Back to Journals » Neuropsychiatric Disease and Treatment » Volume 18
Comparing Theory of Mind Development in Children with Autism Spectrum Disorder, Developmental Language Disorder, and Typical Development
Authors Schwartz Offek E, Segal O
Received 13 April 2022
Accepted for publication 9 August 2022
Published 14 October 2022 Volume 2022:18 Pages 2349—2359
DOI https://doi.org/10.2147/NDT.S331988
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Esther Schwartz Offek, Osnat Segal
Department of Communication Disorders, The Stanley Steyer School of Health Professions, Sackler Faculty of Medicine, Tel-Aviv University, Tel Aviv, Israel
Correspondence: Osnat Segal, Department of Communication Disorders, Tel Aviv University, P.O. Box 39040, Tel Aviv, Israel, Tel +972 522998404, Email [email protected]; [email protected]
Background: Theory of mind (ToM) is the ability to recognize, comprehend, and consider oneself’s and others’ mental states and perspectives to predict and explain behaviors and motivations. It is widely accepted that children with autism spectrum disorder (ASD) experience difficulties with ToM. However, there are also findings suggesting that ToM abilities might also be compromised in children with Developmental Language Disorders (DLD).
Purpose: To assess ToM abilities in three groups of children: 1. ASD with no language difficulties; 2. DLD, known for their language disorder; and 3. TD with no language issues.
Materials and Methods: A total of 41 preschool children aged 5-to-6 were examined and assigned to one of the three groups based on previous clinical reports and a standardized Hebrew language assessment tool. Nonverbal IQ was established with a standardized test to verify within average range placement (> 75 IQ). ToM skills were examined with a Hebrew version of the ToM Task Battery and parent’s questionnaire (ToMI).
Results: Children with ASD had significantly lower ToM scores compared to the children with DLD, and TD. The ToM scores of the children with DLD were similar to the scores of the TD children. According to the parents’ questionnaires, both the ASD children and the DLD children had less developed ToM skills compared to their TD peers.
Conclusion: The present findings suggest that children with ASD have a fundamental difficulty in ToM that is independent of their language abilities. Children with DLD show difficulties in everyday social interactions that involve ToM. It is possible that both ASD and language disorders influence ToM development, suggesting that different developmental routes affect the acquisition of ToM.
Keywords: autism, DLD, ToM, ToMTB, ToMI
Introduction
ToM is considered as the capacity to represent and understand mental states, emotions, motivations, and oneself’s and others’ beliefs.1 Children and adults with Autism Spectrum Disorder (ASD) often present difficulties in ToM, and this impedes their participation in social contexts.2–4 In fact, the ToM Hypothesis for Autism suggests that difficulties in ToM are the core deficit underlying the social, behavioral, and communicative deficits exhibited by individuals with ASD.1,5 Although to-date questions have arisen regarding the universality and uniqueness of theory-of-mind deficits in autism, and about how this hypothesis could explain early symptoms including restricted interests, or repetitive behaviors, studies repeatedly show reduced performance on tasks that assess ToM in ASD.6 Thus, ToM is still considered crucial for understanding social performance in ASD. However, the association between language skills (eg, vocabulary and grammar) and performance on ToM tasks in children with ASD raises the possibility that language abilities affect the performance of ToM tasks in children with ASD.7,8 One way to tease apart the influence of language on ToM abilities is to assess children with ASD and with no language disorder compared to children with language disorder and no ASD. Thus, the present study was aimed to assess ToM abilities in children with ASD whose language is within the norm for their age (ASD-LN)9,10 compared to children with developmental language disorder (DLD) and typically developing children (TD).
Assessment of ToM
ToM is traditionally assessed using false-belief tasks that require children to attribute a false belief to another person to predict his or her behaviour.11 In one classic false-belief task that involves location change, namely, the “Sally-Anne” task,1 the doll Sally hid a marble and left the room, and the other doll Ann changed the location of this marble. When Sally returned, the experimenter asked the child “Where will Sally look for her marble?„ A correct answer would be to point to the previous location of the marble, suggesting that the child has understood the doll’s false belief. An incorrect answer would be to point to the marble’s present location, suggesting that the child has not taken the doll’s belief into account.1 In another well-known false-belief task, which involves unexpected content, the “Smarties” task,12 the child is shown a tube of Smarties and, in contrast to his/her expectation to find sweets inside the tube, he/she found pencils inside. The experimenter then asks the child the following question: “What would a child who has not seen inside the tube think is in there before it is opened”. The correct answer “smarties” or “sweets” reflects the ability to represent another person’s belief.12 In sum, to succeed in false-belief tasks, children must understand that people’s actions are influenced by their mental representations of the world, regardless of the accuracy of this representation.
In recent decades, however, there has been a growing understanding that ToM is a broader concept than the ability to understand false beliefs.13 ToM has been described as a multifaceted ability that includes the understanding and production of intentions, beliefs, mental states, speech acts, pretense, the notion that seeing leads to knowing, as well as empathy and second-order thinking (eg, understanding what x thinks y is thinking).14–17 Accordingly, to achieve a more sensitive measure, researchers have developed task batteries that assess different components and a wider range of ToM skills than traditional false-belief reasoning ToM tasks.14,15 One comprehensive battery is the ToM Task Battery (ToMTB)14 [https://www.theoryofmindinventory.com/task-battery]. The ToM Task Battery is appropriate for verbal and nonverbal children with ASD. It consists of 15 test questions within nine tasks assessing a range of ToM tasks. The items vary in complexity and are presented in the form of a storybook. Memory control questions are included to control the influence of short-term memory on performance. The ToM Task Battery has been evaluated for reliability14 (test–retest, internal consistency).
