Back to Journals » Infection and Drug Resistance » Volume 15
Comparing the Treatment Outcomes of Tuberculosis Patients in a Private Clinic with a Governmental Health Center in Jimma City, Ethiopia: Retrospective Study
Authors Abera EG ![]() , Yeshitla W, Kene K
, Yeshitla W, Kene K ![]() , Gerema U
, Gerema U ![]() , Assefa Y
, Assefa Y
Received 6 January 2022
Accepted for publication 1 May 2022
Published 12 May 2022 Volume 2022:15 Pages 2491—2511
DOI https://doi.org/10.2147/IDR.S354855
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Eyob Girma Abera,1 Wondyifraw Yeshitla,1 Kumsa Kene,2 Urge Gerema,2 Yared Assefa3
1Department of Public Health, Jimma University, Jimma, Oromia, Ethiopia; 2Department of Biomedical Science, Jimma University, Jimma, Oromia, Ethiopia; 3Department of Civil Engineering, Jimma University, Jimma, Oromia, Ethiopia
Correspondence: Eyob Girma Abera, Department of Public Health, Jimma University, PO Box 378, Jimma University, Jimma, Oromia, Ethiopia, Tel +251910093601, Email [email protected]; [email protected]
Background: Tuberculosis (TB) is a common and often deadly infectious disease caused by various strains of mycobacterium, usually mycobacterium tuberculosis in humans. The disease has major causes of morbidity and mortality, particularly where the diagnostic and control program is not far extended.
Objective: To compare the treatment outcomes of tuberculosis patients in a private clinic with a governmental health center in Jimma city, Ethiopia.
Methods: A 10-year cross-sectional retrospective systemic record review was conducted to compare the treatment outcomes, and to describe the socio-demographic factors associated with the outcome in a private clinic with a governmental health center in Jimma city, Jimma, Ethiopia from September 12, 2007, to September 10, 2017. Finally, SPSS/EPI INFO analyzed data.
Results: The present study revealed that within a 10 year duration the private clinic gives anti-TB treatment coverage for 582 patients whereas the governmental health center treats 510 patients. The treatment success rate of the private clinic is 98.1% which is 1.03-fold that of the governmental health center (95.3%); while the treatment failure of the private clinic was 0.2%, but there was no treatment failure in the governmental health center.
Conclusion: Both sectors achieved the expected WHO targets by newly recommended strategy for TB treatment, DOTS (Directly Observed Treatment Short Course) and treatment success is much better to standard. This shows good progress of DOTS strategy and a decrease of noncompliance in this area. Age, educational level, and the types of TB diagnosis and treatment outcome of the patients were statistically associated in both sectors. Better counseling and awareness about the disease should have to be given for every anti-TB treatment receiving patients, despite their educational level and occupational status in both sectors.
Keywords: tuberculosis, treatment outcome, comparing, governmental health center, private clinic
Introduction
Background Information
Tuberculosis (TB) is an infectious airborne disease mostly caused by Mycobacterium tuberculosis, a rod-shaped “Acid fast” bacillus; it can also be caused by Mycobacterium Bovis and Africanum.1 In 1991, the World Health Organization (WHO) assembly announced Tuberculosis as a global emergency due to its global burden.2 The disease affects individuals of all ages and both sexes within every socioeconomic group. However, there are high level risk factors that facilitate developing the disease, such as HIV, malnutrition, and young age; there are also emerging risk factors such as overcrowded living conditions, use of immunosuppressive drugs, smoking habit, and diabetes.3 In addition, consumption of raw milk containing M. Bovis is a possible way of being infected by TB, though it is much less frequent.4 TB is curable and preventable; 85% of TB patients can be successfully treated with a 6-month anti-TB drug regime.5 Following COVID-19, TB is the second leading fatal infectious diseases, and the 13th cause of death. In 2020, 1.5 million people died of TB (including 214,000 people with HIV). An estimated 10 million people (including 1.1 million children) fell ill with TB worldwide.6
TB incidence falls by 1.5% per year globally, but this is challenged by the emergence and increase in drug resistance TB worldwide; furthermore, the association of TB and HIV infections has hindered TB control programs with a poor treatment outcome, and TB still remains one of the world’s major threats to public health.6
Ethiopia ranks third in Africa and seventh among the 22 highest TB burdened countries in the world.7 TB incidence has declined by 21% from the 2015 estimate; the improved detection rate in 2019/2020 was 71%, and TB treatment success of 90% with an 80% cure rate showed a huge improvement. Since 2009, more than 4,900 drug-resistant TB patients were detected and enrolled to second line treatment.8
To achieving one of the three targets of the global End TB Strategy by improving treatment compliance with increasing TB cure rate, Ethiopia implemented the Directly Observed Treatment Short Course (DOTS) strategy in 1992 as a pilot in Arsi and Bale zones of Oromia region. Currently it is provided in almost all public hospitals and health centers as well as in private and non-governmental health facilities. Under the DOTS strategy, treatment outcome is an important indicator of TB control programs. Socio-demographic factors including gender, age, and residence of the patients and the form of TB have been reported to affect the treatment outcome and performance of DOTS services in various studies. However, the effect of the type of health facility has not been studied in Ethiopia so far. Therefore, this study was initiated to determine the treatment outcome of TB patients in private and government health facilities, and identify factors associated with an unsuccessful outcome in each institution with comparing the 10-year reviewing record of the patients.9 Despite there being no difference with the treatment or management of TB in both settings, the study aims to compare the treatment outcome considering the same setup implementation, and this finding will help to outcast which institution has in favors of the problem for the unsuccessful treatment outcome. Hence, the finding will put a direction and to fill the gaps by comparing in each setting.
Statement of the Problem
Tuberculosis is still a problem in Ethiopia with the emergence of a high prevalence of MDR-TB that has threatened to be a drawback factor for the TB control program. We can prevent the emergence of acquired resistance by using good practice, which is the simplest and easiest way of preventing the complicated and serious disease.10 There is only one cross-sectional retrospective cohort study which has been conducted in Addis Ababa in 2012 to compare the treatment outcome between government and private clinic. This study will illustrate a good understanding between the treatment outcome and the underlying factors that could help in program implementation and favors for the successful outcome that later will help for the improvement of the country healthcare system, especially for the TB program. If we know the key factors for success, we can emphasize these and can avoid the unintended consequences.11
Significance of the Study
The study helps to describe the association of social demographic factors with Tuberculosis patients and their treatment outcome, which is useful to assess and compare the treatment outcomes of tuberculosis patients in government health centers and private clinics since there is no previous similar study in the area. Additionally, it has a value to compare the extent of tuberculosis treatment burden which is handled between the sectors. The finding potentially contributes to formulate strategies to give the appropriate tuberculosis care and to sense what really affects the outcome. Furthermore, it will be used as a baseline for further studies.
