Back to Journals » Clinical Ophthalmology » Volume 17
Comparing Outcomes of Phacoemulsification and Endocyclophotocoagulation with Either Dual Blade Goniotomy (PEcK) or Two Trabecular Stents (ICE2)
Authors El Helwe H ![]() , Oberfeld B, Golsoorat Pahlaviani F, Falah H, Trzcinski J, Solá-Del Valle D
, Oberfeld B, Golsoorat Pahlaviani F, Falah H, Trzcinski J, Solá-Del Valle D ![]()
Received 16 August 2023
Accepted for publication 26 September 2023
Published 3 October 2023 Volume 2023:17 Pages 2879—2888
DOI https://doi.org/10.2147/OPTH.S431356
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Hani El Helwe, Blake Oberfeld, Fatemeh Golsoorat Pahlaviani, Henisk Falah, Jonathan Trzcinski, David Solá-Del Valle
Department of Ophthalmology, Harvard Medical School and Mass Eye and Ear, Boston, MA, USA
Correspondence: David Solá-Del Valle, