Back to Journals » Therapeutics and Clinical Risk Management » Volume 17
Comparison of Behavioral Risk Factors and Cardiometabolic Comorbidities of Psoriatic Arthritis and Psoriasis: A Case–Control Study in Chinese Patients
Authors Wang Q ![]() , Luo Y, Chen M, Zheng X
, Luo Y, Chen M, Zheng X ![]() , Zhu W
, Zhu W ![]() , Shen M
, Shen M ![]() , Kuang Y
, Kuang Y
Received 23 February 2021
Accepted for publication 14 April 2021
Published 3 May 2021 Volume 2021:17 Pages 397—404
DOI https://doi.org/10.2147/TCRM.S307102
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor De Yun Wang
Qiaolin Wang,1– 3 Yan Luo,1– 3 Menglin Chen,1– 3 Xuanwei Zheng,1– 3 Wu Zhu,1– 3 Minxue Shen,1– 4 Yehong Kuang1– 3
1Department of Dermatology, Xiangya Hospital, Central South University, Changsha, 410008, People’s Republic of China; 2National Clinical Research Center for Geriatric Disorders (Xiangya Hospital), Changsha, 410008, People’s Republic of China; 3Hunan Engineering Research Center of Skin Health and Disease, Hunan Key Laboratory of Skin Cancer and Psoriasis (Xiangya Hospital), Changsha, 410008, People’s Republic of China; 4Department of Social Medicine and Health Management, Xiangya School of Public Health, Central South University, Changsha, 410078, People’s Republic of China
Correspondence: Yehong Kuang; Minxue Shen
Department of Dermatology, Xiangya Hospital, Central South University, 87 Xiangya Road, Changsha, Hunan, People’s Republic of China
Tel +86-13574171102
; +86-15973164022
Email [email protected]; [email protected]
Purpose: Comparison of risk factors and comorbidities could help indicate the underlying mechanisms of diseases. This study aimed to compare behavioral factors and cardiometabolic comorbidities of PsA/psoriasis versus healthy controls to implicate the similarities and differences in potential pathogenic mechanisms for further research.
Patients and Methods: A case-control study in Chinese patients with PsA or psoriasis and healthy controls was conducted. Clinical information based on patient-reported and measured outcomes were collected. Multivariable logistic regression was used to investigate the associations, in terms of adjusted odds ratios (AORs).
Results: We randomly selected 171 patients with PsA, 342 with psoriasis, and 1026 healthy controls from our database, matching by age and sex. Dyslipidemia (AOR=4.62 for PsA and 2.97 for psoriasis) and alcohol drinking (AOR=3.20 for PsA and 3.62 for psoriasis) were significantly associated with both diseases. Overweight was inversely associated with both PsA (AOR=0.46, P=0.002) and psoriasis (AOR=0.56, P=0.001), while obesity was associated with PsA (AOR=2.02, P=0.025) but not psoriasis (AOR=0.87, P=0.621). Subgroup analysis by onset age of psoriatic lesions showed that former smoking was significantly associated with early-onset psoriasis (AOR=2.44, P=0.016) but not PsA (AOR=0.59, P=0.329). Laboratory test indicated that both PsA and psoriasis were associated with altered lipid profile.
Conclusion: PsA and psoriasis in Chinese patients share common behavioral and cardiometabolic risk factors including dyslipidemia and alcohol consumption. There is a U-shape association between BMI and PsA/psoriasis.
Keywords: psoriatic arthritis, psoriasis, comorbidities, obesity, smoking, alcohol
Introduction
Psoriatic disease is a chronic, systemic inflammatory disease that may afflict skin (psoriasis), joints (psoriatic arthritis) and several other organs such as cardiovascular system, respiratory system, and gastrointestinal system, configuring the wide burden of psoriasis-related comorbidities. The prevalence rate varies from 0.5% to 11.4% globally.1–3 Psoriasis vulgaris is the most common type of psoriasis, and up to 30% patients with psoriasis will develop psoriatic arthritis (PsA).4,5 Remarkably, both chronic systemic inflammation and life styles contribute to create and maintain metabolic disturbance, such as metabolic syndrome or dyslipidemia and diabetes. As a result, identification and management of these factors are crucial for improving disease outcomes and health-related quality of life of the patients, especially for PsA. PsA can cause destruction of the joint structure, and is associated with many other diseases. Moreover, a much lower treatment response will be formed if a delay in diagnosis by only 6 months.6 However, previous findings were inconsistent with respect to the factors for PsA and psoriasis owing to differences in study design, sample size, genetic backgrounds, the region of study population, and relevant data from China are rare. Therefore, in the current case-control study, we enrolled patients with psoriasis or PsA and psoriasis-free cohort participants in China, and compared the behavioral factors and cardiometabolic comorbidities of psoriatic arthritis versus psoriasis.
