ORA and the Reichert 7CR, which is a simplified version of the ORA, are types of NCT. In other words, GT, which is adjusted by various methods, may yield a more appropriate IOP measurement for the evaluation of glaucoma than IOPcc or IOP determined by NCT and adjusted by similar methods.
The purpose of this study was to evaluate the differences in the correlation coefficients between IOP determined by various tonometers and adjusted by CCT or by corneal biomechanical properties and to determine to what extent the tonometer itself is responsible for variation in IOP measurements.
Patients and methods
As the authors had no access to a formal review committee, the study adhered to the tenets of the Declaration of Helsinki, and written informed consent was obtained from all patients. A total of 218 eyes of 218 Japanese patients with primary open-angle glaucoma (POAG) were enrolled in this study. All subjects were recruited from the outpatient section of Yaoeda Eye Clinic. POAG was defined by glaucomatous optic disk damage and abnormal visual field test results with a normal anterior chamber angle. Signs of glaucomatous optic disk damage were considered diffuse or localized neuroretinal rim loss, excavation, and retinal nerve fiber layer defects. An abnormal visual field was defined as a pattern standard deviation outside the 95% normal confidence limits or a glaucoma hemifield test result that fell outside normal limits. Subjects were included if they had a spherical equivalent <±6 D and had three consecutive IOP values <21 mmHg as determined using a CT-90A (Topcon Corporation, Tokyo, Japan) prior to the day of the study.
We used three tonometers (the CT-1P, Reichert 7CR, and GAT) in this study. The CT-1P (Topcon Corporation) is an NCT that is capable of simultaneously measuring CCT by a specular microscope method and measuring IOP. Additionally, CT-1P is capable of determining the IOP adjusted by CCT. The Reichert 7CR (Reichert Technologies, NY, USA) is a new NCT that is positioned as a simplified version of the ORA and is capable of calculating the IOPcc, although it cannot calculate CH and CRF.
The measurement principle of the ORA has been described in other reports.8,9 In brief, the ORA, which is a type of NCT, utilizes a dynamic, bidirectional applanation process for measuring IOP. A rapid air impulse is used to apply force to the cornea. The deformation of the cornea is monitored until two corneal applanation states are attained. The collimated air pulse causes the cornea to move inwards causing applanation, similar to conventional NCT. However, this air pulse continues to deform the cornea past applanation into a slight concavity. As the air pressure decreases, the cornea begins to return to its normal configuration. During this process, it once again passes through an applanated state. From the inward and outward applanation events, two independent pressure values are acquired by the ORA. Due to the dynamic nature of the air pulse, viscous damping (energy absorption) in the cornea causes delays in the inward and outward applanation events, resulting in two different pressure values. The difference between these two pressure values is the CH. IOPcc is the IOP determined from the two pressure values to eliminate the impact of corneal biomechanical properties.
The tIOP (mmHg), providing the Goldmann-correlated IOP, was determined by the average of three consecutive measurements by the CT-1P (with tIOP meaning IOP not adjusted by CCT). Simultaneously, tIOPCCT (mmHg), which was calculated using the formula (tIOP - 0.012× [CCT {μm} - 520]),14 was determined using the CT-1P (with tIOPCCT means IOP adjusted by CCT). The IOPg (mmHg), providing the Goldmann-correlated IOP, was determined by the average of three consecutive measurements by the Reichert 7CR (with IOPg meaning IOP not adjusted by CCT or corneal biomechanical properties). Simultaneously, the IOPcc (mmHg), which was adjusted by corneal biomechanical properties, was determined by the Reichert 7CR. The IOPCCT (mmHg) was calculated by the same formula as tIOPCCT. These IOP measurements by NCT were performed in random order (with IOPCCT meaning IOP adjusted by CCT, as determined using the Reichert 7CR). To eliminate the possible effect that applanation may have on the IOP or hysteresis values, GAT measurements were performed at the end of these IOP measurements. The GT (mmHg) was determined from the average of three consecutive measurements using GAT (Haag-Streit, Bern, Switzerland) (with GT meaning IOP not adjusted by CCT). The GTCCT (mmHg) was calculated by the same formula as tIOPCCT (with GTCCT meaning IOP adjusted by CCT, as determined using the GAT).
