Back to Journals » Journal of Inflammation Research » Volume 15
Comparison of Clinical Characteristics and Risk Factors for Recurrence of Kikuchi–Fujimoto Disease Between Children and Adult
Authors Baek JY, Kang JM, Lee JY, Lim SM, Ahn JG ![]()
Received 16 June 2022
Accepted for publication 8 September 2022
Published 22 September 2022 Volume 2022:15 Pages 5505—5514
DOI https://doi.org/10.2147/JIR.S378790
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Jee Yeon Baek,1 Ji-Man Kang,1,2 Ji Young Lee,1 Sung Min Lim,1 Jong Gyun Ahn1,2
1Department of Pediatrics, Severance Children’s Hospital, Yonsei University College of Medicine, Seoul, Korea; 2Institute for Immunology and Immunological Diseases, Yonsei University College of Medicine, Seoul, Korea
Correspondence: Jong Gyun Ahn, Department of Pediatrics, Severance Children’s Hospital, Yonsei University College of Medicine, 50-1 Yonsei-ro, Seodaemun-gu, Seoul, 03722, Korea, Tel +82-2-2228-2057, Fax +82-2-393-9118, Email [email protected]
Purpose: Kikuchi–Fujimoto disease (KFD) is a rare, benign, and self-limited disease, characterized by cervical lymphadenopathy and fever. Herein, we analyzed the differences in its clinical manifestations and risk factors for recurrence between children and adults.
Patients and Methods: We retrospectively reviewed the medical records of patients diagnosed with KFD at a tertiary referral hospital between 2005 and 2019. Patients were divided into two groups based on their age: children (< 19 years) and adults (≥ 19 years).
Results: During the 14-year study period, 127 patients were diagnosed with KFD. Among these, 34 (26.8%) were children and 93 (73.2%) were adults. The fever duration was longer and the frequency of myalgia was higher in adults than in children; however, no other significant symptomatic differences were noted between the two groups. Lymph node evaluation was mainly performed using ultrasound in children (61.8%) and computed tomography in adults (78.5%). Moreover, the frequency of antibiotic use was higher in children than in adults (76.5% vs 54.8%, P = 0.027). In adults, multivariable logistic regression analysis revealed anti-nuclear antibody (ANA) positivity (titer ≥ 1:80) as a risk factor for recurrence (odds ratio: 7.813; 95% confidence interval = 1.818– 33.333; P = 0.006).
Conclusion: The clinical features of KFD in children and adults were similar; however, the preferred imaging study and frequency of antibiotic use differed significantly between the two groups. Furthermore, in adults, ANA positivity was associated with KFD recurrence. Thus, patients with KFD who present with ANA positivity at diagnosis will benefit from a regular follow-up for monitoring KFD recurrence.
Keywords: histiocytic necrotizing lymphadenitis, recurrence, child, adult
Introduction
Histiocytic necrotizing lymphadenitis (or the Kikuchi–Fujimoto disease [KFD]) is a rare benign disease in which patients mainly present with fever and lymphadenitis of the neck. Other symptoms include rashes, arthritis, and fatigue.1 In KFD, lymph node biopsy usually reveals lymph node necrosis and histiocytic infiltration, which are used as the basis for diagnosis.2,3 KFD is differentiated from other serious conditions (such as lymphomas, systemic lupus erythematosus [SLE], and tuberculosis) by analyzing the patient’s clinical manifestations, laboratory findings, and imaging or pathological findings.4–6
Although the pathophysiology of KFD remains unclear, it is thought to involve the immune responses of T cells and histiocytes to infectious agents, such as Yersinia spp., Toxoplasma gondii, Epstein–Barr virus, human immunodeficiency virus, and parvovirus.7–15 However, the exact causative pathogen has not yet been identified.
Although mostly self-limiting, KFD may recur in some patients. In fact, the recurrence rates of KFD generally range from 3% to 4%,16 although some studies have reported even higher recurrence rates of up to 42.4% among children.17–23 The risk factors for KFD recurrence remain unknown. Furthermore, in some patients, KFD may even progress to autoimmune diseases (such as SLE).
