Back to Journals » OncoTargets and Therapy » Volume 12
Comparing short-time outcomes of three-dimensional and two-dimensional totally laparoscopic surgery for colon cancer using overlapped delta-shaped anastomosis
Authors Su H, Jin W, Wang P, Bao M, Wang X, Zhao C, Wang X, Zhou Z, Zhou H
Received 14 September 2018
Accepted for publication 10 December 2018
Published 18 January 2019 Volume 2019:12 Pages 669—675
DOI https://doi.org/10.2147/OTT.S187535
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Sanjeev K. Srivastava
Hao Su,1,* Weisen Jin,2,* Peng Wang,1 Mandula Bao,1 Xuewei Wang,1 Chuanduo Zhao,1 Xishan Wang,1 Zhixiang Zhou,1 Haitao Zhou1
1Department of Colorectal Surgery, National Cancer Center, National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Chaoyang District, Beijing 100021, People’s Republic of China; 2Department of Anorectal Diseases, General Hospital of Chinese Armed Police Forces, Haidian District, Beijing 100039, People’s Republic of China
*These authors contributed equally to this work
Purpose: Overlapped delta-shaped anastomosis is a newly developed intracorporeal procedure in totally laparoscopic surgery for colon cancer. We explored the safety and efficacy of three-dimensional (3D) totally laparoscopic surgery for colon cancer using overlapped anastomosis and compared its short-term outcomes with those of two-dimensional (2D) surgery.
Materials and methods: From January 2016 to March 2018, 97 colon cancer patients were grouped into the 3D group (43 patients) and the 2D group (54 patients); they underwent totally laparoscopic surgery for colon cancer using overlapped anastomosis by 3D and 2D laparoscopy, respectively. Data regarding the clinical characteristics, surgical and pathological outcomes, postoperative recovery and complications were collected and compared.
Results: These two groups were well balanced in terms of age, gender, body mass index, American Society of Anesthesiologists scores, previous abdominal operation history and preoperative chemotherapy (P>0.05). The overall operation time, intraoperative blood loss and removal method of the specimen were similar between groups (P>0.05), but the anastomosis time was significantly shorter in the 3D group than that in the 2D group (P=0.004). There were no differences in terms of pathological outcomes, postoperative recovery and the postoperative complication rates between the groups (P>0.05). Moreover, no mobility related to the anastomosis, such as anastomotic bleeding, stenosis or leakage, occurred in any patient.
Conclusion: 3D totally laparoscopic surgery for colon cancer using overlapped delta-shaped anastomosis is safe and effective, with satisfactory short-term outcomes. In addition, it is less time-consuming than 2D surgery regarding the overlapped anastomosis procedure.
Keywords: minimally invasive surgery, three-dimensional laparoscopy, intracorporeal anastomosis, colon neoplasms
Introduction
Overlapped delta-shaped anastomosis is a newly developed intracorporeal procedure in totally laparoscopic surgery for colon cancer.1 This procedure is performed intracorporeally by forming a side-to-side anastomosis using only laparoscopic linear staplers, and it has been shown to be safe, effective and less invasive than traditional surgery.2,3 However, performing overlapped delta-shaped anastomoses can be difficult for beginners because these procedures often require surgeons who have extensive experience in this technique and excellent operating skills. With the development of laparoscopic equipment, three-dimensional (3D) laparoscopy has overcome the shortcomings of conventional two-dimensional (2D) laparoscopy, providing surgeons with stereoscopic vision, in which depth perception is achieved using different unique images received by each eye.4–6 Therefore, we retrospectively compared the safety and efficacy of 3D totally laparoscopic surgery for colon cancer using overlapped delta-shaped anastomosis and its short-term outcomes with those of 2D laparoscopy.
Materials and methods
Patients
From January 2016 to March 2018, 97 patients who were diagnosed with colon cancer and prepared to be treated by laparoscopic surgery at the Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, People’s Republic of China were divided into two groups: the 3D group (43 patients), who underwent 3D totally laparoscopic surgery for colon cancer using overlapped delta-shaped anastomosis, and the 2D group (54 patients), who underwent 2D totally laparoscopic surgery for colon cancer using overlapped delta-shaped anastomosis.
