Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 14
Comparison Between Pioglitazone/Metformin Combination Therapy and Sitagliptin/Metformin Combination Therapy on the Efficacy in Chinese Type 2 Diabetic Adults Insufficiently Controlled with Metformin: Study Protocol of an Open-Label, Multicenter, Non-Inferiority Parallel-Group Randomized Controlled Trial
Authors Zhang F, Tang L, Li J ![]() , Yan Z, Li J, Tong N
, Yan Z, Li J, Tong N
Received 21 November 2020
Accepted for publication 18 February 2021
Published 18 March 2021 Volume 2021:14 Pages 1243—1252
DOI https://doi.org/10.2147/DMSO.S293307
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ming-Hui Zou
Fang Zhang, Lizhi Tang, Jing Li, Zhe Yan, Juan Li, Nanwei Tong
Division of Endocrinology and Metabolism, West China Hospital of Sichuan University, Chengdu, People’s Republic of China
Correspondence: Nanwei Tong
Division of Endocrinology and Metabolism, West China Hospital of Sichuan University, 37 Guoxuexiang, Chengdu, Sichuan, 610041, People’s Republic of China
Tel +86-18980601196
Fax +86-28-85423459
Email [email protected]
Introduction: The prevalence of type 2 diabetes (T2D) has risen substantially in China, where its pathophysiology is primarily characterized by insulin resistance (IR). Alleviating IR may help with the management of T2D in the Chinese population. Pioglitazone and sitagliptin are two hypoglycemic medications with different pharmacological actions, both of which are optimal choices for use in combination with metformin. Previous studies have yielded mixed findings regarding the differences in hypoglycemic effects between the two agents. Though pioglitazone is associated with weight gain, both drugs have been shown to decrease visceral adipose tissue (VAT) and improve IR in individuals with T2D. There is a lack of direct comparisons between pioglitazone and sitagliptin among Chinese individuals with T2D. Therefore, this paper describes a protocol for a randomized controlled trial (RCT) that investigates the differences in hypoglycemic efficacy, IR improvement, and safety profiles between these drugs.
Methods and Analysis: This is a 24-week, open-label, multicenter, non-inferiority parallel-group RCT with a 1:1 allocation ratio. It compares pioglitazone/metformin (15 mg/500 mg) combination therapy with sitagliptin/metformin (50 mg/500 mg) combination therapy in Chinese adults with T2D insufficiently controlled with metformin. The primary outcomes are HbA1c reduction, insulin level increase, and IR index change. The secondary outcomes are body weight and abdominal VAT decreases, lipid profiles, and inflammatory indicators. Tolerability and safety data will also be collected.
Conclusion: It is believed that the direct comparisons of the hypoglycemic effects, VAT reductions, and safety profiles between pioglitazone and sitagliptin will help to optimize treatments for Chinese adults with T2D who are primarily characterized by IR.
Trial Registration Number: Chinese Clinical Trial Registry (ChiCTR1900021861).
Keywords: type 2 diabetes, randomized controlled trial, study protocol, pioglitazone, sitagliptin, combination therapy
Introduction
During the last four decades, the prevalence of type 2 diabetes (T2D) has increased dramatically in China. A nationwide cross-sectional study of 98,658 Chinese adults conducted in 2010 determined that the overall prevalence of diabetes in China was approximately 11.6%.1 The study found that only 25.8% of individuals with T2D received treatment, of which only 39.7% had adequate glycemic control.1 Insulin resistance (IR) and islet β-cell dysfunction are the two major factors contributing to the pathophysiology of T2D. Previous studies conducted in Japanese and Asian-American populations indicated that in East Asians, T2D is mainly characterized by β-cell dysfunction rather than IR.2,3 However, a recent cohort study of 94,952 Chinese adults found that IR is more strongly associated with incident diabetes than β-cell dysfunction in this population.4 This finding may underscore the importance of maintaining or reversing insulin sensitivity as a strategy to adequately manage T2D in Chinese adults.
A Brief Overview of Metformin, Pioglitazone, and Sitagliptin
Metformin is considered a first-line treatment, as well as the cornerstone of combination therapy, in the management of hyperglycemia.5 Metformin reduces plasma glucose through multiple mechanisms, such as reducing hepatic glucose output and improving peripheral insulin sensitivity.6 In Chinese patients, it has been shown that metformin may decrease glycated hemoglobin (HbA1c) by 0.7–1.0%.6 Several studies observed that compared with sulfonylureas, metformin was associated with a significant reduction in cardiovascular events in patients with T2D.7,8 When metformin is inadequate for glucose control at its target dose, combination treatment is a recommended option.