Subjects were excluded if they presented best-corrected visual acuity of <20/40, uncorrected IOP and CCT measurement by CT-1P, a waveform score of <7 determined by the Reichert 7CR,15 prior glaucoma surgery, and altered corneal biomechanics, for example, keratoconus, corneal degeneration, and prior refractive surgery. Only one eye of each patient was included in this study. If both eyes were eligible for inclusion, one eye was selected randomly. Pearson’s correlation coefficients were calculated for each IOP and were compared among correlation coefficients using Z-transformation. Intraclass correlation coefficients (ICCs) were also used to evaluate the consistencies of IOPs for each device or each adjustment method.
Statistical analyses were performed with the MedCalc Version 11 software program (MedCalc Software bvba, Mariakerke, Belgium). A value of P<0.05 was considered to be statistically significant.
Results
The characteristics of the 218 patients with POAG are shown in Table 1. The average age of the participants was 71.5±9.6 years. The mean deviation, determined using the 30-2 testing protocol of the SITA-standard strategy, as measured with the Humphrey field analyzer 750 (Carl Zeiss-Humphrey Systems, Dublin, CA, USA), was -3.22±4.50 dB. The average CCT was 498.8±29.8 μm. All subjects were treated with topical antiglaucoma medications. In terms of antiglaucoma medications used in this study, timolol was used in 143 eyes, latanoprost was used in 47 eyes, travoprost was used in two eyes, a timolol and latanoprost combination was used in eleven eyes, a timolol and travoprost combination was used in five eyes, a timolol and dorzolamide combination was used in one eye, and the combination of timolol, travoprost, and brinzolamide was used in three eyes.
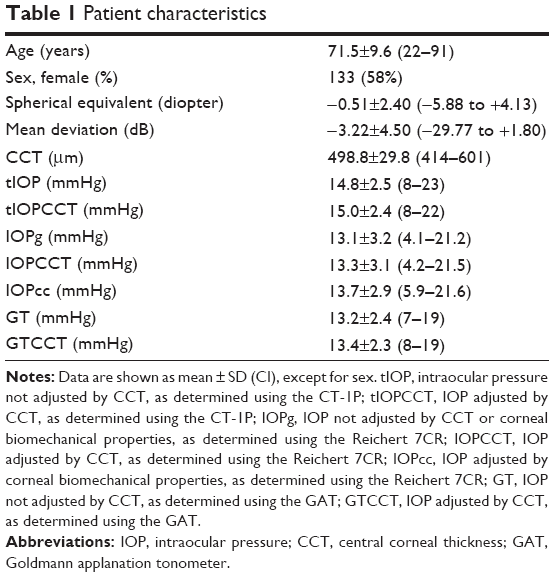 | Table 1 Patient characteristics |
The tIOP, tIOPCCT, IOPg, IOPCCT, IOPcc, GT, and GTCCT were 14.8±2.5 mmHg, 15.0±2.4 mmHg, 13.1±3.2 mmHg, 13.3±3.1 mmHg, 13.7±2.9 mmHg, 13.2±2.4 mmHg, and 13.4±2.3 mmHg, respectively.