Patients and Methods
Study Design and Participants
This was a case-control study in Chinese patients with PsA or psoriasis and healthy controls. A total of 171 patients with PsA and 342 patients with psoriasis who were initially admitted to the dermatology department of Xiangya Hospital from 1 July 2016 to 24 July 2019 were consecutively enrolled. Each diagnosis was confirmed by two or more experienced dermatologist or rheumatologist. Skin biopsy or dermatoscope was used in partial cases who were difficult to diagnose. Diagnosis of PsA was based on the Criteria of the Classification of Psoriatic Arthritis.7 Patients were excluded if they were referred from another hospital. The healthy controls consisted of 1026 participants from a community-based prospective cohort study. The healthy controls were excluded if they reported a history of psoriasis or arthritis. The ratio of PsA, psoriasis, and healthy controls were 1:2:6, matching for sex and age (± 2.5 years). All participants were informed about the purpose of the study, and a consent form was signed by all participants. The study followed the Declaration of Helsinki and was approved by the institutional research ethics boards of Xiangya Hospital.
Data Collection
Clinical information included age, sex, education level, comorbidities, cigarette smoking, and alcohol drinking were collected through face-to-face interview. Comorbidities were determined by self-reporting on history of disease or medication use, and/or laboratory tests. Laboratory cut-offs for diseases are listed as followings. Dyslipidemia was defined as triglycerides (TG) ≥2.3 mmol/L (normal <1.7 mmol/L), total cholesterol (TC) ≥6.2mmol/L (normal <5.2 mmol/L), low-density lipoprotein cholesterol (LDLc) ≥4.1 mmol/L (normal <3.4 mmol/L), or high-density lipoprotein cholesterol (HDLc) ≤1.0mmol/L (normal range: 1.04 to 1.55 mmol/L) based on the Chinese Guideline for the Management of Dyslipidemia in Adults in 2016.8 Hypertension was defined as blood pressure ≥140/90 mmHg based on the Chinese Guidelines for the Management of Hypertension in 2010.9 Diabetes was defined as fasting blood glucose (FBG) ≥7.0mmol/L based on the 1999 WHO diagnostic criteria (normal range: 3.9 to 6.1 mmol/L). Height and weight were measured in a standard way by a research nurse. Body mass index (BMI) was calculated as weight (kg)/height squared (m2). Overweight and obesity were defined by the BMI cut-offs of 24 and 28 kg/m2, respectively.10 We categorized patients who developed psoriatic lesions prior to 40 years old as early onset, and after 40 years old as late onset. Laboratory data for comparison included FBG, TC, TG, HDLc, and LDLc, and samples with missing values in laboratory test were excluded from the analysis.
Statistical Analysis
Continuous variables with normal distribution were expressed as mean ± standard deviation (SD), and compared with analysis of variance (ANOVA). Continuous data with skewed distribution were presented as median (interquartile range, IQR), and compared with Mann–Whitney rank sum test. Categorical variables were summarized as counts (percentages) and compared using the chi-square test or Fisher’s exact test. The associations of PsA or psoriasis with outcomes were assessed by multivariable logistic regression with adjustments for potential confounders. Odds ratio (OR) and 95% confidence interval were used to present the effect size of the associations. P value less than 0.05 was considered statistically significant. The data were analyzed with SPSS 23 (IBM, SPSS Statistics 23).
Results
Characteristics of the Cases and Healthy Controls
We randomly selected 171 patients with psoriatic arthritis, 342 patients with psoriasis, and 1026 healthy controls from our databases, respectively, matching for sex and age. The mean age of the subjects was 46.5±12.7 years, and 37.4% were women. Characteristics of the patients and healthy controls are shown in Table 1. Educational level, comorbidities, smoking and drinking behaviors, and BMI were significantly different across the groups (P<0.05).
