Back to Journals » Clinical Epidemiology » Volume 12
Comparison Between PPOS and GnRHa-Long Protocol in Clinical Outcome with the First IVF/ICSI Cycle: A Randomized Clinical Trial
Authors Xi Q, Tao Y ![]() , Qiu M, Wang Y, Kuang Y
, Qiu M, Wang Y, Kuang Y
Received 7 August 2019
Accepted for publication 6 February 2020
Published 3 March 2020 Volume 2020:12 Pages 261—272
DOI https://doi.org/10.2147/CLEP.S226414
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Eyal Cohen
Qianwen Xi, Yu Tao, Meiting Qiu, Yun Wang, Yanping Kuang
Department of Assisted Reproduction, Shanghai Ninth People’s Hospital Affiliated to JiaoTong University School of Medicine, Shanghai, People’s Republic of China
Correspondence: Yun Wang; Yanping Kuang
Yanping Kuang Department of Assisted Reproduction, Shanghai Ninth People’s Hospital Affiliated to JiaoTong University School of Medicine, Shanghai, People’s Republic of China
Email [email protected]; [email protected]
Purpose: To investigate whether progestin-primed ovarian stimulation (PPOS) can be an alternative as gonadotrophin-releasing hormone agonist (GnRHa) long protocol for infertile women with normal ovarian reserve during IVF/ICSI.
Methods: A prospective randomized controlled trial (RCT) including 257 patients was conducted between 1 August 2017 to 1 January 2018. Computerized randomization was performed to assign participants into two treatment groups at a 1:1 ratio: PPOS (130 patients) or GnRHa long protocol (127 patients) followed by their first IVF/ICSI with fresh/frozen embryo transfer. The primary outcome was the number of oocytes retrieved. Patients with normal ovarian reserve undergoing their first IVF/ICSI procedure were included. The embryological and clinical outcomes were measured. Only the first embryo transfer cycle was followed-up.
Results: Basic characteristics such as infertility duration, age, and body mass index (BMI) were comparable in both groups. No significant difference was found in the number (mean ± SD) oocytes retrieved [11.8 ± 6.5 for PPOS vs 11.3 ± 5.6 for GnRHa long protocol] or viable embryos [4.5 ± 3.0 for PPOS vs 4.2 ± 2.9 for GnRHa long protocol] between the groups. No patient from either group experienced a premature LH surge during the whole process of ovarian stimulation. Besides, there was no moderate or severe ovarian hyperstimulation syndrome during the ovarian stimulation in PPOS group while three patients suffered it in the GnRHa long protocol group. There was no significant difference in the clinical pregnancy rate of the first embryos transfer cycle between the two groups.
Conclusion: PPOS in combination with embryo cryopreservation as an ovarian stimulation regimen was as effective as GnRHa long protocol during controlled ovarian stimulation (COH) under different endocrinal mechanisms. It can also achieve comparable embryological and clinical outcomes while reducing the incidence of moderate and severe ovarian hyperstimulation syndrome (OHSS) and HMG dosage. It can be an alternative of the treatments for infertile patients with normal ovarian reserve undergoing IVF as well as traditional protocols.
Trial Registration Number: ChiCTR-INR-17012089.
Trial Registration Date: Chictr.org.cn: 23 July 2017.
Date of First Patient’s Enrollment: 1 August 2017.
Keywords: medroxyprogesterone acetate, progestin-primed ovarian stimulation, premature LH surge, ovarian stimulation, ovarian hyperstimulation syndrome
Introduction
The Gonadotrophin-releasing hormone agonist (GnRHa) long protocol presents the best clinical pregnancy rates per cycle initiated among the various types of GnRHa ovarian stimulation protocols in the IVF cycle.1 The major benefits of it include synchronisation of follicular development, the recovery of a larger number of oocytes and improvement of the endometrial thickness.2,3 The long protocol can be divided into two types based on GnRHa administration that can be used to lead to hypophysis desensitization: one consisting of daily GnRHa low doses, and another with the administration of analogues in higher long-acting doses (depot).4 A typical regimen using a depot of long-acting GnRHa, which we called the GnRHa-long protocol, was thought to be more comfortable for patients as it makes fewer applications,5 and more flexible to start the controlled ovarian stimulation (COH). It still exists some weakness of the long protocol of higher fees, more complicated procedure and a higher risk of ovarian hyperstimulation syndrome (OHSS) after hCG trigger.6
Since there is still an unmet need for ovarian stimulation protocols with improved efficacy, safety profile, and user convenience, new protocols like GnRH antagonist protocols and mild stimulation protocols were proposed in the last decade. Progestin-primed ovarian stimulation (PPOS), which uses progestin combined with gonadotrophin, and ovulation co-triggered by a low dose of hCG and a GnRH agonist,6,7 is also one of these new ovarian stimulation protocols. This new regimen combined with freeze-all strategy has been proved to get comparable oocytes and embryos without a premature LH surge compared to the short protocol.6 However, PPOS still needs more randomized controlled trials (RCT) to confirm the effect of it.
Being the first study comparing PPOS and GnRHa long protocol, we conduct this RCT to analyze cycle characteristics and endocrinological profiles for patients undergoing their first COH cycle and investigate the subsequent pregnancy outcomes of their first embryo transfer cycles to explore whether the new ovarian stimulation regimen can be an alternative as traditional ones for infertile women with normal ovarian reserve during IVF/ICSI.
Materials and Methods
We carried out a randomized controlled trial at the Department of Assisted Reproduction of the Ninth People’s Hospital, Shanghai JiaoTong University School of Medicine from 1 August 2017 to 1 January 2018. The trial was registered with the Chinese Clinical Trial Registry (ChiCTR-INR-17012089). It was conducted according to the Declaration of Helsinki for medical research. The study was approved by the Ethics Committee (Institutional Review Board) of the Ninth People’ Hospital of Shanghai and informed consent was obtained from all patients. All data were open to the public and can be found in figshare (https://figshare.com/) using the clinical trial registration number. The specific figshare link is https://figshare.com/search?q=ChiCTR-INR-17012089&searchMode=1.
Patient Selection
All patients undergoing their first IVF/ICSI cycles were invited to participate in the trial during this period. Besides, who had any IVF/ICSI cycles in other hospitals were also excluded. The basic characteristics of the patients were investigated to determine whether they were qualified to be enrolled in the study before ovarian stimulation. Women who meet the following criteria are included:1 age no older than 42,2 more than 5 antral follicles on the day 2–3 of menstruation,3 basal serum follicle-stimulating hormone (FSH) concentration of lower than 10 IU/L,4 never had any IVF/ICSI cycles before. At the same time, patients were excluded in this trial if they had an ovarian cyst under transvaginal ultrasound with E2>100 pg/mL, were already taking part in another clinical trial, or any contraindications to ovarian stimulation treatment, diagnosis of polycystic ovarian syndrome, endometriosis grade 3 or higher.