With respect to pathogenicity, the clinical course of KFD may differ between children and adults due to inherent differences in the immune responses between the two groups. Thus, in this study, we aimed to investigate the clinical features of KFD and the risk factors for its recurrence in children and adults.
Materials and Methods
Study Design and Data Collection
We reviewed the medical charts of patients diagnosed with KFD based on lymph node biopsy findings between November 2005 and December 2019 at Severance Hospital (Seoul, South Korea). KFD was diagnosed by pathologists based on the histological findings of the affected lymph nodes. Patients for whom pathology review terms were consistent with the diagnosis of KFD were included in our study; these terms were “subacute necrotizing lymphadenitis”, “necrotizing subacute lymphadenitis”, “Kikuchi’s disease”, “Kikuchi–Fujimoto disease”, and “Kikuchi lymphadenitis.” The following patients were excluded from our study: (1) patients for whom a pathology review was not performed at our center, (2) patients with incomplete medical records, (3) patients who were initially diagnosed with KFD but were later diagnosed with other diseases after several months of follow-up care and further evaluations, and (4) patients who were diagnosed with forms of histiocytic necrotizing lymphadenitis secondary to other etiologies (such as SLE). Patients aged <19 years and those aged ≥19 years were categorized as children and adults, respectively.
We retrieved data on the following variables: locations of the symptomatic lymph nodes, clinical symptoms (fever duration, rash, arthralgia, myalgia, fatigue, loss of appetite, and headache), laboratory findings (complete blood count; erythrocyte sedimentation rate; anti-nuclear antibody [ANA] positivity and titer; and serum levels of C-reactive protein [CRP], procalcitonin, lactate dehydrogenase, ferritin, alanine transaminase, and aspartate transaminase), imaging findings, pathological findings, treatments, follow-up details, and recurrence rates. Fever duration was defined as the period between the onset and subsidence of fever; using medical records, we reviewed the patients’ prehospitalization history of fever and their fever patterns during hospitalization to determine their fever duration. ANA positivity was defined by a titer ≥1:80.
A standardized definition of KFD recurrence was unavailable; thus, we defined it as the recurrence of symptomatic lymphadenitis at least 1 week after a complete clinical resolution, irrespective of whether the pathological lymph nodes affected were the same as those affected initially.
The primary outcome of this study was a comparison of the characteristics between pediatric and adult KFD. The secondary outcomes were the potential risk factors for the recurrence of KFD in children and adults.
Statistical Analysis
The data were analyzed using SAS, version 9.4 (SAS Inc., Cary, NC, USA). The Shapiro–Wilk test was used to test for normality. Normally distributed continuous variables are expressed as mean ± standard deviation; they were analyzed using Student’s t-test. Non-normally distributed continuous variables are expressed as medians and interquartile ranges (IQRs); they were analyzed using the Wilcoxon rank-sum test. Categorical variables are expressed as counts (%) and were analyzed using the chi-square test or Fisher’s exact test, as appropriate.
Potential risk factors for KFD recurrence were identified through a univariable logistic regression analysis. Risk factors that were identified as significant (P <0.05) by the univariable analysis were used for performing a multivariable logistic regression analysis to generate the odds ratios (ORs) and 95% confidence intervals (CIs). P-values of <0.05 were considered statistically significant.
Results
Patient Characteristics
Among the patients diagnosed with KFD during the study period, 140 were diagnosed based on biopsy findings of histiocytic necrotizing lymphadenitis. Among these, six, three, and four patients were excluded from the study because their conditions were diagnosed at other medical centers and lacked pathology reviews, had incomplete medical records, and were later diagnosed with other diseases after a complete evaluation and follow-up care, respectively.
Thus, 127 patients (34 children and 93 adults) were considered eligible for inclusion in this study. Among these, 15 patients (11.8%; 3 children and 12 adults) experienced KFD recurrence.