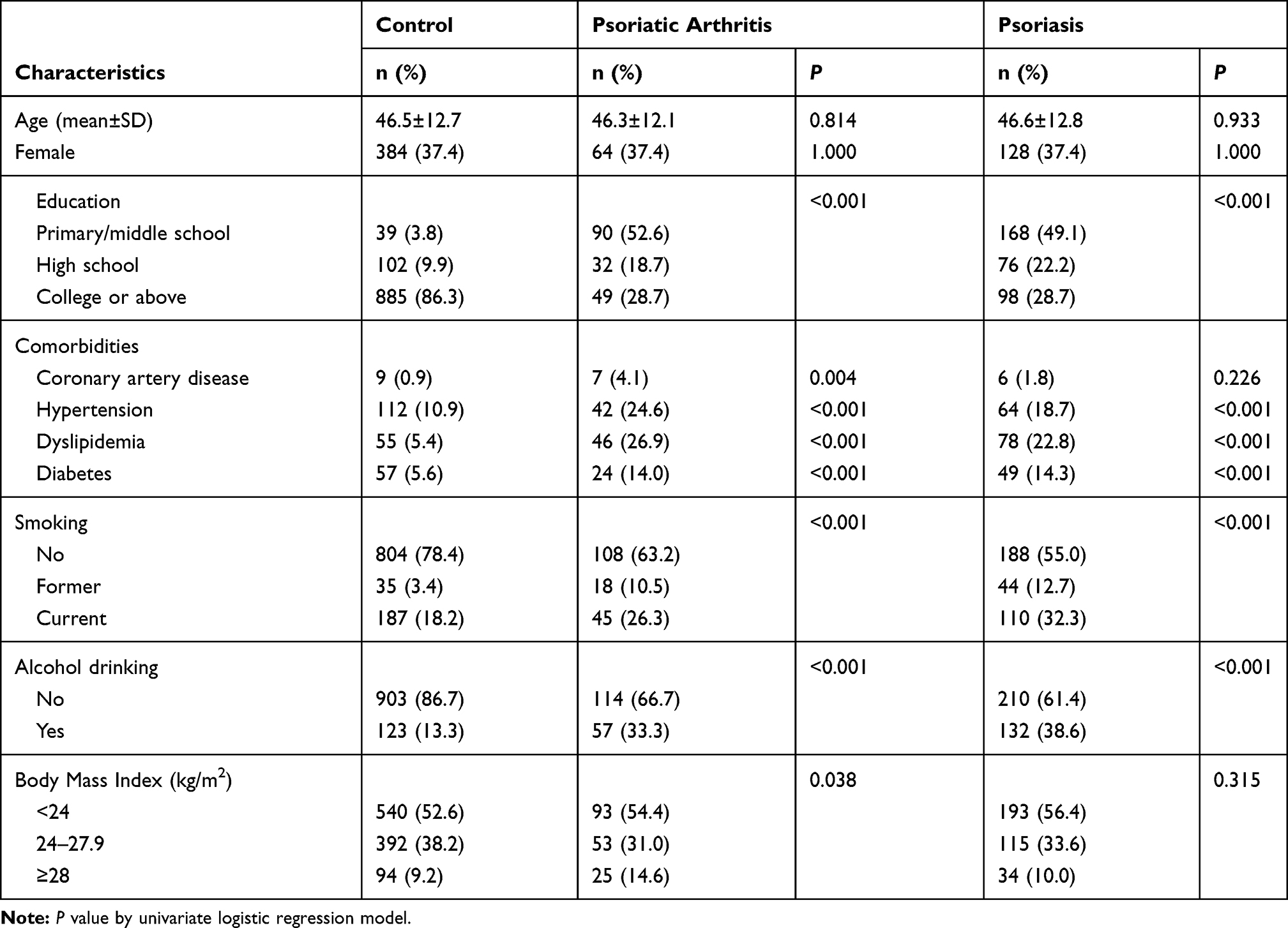 |
Table 1 Characteristics of the Patients with PsA or Psoriasis and Healthy Controls |
Comparison of Cardiometabolic and Behavioral Factors
Table 2 shows the crude ORs and adjusted ORs (AORs) of the potential behavioral risk factors and cardiometabolic comorbidities in association with PsA and psoriasis. The proportion of comorbidities in the case group was higher than that in the healthy control group in general. Compared with the healthy controls, the proportion of dyslipidemia was significantly higher in both diseases with different effect sizes (AOR=4.62 for PsA and 2.97 for psoriasis). Significant difference was not found for cigarette smoking in the cases compared to the healthy controls (P>0.05). Alcohol drinking was significantly associated with both diseases with similar effect sizes (AOR=3.20 for PsA and 3.62 for psoriasis). Overweight was negatively associated with both PsA (AOR=0.46; 95% CI: 0.28–0.74; P=0.002) and psoriasis (AOR=0.56; 95% CI: 0.39–0.79; P=0.001), while obesity was positively associated with PsA (AOR=2.02; 95% CI: 1.09–3.74; P=0.025) but not psoriasis (AOR=0.87; 95% CI: 0.50–1.51; P=0.621).
