Back to Journals » Journal of Multidisciplinary Healthcare » Volume 14
Comparison Between Healthcare Professionals and the General Population on Parameters Related to Natural Remedies Used During the COVID-19 Pandemic
Authors Alotiby A ![]() , Alshareef M
, Alshareef M ![]()
Received 11 October 2021
Accepted for publication 15 December 2021
Published 24 December 2021 Volume 2021:14 Pages 3523—3532
DOI https://doi.org/10.2147/JMDH.S343140
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Amna Alotiby,1 Maram Alshareef2
1Department of Hematology and Immunology, Faculty of Medicine, Umm Al-Qura University, Makkah, Saudi Arabia; 2Department of Community Medicine and Pilgrims Health, Faculty of Medicine, Umm Al-Qura University, Makkah, Saudi Arabia
Correspondence: Amna Alotiby
Department of Hematology and Immunology, Faculty of Medicine, Umm Al-Qura University, Makkah, Saudi Arabia
Email [email protected]
Introduction: Herbal medicine is commonly used for symptom relief and treatment because of its availability and lack of prescription regulation. However, the use of herbs is associated with adverse effects, drug interaction, and sometimes life-threatening complications. During the coronavirus disease (COVID-19) pandemic, herbs were used when modern medicine failed to treat or immunize people against the virus in its early course. Although trials are still ongoing, herbal medicine was recommended for COVID-19 in Eastern countries based on expert consensus.
Methods: A descriptive web-based anonymous survey was created and distributed online all-over Saudi Arabia to gather information on commonly used herbs, knowledge, and attitude towards them among general population (GP) and health care workers (HCWs).
Results: Although the use of natural products was high among the GP, both groups used similar herbs, reflecting cultural traditions and beliefs. However, the GP had better knowledge about and attitudes toward the use of herbal medicine than HCWs did.
Conclusion: Mental exhaustion during the COVID-19 pandemic and a lack of research-based evidence might influence HCWs’ trust in and knowledge about herbal medicine. Therefore, research and educational courses on herbal medicine for all medical practitioners are needed for proper patient counseling to reduce risk and ensure patient safety.
Keywords: COVID-19, herbs, Saudi Arabia, herbal medicine, healthcare worker, healthcare
Introduction
Herbal products are commonly used worldwide to treat diseases, and they contain active ingredients present in natural plants, which can be used to relieve certain symptoms. Herbal products are cheap, which supports its use by the general population (GP).1,2 The manufacturing regulations and commercialization of medicinal herbs and natural products vary between countries without specific control on marketing.3 More than one-third of the elderly population in the United States has used ≥1 herbal supplements for different conditions.4 Although 23–80% of the population in Middle Eastern countries reportedly use herbal medicine, >80% of the GP in Saudi Arabia do, most of whom are women who are interested in herbal and traditional medicine.5,6
In general, the GP uses herbal and natural products as a first-line treatment and believes in the safety thereof.7,8 For this reason, among others, herbs have been used for conditions such as a cough and chronic diseases such as rheumatic diseases or cancer.9 Further, caregivers reportedly often give herbal products to their children because they believe in its safety and they lack awareness about the possible harmful effects of herbs or drug interactions that could be fatal.10 This lack of knowledge of the usage of herbs and natural products can lead to unexpected side effects or life-threatening drug interactions.11,12 Natural products can also cause toxicity if used excessively without prescription or proper supervision.7,13
Healthcare workers (HCWs) who studied modern medicine have limited exposure to herbal medicine in their course curriculum, and most HCWs lack training in this branch of medicine unless pursued out of self-interest.14,15 In such cases, HCWs show interest if they are supported by quality knowledge16 and guidelines.17 Although courses on herbal medicine are being implemented in a few colleges,18 more research and training are needed.
Interestingly, herbal medicine played a significant role during the first severe acute respiratory syndrome epidemic in some countries such as China.19 Previous studies reported traditional Chinese medicines may have an antiviral and a symptom-relieving effect, which may delay or reduce the development of mild diseases into severe ones. However, more validation studies with high-quality evidence are required to support safety and efficacy.20,21
During the initial coronavirus disease (COVID-19) phases, the rapid spread of the virus, its high infection rate, and lack of evidence-based medicine and effective vaccines prompted the use of natural products to enhance the immune system and protect against viral infection.22,23 A review on the use of herbs as adjuvant treatment for patients with COVID-19 was recently published,24 but the safe dosage is based on expert consensus reported mainly from Eastern countries.25 Additionally, several randomized controlled trials on the safety of herbal products as a cotreatment for COVID-19 are still being conducted, thus the results are not yet available.26 Although various regulations have been established, they have not been well implemented because of the lack of randomized control trials and the vast differences in plant species used between countries.1 Despite their lack of knowledge, both the GP and HCWs continue to use herbal medicine to strengthen their immune system and protect themselves against COVID-19 infection. For example, a recent study conducted during the COVID-19 pandemic in Saudi Arabia investigated the GP’s knowledge about the use of herbal medicine; and they showed moderate knowledge.22
Several studies not related to the pandemic found HCWs expressed a need for further education regarding the use of herbal medicine.17,27 However, to the best of our knowledge, no study has compared the knowledge about and attitude toward herbal medicine between the GP and HCWs. Therefore, the current study aimed to compare the knowledge about and attitude toward the use of herbs and natural products as a protective measure during the COVID-19 pandemic between HCWs and the GP in Saudi Arabia.
Materials and Methods
Study Design and Population
The current study was a descriptive cross-sectional study conducted anonymously in the Kingdom of Saudi Arabia between May 1, 2020 and June 31, 2020. The sample size of the study groups was calculated using OpenEpi version 3.028 and considering the population size of Saudi Arabia (approximately 34 million29) and the total number of HCWs in Saudi Arabia (approximately 500,00030) for the GP and HCW groups, respectively. The minimum required sample size to achieve a 95% confidence interval and a 5% margin of error was 385 participants per study group. Every individual and HCW in Saudi Arabia was able to participate in the study regardless of their COVID-19 infection status provided they were ≥18 years old. Any participants aged <18 years were excluded from the study.