The inclusion criteria were: 1) 18–80 years of age at diagnosis; 2) body mass index (BMI) between 18.5 and 30 kg/m2; 3) pathological diagnosis of ascending, transverse or descending colon adenocarcinoma by colonoscopy and 4) no distant metastasis determined by chest and abdominal computer tomography. The exclusion criteria included: 1) multiple colorectal primary carcinomas; 2) uncontrolled diabetes mellitus, immune system diseases or hematological diseases; and 3) severe intestinal obstruction. Every patient gave written informed consent for surgery, and the study was conducted in accordance with the principles of the Declaration of Helsinki. The protocol was approved by the Ethical Committee of the Cancer Hospital (Institute), Chinese Academy of Medical Sciences, Beijing, People’s Republic of China (Approval number NCC2017WJP-002).
Surgical procedures
The 3D group used the Olympus HD 3D laparoscopic surgery system, and both surgeons and assistants wore 3D glasses. The 2D group used the Olympus HD laparoscopic procedure system. The two groups used the same surgical method.
Under general anesthesia, all patients were placed in the supine lithotomy position, and a five-port technique was used as described previously.1 Relevant colons were mobilized from their retroperitoneal attachments according to the principle of complete mesocolic excision. Vessels were isolated and doubly ligated with a laparoscopic blunt tip vessel sealer or divider. D3 lymph node dissection was performed in all patients.
All patients underwent overlapped delta-shaped anastomosis during the procedure: the proximal and distal intestines were transected with two 60-mm linear staplers approximately 10 cm from the tumor (Figure 1A). Resected specimens were collected and stored in specimen bags immediately, and the remnant intestines were evaluated to ensure that they were with adequate blood supply and closed without tension. The proximal and distal intestines were fixed in an overlapped fashion approximately 8 cm long using a piece of absorbable suture to facilitate anastomosis. Two small incisions (10 mm) were made at one broken end and at the related intestinal wall of the other colon. After confirmation that there was no bleeding or intestinal mesentery volvulus, the two intestinal walls at the reversed mesenteric side were approximated and joined with a 60-mm linear stapler (Figure 1B). The warehouse was first placed in the small incision at one broken end of the intestine, the jaws closed temporarily and then the jaws opened before covering the screw anvil using the other broken end of the intestine, which is grasped to cover the screw anvil after the jaws are opened. No attempt was made to place the warehouse and screw anvil into the small incisions simultaneously. Three interrupted sutures were applied to pull the enterotomy, and the enterotomy was then closed with the application of another 60-mm linear stapler (Figure 1C). The staple line in the anastomotic stoma appeared as a curving obtuse triangle after the digestive tract reconstruction was completed (Figure 1D). The specimen was removed either from the anus, the abdominal scar of the previous surgery or a 5–6-cm Pfannenstiel incision that was made above the symphysis pubis at the border of the pubic hair (Figure 2).
 | Figure 1 Surgical procedures of overlapped delta-shaped anastomosis in laparoscopic surgery for colon cancer. |
 | Figure 2 Pfannenstiel incision made 2–3 cm above the symphysis pubis at the border of the pubic hair. |
Evaluations
The clinical characteristics, including age, gender, BMI, tumor location, American Society of Anesthesiologists score, previous abdominal operation history and preoperative chemotherapy, were analyzed. The collected surgical outcomes included the operative time, the blood loss anastomosis time and the removal method of the specimen. The resected specimens were reviewed by two pathologists, and the proximal resection margins, distal resection margins, number of harvested lymph nodes, tumor size and pathological TNM stages (eighth edition) were recorded. The length of the lesion signified the size of the tumor. The factors associated with postoperative recovery, including the average time to ground activities, first flatus, first defecations, postoperative hospitalization and postoperative visual analog scale scores on postoperative days 1, 3 and 5 (POD1, POD3, POD5), were compared. The short-term postoperative complications, such as anastomotic bleeding, anastomotic stenosis, anastomotic leakage, abdominal infection, pulmonary infection, incision infection and bowel obstruction, were recorded.