Thiazolidinedione (TZD) is an insulin sensitizer. Pioglitazone is a TZD that decreases plasma glucose by improving IR.5 Clinical trials in Chinese adults with T2D have found that pioglitazone may decrease HbA1c by 0.7–0.9%.9,10 Several large clinical trials have demonstrated the cardiovascular benefits of pioglitazone. For example, the PROactive study found that pioglitazone may significantly reduce the risk of microvascular complications and cardiovascular disease (CVD) in patients with T2D.11 The IRIS study demonstrated that pioglitazone may significantly reduce the risk of both stroke recurrence and myocardial infarction in non-diabetic participants with IR and a history of stroke or transient ischemic attack.12 Moreover, T2D trials have reported that pioglitazone significantly decreases visceral fat volume and alleviates lipotoxicity, both of which have key roles in the pathogenesis of IR, T2D, and CVD.13,14
Sitagliptin, the first FDA-approved dipeptidyl peptidase 4 (DPP4) inhibitor, is an incretin-based medicine that decreases blood glucose by enhancing the levels of glucagon-like peptide-1 and other incretin hormones.5 Several clinical trials carried out in Chinese patients with T2D have demonstrated that sitagliptin may reduce HbA1c levels by 0.6–0.9%.15–17 Further, the TECOS study suggested that sitagliptin did not increase the risk of major adverse cardiovascular events or heart failure hospitalization in patients with T2D and established CVD.18 A Chinese trial also reported that sitagliptin significantly decreased intrahepatic lipid and abdominal visceral adipose tissue (VAT) in participants with T2D and nonalcoholic fatty liver disease (NAFLD).19
Both pioglitazone and sitagliptin are optimal choices for use in combination with metformin to treat hyperglycemia.5 Since pioglitazone and sitagliptin have different mechanisms of action, the two agents are also suitable for combination use in clinical practice.20 In postmenopausal women and older men, common side effects of pioglitazone include weight gain, edema, and increased bone fracture risk.5 Common side effects of sitagliptin include gastrointestinal events, nasopharyngitis, and headache.15
Previous Findings Comparing Pioglitazone and Sitagliptin
Some studies have compared the effects of pioglitazone and sitagliptin, most of which investigated the differences in their hypoglycemic effects and safety profiles. Findings regarding the comparative effects of the drugs on HbA1c reduction are mixed, with some studies reporting that pioglitazone was superior to sitagliptin,21–23 and others not supporting this finding.24–26 Reasons for these inconsistent findings may include different pioglitazone dosages, different drug combinations, and varying treatment durations. However, results specific to body weight change, tolerability, and safety profiles were quite consistent. Specifically, these studies reported that pioglitazone was inferior to sitagliptin in terms of weight control, and both drugs were generally well tolerated.21–26 It is worth noting that none of the studies based their conclusion on patients with T2D from mainland China.
A propensity score-matched analysis found that compared with DPP4 inhibitors, TZD was significantly better at alleviating IR and inferior at improving β cell function.27 Similarly, a meta-analysis demonstrated that sitagliptin and metformin combination therapy was more effective than pioglitazone and metformin combination therapy in improving β cell function.28 Conversely, a randomized controlled trial (RCT) of the maximum dosages of pioglitazone and sitagliptin showed that both medications had similar effects on β cell function improvement.21 In terms of insulin sensitivity, a study of participants with T2D and NAFLD reported that although pioglitazone users experienced more weight gain than sitagliptin users, they also experienced greater improvements in NAFLD.29
Abdominal obesity, and especially VAT, is closely related to the incidence of IR, T2D, and CVDs.13,14,30 Compared with Westerners at the same body mass index, Chinese individuals have a higher percentage of body fat, which indicates that they are predisposed to abdominal obesity.4,31 Several studies have concluded that although pioglitazone may have induced weight gain, it significantly decreased intrahepatic and visceral fat and led to the improvement of metabolic activity in patients with T2D; this effect may have been independent of its hypoglycemic effect.13,14 Similarly, another study found that when taken in combination with metformin, sitagliptin significantly reduced intrahepatic fat and VAT in Chinese patients with T2D.19 To the best of our knowledge, only one RCT has directly compared the effects of pioglitazone and sitagliptin on abdominal visceral fat volume.32 This study found that neither drug had an effect on VAT in Japanese patients with T2D and NAFLD.32
As there is a lack of direct comparisons of the hypoglycemic effects, tolerability, and safety profiles of pioglitazone and sitagliptin among Chinese adults with T2D, we propose to conduct an RCT in this population of patients who are insufficiently controlled by metformin alone. Additionally, we also propose to investigate the differences between these two medications in abdominal VAT and IR improvement. We believe that this study’s findings will help to optimize treatments for Chinese individuals with T2D who are primarily characterized by IR.
Methods and Analyses
Study Design
This is an open-label, multicenter, non-inferiority parallel-group RCT with a 1:1 allocation ratio comparing pioglitazone/metformin (15 mg/500 mg) combination therapy with sitagliptin/metformin (50 mg/500 mg) combination therapy in adults with T2D who fail to respond to the metformin monotherapy (Figure 1). This study takes place within the Division of Endocrinology and Metabolic Diseases in 33 academic and non-academic hospitals in China, among which nine hospitals are in Chengdu. The study is currently ongoing – the first participant was enrolled on December 9, 2019. We expect that the last participant will be enrolled in June 2021 and study completion will occur by March 2022.