Study Tool
A questionnaire was developed in accordance with previously published studies5,22,27,39 to assess the level of knowledge about the use of herbs and natural product as protective measures during the COVID-19 pandemic of the GP and HCWs. The questionnaire was reviewed by four individuals who were experts in medical immunology, family medicine, preventive medicine, and clinical nutrition to evaluate its appropriateness and adequacy. Then, the questionnaire was translated into Arabic because it is the native language of the participants. The Arabic questionnaire was pretested by the four experts (native speakers of Arabic) and 20 volunteers (a mix of GP and HCWs) to determine if respondents would understand the questions, could perform the tasks, and would have the information the questions required of them. The reliability of the questions was tested using Cronbach’s test. The questionnaire items were observed to be reliable with a minimum reliability score of 0.68 for (nominate a question) and a maximum of 0.82 for (nominate another question).
The questionnaire was divided into three parts and included 14 questions. The first part included eight questions and started by asking the participants whether they were HCWs, and if so, their specialty, etc. The remaining six questions were related to general demographic information such as the area of residence in Saudi Arabia, nationality, gender, age, educational level, and health status. The second part included one question: a broad choice of herbs and natural products (14 items) to estimate their prevalence of use in both study groups during the pandemic. The third part consisted of five questions focusing on the participants’ knowledge about and attitude toward the use of herbs and natural products as protective measures during the COVID-19 pandemic and on information sources. The questionnaire was approved by the Biomedical Ethics Committee at our institute before distributing it to the participants. Since it was not feasible during this time to perform a community-based national sampling survey, we collected the data online via a Google survey, which included an online informed consent form on the first page. The survey was advertised on social media platforms. Furthermore, the Saudi Commission for Health Specialties supported us by emailing the survey to all registered HCWs in their database.
Data Analysis
