Back to Journals » Clinical Interventions in Aging » Volume 17
Comparison Between Percutaneous Endoscopic Gastrostomy and Nasogastric Feeding in 160 Patients with Swallowing Disturbances: A Two-Year Follow-Up Study
Authors Du G, Liu F, Ma X, Chen S, Dai M, Wei L, Liu Z
Received 21 September 2022
Accepted for publication 24 November 2022
Published 5 December 2022 Volume 2022:17 Pages 1803—1810
DOI https://doi.org/10.2147/CIA.S389891
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Ge Du, Fangfang Liu, Xiaomin Ma, Shanshan Chen, Min Dai, Li Wei,* Zishuang Liu*
Department of Rehabilitation Center for Elderly, Beijing Rehabilitation Hospital Affiliated to Capital Medical University, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Li Wei; Zishuang Liu, Department of Rehabilitation Center for Elderly, Beijing Rehabilitation Hospital Affiliated to Capital Medical University, Beijing, 100144, People’s Republic of China, Tel/Fax + 86-010-56981582, Email [email protected]; [email protected]
Purpose: We retrospectively compared the complications, blood biochemical indexes and outcomes in patients with swallowing disturbances receiving nasogastric tube (NGT) feeding and percutaneous endoscopy gastrostomy (PEG).
Methods: Among 160 patients, 72 cases received PEG and 88 cases received NGT. All patients were followed up for two years. We collected their clinical data from the medical records. Indicators, such as body mass index (BMI), white blood cell (WBC), hemoglobin (HGB), complications, including recurrent aspiration pneumonia, gastrointestinal bleeding, reflux esophagitis, and outcomes (survival or death) were compared between the two groups semi-annually.
Results: SAt both six months and one year after receiving treatment, there was no statistical difference between the two groups in indicators, complications and outcomes, with all P > 0.05. It can be seen that, when the patients were followed up for one and a half years18 months, ALB was lower in the NGT group (33.81± 0.46) compared with the PEG group (36.14± 0.50) (P < 0.05). After two years of follow-up, differences between the NGT and PEG group could be seen in a variety of indicators, including BMI (20.08± 0.27 vs 21.03± 0.25), WBC (9.12± 0.56 vs 7.08± 0.29), ALB (33.11± 0.43 vs 35.75± 0.49), creatinine (55.07± 1.83 vs 63.21± 2.94), and the complications, such as aspiration pneumonia, gastrointestinal bleeding, reflux esophagitis, and electrolyte disorder, in the PEG group were significantly reduced compared to the NGT groupthan that in its counterpart, P < 0.05. In the two-year follow-up period, there were 13 and 22 patients died in the PEG group and NGT group, respectively.
Conclusion: Both techniques are safe and effective in the short term. However, on a longer-term basis, PEG is shown to be superior to NGT feeding in improving nutrition and preventing common complications for patients with swallowing disturbances.