Follow-up
The first day after surgery represented the beginning of the follow-up period. Patients were routinely followed up at outpatient clinics at 2 weeks after discharge and every 3 months after the operation. The deadline of the follow-up period was April 1, 2018.
Statistical analysis
Statistical analysis was performed with SPSS software, version 22.0 for Windows (IBM Corporation, Armonk, NY, USA). Quantitative variables are presented as the mean and standard deviations, and were compared with the Student’s t-test. Qualitative variables are given as the number and percentage, and were compared with the χ2-test. P-values less than 0.05 were considered statistically significant.
Results
General data
A total of 97 patients were enrolled in the study, and no cases were lost to follow-up by April 1, 2018. There were no significant differences in terms of age, gender, BMI, American Society of Anesthesiologists scores, previous abdominal operation history and preoperative chemotherapy between the 3D and 2D groups (P>0.05). The details of the clinical characteristics are shown in Table 1.
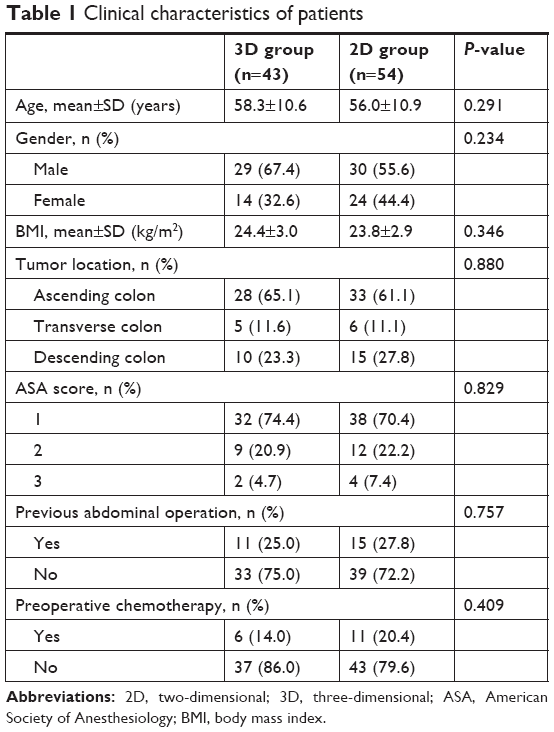 | Table 1 Clinical characteristics of patients |
Surgical and pathological findings
All patients underwent laparoscopic radical surgery and one-stage anastomosis without conversion to open surgery. The operation time (131.9±42.3 min vs 127.1±36.6 min, P=0.555) and intraoperative blood loss (54.7±48.4 mL vs 48.0±45.5 mL, P=0.512) were similar between groups. The mean anastomosis time for the 3D group was 13.2±3.0 min, significantly shorter than the 15.0±3.0 min for the 2D group (P=0.004). There were no differences in the length of the proximal resection margins (9.1±1.7 cm vs 9.3±2.0 cm, P=0.692) and distal resection margins (10.6±2.5 cm vs 10.2±3.3 cm, P=0.562). All patients underwent a D3 lymph node dissection, and the number of lymph nodes retrieved in the 3D and 2D groups were 21.1±7.7 and 22.3±9.4 per patient, respectively (P=0.483). There were no differences in the removal method of the specimen (P=0.802), tumor size (P=0.269) and tumor TNM stage (P=0.772). The operative and pathological details are provided in Table 2.