Literature Review
TB has been present in the human population for many years. Egyptian mummies from 2400 BC show signs of infection from mycobacterium TB, earlier known as consumption. The diseases were thought to arise spontaneously in each affected person until 1865, at which point a French doctor demonstrated that TB could be spread from human to cattle. Over the years the bacteria were identified and, in 1943, streptomycin, the first antibiotic to be used in humans, was developed.12
A cross-sectional survey was conducted by the National tuberculosis control program (NTCP) in Kampala, Uganda, to compare the appropriateness of tuberculosis care in private and public clinics, and the extent of the tuberculosis burden handled in the private sector from June to August 1999. Based on the result, 114 clinics (104 private, 10 public) were surveyed, and 41% of the private clinics saw three or more new tuberculosis patients each month. None of the public or private clinics met all standards for appropriate tuberculosis care. Only 24% of all clinics adhered to WHO-recommended treatment guidelines. Public clinics, younger practitioners, and practitioners with advanced degrees were most likely to provide appropriate care for tuberculosis. TIt is recommended that the private sector cares for many tuberculosis cases in Kampala; however, a new program that offers continuing medical education is needed to improve tuberculosis care and to increase awareness of national guidelines for tuberculosis care.13
Demographic, clinical, and laboratory data were collected prospectively by TLCP to assess tuberculosis services and treatment outcomes in private and public healthcare facilities in Thailand during 2004–2006 from routine medical and laboratory records for all patients with a diagnosis of TB in the national infectious diseases hospital or any public or private facility in the four provinces. Patients were classified according to TB type, previous TB history, and TB treatment outcome using WHO categories. However, the analysis is limited to new pulmonary TB patients registered for TB treatment between 1 October 2004 and 30 September 2006 with a known treatment outcome. Patients previously treated for TB or known to have multidrug-resistant TB (MDR-TB) were excluded from the analysis, as such patients are known to have markedly different treatment outcomes than patients never treated for TB, also patients diagnosed with EPTB were excluded. Between 1 October 2004 and 30 September 2006, 8,392 new pulmonary TB patients were treated in public and private facilities in the Active Surveillance Network. Seventy-three patients with MDR-TB, 461 who transferred in, 161 for whom the diagnosis was changed, and 171 with unknown outcomes were excluded, leaving 7,526 patients eligible for analysis. Of these, 4,539 (60%) were treated in small public facilities, 2,275 (30%) in large public facilities, and 712 (10%) in private facilities. Treatment outcomes were unsuccessful for private sector patients (237, 33%) and for patients in small (1,018, 23%) and large public facilities (655, 29%). Default rates were highest in private facilities. Among patients with poor outcomes, 218 (92%) private patients defaulted compared with 412 (41%) in small and 261 (40%) in large public facilities (P<0.01, both comparisons).14
A cross-sectional study was conducted to assess factors associated with tuberculosis treatment outcomes among tuberculosis patients attending tuberculosis treatment centers in 2016–2017 in Mogadishu, Somalia. In this study, treatment outcomes were successful among 315 (81.8%) TB patients (P<0.001). Specific successful treatment outcomes included cured (237, 61.6%) and treatment completed (78, 20.3%). Specific unsuccessful treatment outcome included treatment failed (26, 6.8%), defaulters (24, 6.2%), transferred (11, 2.9%), and died (9, 2.3%) (P=0.043). Multivariate analysis indicated that marital status, education level, HIV status, and treatment category influenced treatment outcome. Married patients were more likely to have a successful treatment outcome (OR=0.3, 95% CI=0.1–0.6) as compared to the unmarried patients. Illiterate patients, patients who had attended madrassa, and elementary education were less likely (OR=4.1, 95% CI=1–15.9; OR=4.5, 95% CI=1.2–17; OR=5.9, 95% CI=1.6–21.8, respectively) to achieve successful treatment outcome compared to patients who had secondary education. Being HIV positive lowered the chances of successful treatment outcome (OR=4.4, 95% CI=1.1–17.7) compared to the HIV negative patients. New TB treatment cases were more likely to have successful treatment outcome (OR=5.2, 95% CI=2.9–9.2) as compared to re-treatment cases Patients with moderate knowledge on TB were less likely to achieve a successful treatment outcome (OR=2.4, 95% CI=1–5.6) compared to those with knowledge. TB patients’ attitude and institutional factors did not significantly influence treatment outcome.15
A cross-sectional retrospective cohort study was conducted in Addis Ababa in 2012. The 75 DOT-providing health facilities that were eligible included eight public hospitals, 13 private hospitals, 31 public health centers, and 23 private clinics. Two public hospitals, two private hospitals, five public health centers, and five private clinics were randomly selected for the study. To evaluate TB Unit registers for completeness, 18 items were grouped into three sections with six items each, representing demographic information (patient name, clinic ID, address, name and address of contact, age, and sex) and TB care information (TB diagnosis, TB category, treatment regimen, treatment start date, daily medication dose, treatment outcome). The result shows a total of 2,140 TB cases were registered at the study sites during the study period, which summarizes the distribution of PTB–, PTB+, and EPTB cases by category of health facility. Proportions of EPTB were higher in private hospitals (59.8%) and clinics (41.8%) than in public hospitals (37.3%) and health centers (36.8%). There were fewer PTB– cases in private hospitals (10.9%) and private clinics (33.5%) than in public hospitals (35.1%) and clinics (38.8%), whereas PTB+ cases were registered in approximately equal proportions, ranging from 21.0–27.6% across all categories of facilities. However, substantial variations were observed between facilities. Interestingly, PTB+ patients had lower percentages of favorable outcomes recorded (73.8%) than either PTB– (80.0%) or EPTB (79.2%) patients. Public (63.8%) and private (71.2%) hospitals recorded lower percentages of favorable outcomes than public (80.4%) and private (78.5%) clinics. Finally, in addition to other factors, favorable outcomes were also strongly associated with record completion in the TB unit registers.11
Objectives
General Objective
To compare the treatment outcomes of tuberculosis patients in a private clinic with a governmental health center in Jimma city, Ethiopia.
Specific Objectives
- To describe the socio-demographic factors associated with tuberculosis patients in Jimma Medium Clinic and Jimma Health Center, Jimma town, Oromia region, Ethiopia from September 12, 2007, to September 10, 2017.
- To assess the treatment outcomes of tuberculosis patients in Jimma town.
- To compare the treatment outcomes of tuberculosis patients in Jimma Medium Clinic with Jimma Health Center, which include type of tuberculosis diagnosis, category of patients, and various outcomes of treatment.
- To assess the effectiveness of TB control program strategies.
Materials and Methods
Study Design, Setting, and Participants
A 10-year retrospective systemic record review was conducted in Jimma Health Center and Jimma Medium Clinic since September 12, 2007, to September 10, 2017. All patients who had been following anti-TB treatment used from the registration book were selected; however, those patients who were diagnosed and started treatment in JHC and JMC then transferred to another health institution for completions of a regimen, and patients with the treatment outcome not recorded on the TB registration book have been excluded.
