")
Back to Journals » Open Access Emergency Medicine » Volume 12
Comparing Surf Lifeguards and Nurse Anesthetists’ Use of the i-gel Supraglottic Airway Device – An Observational Simulation Study
Authors Nørkjær L, Stærk M , Lauridsen KG, Gallacher TK, Løyche JB, Krogh K, Løfgren B
Received 18 November 2019
Accepted for publication 18 February 2020
Published 2 April 2020 Volume 2020:12 Pages 73—79
DOI https://doi.org/10.2147/OAEM.S239040
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hans-Christoph Pape
Louise Nørkjær,1 Mathilde Stærk,1– 3 Kasper G Lauridsen,1– 3 Tabita K Gallacher,4 Jakob B Løyche,5 Kristian Krogh,1,4 Bo Løfgren1,3,6,7
1Research Center for Emergency Medicine, Aarhus University Hospital, Aarhus, Denmark; 2Clinical Research Unit, Randers Regional Hospital, Randers, Denmark; 3Department of Internal Medicine, Randers Regional Hospital, Randers, Denmark; 4Department of Anesthesiology and Intensive Care, Aarhus University Hospital, Aarhus, Denmark; 5Department of Surgery and Intensive Care, Randers Regional Hospital, Randers, Denmark; 6Department of Cardiology, Aarhus University Hospital, Aarhus, Denmark; 7Institute of Clinical Medicine, Aarhus University, Aarhus, Denmark
Correspondence: Bo Løfgren
Department of Internal Medicine, Randers Regional Hospital, Skovlyvej 15, Randers, NE DK-8930, Denmark
Email [email protected]
Purpose: Using a supraglottic airway (SGA) may provide more effective ventilations compared with a mouth-to-pocket-mask for drowning victims. SGAs are widely used by nurse anesthetists but it is unknown whether surf lifeguards can use SGAs effectively. We aimed to compare the use of SGA by surf lifeguards and experienced nurse anesthetists.
Materials and Methods: Surf lifeguards inserted a SGA (i-gel O2, size 4) in a resuscitation manikin during cardiopulmonary resuscitation (CPR) and nurse anesthetists inserted a SGA in a resuscitation manikin placed on a bed, and performed ventilations. Outcome measures: time to first ventilation, tidal volume, proportion of ventilations with visible manikin chest rise, and ventilations within the recommended tidal volume (0.5– 0.6 L).
Results: Overall, 30 surf lifeguards and 30 nurse anesthetists participated. Median (Q1–Q3) time to first ventilation was 20 s (15– 22) for surf lifeguards and 17 s (15– 21) for nurse anesthetists (p=0.31). Mean (SD) tidal volume was 0.55 L (0.21) for surf lifeguards and 0.31 L (0.10) for nurse anesthetists (p< 0.0001). Surf lifeguards and nurse anesthetists delivered 100% and 95% ventilations with visible manikin chest rise (p=0.004) and 19% and 5% ventilations within the recommended tidal volume, respectively (p< 0.0001).
Conclusion: In a simulated setting, there was no significant difference between surf lifeguards and experienced nurse anesthetists in time to first ventilation when using a SGA. Surf lifeguards delivered a higher tidal volume, and a higher proportion of ventilations within guideline recommendations, but generally ventilations caused visible manikin chest rise for both groups.