ToM in Children with ASD
In a seminal study,1 the researchers demonstrated that compared to Down Syndrome controls, and typical developing children, those with ASD were significantly impaired on tasks of false beliefs. They tested 20 autistic children aged 11;11 (years; months), with nonverbal mental age of 9;3, and verbal mental age of 5;5 on the Sally-Ann task. The autistic group was compared to a group of children with Down Syndrome, aged 10;11, with nonverbal mental age of 5;11, and verbal mental age of 2;11. They found that 80% of the autistic group failed on this task, whereas 86% of Down Syndrome children (12/14) with lower nonverbal and verbal mental age succeeded on the task, as did 85% (23/27) of the 3;5–5;9 year old typically developing children. Additional studies have replicated the finding that most autistic individuals fail on tasks requiring them to understand false beliefs.2,18,19 Although the researchers tried to control for nonverbal and verbal skills by comparing children with ASD to children with Down syndrome, this study does not provide information on how children with ASD with preserved nonverbal cognition and language abilities perform on ToM tasks.1 In fact, only a handful of studies assessed children with ASD who had normal nonverbal mental age and language skills.20,21 One study assessed children with ASD with superior IQ (SIQ) and high functioning autism (HFA). Children with SIQ had fewer autistic traits and higher verbal IQ scores compared to children with HFA. Only the HFA group demonstrated deficits in theory of mind, performing more poorly than both children with SIQ and TD controls matched for nonverbal and verbal IQ. The results suggest that language abilities may play an important role in the performance of ToM tasks.21 This assumption was supported by other studies. In a study sample, the verbal mental age of the six participants who passed the false-belief task (M = 7; 5) was significantly higher than that of the 13 children who failed (M = 6; 0), and a significant correlation was found between mental verbal age and success on false-belief tasks (r = 0.497, p < 0.05).18 However, there was no difference in the chronological age and nonverbal mental age between children who passed the false-belief task and children who failed it. Additional studies have shown a positive relationship between language abilities, such as receptive vocabulary and grammar, and performance on ToM task in individuals with ASD, supporting the notion that ToM performance is linked to language skills.7,8 There is also evidence that co-occurrence of ASD and language impairment is associated with greater impairment in receptive language and functional communication.22 A meta-analysis found a significant relationship between language skills and false belief performance, in children younger than age 7, with language ability accounting for a significant 18% of the variance.23 In a study addressing morpho-syntax abilities, one subgroup of children with ASD showed a morpho-syntactic deficit, while another subgroup displays intact language abilities. These differences were related to theory of mind.24
Some researchers proposed that children with ASD use syntactic structures to facilitate ToM comprehension and language has been described as a compensation-mediating strategy to find solutions to ToM tasks.25,26 For example, it has been suggested that complement syntax (eg, “Dana said that she saw a fairy in her room”) is an important syntactic structure that facilitates theory of mind in typically developing children26,27 and in children with ASD by providing a representation to the perspective of another person irrespective of whether he or she is right or wrong.28 However, this assumption was only partially supported, namely, in the location-change task (“Sally-Anne” task) but not in the unexpected-content task (the “Smarties” task).29 Also, there is evidence suggesting that language abilities are insufficient for succeeding in ToM task because some children with ASD and high mental abilities fail nonetheless in the false-belief task.30 A recent longitudinal study on ToM in ASD children suggests not only a delay in ToM skills but also a deficit in the ability to spontaneously attribute mental states to explain behaviors of story characters.31
The literature on whether or not language is a mediating factor in ToM performance remains unresolved. One explanation of these mixed results derives from a proposal of two distinct systems supporting ToM task performance.32 One system is fast, automatic system, permitting social-perceptual processing, whereas the second system is a verbally mediated, deliberate, effortful, and slower. Individuals with no access to language (eg, infants) could presumably solve some ToM tasks by utilizing the former system.33
The link between language and ToM is also supported by studies in TD children. There is evidence to suggest that language abilities predicted later false-belief performance, whereas false-belief performance did not predict later language abilities in TD children.25,34 In addition, experimental training studies suggested that exposing children to training on linguistic tasks caused improvement in their false-belief performance.35 Also, deaf children of deaf parents showed better ToM abilities than deaf children of hearing parents, suggesting the influence of early exposure to sign language on ToM.36
The population of children with ASD is heterogeneous and includes children with language impairment (ASD-LI), and children whose language skills are within the norm for their age (ASD-LN) in the domains of content (lexicon) and form (morpho-syntax).8,9,37 Considering that most studies have not differentiated between children with ASD –LI and ASD-LN, and in view of the scarcity of data on ToM abilities in children with ASD-LN collected so far, the possibility that language deficits affect ToM performance in children with ASD cannot be ruled out. Thus, it is important to investigate children with ASD and preserved language (ASD-LN) to support the ToM hypothesis for ASD, which suggests that ToM is problematic in this population regardless of language ability.
ToM in Children with DLD
Children with developmental language disorder (DLD), which was termed in earlier studies as specific language impairment (SLI), have delays and deficits in language development.38 Traditionally, children with DLD have normal nonverbal intelligence and do not present any hearing, motor articulation impairment, oral-motor abnormality, or neurological deficits.39 The literature on Tom in children with DLD presents inconsistent results.