Study Population
Jimma town is found 256 km southwest from the capital city, Addis Ababa. The town has a total population of 128,306, of whom 67,482 are men and 60,824 women. With an area of 50.52 square kilometers, Jimma has a population density of 2,394.30, and all are urban inhabitants.16 The study was conducted in Jimma Health Center and Jimma Medium Clinic. The public health center gives service for 42,164 people in its catchment area, and the private medium clinic has 40,104 people in its catchment area. The public health center gives service for those coming out of its catchment area by 19 different categories of health professionals and 19 supportive staff. The private medium clinic gives service by 22 different categories of health professional and 21 supportive staff. According to the 2017 Jimma town health bureau, the town has one specialized hospital, one zonal hospital, three private hospitals, four health centers, two NGOs, two health posts, and 28 private clinics. Among them, TB treatment is available in six private clinics, three private hospitals, two NGOs, and the rest are all governmental health sectors.17
Data Collection
A structured questionnaire was used for collecting the data. The questionnaire includes items on sociodemographic characteristics, biometric and biomedical indicators; those are Treatment outcome, Category of the Patient, and Types of TB diagnosis. Data were collected by the trained and assigned TB and leprosy unit personnel in the private and public health sectors.
Variables and Measurements
Independent Variable
- Age
- Sex
- Occupational status
- Educational status
Biometric and Biomedical Indicators
- Treatment outcome: It is the result obtained after the initiation of the treatment of TB (Success, Complete, Cured, Failure, Defaulter, Died)
- Successfully Treated: A patient who was cured or completed treatment
- Completed Treatment: Finishing treatment but without bacteriology result at the end of treatment.
- Cured: Finishing treatment with negative bacteriology result at the end of treatment.
- Failure: Remaining smear positive at 5 months despite correct intake of medication.
- Defaulted Treatment: Patients who interrupted their treatment for two consecutive months or more after registration.
- Died: Patients who died from any cause during the course of treatment.9
2. Category of the Patient: (New, relapse, transfer in, others)
- New case (N): A patient who has never had treatment for TB or has been on anti-TB treatment for less than 4 weeks.
- Relapse: A patient who has been declared or treatment completed of any form of TB.
- In the past but who reports back to the healthcare and is found to be AFB
- Smear positive or culture positive
- Transfer out (T): A patient who started treatment and has been transferred to another health facility and for whom the treatment outcome is not known at the time of evaluation of treatment results.
- Others (O): A patient who does not fit in any of the above-mentioned categories (eg, a PTB smear negative patient who returns after treatment interruption).18
3. Types of TB diagnosis:
- Extra pulmonary TB /EPTB/: TB, which involve other organ except the lungs.
- Pulmonary TB /PTB/: are two types.
- /PTB +VE/: A patient with at least two sputum specimens which are positive for AFB by microscopy or a patient with only one sputum specimen which was positive for AFB by microscopy and chest radiographic abnormalities consistent with Active PTB.
- /PTB –VE/: A patient with symptoms suggestive of TB with at least two sputum specimens which were negative for AFB by microscopy and with a chest radiographic abnormalities consistent with active pulmonary TB or a patient with two sets of at least two sputum specimens taken at least 2 weeks apart and which were negative for AFB by microscopy and radiographic abnormalities consistent with pulmonary TB and lack of clinical response to 1 week of broad spectrum antibiotic therapy.19
Data Processing and Analysis
The collected data were checked for completeness, and then were double entered, validated, and cleaned using EpiData and analyzed using SPSS.
Result
Jimma Health Center (Governmental) Result
A total of 510 patients was registered at the Jimma Health Center from September 11, 2006, to September 10, 2017, and all patients were included in a study that were diagnosed and started their treatment at a TB-Leprosy follow-up clinic. Males constituted 46.3% (n=236) and females constituted 53.7% (n=274). The majority of patients were between the ages of 15–49 years, which accounted for 82.2% (n=419), with a mean age of 34.4 years. Among those patients, 91.2% (n=465) were new, 3.1% (n=16) were transferred in, 3.7% (n=19) were relapsed, and 2.0% (n=10) were others. Regarding the category of TB, extra pulmonary tuberculosis constituted 48.4% (n=247), smear positive pulmonary tuberculosis was 47.6% (n=243), while smear negative pulmonary tuberculosis was 3.9% (n=20). Fifty patients had data for occupational and educational level status, which had been taken from March 12–August 11. The majority (34%, n=17) of patients were educated in higher education and 20% (n=10) of patients were governmental employees (Table 1).
 |
Table 1 Distribution of Sex, Age, Educational Level, Occupational Status, Category of Patients, and Types of TB Diagnosis in Jimma Health Center, Jimma Town, Oromia Region, South West Ethiopia from September 11, 2006–September 10, 2017 |
According to treatment outcome, 49.2% (n=251) completed treatment, 46.1% (n=235) were cured, 4.1% (n=21) defaulted, 0.6% (n=3) died, with no treatment failure. The overall treatment success rate in the area was 95.3% (n=486, cure plus treatment complete). The overall defaulting rate was 4.1% (n=21) (Table 2).
 |
Table 2 Distribution of TB Treatment Outcome in Jimma Health Center, Jimma Town, Oromia Region, South West Ethiopia from September 11, 2006–September 10, 2017 |
Three patients died in all types of TB, and they were new. In total, 94.3% (n=233) EPTB patients completed anti-TB treatment and 15% (n=3) of pulmonary smear negative patients were defaulters. A total of 96.7% (n=235) smear positive pulmonary patients were cured (Table 3).
 |
Table 3 Distribution of Category of TB and Patient Diagnosis with Treatment Outcome in Jimma Health Center, Jimma Town, Oromia Region, Southwest Ethiopia from September 11, 2006–September 10, 2017 |
The dominant type of TB in children was EPTB, accounting for 10.1%, and both genders had equal exposure for smear positive pulmonary TB (Table 4).
 |
Table 4 Distribution of Types of TB Diagnosis According to Age and Sex of Patients in Jimma Health Center, Jimma Town, Oromia Region, South West Ethiopia from September 11, 2006–September 10, 2017 |
Age, educational level, and types of TB diagnosis with treatment outcome of the patients were statistically significant (P<0.05) and associated; while sex, category of the patient, and occupational status of the patients and their treatment outcome were not statistically significant (P>0.05) (Table 5).
 |
Table 5 Distribution of Age, Sex, Educational Level, Occupational Status, Types of TB, and Category of Patients in Relation to Their Treatment Outcome in Jimma Health Center, Jimma Town, Oromia Region, South West Ethiopia from September 11, 2006–September 10, 2017 |
Multivariate logistic regression analysis has been carried out for socio-demographic and clinical risk factors, including age, sex, educational level, and occupational status; the type of TB and treatment category of patients. The proportion recorded on the multivariate logistic model as having an unsuccessful treatment outcome varied by the age group, educational level, and the type of TB. A poor treatment outcome was observed in 15–49 years old TB patients (AOR=1.26, 95% CI=1.06–2.24) compared to patients aged 0–14 years and over 50 years old. In other predictors the illiterate patients had 3.63 (CI=1.98–5.45) greater risks of unsuccessful treatment outcome than the literate patients. EPTB and PTB– patients were more likely to experience unsuccessful treatment outcome (AOR=2.12, CI=1.02–3.67 and AOR=1.66, CI=1.21–2.87, respectively) than PTB+ patients. Sex, occupational status, and category of patients did not show any statistically significant association with unsuccessful treatment outcome in the multivariate analysis (Table 6).