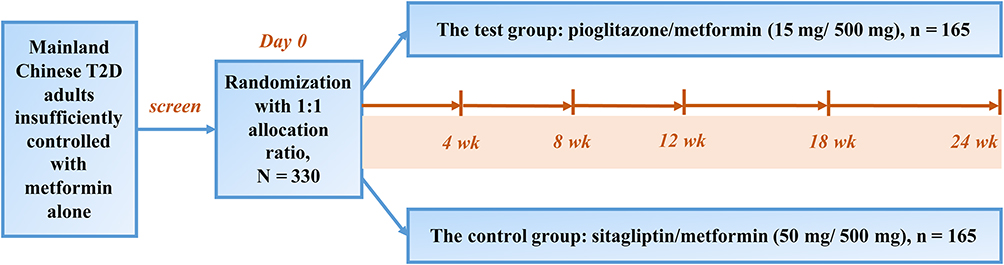 |
Figure 1 The flowchart of study design. T2D, type 2 diabetes; wk, week. |
The protocol of this study was designed in accordance with the recommendations of the Standard Protocol Items: Recommendations for Interventional Trials guideline.33
Participants
The diagnosis of T2D in this study is in accordance with the 1999 World Health Organization recommendations.34 Individuals who meet all the inclusion/exclusion criteria (Figure 2) are eligible for participation. Individuals who do not pass the primary screening, are lost to follow-up, or withdraw will no longer be included in the study and their participant identification number and treatment will not be reused.
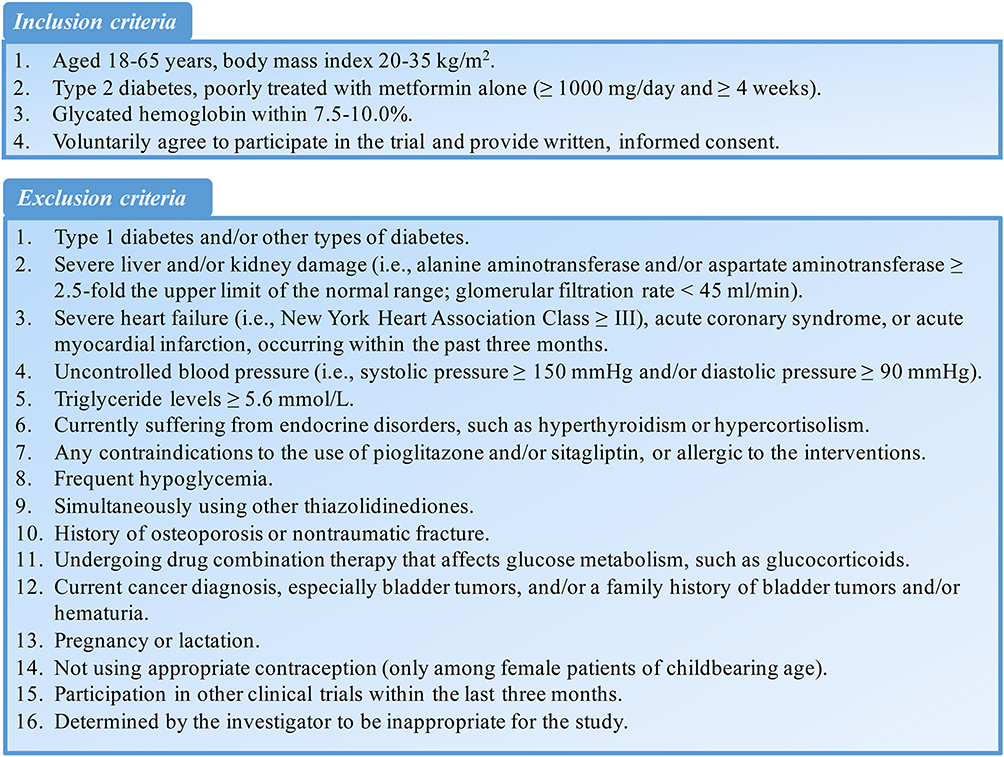 |
Figure 2 The inclusion and exclusion criteria of this study. |
Sample Size Calculation
As a non-inferiority RCT, the sitagliptin/metformin tablets (brand name Janumet®) are chosen as the positive control. The primary outcome is the reduction from baseline in HbA1c after 24-weeks of treatment. According to the “Guidelines for Clinical Trials of Drugs and Biological Products for the Treatment of Diabetes” issued by the National Medical Products Administration,35 the HbA1c threshold is suggested as 0.3% or 0.4% in a non-inferiority RCT with a positive drug as the control. Therefore, the non-inferiority margin was set at 0.4%.
Based on the guideline,35 it is estimated to provide 80% power to detect a non-inferiority margin (δ) of 0.4% for HbA1c change, by using a one-sided test with 0.025 significance level. Since this is a non-inferiority trial, we set the treatment difference as zero. Based on a previous trial,24 an estimated standard deviation (SD) of 1.23 for the intrasubject difference is expected. The sample size of the test group and the control group is equal, and the sample size of each group is 150 calculated by the PASS version 15.0 (NCSS, LLC).36 Additionally, with a 10% discontinuation rate, the final sample size for each group is 165.
The study sites located in Chengdu will also evaluate the effects of pioglitazone/metformin and sitagliptin/metformin combination therapies on visceral fat, pancreatic fat, and skeletal muscle fat. Since this part is an exploratory work, it does not require a sample size estimation.37 Magnetic resonance imaging (MRI) is considered to be the golden standard for the measurement of body composition, as well as intracellular fat in liver, pancreas, and skeletal muscle.38,39 Based on previous studies that included 12 to 25 individuals per group,40–42 the sample size for this part of work is set to 30 participants per group.