Some studies report delayed ToM development, while others do not.40,47 A meta-analysis of 17 studies with 745 children between the ages of 4 and 12 found that children with DLD had substantially lower ToM performance compared to age-matched typically developing children with a high effect size (d = 0.98). This effect size was not moderated by age and gender.41 However, in a study that assessed recognition of mental states and the use of mental state lexicon, children with DLD performed similarly to TD children.42 Additionally, preschool and school-age children with language impairments but intact pragmatic abilities performed on ToM tasks similarly to their typically developing peers, especially in tasks with low linguistic demands.42,43 One study investigated the relative contributions of grammar (general and expressive grammar), syntax (sentential complements), and semantics (receptive vocabulary) to understanding ToM tasks in preschool children with DLD. They found that sentential compliments did not contribute significantly to understanding ToM, whereas general grammar abilities and semantics did.44
Only a few studies compared children with ASD to children with DLD on ToM tasks.31 These studies mainly assessed school-aged children and suggested that children with ASD perform more poorly on ToM tasks than children with DLD.45 However, one study of 12-year olds tested on the strange-stories task found similar ToM performance in children with HFA and those with DLD, and both groups demonstrated difficulties in understanding the characters’ mental states.46 In a recent study 43 children with DLD (age 4–10 years), 44 children with ASD (age 5–12 years), and 227 typically developing children (age 3–11 years) completed the ToM Storybooks. The task measured the ability to recognize and explicitly explain responses in terms of mental states. Children with ASD showed difficulties in both types of tasks. Children with DLD did not show any difficulties and performed similarly to the TD group.31
The aim of the present study was to contribute to the debate on whether children with ASD and DLD demonstrate ToM difficulties by testing preschool Hebrew-speaking children with a comprehensive ToM battery. Our first research hypothesis was that children with ASD and no language difficulties (ASD-LN) would demonstrate reduced ToM abilities compared to children with TD, given that according to the ToM hypothesis for ASD, difficulty in reasoning about mental states are core deficits in ASD regardless of language skills.1 Our second hypothesis was that children with DLD would demonstrate preserved ToM skills. Previous studies suggested that difficulties in language acquisition may be linked to secondary difficulties in ToM.40 However, some studies suggest that when tasks of low linguistic complexity are used, children with DLD perform similarly to TD peers.43,48 The present study suggests an important contribution to the literature because it includes a comprehensive ToM battery (ToMTB),14 a more complex measure of ToM competence than false-beliefs tasks, as well as a parental questionnaire for assessing ToM (ToMI).15 It also examines young preschool children with ASD and DLD, a population that has not been investigated extensively in an understudied language, which in this case is Hebrew.
Materials and Methods
Participants
Forty-one children across three groups participated in this study. They comprised an ASD group (n = 13, 2 girls and 11 boys) and two control groups, namely, a DLD group (n = 13, 6 girls and 7 boys) and a TD group (n = 15, 6 girls and 9 boys). Children ranged in age from 60 to 73 months (5–6.8 yr olds). A one-way analysis of variance (ANOVA) revealed no significant age differences across the three groups; ASD (M = 66.15, SD = 4.75), DLD (M = 66.13, SD = 4.50) and TD (M = 69.08, SD = 2.84) [F (2, 38) = 2.27, p = 0.12.]. The children with ASD in this study were evaluated by psychiatric specialists and diagnosed according to the Diagnostic and Statistical Manual of Mental Disorders (DSM 5) criteria for autistic disorder [APA 2013 DSM 5].49 The children with DLD were evaluated by both pediatricians and SLPs according to the DSM 5 Diagnostic criteria for language disorder.
Inclusion Criteria for All Participants
All participants were native monolingual Hebrew speakers, with normal vision, hearing, and within-norm nonverbal IQ. According to parental reports, they had no history of neurological problems (such as epilepsy, head injury, or cerebral palsy). All specific inclusion criteria for each group are presented below.
Procedure
All children were recruited by targeting each of the three groups. Confirmation of group assignment was achieved using our inclusion criteria (see below). Children with ASD and DLD were recruited from either special education kindergarten programs or from mainstream kindergartens in which they received speech-language therapy. They were referred to the current study by their speech and language pathologist (SLP). Children with typical development were recruited through ads posted on social media.
The children attended two individual sessions, each lasting approximately one hour. The order of the tests was counterbalanced across participants and groups. The clinical diagnostic measures (see below) and the ToM tasks were administered during these sessions as shown in Figure 1. The study was approved the Research Ethics Committee of Tel-Aviv University and complies with the Declaration of Helsinki. All parents signed a consent form prior to the study commencement.
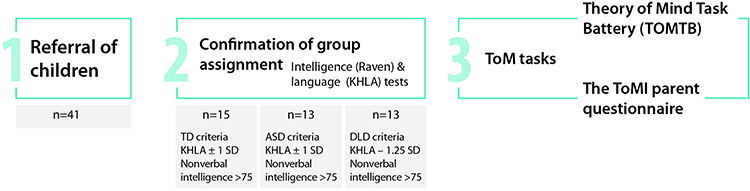 |
Figure 1 A flow chart of the procedure. |
Clinical Diagnostic Procedure and Inclusion Criteria
All children completed intelligence and language assessment as described below to determine IQ, language status, and group assignment.
Intelligence measure. Cognitive nonverbal ability was assessed using Raven’s Coloured Progressive Matrices™ (CPM),50 henceforth termed Raven. The inclusion criterion for participants in the three groups was an IQ cut-off score of 75.