Keywords: cardiopulmonary resuscitation, drowning, ventilation, supraglottic airway, surf lifeguards, nurse anesthetists
Introduction
The World Health Organization (WHO) estimates that approximately 320,000 people die due to drowning every year.1 Cardiac arrest due to drowning is associated with severe hypoxia, which is the single most important determinant of survival and neurological outcome.2,3 Effective ventilations should, therefore, be initiated as soon as possible to reverse hypoxia and improve survival. Accordingly, the European Resuscitation Council (ERC) guidelines for resuscitation in drowning emphasise the importance of ventilation by recommending five initial rescue breaths.3
When drowning incidents occur, first responders are often surf lifeguards trained to perform cardiopulmonary resuscitation (CPR).4 The International Lifesaving Federation (ILS) recommends the use of mouth-to-pocket-mask ventilation.4 During advanced life support, tracheal intubation and other airway interventions may be used. However, tracheal intubation should only be attempted by persons trained, competent, and experienced in this skill.5 In the absence of tracheal intubation skills, a supraglottic airway (SGA) may be an alternative airway method. SGAs are easier and safer to insert compared with a tracheal tube.5 Simulation studies on surf lifeguards indicate that the quality of resuscitation is directly related to the equipment used.6,7 Potential advantages of using SGA compared with mask ventilation may be shorter interruptions in chest compressions and reduced risk of gastric regurgitation.8–10
In Denmark, SGAs are used by nurse anesthetists independently of physician anesthesiologists as a standard airway management device during anesthesia. In this setting, nurse anesthetists’ use of SGAs is considered as gold standard. We have previously shown that surf lifeguards, who are often non-healthcare providers, can use SGAs successfully in a manikin.11 However, no comparison with experienced clinicians has been undertaken. The aim of this study was to compare the use of a SGA by surf lifeguards and experienced nurse anesthetists in a comparable setting.
Materials and Methods
Study Design
This was an observational simulation study. Surf lifeguards from two Danish open water lifeguard services were recruited. All surf lifeguards had undergone standardized surf lifeguard training in accordance with national standards in Denmark, including training in CPR and ventilation with a pocket mask. All surf lifeguards were in active service. Nurse anesthetists were recruited from the Department of Anesthesiology at Randers Regional Hospital, Denmark. The hospital has a catchment area of approximately 230,000 inhabitants and annually around 16,000 surgeries and 16,000 endoscopies are performed.12 According to Danish law, an ethical review committee approval was not required for this study. Study participation was voluntary. Oral and written consent were obtained from all participants.
Surf lifeguards and nurse anesthetists were asked to insert a SGA in a resuscitation manikin and perform ventilations. Prior to testing, surf lifeguards completed a 20-min training session to obtain knowledge and practice of using a SGA in a resuscitation manikin. Surf lifeguards were tested after the training session. The nurse anesthetists were all using SGAs on a daily basis in clinical practice. All nurse anesthetists familiarized themselves with the study equipment, i.e. inserted the SGA and ventilated the manikin immediately before the test.
Simulation and Data Collection
Participants inserted a SGA (i-gel O2, size 4, Intersurgical® Ltd, Wokingham, UK) in an adult-sized resuscitation manikin (Ambu® Cardiac Care Trainer, Ambu, Ballerup, Denmark), and performed ventilations with a ventilation bag (The BAG II Resuscitator Adult, Laerdal, Stavanger, Norway). The i-gel is a SGA designed for use during anesthesia. It has a cuff made of a soft gel-like material, which does not require inflation, and it is designed to fit the anatomy of the larynx.13 During the test, application of lubricant gel on the SGA was simulated as the manikin’s airway was lubricated prior to testing according to manikin manufacturer instructions.
To reflect the clinical use of SGAs in the two groups, surf lifeguards were asked to insert the SGA in a manikin placed on the floor as part of the airway management during resuscitation with 30:2 chest compressions and ventilations ratio according to ERC guidelines.3 Nurse anesthetists were asked to insert the SGA and perform five ventilations with the manikin placed on a bed similar to the setting in an operating theatre.
The manikin used for testing was connected to a laptop with Ambu® CPR Software (Ambu) to collect ventilation quality data. All tests were undertaken by a researcher to ensure that the test protocol was followed. All tests were video recorded for subsequent analysis.
Questionnaires were distributed to surf lifeguards and nurse anesthetists. Demographic data on age, sex, education, and experience were collected. In addition, surf lifeguards were asked to rate their skills in using the SGA on a 5-point Likert scale with the response options “totally agree,” “predominantly agree,” “neither agree nor disagree,” “predominantly disagree”, and “totally disagree.” Surf lifeguards also rated the user-friendliness of the SGA on a 10-point scale. After the test, all nurse anesthetists were asked if they knew the ERC guidelines for tidal volume (i.e. 0.5–0.6 L, all values within the range were accepted as correct), and the number of ventilations per minute during continuous chest compressions (10 ventilations per minute). Nurse anesthetists were asked to state which SGA device they preferred to use of three different SGAs (i-gel O2 (Intersurgical® Ltd), Portex® Soft Seal® Laryngeal Mask (Smiths Medical International Ltd, Ashford, UK) and Ambu® AuraOnce (Ambu)). Furthermore, nurse anesthetists were asked to evaluate the insertion of the SGA in the manikin compared with their experiences with real patients.