Study data were extracted, revised, coded, and inputted to statistical software IBM SPSS version 22 (SPSS, Inc., Chicago, IL), then statistically analyzed using two-tailed tests. For knowledge items, each correct answer scored one point, and discrete scores for the knowledge items were summed to get an overall knowledge score (0–5). A participant with a score <60% of the maximum score (<3 points) was considered to have poor knowledge, while good knowledge was considered if he had a score ≥60% of the maximum. Descriptive analysis based on the frequency and percent distribution was performed for all variables according to study group (HCWs or GP), including demographic data, herbs, product use, awareness, and practice. Cross-tabulation was used to assess the distribution of herbs utilized by the study groups and their awareness according to participants’ personal and work situations. Relationships were verified using the Pearson chi-square test. A result was considered statistically significant for a P-value ≤0.05.
Results
Sociodemographic Data
The study included 1249 participants: 274 HCWs (mean age, 28.6±9.6 years; females, 176 [64.2%]) and 975 of the GP (mean age, 27.4±8.6 years; females, 785 [80.5%]). Regarding qualification, 142 (51.8%) HCWs had a bachelor’s degree compared with 571 (58.6%) of the GP, whereas 39.1% HCWs had a postgraduate degree compared with 12.3% of the GP. A total of 29.2% of HCWs had chronic health problems compared with 26.2% of the GP (Table 1).
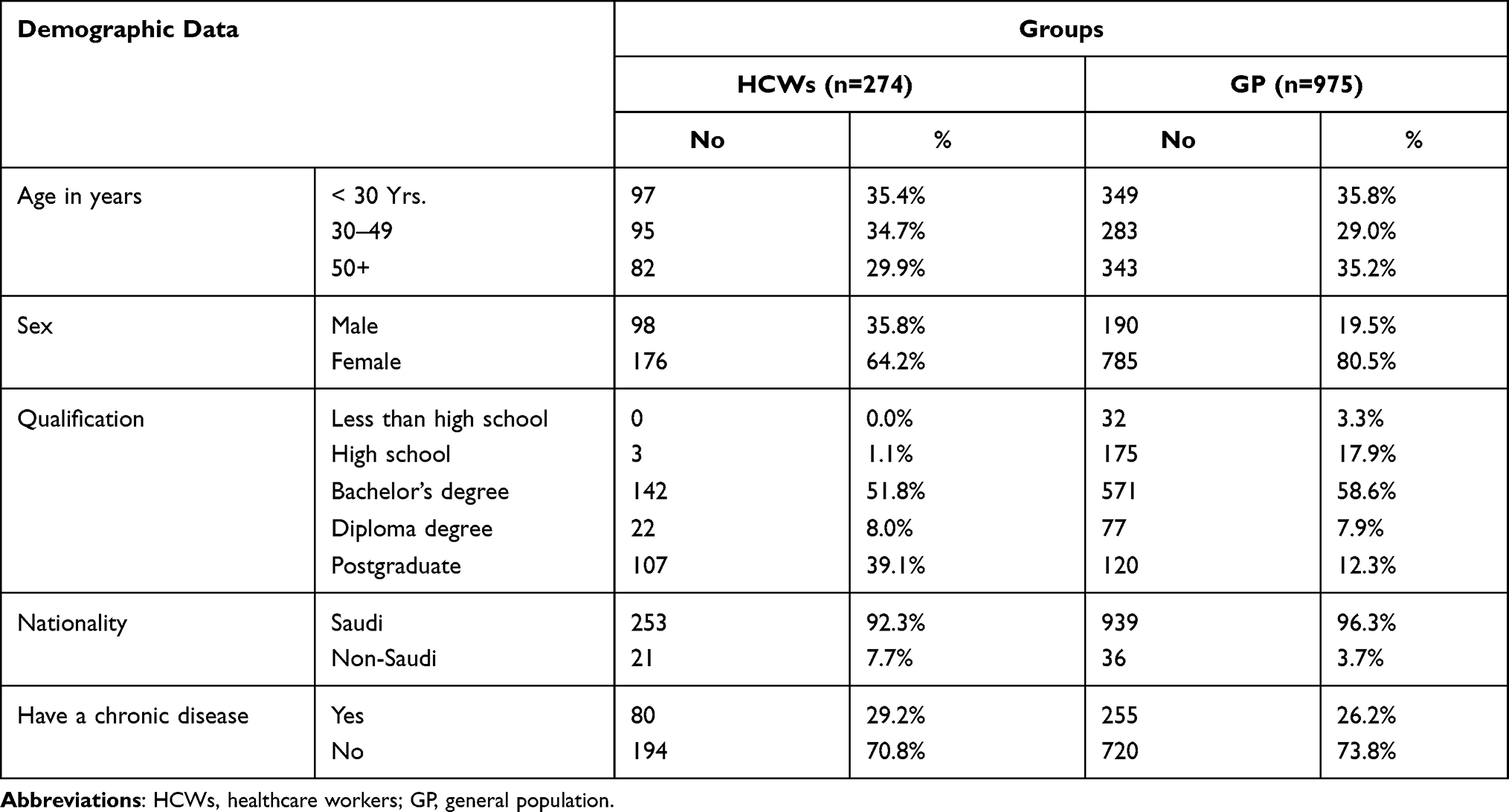 |
Table 1 Demographic Data of HCWs and the GP, Saudi Arabia |
Comparison of Commonly Used Herbs and Natural Products Between Participants
Table 2 illustrates the prevalence of which herbs and natural products were used as a protective measure against COVID-19 infection. In general, the use of herbs and natural products was higher in the GP than in HCWs. There were statistically significant differences (all P=0.001) between the GP and HCWs in terms of the most used products, which were honey (GP: 83.9% vs HCW: 79.2%), lemon (75.3% vs 69%), orange (70.9% vs 66.8%), black seed (69.7% vs 68.2%), and garlic (64.1% vs 52.2%).
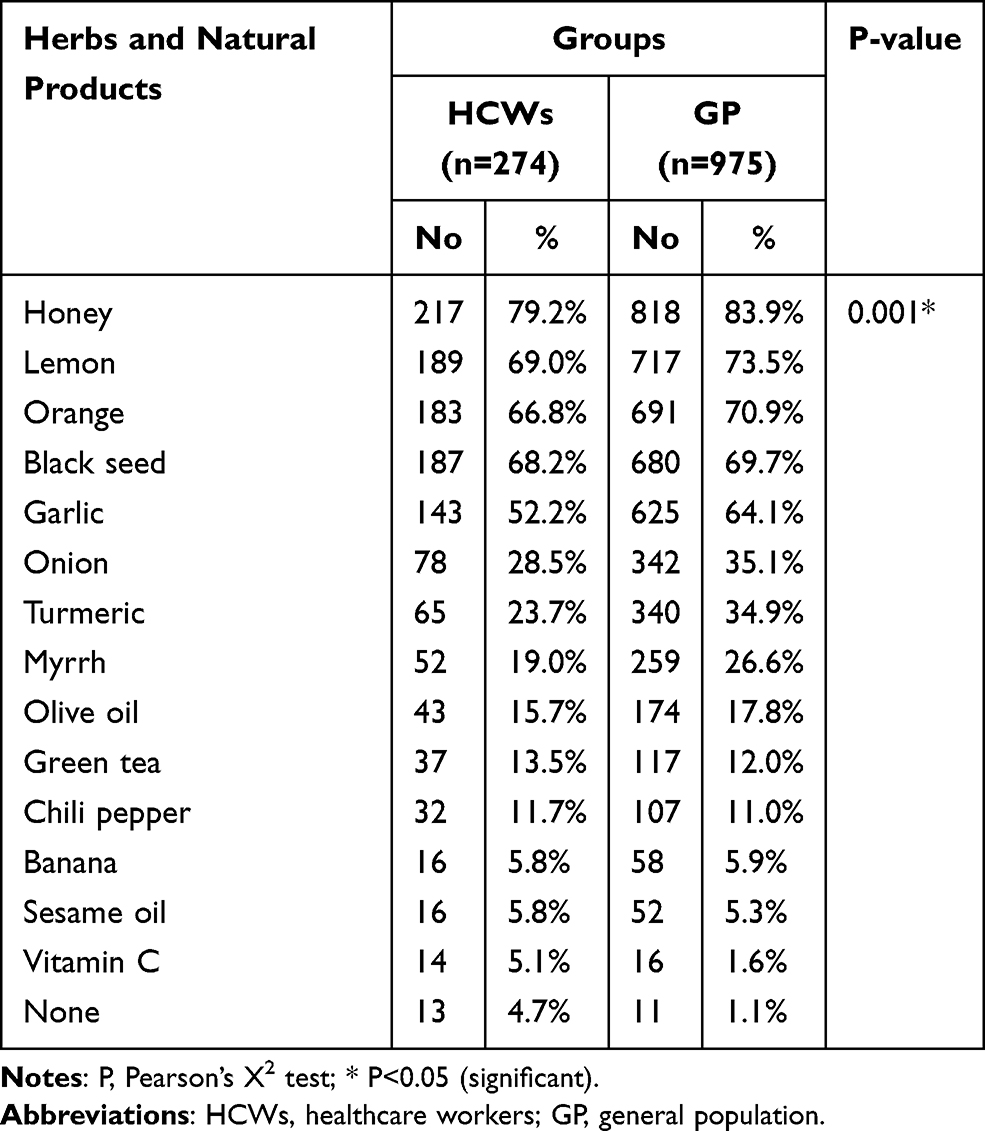 |
Table 2 Herbs and Natural Products Use as Protective Measure Against COVID-19 Infection by Study Groups |
Interestingly, even the difference in the prevalence of using herbs and natural products between the study groups was statistically significant. However, the types of natural products chosen were similar between groups (Figure 1).