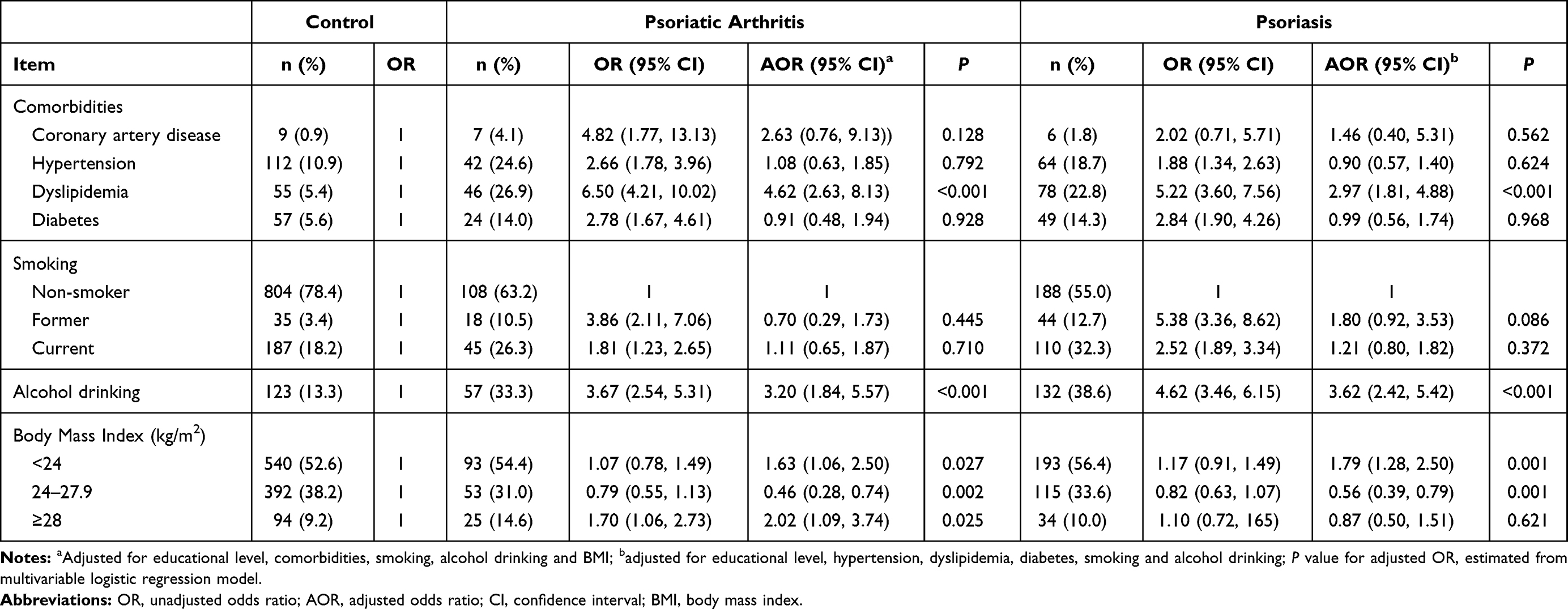 |
Table 2 Comparison of Cardiometabolic and Behavioral Factors of PsA or Psoriasis |
Subgroup Analysis by Disease Onset
Subgroup analysis for the associations of PsA and psoriasis with cardiometabolic and behavioral factors by psoriatic lesions onset is presented in Table 3. Early-onset group of both diseases shared cardiometabolic and behavioral risk factors including dyslipidemia and alcohol drinking. Early-onset psoriasis was negatively associated with hypertension (AOR=0.33, P=0.001) and diabetes (AOR=0.44, P=0.041). Former cigarette smoking was significantly associated with early-onset psoriasis (AOR=2.44; 95% CI: 1.18–5.02; P=0.016) but not early-onset PsA (AOR=0.59; 95% CI: 0.20–1.70; P=0.329). Overweight was negatively associated with early-onset group of both diseases (AOR=0.48 for PsA and 0.59 for psoriasis), while obesity was associated with early-onset PsA (AOR=2.57; 95% CI: 1.34–4.92; P=0.004) but not psoriasis (AOR=0.90; 95% CI: 0.47–1.74; P=0.760).