Data Analysis and Outcome Measures
The first six ventilations were analyzed for surf lifeguards as ventilations were performed during a 30:2 chest compressions and ventilation CPR sequence. For nurse anesthetists, continuous ventilations were performed and all five ventilations were analyzed. Data on tidal volume were collected from the manikin, and correct tidal volume was defined as 0.5–0.6 L as recommended by the ERC.14 Data on time to first ventilation and ventilations with visible manikin chest rise were assessed and collected from video recordings by two independent assessors. In case of discrepancies in assessment, videos were jointly reassessed until consensus was reached. Time to first ventilation was defined as the time from the start of unpacking the SGA to the initiation of ventilation. The initiation of ventilation was determined as the beginning of compression of the resuscitation bag connected to the SGA. The outcome measures were time to first ventilation, tidal volume, proportion of ventilations with visible manikin chest rise, and proportion of ventilations with recommended tidal volume.
Statistical Analysis
Data were analyzed for normality using histograms, QQ-plots, and Shapiro–Wilks test. Variances were tested using a standard deviation test. Normally distributed data are reported as mean (standard deviation (SD)), non-normally distributed data are reported as median (Q1–Q3), and categorical data are reported as number (n) and percentage (%). Time to first ventilation was compared using the Wilcoxon rank-sum test and tidal volumes were compared with unequal variance t-test. The proportions of ventilations with visible manikin chest rise and ventilations with recommended tidal volume were compared using Fisher’s exact test. A value of p<0.05 was considered statistically significant. The study was based on a convenience sample and no sample size calculation was performed.