Sample Size and Randomization
This is a prospective noninferiority trial. Based on the previous study, the number of oocytes retrieved was about 9.6 and the standard deviation was 4.2 in the GnRHa long protocol.3 It was determined that 93 patients would be required in each group to discover a significant difference between the two regimens with a two-sided significance level of 0.05 and 90% power. Given the possibility of dropouts, we designed the study to include a total of 103 women in each group (206 in total) at least. Eligible volunteers were randomized using a computer-generated random number to either treatment group; treatment allocation was generated and then given to researchers in a sealed envelope by an administration. Each patient was enrolled by a physician. After signing the written informed consent form, they were allocated to a specific treatment arm by opening the sealed envelope.
Ovarian Stimulation and Embryo Culture
PPOS
Patients in the study group were given hMG (Anhui Fengyuan Pharmaceutical Co, China) at a dose of 150 to 225 IU/day and MPA (Beijing Zhong Xin Pharmaceutical, China) 4mg/day from day 3 of menstruation, after ultrasound screen and blood test confirmed the presence of a baseline hormone profile. The 150 IU daily hMG dose was used for patients with high antral follicle count (AFC)>20 or slightly elevated basal follicle-stimulating hormone (FSH) (7–10 IU/L), for all other patients, a daily dose of 225 IU hMG was used. Follicular monitoring started on menstruation cycle day (MC) 7 to 8 and was carried out every 2 to 3 days by transvaginal ultrasound examination to record the number of developing follicles. On the same days, serum FSH, LH, E2, and P values were measured using blood tests. hMG dosage would be adjusted according to oestradiol concentrations and ovarian response. Our previous work showed that co-triggering by a low dose of hCG and GnRH-a 0.1 mg had a more favorable effect on oocyte maturation than triggering by GnRH-a alone in the MPA co-treatment with gonadotropin in the general infertile women. So when 3 dominant follicles reached 18 mm in diameter, the final stage of oocyte maturation was co-triggered by Decapeptyl (0.1 mg) (Ferring International Center SA, Germany) and hCG 1000IU (Lizhu Pharmaceutical Trading Co, China). Transvaginal ultrasound–guided oocyte retrieval was conducted 34–36 hrs after the trigger. All follicles with diameters of more than 10 mm were retrieved.8
The process of oocytes fertilization was carried out in vitro, by conventional insemination or intracytoplasmic sperm injection, depending on semen quality.9 On the third day, the degree of embryonic fragmentation, the regularity and number of blastomeres of the embryos were examined according to Cummins et al’s criteria.10 All the grade 1 and grade 2 8-cell embryos, which we defined as good-quality embryos were frozen by vitrification. The other embryos (non-top-quality embryos) were extended cultured until the blastocyst stage. On day 5 or day 6, blastocysts with good-morphology were frozen. The Cryotop carrier system (Kitazato Biopharma Co.) was used for the vitrification of cleavage-stage embryos and blastocysts. The cryoprotectant solution is mixed with 0.5 M sucrose, 15% (v/v) dimethyl sulfoxide, and 15% (v/v) ethylene glycol. Solutions of 0, 0.5, and 1 M sucrose were sequentially used as cryoprotectant dilutions for thawing. During the procedure of vitrification and warming, all steps were performed at room temperature except that the first warming step should be conducted at 37°C.6
GnRHa-Long Protocol
In the GnRHa-long protocol, pituitary down-regulation was obtained with a standard full dose (3.75 mg) of Leuprorelin Acetate Microspheres (Lizhu Pharmaceutical Trading Co, China) in the early follicular phase. Patients came back to check whether they had met the criteria for adequate suppression. The criteria for defining adequate pituitary–ovarian suppression were: E2 < 40 pg/mL, P < 1 ng/mL, LH < 3 IU/L, a dense endometrium < 4 mm, and the absence of any growing follicle > 6 mm. The COH was postponed by 1 week if E2 was > 40 pg/mL and/or in case of the presence of an ovarian anechoic image > 6 mm. Controlled ovarian hyperstimulation (COH) was performed by using hMG (Anhui Fengyuan Pharmaceutical Co, China) at a dose of 150–225 IU/day as it was the first stimulation cycle of all the patients. Follicular monitoring started 7 or 8 days later and was performed every 2 to 3 days using a transvaginal ultrasound examination to record the number of developing follicles. Serum FSH, LH, E2, and P concentrations were measured using patient blood tests on the same days as the ultrasound exams. When 3 dominant follicles reached 18 mm in diameter, the final stage of oocyte maturation was triggered by hCG 5000IU (Lizhu Pharmaceutical Trading Co, China). Transvaginal ultrasound-guided oocyte retrieval was conducted 34–36 hrs after the trigger. All follicles with diameters of more than 10 mm were retrieved. Oocytes are fertilized conventionally or by intracytoplasmic sperm injection. Embryos were graded in the same way on the third day. One or 2 good-quality embryos was/were transferred and the procedure for freezing and thawing embryos was carried out as previously described. Luteal phase support was sustained with oral Duphaston (Abbott Biologicals B.V., America) 40 mg/day and soft vaginal P capsules (Laboratoires Besins International) 200 mg two times per day from the day of oocyte retrieval.
In patients who were not prepared adequately for fresh embryo transfer (ET) due to high risk of OHSS, elevated P on trigger day, unqualified endometrium, or some other personal reasons, all highest quality embryos were frozen by verification. Frozen-thawed embryo transfer (FET) was performed for these patients later. In brief, natural FET cycles were used for women with regular menstrual cycles and letrozole was added for the cases with irregular menstrual cycles. Endometrial preparation and FET were performed in either a natural cycle or a stimulation cycle as described elsewhere.11 Hormone treatment was recommended for patients with thin endometria as endometrial preparation. From cycle day 3, red Fematon tablets (including 2 mg micronized estradiol per tablet; Abbott Healthcare Products B.V.) was administrated orally 2 tablets two times per day. Fourteen days afterwards, when the endometrial lining was thicker than 8 mm under transvaginal ultrasound, soft vaginal P capsules (Laboratoires Besins International) were administered 200 mg two times per day and yellow Fematon tablets (Abbott Healthcare Products B.V.) including 2 mg micronized estradiol and 10 mg dydrogesterone per tablet were also administered orally 2 tablets two times per day. The transfer of Day 3 embryos was performed 3 days later oocyte retrieved. Blastocysts transfer was arranged to be carried out on the fifth day. Exogenous estrogen and progesterone supplement lasted until 10 weeks of gestation if pregnancy was achieved.
Hormone Measurement
Serum concentration of sex hormone (FSH, LH, E2, and P) were measured on MC3 (the start day of the stimulation cycle), MC 7–8 (after 4–5 days of stimulation), MC 9–11 (after 6–8 days of stimulation), trigger day (injection of GnRHa and/or hCG), and the day after trigger day (approximately 10 hrs after trigger). Chemiluminescence (Abbott Biologicals B.V.) was used to measure the hormone values. The lower limits of the hormone measurement were as follows: LH=0.09 IU/L, FSH=0.06 IU/L, P=0.1 ng/mL, and E2=10 pg/mL. The E2 level was recorded as 5000 pg/mL if it was higher than that.