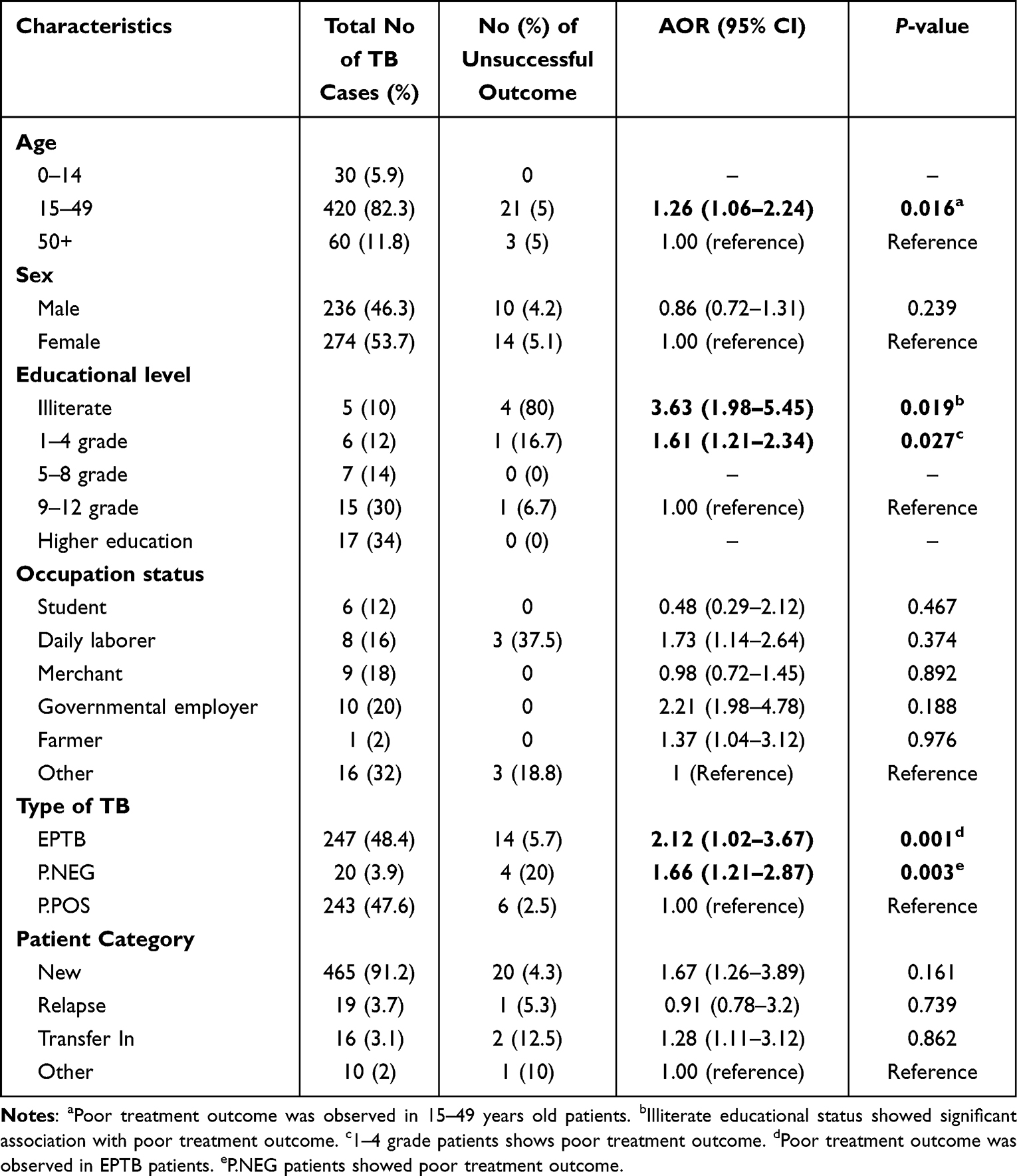 |
Table 6 Distribution of Individual Factors Associated with Treatment Outcome of TB Patients in Jimma Health Center, Jimma Town, Oromia Region, South West Ethiopia from September 11, 2006–September 10, 2017 |
Jimma Medium Clinic/Private/Result
A total of 586 patients were registered at the Jimma Medium Clinic from September 11, 2006 to September 10, 2017, out of which a total of 582 patients were included in this study that were diagnosed and started their treatment at a TB-Leprosy follow-up clinic, while four cases were transferred out to other health institutions with no record of the treatment outcome. Males constituted 50.9% (n=298) and females constituted 49.1% (n=288). The majority of patients were between the ages of 15–49 years, which accounted for 74.2% (n=432), with tae mean age of 32.4 years. Among those patients, 96.9% (n=564) were new, 1.0% (n=6) were transferred in, 0.5% (n=3) were relapses, and 1.5% (n=9) were others. Regarding the category of TB, extrapulmonary tuberculosis constituted 41.8% (n=243), smear positive pulmonary tuberculosis was 23.2% (n=135), while smear negative pulmonary tuberculosis was 35.1% (n=204). Forty-two patients had data for occupational and educational level status, which was taken from September 4–April 3, 2015. The majority (35.7%, n=15) of patients were educated in higher education and 21.4% (n=9) of patients were students (Table 7).
 |
Table 7 Distribution of Sex, Age, Educational Level, Occupational Status, Category of Patients, and Types of TB Diagnosis in Jimma Medium Clinic, Jimma Town, Oromia Region, South West Ethiopia from September 11, 2006–September 10, 2017 |
According to treatment outcome, 76.3% (n=444) completed treatment, 21.8% (n=127) were cured, 1.2% (n=7) defaulted, 0.5% (n=3) died, and there was 0.2% (n=1) treatment failure. The overall treatment success rate in the area was 98.1% (n=571, cure plus treatment complete). The overall defaulting rate was 1.2% (n=7) (Table 8).