Keywords: percutaneous endoscopy gastrostomy, nasogastric tube feeding, swallowing disturbances, two-year, follow-up
Introduction
Patients, who are under the conditions related with swallowing disorders such as dementia, stroke, neurological diseases, head or neck cancers, physical obstruction, can develop low nutrition affecting their recovery from surgery, injury or illness.1 Data showed that dysphagia occurs in 11–14% of community-dwelling older people, 13–15% of old patients with pneumonia and 35–69% of stroke patients.2 For patients at nutritional risk or malnourished who cannot meet their nutrient requirements by normal dietary intake, who have a functioning gastrointestinal tract, enteral feeding is essential way and is recommended by European Society for Clinical Nutrition and Metabolism (ESPEN) to provide nutritional support to meet metabolic requirements.3 In clinic, a tube is frequently used to insert into the stomach of somebody who cannot eat, and this is called enteral tube feeding. The tube could be inserted into the stomach through a small cut in patients’ belly, or pass through their nose into their stomach.4,5 These two ways are called percutaneous endoscopy gastrostomy (PEG) and nasogastric tube (NGT) feeding, and both of them are commonly-used, effective techniques to provide nutritional support.6
NGT feeding seems to maintain enteral immunity and prevent bacterial translocation since it refers to intake of food through the gastrointestinal tract via a tube.7 However, it has been found to be associated with swallowing dysfunction, pain discomfort, and a higher risk for patients who have problems to remove the tube.8 Moreover, the benefits of NGT feeding in older individuals with eating disorders are controversial. Some research indicated that it could improve their nutritional status and increase survival rate.9 Some other retrospective observational studies reported NGT increases physical suffering while offering no benefits in survival, nutritional status and other complications.10 PEG, which is the most common endoscopic procedure performed worldwide, is a route preferred for patients with a functional gastrointestinal system. Although generally considered to be safe, having well-known advantages, there are still minor and major short-term and long-term complications of this technique. Minor complications reported include wound infection, tube leakage to abdominal cavity, stoma leakage, tube blockage, gastric outlet obstruction, etc. Meanwhile, major complications, such as aspiration pneumonia, hemorrhage, buried bumper syndrome, perforation of bowel, are not common but can also occur after PEG tube insertion.11 At present, there are few comparative studies on the long-term effects of the two methods in patients with intake disorders.
In this study, we compared complications, indications and outcomes of these two techniques in 160 patients with swallowing disturbances observed at 6, 12, 18, and 24 months, respectively.
Materials and Methods
Subjects
We retrospectively analyzed the clinical data of all 670 patients admitted to our hospital from January 2019 to June 2020 and received enteral nutritional support (NGT or PEG); 160 cases were then recruited for further analysis. Inclusion criteria were: (1) nutrition support time of tube feeding was more than six months and (2) the clinical data were well-documented in the follow-up period. Exclusion criteria were: (1) congenital or acquired organic gastrointestinal diseases, (2) severe liver and kidney dysfunction, and (3) severe metabolic diseases. Among 160 patients, 88 cases received NGT and 72 cases received PEG and were named NGT and PEG group, respectively.
NGT Feeding
The patient was in sitting or lying position, with head back slightly. After checking and cleaning the patient’s nasal cavity with a wet cotton swab, the operator dragged the gastric tube with gauze in his left hand, and clamped the front end of the gastric tube with vascular forceps in his right hand to measure the length of the intubation. For adults, it is 45–55 cm. The gastric tube was marked by adhesive tape and lubricated, then was slowly pushed along one of the patient’s nostrils. The patient was instructed to swallow when the gastric tube was 14 to 16 cm deep. If the patient had choking and dyspnea, considering it entering into the trachea by mistake, the operator should pull out the gastric tube immediately. When the gastric tube reached its expected depth, it was fixed on the nasal wing and cheek with adhesive tape.
Peg
Before operation, fasting time for the patient should be more than 6 hours. He or she was placed in the supine position with his or her head to the left, then was given propofol intravenously under ECG monitoring. Firstly, the gastroscope was performed to observe the structure, mucosa of stomach and duodenum, and inflate the stomach to make it fill and expand until its wall and the abdominal wall were close together. The endoscopist observed the gastroscope light through the abdominal wall, moved the gastroscope light to the rear of the proposed fistula position, and selected the puncture point at the anterior wall of the junction of the antral body to avoid the area with abundant blood vessels as far as possible. Then, the puncture site was sterilized, a paved sterile sheet was applied and local infiltration anesthesia was performed. The operator made a 0.5–1.0 cm incision on the skin of the puncture site, slowly entered the gastric cavity with the injection needle, withdrew the injection needle, took the trocar and punctured it into the gastric cavity through the abdominal wall, put the guide wire into the gastric cavity and put the snare into the stomach through the live inspection hole of the gastroscope. Next, the endoscopist grasped the guide wire and pulled it out, together with the gastroscope. After connecting the guide wire with the gastrostomy tube, the guide wire was pulled from the abdominal wall to make the gastrostomy tube enter the stomach through the esophagus. The gastroscope was inserted into the stomach again to observe the situation of the gastrostomy tube. In the last step, gastrostomy tube was fixed after the disc in the stomach was closely fitted with the stomach wall, gastrostomy tube disc and the abdominal wall was kept in a slight tension state. All patients underwent routine CT scanning after PEG to ensure successful catheterization.