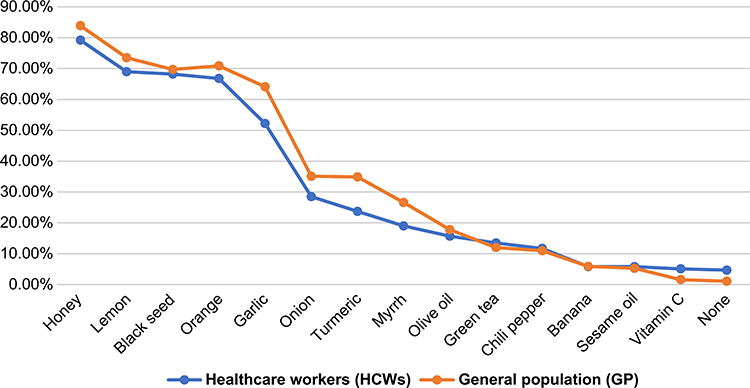 |
Figure 1 Preferred types of herbs and natural products used during the COVID-19 pandemic in both study groups in Saudi Arabia. |
Knowledge About and Attitude Toward the Use of Herbs and Natural Products
Regarding the participants’ knowledge about and attitude toward the use of herbs and natural products as a protective measure during the COVID-19 pandemic (Table 3), only 10.6% of HCWs agreed herbs or natural products could protect against COVID-19 infection compared with 11.4% of the GP (P=0.097). The rate of HCWs agreeing that herbs or natural products could strengthen the immune system and protect against COVID-19 infection even upon contact with an infected patient was also lower than that of the GP (10.9% vs 12%, P=0.227). The lack of side effects of regular herbs or natural products use as preventive medicine was reported by significantly fewer HCWs than the GP (77.7% vs 87.7%, P=0.001). Interestingly, 85.2% of HCWs and 83.9% of the GP (P=0.811) believed that herbs and natural products could aid a healthy immune system, but that they are not specifically related to protection against COVID-19 infection (Table 3).
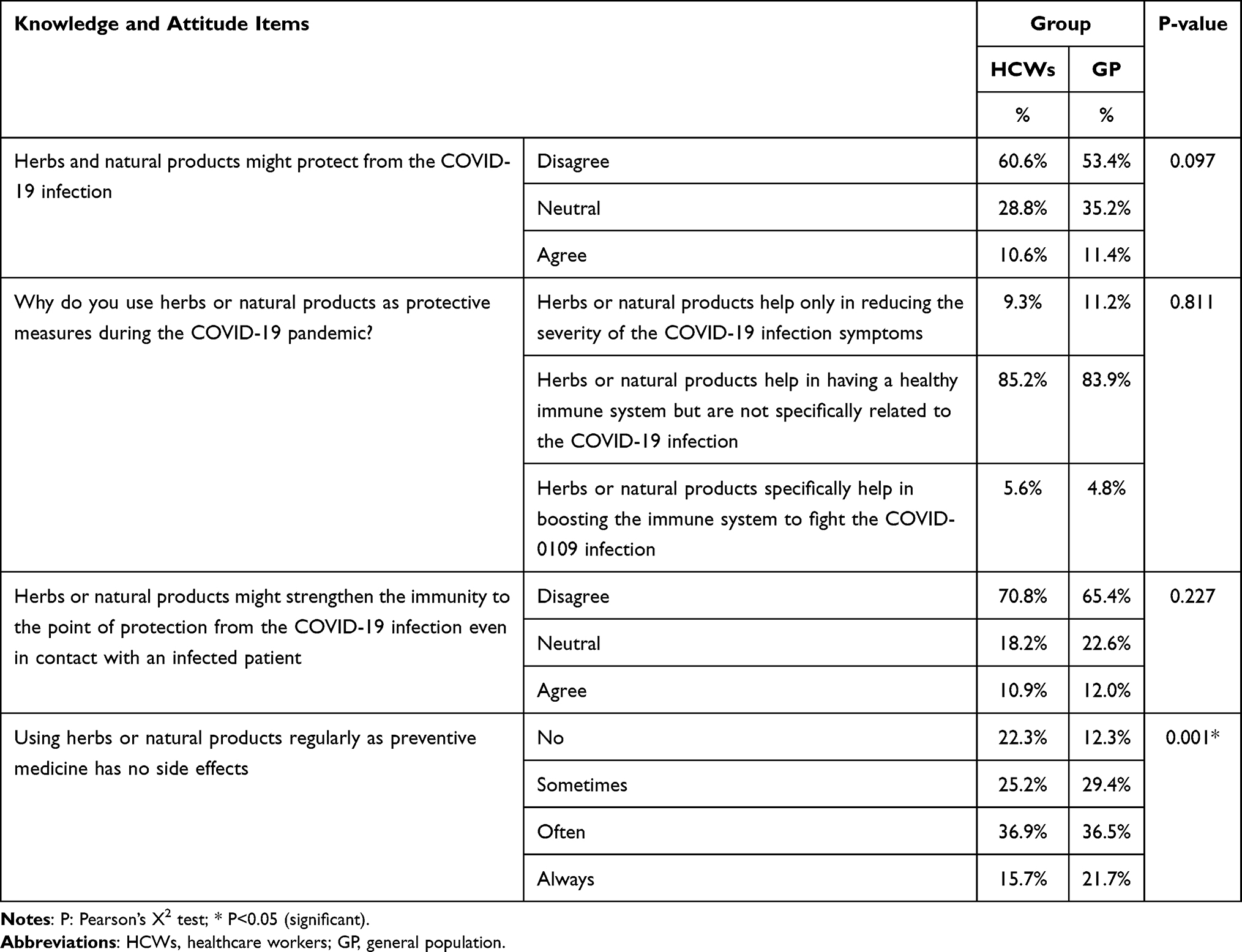 |
Table 3 Participant’s Knowledge and Attitude Regarding Herb and Natural Product Use as a Protective Measure During the COVID-19 Pandemic |
Table 4 illustrates the distribution of participants’ knowledge level according to their sociodemographic data. Good knowledge of the herbs and products used to protect against COVID-19 infection was found in 42.7% of the GP compared with 34.3% of HCWs (P=0.013). In addition, 46.4% of the older participants (≥50 years) showed good knowledge compared with 35.7% of the younger ones (P=0.006).