Intervention
The intervention group receives pioglitazone/metformin tablets (15 mg/500 mg, brand name Kashuangping®, National Medicine Approval Number: H20100180, produced by Hangzhou Zhongmei Huadong Pharmaceutical Co. Ltd.), while the control group receives sitagliptin/metformin tablets [50 mg/500 mg, brand name Janumet®, Imported Medicine Registration Certificate Number: H20130233, produced by MSD Pharma (Singapore) Pte. Ltd.]. Both of the medications are currently available for purchase on the market.
The intervention starts after randomization. The total treatment duration of the study is 24 weeks. The intervention tablets are prescribed twice a day (five minutes before breakfast and dinner), in both the pioglitazone/metformin test group and the sitagliptin/metformin control group. After 4-weeks of treatment, those with excellent glycemic control are to remain with the medication regimen for another 20 weeks. However, for participants with poor glycemic control (fasting plasma glucose > 7 mmol/L), in (a) the treatment group, the dose frequency of the pioglitazone/metformin tablets will be adjusted to three times a day (to be taken 5 minutes before breakfast, lunch and dinner), while in (b) the control group, a tablet of metformin (500 mg) will be added (to be taken 5 minutes before lunch) to the same regimen of sitagliptin/metformin as before, for the last 20 weeks.
Randomization and Treatment Allocation
Randomization will occur after participants provide signed informed consent. The School of Public Health, Tongji Medical College, Huazhong University of Science and Technology is responsible for randomization. Stratified block randomization will be performed according to HbA1c ≥ 8.5% or HbA1c < 8.5%. The allocation ratio is 1:1. The random number and group are automatically assigned by an interactive web response system.
After an individual completes the screening tests, investigators will judge whether he/she meets the eligibility criteria. Then, investigators will input the basic information (eg, initials, age, gender, screening number, etc.) and HbA1c result (the stratification factor) of the successfully screened individual into the network central randomization system. The system will automatically generate a random number and subject ID according to the aforementioned protocol and rapidly inform the investigators about whether the participant is assigned to the treatment or the control group. Randomization information will be generated in the system by the statisticians based on the preset number of seeds and blocks. After receiving the randomization results, investigators at each center will treat the participants according to the assigned intervention.
Participant Timeline
At screening, potential participants are asked to provide self-report information about their baseline characteristics, past history, and medicine treatment. After randomization, participants will receive the assigned intervention regimen. During the 24-week study period, all participants are required to visit the study centers every 4 to 6 weeks, as displayed in Figure 3.
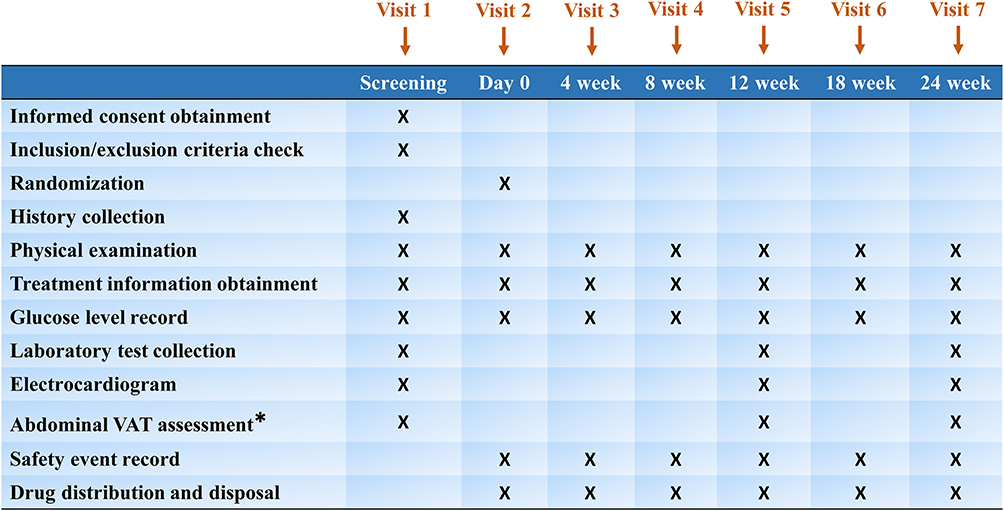 |
Figure 3 The participant timeline in this study. VAT, visceral adipose tissue. *The participants in Chengdu will be assessed by magnetic resonance imaging, while the others assessed by color Doppler ultrasound. |
Outcome Measures
This study aims to compare the therapeutic effects of pioglitazone/metformin combination therapy with sitagliptin/metformin combination therapy in Chinese adults with T2D, with a focus on changes in HbA1c, insulin sensitivity, inflammatory factors, visceral fat, and safety profiles.
The primary outcomes include HbA1c reduction, fasting insulin increase, and changes in homeostasis model assessment as an index of IR (HOMA-IR), and the proinsulin-to-insulin ratio.
There are seven secondary outcomes: (i) reductions in fasting plasma glucose and two-hour plasma glucose after a standard meal; (ii) changes in the lipid profile, including triglycerides, cholesterol, high density lipoprotein cholesterol, and low density lipoprotein cholesterol; (iii) changes in inflammatory indicators, such as interleukin-6 and adiponectin; (iv) decreases in body weight and visceral fat (where the intracellular fat in the liver, pancreas, and skeletal muscle of participants in Chengdu is assessed by MRI and the changes in liver fat are assessed by color Doppler ultrasound in participants outside of Chengdu); (v) changes in liver enzyme indicators including alanine aminotransferase and aspartate aminotransferase; (vi) changes in the urine albumin-to-creatinine ratio; and (vii) changes in blood pressure.