Results
In total, 30 surf lifeguards and 30 nurse anesthetists were included in the present study. We contacted the Chief Surf Lifeguards of the two lifeguard services and the Head Anesthetist Nurse before recruiting surf lifeguards and nurse anesthetists in service, of whom all approached accepted the invitation to participate in the study. Demographics are shown in Table 1.
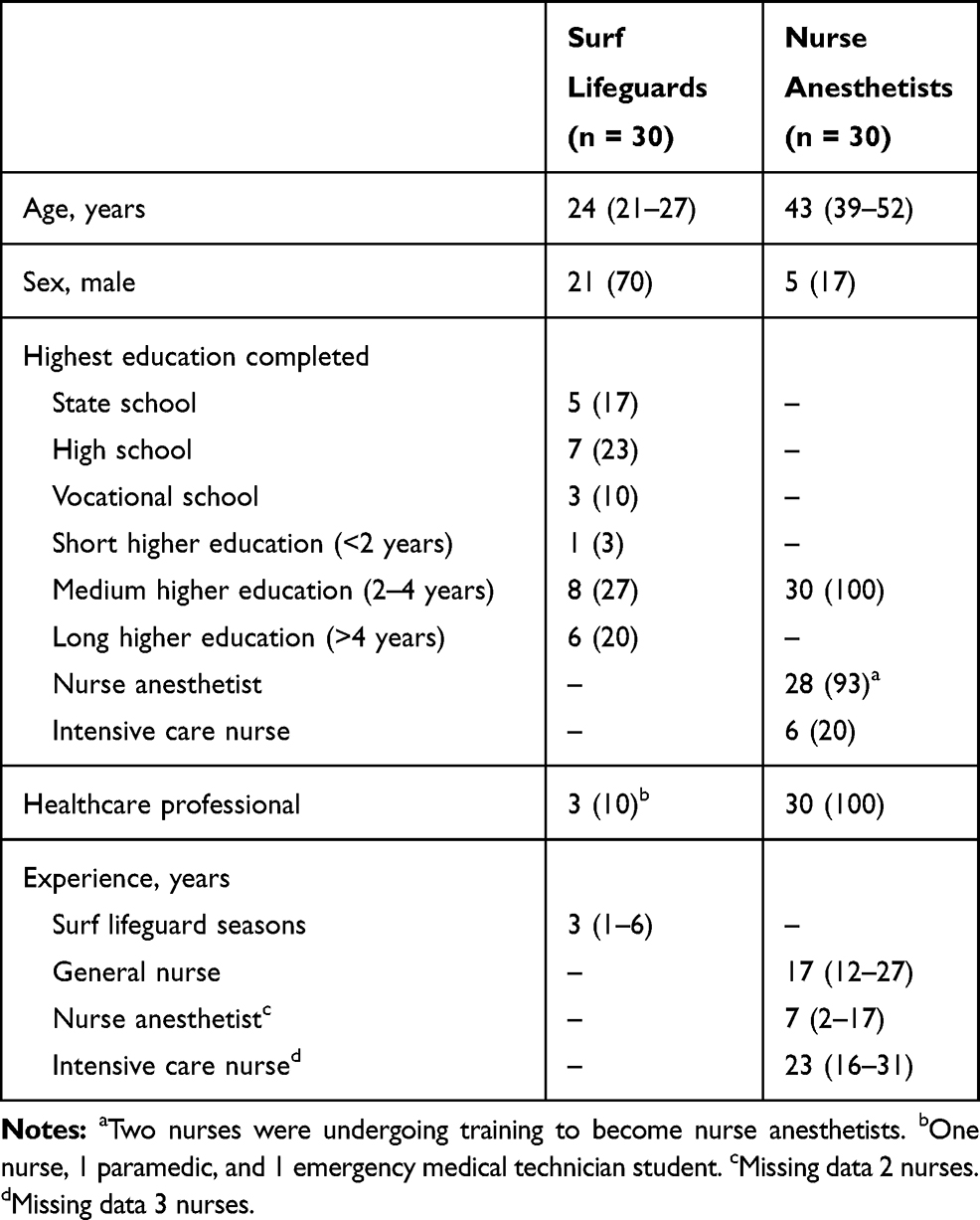 |
Table 1 Characteristics of the Surf Lifeguards and Nurse Anesthetists Included in the Study. Data are Presented as Median (Q1–Q3) or Number (Percentage) |
The median (Q1–Q3) time to first ventilation was 20 s(15–22) for surf lifeguards and 17 s (15–21) for nurse anesthetists (p=0.31) (Figure 1A). The mean (SD) tidal volume was 0.55 L (0.21 L) for surf lifeguards and 0.31 L (0.10 L) for nurse anesthetists (diff. 0.24 L, 95% CI: 0.15–0.32 L, p<0.0001) (Figure 1B).
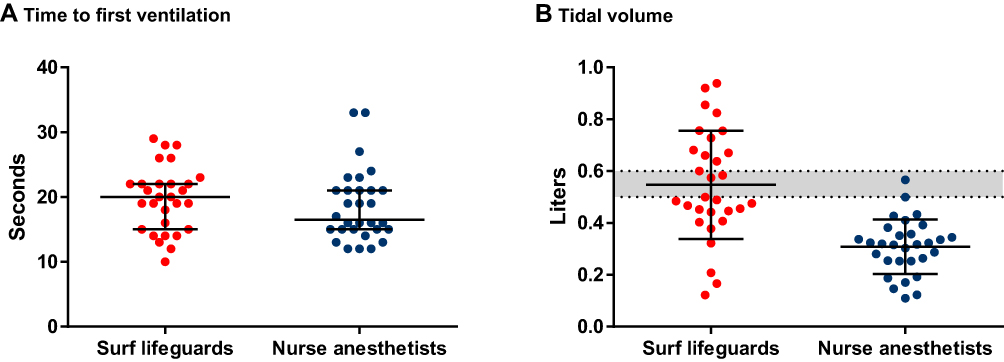 |
Figure 1 Ventilations. (A) Time to first ventilation. Each dot represents a participant’s time to first ventilation. Data are median time to first ventilation with first and third quartile. Data on one surf lifeguard are missing. (B) Tidal volume. Each dot represents a participant’s mean tidal volume. Data are mean tidal volume with standard deviations. The gray area marks the recommended tidal volume by the ERC (0.5–0.6 L). |
Surf lifeguards and nurse anesthetists delivered 100% and 95% ventilations with visible manikin chest rise (p=0.004) and 19% and 5% ventilations within recommended tidal volume (p<0.0001), respectively.