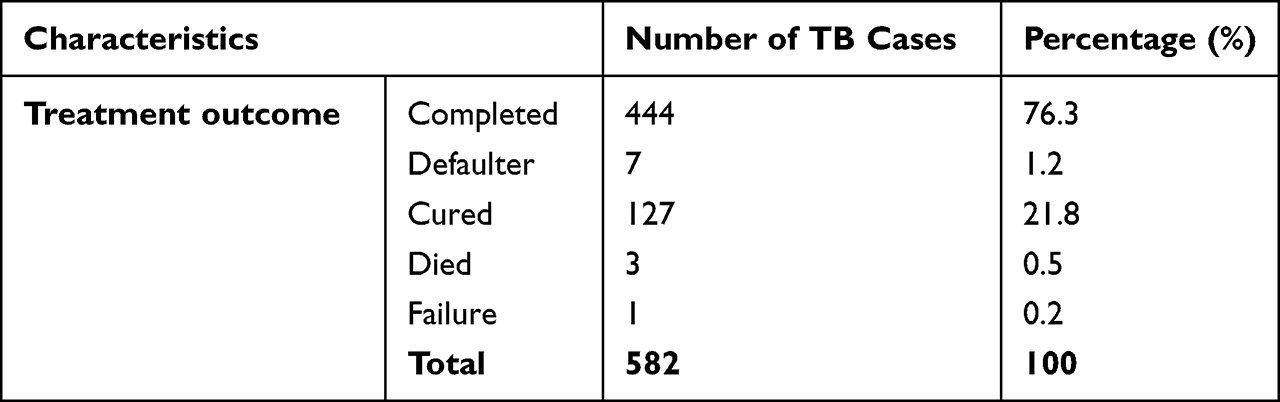 |
Table 8 Distribution of TB Treatment Outcome in Jimma Medium Clinic, Jimma Town, Oromia Region, South West Ethiopia from September 11, 2006–September 10, 2017 |
Two EPTB and one P.NEG patients died, and those were new and transfer in, respectively. In total, 97.5% (n=237) EPTB patients completed anti-TB treatment and 1.0% (n=2) pulmonary smear negative patients were defaulters. A total of 90.4% (n=122) smear positive pulmonary patients were cured and 0.7% (n=1) smear positive pulmonary patients were treatment failure (Table 9).
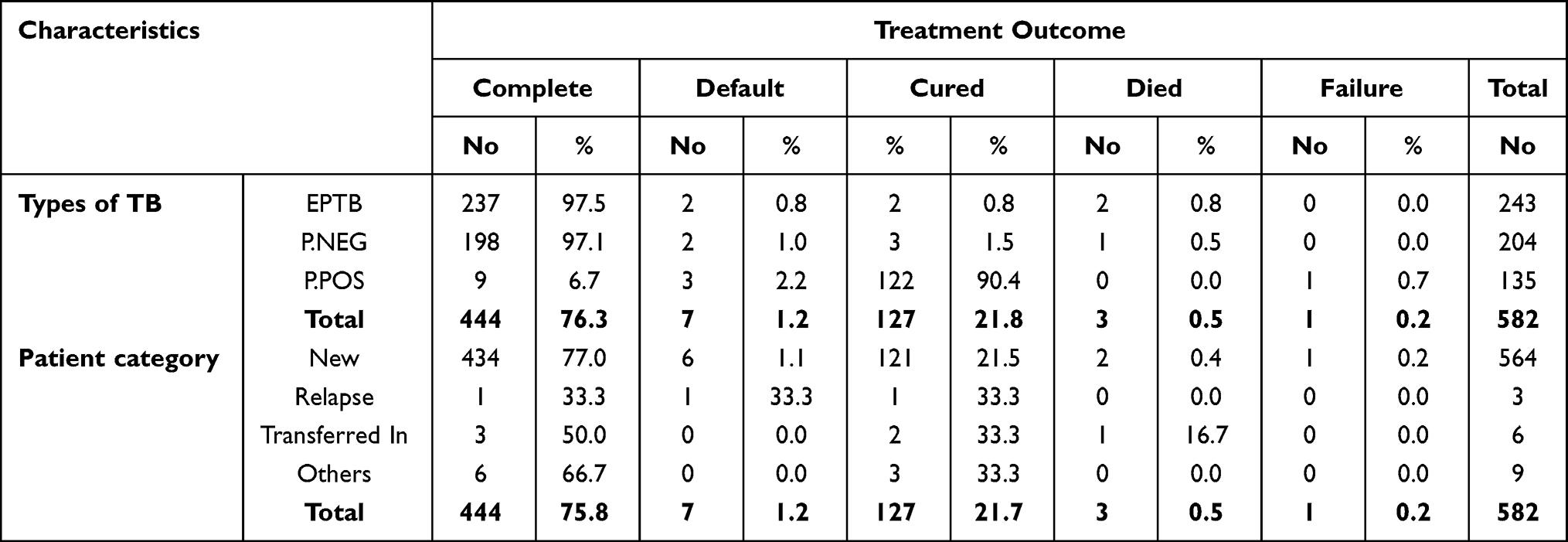 |
Table 9 Distribution of Category of TB and Patient Diagnosis with Treatment Outcome in Jimma Medium Clinic, Jimma Town, Oromia Region, Southwest Ethiopia from September 11, 2006–September 10, 2017 |
The dominant type of TB in children was P.NEG, accounting for 17.6% (n=36), and males are more exposed for smear positive pulmonary TB (55.6%, n=75) (Table 10).
 |
Table 10 Distribution of Types of TB Diagnosis According to Age and Sex of Patients in Jimma Medium Clinic, Jimma Town, Oromia Region, South West Ethiopia from September 11, 2006–September 10, 2017 |
Age, educational level, and types of TB diagnosis with treatment outcome of the patients were statistically significant (p<0.05) and associated. While sex, category of the patient, and occupational status of the patients and their treatment outcome were not statistically significant (p>0.05) (Table 11).
 |
Table 11 Distribution of Age, Sex, Educational Level, Occupational Status, Types of TB, and Category of Patients in Relation to Their Treatment Outcome in Jimma Medium Clinic, Jimma Town, Oromia Region, South West Ethiopia from September 11, 2006–September 10, 2017 |
Multivariate logistic regression analysis was carried out for socio-demographic and clinical risk factors, including age, sex, educational level, and occupational status; the type of TB and treatment category of patients. The proportion recorded on the multivariate logistic model as having an unsuccessful treatment outcome varied by the age group, educational level, and the type of TB. The poor treatment outcome was observed in 15–49 years old TB patients (AOR=2.16, 95% CI=1.67–3.09) compared to those aged 0–14 years and over 50 years old . In other predictors, the illiterate patients had a 2.73 (CI=1.18–4.31) greater risk of unsuccessful treatment outcome than literate patients. EPTB and PTB– patients were more likely to have experienced unsuccessful treatment outcome (AOR=1.84, CI=1.01–3.78 and AOR=0.47, CI=0.24–2.71, respectively) than PTB+ patients. Sex, occupational status, and category of patients did not show any statistically significant association with unsuccessful treatment outcome in the multivariate analysis (Table 12).
