Back to Journals » Journal of Pain Research » Volume 19
Comparison of Cumulative Opioid Consumption Between Time-Programmed Decremental Infusion and Fixed-Rate Basal Infusion Modes of Intravenous Patient-Controlled Analgesia Following Mixed Surgery: Protocol for a Randomized Controlled Trial
Authors Ma Y, Liu M, Sun H, Luo F ![]() , Wan L
, Wan L
Received 31 March 2026
Accepted for publication 29 May 2026
Published 4 June 2026 Volume 2026:19 613446
DOI https://doi.org/10.2147/JPR.S613446
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Karina Gritsenko
Yun Ma,1,* Minying Liu,2,* Hu Sun,3,* Fang Luo,2 Lei Wan1
1Department of Anesthesiology, China Rehabilitation Research Center, Rehabilitation School of Capital Medical University, Beijing, People’s Republic of China; 2Department of Pain Management, Beijing Tiantan Hospital, Capital Medical University, Beijing, People’s Republic of China; 3Department of Anesthesiology, The Second Affiliated Hospital of Hainan Medical University, Hainan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Lei Wan, Department of Anesthesiology, China Rehabilitation Research Center, Rehabilitation School of Capital Medical University, No. 10, Jiaomen North Road, Fengtai District, Beijing, 100068, People’s Republic of China, Email [email protected] Fang Luo, Department of Pain Management, Beijing Tiantan Hospital, Capital Medical University, No. 119, Nansihuan Xilu, Fengtai District, Beijing, 100070, People’s Republic of China, Email [email protected]
Background: Effective postoperative pain management remains a clinical challenge, with a substantial proportion of patients experiencing moderate to severe pain after surgery. Intravenous patient-controlled analgesia (PCA) is widely used; however, conventional fixed-rate basal infusion does not account for the dynamic temporal pattern of postoperative pain, potentially leading to suboptimal analgesia and unnecessary opioid exposure. Time-programmed decremental infusion has been proposed as an alternative strategy to better align opioid delivery with postoperative pain trajectories, but high-quality evidence in mixed surgical populations is limited.
Methods and Analysis: This study is a prospective, multicenter, randomized, double-blind controlled trial conducted across three tertiary hospitals. A total of 1444 adult patients undergoing elective thoracic, abdominal, spinal, and orthopaedic procedures performed using either minimally invasive or open approaches will be randomized in a 1:1 ratio to receive either time-programmed decremental infusion or fixed-rate basal infusion PCA. All patients will receive a standardized PCA solution containing sufentanil 200 μg and ondansetron 32 mg diluted to 200 mL. The control group will receive a constant background infusion of 2 mL/h, whereas the intervention group will receive a predefined decremental infusion schedule (4.0, 3.0, 2.0, and 1.0 mL/h across successive postoperative time intervals). The primary outcome is cumulative opioid consumption at 48 hours postoperatively. Secondary outcomes include pain intensity, cumulative PCA volume, bolus demand frequency, rescue analgesic use, quality of recovery, sleep quality, sedation level, incidence of nausea and vomiting, and patient satisfaction. Analyses will be performed on the intention-to-treat and per-protocol populations.
Ethics and Dissemination: The study protocol has been approved by the institutional review boards of all participating centers. The trial will be conducted in accordance with the Declaration of Helsinki, and written informed consent will be obtained from all participants. The findings will be disseminated through peer-reviewed journals and academic conferences.
Trial Registration: Clinical Trials.gov identifier: NCT07375121. Registered on January, 2026. (https://clinicaltrials.gov/study/NCT07375121?term=NCT07375121&viewType=Card&rank=1).
Keywords: patient-controlled analgesia, cumulative opioid consumption, time-programmed decremental infusion, fixed-rate basal infusion, randomized controlled trial
Introduction
Effective postoperative pain management remains a fundamental component of perioperative care, yet a substantial proportion of patients continue to experience moderate to severe pain following surgery, with reported incidences as high as 70%-75%. Inadequately controlled pain is associated with delayed mobilization, impaired respiratory function, increased risk of cardiovascular and pulmonary complications, and prolonged hospitalization. Furthermore, poorly managed acute postoperative pain may contribute to the development of chronic postsurgical pain, thereby increasing long-term healthcare burden.1 Therefore, optimizing analgesic strategies is essential to improve both short-term recovery and long-term outcomes.
Intravenous patient-controlled analgesia (PCA) has become a cornerstone in postoperative pain management, allowing patients to self-administer opioids according to their individual needs. Compared with conventional clinician-administered analgesia, PCA provides superior patient autonomy and often improves analgesic satisfaction. With advances in device technology, PCA systems have evolved from elastomeric pumps to programmable electronic pumps and, more recently, to network-integrated intelligent infusion systems capable of precise drug delivery and real-time data recording.2 Despite these technological developments, the optimization of infusion modes, particularly the background infusion strategy, remains an area of ongoing investigation.