Comparison of the Clinical Features of KFD Between Children and Adults
Table 1 presents a comparison of the clinical features of KFD between children and adults. The fever duration was significantly longer in adults than in children (18 vs 13.5 days, P = 0.037). Myalgia was also significantly more prevalent in adults than in children (17.2% vs, 2.9%, P = 0.040). Regarding laboratory findings, the median serum levels of CRP and ferritin were significantly higher in adults than in children (CRP: 24.35 vs 12.3 mg/L, P = 0.003; ferritin: 376.9 vs 214 ng/mL, P = 0.003). The absolute lymphocyte count was lower in adults than in children (981/μL vs 1314/μL, P = 0.001). The neutrophil percentage, absolute neutrophil count, lymphocyte percentage, and platelet count differed significantly between adults and children; however, their median values and IQRs barely deviated from their corresponding normal ranges. The remaining clinical features did not differ significantly between the groups.
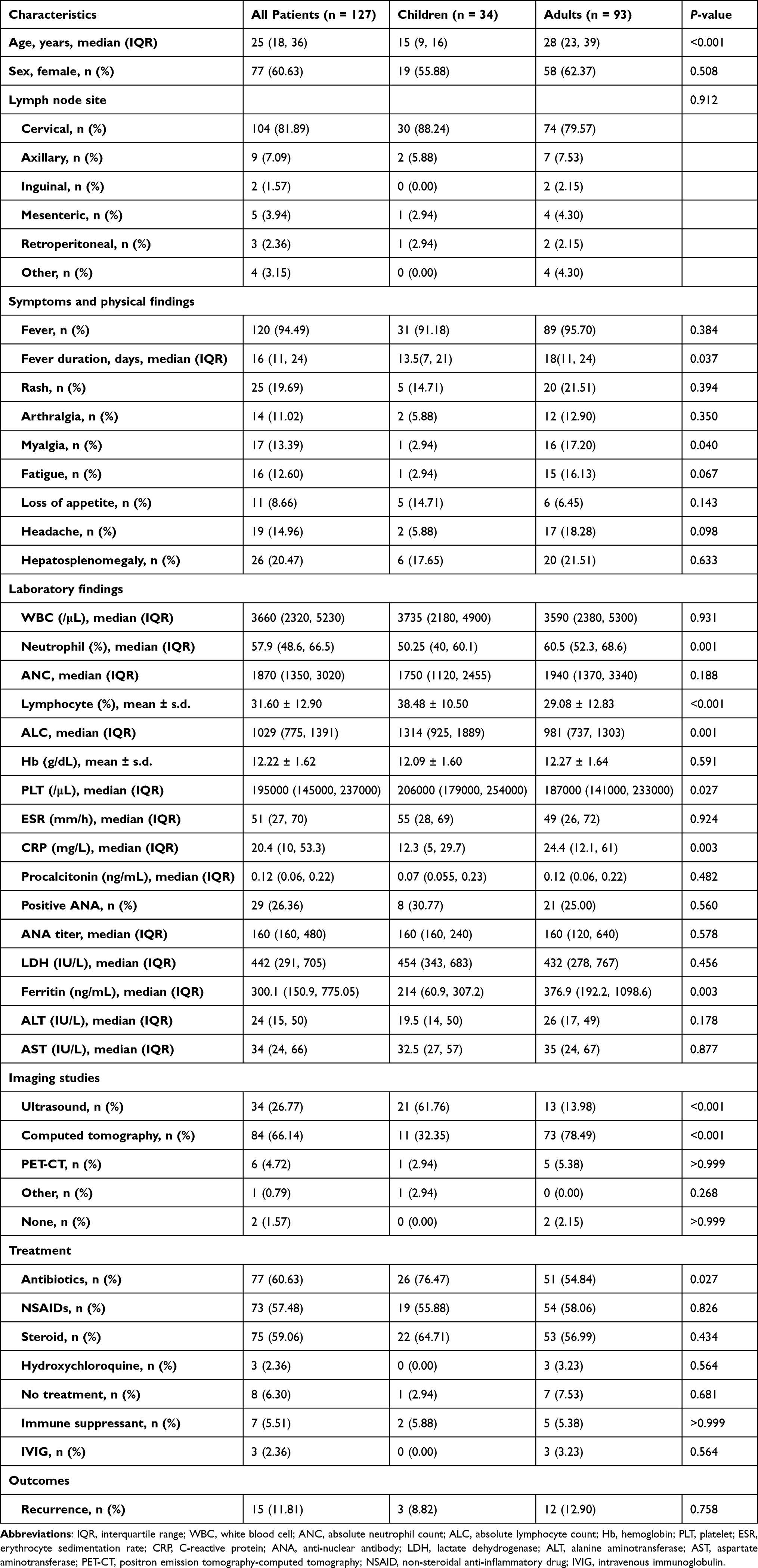 |
Table 1 Comparison of Clinical Features of Children and Adults with Kikuchi–Fujimoto Disease |
Regarding imaging studies, ultrasound was performed more frequently in children (61.8%), while computed tomography (CT) was performed more frequently in adults (78.5%). Antibiotics were administered more frequently in children than in adults (76.5% vs 54.8%, P = 0.027). However, the KFD recurrence rates did not differ significantly between the groups.