Surf lifeguards rated their own skills using the SGA on a 5-point Likert scale. These results are presented in Table 2. The surf lifeguards rated the SGA 9 (8–10) in user-friendliness on a scale of 1–10, with 10 being most user-friendly.
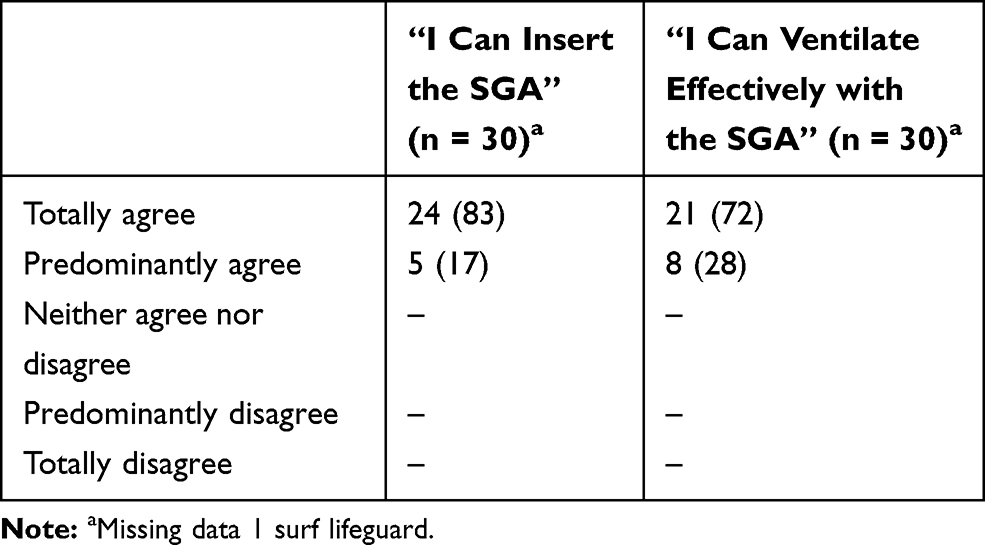 |
Table 2 Surf Lifeguard Rating of Own Skills Using the SGA. Data are Presented as Number (Percentage) |
Overall, 80% (n=24) of the nurse anesthetists stated that they knew the ERC guidelines. Of these, 83% (n=20) stated the correct recommended tidal volume and 32% (n=7) (missing data: 2 nurse anesthetists) stated the correct number of ventilations per minute during continuous chest compressions. Of the three SGAs, 53% (n=16) preferred i-gel, while 40% (n=12) preferred AuraOnce and 7% (n=2) preferred Soft Seal. The majority of the nurse anesthetists (57%, n=17) stated that they thought it was easier to ventilate a manikin compared with an actual patient, while 33% (n=10) stated no difference, and 10% (n=3) stated it was easier to ventilate a patient.
Discussion
In a simulated setting, there was no significant difference between surf lifeguards and experienced nurse anesthetists in time to first ventilation when using a SGA. Surf lifeguards delivered a higher tidal volume, and a higher proportion of ventilations within the recommended tidal volume compared with experienced nurse anesthetists. Generally, ventilations caused visible manikin chest rise for both groups.