While morphine is traditionally considered the standard opioid for intravenous PCA, its clinical application is frequently hindered by active metabolites (eg, morphine-6-glucuronide) that can accumulate and provoke delayed respiratory depression and postoperative nausea and vomiting3 In recent years, sufentanil has become the predominant opioid for intravenous PCA in Chinese clinical practice due to its widespread clinical use and favorable pharmacological profile4 As a highly lipophilic synthetic piperidine derivative, sufentanil exhibits a profound affinity for μ-opioid receptors, providing enhanced analgesic potency. Crucially, unlike morphine, sufentanil produces no active metabolites, with a lower risk of respiratory depression than morphine.3 Its rapid onset effectively blunts breakthrough pain during PCA demand boluses, while its higher therapeutic index and lower frequency of respiratory suppression offer an optimized safety profile for postoperative use.5,6
Nevertheless, maximizing the safety and efficacy of sufentanil-based intravenous PCA also requires an optimal delivery mode. In clinical practice, PCA regimens commonly combine demand boluses with a continuous basal infusion to maintain stable analgesia throughout the postoperative period. Compared with demand-only PCA, basal infusion may help reduce fluctuations in analgesic effect and provide more consistent pain control during sleep or periods of limited patient activation, particularly in the early postoperative phase. However, the conventional fixed-rate basal infusion mode also has notable limitations. Postoperative pain typically follows a dynamic trajectory, characterized by higher intensity in the immediate postoperative period followed by a gradual decline over time.7,8 A constant infusion rate fails to accommodate this temporal variability, potentially leading to insufficient analgesia in the early phase and unnecessary opioid exposure during later recovery. This mismatch may increase the risk of opioid-related adverse effects, including respiratory depression, sedation, nausea, and vomiting, and may hinder enhanced recovery pathways.9
To address these limitations, alternative PCA infusion strategies have been explored. One approach involves feedback-regulated infusion systems, in which the background rate is adjusted according to patient demand. Previous randomized controlled trials have demonstrated that such variable-rate feedback infusion modes can reduce opioid consumption and bolus requirements compared with fixed-rate infusion, without compromising analgesic efficacy.10–12 However, these systems rely on real-time patient interaction and may be influenced by patient behavior, cognitive status, or delayed activation, particularly during sleep or early recovery.
Another strategy is the use of time-programmed decremental infusion, in which the background infusion rate is reduced according to a predefined schedule to reflect the predictable temporal pattern of postoperative nociception. This approach aims to provide higher opioid delivery during the early postoperative period while minimizing exposure during later stages. Compared with feedback-regulated PCA strategies, time-programmed decremental infusion enables automatic adjustment of opioid delivery without requiring additional patient interaction or manual intervention, which may be advantageous during nighttime recovery and early postoperative care. A prospective randomized double-blind study in patients undergoing laparoscopic radical surgery for cervical cancer found that time-scheduled decremental infusion of oxycodone reduced cumulative opioid consumption while maintaining analgesia comparable to that of continuous infusion, without increasing sedation, nausea and vomiting, or lowering patient satisfaction.13 In addition, a randomized study of postoperative fentanyl PCA in patients undergoing laparoscopic-assisted hysterectomy under total intravenous anesthesia reported that decremental background infusion regimens were associated with lower pain scores, fewer episodes of inadequate analgesia, and fewer PCA interventions than fixed-rate infusion, particularly during the early postoperative period, without increasing ventilatory depression or postoperative nausea and vomiting.14 Collectively, these findings suggest that aligning opioid delivery with the temporal evolution of postoperative pain may improve analgesic efficiency while maintaining an acceptable safety profile.
Despite these encouraging findings, existing evidence remains limited in several aspects. Most studies have been conducted in single-center settings with relatively small sample sizes and focused on specific surgical populations, thereby limiting external validity and generalizability. In addition, previous decremental infusion studies mainly evaluated opioids such as oxycodone or fentanyl, whereas evidence specifically regarding sufentanil-based intravenous PCA remains limited.
Therefore, we propose a prospective, multicenter, randomized, double-blind controlled trial to compare time-programmed decremental infusion with conventional fixed-rate basal infusion in patients undergoing mixed surgery. We hypothesize that the time-programmed decremental infusion mode will reduce cumulative opioid consumption without compromising analgesic efficacy, thereby offering a practical and effective strategy for optimizing postoperative pain management.
Materials and Methods
Study Design and Setting
This study is a prospective, multicenter, randomized, double-blind, controlled trial that will be conducted at Beijing Tiantan Hospital, China Rehabilitation Research Center, and the Second Affiliated Hospital of Hainan Medical University. The trial is designed to compare the efficacy and opioid-sparing effects of a time-programmed decremental infusion mode with a conventional fixed-rate basal infusion mode in patients receiving intravenous PCA following mixed surgery.