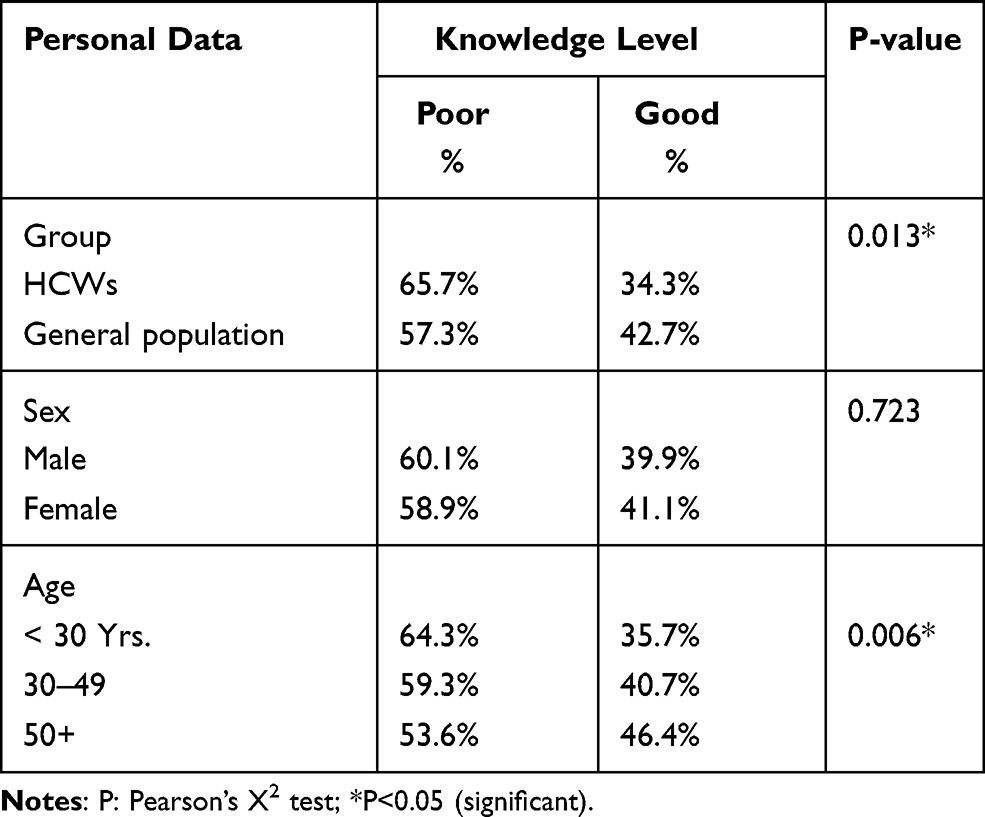 |
Table 4 Distribution of Participants’ Knowledge Level by Their Sociodemographic Data. The Knowledge Level Was Evaluated as Poor or Good Based on the Scoring System Mentioned in the Materials and Methods |
Knowledge About Herbs and Natural Products as a Protective Measure Against COVID-19 According to Specialty in the HCW Group
The total number of HCWs in the current study was 275, and their specialties are illustrated in Figure 2. Regarding the use of herbs and natural products as a protective measure during the COVID-19 pandemic, 50% of the clinical nutrition specialists had a good knowledge level compared with 80% of the public health specialists, 80% of radiologists, 47.7% of nurses, 30% of physicians, and 21.7% of pharmacists (Table 5; P=0.004).
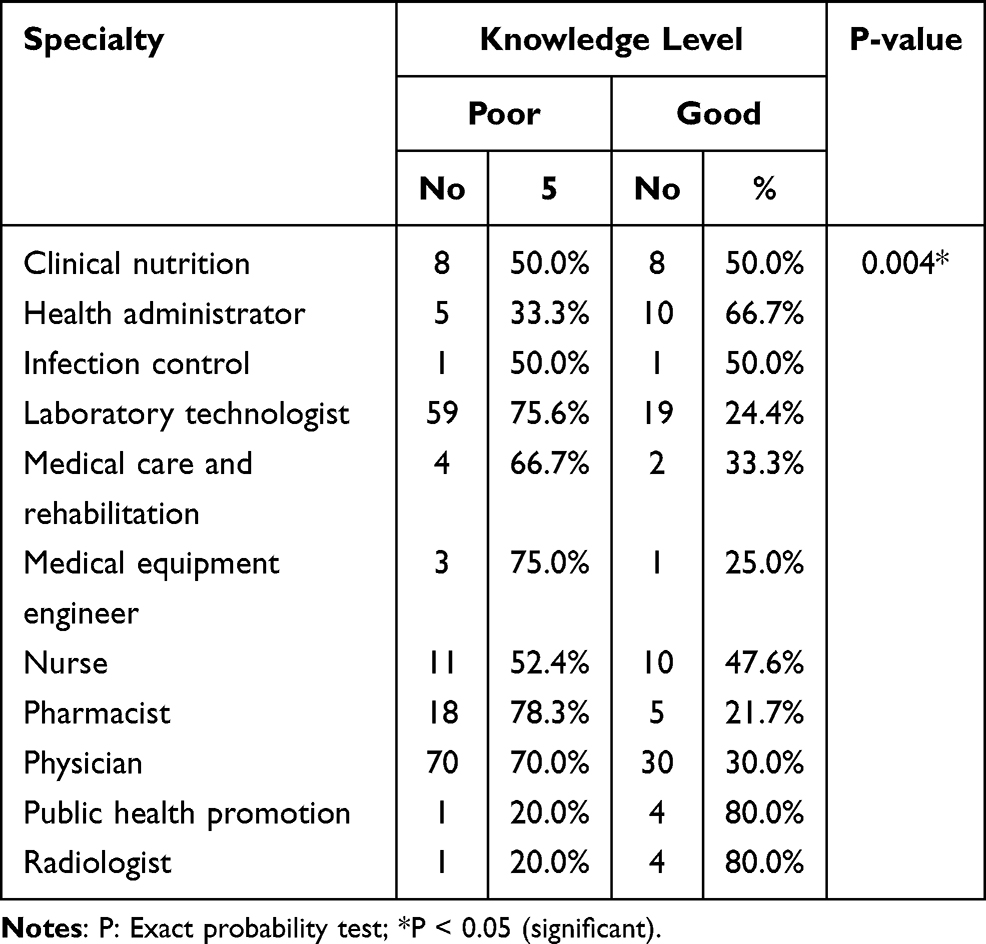 |
Table 5 Distribution of HCWs Knowledge Level Regarding Herbs by Specialties. The Knowledge Level Was Evaluated as Poor or Good Based on the Scoring System Mentioned in the Materials and Methods |
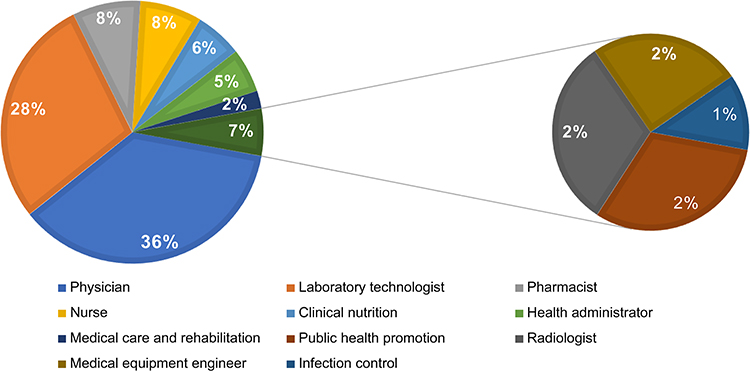 |
Figure 2 Distribution of HCW participants regarding their specialties. Abbreviation: HCWs, healthcare workers. |
Sources of Information for Using Herbs and Natural Products as a Protective Measure Against COVID-19
Figures 3 and 4 show the most used sources of information for understanding the role of herbs and natural products in protecting against COVID-19 infection during the pandemic. The most frequently used sources of information were social media (30.8%), followed by family and friends (20.5%), previous experience (16.7%), and published articles (16.4%). Social media was the most frequent source of information in both groups (33.6% and 30.1%; P=0.639). However, the second most used source of information was published articles (19.7%) in the HCW group and family and friends (21.6%) in the GP group.
 |
Figure 3 Sources of information for using herbs and natural products as a protective measure during the COVID-19 pandemic in all participants. |
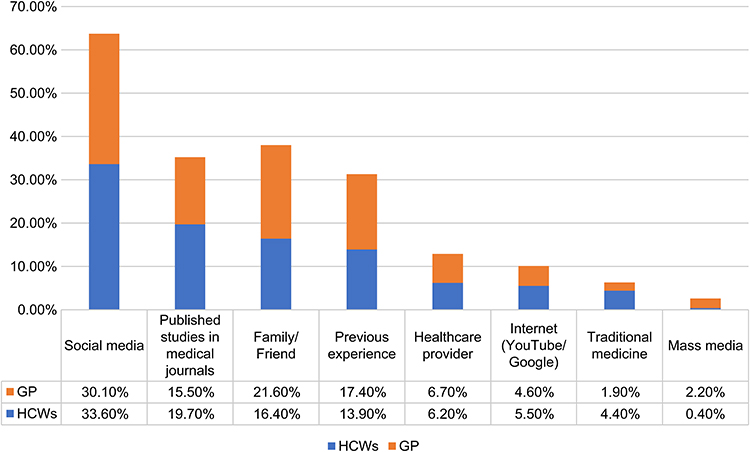 |
Figure 4 Sources of information for using herbs and natural products as a protective measure during the COVID-19 pandemic according to groups. Abbreviations: HCWs, healthcare workers; GP, general population. |
Discussion