Follow-Up and Data Collection
After the operation, all the patients were hospitalized at least every six months for swallowing function test and nutritional status assessment. The blood tests were done immediately after the patient was admitted to our department. The height was identified by a tape measure in the patient’s supine position, and the weight was checked by a bed with a scale. We made a diagnosis of reflux esophagitis by the symptoms of acid regurgitation and heartburn. Gastrointestinal bleeding was diagnosed by positive fecal occult blood test. We collected their clinical data from the medical record for two years. Indicators, such as body mass index (BMI), white blood cell (WBC), hemoglobin (HGB), platelet (PLT), albumin (ALB), creatinine, blood urea nitrogen (BUN), C-reactive protein, complications including aspiration pneumonia, gastrointestinal bleeding, reflux esophagitis, etc., and outcomes (survival or death) were compared between two groups semi-annually. If the patient was not admitted on time, the charge nurse in our department would connect with him or her family members and found out the reason. It should be noted that the cases of death in short-time follow-up was also calculated as the death cases in the next round of follow-up. For example, if the patient died in one half of the year, he or she could also be calculated as a case of death in every semi-annual follow-up. Our study, with the protection of privacy and no harm for the rights of patients, was conducted according to the principles of the Declaration of Helsinki. Informed consents were obtained from all the participants.
Statistical Analysis
We selected Microsoft Excel for data collecting and used the SPSS 26.0 statistical package for data analysis. The measurement data were expressed as mean ± standard deviation and the student’s t-test was used to evaluate the two groups’ differences with normally distributed variables. For those data not meeting the normal distribution, Mann–Whitney U-test was performed. The count data were expressed as numbers and percentages (%), and the chi-square test was adopted to compare variables between the two groups. We used a continuity-adjusted formula for the chi-square test if the value of expected cases in one cell was ≥1 but <5. If a cell had few expected cases (i.e.,< 1) in the table, Fisher’s exact test was used. A two-tailed P<0.05 was considered statistically significant.
Results
Population Characteristics
A total of 160 patients who had swallowing disturbance were recruited in our study: 72 cases receiving PEG and 88 patients undertaking NGT. They were defined as PEG group and NGT group, respectively. Table 1 compares the demographic and clinical details of the study populations. The mean age of PEG group was 76.44±1.95 years, having no significant difference from that of NGT group (73.79±1.90 years); P >0.05. Men accounted for 66.7% and 59.1% in the two groups, respectively, and there was no statistical significance (P >0.05). As shown in Table 1, basic diseases of patients in both groups were cerebral infarction, cerebral hemorrhage, Alzheimer’s disease, brain injury, brain tumor, Parkinson’s disease, myasthenia gravis, ischemic hypoxic encephalopathy (P >0.05). We have not found any significant differences between the two groups in terms of other demographic information, including smoking status, place of residence, age-adjusted Charlson Comorbidity Index (aCCI), marital status, and selected laboratory indicators.