The follow-up duration and time to recurrence were also compared between children and adults with KFD recurrence. The median follow-up periods in children and adults with KFD recurrence were 60.2 months (IQR: 30.6–64.1 months) and 53.8 months (IQR: 27.1–110 months), respectively. The median time to recurrence in children and adults with KFD recurrence were 32.7 months (IQR: 16.8–50.1 months) and 16.5 months (IQR: 1.2–51.3 months), respectively. However, these differences were not significant (follow-up period: P = 0.536; time to recurrence: P = 1.000). No patients with recurrence were lost to follow-up. Conversely, one child and seven adults with no recurrence did not visit the outpatient clinic after treatment, respectively, and were lost to follow-up.
Risk Factors for KFD Recurrence
Among the 34 children with KFD, 3 experienced a recurrence after treatment completion; however, no significant differences in the clinical characteristics were observed between children with and without KFD recurrence (Table 2). Conversely, among the 93 adults with KFD, 12 experienced a recurrence after treatment completion. Univariable analysis revealed that arthralgia, ANA positivity, alanine aminotransferase level, aspartate aminotransferase level, and hydroxychloroquine usage were significant risk factors for KFD recurrence in adults. However, multivariable analysis revealed that only ANA positivity (OR: 7.813; 95% CI = 1.818–33.333; P = 0.006) was significantly associated with KFD recurrence in adults (Table 3); however, no risk factors were identified for KFD recurrence in children.
 |
Table 2 Risk Factors for Kikuchi–Fujimoto Disease Recurrence in Children |
 |
Table 3 Risk Factors for Kikuchi–Fujimoto Disease Recurrence in Adults |
Discussion
The present study focused on the differences in the clinical features and risk factors for KFD recurrence between children and adults. We found that with the exception of the imaging studies performed and the antibiotic usage frequency, most clinical features were similar between the two groups. Furthermore, ANA positivity was a significant risk factor for KFD recurrence in adults; however, no such risk factors were identified for KFD recurrence in children.
While the prevalence of KFD is increasing in children, only few studies have compared the clinical differences between pediatric and adult KFD. In terms of clinical symptoms, patients with KFD can present with fever; accordingly, most studies on KFD have only demonstrated the presence of fever or the duration of fever in one group but have not compared these between children and adults.17,18,21–26
Herein, we found that the duration of fever was longer, and myalgia was more common in adults than in children. The shorter fever duration in children can probably be explained by an earlier initiation of treatment, since caregivers tend to present their children to the hospital earlier. The greater prevalence of myalgia in adults may be explained by the fact that children cannot describe their symptoms properly; thus, caregivers or healthcare providers cannot diagnose myalgia without sufficient details. Another study also revealed that myalgia was more common in adults with KFD than in children with KFD, thereby corroborating our findings.24
Regarding laboratory findings, inflammatory marker levels (ie, CRP and ferritin levels) tended to be more elevated in adults than in children; this may be explained by the longer fever duration in adults than in children. The laboratory courses seemed to be better in children with KFD than in adults with KFD, because as mentioned previously, children seemed to visit the hospital and start treatment earlier than adults. Conversely, a few studies have noted no significant differences in the laboratory findings between adults and children with KFD.24,27
The choice of imaging studies also differed between the groups. For children with KFD, ultrasound was preferred over CT for lymph node evaluation; however, for adults with KFD, CT was preferred over ultrasound. In children, ultrasound is often preferred over CT to reduce the radiation exposure and avoid sedation.