The study protocol has been approved by the Institutional Review Board of Beijing Tiantan Hospital (KY2025-387-02) and other participating centers. The trial will be conducted in accordance with the Declaration of Helsinki and Good Clinical Practice guidelines. Written informed consent will be obtained from all participants prior to enrollment. The trial was prospectively registered at ClinicalTrials.gov (NCT07375121) in January 2026 prior to patient enrollment. All trial procedures are summarized in Table 1, and the flowchart is briefly illustrated in Figure 1.
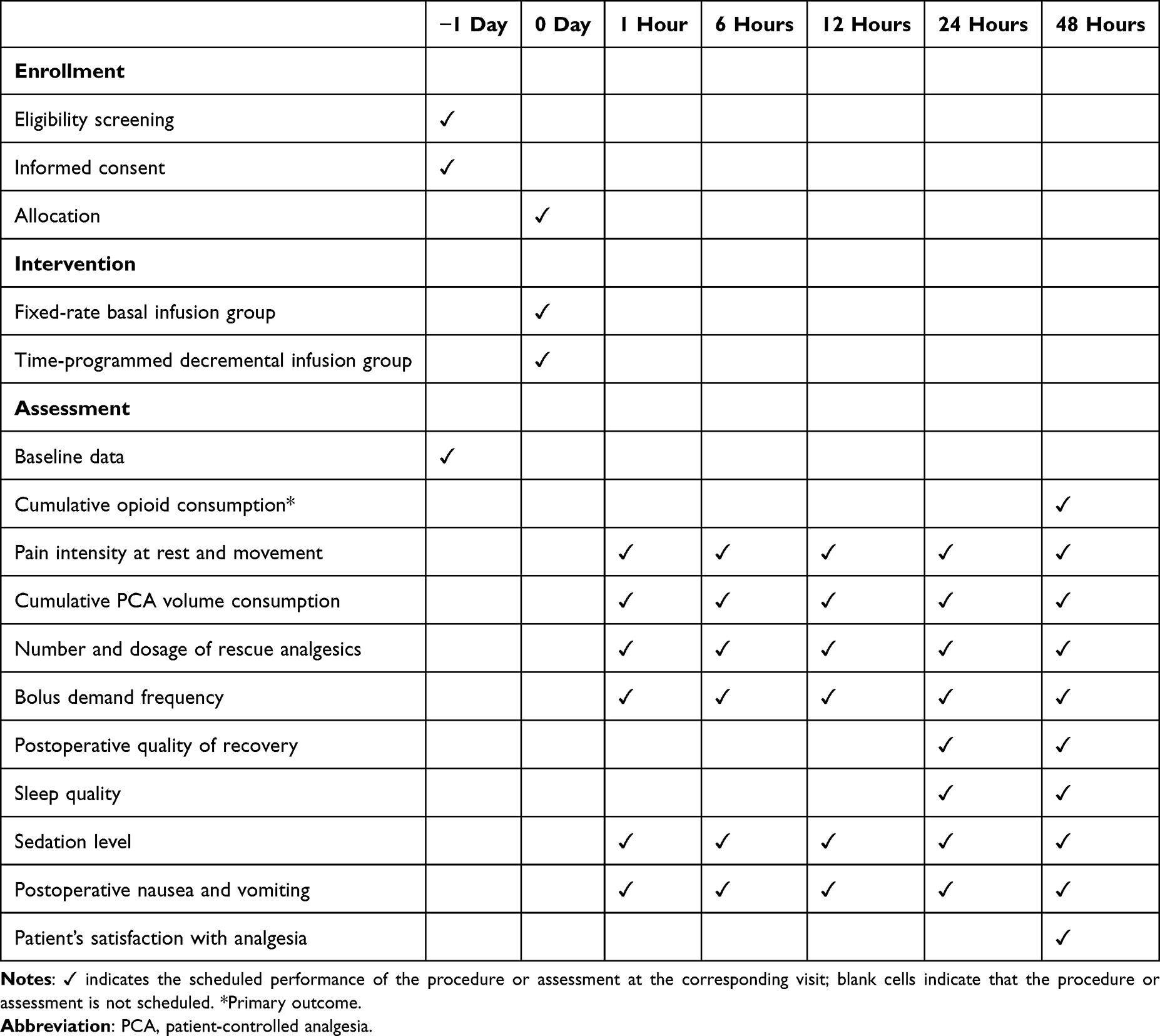 |
Table 1 The Schedule of Enrollment, Interventions, and Assessments |
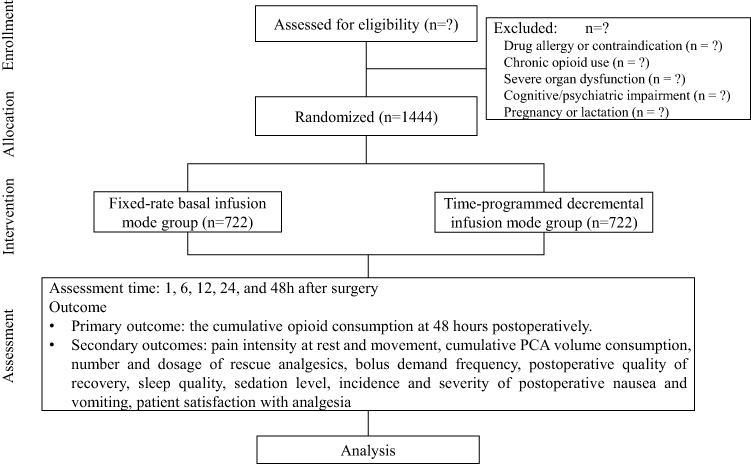 |
Figure 1 Flowchart of enrollment, allocation, intervention, and assessment. |
Participants
Inclusion Criteria
- Age 18–65 years;
- American Society of Anesthesiologists (ASA) physical status I-III;
- Scheduled for elective mixed surgery under general anesthesia, including thoracic, abdominal, spinal, and orthopaedic procedures performed using either minimally invasive or open approaches;
- Ability to understand and operate the PCA device;
- Provision of written informed consent.