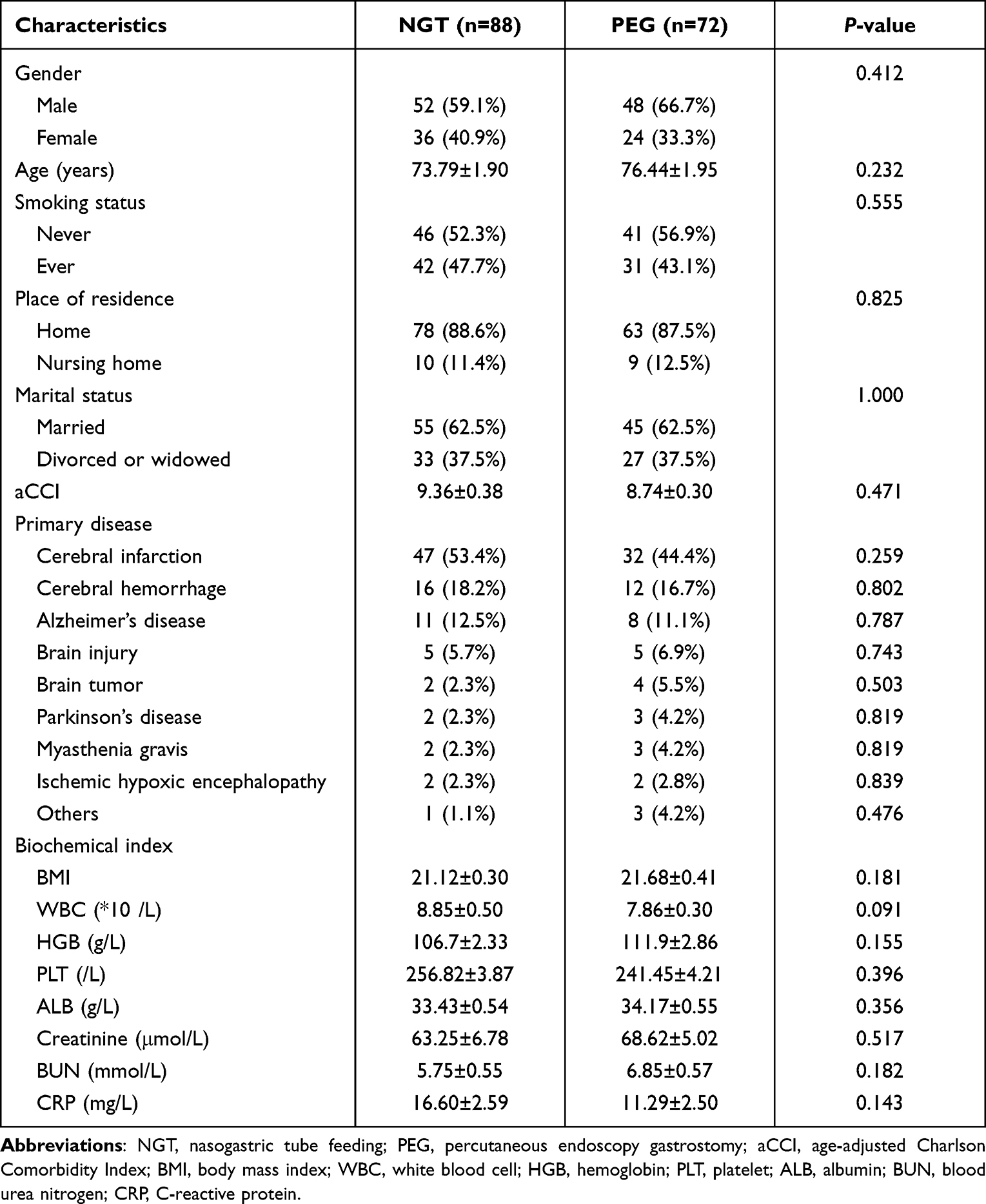 |
Table 1 Baseline Demographic and Clinical Characteristics of Patients in the Two Groups |
Semi-Annual Follow-Up
Table 2 gives us the information that when the patients were followed up at both six months and one year after receiving treatment, there was no statistical difference between two groups in indicators, complications and outcomes, with all P >0.05. At the time of being followed up for 18 months, it could be seen that the indicator of ALB of PEG group (36.14±0.50) was higher than that of NGT group (33.81±0.46). Besides that, patients had similar possibility to have complications in two group statistically, including pneumonia, gastrointestinal bleeding, reflux esophagitis, electrolyte disorder, with all P >0.05. When all the patients were followed up at two years, obvious differences of some indicators and complications could be seen in the two groups Specifically, BMI (21.03±0.25), ALB (35.75±0.49) and creatinine (63.21±2.94) were higher in PEG group than those in NGT group (20.08±0.27, 33.11±0.43, 55.07±1.83), while WBC was markedly decreased in PEG group (7.08±0.29 vs 9.12±0.56). Meanwhile, complications of patients, such as aspiration pneumonia (40.3%), gastrointestinal bleeding (26.4%), reflux esophagitis (27.8%), electrolyte disorder (43.1%) in PEG group were significantly reduced compared with those in NGT group (56.8%, 43.2%, 47.7%, 59.1%), with all P <0.05. In addition to that, 13 and 22 patients died of complications in PEG and NGT groups, respectively, during the two-year follow-up period.