Safety outcomes are also of interest in the study and are assessed through physical examination, blood and urine routine laboratory tests, an electrocardiogram, and the incidence of hypoglycemic events and other adverse events (AEs)/serious AEs (SAEs).
All the laboratory inspection items will be sent to the central laboratory in Shanghai (the Adicon Clinical Laboratories, Ltd.) for testing. For the comparison in the VAT change, the Chengdu participants will use the MRI data, while the other area participants will use the ultrasound data for liver fat assessment. According to the methodological consistency, the liver fat comparisons will be carried out respectively, distinguishing the MRI-users from the ultrasound-users.
Training Plans, Handling and Storage of Data and Documents
All the principal investigators have ensured that the staff who work on the trial within each study site (including physicians and nurses) are properly trained. This includes awareness of the inclusion/exclusion criteria, the whole study process, the usage of electronic case report forms (eCRF), the AE/SAE reporting process, etc. In the event that the study protocol is updated, all the investigators will be provided with the latest information.
According to protocol requirements, investigators must accurately and completely record the data in the eCRF and answer queries in a timely manner. All the completed eCRFs are to be printed out and signed by the investigators and preserved for five years after study completion at each site.
Monitoring and Quality Assurance
Before the trial began, the principal investigators from each site discussed and developed the study protocol together, after which all of the study staff were trained in study protocols at the same time. All the participating sites are to adopt the study’s standard operating procedures to ensure the quality of the study and the implementation of quality assurance systems.
To ensure the reliability and completeness of data, the authorized third-party clinical research associates will regularly conduct systematic monitoring of each site to determine whether trial implementation is consistent with the protocol and whether the online data are consistent with the original records. A monitoring report is to be recorded for each visit.
Moreover, to better supervise the study, the project leader and the study sponsor will audit each site from time to time to evaluate whether the implementation and the data recording and analysis are performed in compliance with the protocol and the Good Clinical Practice (GCP) rules and regulations. An audit report is to be created after each visit.
Statistical Analysis
There are three types of analysis sets in this study: the full analysis set (FAS), the per protocol set (PPS), and the safety set (SS). Based on the principle of intention to treat, the FAS contains the participants who do not violate the inclusion/exclusion criteria, use at least one tablet after randomization, and have at least one post-treatment efficacy evaluation. The PPS is a subset of the FAS, and consists of the participants without any major deviations from the study protocol. The participants in the SS are those who use their assigned tablets at least once after randomization.
The FAS will be used for all of the validity analyses, including demographic characteristics and the baseline equilibrium evaluation. The PPS will be used in analyses of the main effectiveness indicators (ie, the primary and secondary outcomes). The safety evaluation will be performed within the SS.
Descriptive statistics will be calculated to examine whether observations have normal distributions. Continuous variables will be summarized as either means and SDs or medians and interquartile ranges. Dichotomous variables will be reported as counts and proportions. Depending on the distribution of the data, continuous variables will be compared using t-tests (when there is homogeneity of variance and a normal distribution) or the Wilcoxon rank sum test. Categorical variables will be compared using the chi-square test or the exact probability method (if the chi-square test is inappropriate). Finally, ranked ordinal data will be analyzed with the Wilcoxon rank sum test. All statistical tests will be two-sided and a P value < 0.05 is considered statistically significant.
AEs, SAEs and Other Adverse Reactions
AEs are defined as any medical adverse experience occurring to a participant during the study, whether or not it is considered to be related to the interventions. All AEs are to be recorded in the eCRF and the causal relationship between the AE and the intervention should be judged by investigators. The investigator should give a corresponding processing to any AE and the AE is to be followed up until resolution or stabilization.
SAEs refer to events that occur during the study that require hospitalization or prolonged hospitalization; are life-threatening; and/or cause disability, incapacity to work, congenital malformation, death or other important medical events. All SAEs are to be recorded and reported to the State Food and Drug Administration, the Health Administration, the Provincial Food and Drug Administration, the Ethics Committee of the local site, and the study sponsor within 24 hours of the investigator becoming aware of it. A follow-up report or a summary report is to be completed when the SAE resolves, reaches a final outcome, or 30 days pass since it first occurred.
Suspected unexpected serious adverse reactions (SUSARs) are defined as unintended and serious adverse reactions that occur in the study that are determined to be related to the interventions (including both the test and the control drugs). All SUSARs are to be recorded and reported to the Ethics Committee of the local center, the Health Administration, and the study sponsor. The follow-up process for SUSARs is the same as that of SAEs. A list that provides an overview of recorded SUSARs will be submitted by the study sponsor to the Ethics Committee at the lead hospital every half year. When a SUSAR is identified, an investigator alert will be issued to all the involved investigators.
In this study, hypoglycemia will be reported separately as an AE of particular concern. Investigators are to train and instruct participants to record hypoglycemic events in time. Investigators will record hypoglycemic events in the eCRF based on their original records and are to deal with the hypoglycemic event as soon as possible after the information is made available. If a hypoglycemic event meets the withdrawal criteria for the study, participants are to terminate their treatment and will be withdrawn from the study.