The correlation matrix of the IOP is shown in Table 2. All correlation coefficients between IOPs were significantly and positively associated (r=0.659-0.989, all P<0.001). In a comparison of correlation coefficients between corrected IOPs and other IOPs, the correlation coefficient between tIOPCCT and tIOP (r=0.979) was significantly higher than that between tIOPCCT and IOPg, IOPCCT, IOPcc, GT, or GTCCT (r=0.668-0.852; all P<0.001). The correlation coefficient between IOPCCT and IOPg (r=0.994) was significantly higher than that between IOPCCT and tIOP, tIOPCCT, GT, and GTCCT (r=0.745-0.847; all P<0.001), except for the correlation coefficient between IOPcc and IOPg (r=0.892; P=0.674). The correlation coefficient between IOPcc and IOPg (r=0.892) was significantly greater than that between IOPcc and tIOP, tIOPCCT, GT, and GTCCT (r=0.659-0.669; all P<0.001) except for the correlation coefficient between IOPCCT and IOPg (r=0.994; P=0.674). The correlation coefficient between GTCCT and GT (r=0.989) was significantly greater than that between GTCCT and tIOP, tIOPCCT, IOPg, IOPCCT, and IOPcc (r=0.669-0.745; all P<0.001).
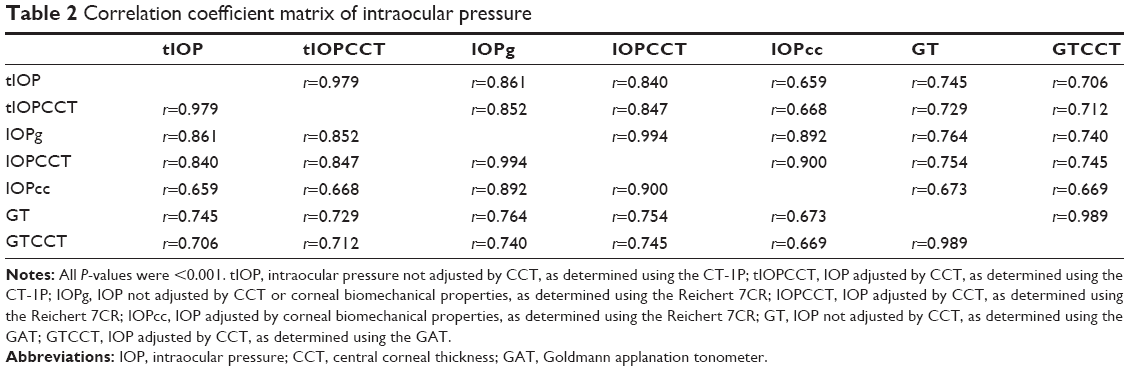 | Table 2 Correlation coefficient matrix of intraocular pressure |
The ICC of tIOP, IOPg, and GT, which were not adjusted IOPs, was 0.870 (95% confidence interval [CI]: 0.728–0.927). The ICC of tIOPCCT, IOPCCT, and GTCCT, which were adjusted IOPs by CCT, was 0.859 (95% CI: 0.722–0.918). The ICC of tIOP and tIOPCCT, which were determined by CT-1P, was 0.988 (95% CI: 0.981–0.992). The ICC of IOPg, IOPCCT, and IOPcc, which were determined by Reichert 7CR, was 0.971 (95% CI: 0.960–0.979). The ICC of GT and GTCCT, which were determined by GT, was 0.991 (95% CI: 0.971–0.996).