Outcome Measures
The primary outcome measurement for this study was the number of oocytes retrieved. The secondary measures included the duration and dosage of hMG, hormone measurements, fertilization rate, number of viable embryos (eight-cell embryos, grade 1 and grade 2 embryos on day3 after oocyte retrieval and day 5 or 6 blastocysts with good morphology derived from the non-standard embryos on the third day) per oocyte retrieved, cycle cancellation rate, incidence of moderate and severe OHSS, and pregnancy outcomes of the first FET cycle.
No viable embryos after COH was defined as a cycle cancellation. Implantation rate was the ratio of the number of gestational sacs to the number of embryos transferred. The definition of clinical pregnancy is the existence of a gestational sac whether there is a fetal heart activity or not under transvaginal 4 weeks after embryo transfer. The spontaneous abortion rate was defined as the number of patients with spontaneous loss before 12 weeks gestation divided by those with a clinical pregnancy. Cumulative pregnancy was defined as the total number of pregnancy using multiple embryo transfers.
Statistical Analysis
All data were processed by SPSS 22.0 (IBM SPSS Statistics, IBM Corporation, USA). All patients being randomized were involved in the intent-to-treat analysis. Normal distribution of quantity variables was tested by Shapiro–Wilk test of normality. Values are reported as mean (standard deviation (SD)) for distributed variables. Continuous variables were compared via Student’s t-tests if the normality assumption was true; otherwise, the Kruskal–Wallis test was applied. Proportions were compared using the Fisher’s exact test or the chi-square test when appropriate. A P-value of 0.05 was considered statistically significant.
Results