Participant Withdrawal
Participants are free to withdraw from the study for any reason and at any time. Investigators may also withdraw participants when they meet any of the withdrawal criteria (Figure 4). All the withdrawn cases will be recorded in the eCRF along with the reason for withdrawal. Participants who withdraw will be asked to return for a final safety check as well as to undergo a final laboratory sample collection. If the withdrawal is due to pregnancy or any AE, the participant will be followed until the pregnancy or AE reaches its final outcome.
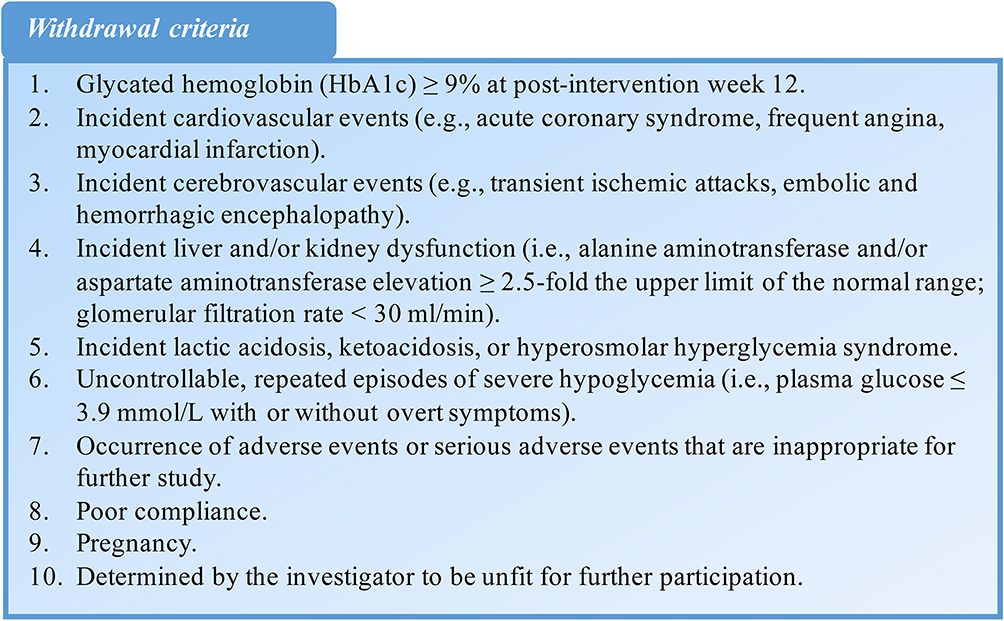 |
Figure 4 The withdrawal criteria of this study. |
Protocol Amendments
Once the study protocol is approved, any modification is to be submitted to the Ethics Committee. Amendments will be tracked in the protocol appendix and the updated version of the protocol will be issued to each site and investigator immediately after its approval.
Ancillary Study
The ancillary study is an exploratory study whose purpose is to assess the effects of pioglitazone/metformin combination therapy and sitagliptin/metformin combination therapy on whole body composition change. It will only be conducted in Chengdu and all of its participants will undergo dual energy x-ray absorptiometry scans at the West China Hospital of Sichuan University.
Dissemination Policy
Upon completion of the trial, each site is to be involved in the publication of manuscripts and presentation of findings at academic conferences with the permission of the study sponsor. Authorship will be determined according to internationally agreed upon authorship criteria. The funding source will be appropriately declared in knowledge translation products. After publication of the primary findings, data requests can be provided to researchers.
Patient and Public Involvement
Patients and/or the public have not and will not be involved in the design, conduction, report, or dissemination plans of this study.
Ethics and Dissemination
The study will adhere to the principles of the Declaration of Helsinki (latest version WMA General Assembly 2013, Fortaleza) and the GCP. This protocol is approved by the Ethics Committee at the West China Hospital of Sichuan University (as the lead center for the trial), whose reference number is 2018 Clinical Trial (Marketing) Review (12). This study is registered in the Chinese Clinical Trial Registry (registration number: ChiCTR1900021861). Results will be published in peer-reviewed journals and disseminated at academic conferences.
Consent
This study’s informed consent process was approved by the Ethics Committee and adheres to GCP. The informed consent form introduces the study purpose, steps and process; participants’ rights and obligations; the benefits and risks; possible compensation; and confidentiality. A physician on the research team will obtain written informed consent from potentially eligible participants at the beginning of the study. If important new information about the study drugs is observed, an amendment to the informed consent must be submitted to and approved by the Ethics Committee, after which the physician is to obtain the new signed consents from all of the enrolled participants.