Regarding KFD treatment, antibiotics were used significantly more frequently in children than in adults. This suggests that when children visit hospitals for fever or lymphadenopathy, medical practitioners tend to speculate bacterial infections and prescribe empiric antibiotics. There were no differences in other treatments between adults and children with KFD.
No significant risk factors were identified for KFD recurrence in children. However, ANA positivity was significantly associated with KFD recurrence in adults. In a risk assessment study on KFD recurrence, patients with recurrent KFD had significantly more extranodal symptoms, higher prevalence of lymphopenia, and longer durations of lymphocyte count recovery.28 Another study revealed that extranodal involvement and a long duration of symptoms were significant predictors of KFD recurrence. ANA positivity was more prevalent in the recurrent KFD group in that study, which is also consistent with our observations.29 Thus, adults with KFD and ANA positivity should undergo regular follow-up for KFD recurrence monitoring; this also applies to children with KFD and ANA positivity, because although no risk factors for KFD recurrence were identified for this population, KFD can relapse in adulthood in these individuals.
The strength of our study lies in the fact that it is one of the few studies to separately analyze the risk factors for KFD recurrence in both children and adults.
Our study also has some limitations. These include its retrospective and single-center design, relatively small sample size (patients were grouped by age into children and adults), and inclusion of an even smaller number of patients with KFD recurrence. Therefore, our findings may not be representative of all adults and children with KFD. A study with a larger population of patients with KFD recurrence is warranted. Furthermore, eight patients with no KFD recurrence were lost to follow-up, and it is unknown whether they experienced a recurrence later in life. However, considering that patients with a poor prognosis or with a recurrence tend to visit the hospital again, we speculate that most of these eight patients may not have experienced a recurrence; thus, this population may not have a significant impact on our findings.
Conclusion
Children and adults with KFD presented with similar clinical manifestations but differed in terms of the preferred imaging study and frequency of antibiotic use. However, these differences can be explained by the typical differences between pediatric and adult practices and the corresponding practices of the healthcare providers. Interestingly, ANA positivity was more prevalent in adults than in children with KFD, suggesting that a longer follow-up period in those with ANA positivity at diagnosis would help in the surveillance of recurrence.
Abbreviations
ANA, anti-nuclear antibody; CI, confidence intervals; CT, computed tomography; KFD, Kikuchi–Fujimoto disease; OR, odds ratios.
Data Sharing Statement
The data supporting the results reported in the manuscript are available from the corresponding author upon reasonable request.
Ethics
This study was conducted ethically in accordance with the standards laid down by the World Medical Association and the Declaration of Helsinki. The study was approved by the institutional review board of the Yonsei University Health System (no. 4-2021-1086). The requirement for obtaining informed consent was waived due to the retrospective study design. Patient’s data including patients’ privacy and personal identifiable information were protected with strict confidentiality throughout the study.
Acknowledgments
This study was supported by the National Research Foundation of Korea (NRF) grant funded by the Korean government (MSIT) (No. 2022R1G1A100844111) and the faculty research grant of Yonsei University College of Medicine (6-2021-0145). The sponsor had no involvement in any of the stages from study design to submission of the paper for publication.
Disclosure
The authors report no conflicts of interest related to this work.