Language measures. Children were classified as DLD in the current study based on the Katzenberger Hebrew Language Assessment for Preschool Children (KHLA). This included a standard z-score of −1.25 or below (at least 1.25 SD below normal scores on the total KHLA score).51
The inclusion criteria for children in the ASD group and the TD group were a standard score within the average range on the KHLA test. Inclusion criteria for the DLD group were based on the norms of the KHLA. Participants in the DLD group scored below average for their age (z-score −1.25).
All participants were assessed by two certified SLPs who also consulted regularly with the authors, as well as certified SLPs. The second author independently reviewed each participant’s evaluation. The reliability between the three SLPs (two certified SLPs and the second author) was 100%.
Theory of Mind Task Battery (TOMTB). This instrument assesses the child’s understanding of different situations that require ToM and consists of 15 test questions within nine tasks presented in ascending difficulty.14 Among the nine tasks, the initial task assesses identification of emotions based on facial expressions. The second task requires understanding desire-based emotions, that is, that people are happy when their desires are fulfilled. The third task requires an understanding of the notion that seeing leads to knowing. The fourth task aims to assess the understanding that people may not see the same things depending on their position, and the fifth task assesses the understanding that visual perception and knowledge drive behavior. The remaining four tasks assess advanced abilities, including first- and second-order false beliefs.
Tasks were presented as pictures in story-book format. Each page had color illustrations and accompanying text that the experimenter read out loud. For all tasks, children were presented with one correct response option and three plausible distractors. The children answered by pointing to the correct picture. Memory control questions were included and had to be answered correctly for the child to receive scores on the test questions. Each ToM question is scored as pass (1) or fail (0).
The ToMI parent questionnaire. The 42-item ToMI is a parent-report questionnaire for assessing the child’s functional level of ToM for children aged 3–17 years.15 Each of the 42 items assesses a particular ToM aspect using items that range from simple content (eg “My child understands that when someone puts on a jacket, it is probably because he/she is cold”) to those that evaluate more complex skills (eg “My child understands that if Bruce is a mean boy and John is a nice boy, Bruce is more likely than John to engage in malicious or hurtful behaviors”). Each item is rated on a 20-unit continuous scale ranging from ‘Definitely Not’ to ‘Definitely.’ Responses for each item are scored by a ruler (possible range = 0–20). Parents specify their response with a vertical mark at the point on the scale that best reflects their answer. The higher the value, the more the extent to which parents believe that the child has a particular ToM skill. The ToMI is considered a socially and ecologically valid measure of ToM in everyday social interactions.15,49,52,53 Cronbach's alpha in the ToMI questionnaire translated to Hebrew is high (0.940) and suggests reliability. In the present study, children’s mothers filled out the questionnaire.
Data Analysis
All the analyses were done using the Statistical Package for Social Science (SPSS) version 26 (IBM, 201953). The correct responses of the ToMTB and the ToMI task were normally distributed with skewness and kurtosis values between 2 and −2 for the three groups. Although the number of girls was higher in the DLD group, no differences were found between girls and boys in performance on the ToMTB and ToMI task in each group. No Pearson’s correlations were found between age, IQ, the HKLA and the performance in the ToM and ToMI tasks. Thus, a series of one-way ANOVA was used to assess the differences between the three groups in age, IQ, the HKLA, the ToMTB, and the TOMI tasks. All the following pairwise comparisons were performed with Bonferroni correction.
Results
Background Measures
Age. The average age in the three groups of participants was similar: the ASD (M = 66.15, SD = 4.76), the TD group (M = 66.13, SD = 4.50) and the DLD group (M = 69.08, SD = 2.84). One-way ANOVA with age as the dependent variable and GROUP as the independent variable showed no main effect for GROUP [F (2, 38) = 2.23, p=0.12].
Nonverbal intelligence. The average score in the three groups of participants on the RAVEN test was similar: The ASD received the highest scores (in percentiles) (M = 85.00, SD = 12.24), following the TD group (M = 77.00, SD = 10.82), and the DLD group had the lowest score (M = 76.92, SD = 7.23). One-way ANOVA with nonverbal intelligence (RAVEN) as the dependent variable and GROUP as the independent variable showed no main effect for GROUP [F (2, 38) = 2.68, p=0.08].
Language measure. Children classified as ASD had the highest z-score on the HKLA (M = −0.02, SD = 0.83), followed by children with TD (M = −0.27, SD = 0.70), and the DLD group, which had the lowest score (M= −2.94, SD = 1.91). One-way ANOVA with HKLA as the dependent variable and GROUP as the independent variable showed the main effect for GROUP [F(2,38) = 22.28, p = 0.0001]. Multiple comparisons with Bonferroni correction showed a significant difference between TD and DLD (p = 0.001), and between ASD and DLD (p = 0.001). No significant difference was found between TD and ASD.