Exclusion Criteria
- Known allergy or contraindication to opioids or study medications;
- Pre-existing chronic pain requiring long-term opioid therapy;
- Severe hepatic, renal, cardiovascular, or cerebrovascular dysfunction;
- Psychiatric or cognitive disorders interfering with PCA use;
- Pregnancy or lactation.
Randomization and Blinding
Eligible participants will be randomly assigned in a 1:1 ratio to either the time-programmed decremental infusion group, or the fixed-rate basal infusion group. Randomization will be stratified by study center and type of surgery (including thoracic, abdominal, spinal, and orthopaedic procedures), and surgical approach (minimally invasive or open approaches) using a computer-generated block randomization sequence (block size = 4 or 6) generated via SAS software.
Allocation concealment will be ensured using sequentially numbered, opaque, sealed envelopes. Participants, outcome assessors, clinicians responsible for postoperative evaluation, and statisticians will remain blinded to group allocation. PCA devices will be pre-programmed by an independent investigator not involved in outcome assessment.
Standard Anesthesia Protocol
In the preanesthetic area, all enrolled patients will receive standardized instructions on pain assessment using the numerical rating scale (NRS), where 0 indicates no pain, and 10 indicates the worst imaginable pain, as well as the use of the PCA device (Intelligent Network Pump, TUOREN Medical, Henan, China). All patients will undergo a standardized general anesthesia protocol. No preoperative sedatives will be administered before transfer to the operating room. Upon arrival in the operating room, standard monitoring will be applied, including blood pressure, pulse oximetry, electrocardiography, bispectral index, end-tidal carbon dioxide, minimum alveolar concentration of the inhaled anesthetic, and urine output.
Anesthesia will be induced with sufentanil (0.3–0.4 μg/kg), propofol (1.5–2.5 mg/kg) or ciprofol (0.3–0.4 mg/kg), and mivacurium (0.15–0.25 mg/kg) or cisatracurium (0.1–0.15 mg/kg), followed by endotracheal intubation or double-lumen endobronchial intubation for thoracic procedures. Mechanical ventilation will be maintained with a tidal volume of 6–8 mL/kg, a respiratory rate of 12–15 breaths/min, an inspiratory-to-expiratory ratio of 1:2, and an inspired oxygen fraction of 40–60% at a flow rate of 1–2 L/min, with end-tidal carbon dioxide maintained between 35 and 45 mmHg. Anesthesia will be maintained with remifentanil (0.05–0.2 μg/kg/min) in combination with sevoflurane or desflurane at 0.7–1.2 minimum alveolar concentration to maintain a bispectral index of 40–50 and hemodynamic variables within ±20% of baseline. Supplemental sufentanil (0.1–0.2 μg/kg) will be administered in response to noxious stimulation. Intraoperative analgesia will be titrated based on patient responses and surgical stimuli. Triggers include autonomic signs (eg, lacrimation, sweating), hemodynamic shifts (heart rate or mean arterial pressure >20% above baseline), and intense nociceptive events (eg, skin incision, deep tissue dissection, and wound closure) The remifentanil infusion rate will be titrated within predefined ranges according to intraoperative nociceptive intensity. Supplemental sufentanil will be administered if nociceptive responses persist despite optimal remifentanil titration, or when otherwise clinically indicated.12 Intraoperative fluid therapy will consist of crystalloid infusion at 5–10 mL/kg/h. All patients will additionally receive intravenous flurbiprofen axetil 50 mg every 12 hours postoperatively as part of standardized multimodal analgesia unless contraindicated. Regional anesthesia and local anesthetic infiltration will not be used. All drug doses and fluid volumes will be calculated on the basis of ideal body weight.