References
1. Ahmed Z, Quadir H, Hakobyan K, et al. Kikuchi-Fujimoto Disease: a Rare Cause of Cervical Lymphadenopathy. Cureus. 2021;13(8):e17021. doi:10.7759/cureus.17021
2. Park SG, Koo HR, Jang K, et al. Efficacy of ultrasound-guided needle biopsy in the diagnosis of Kikuchi-Fujimoto disease. Laryngoscope. 2021;131(5):E1519–E1523. doi:10.1002/lary.29160
3. Viguer JM, Jimenez-Heffernan JA, Perez P, Lopez-Ferrer P, Gonzalez-Peramato P, Vicandi B. Fine-needle aspiration cytology of Kikuchi’s lymphadenitis: a report of ten cases. Diagn Cytopathol. 2001;25(4):220–224. doi:10.1002/dc.2042
4. Atwater AR, Longley BJ, Aughenbaugh WD. Kikuchi’s disease: case report and systematic review of cutaneous and histopathologic presentations. J Am Acad Dermatol. 2008;59(1):130–136. doi:10.1016/j.jaad.2008.03.012
5. Dorfman RF, Berry GJ. Kikuchi’s histiocytic necrotizing lymphadenitis: an analysis of 108 cases with emphasis on differential diagnosis. Semin Diagn Pathol. 1988;5(4):329–345.
6. Shim EJ, Lee KM, Kim EJ, Kim HG, Jang JH. CT pattern analysis of necrotizing and nonnecrotizing lymph nodes in Kikuchi disease. PLoS One. 2017;12(7):e0181169. doi:10.1371/journal.pone.0181169
7. Iguchi H, Sunami K, Yamane H, et al. Apoptotic cell death in Kikuchi’s disease: a TEM study. Acta Otolaryngol Suppl. 1998;538:250–253.
8. Perry AM, Choi SM. Kikuchi-Fujimoto disease: a review. Arch Pathol Lab Med. 2018;142(11):1341–1346. doi:10.5858/arpa.2018-0219-RA
9. Ohshima K, Shimazaki K, Kume T, Suzumiya J, Kanda M, Kikuchi M. Perforin and Fas pathways of cytotoxic T-cells in histiocytic necrotizing lymphadenitis. Histopathology. 1998;33(5):471–478. doi:10.1046/j.1365-2559.1998.00532.x
10. Hudnall SD, Chen T, Amr S, Young KH, Henry K. Detection of human herpesvirus DNA in Kikuchi-Fujimoto disease and reactive lymphoid hyperplasia. Int J Clin Exp Pathol. 2008;1(4):362–368.
11. Yen A, Fearneyhough P, Raimer SS, Hudnall SD. EBV-associated Kikuchi’s histiocytic necrotizing lymphadenitis with cutaneous manifestations. J Am Acad Dermatol. 1997;36(2 Pt 2):342–346. doi:10.1016/s0190-9622(97)80413-6
12. Chong Y, Lee JY, Kang CS, Lee EJ. Identification of torque teno virus/torque teno-like minivirus in the cervical lymph nodes of Kikuchi-Fujimoto lymphadenitis patients (histiocytic necrotizing lymphadenitis): a possible key to idiopathic disease. Biomed Hub. 2020;5(1):1–5. doi:10.1159/000506501
13. Huh J, Kang GH, Gong G, Kim SS, Ro JY, Kim CW. Kaposi’s sarcoma-associated herpesvirus in Kikuchi’s disease. Hum Pathol. 1998;29(10):1091–1096. doi:10.1016/s0046-8177(98)90419-1
14. Yufu Y, Matsumoto M, Miyamura T, Nishimura J, Nawata H, Ohshima K. Parvovirus B19-associated haemophagocytic syndrome with lymphadenopathy resembling histiocytic necrotizing lymphadenitis (Kikuchi’s disease). Br J Haematol. 1997;96(4):868–871. doi:10.1046/j.1365-2141.1997.d01-2099.x
15. Chiu CF, Chow KC, Lin TY, Tsai MH, Shih CM, Chen LM. Virus infection in patients with histiocytic necrotizing lymphadenitis in Taiwan. Detection of Epstein-Barr virus, type I human T-cell lymphotropic virus, and parvovirus B19. Am J Clin Pathol. 2000;113(6):774–781. doi:10.1309/1A6Y-YCKP-5AVF-QTYR
16. Hutchinson CB, Wang E. Kikuchi-Fujimoto disease. Arch Pathol Lab Med. 2010;134(2):289–293. doi:10.1043/1543-2165-134.2.289
17. Kang HM, Kim JY, Choi EH, Lee HJ, Yun KW, Lee H. Clinical characteristics of severe histiocytic necrotizing lymphadenitis (Kikuchi-Fujimoto disease) in children. J Pediatr. 2016;171:208–212 e201. doi:10.1016/j.jpeds.2015.12.064
18. Seo JH, Shim HS, Park JJ, et al. A clinical study of histiocytic necrotizing lymphadenitis (Kikuchi’s disease) in children. Int J Pediatr Otorhinolaryngol. 2008;72(11):1637–1642. doi:10.1016/j.ijporl.2008.07.019
19. Wang TJ, Yang YH, Lin YT, Chiang BL. Kikuchi-Fujimoto disease in children: clinical features and disease course. J Microbiol Immunol Infect. 2004;37(4):219–224.