Results of ToM Measures
Figure 2 presents the distribution of the data (in raw scores), for the correct responses in the ToMTB task for each group of participants (TD, DLD, and ASD). The range of results in the TD group was between 8-to-15 correct (M = 11.27, SD = 1.71). The range of results in the DLD group was between 9-to-14 correct (M = 11.15, SD = 1.57), and the range of results in the group of ASD was between 5-to-12 (M = 9.31, SD = 1.80).
 |
Figure 2 Box-and-whisker plots of the percentage of correct scores in the Theory of Mind Task Battery (TOMTB) for each group of participants (TD, DLD, and ASD). Box limits contain the 25th to 75th percentile data. The horizontal lines within each box represent the median. Bars extend to the 10th and 90th percentiles. |
One-way analysis of variance (ANOVA) was performed on the data, with the raw score in the ToMTB task as the dependent variable, and GROUP of participants (TD, DLD and ASD) as the between-subject variable. A main effect was found for GROUP [F(2, 38) = 5.62, p = 0.007, ŋ2 = 0.228] suggesting that the three groups differed in their ToMTB scores, which reflects the understanding of ToM. The following pairwise comparisons confirmed that the mean correct scores of the TD group was higher compared to the mean score of the ASD group (p = 0.013). Also, the mean correct scores of the DLD group were higher compared to the mean correct scores of the ASD group (p = 0.026). However, the mean results of the DLD group were not significantly lower compared to the TD group (p = 1.000).
Figure 3 presents the distribution of the data (mean raw score per item) for the responses in the ToMI task for each group of participants (TD, DLD, and ASD). Note that higher values suggest that the parent is more convinced that the child has ToM skills. The range of results in the TD group was 14.96-to-18.41 (M = 17.02, SD = 0.30). The range of results in the DLD group was 12.05-to-17.77 (M = 14.88, SD = 1.56), and the range of results in the ASD group was 9.38-to-17.09 (M = 14.19, SD = 2.26).
 |
Figure 3 Box-and-whisker plots of the percentage of correct scores The ToMI parent questionnaire for each group of participants (TD, DLD, and ASD). Box limits contain the 25th to 75th percentile data. The horizontal lines within each box represent the median. Bars extend to the 10th and 90th percentiles. Dots represent the outliers. The numbers above the outliers refer to the number of the participant. |
One-way analysis of variance (ANOVA) was performed on the data, with the correct response in the ToMI task as the dependent variable, and GROUP of participants (TD, DLD, and ASD) as the between-subject variable. A main effect was found for GROUP [F(2, 37) = 10.67, p < 0.001, ŋ2 = 0.366] suggesting that the three groups differed in their ToMI scores, which reflects the functional level of ToM. The following pairwise comparisons confirmed that the mean correct scores of the TD group were higher compared to the mean correct scores of the ASD group (p < 0.001) and the DLD group (p = 0.007). However, the mean results of the DLD group were not significantly different compared to the ASD group (p = 0.958).
Discussion
The main objective of this study was to examine ToM abilities in preschool children with ASD-LN. Based on the ToM hypothesis for ASD, which views ToM as the core of the deficit in ASD, we hypothesized that children with ASD would show reduced ToM abilities compared to TD peers. Our findings support this view. Children with ASD showed reduced ToM abilities in a comprehensive ToM assessment (ToMTB) compared to the TD group and the DLD group. However, both groups of children with ASD and children with DLD received lower evaluations from their parents (mothers) on the functional level of ToM (ToMI) compared to the TD group, suggesting that in everyday life, both children with ASD and children with DLD may exhibit social difficulties. In the remainder of the discussion, we will elaborate on these findings and their implications.
As expected, the first finding of the present study suggests that the group of children with ASD-LN present worse ToM skills compared to the TD group, based on the direct assessment of ToM (ToMTB) and the parent questionnaire (ToMI). This finding supports a dissociation between language and ToM and is therefore in agreement with a modular view of ToM according to which ToM processes can be delayed or deficient independently of language and IQ. According to this view, there is an underlying neurocognitive “theory-of mind mechanism” (ToMM). This mechanism is in many cases attributed to the medial frontal cortex, that is critically involved in selective belief–desire reasoning that includes both the ability to represent intentions and beliefs as well as the ability to inhibit the representation of one’s own intention or belief and to select the other’s belief or intention in order to understand his or her point of view.54 This does not mean that language cannot be used to facilitate or mediate ToM comprehension,25,26 but that even when language is intact, some difficulties may occur. Overall, the findings on reduced ToM abilities in children with ASD-LN both in the direct assessment and the parent questionnaire suggest that the children with ASD-LN do not only demonstrate difficulties in ToM tasks presented in a test but also cope with difficulties in understanding the social world in everyday life.
The second main finding of the present study suggests mixed results concerning ToM skills in children with DLD. As expected, children with DLD performed similarly to TD and better than ASD-LN on the ToMTB. However, on the parent questionnaire for assessing ToM competencies (ToMI), children with DLD received lower scores compared to TD and scores similar to the ASD-LN group. It is plausible that the ability to respond nonverbally on the ToMTB enabled the children with DLD to demonstrate their competence to identify and understand emotions, different perspectives, and false beliefs. Other studies also suggest that in tasks with low linguistic demands, children were able to demonstrate ToM abilities that are similar to their TD peers.42,43 Miller,55 for example, showed that DLD children performed below their TD-matched peers on ToM verbal tasks but not on ToM low verbal tasks. However, as mentioned earlier, in the ToMI children with DLD did not demonstrate the same use of ToM skills in real-life situations as TD peers. Unlike the ToMTB, the ToMI is based on the way parents judge ToM functioning in everyday life. In dynamic real-life situations,56 there could be many distractions and the child has to respond quickly, automatically,57 and verbally. Children with DLD are challenged in such situations. Since language may assist and facilitate the representation of different perspectives, false beliefs and mental states,27,58 it is plausible that a developmental language disorder has a detrimental effect on ToM performance at least in everyday situations in which quick, spontaneous responses are required. Consistent with our finding that children with DLD have reduced ToM functioning in everyday life situations, there is evidence to suggest that children with DLD are socially withdrawn,59 and are prone to being victimized,60 possibly because compared to their peers, their social skills are less developed.