Intervention
All patients will receive a standardized intravenous PCA solution containing 200 μg of sufentanil and 32 mg of ondansetron, diluted with normal saline to a total volume of 200 mL. Similar PCA regimens have been reported in previous postoperative analgesia studies,5,15 and prior in vitro studies have demonstrated the physicochemical stability of sufentanil and ondansetron mixtures in PCA delivery systems.16,17 The PCA device used will be a network-integrated intelligent infusion pump capable of automated data recording.
In the fixed-rate basal infusion group, which served as the control group, the PCA device will be programmed to deliver a bolus dose of 2 mL with a lockout interval of 15 minutes and a constant background infusion rate of 2 mL/h throughout the postoperative period. This setting was based on prior sufentanil-based PCA studies.5,18 In the time-programmed decremental infusion group, which served as the intervention group, the bolus dose and lockout interval will remain the same, whereas the background infusion rate will be reduced according to a predefined postoperative schedule intended to reflect the general temporal decline in postoperative pain intensity and opioid requirements.8 Specifically, the background infusion rate will be set at 4.0 mL/h during the first 6 postoperative hours, reduced to 3 mL/h from 6 to 12 hours, decreased to 2.0 mL/h from 12 to 24 hours, and further reduced to 1.0 mL/h from 24 to 48 hours after surgery. Because there is currently no established time-programmed decremental infusion formula specifically for sufentanil in postoperative PCA, the dosing schedule in the present study was developed with reference to previously published decremental infusion regimens of other opioids, including fentanyl, oxycodone, and alfentanil, as well as their relative potency relationships.13,14,19
At the end of surgery, patients will be transferred to the post-anesthesia care unit, where PCA instructions will be reinforced. Postoperative pain intensity will be assessed using the NRS. When postoperative pain remains inadequately controlled despite PCA use, particularly when the NRS pain score exceeds 4 during the lockout interval, rescue analgesia may be administered at the discretion of the attending physician using an oral combination tablet containing oxycodone hydrochloride 5 mg and acetaminophen 325 mg. Rescue analgesics may be administered at intervals of no less than 6 hours, with a maximum daily dose of four tablets.
Data Management and Quality Control
Study data will be collected by trained investigators using protocol-specific standardized case report forms. To ensure data integrity and accuracy, all study information will be entered into a centralized electronic data management system (EpiData Manager, version 4.6.0.6; EpiData Association, Denmark). Independent double data entry will be performed for data verification, and any discrepancies between the two datasets will be checked against the original source documents and resolved accordingly.
An independent Data and Safety Monitoring Committee will be established to oversee trial conduct and safety. The committee will meet twice yearly to review cumulative safety data, trial progress, and overall protocol adherence. Based on these evaluations, the committee will provide formal recommendations to the Steering Committee regarding trial continuation, protocol modification, or early termination, if necessary.
Patient and Public Involvement
Patients and members of the public were not involved in formulating the research question, designing the study protocol, or selecting the outcome measures. Participants will be recruited through physician referral at the participating multicenter sites.
After study completion, the findings will be disseminated through presentations at scientific conferences and publication in peer-reviewed journals. In addition, a plain-language summary of the study results will be made available to participants upon request after completion of the final data analysis.
Outcomes
Primary Outcome
The primary outcome is the cumulative opioid consumption at 48 hours postoperatively.
Secondary outcomes
Secondary outcomes are assessed at 1, 6, 12, 24, and 48 hours postoperatively.
- Pain intensity at rest and movement will be assessed using the NRS. Movement-evoked pain will be evaluated during activities including coughing, deep breathing, limb movement, sitting up, or turning in bed.20
- Cumulative PCA volume consumption.
- Number and dosage of rescue analgesics.
- Bolus demand frequency.
- Postoperative quality of recovery will be assessed using the validated Chinese version of the 15-item Quality of Recovery questionnaire, a validated patient-reported outcome measure that evaluates recovery across multiple dimensions, including physical comfort, emotional state, physical independence, psychological support, and pain. Higher scores indicate better postoperative recovery.21
- Sleep quality will be assessed using the Medical Outcomes Study Sleep Scale, which evaluates several domains of sleep, including sleep disturbance, sleep adequacy, somnolence, and overall sleep problems. This instrument will be used to assess postoperative sleep quality during the study period.22
- Sedation level will be evaluated using the Richmond Agitation-Sedation Scale.23 This scale ranges from +4, indicating combative behavior, to −5, indicating an unarousable state, with 0 representing an alert and calm patient. It will be used to monitor the level of postoperative sedation and agitation.
- Incidence and severity of postoperative nausea and vomiting (PONV) will be defined as the occurrence of any nausea, retching, or vomiting within 48 hours after surgery. PONV severity will be assessed using an 11-point NRS ranging from 0 to 10, with higher scores indicating greater intensity. Clinically important PONV will be defined as any vomiting episode or nausea rated ≥4 on the NRS.24
- Patient satisfaction with analgesia.