Author Contributions
All authors made substantial contributions to conception and design and acquisition of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
This trial is funded by the Hangzhou Zhongmei Huadong Pharmaceutical Co., Ltd and the 1-3-5 Project for Disciplines of Excellence in West China Hospital of Sichuan University. This work is also funded by Sichuan Provincial Science and Technology Foundation (Grant number 2021YJ0441). The funding bodies have not and will not participate in the study design, the collection, management, analysis or interpretation of data, nor writing the findings for publication.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Xu Y, Wang L, He J, et al. Prevalence and control of diabetes in Chinese adults. JAMA. 2013;310(9):948–959. doi:10.1001/jama.2013.168118
2. Kodama K, Tojjar D, Yamada S, et al. Ethnic differences in the relationship between insulin sensitivity and insulin response: a systematic review and meta-analysis. Diabetes Care. 2013;36(6):1789–1796. doi:10.2337/dc12-1235
3. Ahuja V, Kadowaki T, Evans RW, et al. Comparison of HOMA-IR, HOMA-β% and disposition index between US white men and Japanese men in Japan: the ERA JUMP study. Diabetologia. 2015;58(2):265–271. doi:10.1007/s00125-014-3414-6
4. Wang T, Lu J, Shi L, et al. Association of insulin resistance and β-cell dysfunction with incident diabetes among adults in China: a nationwide, population-based, prospective cohort study. Lancet Diabetes Endocrinol. 2020;8(2):115–124. doi:10.1016/S2213-8587(19)30425-5
5. Garber AJ, Abrahamson MJ, Barzilay JI, et al. Consensus statement by the American Association of Clinical Endocrinologists and American College of Endocrinology on the comprehensive type 2 diabetes management algorithm - 2018 Executive Summary. Endocr Pract. 2018;24(1):91–120.
6. Jia W, Weng J, Zhu D, et al. Standards of medical care for type 2 diabetes in China 2019. Diabetes Metab Res Rev. 2019;35(6):e3158. doi:10.1002/dmrr.3158
7. UK Prospective Diabetes Study (UKPDS) Group. Effect of intensive blood‐glucose control with metformin on complications in overweight patients with type 2 diabetes (UKPDS 34). Lancet. 1998;352:
8. Hong J, Zhang Y, Lai S, et al. Effects of metformin versus glipizide on cardiovascular outcomes in patients with type 2 diabetes and coronary artery disease. Diabetes Care. 2013;36(5):1304–1311. doi:10.2337/dc12-0719
9. Lu ZH, Pan CY, Gao Y, et al. A randomized, double blind, placebo-controlled, parallel and multicenter study to evaluate the safety and efficacy of pioglitazone with sulphonylurea in type 2 diabetic patients. Zhonghua Nei Ke Za Zhi. 2011;50(10):826–830.
10. Pan C, Gao Y, Gao X, et al. The efficacy and safety of pioglitazone hydrochloride in combination with sulphonylureas and metfomin in the treatment of type 2 diabetes mellitus a 12-week randomized multi-centres placebo-controlled parallel study. Zhonghua Nei Ke Za Zhi. 2002;41(6):388–392.
11. Dormandy JA, Charbonnel B, Eckland DJ, et al. Secondary prevention of macrovascular events in patients with type 2 diabetes in the PROactive Study (PROspective pioglitAzone Clinical Trial In macroVascular Events): a randomised controlled trial. Lancet. 2005;366:1279–1289. doi:10.1016/S0140-6736(05)67528-9
12. Kernan WN, Viscoli CM, Furie KL, et al. Pioglitazone after ischemic stroke or transient ischemic attack. N Engl J Med. 2016;374(14):1321–1331. doi:10.1056/NEJMoa1506930
13. Kodama N, Tahara N, Tahara A, et al. Effects of pioglitazone on visceral fat metabolic activity in impaired glucose tolerance or type 2 diabetes mellitus. J Clin Endocrinol Metab. 2013;98(11):4438–4445. doi:10.1210/jc.2013-2920
14. Bi Y, Zhang B, Xu W, et al. Effects of exenatide, insulin, and pioglitazone on liver fat content and body fat distributions in drug-naive subjects with type 2 diabetes. Acta Diabetol. 2014;51(5):865–873. doi:10.1007/s00592-014-0638-3
15. Ji L, Han P, Wang X, et al. Randomized clinical trial of the safety and efficacy of sitagliptin and metformin co-administered to Chinese patients with type 2 diabetes mellitus. J Diabetes Investig. 2016;7(5):727–736. doi:10.1111/jdi.12511
16. Mohan V, Yang W, Son HY, et al. Efficacy and safety of sitagliptin in the treatment of patients with type 2 diabetes in China, India, and Korea. Diabetes Res Clin Pract. 2009;83(1):106–116. doi:10.1016/j.diabres.2008.10.009
17. Yang W, Guan Y, Shentu Y, et al. The addition of sitagliptin to ongoing metformin therapy significantly improves glycemic control in Chinese patients with type 2 diabetes. J Diabetes. 2012;4(3):227–237. doi:10.1111/j.1753-0407.2012.00213.x
18. Green JB, Bethel MA, Armstrong PW, et al. Effect of sitagliptin on cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2015;373(3):232–242. doi:10.1056/NEJMoa1501352
19. Yan J, Yao B, Kuang H, et al. Liraglutide, sitagliptin, and insulin glargine added to metformin: the effect on body weight and intrahepatic lipid in patients with type 2 diabetes mellitus and nonalcoholic fatty liver disease. Hepatology. 2019;69(6):2414–2426. doi:10.1002/hep.30320