In total, 260 patients were enrolled in this trial. One hundred and thirty of them were allocated to the PPOS group and 130 to the GnRHa-long group. A Consolidated Standards of Reporting Trials (CONSORT) flow diagram is shown in Figure 1. At the end of the study, a total of 257 women completed oocyte retrieval cycles, and 237 women completed ET/FET cycles. The basic characteristics of the patients in the study are presented in Table 1. Patient age, body mass index and infertility duration were similar between the two groups (P>0.05). There were no differences in the insemination method of patients in two groups. Table 2 describes the clinical and cycle characteristics of COH treatment in both groups. No statistically significant difference was found in the AFC on the first day of gonadotropin stimulation and the number of follicles over 14 mm in diameter in the two groups. The stimulation duration (9.1±1.3 versus 11.9±2.3 IU, P=0.00) and hMG dose (2027.9±333.9 versus 2672.8±599.5IU, P=0.00) in the study group were significantly lower than those in the control group. No patients suffered a premature LH surge in either group. No one experienced moderate or severe OHSS in the study group, while three patients did in the GnRHa long protocol group (P=0.24). The number of oocytes retrieved in the PPOS group had an increasing trend compared to GnRHa long group (11.8±6.5 versus 11.3±5.6; P=0.81), but there was no significant difference. No significant differences were found in the number of fertilized embryos, top-quality embryos and viable embryos between the two groups (P>0.05). The oocyte retrieval rate, mature oocyte rate, fertilization rate, and cleavage rate were also comparable between the patient cohorts. Eight women had poor-quality embryos or no fertilized oocytes in either group (Table 3). Figure 2 and Table 4 present the serum concentrations of FSH, LH, E2, and P in both groups. The endocrine characteristics on the first day of gonadotropin stimulation were significantly higher in the PPOS group as pituitary down-regulation was obtained in the GnRHa-long protocol. FSH concentration increased significantly after administrating hMG and kept steady until the trigger day in the two groups. On the day after the trigger, FSH increased in the PPOS group but decreased in the GnRHa-long group.