20. Jun-Fen F, Chun-Lin W, Li L, Dayan C, Guan-Ping D, Fang H. Kikuchi-Fujimoto disease manifesting as recurrent thrombocytopenia and Mobitz type II atrioventricular block in a 7-year-old girl: a case report and analysis of 138 Chinese childhood Kikuchi-Fujimoto cases with 10 years of follow-up in 97 patients. Acta Paediatr. 2007;96(12):1844–1847. doi:10.1111/j.1651-2227.2007.00523.x
21. Park HS, Sung MJ, Park SE, Lim YT. Kikuchi-Fujimoto disease of 16 children in a single center of Korea. Pediatr Allergy Immunol. 2007;18(2):174–178. doi:10.1111/j.1399-3038.2006.00505.x
22. Han HJ, Lim GY, Yeo DM, Chung NG. Kikuchi’s disease in children: clinical manifestations and imaging features. J Korean Med Sci. 2009;24(6):1105–1109. doi:10.3346/jkms.2009.24.6.1105
23. Yoo IH, Na H, Bae EY, et al. Recurrent lymphadenopathy in children with Kikuchi-Fujimoto disease. Eur J Pediatr. 2014;173(9):1193–1199. doi:10.1007/s00431-014-2306-6
24. Kim HY, Jo HY, Kim SH. Clinical and laboratory characteristics of Kikuchi-Fujimoto disease according to age. Front Pediatr. 2021;9:745506. doi:10.3389/fped.2021.745506
25. Selvanathan SN, Suhumaran S, Sahu VK, Chong CY, Tan NWH, Thoon KC. Kikuchi-Fujimoto disease in children. J Paediatr Child Health. 2020;56(3):389–393. doi:10.1111/jpc.14628
26. Batton E, Alali M, Hageman JR, Parilla M, Yu KOA. Kikuchi-Fujimoto disease in children: an important diagnostic consideration for cervical lymphadenitis. Pediatr Ann. 2019;48(10):e406–e411. doi:10.3928/19382359-20190920-01
27. Kim TY, Ha KS, Kim Y, Lee J, Lee K, Lee J. Characteristics of Kikuchi-Fujimoto disease in children compared with adults. Eur J Pediatr. 2014;173(1):111–116. doi:10.1007/s00431-013-2131-3
28. Jung HJ, Lee IJ, Yoon SH. Risk assessment of recurrence and autoimmune disorders in Kikuchi disease. Risk Manag Healthc Policy. 2020;13:1687–1693. doi:10.2147/RMHP.S271283
29. Song JY, Lee J, Park DW, et al. Clinical outcome and predictive factors of recurrence among patients with Kikuchi’s disease. Int J Infect Dis. 2009;13(3):322–326. doi:10.1016/j.ijid.2008.06.022
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Recurrence of Histiocytic Necrotizing Lymphadenitis in Children: A 10-year Multicenter Retrospective Study
Xie YP, Xu YW, Li Y, Zhang H, Xu SS, Lu MN, Chen YP, Tian JM, Huang XF, Liu ZF, Gao ZG, Huang LS
Journal of Inflammation Research 2025, 18:4307-4318
Published Date: 24 March 2025