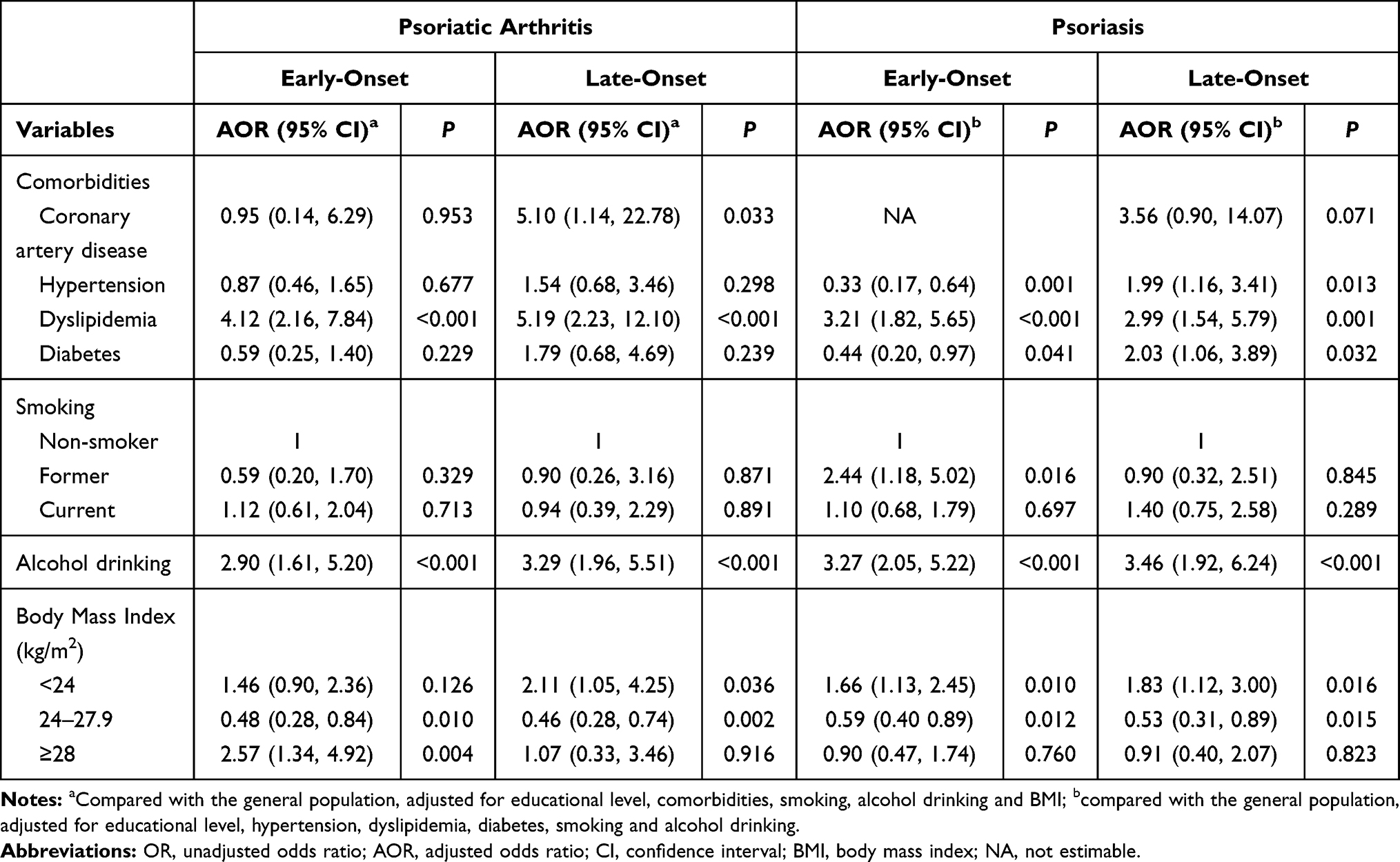 |
Table 3 Subgroup Analysis for the Associations of PsA and Psoriasis with Cardiometabolic and Behavioral Factors by Disease Onset |
Similarly, late-onset group of both diseases shared cardiometabolic and behavioral risk factors including dyslipidemia and alcohol drinking. Late-onset PsA was associated with coronary artery disease (AOR=5.10, P=0.033), while late-onset psoriasis was positively associated with hypertension (AOR=1.99, P=0.013) and diabetes (AOR=2.03, P=0.032). Overweight was negatively associated with late-onset group of both diseases (AOR=0.46 for PsA and 0.53 for psoriasis). Significant differences were not found for cigarette smoking and obesity in late-onset group of both diseases (P>0.05).
Comparison of Fasting Blood Glucose and Lipid Profile
A comparison of fasting blood glucose and lipid profile between cases and healthy controls is presented in Table 4. The level of HDLc was significantly lower in both diseases with different effect sizes (AOR=0.03 for PsA and 0.33 for psoriasis). On the contrary, the level of LDLc was higher in both diseases with similar effect sizes (AOR=2.09 for PsA and 1.97 for psoriasis). There were no significant differences in the level of FBG, TG, and TC across the groups (P>0.05). Subgroup analysis by early or late onset of psoriatic lesions showed consistent results in general.