Discussion
In this study of the eyes of patients with POAG, the correlation between IOP adjusted by CCT or for corneal biomechanical properties and IOP not adjusted by these factors, determined using the same tonometer, was stronger than that when the IOP was determined by other tonometers. Additionally, ICCs (0.971–0.991), which were used to evaluate the consistencies of IOPs for each adjustment method, were relatively higher than that (0.859–0.870) for each device. In other words, the value of the IOP adjusted by CCT or corneal biomechanical properties depended on the measurement instrument itself, more than the adjustment methods used, for eyes of patients with POAG. Moreover, the correlation coefficient between IOP adjusted by CCT or corneal biomechanical properties and IOP not adjusted in this way was higher when using the Reichert 7CR than that obtained with the CT-1P, even though these devices are equivalent in that both are types of NCT. On the other hand, the correlation coefficient between IOPCCT and IOPg was not significantly higher than that between IOPcc and IOPg. This result was considered to be derived from the fact that CCT is positively and partially characterized by the corneal biomechanical properties.8
Evaluation of corneal biochemical properties and measurements of the IOPcc are thought to be useful for diagnosis and treatment of glaucoma. GT measurements are known to be influenced by the CCT.3 The IOP is overestimated in thick corneas and underestimated in thin corneas. Factors other than CCT, such as corneal hydration, connective tissue composition, and bioelasticity, are likely to contribute to the response of the corneoscleral shell to the force applied during the measurement of IOP.11 The ORA and Reichert 7CR provide IOPcc measurements that take these corneal biomechanical properties into consideration. The IOPcc measurements are not associated with the CCT, corneal curvature, axial length, or age.9 On the other hand, the difference between the GT and IOPcc is significantly associated with CCT.11 Congdon et al11 also reported that lower CH, but not CCT, was associated with progression of visual field deterioration in glaucoma patients. Touboul et al10 reported that CH values were lower in glaucomatous eyes than in normal eyes. However, IOP measurements using the ORA and the Reichert 7CR are technically and theoretically based on IOP measurements using an NCT.
NCTs are useful devices for the diagnosis and treatment of glaucoma because an NCT allows easy and low invasive measurements; however, it is also considered as a screening device because it is less accurate than GAT for a number of reasons.13 First, the time interval for an average NCT measurement is 1–3 ms (500th of the cardiac cycle) and is random with respect to the phase of the cardiac cycle, so that the ocular pulse becomes a significant variable. That is, unlike with some tonometers, the value cannot be averaged.16 This ocular pulse wave is thought to be a major cause of IOP fluctuation, amounting to ~1–3 mmHg.17 Second, the NCT is less reliable in patients with elevated IOP since studies comparing it with GAT have shown poor correlations in the higher pressure ranges.13,18,19 Third, the NCT is limited by an abnormal cornea or poor fixation, which may interfere with accurate pressure measurements. Fourth, the NCT is more susceptible to corneal elasticity than the GAT.20 Therefore, IOP measurements by the ORA or the Reichert 7CR, which are based on the principles of the NCT, may exhibit lower measurement accuracy than those by the GAT. In other words, by correcting for corneal biomechanical properties using the GAT rather than the NCT, IOP measurements may be more accurate than obtained using the ORA or Reichert 7CR.
There are several limitations to this study. First, participants in this study were limited to only Japanese patients with POAG. There is a difference in CH values between eyes with glaucoma and normal eyes.10 Additionally, CH measurements differ significantly between Black, Hispanic, and White subjects, independent of CCT.21 Therefore, our limited study population may have affected the results. Second, patients in this study were treated with IOP-lowering therapy. Antiglaucoma medications not only lower IOP but may also affect the corneal biomechanical properties. Wu et al22 reported that latanoprost affected the function of cultured porcine corneal stromal cells. Therefore, there is a need to consider the impact of antiglaucoma medication on corneal biomechanical properties. Third, CH and CRF cannot be calculated by the Reichert 7CR. For this reason, the IOP calculated by the CT-1P and GAT could not be adjusted by CH or CRF in this study. Further studies using the ORA are needed to investigate the relationship between tonometers and adjustment methods.
Conclusion
We investigated the correlation coefficients between IOP before and after adjusting for CCT and corneal biomechanical properties. The IOP adjusted by CCT or corneal biomechanical properties was influenced more by the measurement instrument itself than by the adjustment methods used in the eyes of patients with POAG. Therefore, the IOPs measured with different instruments are interchangeable.
Disclosure
The authors report no conflicts of interest in this work.