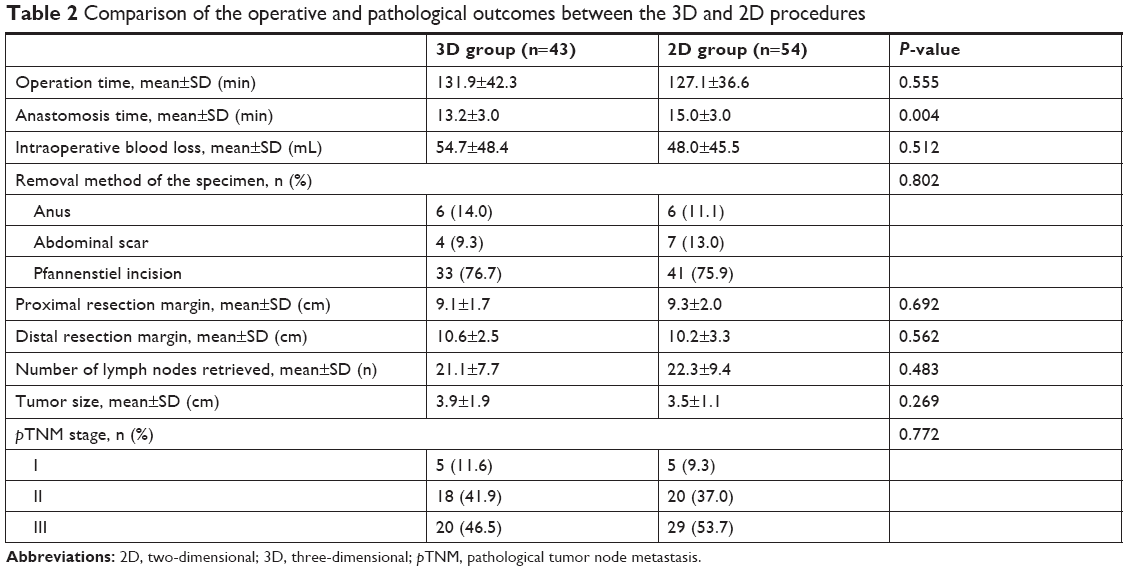 | Table 2 Comparison of the operative and pathological outcomes between the 3D and 2D procedures |
Postoperative recovery and complications
As shown in Table 3, no significant differences were observed between the groups in terms of the time to ground activities (1.2±0.4 days vs 1.3±0.5 days, P=0.222), first flatus (3.1±0.7 days vs 3.3±0.9 days, P=0.277), first defecations (5.3±0.9 vs 5.6±1.0 days, P=0.130) or postoperative hospitalization (6.9±1.1 days vs 6.6±0.9 days, P=0.096). Moreover, the postoperative visual analog scale scores were similar between the 3D and 2D groups on POD1 (4.3±0.9 vs 4.5±1.0, P=0.155), POD3 (2.9±0.7 vs 3.1±0.8, P=0.116) and POD5 (0.7±0.6 vs 0.8±0.7, P=0.280).
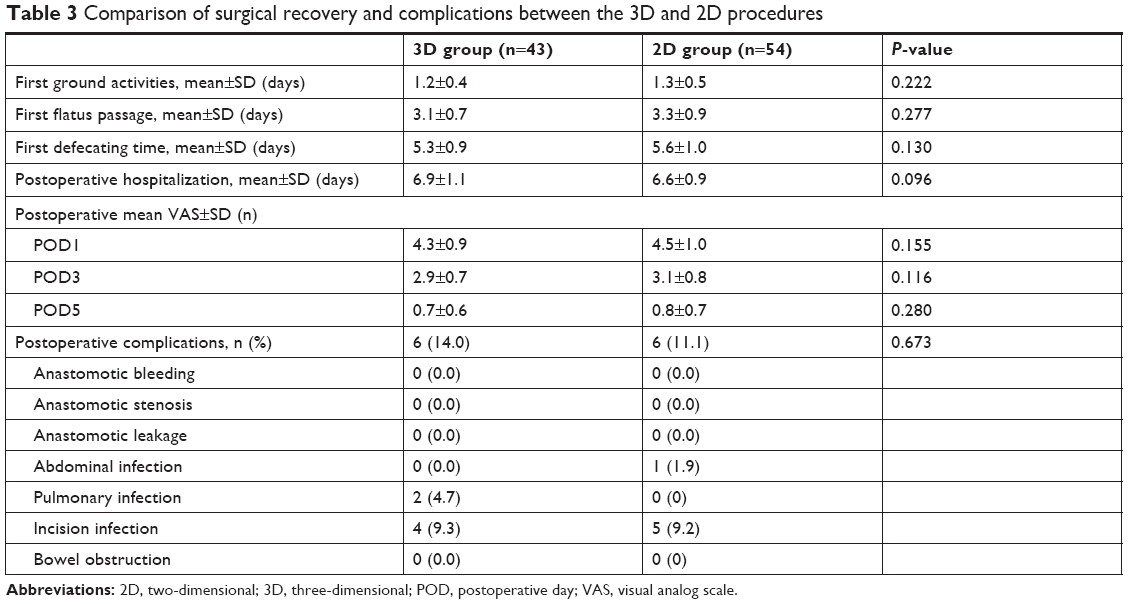 | Table 3 Comparison of surgical recovery and complications between the 3D and 2D procedures |
The overall rate of complications was comparable between the groups (14.0% vs 11.1%, P=0.673) (Table 3). No mobility related to the anastomosis, such as anastomotic bleeding, stenosis and leakage, occurred in any patient. Four patients in the 3D group and five patients in the 2D group suffered from incision infections. Two patients in the 3D group suffered pulmonary infection due to age and smoking history. All of these complications resolved successfully. In addition, one patient in the 2D group suffered an abdominal infection on the basis of an abdominal chyle leak, and the patient was managed successfully by conservative treatment that included fasting, parenteral nutrition, somatostatin and intravenous antibiotic.
Discussion
Colorectal cancer in People’s Republic of China has increased in incidence rapidly and has become the fifth most commonly diagnosed cancer among men and the fourth most common among women.7 Surgery remains the standard treatment for colorectal cancer with curative intent. Clinical