This study is the first to compare knowledge about and attitudes toward the use of herbal medicine as a protective measure during the COVID-19 pandemic between the GP and HCWs. Most respondents were young females in both groups, as noted in previous studies.31,32 The mean age of respondents was 28±9 years, which is similar to that in previous studies;22,31,32 this phenomenon might be explained by the methodology, which was an online questionnaire because of COVID-19 precautions, and by most older adults having limited interest in prolonged online surveys.33 However, older participants might have responded if an incentive had been given to answer the survey.34
The current study shows commonly used herbs in Saudi Arabia in both study groups during the pandemic were honey, lemon, orange, black seed, and garlic. These were reasonable findings because of availability and because cultural practices emphasize these products can strengthen the immune system. However, a recent study in Saudi Arabia on herbs and natural products used during the pandemic showed garlic as the most used, followed by vitamin C.22 This difference might be because the current study included a broader choice of herbs and natural products than did the Alyami et al. study.22
Remarkably, most of the participants in both groups agreed that using herbs does not protect against COVID-19 infection but that it can enhance the immune system.23 However, the overall comparison found that the GP had better knowledge than HCWs about the use of herbal medicine for COVID-19 as an immune system booster but not as protective agents. Consistent with this finding, several studies reported HCWs need further education and training on herbal medicine to improve their knowledge.17,27,35 The good knowledge of the GP might be explained by them actively seeking natural immune system boosters to protect themselves against COVID-19 infection during the pandemic and by the influence of cultural beliefs on Islamic and traditional medicine in Saudi Arabia. With regard to HCWs, their scientific thinking and reasoning tendency, lack of interest or trust concerning topics supported by insufficient evidence, and mental exhaustion might explain their poor level of knowledge. Mental exhaustion is highly reported in front-line HCWs most exposed to COVID-19 patients36,37 and was observed in the current study among physicians and nurses but less among radiologists, who are the least exposed to patients and public health specialists involved in patient education during the pandemic.