Data Collection and Management
All data will be collected prospectively by a research assistant who is blinded to group allocation. After written informed consent is obtained, baseline data will be collected 1 day before surgery, including sex, age, height, weight, medical history, medication history, ASA physical status, and education level. Perioperative variables will include surgical type, surgical approach, surgical incision size, type of intubation, duration of anesthesia and surgery, intraoperative fluid administration, blood loss, urine output, and total intraoperative doses of sufentanil and remifentanil.
Secondary outcomes will be assessed at 1, 6, 12, 24, and 48 hours after surgery. PCA-related data, including cumulative opioid consumption, cumulative PCA volume, postoperative pain scores, bolus demand counts, and background infusion rates, will be directly downloaded from the device through its built-in mobile network system. The number of patients requiring additional rescue analgesia will be recorded at 1, 6, 24, and 48 hours after surgery. Postoperative quality of recovery, sleep quality, functional activity, and overall satisfaction with PCA will also be assessed. Safety outcomes will include the incidence and severity of opioid-related adverse events, particularly sedation, nausea, and vomiting.
Sample Size Calculation
The sample size was estimated based on the primary outcome of cumulative sufentanil consumption at 48 hours after surgery using PASS 11.0 software (NCSS, LLC, USA). Because no established reference values are available for sufentanil consumption using time-programmed decremental infusion, the estimation was informed by previously published studies of opioid consumption in intravenous PCA. In a randomized study investigating optimized background infusion strategies reported cumulative sufentanil consumption of 169.1 ± 35.9 μg and 181.8 ± 34.8 μg at 48 hours.10 Considering the variability in surgical procedures and analgesic requirements, and to provide a conservative and clinically realistic estimate for a mixed surgical population, the expected cumulative sufentanil consumption in the present study was assumed to be 151.0 ± 50.0 μg in the fixed-rate basal infusion group and 142.0 ± 50.0 μg in the time-programmed decremental infusion group. Based on these assumptions, a total of 649 patients per group would be required to achieve 90% power at a two-sided significance level of 0.05. Allowing for a 10% dropout rate, the final sample size was set at 722 patients per group, resulting in a total of 1444 patients to be enrolled in the study. A 9 μg reduction in cumulative sufentanil consumption approximately corresponds to a 9 mg reduction in morphine consumption based on commonly accepted opioid conversion ratios, which is within the range of clinically meaningful postoperative opioid reduction reported in previous anchor-based studies.25 However, because no universally accepted minimal clinically important difference has been established for postoperative opioid consumption, the clinical relevance of opioid reduction in the present study will be interpreted together with analgesic efficacy, rescue analgesic requirements, and opioid-related adverse events.
Statistical Analysis
All statistical analyses will be performed using IBM SPSS Statistics version 27.0 (IBM Corp., Armonk, NY, USA). Statistical analysis will be conducted primarily according to the intention-to-treat principle, including all randomized patients. A per-protocol analysis may also be performed as a sensitivity analysis to assess the robustness of the primary findings.
Continuous variables will first be assessed for normality using the Shapiro–Wilk test. Normally distributed continuous variables will be presented as mean ± standard deviation and compared using Student’s t-test, whereas non-normally distributed variables will be expressed as median and interquartile range and compared using the Mann–Whitney U-test. Categorical variables will be summarized as frequencies and percentages and analyzed using the chi-square test or Fisher’s exact test, as appropriate.
The primary outcome, cumulative opioid consumption at 48 hours after surgery, will be analyzed using an adjusted linear regression model with treatment group as the primary independent variable. Predefined covariates will include study center, surgical type, surgical approach, age, gender, ASA physical status. Treatment effect will be presented as adjusted mean difference with corresponding 95% confidence intervals. Unadjusted between-group comparisons using Student’s t-test or the Mann–Whitney U-test will additionally be performed as sensitivity analyses where appropriate. Subgroup analyses will be performed according to age, sex, ASA physical status, study center, surgery duration, type of surgery, and surgical approach to explore the consistency of the treatment effect across clinically relevant subgroups. These subgroup analyses will be considered exploratory. Missing data for the primary outcome will initially be assessed using complete-case analysis. If the extent of missing data is substantial, sensitivity analyses using multiple imputation under the missing-at-random assumption will be performed. The imputation model will include treatment group, baseline characteristics, and available postoperative outcome measurements. Worst-case scenario analyses may additionally be conducted as robustness analyses.
Repeated continuous secondary outcomes, including pain scores, cumulative PCA volume, and other postoperative measures, will be analyzed using linear mixed-effects models including treatment group, time, and treatment-by-time interaction as fixed effects, with participant-level random effects where appropriate.
All tests will be two-sided, and a P value < 0.05 will be considered statistically significant.