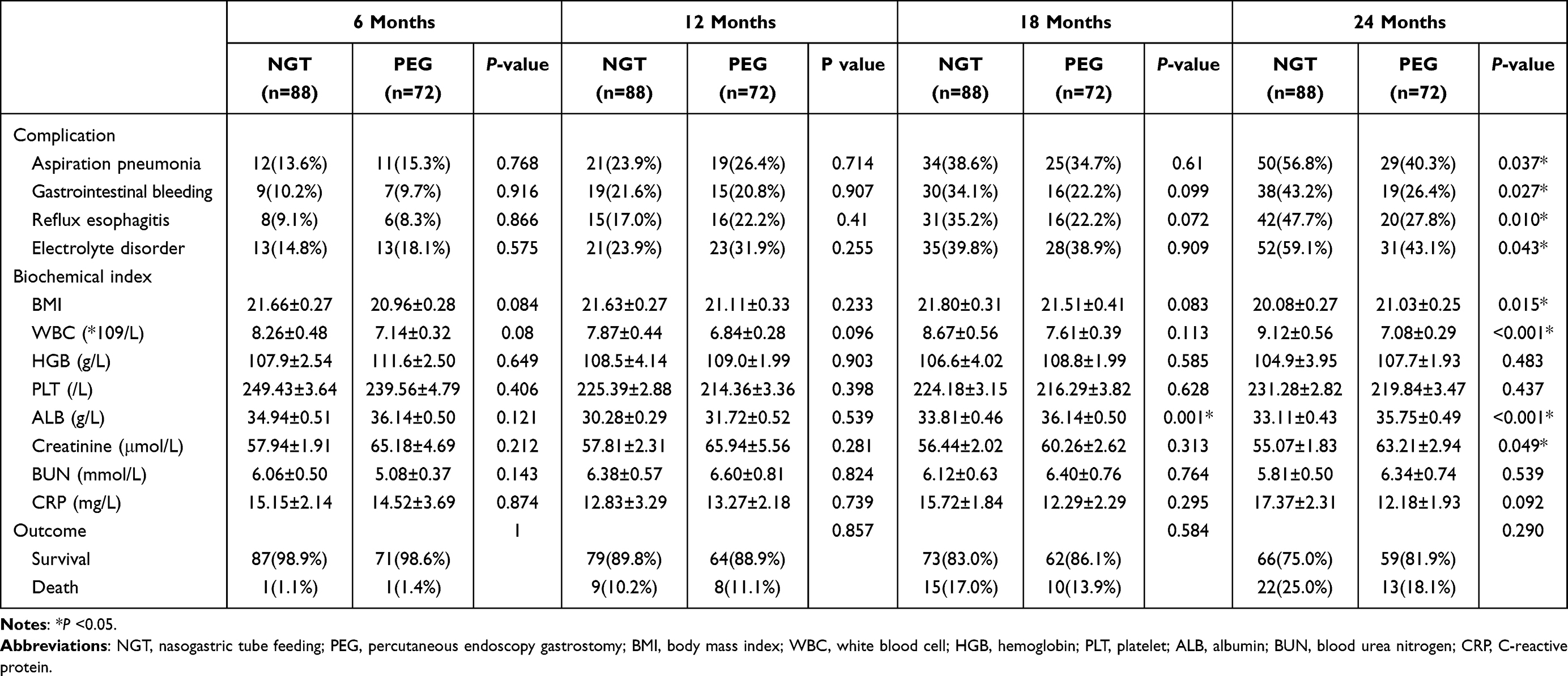 |
Table 2 Comparison of Complications, Blood Biochemical Index and Outcomes in the Two Groups Postoperatively Every Six Months |
Discussion
NGT feeding is a very common method of enteral nutrition. Although it is effective, it also brings a variety of difficulties and complications when applied in clinic.12 PEG, as another technique commonly used by clinicians, was first introduced in 1980 by the application of endoscopy to insert a feeding tube into the stomach.13 Its whole procedure is easy, associated with low morbidity and mortality.14 Many previous studies have compared the advantages and disadvantages of the two techniques. Baeten et al recruited 90 patients in their study, of whom 44 were randomized to the NGT group and 44 to the PEG group. The primary diseases for these patients were neoplasia of the ear, nose, throat and neurologic or post-operative diseases, and their mean age was 72 years.15 In another study, investigators only included patients with dysphagia secondary to neurologic diseases in their sample. The mean age of the patients in PEG group was 56 years, whereas the mean age of those in NGT group was 65 years.16 Follow-up time of these two studies was no more than four weeks. Two studies in 2006 and 2008 included patients with dysphagia after acute stroke with a median age of 65 years and patients with head or neck cancer with a median age of 60 years.17,18 Compared with these previous studies, patients included in our sample had more basic diseases, higher mean age and longer follow-up time. This may suggest that the indications of enteral nutrition have widened in recent years. The outcome of aspiration pneumonia was examined in seven studies from 1992 to 2008 and data showed that 106 out of 332 cases (31.93%) had pneumonia in the PEG group and 130 out of 313 patients (41.54%) in the NGT group.15,19–22 However, the results of a meta-analysis did not favor PEG in the outcome of pneumonia.23 For other complications, like reflux esophagitis, a study in 2001 analyzed 82 patients in total and data showed PEG was obviously better than NGT in reducing it.24 Additionally, three researches in 1996, 2008 and 2012 analyzed weight (kg) in patients with swallowing disturbance, while the result favored neither NGT or PEG.18,21,22 Two studies in 2001 and 2012, nevertheless, reported that serum albumin levels and hemoglobin were higher in PEG group than in NGT group.22,24 Our data showed that there were no significant differences between NGT and PEG within one