The current study showed that the older population had a significantly better knowledge than the younger one, which could be attributed to their life experience. Worldwide regulations on the use of herbal medicine are still not well established or consistent despite being implemented in both Western and Eastern countries.27 In Saudi Arabia, no well-formulated body of work provides supporting evidence for herbal medicine.28 Therefore, the present study found the main sources of information for herbal medicine in both groups were social media, nonevidence-based blogs, and relatives, which all lead to incorrect practices. Indeed, there is an urgent need for specific guidelines on herbs in Saudi Arabia besides the implementation of herbal medicine education as part of the modern medical curriculum.
HCWs do not receive education or training on complementary and alternative medicine or herbs during their undergraduate or postgraduate studies, resulting in a lack of knowledge and competency in this type of medicine.17 However, HCWs showed a better general understanding of the benefits and side effects of herbs than the GP did.27,39 Additionally, research must be conducted on the specific herbs available in Saudi Arabia because each country’s herbs differ based on agriculture.2,38 HCWs, especially physicians, pharmacists, nurses, and dietitians, who frequently interview patients who take herbs that can potentially cross-react with other chemicals, which could be life-threatening, need to have adequate knowledge about herbal medicine to conduct proper patient counseling regarding its use.
The current study is limited by the small sample size of the HCW group due to the pandemic and stress. Therefore, we suggest performing another study, one more extensive than ours, that includes numerous HCWs, particularly those with regular contact with patients such as physicians, nurses, and pharmacists.
Conclusions
Herbal medicine is commonly used without restriction by the GP. Research on the most common types of herbs utilized in a particular geographical area must be conducted to define evidence-based protocols and create local guidelines. Complementary and alternative medicine education should be integrated into the undergraduate medical curricula to empower HCWs to conduct proper patient counseling to reduce complications and ensure patient safety.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Ethics Approval and Consent to Participate
The study was approved by the Biomedical Ethics Committee, Faculty of Medicine, Umm Al-Qura University (approval no.: HAPO-02-K-012-2020-04-378) and it conformed to the ethics guidelines of the Declaration of Helsinki. The participants were recruited online and provided with a URL that took them to the survey page. Participants then had to agree to participate after reading the informed consent on the survey’s front page.
Acknowledgments
The authors would like to thank all participants who spent their time filling in the survey and giving the authors insight into the herbal practice in Saudi Arabia. The authors are also grateful to the Deanship of Scientific Research at Umm Al-Qura University, Makkah, Saudi Arabia for their continuous support and the Saudi Commission for Health Specialties for distributing the survey to the HCWs. The authors also would like to thank Dr. Bayan Hashim Alsharif, associate consultant in preventive medicine and public health at King Abdullah Medical City, for revising and validating the questionnaire.
Author Contributions
All authors: made a significant contribution to the work reported, including conception, study design, execution, acquisition of data, analysis, and interpretation; drafted, revised, or critically reviewed the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors have no conflicts of interest to declare.
References
1. Parveen A, Parveen B, Parveen R, Ahmad S. Challenges and guidelines for clinical trial of herbal drugs. J Pharm Bioallied Sci. 2015;7(4):329–333. doi:10.4103/0975-7406.168035
2. Tilburt JC, Kaptchuk TJ. Herbal medicine research and global health: an ethical analysis. Bull World Health Organ. 2008;86(8):594–599. doi:10.2471/blt.07.042820
3. World Health Organization. Regulatory situation of herbal medicines: a worldwide review: the evaluation of these products and ensuring their safety and efficacy through registration and regulation present important challenges. Geneva: World Health Organization; 1998.
4. Rashrash M, Schommer JC, Brown LM. Prevalence and predictors of herbal medicine use among adults in the United States. J Patient Exp. 2017;4(3):108–113. doi:10.1177/2374373517706612
5. Al Akeel MM, Al Ghamdi WM, Al Habib S, Koshm M, Al Otaibi F. Herbal medicines: Saudi population knowledge, attitude, and practice at a glance. Fam Med Prim Care Rev. 2018;7(5):865–875. doi:10.4103/jfmpc.jfmpc_315_17
6. John LJ, Shantakumari N. Herbal medicines use during pregnancy: a review from the Middle East. Oman Med J. 2015;30(4):229–236. doi:10.5001/omj.2015.48
7. Alkhamaiseh SI, Aljofan M. Prevalence of use and reported side effects of herbal medicine among adults in Saudi Arabia. Complement Ther Med. 2020;48:102255. doi:10.1016/j.ctim.2019.102255
8. Tengku Mohamad TAS, Islahudin F, Jasamai M, Jamal JA. Preference, perception and predictors of herbal medicine use among Malay women In Malaysia. Patient Prefer Adherence. 2019;13:1829–1837. doi:10.2147/PPA.S227780
9. Barry AR. Patients’ perceptions and use of natural health products. CPJ. 2018;151(4):254–262. doi:10.1177/1715163518779409
10. Lanski SL, Greenwald M, Perkins A, Simon HK. Herbal therapy use in a pediatric emergency department population: expect the unexpected. Pediatrics. 2003;111(5):981–985. doi:10.1542/peds.111.5.981
11. Faizi N, Kazmi S. Universal health coverage - There is more to it than meets the eye. Fam Med Prim Care Rev. 2017;6(1):169–170. doi:10.4103/jfmpc.jfmpc_13_17
12. Yang Y. Use of herbal drugs to treat COVID-19 should be with caution. Lancet. 2020;395(10238):1689–1690. doi:10.1016/S0140-6736(20)31143-0
13. Fatima N, Nayeem N. Toxic effects as a result of herbal medicine intake. In: Toxicology - New Aspects to This Scientific Conundrum. InTech; 2016. doi10.5772/64468
14. Albadr BO, Alrukban M, Almajed J, et al. Attitude of Saudi medical students towards complementary and alternative medicine. J Family Community Med. 2018;25(2):120–126. doi:10.4103/jfcm.JFCM_98_17
15. Clement YN, Williams AF, Khan K, et al. A gap between acceptance and knowledge of herbal remedies by physicians: the need for educational intervention. BMC Complement Altern Med. 2005;5:20. doi:10.1186/1472-6882-5-20
16. Hussain I, Majeed A, Saeed H, et al. A national study to assess pharmacists’ preparedness against COVID-19 during its rapid rise period in Pakistan. PLoS One. 2020;15(11):e0241467. doi:10.1371/journal.pone.0241467
17. Hilal M, Hilal S. Knowledge, attitude, and utilization of herbal medicines by physicians in the Kingdom of Bahrain: a cross-sectional study. J Assoc Arab Univ Basic Appl Sci. 2017;24(1):325–333. doi:10.1016/j.jaubas.2016.11.001
18. Dvorkin L, Gardiner P, Whelan JS. Herbal medicine course within pharmacy curriculum. J Herb Pharmacother. 2004;4(2):47–58. doi:10.1080/j157v04n02_05
19. World Health Organization. SARS: clinical trials on treatment using a combination of traditional Chinese medicine and Western medicine. Geneva: World Health Organization; 2004.