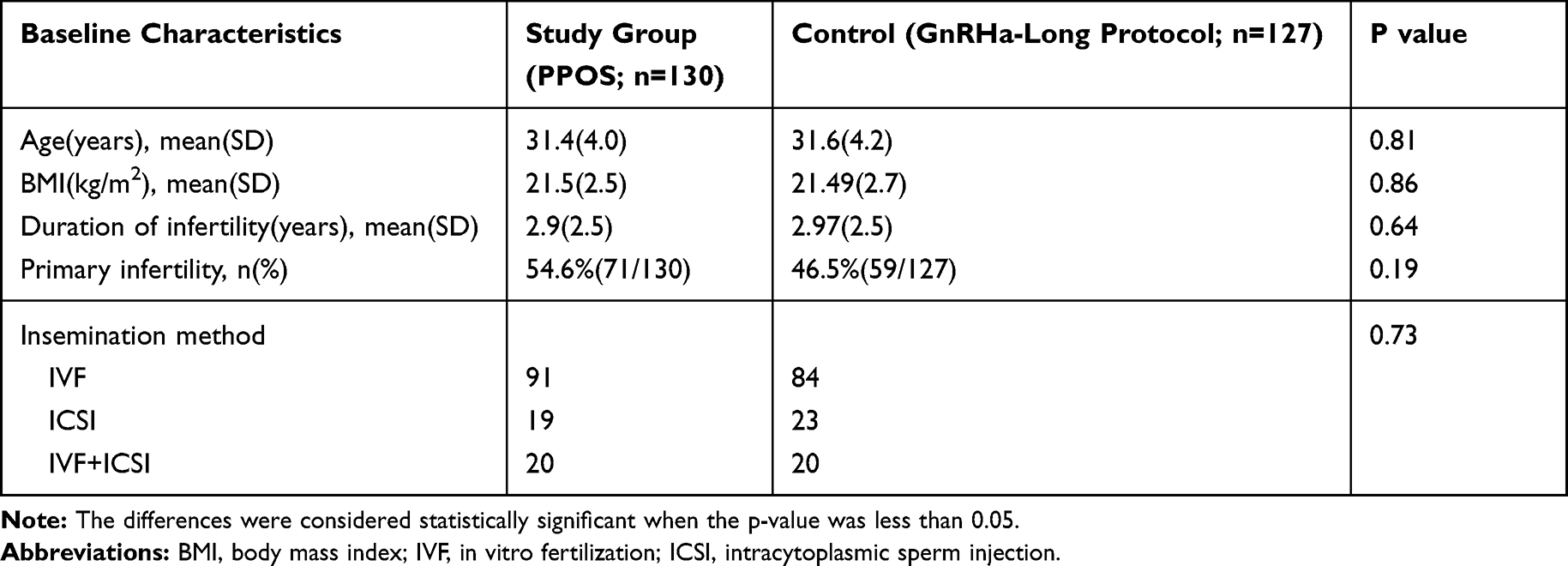 |
Table 1 The Basic Characteristics of Women Undergoing IVF/ICSI Treatment in the Two Ovarian Stimulation Groups |
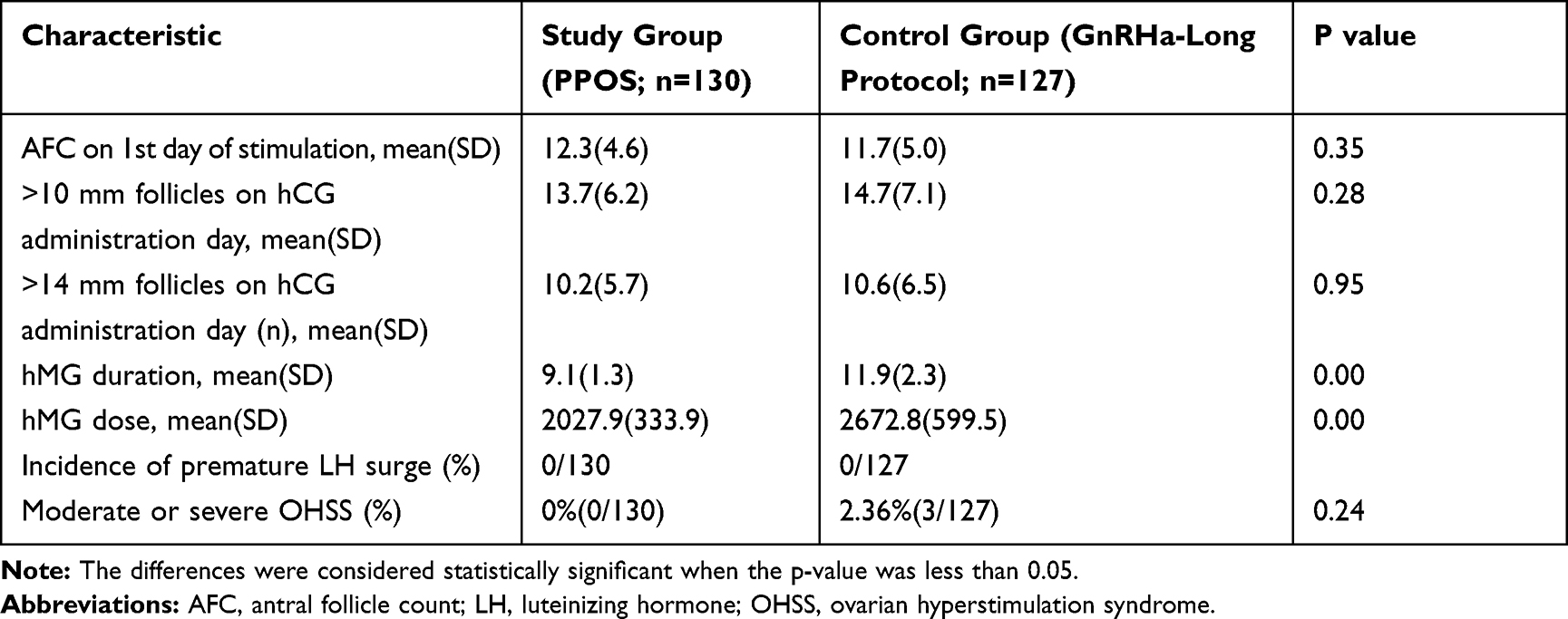 |
Table 2 The Cycle Characteristics of Controlled Ovarian Stimulation in Two Regimens |
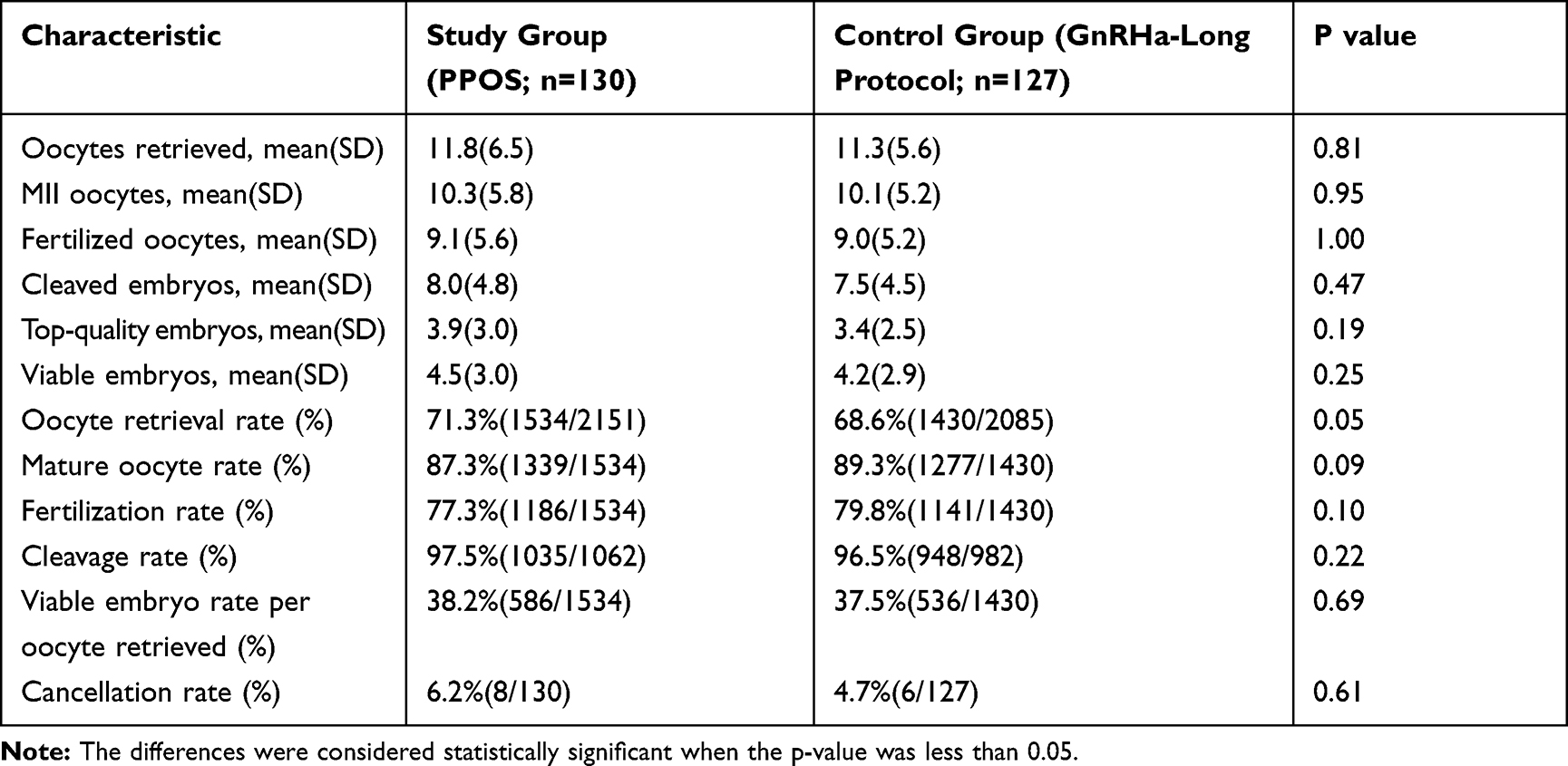 |
Table 3 The Embryological Outcomes of Controlled Ovarian Stimulation in Two Regimens |
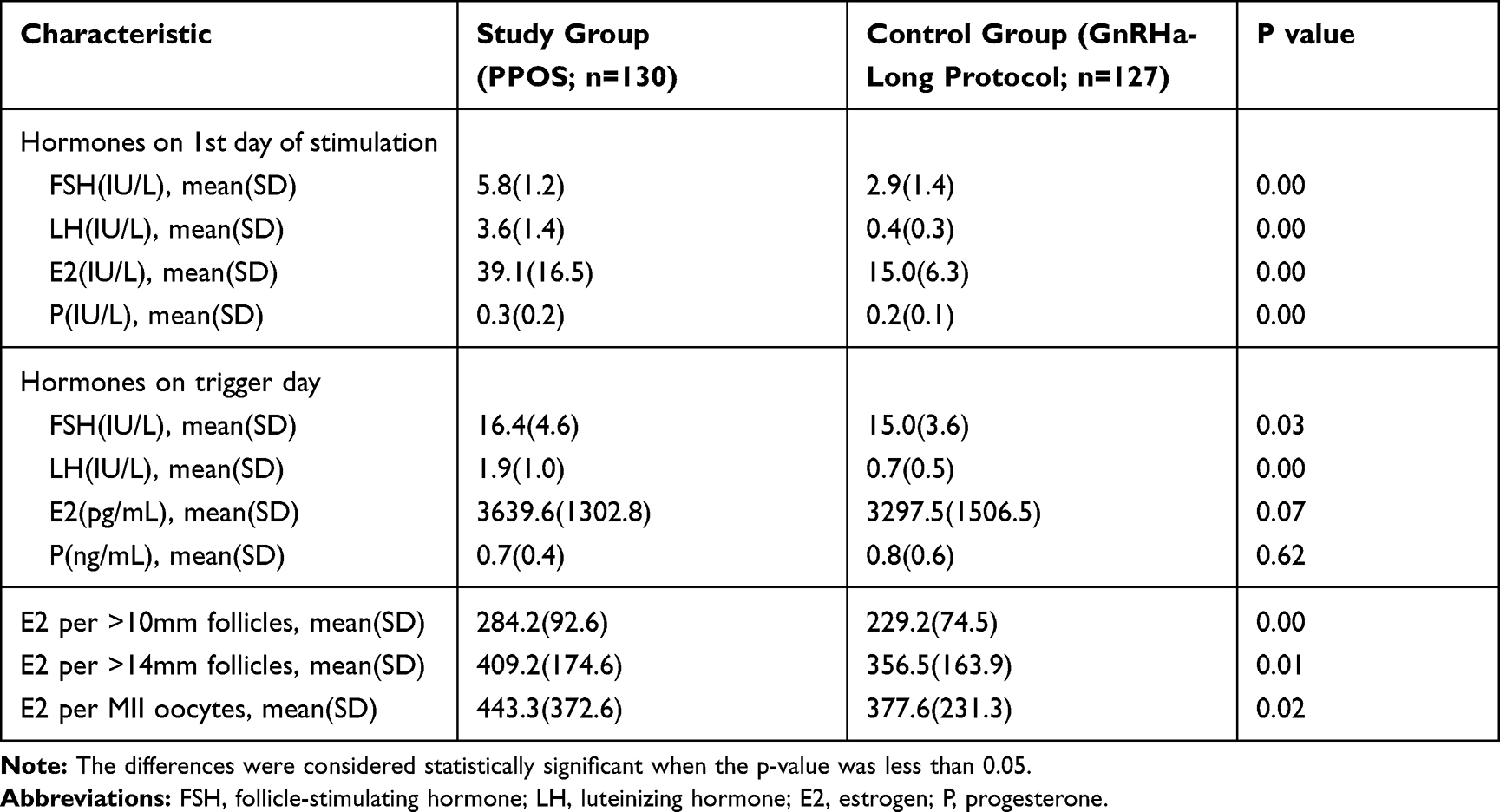 |
Table 4 Hormone Profiles During Ovarian Stimulation in the Two Groups |
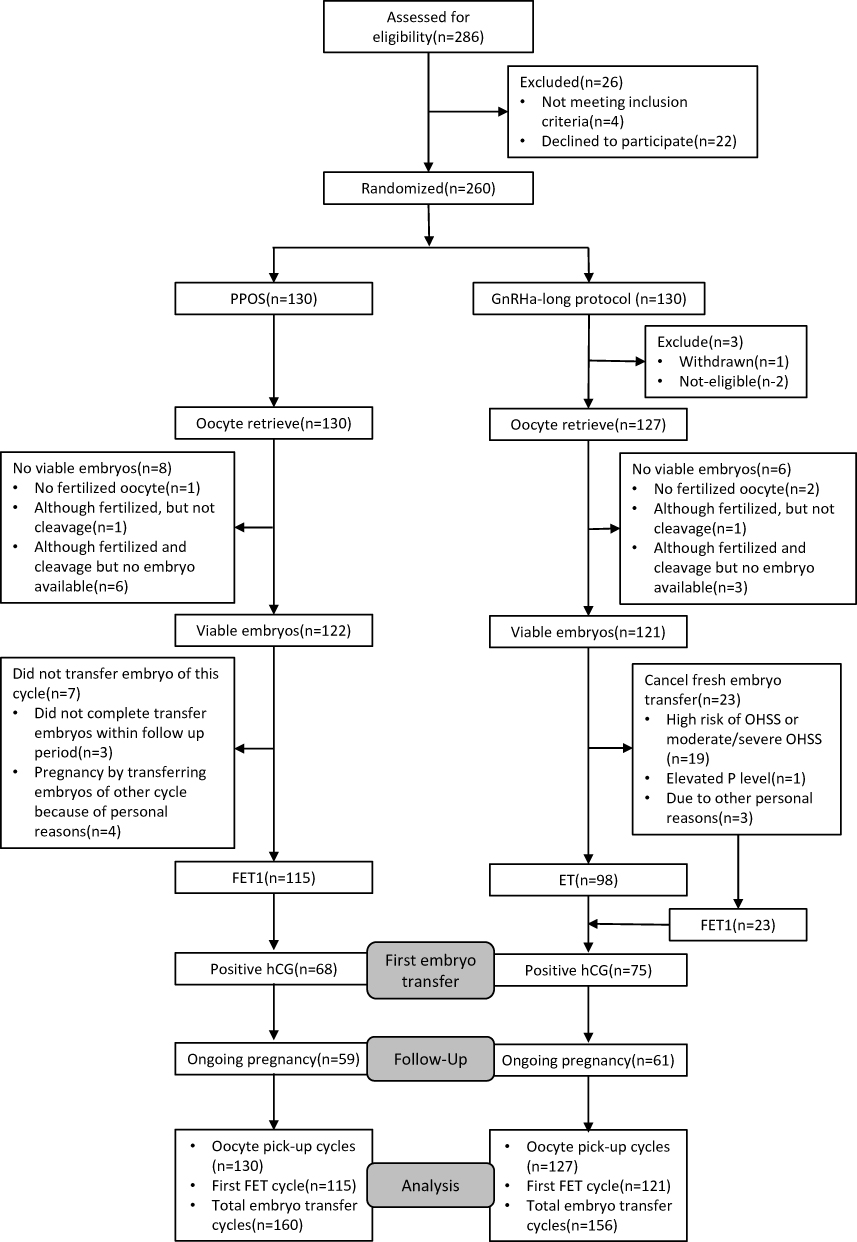 |
Figure 1 A flow chart of the patient allocation in an RCT of PPOS versus GnRHa-long protocol. Abbreviations: PPOS, progesterone-primed ovarian stimulation; MPA, medroxyprogesterone acetate; ET, fresh embryo transfer; FET, frozen embryo transfer. |
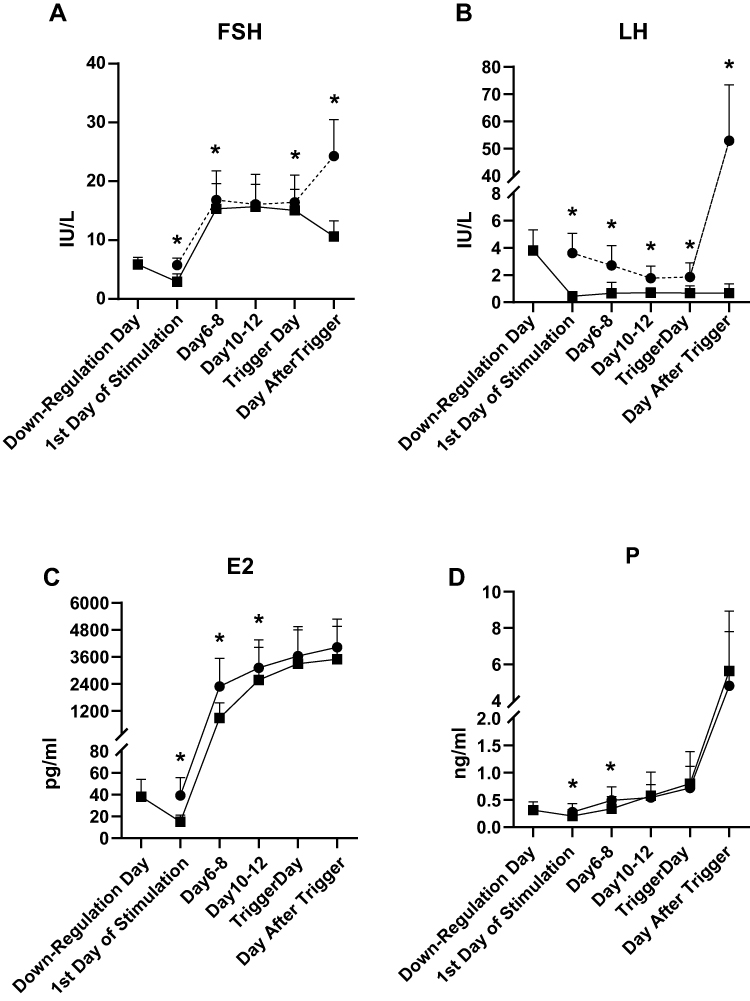 |
Figure 2 Concentrations of FSH, LH, E2, and P in the two groups during controlled ovarian stimulation. Abbreviations: FSH, follicle-stimulating hormone; LH, luteinizing hormone; E2estrogen; P, progesterone. |
In the PPOS group, the LH levels decreased gradually during the controlled ovarian stimulation, and the basal LH value was significantly higher than the average LH values on the trigger day (P<0.01). However, the LH value increased significantly to 50.88±20.55 IU/L 10 hrs after the trigger. Meanwhile, the LH level increased slowly all the way during the stimulation, and the average LH level on the trigger day was significantly higher than that on the first day of stimulation (P<0.01) in the control group.
Serum E2 values showed a gradual increase accompanying the growth of follicles during ovarian stimulation in both group and the average E2 level was significantly higher in the PPOS group than that in the GnRHa-long group all the time during the stimulation (P<0.05). We also analysed the E2 level per matured oocytes and it turned to be significantly higher in the PPOS group than the control group (443.3±372.6 versus 377.6±231.3, P<0.05).