The mean time to first ventilation in the present study is comparable to previous findings showing time to ventilation of 15.6 s for Danish surf lifeguards using a SGA (i-gel).11 Other studies on health-care professionals using a SGA (i-gel) in a manikin reporting faster time to first ventilation have used different definitions of time to first ventilation. Two studies on health-care professionals reported mean time to first ventilation of 6.6 s and 11.3 s,15,16 defined as the time from insertion of the SGA (i-gel) between the teeth until the device was placed above the glottis. Another study on nurse anesthetists’ use of a SGA (i-gel, size 1.5) in a child manikin reported a median (range) time to first ventilation of 6.0 s (3.6–10.0 s), defined as the time from picking up the SGA to inflation of the lungs.17 The nurses in previous studies may not have unpacked the SGA and applied lubricant gel on the SGA. These differences may explain why the present study resulted in longer time to first ventilation.
We found that the tidal volumes delivered by surf lifeguards are similar compared with findings from a previous study that found a mean tidal volume of 0.5 L.11 As nurse anesthetists are experienced in airway management, one may expect them to perform better than surf lifeguards, contrary to our results. In the present study, only a small number of surf lifeguards and nurse anesthetists delivered a tidal volume within the recommendations.14 The surf lifeguards delivered a higher tidal volume than the nurse anesthetists but with a much larger variation. A vast majority of the nurse anesthetists knew the recommended tidal volume, indicating their low tidal volumes were not due to a lack of knowledge. Possibly, the low tidal volumes could be due to leakage of air. However, it was not possible to measure the leakage in our study. It is possible that there was leakage of air in the manikin, which might be more pronounced compared with real patients.
Both surf lifeguards and nurse anesthetists are trained to assess the effectiveness of ventilations by chest rise. Our results show that both groups mostly delivered ventilations with visible manikin chest rise. Visible manikin chest rise was subjectively assessed by two independent assessors based on video recordings. As they were two assessors, who evaluated the videos independently using identical evaluation criteria for both surf lifeguards and nurse anesthetists, we do not believe this has had any impact on the results. The difference between surf lifeguards and nurse anesthetists regarding the proportion of ventilations with visible manikin chest rise may be due to the difference in tidal volume, but also nurse anesthetists being more aware of the risk of hyperinflation of the lungs and gastric inflation caused by higher tidal volumes during manual ventilation.18 To avoid these complications, experienced nurse anesthetists likely have an almost automated muscle response when delivering manual ventilation, ensuring a constant flow and tidal volume. In comparison, surf lifeguards are inexperienced in ventilating patients and are more likely to deliver an uneven flow and a larger variation in tidal volume, as shown. Overall, this may explain why nurse anesthetists delivered smaller tidal volumes compared with surf lifeguards.
Future resuscitation training should focus on practical training in the delivery of recommended tidal volume, flow, and rate of ventilation to ensure optimal resuscitation.
I-gel was chosen for this study because it has been reported to be the preferred SGA among surf lifeguards.11 Therefore, it was interesting to find out which SGA was preferred among nurse anesthetists. In the present study, it was found that nurse anesthetists preferred i-gel over other SGAs. A previous study found that medical students inexperienced in airway management also preferred i-gel to other SGAs due to its ease of use.10,11 This indicates that the choice of SGA in specific settings must be evaluated to meet the resources, the skills of the provider, and the need for the given purpose.
The surf lifeguards felt confident in both insertion and ventilation with the SGA. The belief in their own abilities may result in a greater likelihood of using the SGA during resuscitation and a greater chance of successful use. However, continuous practice to maintain sufficient skills and avoid incorrect use may be necessary. This may be one reason why it is an ongoing discussion about whether surf lifeguards should be trained and have permission to use SGAs in drowning resuscitation instead of the recommended pocket mask.11,19,20 A recent manikin study performed with Australian surf lifeguards evaluated their competence in the use of different airway techniques (pocket mask, bag-valve-mask, and two SGAs). They found that the use of SGAs was not superior compared with the pocket mask and bag-valve-mask and it was recommended that the pocket mask and bag-valve-mask should continue to be used as ventilation devices in drowning resuscitation by lifeguards.8 However, SGA may result in shorter (or no) interruptions in chest compressions and less aspiration during resuscitation, although this needs to be confirmed in a clinical study among surf lifeguards.