Taken together, a possible conclusion of the present findings is that different pathways may lead children with ASD-LN and children with DLD to exhibit similar difficulties in ToM functioning in everyday life. The core deficit in children with ASD-LN relates primarily to a direct deficit in the neurocognitive ToM system, whereas the core deficit in children with DLD relates primarily to language skills and possibly other attentional factors. Further studies that would assess the link between executive functions, including attention, working memory, and inhibition to ToM abilities in both children with ASD and DLD are needed in order to support this conclusion. Although it is beyond the scope of this study, there is a need for neuro- imaging study to determine how brain systems involved in ToM and language are affected in children with ASD-LN and children with DLD.
Limitations
The present study shows that 5-to-6-year-old preschool children with ASD-LN present reduced ToM abilities compared to TD peers on both a direct comprehensive assessment and a parent questionnaire. However, preschool 5-to-6-year-old children with DLD present less developed skills compared to TD peers and, like the ASD-LN group, only on the parent questionnaire. The sample of the present study is relatively small; the number of girls did not match the number of boys, and additional explanatory factors, such as executive functions, were not assessed. Despite these limitations, the present study adds to our understanding of ToM abilities in children with neurodevelopmental difficulties and adds to the scarce data on ToM in preschool children with normal nonverbal intelligence and without structural language difficulties.
Conclusion
The population of children with ASD is heterogeneous in terms of their nonverbal intelligence, language, and ToM abilities. Thus, identifying groups of children with ASD with different profiles is essential to propose appropriate therapeutic programs and to implement adequate intervention strategies. The present findings suggest that the subgroup of children with ASD-LN may demonstrate difficulties with ToM regardless of their nonverbal intelligence and language skills. Thus, for this subgroup, working directly on language abilities may not necessarily improve ToM skills. Other intervention strategies for developing ToM skills should be considered, such as discussing books, movies, television shows and short videos with social context, developing pretend play, and visual representation of false beliefs, complex emotions, and different perspectives. However, for children with DLD, developing language abilities that support ToM, such as complex syntactic structures and mental vocabulary26,27 might be a more fruitful strategy. Children with both ASD and language difficulties should be treated with both types of strategies described above.
The findings of the present study highlight the importance of understanding the reasons that led to reduced ToM performance. To this aim, a comprehensive assessment is needed that includes nonverbal IQ, language abilities, and real-life executive functions. It is recommended to assess ToM with both a comprehensive battery that allows nonverbal responses and a parent open-ended questionnaire for a view into their performance in everyday life. Such a comprehensive evaluation may shed light on their function in different contexts and facilitate planning appropriate treatment.
Acknowledgments
The authors wish to thank the children and families for their participation in this study. We wish to acknowledge Dr. Ariela Jokel (Ph.D), Moran Kadrya and Revital Tsuriel MA students in the Department of Communication Disorder, Tel-Aviv University, for assistance in translating the ToMTB and the ToMI.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Baron-Cohen S, Leslie AM, Frith U. Does the autistic child have a “theory of mind”? Cognition. 1985;21(1):37–46. doi:10.1016/0010-0277(85)90022-8
2. Baron-Cohen S. The autistic child’s theory of mind: a case of specific developmental delay. J Child Psychol Psychiat. 1989;30(2):285–297. doi:10.1111/j.1469-7610.1989.tb00241.x
3. Frith U. Autism and “Theory of Mind.”. In: Gillberg C, editor. Diagnosis and Treatment of Autism. Boston: Springer; 1989:33–52. doi:10.1007/978-1-4899-0882-7_4
4. Chiu HM, Chen CT, Tsai CH, et al. Theory of mind predicts social interaction in children with autism spectrum disorder: a two-year follow-up study. J Autism Dev Disord. 2022. doi:10.1007/s10803-022-05662-4
5. Baron-Cohen S, Campbell R, Karmiloff-Smith A, Grant J, Walker J. Are children with autism blind to the mentalistic significance of the eyes? Br J Dev Psychol. 1995;13(4):379–398. doi:10.1111/j.2044-835X.1995.tb00687.x
6. Tager-Flusberg H. Evaluating the theory-of-mind hypothesis of autism. Curr Dir Psychol Sci. 2007;16(6):311–315. doi:10.1111/j.1467-8721.2007.00527.x
7. Fisher N, Happe F, Dunn J. The relationship between vocabulary, grammar, and false belief task performance in children with autistic spectrum disorders and children with moderate learning difficulties. J Child Psychol Psychiat. 2005;46(4):409–419. doi:10.1111/j.1469-7610.2004.00371.x
8. Tager-Flusberg H, Joseph RM. How language facilitates the acquisition of false-belief understanding in children with autism. In: Astington JW, Baird JA, editors. Why Language Matters for Theory of Mind. New York: Oxford University Press; 2005:298–318.