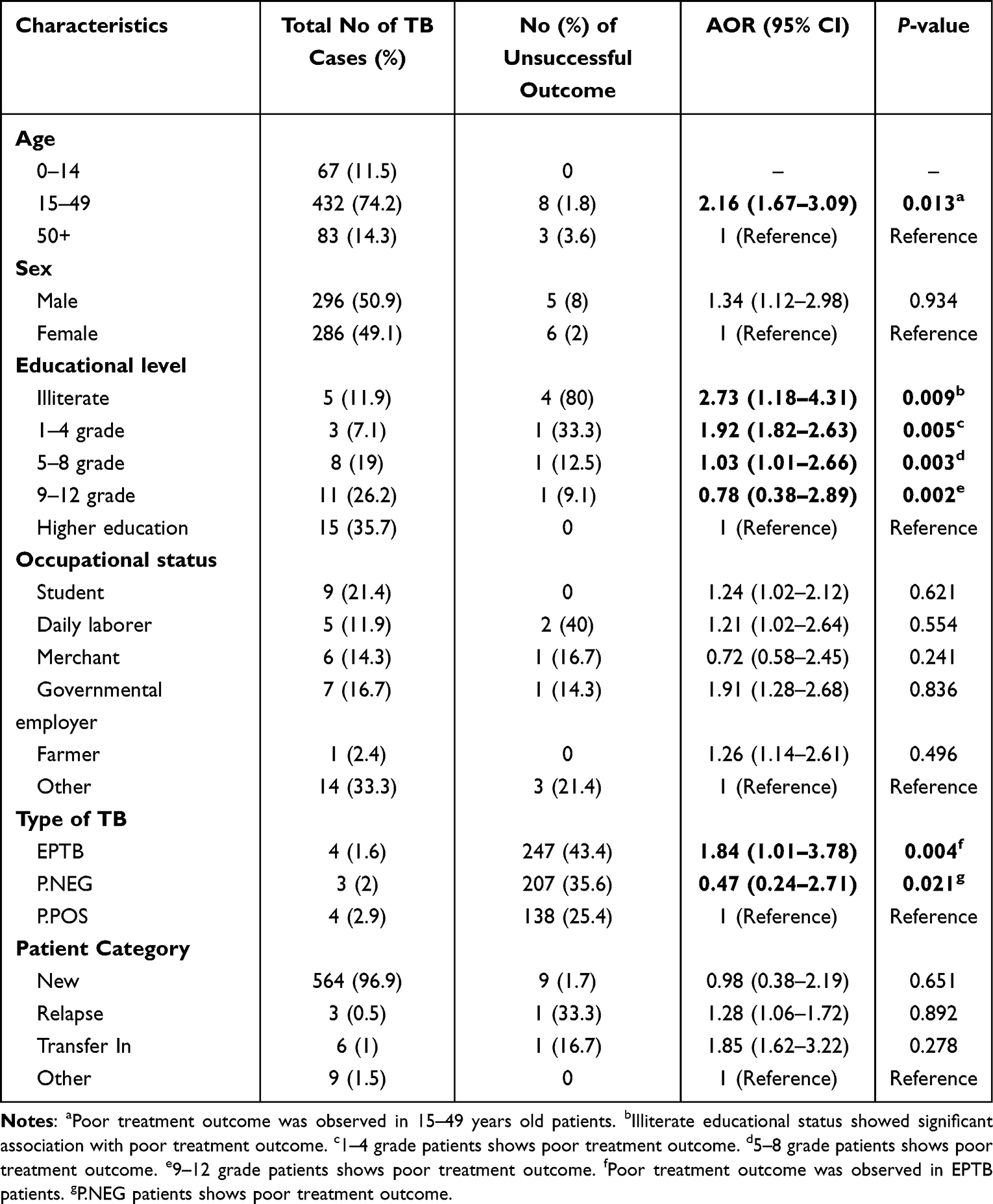 |
Table 12 Distribution of Age, Sex, Educational Level, Occupational Status, Types of TB, and Category of Patients in Relation to Their Treatment Outcome in Both Jimma Medium Clinic and Jimma Health Center, Jimma Town, Oromia Region, South West Ethiopia from September 11, 2006–September 10, 2017 |
Comparing the Institutions
Socio-Demographic and Clinical Characteristics of the Patients with the TB Trend
A total of 510 and 582 patients followed anti-TB treatment in the governmental and private clinic, respectively. The majority of the patients in the governmental clinic were females (53.7%, n=274) and males in the private clinic constituted 50.9% (n=298). In both sectors, themajorities of patients were between the ages of 15–49 years, which accounted for 82.2% (n=419) in the governmental health center and 74.2% (n=432) in the private clinic with similar mean ages of 34.4 and 32.4 years, respectively. In both sectors new patients were the majority number, 91.2% (n=465) and 96.9% (n=564), whereas 3.1% (n=16) and 1.0% (n=6) were transferred in, 3.7% (n=19) and 0.5% (n=3) were relapses, and 2.0% (n=10) and 1.5% (n=9) were others in the governmental health center and private clinic, respectively. Regarding category of TB, in both sectors extrapulmonary tuberculosis constituted a similar number, 48.4% (n=247) in the governmental health center and 41.8% (n=243) in the private clinic, while smear negative pulmonary tuberculosis was 3.9% (n=20) in the governmental health center and 35.1% (n=204) in the private clinics. Smear positive pulmonary tuberculosis in the governmental health center is higher than the private clinic (47.6%, n=243; and 23.2%, n=135,) respectively). Ninety-two patients had the data for occupational status and educational level, 50 patients were from the governmental health center and 42 from the private clinic, which were taken from March 12–August 11 and from September 4–April 3, 2015 respectively. The majority of educational level was higher educated patients, which are similar in both sectors (34%, n=17; and 35.7%, n=15). The occupational status of governmental health center patients was governmental employee 20% (n=10), whereas 21.4% (n=9) of private clinic patients were students (Tables 1 and 7). The 10-years TB trend was analyzed and, in the private clinic, anti-TB treatment coverage was decreased by 2% from September 12, 2016 to September 10, 2017, while for the past 4 years (September 12, 2013, to September 10, 2017) the governmental clinic shows revitalization of anti-TB treatment coverage which shows laxity for the consecutive 4 years since September 12, 2009, to September 11, 2013 (Figure 1).
 |
Figure 1 Trend of all types of registered TB cases in Jimma Medium Clinic and Jimma Health Center September 12, 2017–September 2017. |
Treatment Outcome of TB
The 10-year treatment outcome for 1,092 patients from both sectors was analyzed. Hence, the majority of patients completed the anti-TB treatment in both sectors (49.2%, n=251) in the governmental health center and 76.3% (n=444) in the private clinic, also the cure rate was 46.1% (n=235) and 21.8% (n=127), respectively, whereas the default rate was 4.1% (n=21) and 1.2% (n=7) in the governmental and the private sectors, respectively. In both sectors three patients died. No treatment failure patients were documented in the governmental health center, whereas 0.2% (n=1) were documented in the private clinic. The overall treatment success rate of the private clinic is higher than the governmental health center, at 98.1% (n=571) and 95.3% (n=486), respectively. In addition, the overall unsuccessful treatment outcome rate of the governmental health center was 4.7% (n=24), which is higher than the 1.9% (n=11) of the private clinic (Tables 2 and 8).