A proof-of-concept study evaluated the performance of a SGA (i-gel) used by medical students, non-anesthetist physicians, and allied health professionals, all unfamiliar with the SGA.21 This study showed high success rates for insertion of the SGA both in manikins (88% placed in first attempt) and in patients classified as American Society of Anesthesiologists (ASA) 1–2 and with normal Body Mass Index (BMI) (83% placed in first attempt). The study suggests that manikins and humans may be comparable regarding insertion of a SGA. However, nurse anesthetists (57%) in our study reported that SGA insertion in a manikin was easier compared with humans. In the future, human studies should address clinical relevant outcome measures in the comparison of SGA use versus the use of a pocket mask in drowning resuscitation.
Limitations of the Study
The present study was a simulation study and extrapolation to humans should be taken with caution. In drowning, airway compliance may decrease, resulting in increased airway resistance and difficulties ventilating using a SGA, and failure to ventilate with SGAs in drowning victims have been reported.22 Furthermore, regurgitation may occur during drowning resuscitation,23 which was not simulated in our study.
Nurse anesthetists were recruited from only one hospital, in contrast to surf lifeguards, recruited from two lifeguard services. Even though the Danish hospitals and health-care system including training of nurse anesthetists are very homogenous, we cannot rule out that the skills of the nurse anesthetists may somewhat differ from other hospitals and health-care systems. Also, the simulation settings were different for the two groups to imitate each of the two groups’ usual setting during airway management. The surf lifeguards may be disadvantaged compared to the nurse anesthetists as they had more psychomotor skills during testing, i.e. chest compressions. Surf lifeguards were tested right after the SGA training session and we cannot infer on their skill retention. Finally, this study was based on a convenience sample and no sample size calculation was performed.
Conclusion
In a simulated setting, there was no significant difference between surf lifeguards and experienced nurse anesthetists in time to first ventilation when using a SGA. Surf lifeguards delivered a higher tidal volume, and a higher proportion of ventilations within guideline recommendations but generally ventilations caused visible manikin chest rise for both groups.
Abbreviations
SGA, supraglottic airway; WHO, World Health Organization; ERC, European Resuscitation Council; CPR, cardiopulmonary resuscitation; ILS, International Lifesaving Federation; ASA, American Society of Anesthesiologists; BMI, body mass index.
Acknowledgments
We are grateful to all the volunteer surf lifeguards and nurse anesthetists. We thank Chief Lifeguard of the North Zealand Surf Lifeguard Service, John Mogensen, and Chief Lifeguard of Aalborg Surf Lifeguard Service, Carsten Jørgensen for excellent collaboration.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Drowning. Available from: http://who.int/mediacentre/factsheets/fs347/en/.
2. Berg RA, Hemphill R, Abella BS, et al. Part 5: adult basic life support: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2010;122(18Suppl 3):S685–S705. doi:10.1161/CIRCULATIONAHA.110.970939
3. Truhlar A, Deakin CD, Soar J, et al. European resuscitation council guidelines for resuscitation 2015: section 4. Cardiac arrest in special circumstances. Resuscitation. 2015;95:148–201. doi:10.1016/j.resuscitation.2015.07.017
4. International Life Saving Federation. Position statement: MPS-11 2016 CPR Skills for Lifeguards. Available from: https://www.ilsf.org/wp-content/uploads/2018/11/MPS-11-2016-CPR-Skills-for-Lifeguards.pdf.