20. Del Prato S, Chilton R. Practical strategies for improving outcomes in T2DM: the potential role of pioglitazone and DPP4 inhibitors. Diabetes Obes Metab. 2018;20(4):786–799. doi:10.1111/dom.13169
21. Russell-Jones D, Cuddihy RM, Hanefeld M, et al. Efficacy and safety of exenatide once weekly versus metformin, pioglitazone, and sitagliptin used as monotherapy in drug-naive patients with type 2 diabetes (DURATION-4): a 26-week double-blind study. Diabetes Care. 2012;35(2):252–258. doi:10.2337/dc11-1107
22. Bergenstal RM, Wysham C, Macconell L, et al. Efficacy and safety of exenatide once weekly versus sitagliptin or pioglitazone as an adjunct to metformin for treatment of type 2 diabetes (DURATION-2): a randomised trial. Lancet. 2010;376(9739):431–439. doi:10.1016/S0140-6736(10)60590-9
23. Hsia SH, Navar MD, Duran P, et al. Sitagliptin compared with thiazolidinediones as a third-line oral antihyperglycemic agent in type 2 diabetes mellitus. Endocr Pract. 2011;17(5):691–698. doi:10.4158/EP10405.OR
24. Liu SC, Chien KL, Wang CH, et al. Efficacy and safety of adding pioglitazone or sitagliptin to patients with type 2 diabetes insufficiently controlled with metformin and a sulfonylurea. Endocr Pract. 2013;19(6):980–988. doi:10.4158/EP13148.OR
25. Jameshorani M, Sayari S, Kiahashemi N, et al. Comparative study on adding pioglitazone or sitagliptin to patients with type 2 diabetes mellitus insufficiently controlled with metformin. Open Access Maced J Med Sci. 2017;5(7):955–962. doi:10.3889/oamjms.2017.193
26. Chawla S, Kaushik N, Singh NP, et al. Effect of addition of either sitagliptin or pioglitazone in patients with uncontrolled type 2 diabetes mellitus on metformin: a randomized controlled trial. J Pharmacol Pharmacother. 2013;4(1):27–32. doi:10.4103/0976-500X.107656
27. Bae J, Kim G, Lee YH, et al. Differential effects of thiazolidinediones and dipeptidyl peptidase-4 inhibitors on insulin resistance and β-cell function in type 2 diabetes mellitus: a propensity score-matched analysis. Diabetes Ther. 2019;10(1):149–158. doi:10.1007/s13300-018-0541-y
28. Lu J, Zang J, Li H. Impact of three oral antidiabetic drugs on markers of β-cell function in patients with type 2 diabetes: a meta-analysis. PLoS One. 2013;8(10):e76713. doi:10.1371/journal.pone.0076713
29. Ohki T, Isogawa A, Iwamoto M, et al. The effectiveness of liraglutide in nonalcoholic fatty liver disease patients with type 2 diabetes mellitus compared to sitagliptin and pioglitazone. Sci World J. 2012;2012:496453. doi:10.1100/2012/496453
30. Han M, Qin P, Li Q, et al. Chinese visceral adiposity index: a reliable indicator of visceral fat function associated with risk of type 2 diabetes. Diabetes Metab Res Rev. 2020;e3370.
31. Wang H, Zhai F. Options for preventing obesity in China. Obes Rev. 2013;14:134–140. doi:10.1111/obr.12106
32. Yabiku K, Mutoh A, Miyagi K, et al. Effects of oral antidiabetic drugs on changes in the liver-to-spleen ratio on computed tomography and inflammatory biomarkers in patients with type 2 diabetes and nonalcoholic fatty liver disease. Clin Ther. 2017;39(3):558–566. doi:10.1016/j.clinthera.2017.01.015
33. Chan AW, Tetzlaff JM, Gøtzsche PC, et al. SPIRIT 2013 explanation and elaboration: guidance for protocols of clinical trials. BMJ. 2013;346:e7586. doi:10.1136/bmj.e7586
34. World Health Organization. Definition, Diagnosis and Classification of Diabetes Mellitus and Its Complications; Part 1: Diagnosis and Classification of Diabetes Mellitus. Geneva: Department of Noncommunicable Disease Surveillance; 1999.
35. National Medical Products Administration. Guidelines for clinical trials of drugs and biological products for the treatment of diabetes. National Food and Drug Administration Note [2012] No. 122. 2012.
36. Chow SC, Shao J, Wang H, et al. Sample Size Calculations in Clinical Research.
37. European Medicines Agency. ICH E9: Statistical Principles for Clinical Trials. 1998.
38. Lee RC, Wang ZM, Heymsfield SB. Skeletal muscle mass and aging: regional and whole body measurement methods. Can J Appl Physiol. 2001;26:102–122. doi:10.1139/h01-008
39. Chen LK, Liu LK, Woo J, et al. Sarcopenia in Asia: consensus report of the Asian Working Group for Sarcopenia. J Am Med Dir Assoc. 2014;15(2):95–101. doi:10.1016/j.jamda.2013.11.025
40. Cui J, Philo L, Nguyen P, et al. Sitagliptin vs. placebo for non-alcoholic fatty liver disease: a randomized controlled trial. J Hepatol. 2016;65(2):369–376. doi:10.1016/j.jhep.2016.04.021
41. Teranishi T, Ohara T, Maeda K, et al. Effects of pioglitazone and metformin on intracellular lipid content in liver and skeletal muscle of individuals with type 2 diabetes mellitus. Metabolism. 2007;56(10):1418–1424. doi:10.1016/j.metabol.2007.06.005
42. Tushuizen ME, Bunck MC, Pouwels PJ, et al. Pancreatic fat content and beta-cell function in men with and without type 2 diabetes. Diabetes Care. 2007;30(11):2916–2921. doi:10.2337/dc07-0326
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.