application of laparoscopic surgery is becoming increasingly widespread with the advantages of fewer injuries, earlier postoperative recovery and lower complication rates compared to those of open surgery.8,9 The performance of totally laparoscopic surgery for colon cancer with intracorporeal anastomosis has been described in several studies, and it is expected to be less invasive than laparoscopic-assisted surgery with extracorporeal anastomosis.10,11
Overlapped delta-shaped anastomosis is a new procedure. Different from previous totally laparoscopic surgeries,12 we use three interrupted sutures to pull the enterotomy and then close the enterotomy using another 60-mm linear stapler instead of a running suture. We think the application of linear stapler can decrease the risk of anastomosis leakage and three interrupted sutures are more time-saving than a running suture. We applied the technique of overlapped delta-shaped anastomosis in totally laparoscopic treatment for colon cancer and verified its efficacy and safety.1 For overlapped delta-shaped anastomosis, disarticulation and anastomosis do not need to be performed extracorporeally; therefore, a smaller portion of the intestines is required to be freed laparoscopically. In addition, this anastomosis technique does not limit the location of the incision, so smaller Pfannenstiel incisions can be used using this technique; it is less invasive, gives better cosmetic results and can decrease the incidence of incisional hernias.13,14 Above all, this procedure is associated with fewer complaints of postoperative pain and leads to earlier postoperative recovery. However, due to the lack of stereoscopic vision, overlapped delta-shaped anastomosis by 2D laparoscopy may be difficult for beginners, who must identify anatomical structures, judge distances between tissues, and find and separate tissues at the anatomical level.