Discussion
This multicenter randomized controlled trial is designed to determine whether a time-programmed decremental infusion mode can reduce cumulative opioid consumption while maintaining adequate analgesia compared with a conventional fixed-rate basal infusion mode in patients undergoing mixed surgery. Because postoperative pain management requires a balance between effective analgesia and opioid minimization, optimizing PCA infusion strategies remains clinically important.
A major strength of this study is its multicenter design and inclusion of a mixed surgical population. Previous studies of decremental infusion have largely been conducted in single-center settings and within relatively specific surgical populations, such as gynecologic or laparoscopic procedures.13,14 Although those studies have provided important preliminary evidence, their generalizability is limited. By enrolling patients undergoing mixed surgery across multiple centers, the present trial may provide more externally valid evidence for the effectiveness of time-programmed decremental infusion in routine clinical practice.
Several limitations should be considered. Although stratified randomization will be used according to surgical type, the inclusion of a mixed surgical population may still introduce heterogeneity in postoperative pain intensity and analgesic requirements, which should be considered when interpreting the study findings. In addition, although cumulative opioid consumption is an objective and clinically meaningful primary endpoint, subjective outcomes such as pain scores and patient satisfaction may be influenced by individual factors. Finally, the decremental infusion schedule in this study is based on general postoperative pain patterns rather than individual analgesic demand, and future studies may be needed to evaluate more personalized infusion strategies.
In summary, this trial will provide evidence on the efficacy of time-programmed decremental infusion for intravenous PCA after mixed surgery. By aligning opioid delivery with the temporal course of postoperative pain, this approach may reduce cumulative opioid consumption without compromising analgesic efficacy and may help refine postoperative PCA strategies.
Abbreviations
PCA, patient-controlled analgesia; ASA, American Society of Anesthesiologists; NRS, numerical rating scale; PONV, postoperative nausea and vomiting.
Provenance and Peer Review
Not commissioned, externally peer reviewed.
Data Sharing Statement
This is the protocol only; no participant data are included.
Patient Consent for Publication
Obtained.
Acknowledgment
The recruitment for this study is ongoing. We anticipate that it will take approximately 2 years to complete this trial.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Key Research and Development Program of China (No. 2022YFC3602200, No. 2022YFC3602201, No. 2022YFC3602202, No. 2022YFC3602203, No. 2022YFC3602205), and the National Health Commission Capacity Building and Continuing Education Center Cancer Pain Management (No. PMT1001-1). The sponsors were not involved in the trial design, trial conduct, data handling, data analysis, interpretation, manuscript preparation, or the decision to submit the article for publication.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Mitra S, Carlyle D, Kodumudi G, Kodumudi V, Vadivelu N. New advances in acute postoperative pain management. Curr Pain Headache Rep. 2018;22(5):35. doi:10.1007/s11916-018-0690-8
2. Momeni M, Crucitti M, De Kock M. Patient-controlled analgesia in the management of postoperative pain. Drugs. 2006;66(18):2321–10. doi:10.2165/00003495-200666180-00005
3. Smith HS. The metabolism of opioid agents and the clinical impact of their active metabolites. Clin J Pain. 2011;27(9):824–838. doi:10.1097/AJP.0b013e31821d8ac1
4. Monk JP, Beresford R, Ward A. Sufentanil. A review of its pharmacological properties and therapeutic use. Drugs. 1988;36(3):286–313. doi:10.2165/00003495-198836030-00003
5. Oh SK, Lee IO, Lim BG, et al. Comparison of the analgesic effect of sufentanil versus fentanyl in intravenous patient-controlled analgesia after total laparoscopic hysterectomy: a randomized, double-blind, prospective study. Int J Med Sci. 2019;16(11):1439–1446. doi:10.7150/ijms.34656
6. Ved SA, Dubois M, Carron H, Lea D. Sufentanil and alfentanil pattern of consumption during patient-controlled analgesia: a comparison with morphine. Clin J Pain. 1989;5(Suppl 1):S63–S70. doi:10.1097/00002508-198903001-00012
7. Nielsen RV, Fomsgaard JS, Dahl JB, Mathiesen O. Insufficient pain management after spine surgery. Dan Med J. 2014;61(5):A4835.