year. These results attributed to NGT could be effective for nutrition for a short time, while PEG, which could be considered a surgical strike for patients, may cause body stress reaction and thus could not show advantage in nutrition support in a short time. Along with time extension, the stimulation of the nasal feeding tube to the gastrointestinal tract becomes worse, resulting in more obviously adverse reactions, while, after organism adaptation, PEG becomes a better choice because it is more efficient, less invasive, and more suitable to meet the physiological requirements.25 After two years of follow-up, it can still be seen that the mortality rate was higher in NGT group (25.0%) though it is not statistically significant, and most patients died of serious complications and underlying disease itself. The outcome of mortality was examined in nine previous studies (644 cases in total); most of the follow-up time in these studies was shorter than ours, and data indicated that 118 out of 330 participants (35.76%) died in the PEG group and 115 out of 330 participants (36.62%) died in the NGT group.23 Since these studies were carried out earlier, this inconformity may be caused by differences in basic diseases and the quality of long-term care obtained by the participants.
Although PEG is a well-established technique for providing nutrition in malnourished patients, many clinical workers still have limited understanding about this operation. A survey conducted in China indicated that only 8% of oncologists had a high level of knowledge about this method; one of the main reasons for those participants not choosing PEG was unfamiliarity with it or cost of the method.26
There are also some limitations in our study. Concerning ethics, it is not possible to carry out a randomized controlled trial in clinic. NGT or PEG was conducted according to the patients’ or their family members’ wishes. On the other hand, the sample in our study is relatively small; cases with some primary diseases were less than ten.
Conclusions
Our experiments identify that, in the short term, both PEG and NGT are safe and effective. On a longer-term basis, however, PEG is superior to NGT feeding in terms of improving nutrition and preventing common complications for patients. Thus, for those patients with swallowing disturbances who need longer-term enteral nutrition, PEG could be a preferred method. In future, we expect to include more samples with a wider variety of primary diseases for longer follow-up times to confirm this conclusion.