With advances in the technique, 3D laparoscopy has been developed as an alternative to conventional 2D laparoscopy. 3D laparoscopy is a dual-lens system in which two separate lenses are present within a single laparoscope along with two cameras. Each camera captures images that are then displayed and synchronized on a video monitor.15 Compared with 2D laparoscopy, it is easier to precisely grasp tissue, dissect tissue, separate tissues, stop bleeding and ligate vessels because 3D laparoscopy offers the surgeon a better depth of field and hand–eye coordination. Many obvious advantages of 3D laparoscopy have been reported: Sørensen et al16 found that 3D laparoscopy appeared to improve the speed and reduced the number of performance errors compared to 2D laparoscopy; Sinha et al17 found that in gynecological surgery, 3D laparoscopy took less time than 2D laparoscopy, enhanced the skills of a good surgeon and shortened the learning curve of a novice surgeon; and Currò et al18 found that the task of “side-to-side ileotransverse anastomosis” was a more time-saving procedure for 3D laparoscopy in laparoscopic right hemicolectomy.
We applied the technique of overlapped delta-shaped anastomosis in 3D totally laparoscopic surgery for colon cancer and compared its short-term effects with those of 2D laparoscopy. Overlapped delta-shaped anastomosis demands a high degree of spatial perception because of its more difficult procedures, such as suturing and knotting, compared to conventional extracorporeal anastomosis. We found that the anastomosis time was significantly shorter in the 3D group than in the 2D group (P=0.004), and we attributed this difference to the remarkable precision, accuracy and depth perception of 3D laparoscopy. There were no differences in terms of the operation time and blood loss, which are important evaluation parameters, possibly because of the relatively small number of patients and our rich experience in 2D laparoscopic surgery for colon cancer. There was also no significant difference in the number of lymph nodes retrieved in the 3D and 2D groups; however, the number of lymph nodes retrieved for both groups met the demands of the TNM cancer staging system set by the International Union Against Cancer and the American Joint Committee on Cancer that state that accurate pathological staging requires more than 12 lymph nodes examined in resected specimens.19 In terms of postoperative recovery and complication rates, no differences were found between the 3D and 2D groups (P>0.05). Overlapped delta-shaped anastomosis is a new anastomotic technique; therefore, complications related to the anastomosis were the main concerns of our study. It is fortunate that no patient suffered any mobility related to the anastomosis, such as anastomotic bleeding, stenosis or leakage. In addition, adequate mechanical bowel preparation before surgery plus use of an aseptic technique to the greatest extent possible resulted in no abdominal infections in any patient, despite the fact that the overlapped delta-shaped anastomosis is performed intracorporeally.
This was a retrospective study of short-term effects, and the presented outcomes were from a single surgeon and a relatively small number of patients. Therefore, prospective randomized controlled trials from multiple centers with larger sample sizes and longer follow-up periods are needed to validate our results.
Conclusion
We found that the use of 3D totally laparoscopic surgery for colon cancer using overlapped delta-shaped anastomosis was safe and effective, with satisfactory short-term outcomes. We also found that 3D laparoscopy is more time-saving than 2D for the procedure of overlapped anastomosis.
Acknowledgments
This research was supported by the Beijing Terry Fox Run Foundation of Cancer Foundation of China (No. LC2016B10) and CAMS Initiative for Innovative Medicine (CAMS-2017-I2M-4–002). The funders had no role in study design, data collection and analysis, decision to publish, or in the preparation of the manuscript.