P levels remained low during ovarian stimulation until the day of trigger and increased significantly after trigger (P<0.05) in the two groups. The average P level was significantly higher in the PPOS group (0.3±0.2 versus 0.2±0.1, P<0.05) on the start day of hMG while they were comparable on the trigger day between the two groups (P>0.05).
During the 5 months of the trial follow-up, 236 patients of both groups completed their first embryo transfer cycles (Table 5). One hundred and fifteen patients with viable embryos underwent their first frozen-thawed embryo transfer in the study group. All the 121 women in the control group finished their first embryo transfer cycle, including 98 fresh embryo transfer cycles and 23 FET cycles. The rate of viable frozen-thawed embryos was 100% (235/235). In total, nine patients in the study group and seven patients in the control group had a single embryo transfer. Meanwhile, 106 patients in the study group and 114 ones in the control group had a double embryo transfer, and no difference was found between two groups (P = 0.53). The clinical pregnancy rate per transfer was 56.5% (65/115) in the PPOS group, in contrast with 57.0% (69/121) in the GnRHa long group (P=0.94). The endometrial thickness was significantly thinner in the study group (11.5±2.4 versus 12.3±2.6, P=0.02) while using different endometrium preparations. Patients who had early miscarriages are fewer in the study group compared with that in the control group but did not reach statistical significance (4.6% versus 8.7%, P=0.55). The multiple pregnancy rate was similar between the two groups (27.7% versus 30.4%, P=0.73). There was one woman in the study group who had an intrauterine and ectopic pregnancy, she had surgery to deal with the ectopic one and had ongoing pregnancy with the intrauterine one till the end of the study. The implantation rate of embryos from the two groups appeared to be similar (38.0% versus 39.2%, P=0.80). This implied that the embryos shared comparable development potential in the two groups.