Ethics Approval and Consent to Participate
The protocols were approved by the Institutional Review Boards of Beijing Rehabilitation Hospital Affiliated to Capital Medical University, and informed consent of confirmation that this study complied with all regulations has been obtained. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests.
References
1. Christmas C, Rogus-Pulia N. Swallowing disorders in the older population. J Am Geriatr Soc. 2019;67(12):2643–2649. PMID: 31430395; PMCID: PMC7102894. doi:10.1111/jgs.16137
2. Jaafar MH, Mahadeva S, Tan KM, et al. Long-term nasogastric versus percutaneous endoscopic gastrostomy tube feeding in older asians with dysphagia: a pragmatic study. Nutr Clin Pract. 2019;34(2):280–289. PMID: 30251336. doi:10.1002/ncp.10195
3. Bischoff SC, Austin P, Boeykens K, et al. ESPEN guideline on home enteral nutrition. Clin Nutr. 2020;39(1):5–22. PMID: 31255350. doi:10.1016/j.clnu.2019.04.022
4. Gosa MM, Carden HT, Jacks CC, Threadgill AY, Sidlovsky TC. Evidence to support treatment options for children with swallowing and feeding disorders: a systematic review. J Pediatr Rehabil Med. 2017;10(2):107–136. PMID: 28582883. doi:10.3233/PRM-170436
5. Rowat A. Enteral tube feeding for dysphagic stroke patients. Br J Nurs. 2015;24(3):142–145. doi:10.12968/bjon.2015.24.3.138
6. Ojo O, Brooke J. The use of enteral nutrition in the management of stroke. Nutrients. 2016;8(12):827. PMID: 27999383; PMCID: PMC5188480. doi:10.3390/nu8120827
7. Sánchez-Sánchez E, Ruano-álvarez MA, Díaz-Jiménez J, Díaz AJ, Ordonez FJ. Enteral nutrition by nasogastric tube in adult patients under palliative care: a systematic review. Nutrients. 2021;13(5):1562. PMID: 34066386; PMCID: PMC8148195. doi:10.3390/nu13051562
8. Beavan J, Conroy SP, Harwood R, et al. Does looped nasogastric tube feeding improve nutritional delivery for patients with dysphagia after acute stroke? A randomised controlled trial. Age Ageing. 2010;39(5):624–630. PMID: 20667840. doi:10.1093/ageing/afq088
9. Wang H, Huang C, Yang Y, Kong L, Zheng X, Shan X. Cost-effectiveness analysis of nasojejunal tube feeding for the prevention of pneumonia in adults who are critically ill. JPEN J Parenter Enteral Nutr. 2022;46(5):1167–1175. PMID: 34751960. doi:10.1002/jpen.2302
10. Ho KM, Dobb GJ, Webb SA. A comparison of early gastric and post-pyloric feeding in critically ill patients: a meta-analysis. Intensive Care Med. 2006;32(5):639–649. PMID: 16570149. doi:10.1007/s00134-006-0128-3
11. Rahnemai-Azar AA, Rahnemaiazar AA, Naghshizadian R, Kurtz A, Farkas DT. Percutaneous endoscopic gastrostomy: indications, technique, complications and management. World J Gastroenterol. 2014;20(24):7739–7751. PMID: 24976711; PMCID: PMC4069302. doi:10.3748/wjg.v20.i24.7739
12. Abunnaja S, Cuviello A, Sanchez JA. Enteral and parenteral nutrition in the perioperative period: state of the art. Nutrients. 2013;5(2):608–623. PMID: 23429491; PMCID: PMC3635216. doi:10.3390/nu5020608
13. Gauderer MW, Ponsky JL, Izant RJ
14. Fugazza A, Capogreco A, Cappello A, et al. Percutaneous endoscopic gastrostomy and jejunostomy: indications and techniques. World J Gastrointest Endosc. 2022;14(5):250–266. PMID: 35719902; PMCID: PMC9157691. doi:10.4253/wjge.v14.i5.250
15. Baeten C, Hoefnagels J. Feeding via nasogastric tube or percutaneous endoscopic gastrostomy. A comparison. Scand J Gastroenterol Suppl. 1992;194:95–98. doi:10.3109/00365529209096035
16. Park RH, Allison MC, Lang J, et al. Randomised comparison of percutaneous endoscopic gastrostomy and nasogastric tube feeding in patients with persisting neurological dysphagia. BMJ. 1992;304(6839):1406–1409. PMID: 1628013; PMCID: PMC1882203. doi:10.1136/bmj.304.6839.1406
17. Hamidon BB, Abdullah SA, Zawawi MF, Sukumar N, Aminuddin A, Raymond AA. A prospective comparison of percutaneous endoscopic gastrostomy and nasogastric tube feeding in patients with acute dysphagic stroke. Med J Malaysia. 2006;61(1):59–66. PMID: 16708735.