8. Chapman CR, Davis J, Donaldson GW, Naylor J, Winchester D. Postoperative pain trajectories in chronic pain patients undergoing surgery: the effects of chronic opioid pharmacotherapy on acute pain. J Pain. 2011;12(12):1240–1246. doi:10.1016/j.jpain.2011.07.005
9. Chen W-H, Liu K, Tan P-H, Chia Y-Y. Effects of postoperative background PCA morphine infusion on pain management and related side effects in patients undergoing abdominal hysterectomy. J Clin Anesth. 2011;23(2):124–129. doi:10.1016/j.jclinane.2010.08.008
10. Jung KT, So KY, Kim SU, Kim SH. The optimizing background infusion mode decreases intravenous patient-controlled analgesic volume and opioid consumption compared to fixed-rate background infusion in patients undergoing laparoscopic cholecystectomy: a prospective, randomized, controlled, double-blind study. Medicina. 2021;57(1):42. doi:10.3390/medicina57010042
11. Jang YK, Kim NY, Lee JS, et al. Comparison of postoperative pain and adverse effects between variable-rate feedback infusion and conventional fixed-rate basal infusion modes of patient-controlled epidural analgesia following open gastrectomy: a randomized controlled trial. Int J Environ Res Public Health. 2021;18(16):8777. doi:10.3390/ijerph18168777
12. Lee SH, Baek CW, Kang H, et al. A comparison of 2 intravenous patient-controlled analgesia modes after spinal fusion surgery: constant-rate background infusion versus variable-rate feedback infusion, a randomized controlled trial. Medicine. 2019;98(10):e14753. doi:10.1097/MD.0000000000014753
13. Zhu Y, Xie K, Yuan J, et al. Efficacy of oxycodone in intravenous patient-controlled analgesia with different infusion modes after laparoscopic radical surgery of cervical cancer a prospective, randomized, double-blind study. Medicine. 2019;98(34):e16810. doi:10.1097/MD.0000000000016810
14. Kim J-Y, Park S-Y, Chang HS, Nam S-K, Min S-K. The efficacy of the time-scheduled decremental continuous infusion of fentanyl for postoperative patient-controlled analgesia after total intravenous anesthesia. Korean J Anesthesiol. 2013;65(6):544–551. doi:10.4097/kjae.2013.65.6.544
15. Yang C, Geng WL, Hu J, Huang S. The effect of gestational diabetes mellitus on sufentanil consumption after cesarean section: a prospective cohort study. BMC Anesthesiol. 2020;20(1):14. doi:10.1186/s12871-019-0925-1
16. Chapalain-Pargade S, Laville I, Paci A, Chachaty E, Mercier L, Bourget P. Microbiological and physicochemical stability of fentanyl and sufentanil solutions for patient-controlled delivery systems. J Pain Symptom Manage. 2006;32(1):90–97. doi:10.1016/j.jpainsymman.2006.01.006
17. Lee CH, Kim AR, Lee MK, Oh JS, Lee DK, Choi SS. Intravenous patient-controlled analgesia: in vitro stability profiles of mixtures containing fentanyl, hydromorphone, oxycodone, nefopam, ondansetron, and ramosetron. J Anal Sci Technol. 2020;11(1):32. doi:10.1186/s40543-020-00230-w
18. Li S, Li R, Li M, et al. Dexmedetomidine administration during brain tumour resection for prevention of postoperative delirium: a randomised trial. Br J Anaesth. 2022;130(2):e307–e316. doi:10.1016/j.bja.2022.10.041
19. Kwon YS, Jang JS, Lee NR, et al. A comparison of oxycodone and alfentanil in intravenous patient-controlled analgesia with a time-scheduled decremental infusion after laparoscopic cholecystectomy. Pain Res Manag. 2016;2016:7868152. doi:10.1155/2016/7868152
20. Leemans L, Polli A, Nijs J, Wideman T, den Bandt H, Beckwée D. It hurts to move! Intervention effects and assessment methods for movement-evoked pain in patients with musculoskeletal pain: a systematic review with meta-analysis. J Orthop Sports Phys Ther. 2022;52(6):345–374. doi:10.2519/jospt.2022.10527
21. Stark PA, Myles PS, Burke JA. Development and psychometric evaluation of a postoperative quality of recovery score: the QoR-15. Anesthesiology. 2013;118(6):1332–1340. doi:10.1097/ALN.0b013e318289b84b
22. Hays RD, Martin SA, Sesti AM, Spritzer KL. Psychometric properties of the medical outcomes study sleep measure. Sleep Med. 2005;6(1):41–44. doi:10.1016/j.sleep.2004.07.006
23. Ely EW, Truman B, Shintani A, et al. Monitoring sedation status over time in ICU patients: reliability and validity of the Richmond Agitation-Sedation Scale (RASS). JAMA. 2003;289(22):2983–2991. doi:10.1001/jama.289.22.2983
24. Rambod M, Pasyar N, Karimian Z, Farbood A. The effect of lemon inhalation aromatherapy on pain, nausea, as well as vomiting and neurovascular assessment in patients for lower extremity fracture surgery: a randomized trial. BMC Complement Med Ther. 2023;23(1):208. doi:10.1186/s12906-023-04047-z
25. Karlsen APH, Laigaard J, Pedersen C, et al. Minimal important difference in postoperative morphine consumption after Hip and knee arthroplasty using nausea, vomiting, sedation and dizziness as anchors. Acta Anaesthesiol Scand. 2024;68(5):610–618. doi:10.1111/aas.14388
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.