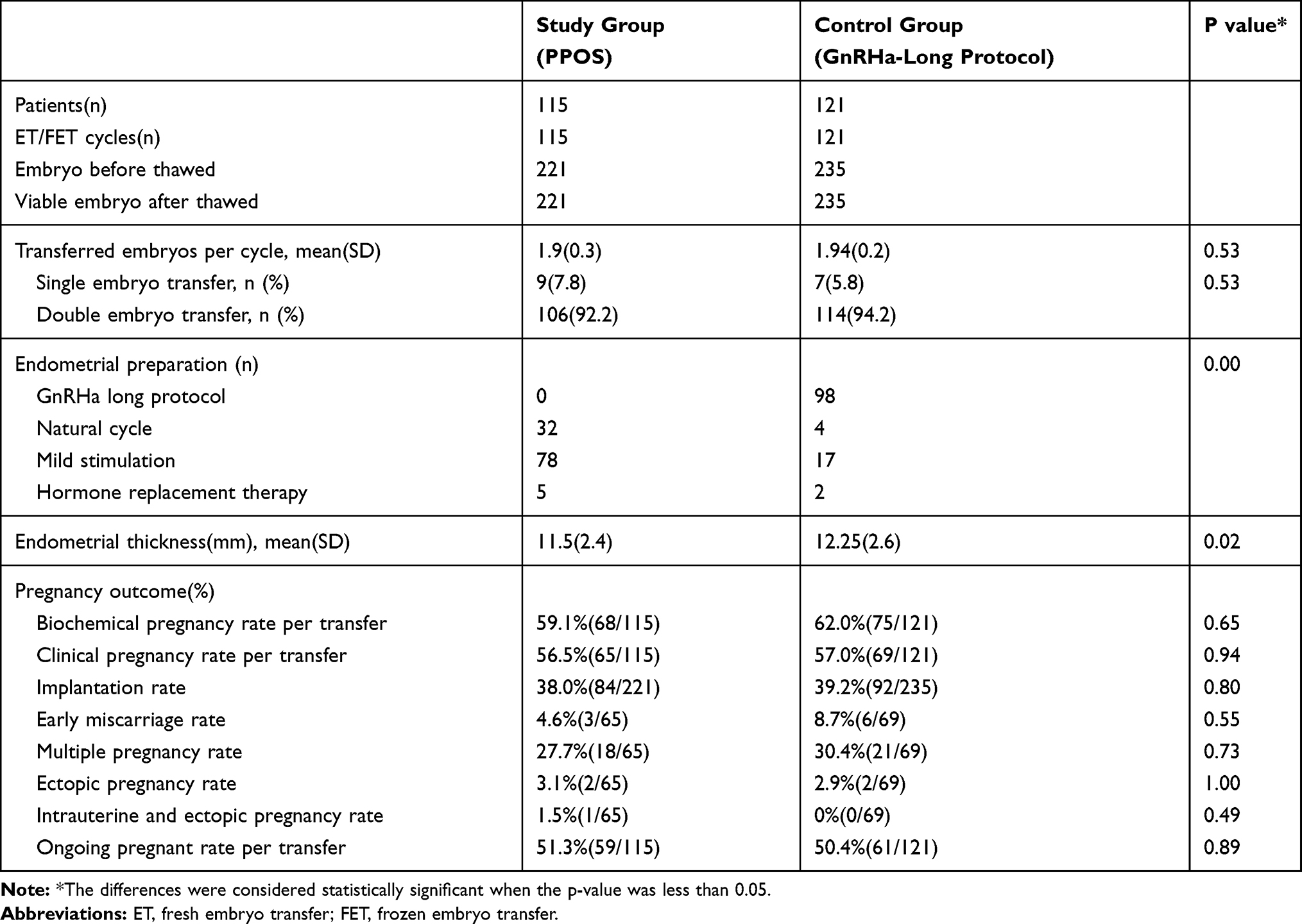 |
Table 5 Pregnancy Outcomes of the First ET/FET Cycles Originating from the Two Regimens |
Twenty-three women who cancelled fresh embryo transfer in the GnRHa-long group transferred frozen ones for the first embryo transfer cycle. Meanwhile, 115 women with viable embryos underwent their first frozen-thawed embryo transfer in the PPOS group. The pregnancy outcomes of the first FET cycles originating from the two groups are presented in Table 6. Since we used similar regimens to did endometrial preparation in both groups for FET cycles, the endometrial thickness was comparable (P=0.53). There was also no significant difference in the pregnancy outcomes including implantation rate (38.0% versus 48.9%, P=0.17), clinical pregnancy rate (56.5% versus 69.6%, P=0.25), early miscarriage rate (4.6% versus 12.5%, P=0.26) and ongoing pregnant rate (51.3% versus 56.5%, P=0.65).
 |
Table 6 Pregnancy Outcomes of the First FET Cycles Originating from the Two Groups |
Discussion
This is the first randomized controlled trial comparing PPOS (combination of hMG and MPA) and GnRHa long protocol in IVF/ICSI cycles. The cycle characteristics and clinical efficiency of the two protocols were explored. The result of this study shows that PPOS can achieve a comparable number of oocyte retrieved to GnRHa long protocol while using less HMG dosage. Furthermore, there was no moderate and severe OHSS in the study group but three in the control protocol. The similar clinical outcomes of their first ET/FET cycles indicate that the embryos derived from PPOS had identical developmental potential compared to those from the GnRHa long protocol. All of these suggest that PPOS could be an appropriate alternative like GnRHa long protocol in young normogonadotropic women undergoing IVF.
The results showed that no statistically significant difference was noted in the number of oocytes retrieved, the number of top-quality embryos, and the rate of viable embryo rate per oocyte retrieved in the two groups. However, a short duration of gonadotropin stimulation and a lower total amount of HMG are required in the PPOS group. This may have a relation with the FSH and E2 levels, which were always higher than that in the control group in the PPOS group during the entire process of ovarian stimulation. The same trend also reflected on the LH concentration. These findings are in agreement with those of previous studies that compared PPOS with the short protocol.6,12,13 The results suggest that using progesterone during ovarian stimulation may have a weaker ability to suppress the HPO axis than GnRH agonist. One possible reason for this phenomenon is related to the different mechanisms to suppress the LH surge of the two protocols during COH. However, the mechanism underlying the process of progesterone blocking the LH surge in females still remains to be explored.
Ovarian hyperstimulation syndrome (OHSS) is the most important iatrogenic complication of exogenous gonadotropin therapy used for assisted reproductive treatments.14 It always presents early onset (3–7 days after hCG administration in susceptible patients) or late-onset (during early pregnancy, 12–17 days after hCG administration).15 Another highlight of this study is that none of the patients went through moderate and severe OHSS in the study group, which showed the same result with our previous studies.6,12,13 However, there were three women in the GnRHa long group suffered moderate and severe OHSS. In this trial, PPOS was a protocol in combination with “freeze-all strategy”, and we cancelled the fresh embryo transfer of the women who were at high risk of OHSS in the GnRHa long protocol. These effectively prevented the patients from late OHSS, which is induced by endogenous hCG from the early pregnancy.16 Accordingly, early OHSS, which is classically thought to be a consequence of exogenous hCG administration used to triggering oocyte maturation,16 is considered to be the main concern. In the study group, we used a dual trigger of a low dose of hCG (1000IU) with GnRH-a to avoid a poor response of the HPO axis, as it was shown to have a beneficial effect on the maturity of oocytes in this regimen.6,7 However, a high dose of hCG (5000IU), which was shown to be the recommended minimum dose of hCG considering safety and effectiveness,17 was used for trigger in GnRHa long protocol group. Therefore, we thought that this is the main cause of the higher incidence of moderate and severe OHSS in the control group.
PPOS is an ovarian regimen based on a high progesterone circumstance during COH, which has a negative impact on endometrium receptivity. Embryos obtained from PPOS thus require total freezing and delayed transfer after thawing instead of fresh transfer. On the contrary, we did a fresh embryo transfer as the first choice in the GnRHa long protocol group. However, for those who were at high risk of OHSS, had an elevated P on the trigger day or other personal reasons, we cancelled the fresh transfer and cryopreserved all the embryos for frozen transfer later. Therefore, we observed and analyzed the first embryo transfer cycle of both groups, and the result showed that the clinical pregnancy rate, ongoing pregnancy rate and implantation rate were all similar between the two groups. To exclude the effects of different endometrium preparations, results of the first frozen embryos transfer cycles of the patients who cancelled fresh transfer in the GnRHa long protocol group and the ones in the PPOS group who did frozen embryos transfer originally were also compared in our trial (Table 6). No difference was found in clinical pregnancy rate, implantation rate and ongoing pregnancy rate between the two groups. Consequently, it is reasonable to believe that embryos derived from PPOS had equal developmental potential as those originating from the GnRHa long protocol.