5. Soar J, Nolan JP, Bottiger BW, et al. European resuscitation council guidelines for resuscitation 2015: section 3. Adult advanced life support. Resuscitation. 2015;95:100–147. doi:10.1016/j.resuscitation.2015.07.016
6. Adelborg K, Dalgas C, Grove EL, Jorgensen C, Al-Mashhadi RH, Lofgren B. Mouth-to-mouth ventilation is superior to mouth-to-pocket mask and bag-valve-mask ventilation during lifeguard CPR: a randomized study. Resuscitation. 2011;82(5):618–622. doi:10.1016/j.resuscitation.2011.01.009
7. Adelborg K, Bjornshave K, Mortensen MB, Espeseth E, Wolff A, Lofgren B. A randomised crossover comparison of mouth-to-face-shield ventilation and mouth-to-pocket-mask ventilation by surf lifeguards in a manikin. Anaesthesia. 2014;69(7):712–716. doi:10.1111/anae.12669
8. Holbery-Morgan L, Angel C, Murphy M, et al. Competence in the use of supraglottic airways by Australian surf lifesavers for cardiac arrest ventilation in a manikin. Emerg Med Australas. 2017;29(1):63–68. doi:10.1111/1742-6723.12719
9. Stone BJ, Chantler PJ, Baskett PJF. The incidence of regurgitation during cardiopulmonary resuscitation: a comparison between the bag valve mask and laryngeal mask airway. Resuscitation. 1998;38(1):3–6. doi:10.1016/S0300-9572(98)00068-9
10. Fischer H, Hochbrugger E, Fast A, et al. Performance of supraglottic airway devices and 12 month skill retention: a randomized controlled study with manikins. Resuscitation. 2011;82(3):326–331. doi:10.1016/j.resuscitation.2010.11.014
11. Adelborg K, Al-Mashhadi RH, Nielsen LH, Dalgas C, Mortensen MB, Lofgren B. A randomised crossover comparison of manikin ventilation through Soft Seal(R), i-gel and AuraOnce supraglottic airway devices by surf lifeguards. Anaesthesia. 2014;69(4):343–347. doi:10.1111/anae.12545
12. Randers Regional Hospital. Nøgletal og organisering - Kirurgisk Fællesafdeling. Available from: https://www.regionshospitalet-randers.dk/afdelinger/kirurgisk-fallesafdeling/om-afdelingen/nogletal-og-organisering/.
13. Intersurgical. i-gel product information sheet. Available from: http://www.intersurgical.com/info/igel.
14. Perkins GD, Handley AJ, Koster RW, et al. European resuscitation council guidelines for resuscitation 2015: section 2. Adult basic life support and automated external defibrillation. Resuscitation. 2015;95:81–99. doi:10.1016/j.resuscitation.2015.07.015
15. Leventis C, Chalkias A, Sampanis MA, Foulidou X, Xanthos T. Emergency airway management by paramedics: comparison between standard endotracheal intubation, laryngeal mask airway, and I-gel. Eur J Emerg Med. 2014;21(5):371–373. doi:10.1097/MEJ.0000000000000101
16. Stroumpoulis K, Isaia C, Bassiakou E, et al. A comparison of the i-gel and classic LMA insertion in manikins by experienced and novice physicians. Eur J Emerg Med. 2012;19(1):24–27. doi:10.1097/MEJ.0b013e3283474ab3
17. Schunk D, Ritzka M, Graf B, Trabold B. A comparison of three supraglottic airway devices used by healthcare professionals during paediatric resuscitation simulation. Emerg Med J. 2013;30(9):754–757. doi:10.1136/emermed-2012-201570
18. Dörges V, Ocker H, Hagelberg S, Wenzel V, Idris AH, Schmucker P. Smaller tidal volumes with room-air are not sufficient to ensure adequate oxygenation during bag-valve-mask ventilation. Resuscitation. 2000;44(1):37–41. doi:10.1016/S0300-9572(99)00161-6
19. McKenna M, Davies M. Supraglottic airway use by lifeguards. Anaesthesia. 2014;69(8):928. doi:10.1111/anae.12723
20. Baker P, Webber J. Should supraglottic airway devices be used by lifeguards at all? Anaesthesia. 2014;69(8):928–929. doi:10.1111/anae.12725
21. Wharton NM, Gibbison B, Gabbott DA, Haslam GM, Muchatuta N, Cook TM. I-gel insertion by novices in manikins and patients. Anaesthesia. 2008;63(9):991–995. doi:10.1111/j.1365-2044.2008.05542.x
22. Baker PA, Webber JB. Failure to ventilate with supraglottic airways after drowning. Anaesth Intens Care. 2011;39(4):675–677. doi:10.1177/0310057x1103900423
23. Szpilman D, Bierens JJ, Handley AJ, Orlowski JP. Drowning. N Engl J Med. 2012;366(22):2102–2110. doi:10.1056/NEJMra1013317
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.