9. Kjelgaard MM, Tager-Flusberg H. An investigation of language impairment in autism: implications for genetic subgroups. Lang Cogn Process. 2001;16(2–3):287–308. doi:10.1080/01690960042000058
10. Roberts JA, Rice ML, Tager–Flusberg H. Tense marking in children with autism. Appl Psycholinguist. 2004;25(3):429–448. doi:10.1017/S0142716404001201
11. Dennett DC. Beliefs about beliefs. Behav Brain Sci. 1978;1(4):568–570. doi:10.1017/S0140525X00076664
12. Perner J, Leekam SR, Wimmer H. Three-year olds’ difficulty with false belief: the case for a conceptual deficit. Br J Dev Psychol. 1987;5(2):125–137. doi:10.1111/j.2044-835X.1987.tb01048.x
13. Beaudoin C, Leblanc É, Gagner C, Beauchamp MH. Systematic review and inventory of theory of mind measures for young children. Front Psychol. 2020;10:2905. doi:10.3389/fpsyg.2019.02905
14. Hutchins TL, Bonazinga LA, Prelock PA, Taylor RS. Beyond false beliefs: the development and psychometric evaluation of the perceptions of children’s theory of mind measure—experimental version (PCToMM-E). J Autism Dev Disord. 2008;38(1):143–155. doi:10.1007/s10803-007-0377-1
15. Hutchins TL, Prelock PA, Bonazinga L. Psychometric evaluation of the theory of mind inventory (ToMI): a study of typically developing children and children with autism spectrum disorder. J Autism Dev Disord. 2012;42(3):327–341. doi:10.1007/s10803-011-1244-7
16. Altschuler M, Sideridis G, Kala S, et al. Measuring individual differences in cognitive, affective, and spontaneous theory of mind among school-aged children with autism spectrum disorder. J Autism Dev Disord. 2018;48(11):3945–3957. doi:10.1007/s10803-018-3663-1
17. Apperly IA. What is “theory of mind”? Concepts, cognitive processes and individual differences. Q J Exp Psychol. 2012;65(5):825–839. doi:10.1080/17470218.2012.676055
18. Leekam SR, Perner J. Does the autistic child have a metarepresentational deficit? Cognition. 1991;40(3):203–218. doi:10.1016/0010-0277(91)90025-Y
19. Happe FGE, The role of age and verbal ability in the theory of mind task performance of subjects with autism. Child Dev. 1995;66(3):843–855. doi:10.2307/1131954
20. Bowler DM. “Theory of mind” in Asperger’s syndrome. J Child Psychol Psychiatry. 1992;33(5):877–893. doi:10.1111/j.1469-7610.1992.tb01962.x
21. Ozonoff S, Pennington BF, Rogers SJ. Executive function deficits in high-functioning autistic individuals: relationship to theory of mind. J Child Psychol Psychiatry. 1991;32(7):1081–1105. doi:10.1111/j.1469-7610.1991.tb00351.x
22. Loucas T, Charman T, Pickles A, et al. Autistic symptomatology and language ability in autism spectrum disorder and specific language impairment: autistic symptomatology and language ability. J Child Psychol Psychiatry. 2008;49(11):1184–1192. doi:10.1111/j.1469-7610.2008.01951.x
23. Milligan K, Astington JW, Dack LA. Language and theory of mind: meta-analysis of the relation between language ability and false-belief understanding. Child Dev. 2007;78(2):622–646. doi:10.1111/j.1467-8624.2007.01018.x
24. Durrleman S, Delage H. Autism spectrum disorder and specific language impairment: overlaps in syntactic profiles. Lang Acquis. 2016;23(4):361–386. doi:10.1080/10489223.2016.1179741
25. Steele S, Joseph RM, Tager-Flusberg H. Brief report: developmental change in theory of mind abilities in children with autism. J Autism Dev Disord. 2003;33(4):461–467. doi:10.1023/A:1025075115100
26. De Villiers J. Language and theory of mind: what are the developmental relationships. In: Baron-Cohen S, Tager-Flusberg H, Cohen DJ, editors. Understanding Other Minds: Perspective from Developmental Neuroscience. Oxford: Oxford University Press; 2000:83–123.
27. Durrleman S. Mentalizing: what’s language got to do with it? Lang Acquis. 2020;27(3):255–275. doi:10.1080/10489223.2020.1769624
28. Durrleman S, Bentea A, Prisecaru A, Thommen E, Delage H. Training syntax to enhance theory of mind in children with ASD. J Autism Dev Disord. 2022. doi:10.1007/s10803-022-05507-0
29. Lind SE, Bowler DM. Language and theory of mind in autism spectrum disorder: the relationship between complement syntax and false belief task performance. J Autism Dev Disord. 2009;39(6):929–937. doi:10.1007/s10803-009-0702-y
30. Charman T, Baron-Cohen S. Understanding drawings and beliefs: a further test of the metarepresentation theory of autism: a research note. J Child Psychol Psychiat. 1992;33(6):1105–1112. doi:10.1111/j.1469-7610.1992.tb00929.x
31. Bulgarelli D, Testa S, Molina P. Theory of mind development in Italian children with specific language impairment and autism spectrum disorder: delay, deficit, or neither? J Autism Dev Disord. 2022:1. doi:10.1007/s10803-021-05389-8.