At present, research about the safety of PPOS is limited. Our previous study demonstrated that high progesterone level did not appear to have a detrimental role in oocytes and embryos.6,12 Although MPA was contraindicated in human pregnancy, a study following up 1893 live-born infants born from HMG+MPA treatment found that it did neither compromised neonatal outcomes nor increase the prevalence of congenital malformations compared with short protocol and mild ovarian stimulation.18 In contrast, the GnRHa long protocol has been generally reorganized and extensively used worldwide for IVF treatment.
A weakness of the study is that the physician and patients were not blinded to the trial. Moreover, at the end of the study, there were still some people who had not finished their first embryo transfer cycle. It would be better if the live-birth rates were observed in the follow-up period and the result could be demonstrated.
Conclusion
This RCT showed that PPOS in combination with embryo cryopreservation as an ovarian stimulation regimen was as effective as GnRHa long protocol during COH under different endocrinal mechanism. It can also achieve comparable embryological and clinical outcomes while reducing the incidence of moderate and severe OHSS and HMG dosage. MPA has the advantages of an oral administration route, easy access, more control over LH levels. It can be an alternative to the treatments for infertile patients with normal ovarian reserve undergoing IVF.
Acknowledgments
We gratefully acknowledge all the staff of the department of assisted reproduction in Shanghai Ninth People’s Hospital for their cooperation and support.
Funding
This study was supported by the National Nature Science Foundation of China (No. 31770989, 81501334), and Shanghai Ninth Hospital Foundation of China (JYLJ030).
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Dada T, Salha O, Baillie HS, Sharma V. A comparison of three gonadotrophin-releasing hormone analogues in an in-vitro fertilization programme: a prospective randomized study. Hum Reprod. 1999;14(2):288–293. doi:10.1093/humrep/14.2.288
2. Caspi E, Ron-El R, Golan A, et al. Results of in vitro fertilization and embryo transfer by combined long-acting gonadotropin-releasing hormone analog D-Trp-6-luteinizing hormone-releasing hormone and gonadotropins. Fertil Steril. 1989;51(1):95–99. doi:10.1016/S0015-0282(16)60435-1
3. Ren J, Sha A, Han D, Li P, Geng J, Ma C. Does prolonged pituitary down-regulation with gonadotropin-releasing hormone agonist improve the live-birth rate in in vitro fertilization treatment? Fertil Steril. 2014;102(1):75–81. doi:10.1016/j.fertnstert.2014.03.030
4. Albuquerque LE, Saconato H, Maciel MC. Depot versus daily administration of gonadotrophin releasing hormone agonist protocols for pituitary desensitization in assisted reproduction cycles. Cochrane Database Syst Rev. 2005;1:Cd002808.
5. Oyesanya OA, Teo SK, Quah E, Abdurazak N, Lee FY, Cheng WC. Pituitary down-regulation prior to in-vitro fertilization and embryo transfer: a comparison between a single dose of Zoladex depot and multiple daily doses of suprefact. Hum Reprod. 1995;10(5):1042–1044. doi:10.1093/oxfordjournals.humrep.a136090
6. Kuang Y, Chen Q, Fu Y, et al. Medroxyprogesterone acetate is an effective oral alternative for preventing premature luteinizing hormone surges in women undergoing controlled ovarian hyperstimulation for in vitro fertilization. Fertil Steril. 2015;104(1):62–70 e3. doi:10.1016/j.fertnstert.2015.03.022
7. Lu X, Hong Q, Sun L, et al. Dual trigger for final oocyte maturation improves the oocyte retrieval rate of suboptimal responders to gonadotropin-releasing hormone agonist. Fertil Steril. 2016;106(6):1356–1362. doi:10.1016/j.fertnstert.2016.07.1068
8. Qin N, Chen Q, Hong Q, et al. Flexibility in starting ovarian stimulation at different phases of the menstrual cycle for treatment of infertile women with the use of in vitro fertilization or intracytoplasmic sperm injection. Fertil Steril. 2016;106(2):334–341.e1. doi:10.1016/j.fertnstert.2016.04.006
9. Henkel RR, Schill WB. Sperm preparation for ART. Reprod Biol Endocrinol. 2003;1:108. doi:10.1186/1477-7827-1-108
10. Cummins JM, Breen TM, Harrison KL, Shaw JM, Wilson LM, Hennessey JF. A formula for scoring human embryo growth rates in in vitro fertilization: its value in predicting pregnancy and in comparison with visual estimates of embryo quality. J In Vitro Fert Embryo Transf. 1986;3(5):284–295. doi:10.1007/BF01133388
11. Yu S, Long H, Chang HY, et al. New application of dydrogesterone as a part of a progestin-primed ovarian stimulation protocol for IVF: a randomized controlled trial including 516 first IVF/ICSI cycles. Hum Reprod. 2018;33(2):229–237.
12. Wang Y, Chen Q, Wang N, Chen H, Lyu Q, Kuang Y. Controlled ovarian stimulation using medroxyprogesterone acetate and hMG in patients with polycystic ovary syndrome treated for IVF: a double-blind randomized crossover clinical trial. Medicine (Baltimore). 2016;95(9):e2939. doi:10.1097/MD.0000000000002939
13. Zhu X, Ye H, Fu Y. The utrogestan and hMG protocol in patients with polycystic ovarian syndrome undergoing controlled ovarian hyperstimulation during IVF/ICSI treatments. Medicine (Baltimore). 2016;95(28):e4193. doi:10.1097/MD.0000000000004193
14. Practice Committee of American Society for Reproductive Medicine. Ovarian hyperstimulation syndrome. Fertil Steril. 2008;90(5 Suppl):S188–S193. doi:10.1016/j.fertnstert.2008.08.034
15. Orvieto R. Triggering final follicular maturation–hCG, GnRH-agonist or both, when and to whom? J Ovarian Res. 2015;8:60. doi:10.1186/s13048-015-0187-6
16. Mathur RS, Akande AV, Keay SD, Hunt LP, Jenkins JM. Distinction between early and late ovarian hyperstimulation syndrome. Fertil Steril. 2000;73(5):901–907. doi:10.1016/S0015-0282(00)00492-1
17. Abdalla HI, Ah-Moye M, Brinsden P, Howe DL, Okonofua F, Craft I. The effect of the dose of human chorionic gonadotropin and the type of gonadotropin stimulation on oocyte recovery rates in an in vitro fertilization program. Fertil Steril. 1987;48(6):958–963. doi:10.1016/S0015-0282(16)59591-0
18. Zhang J, Mao X, Wang Y, et al. Neonatal outcomes and congenital malformations in children born after human menopausal gonadotropin and medroxyprogesterone acetate treatment cycles. Arch Gynecol Obstet. 2017;296(6):1207–1217. doi:10.1007/s00404-017-4537-z
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.