Author contributions
HS collected the data and drafted the manuscript. HZ and WJ designed the study and helped revise the manuscript. PW and MB conceived the study and participated in its coordination. XW collected the surgical specimens. CZ participated in the discussions of the postoperative pathology. XW and ZZ participated in the data interpretation. All authors read and approved the final manuscript. All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Zhou HT, Wang P, Liang JW, Su H, Zhou ZX. Short-term outcomes of overlapped delta-shaped anastomosis, an innovative intracorporeal anastomosis technique, in totally laparoscopic colectomy for colon cancer. World J Gastroenterol. 2017;23(36):6726–6732. | ||
Zhang B, Tu JC, Fang J, Zhou L, Liu YL. Comparison of early-term effects between totally laparoscopic distal gastrectomy with delta-shaped anastomosis and conventional laparoscopic-assisted distal gastrectomy: a retrospective study. Int J Clin Exp Med. 2015;8(6):9967–9972. | ||
Kanaya S, Kawamura Y, Kawada H, et al. The delta-shaped anastomosis in laparoscopic distal gastrectomy: analysis of the initial 100 consecutive procedures of intracorporeal gastroduodenostomy. Gastric Cancer. 2011;14(4):365–371. | ||
Tanagho YS, Andriole GL, Paradis AG, et al. 2D versus 3D visualization: impact on laparoscopic proficiency using the fundamentals of laparoscopic surgery skill set. J Laparoendosc Adv Surg Tech A. 2012;22(9):865–870. | ||
Kunert W, Storz P, Kirschniak A. For 3D laparoscopy: a step toward advanced surgical navigation: how to get maximum benefit from 3D vision. Surg Endosc. 2013;27(2):696–699. | ||
McLachlan G. From 2D to 3d: the future of surgery? Lancet. 2011;378(9800):1368. | ||
Chen W, Zheng R, Baade PD, et al. Cancer statistics in China, 2015. CA Cancer J Clin. 2016;66(2):115–132. | ||
Allaix ME, Giraudo G, Mistrangelo M, Arezzo A, Morino M. Laparoscopic versus open resection for colon cancer: 10-Year outcomes of a prospective clinical trial. Surg Endosc. 2015;29(4):916–924. | ||
Niitsu H, Hinoi T, Kawaguchi Y, et al. Laparoscopic surgery for colorectal cancer is safe and has survival outcomes similar to those of open surgery in elderly patients with a poor performance status: subanalysis of a large multicenter case-control study in Japan. J Gastroenterol. 2016;51(1):43–54. | ||
Vignali A, Bissolati M, De Nardi P, Di Palo S, Staudacher C. Extracorporeal vs. intracorporeal ileocolic stapled anastomoses in laparoscopic right colectomy: an interim analysis of a randomized clinical trial. J Laparoendosc Adv Surg Tech A. 2016;26(5):343–348. | ||
Shapiro R, Keler U, Segev L, Sarna S. Laparoscopic right hemicolectomy with intracorporeal anastomosis: short- and long-term benefits in comparison with extracorporeal anastomosis. Surg Endosc. 2015;30(9):1–7. | ||
Reggio S, Sciuto A, Cuccurullo D, et al. Single-layer versus double-layer closure of the enterotomy in laparoscopic right hemicolectomy with intracorporeal anastomosis: a single-center study. Tech Coloproctol. 2015;19(12):745–750. | ||
Luijendijk RW, Jeekel J, Storm RK, et al. The low transverse Pfannenstiel incision and the prevalence of incisional hernia and nerve entrapment. Ann Surg. 1997;225(4):365–369. | ||
Iemsupakkul P, Kongchareonsombat W, Kijvikai K. Comparison of Pfannenstiel or extended iliac port site kidney extraction in laparoscopic donor nephrectomy: do we have consensus? Exp Clin Transplant. 2017;15(2):138–142. | ||
Sahu D, Mathew MJ, Reddy PK. 3D Laparoscopy – help or hype; initial experience of a tertiary health centre. J Clin Diagn Res. 2014;8(7):NC01–NC03. | ||
Sørensen SM, Savran MM, Konge L, Bjerrum F. Three-dimensional versus two-dimensional vision in laparoscopy: a systematic review. Surg Endosc. 2016;30(1):11–23. | ||
Sinha R, Sundaram M, Raje S, Rao G, Sinha M, Sinha R. 3D laparoscopy: technique and initial experience in 451 cases. Gynecol Surg. 2013;10(2):123–128. | ||
Currò G, Cogliandolo A, Bartolotta M, Navarra G. Three-dimensional versus two-dimensional laparoscopic right hemicolectomy. J Laparoendosc Adv Surg Tech A. 2016;26(3):213–217. | ||
West N. Commentary: lymph node retrieval in colorectal cancer specimens: national standards are achievable, and low numbers are associated with reduced survival. Colorectal Dis. 2010;12(4):309–311. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.