32. Apperly IA, Butterfill SA. Do humans have two systems to track beliefs and belief-like states? Psychol Rev. 2009;116(4):953–970. doi:10.1037/a0016923
33. Eigsti IM, Irvine CA. Verbal mediation of theory of mind in verbal adolescents with autism spectrum disorder. Lang Acquis. 2021;28(2):195–213. doi:10.1080/10489223.2021.1877705
34. Astington JW, Jenkins JM. A longitudinal study of the relation between language and theory-of-mind development. Dev Psychol. 1999;35(5):1311–1320. doi:10.1037/0012-1649.35.5.1311
35. Sellabona ES, Sánchez CR, Majoral EV, Guitart ME, Caballero FS, Ortiz JS. Labelling improves false belief understanding. A training study. Span J Psychol. 2013;16:E6. PMID: 23866253. doi:10.1017/sjp.2013.8
36. Schick B, de Villiers P, de Villiers J, Hoffmeister R. Language and theory of mind: a study of deaf children. Child Dev. 2007;78(2):376–396. doi:10.1111/j.1467-8624.2007.01004.x
37. Lindgren KA, Folstein SE, Tomblin JB, Tager-Flusberg H. Language and reading abilities of children with autism spectrum disorders and specific language impairment and their first-degree relatives. Autism Res. 2009;2(1):22–38. doi:10.1002/aur.63
38. Bishop DVM. Why is it so hard to reach agreement on terminology? The case of developmental language disorder (DLD): terminology and the case of DLD. Int J Lang Commun Disord. 2017;52(6):671–680. doi:10.1111/1460-6984.12335
39. Leonard LB. Specific language impairment across languages. Child Dev Perspect. 2014;8(1):1–5. doi:10.1111/cdep.12053
40. Spanoudis G. Theory of mind and specific language impairment in school-age children. J Commun Disord. 2016;61:83–96. doi:10.1016/j.jcomdis.2016.04.003
41. Nilsson KK, de López KJ. Theory of mind in children with specific language impairment: a systematic review and meta-analysis. Child Dev. 2016;87(1):143–153. doi:10.1111/cdev.12462
42. Bulgarelli D, Molina P. Teoria della mente nei bambini con disturbo specifico di linguaggio: una questione di competenza o di Performance? G Ital Psicol. 2013;4:761–784. doi:10.1421/76946
43. Loukusa S, Mäkinen L, Kuusikko-Gauffin S, Ebeling H, Moilanen I. Theory of mind and emotion recognition skills in children with specific language impairment, autism spectrum disorder and typical development: group differences and connection to knowledge of grammatical morphology, word-finding abilities and verbal working memory: social perception in SLI, ASD and TD. Int J Lang Commun Disord. 2014;49(4):498–507. doi:10.1111/1460-6984.12091
44. Farrar MJ, Johnson B, Tompkins V, Easters M, Zilisi-Medus A, Benigno JP. Language and theory of mind in preschool children with specific language impairment. J Commun Disord. 2009;42(6):428–441. doi:10.1016/j.jcomdis.2009.07.001
45. Shields J, Varley R, Broks P, Simpson A. Social cognition in developmental language disorders and high-level autism. Dev Med Child Neurol. 2008;38(6):487–495. doi:10.1111/j.1469-8749.1996.tb12109.x
46. Gillott A, Furniss F, Walter A. Theory of mind ability in children with specific language impairment. Child Lang Teach Ther. 2004;20(1):1–11. doi:10.1191/0265659004ct260oa
47. Schaeffer J. Linguistic and cognitive abilities in children with specific language impairment as compared to children with high-functioning autism. Lang Acquis. 2018;25(1):5–23. doi:10.1080/10489223.2016.1188928
48. van Buijsen M, Hendriks A, Ketelaars M, Verhoeven L. Assessment of theory of mind in children with communication disorders: role of presentation mode. Res Dev Disabil. 2011;32(3):1038–1045. doi:10.1016/j.ridd.2011.01.036
49. Guha M. Diagnostic and Statistical Manual of Mental Disorders: DSM-5.
50. Raven JC, Court JH, Raven J. Coloured Progressive Matrices. Oxford Psychological Press; 1995.
51. Katzenberger I, Meilijson S. Hebrew language assessment measure for preschool children: a comparison between typically developing children and children with specific language impairment. Lang Test. 2014;31(1):19–38. doi:10.1177/0265532213491961
52. Hutchins TL, Prelock PA, Chace W. Test-retest reliability of a theory of mind task battery for children with autism spectrum disorders. Focus Autism Other Dev Disabl. 2008;23(4):195–206. doi:10.1177/1088357608322998
53. IBM Corp. IBM SPSS Statistics for Windows, Version 26.0. Armonk, NY: IBM Corp; 2019.
54. Leslie AM, Friedman O, German TP. Core mechanisms in ‘theory of mind. Trends Cogn Sci. 2004;8(12):528–533. doi:10.1016/j.tics.2004.10.001
55. Miller CA. False belief and sentence complement performance in children with specific language impairment. Int J Lang Commun Disord. 2004;39(2):191–213. doi:10.1080/13682820310001616994
56. Hutchins TL, Prelock PA, Morris H, Benner J, LaVigne T, Hoza B. Explicit vs. applied theory of mind competence: a comparison of typically developing males, males with ASD, and males with ADHD. Res Autism Spectr Disord. 2016;21:94–108. doi:10.1016/j.rasd.2015.10.004
57. Schneider D, Slaughter VP, Dux PE. Current evidence for automatic theory of mind processing in adults. Cognition. 2017;162:27–31. doi:10.1016/j.cognition.2017.01.018
58. Lindquist KA, Satpute AB, Gendron M. Does language do more than communicate emotion? Curr Dir Psychol Sci. 2015;24(2):99–108. doi:10.1177/0963721414553440
59. Chen J, Justice LM, Rhoad-Drogalis A, Lin TJ, Sawyer B. Social networks of children with developmental language disorder in inclusive preschool programs. Child Dev. 2020;91(2):471–487. doi:10.1111/cdev.13183
60. Redmond SM. Peer victimization among students with specific language impairment, attention-deficit/hyperactivity disorder, and typical development. LSHSS. 2011;42(4):520–535. doi:10.1044/0161-1461(2011/10-0078)
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.