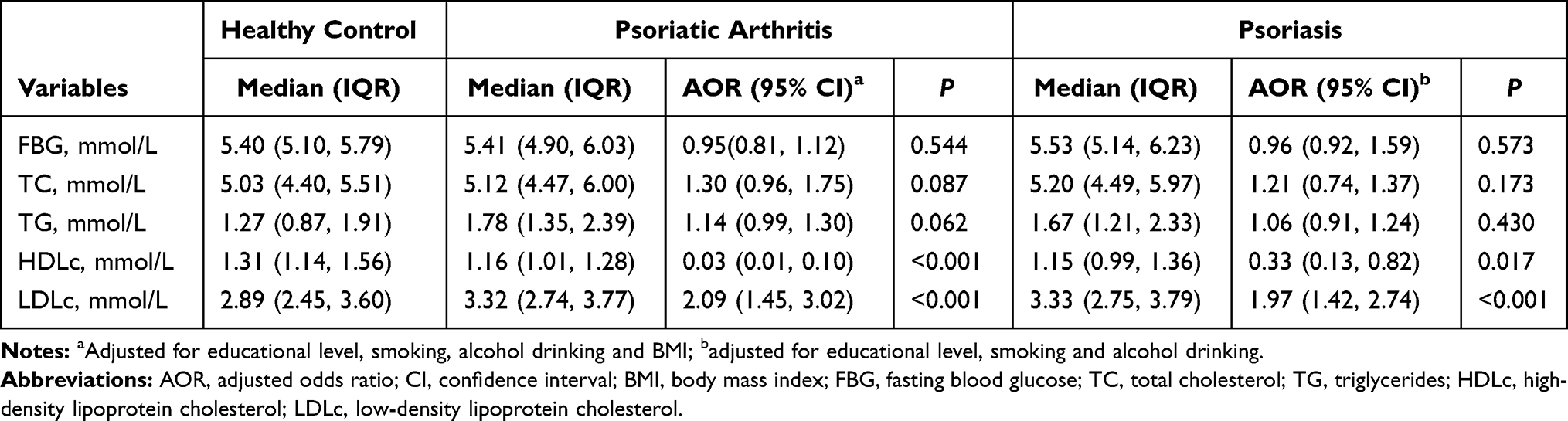 |
Table 4 Comparison of Fasting Blood Glucose and Lipid Profile Between PsA and Psoriasis |
Discussion
By comparing behavioral risk factors and cardiometabolic comorbidities of psoriatic arthritis and psoriasis in Chinese patients, we found that dyslipidemia, and alcohol drinking were common cardiometabolic and behavioral risk factors for PsA and psoriasis. In contrast, former cigarette smoking was associated with early-onset psoriasis not but PsA. Overweight was negatively associated with both diseases, while obesity was positively correlated with PsA. Lower HDLc and higher LDLc were observed in both diseases compared with the healthy controls.
Accumulated evidence demonstrates that PsA and psoriasis are associated with many comorbidities, such as hypertension, dyslipidemia, diabetes.11–13 In our study, dyslipidemia was positively associated with both diseases, and a greater effect size was found in PsA than psoriasis. Diabetes was more common in late-onset psoriasis, which is consistent with a previous study.14 However, an inverse association was found for hypertension and diabetes in early-onset psoriasis. The difference may be explained by the bias of patient-reported measurement. In addition, the underlying pathophysiologic differences between early-and late-onset group of PsA/psoriasis are implied.
Former cigarette smoking was only associated with early-onset psoriasis but not PsA in our study. Many studies showed the positive association between smoking and psoriasis.15–17 But an inverse relationship was previously reported between smoking and the development of PsA in the patients with psoriasis, which has been referred as the “smoking paradox” of PsA.18,19 However, the so-called paradox had been documented that a collider bias may result in the observed association.20 In addition, the differences in the patient subgroups may be another explanation for the controversial results about smoking and its effects on the disease.
The association between alcohol consumption and psoriasis was controversial. Murzaku et al found that excessive alcohol intake was significantly associated with psoriasis severity and poor treatment efficacy.21 However, a study from a Taiwanese population-based cohort study revealed that alcohol is not associated with the risk of psoriasis,15 while a cohort study of US women indicated that those who took excessive alcohol had an increased risk of PsA.22 Our study conclusion supports that alcohol consumption was positively associated with PsA/psoriasis, and a stronger association was found between alcohol consumption and psoriasis than PsA. The association between alcohol and psoriatic diseases is difficult to assess owing to the recall bias and measurement error of the volume and type of alcohol drinks.
Patients with PsA had a significantly higher proportion of obesity in our study, but a lower proportion of overweight was observed in PsA/psoriasis. A U-shaped association between BMI and PsA/psoriasis was suggested in our study, which revealed differential effects of adiposity on PsA/psoriasis. Many studies have indicated that obesity was associated with PsA and psoriasis.17,23–26 Previous studies manifested gut microbiota were related to PsA/psoriasis,27–29 and the diversity of the gut microbiota was different in different body sizes.30,31 As is well known, psoriasis is intertwined with metabolic disorders. Therefore, besides the gut microbiota, metabolic factors also probably play roles in the association between BMI and PsA/psoriasis. In addition, BMI is usually used to assess the degree of body fat; however, BMI might not reflect body fat distribution well.23 A study from Korea found that man with normal BMI and high waist circumference (WC) had the highest risk of psoriasis.32 Relevant mechanism needs further investigation.