Treatment Outcome and Its Associated Predictors
Multivariate logistic regression analysis was carried out to predict factors affecting the treatment outcome with socio-demographic and clinical risk factors including, age, sex, educational level, and occupational status, the type of TB and treatment category of patients. The proportion recorded on the multivariate logistic model as having an unsuccessful treatment outcome varied by the age group, educational level, and the type of TB. The risk of unsuccessful treatment outcome was 1.26 (95% CI=0.96–2.24) and 2.16 (95% CI=0.67–3.09) times higher among 15–49 years old TB patients in governmental and private clinics, respectively, compared to those aged 0–14 and over 50 years old. In another predictor the illiterate patients in the governmental health center had 3.63-times (95% CI=1.98–5.45) and in the private clinic 2.73-times (95% CI=1.18–4.31) greater risk of unsuccessful treatment outcome compared to the literate patients. The governmental health center had a higher poor treatment outcome in EPTB type of patients (AOR=2.12, 95% CI=1.02–3.67) than the private clinic (AOR=1.84, 95% CI=1.01–3.78), compared with their counterparts of type TB. Sex, occupational status, and category of patients did not show any statistically significant association with unsuccessful treatment outcome in the multivariate analysis (Tables 6 and 12).
Discussion
Correct treatment of TB aims to cure the patient, interrupting transmission of TB to other people and preventing bacilli from becoming drug resistant. As such, insuring successful treatment completion might be required, addressing multiple factors beyond simple supervision of the drug intake.20 In one of the health indicators of sustainable development, the goal is to bring the non-completion of TB treatment below 10% in order to have treatment success of 85% in all detected smear positive cases. Different studies showed that the current running on DOTS strategy has increased treatment success rate. In Ethiopia, national treatment success was 94% in 2017.8
Both sectors have almost the same catchment area. The present study revealed that within a 10-year duration the private clinic gave anti-TB treatment coverage for 582 patients, whereas the governmental clinic served 510 patients. The treatment success rate of the private clinic is 98.1%, which is 1.03-fold that of the governmental health center (95.3%). The governmental health center defaulting rate was triple-fold that of the private clinic (4.1% and 1.2%, respectively), while the treatment failure of the private clinic was 0.2%, but there was no treatment failure in the governmental health center (Figure 2).
 |
Figure 2 The overall treatment outcome of Jimma Medium Clinic and Jimma Health Center. |
In both sectors, 15–49 years old patients had a high treatment success rate, whereas children did not account a defaulting rate (Figure 3). The male treatment success rate in both sectors was higher than the female rate, 98.31% in the private and 95.76% in the governmental health center, with their respective of 97.9% and 94.8%. The defaulting rate of both sexes in the governmental sector was higher than the private sector, 18.88% of females and 35.62% males, with their respective 5.92% females and 14.3% males(Figure 4).
 |
Figure 3 Patient age with TB treatment outcome in Jimma Medium Clinic and Jimma Health Center. |
 |
Figure 4 The sex of the patient with TB treatment outcome in Jimma Medium Clinic and Jimma Health Center. |
In both sectors the treatment success rate was higher with a higher educational level; most of the defaulting patients were illiterate patients (Figure 5).
 |
Figure 5 Educational level of the patient with the TB treatment outcome in Jimma Medium Clinic and Jimma Health Center. |
Despite there being no statistical association between the occupational status of patients and the TB treatment outcome, a governmental employee had a better treatment success rate in the governmental institution than the private institution; however, students showed a better treatment outcome in the private clinic than the governmental clinic. The daily laborers defaulting rate in the governmental health institution was higher than the private clinic (Figure 6).
 |
Figure 6 Occupational status of the patient with the TB treatment outcome in Jimma Medium Clinic and Jimma Health Center. |
Smear positive pulmonary TB prevalence in the governmental health center was double higher than the private clinic, whereas the number of pulmonary negative TB patients of the private clinic was 30-times folds of the governmental health center. This is due to the lack of x-ray technology with untrained professionals for further Tuberculosis diagnostic criteria. The success rate of smear pulmonary positive patients was almost the same, whereas smear negative pulmonary TB patients and EPTB treatment success rate were 98.6% and 98.3% in the private clinic, respectively, which is higher than that of the governmental health center, at 80% and 94.3% (Figure 7).
 |
Figure 7 The type of TB with the TB treatment outcome in Jimma Medium Clinic and Jimma Health Center. |
The newly-diagnosed tuberculosis patient treatment success rate in the private clinic is higher than the governmental health center, at 98.5% and 95.7%, respectively. The defaulting rate after relapse of the disease in the private clinic is 33.3%, which is higher than the governmental health center, at 21.1% (Figure 8).
 |
Figure 8 The category of the patient with the TB treatment outcome in Jimma Medium Clinic and Jimma Health Center. |
Besides anti-TB treatment being free, the differences may be due to awareness about drug adherence and also different socioeconomic status. This shows good progress of the DOTS strategy and a decrease of noncompliance in both sectors.
Age, educational level, and the types of TB diagnosis with the treatment outcome of the patients were statistically significant (P<0.05) and associated in both sectors. (The P-value of the governmental health center was 0.000, 0.005, and 0.000, and the private clinic 0.001, 0.000, and 0.000, respectively). Sex, category of the patient, and occupational status of the patients with their treatment outcome were not statistically significant (P>0.05) (p-value for the governmental health center was 0.239, 0.232, and 0.161 in the governmental health center, and the private clinic 0.263, 0.478, and 0.344, respectively) (Tables 5 and 11).
The literacy level plays a greater role for treatment success rate. Hence, the current study revealed a poorer treatment outcome was observed in uneducated patients (Tables 6 and 12).
Conclusion
The public health priority of national TB control programmers is to work towards the objective to treat successfully 85%. Ensuring adherence to treatment is very important to achieve this priority.8,21 The DOTS strategy appears to have improved TB treatment success in both health facilities across 10 years. According to the result of this study, the mean treatment success rate of all registered patients in both sectors achieved the expected WHO targets. The unsuccessful treatment outcome was significantly associated with age, educational status, and type of TB. Regular follow-up of patients with unsuccessful outcome and awareness creation through health education for patients in the course of treatment is vital. Moreover, attention should be given to regular sputum follow-up tests for registered PTB+ cases and proper registration to record the results of treatment outcome.