20. Wang Z, Yang L. Chinese herbal medicine: fighting SARS-CoV-2 infection on all fronts. J Ethnopharmacol. 2021;270:113869. doi:10.1016/j.jep.2021.113869
21. Huang F, Li Y, Leung ELH, et al. A review of therapeutic agents and Chinese herbal medicines against SARS-COV-2 (COVID-19). Pharmacol Res. 2020;158:104929. doi:10.1016/j.phrs.2020.104929
22. Alyami HS, Orabi MAA, Aldhabbah FM, et al. Knowledge about COVID-19 and beliefs about and use of herbal products during the COVID-19 pandemic: a cross-sectional study in Saudi Arabia. SPJ. 2020;28(11):1326–1332. doi:10.1016/j.jsps.2020.08.023
23. Panyod S, Ho CT, Sheen LY. Dietary therapy and herbal medicine for COVID-19 prevention: a review and perspective. J Tradit Complement Med. 2020;10(4):420–427. doi:10.1016/j.jtcme.2020.05.004
24. Silveira D, Prieto-Garcia JM, Boylan F, et al. COVID-19: is there evidence for the use of herbal medicines as adjuvant symptomatic therapy? Front Pharmacol. 2020;11:581840. doi:10.3389/fphar.2020.581840
25. Ang L, Lee HW, Kim A, Lee MS. Herbal medicine for the management of COVID-19 during the medical observation period: a review of guidelines. Integr Med Res. 2020;9(3):100465. doi:10.1016/j.imr.2020.100465
26. López-Alcalde J, Yan Y, Witt CM, Barth J. Current state of research about Chinese herbal medicines (CHM) for the treatment of coronavirus disease 2019 (COVID-19): a scoping review. J Altern Complement Med. 2020;26(7):557–570. doi:10.1089/acm.2020.0189
27. Fathy H, El-Hawy R, Hassan R. Attitudes, knowledge and practice of herbal remedy use among the population visiting pharmacies and health care providers in Alexandria, Egypt: a cross-sectional study. Eur J Med Plants. 2019;1–10. doi:10.9734/ejmp/2019/v30i230170
28. Sullivan KM, Dean A, Soe MM. On Academics: openEpi: a web-based epidemiologic and statistical calculator for public health. Public Health Rep. 2009;124(3):471–474. doi:10.1177/003335490912400320
29. General Authority for Statistics in Saudi Arabia. Population Estimates. Kingdom of Saudi Arabia; 2020. Available from: https://www.stats.gov.sa/en/43.
30. Saudi Commission for Health Specialties. The annual report of the Saudi Commission for Health Specialties. Kingdom of Saudi Arabia: SCHS; 2020.
31. Stjernberg L, Berglund J, Halling A. Age and gender effect on the use of herbal medicine products and food supplements among the elderly. Scand J Prim Health Care. 2006;24(1):50–55. doi:10.1080/02813130500475522
32. Zhang Y, Leach MJ, Hall H, et al. Differences between male and female consumers of complementary and alternative medicine in a national US population: a secondary analysis of 2012 NIHS data. Evid Based Complement Alternat Med. 2015;2015:413173. doi:10.1155/2015/413173
33. Smith W. Does gender influence online survey participation? A record-linkage analysis of university faculty online survey response behavior. Online Submission; 2008.
34. Saleh A, Bista K. Examining Factors impacting online survey response rates in educational research: perceptions of graduate students. J Multidiscip Eval. 2017;13(29):63–74.
35. Kemper KJ, Amata-Kynvi A, Sanghavi D, et al. Randomized trial of an internet curriculum on herbs and other dietary supplements for health care professionals. Acad Med. 2002;77(9):882–889. doi:10.1097/00001888-200209000-00014
36. Arshad MS, Hussain I, Nafees M, et al. Assessing the impact of COVID-19 on the mental health of healthcare workers in three metropolitan cities of Pakistan. Psychol Res Behav Manag. 2020;13:1047–1055. doi:10.2147/PRBM.S282069
37. Lai J, Ma S, Wang Y, et al. Factors associated with mental health outcomes among health care workers exposed to coronavirus disease 2019. JAMA Network Open. 2020;3(3):e203976. doi:10.1001/jamanetworkopen.2020.3976
38. Jagadeeswara Reddy K, Alex M, Thomas A. Regulations for herbal medicine-worldwide: a focus on current regulations and their requirements. Saarbrücken, Germany: Lambert Academic Publishing; 2020:1–92.
39. Asmelashe Gelayee D, Binega Mekonnen G, Asrade Atnafe S, Birarra MK, Asrie AB. Herbal medicines: personal use, knowledge, attitude, dispensing practice, and the barriers among community pharmacists in Gondar, Northwest Ethiopia. Evid Based Complement Alternat Med. 2017;2017:6480142. doi:10.1155/2017/6480142
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.