18. Corry J, Poon W, McPhee N, et al. Randomized study of percutaneous endoscopic gastrostomy versus nasogastric tubes for enteral feeding in head and neck cancer patients treated with (chemo)radiation. J Med Imaging Radiat Oncol. 2008;52(5):503–510. PMID: 19032398. doi:10.1111/j.1440-1673.2008.02003.x
19. Dennis M, Lewis S, Cranswick G, Forbes J. FOOD Trial Collaboration. FOOD: a multicentre randomised trial evaluating feeding policies in patients admitted to hospital with a recent stroke. Health Technol Assess. 2006;10(2):iii–iv, ix–x, 1–120. doi:10.3310/hta10020
20. Douzinas EE, Tsapalos A, Dimitrakopoulos A, Diamanti-Kandarakis E, Rapidis AD, Roussos C. Effect of percutaneous endoscopic gastrostomy on gastro-esophageal reflux in mechanically-ventilated patients. World J Gastroenterol. 2006;12(1):114–118. PMID: 16440428; PMCID: PMC4077500. doi:10.3748/wjg.v12.i1.114
21. Norton B, Homer-Ward M, Donnelly MT, Long RG, Holmes GK. A randomised prospective comparison of percutaneous endoscopic gastrostomy and nasogastric tube feeding after acute dysphagic stroke. BMJ. 1996;312(7022):13–16. PMID: 8555849; PMCID: PMC2349687. doi:10.1136/bmj.312.7022.13
22. Sadasivan A, Faizal B, Kumar M. Nasogastric and percutaneous endoscopic gastrostomy tube use in advanced head and neck cancer patients: a comparative study. J Pain Palliat Care Pharmacother. 2012;26(3):226–232. PMID: 22973911. doi:10.3109/15360288.2012.702199
23. Gomes CA, Andriolo RB, Bennett C, et al. Percutaneous endoscopic gastrostomy versus nasogastric tube feeding for adults with swallowing disturbances. Cochrane Database Syst Rev. 2015;2015(5):CD008096. PMID: 25997528; PMCID: PMC6464742. doi:10.1002/14651858.CD008096.pub4
24. Yata M, Date K, Miyoshi H, Matsuo N, Nishida M, Harima T. Comparison between nasogastric tube feeding and percutaneous endoscopic gastrostomy feeding a long-term randomized controlled study. Gastrointest Endosc. 2001;53:5.
25. Zhukhovitskaya A, Weiland DJ, Goshtasbi K, Verma SP. Is nasogastric tube feeding necessary after hypopharyngeal diverticulum surgery? Am J Otolaryngol. 2020;41(3):102453. PMID: 32199712. doi:10.1016/j.amjoto.2020.102453
26. Fan L, Li J, Xiang M, et al. Attitudes of radiation oncologists to percutaneous endoscopic gastrostomy in patients with head and neck cancer and eating difficulties: a survey in China. J Int Med Res. 2018;46(5):1709–1716. PMID: 29512428; PMCID: PMC5991233. doi:10.1177/0300060518756244
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.