The laboratory examination results from our data indicated higher levels of LDLc and lower levels of HDLc in the cases than the healthy controls, and PsA had a stronger effect on the serum lipid levels than psoriasis; this is consistent with the findings in other studies.12,33 Analysis of the laboratory data is consistent with the finding that dyslipidemia was a risk factors for PsA and psoriasis.
The limitations of the study included the impossibility to account for previously considered factors that in the present are not collected, a lack of generalizability to non-Chinese patients, a lack of psoriasis severity information which should be adjusted, and interfered laboratory examination results due to the treatment for PsA/psoriasis or the comorbidities.
Conclusion
PsA and psoriasis in Chinese patients share common behavioral and cardiometabolic risk factors including dyslipidemia and alcohol consumption. The U-shape association between BMI and PsA/psoriasis needs further validation and research for its mechanism.
Ethics Approval
This study was approved by the institutional research ethics boards of Xiangya Hospital, Central South University (Changsha, China).
Acknowledgment
The authors would like to thank Dr. Tingyin Chen (Xiangya Hospital, Central South University) for his contribution to the data collection.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the key project of the National Science Foundation (81430075, 81830096), National Natural Science Foundation of China (81573049, 81974479, 81773329), Key R & D Program of Hunan Province (2018SK2082), National key R & D program (2016YFC0900802, 2018YFC0117004, 2016YFC0901705).
Disclosure
The authors have no conflicts of interest to declare.
References
1. Zeng C, Wen B, Hou G, et al. Lipidomics profiling reveals the role of glycerophospholipid metabolism in psoriasis. Gigascience. 2017;6(10):1–11. doi:10.1093/gigascience/gix087
2. Tan L, Zhao S, Zhu W, et al. The Akkermansia muciniphila is a gut microbiota signature in psoriasis. Exp Dermatol. 2018;27(2):144–149. doi:10.1111/exd.13463
3. Michalek IM, Loring B, John SM. A systematic review of worldwide epidemiology of psoriasis. J Eur Acad Dermatol Venereol. 2017;31(2):205–212. doi:10.1111/jdv.13854
4. Langley RG, Krueger GG, Griffiths CE. Psoriasis: epidemiology, clinical features, and quality of life. Ann Rheum Dis. 2005;64(Suppl 2):ii18–ii23. doi:10.1136/ard.2004.033217
5. Ritchlin CT, Colbert RA, Gladman DD. Psoriatic arthritis. N Engl J Med. 2017;376(10):957–970. doi:10.1056/NEJMra1505557
6. Haroon M, Gallagher P, FitzGerald O. Diagnostic delay of more than 6 months contributes to poor radiographic and functional outcome in psoriatic arthritis. Ann Rheum Dis. 2015;74(6):1045–1050. doi:10.1136/annrheumdis-2013-204858
7. Taylor W, Gladman D, Helliwell P, et al. Classification criteria for psoriatic arthritis: development of new criteria from a large international study. Arthritis Rheum. 2006;54(8):2665–2673. doi:10.1002/art.21972
8. Jun-Ren ZH, Run-Lin GA, Shui-Ping ZH, et al. 2016 Chinese guidelines for the management of dyslipidemia in adults. J Geriatr Cardiol. 2018;15(1):1–29.
9. Liu LS. [2010 Chinese guidelines for the management of hypertension]. Zhonghua Xin Xue Guan Bing Za Zhi. 2011;39(7):579–615. Chinese.