Strengths and Limitations of the Study
- Since it is secondary data there was no problem to collect the appropriate information which is clear of bias.
- Data accuracy is under question with some incomplete subjects since it is a secondary data.
- The sources of this study are Jimma health center and Jimma medium clinic records; hence, the result may lack external validity.
- Lack of stable internet from Ethiopia during data collection.
Abbreviations
JMC, Jimma Medium Clinic; TB, Tuberculosis; JHC, Jimma Health Center; AIDS, Acquired Immune Deficiency Syndrome; AFB, Acid-fast bacilli; ARI, Annual risk of TB infection; DOTS, Directly observed treatment of short course; EPTB, Extra pulmonary tuberculosis; HIV, Human Immune Deficiency Virus; MDR-TB, Multi-drug resistant Tuberculosis; MOH, Ministry of Health, PTB; Pulmonary Tuberculosis; TLCP, TB and leprosy control program; PTB +ve, Smear positive pulmonary TB; PTB -ve, Smear negative pulmonary TB; WHO, World Health Organization; NTCP, National Tuberculosis Control Program; TLCP, TB and Leprosy Control Program.
Ethical Approval
A formal letter was written by Tsinghua university public health and research center to Jimma university medical research center to get the permission, then the study approval and ethical clearance was obtained from Jimma University institutional review board. An official letter of permission was obtained from Jimma Institute of Health Ethical review board and given to Jimma town health office to conduct the study, then forwarded to the respective private and governmental health institutions. Since the data was a long-term retrospective study and secondary from the Anti-TB registration, it was difficult to get the written informed consent obtained from study participants; hence, it was waived. The study was conducted per the declaration of Helsinki. Confidentiality of participants’ information was kept using unique codes rather than personal identification.
Acknowledgment
We would like to express our sincere and deep- rooted thanks for Professor Cheng Feng to his constructive advice, comments, guides and support. Thanks also to all our colleagues and friends who assisted us by providing the necessary information. We would like to extend our gratitude to Tsinghua University for offering a broad band free internet service and free international call that helped the first author to communicate with the rest authors. Finally, we would like to thank Jimma city health office, Jimma health center, Jimma medium clinic with their respective TB treatment personnel’s for their permission and cooperation for giving us the necessary data.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kumar, V, Abbas, AK, Aster, JC. Robbins Basic Pathology. Vol. 10.
2. Farzianpour F, Kooshad M-M. Study of the status of tuberculosis control program based on the implementation of the directly observed treatment short-course strategy (DOTS). Mater Socio Med. 2016;28(4):249. doi:10.5455/msm.2016.28.249-252
3. Narasimhan P, Wood J, MacIntyre CR, Mathai D. Risk factors for tuberculosis. Pulmonary Med. 2013;2013. doi:10.1155/2013/828939
4. Thoen, CO, Steele JH, Gilsdorf MJ. Mycobacterium bovis Infection in Animals and Humans. John Wiley & Sons; 2008.
5. World Health Organization. Global Tuberculosis Report 2021. Geneva, Switzerland: World Health Organization; 2021.
6. Tuberculosis. Available from: https://www.who.int/news-room/fact-sheets/detail/tuberculosis.
7. Biadglegne F, Tesfaye W, Anagaw B, et al. Tuberculosis lymphadenitis in Ethiopia. Jpn J Infect Dis. 2013;66(4):263–268. doi:10.7883/yoken.66.263
8. Health, Mo. Health Sector Transformation Plan II (HSTP II) 2020/21 - 2024/25 (2013 EFY-2017 EFY), H. services, Editor. 20. Addis Ababa: Ministry of Health - Ethiopia.
9. Gebrezgabiher G, Romha G, Ejeta E, Asebe G, Zemene E, Ameni G. Treatment outcome of tuberculosis patients under directly observed treatment short course and factors affecting outcome in southern Ethiopia: a five-year retrospective study. PLoS One. 2016;11(2):e0150560. doi:10.1371/journal.pone.0150560
10. Girum T, Muktar E, Lentiro K, Wondiye H, MJTd S. Epidemiology of multidrug-resistant tuberculosis (MDR-TB) in Ethiopia: a systematic review and meta-analysis of the prevalence, determinants and treatment outcome. Trop Dise Travel Med Vaccines. 2018;4(1):1–12.
11. Tesgaye F, Defar A, Beyene T, Shafi O, Klinkenberg E, Howe R. Documentation and treatment outcomes of smear-negative and extra-pulmonary tuberculosis in Ethiopia. Public Health Action. 2014;4(3):S25–S30. doi:10.5588/pha.14.0052
12. Pinnas J, Schwartz H, Yancey S, Rickard K. Six month comparison of beclomethasone vs. salmeterol or placebo in adults with asthma. Am J Respir Crit Care Med. 1998;157(Suppl 3):A417.
13. Nshuti L, Neuhauser D, Johnson JL, Adatu F. Whalen C Cjtijo T, Disease L. Public and Private Providers’ Quality of Care for Tuberculosis Patients in Kampala, Uganda. Int J Tuberc Lung Dis. 2001;5(11):1006–1012.
14. Chengsorn N, Bloss E, Anekvorapong R, et al. Tuberculosis services and treatment outcomes in private and public health care facilities in Thailand, 2004–2006. Int J Tuberc Lung Dis. 2009;13(7):888–894.
15. Ali MK, Karanja S, Karama M. Factors associated with tuberculosis treatment outcomes among tuberculosis patients attending tuberculosis treatment centres in 2016–2017 in Mogadishu, Somalia. Pan Afr Med J. 2017;28(1). doi:10.11604/pamj.2017.28.197.13439
16. Bureau, JZA. Jimma zone population. 2017.
17. Office, JTH. Jimma Town Health Facility Status. Jimma: Jimma Town Health Office; 2017.
18. Sinshaw Y, Alemu S, Fekadu A, Gizachew M. Successful TB treatment outcome and its associated factors among TB/HIV co-infected patients attending Gondar University Referral Hospital, Northwest Ethiopia: an institution based cross-sectional study. BMC Infect Dis. 2017;17(1):1–9.
19. Berhe G, Enquselassie F, Aseffa A. Treatment outcome of smear-positive pulmonary tuberculosis patients in Tigray Region, Northern Ethiopia. BMC Pub Health. 2012;12(1):1–9.
20. LoBue P, Sizemore C, Castro KG. Plan to combat extensively drug-resistant tuberculosis: recommendations of the federal tuberculosis task force. MMWR Recomm Rep. 2009;58(RR–3):1–43.
21. World Health Organization. National strategic plan tuberculosis and leprosy control 2006 – 2013 EC (2013/14 – 2020). World Health Organization. Available from: https://www.afro.who.int/publications/national-strategic-plan-tuberculosis-and-leprosy-control-2006-2013-ec-201314-2020.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.