References
Committee of the Japan Glaucoma Society Guidelines for Glaucoma. The Japan Glaucoma Society guidelines for glaucoma (3rd eds). Nippon Ganka Gakkai Zasshi. 2012;116(1):3–46. | ||
Goldmann H, Schmidt T. Applanation tonometry. Ophthalmologica. 1957;134(4):221–242. | ||
Ehlers N, Hansen FK, Aasved H. Biometric correlations of corneal thickness. Acta Ophthalmol (Copenh). 1975;53(4):652–659. | ||
Tonnu PA, Ho T, Newson T, et al. The influence of corneal thickness and age on intraocular pressure measured by pneumotonometry, non-contact tonometry the Tono-Pen XL, and Goldmann applanation tonometry. Br J Ophthalmol. 2005;89(7):851–854. | ||
Herndon LW. Measuring intraocular pressure-adjustments for corneal thickness and new technologies. Curr Opin Ophthalmol. 2006;17(2):115–119. | ||
Liu J, Roberts CJ. Influence of corneal biomechanical properties on intraocular pressure measurement: quantitative analysis. J Cataract Refract Surg. 2005;31(1):146–155. | ||
Luce DA. Determining in vivo biomechanical properties of the cornea with an ocular response analyzer. J Cataract Refract Surg. 2005;31(1):156–162. | ||
Kotecha A, Elsheikh A, Roberts CR, Zhu H, Garway-Heath DF. Corneal thickness- and age-related biomechanical properties of the cornea measured with the ocular response analyzer. Invest Ophthalmol Vis Sci. 2006;47(12):5337–5347. | ||
Medeiros FA, Weinreb RN. Evaluation of influence of corneal biomechanical properties on intraocular pressure measurements using the ocular response analyzer. J Glaucoma. 2006;15(5):364–370. | ||
Touboul D, Roberts C, Kérautret J, et al. Correlations between corneal hysteresis, intraocular pressure, and corneal central pachymetry. J Cataract Refract Surg. 2008;34(4):616–622. | ||
Congdon NG, Broman AT, Bandeen-Roche K, Grover D, Quigley HA. Central corneal thickness and corneal hysteresis associated with glaucoma damage. Am J Ophthalmol. 2006;141(5):868–875. | ||
Ehrlich JR, Radcliffe NM, Shimmyo M. Goldmann applanation tonometry compared with corneal-compensated intraocular pressure in the evaluation of primary open-angle glaucoma. BMC Ophthalmol. 2012;12:52. | ||
Shields MB. The non-contact tonometer. Its value and limitations. Surv Ophthalmol. 1980;24(4):211–219. | ||
Suzuki S, Suzuki Y, Iwase A, Araie M. Corneal thickness in an ophthalmologically normal Japanese population. Ophthalmology. 2005;112(8):1327–1336. | ||
Ayala M, Chen E. Measuring corneal hysteresis: threshold estimation of the waveform score from the ocular response analyzer. Graefes Arch Clin Exp Ophthalmol. 2012;250(12):1803–1806. | ||
Grolman B. A new tonometer system. Am J Optom Arch Am Acad Optom. 1972;49(8):646–660. | ||
Forbes M, Pico G Jr, Grolman B. A noncontact applanation tonometer. Sight Sav Rev. 1973;43(3):155–161. | ||
Mosely MJ, Evans NM, Fielder AR. Comparison of a new non-contact tonometer with Goldmann applanation. Eye (Lond). 1989;3(Pt 3):332–337. | ||
Rouhiainen H, Teräsvirta M. Incident of open-angle glaucoma and screening of the intraocular pressure with a non-contact tonometer. Acta Ophthalmol (Copenh). 1990;68(3):344–346. | ||
Recep OF, Hasiripi H, Cağil N, Sarikatipoğlu H. Relation between corneal thickness and intraocular pressure measurement by noncontact and applanation tonometry. J Cataract Refract Surg. 2001;27(11):1787–1791. | ||
Haseltine SJ, Pae J, Ehrlich JR, et al. Variation in corneal hysteresis and central corneal thickness among black, Hispanic and white subjects. Acta Ophthalmol. 2012;90(8):e626–e631. | ||
Wu KY, Wang HZ, Hong SJ. Effect of latanoprost on cultured porcine corneal stromal cells. Curr Eye Res. 2005;30(10):871–879. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.