10. Chen CM. Overview of obesity in Mainland China. Obes Rev. 2008;9(Suppl 1):14–21. doi:10.1111/j.1467-789X.2007.00433.x
11. Tam LS, Tomlinson B, Chu TT, et al. Cardiovascular risk profile of patients with psoriatic arthritis compared to controls–the role of inflammation. Rheumatology. 2008;47(5):718–723. doi:10.1093/rheumatology/ken090
12. Snekvik I, Nilsen TIL, Romundstad PR, Saunes M. Psoriasis and cardiovascular disease risk factors: the HUNT Study, Norway. J Eur Acad Dermatol Venereol. 2018;32(5):776–782. doi:10.1111/jdv.14835
13. Gelfand JM, Wan MT. Psoriasis: a novel risk factor for type 2 diabetes. Lancet Diabetes Endocrinol. 2018;6(12):919–921. doi:10.1016/S2213-8587(18)30127-X
14. Theodorakopoulou E, Yiu ZZ, Bundy C, et al. Early- and late-onset psoriasis: a cross-sectional clinical and immunocytochemical investigation. Br J Dermatol. 2016;175(5):1038–1044. doi:10.1111/bjd.14886
15. Dai YX, Wang SC, Chou YJ, et al. Smoking, but not alcohol, is associated with risk of psoriasis in a Taiwanese population-based cohort study. J Am Acad Dermatol. 2019;80(3):727–734. doi:10.1016/j.jaad.2018.11.015
16. Lee EJ, Han KD, Han JH, Lee JH. Smoking and risk of psoriasis: a nationwide cohort study. J Am Acad Dermatol. 2017;77(3):573–575. doi:10.1016/j.jaad.2017.04.015
17. Green A, Shaddick G, Charlton R, et al. Modifiable risk factors and the development of psoriatic arthritis in people with psoriasis. Br J Dermatol. 2020;182(3):714–720. doi:10.1111/bjd.18227
18. Pattison E, Harrison BJ, Griffiths CE, Silman AJ, Bruce IN. Environmental risk factors for the development of psoriatic arthritis: results from a case-control study. Ann Rheum Dis. 2008;67(5):672–676. doi:10.1136/ard.2007.073932
19. Eder L, Shanmugarajah S, Thavaneswaran A, et al. The association between smoking and the development of psoriatic arthritis among psoriasis patients. Ann Rheum Dis. 2012;71(2):219–224. doi:10.1136/ard.2010.147793
20. Nguyen US, Zhang Y, Choi HK. Response to: ‘Smoking paradox in the development of psoriatic arthritis among patients with psoriasis’ by Lee and Song. Ann Rheum Dis. 2018;77(11):e76. doi:10.1136/annrheumdis-2017-212770
21. Murzaku EC, Bronsnick T, Rao BK. Diet in dermatology: Part II. Melanoma, chronic urticaria, and psoriasis. J Am Acad Dermatol. 2014;71(6):1053–e1. doi:10.1016/j.jaad.2014.06.016
22. Wu S, Cho E, Li WQ, Han J, Qureshi AA. Alcohol intake and risk of incident psoriatic arthritis in women. J Rheumatol. 2015;42(5):835–840. doi:10.3899/jrheum.140808
23. Snekvik I, Smith CH, Nilsen TIL, et al. Obesity, waist circumference, weight change, and risk of incident psoriasis: prospective data from the HUNT study. J Invest Dermatol. 2017;137(12):2484–2490. doi:10.1016/j.jid.2017.07.822
24. Aune D, Snekvik I, Schlesinger S, Norat T, Riboli E, Vatten LJ. Body mass index, abdominal fatness, weight gain and the risk of psoriasis: a systematic review and dose-response meta-analysis of prospective studies. Eur J Epidemiol. 2018;33(12):1163–1178. doi:10.1007/s10654-018-0366-z
25. Greb JE, Goldminz AM, Elder JT, et al. Psoriasis. Nat Rev Dis Primers. 2016;2:16082. doi:10.1038/nrdp.2016.82
26. Zhang C, Zhu KJ, Zheng HF, et al. The effect of overweight and obesity on psoriasis patients in Chinese Han population: a hospital-based study. J Eur Acad Dermatol Venereol. 2011;25(1):87–91. doi:10.1111/j.1468-3083.2010.03706.x
27. Hidalgo-Cantabrana C, Gomez J, Delgado S, et al. Gut microbiota dysbiosis in a cohort of patients with psoriasis. Br J Dermatol. 2019;181(6):1287–1295. doi:10.1111/bjd.17931
28. Scher JU, Ubeda C, Artacho A, et al. Decreased bacterial diversity characterizes the altered gut microbiota in patients with psoriatic arthritis, resembling dysbiosis in inflammatory bowel disease. Arthritis Rheumatol. 2015;67(1):128–139. doi:10.1002/art.38892
29. Codoner FM, Ramirez-Bosca A, Climent E, et al. Gut microbial composition in patients with psoriasis. Sci Rep. 2018;8(1):3812. doi:10.1038/s41598-018-22125-y
30. Cotillard A, Kennedy SP, Kong LC, et al. Dietary intervention impact on gut microbial gene richness. Nature. 2013;500(7464):585–588. doi:10.1038/nature12480
31. Turnbaugh PJ, Hamady M, Yatsunenko T, et al. A core gut microbiome in obese and lean twins. Nature. 2009;457(7228):480–484. doi:10.1038/nature07540
32. Han JH, Lee JH, Han KD, et al. Increased risk of psoriasis in subjects with abdominal obesity: a nationwide population-based study. J Dermatol. 2019;46(8):695–701. doi:10.1111/1346-8138.14939
33. Pietrzak A, Michalak-Stoma A, Chodorowska G, Szepietowski JC. Lipid disturbances in psoriasis: an update. Mediators Inflamm. 2010;2010. doi:10.1155/2010/535612
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.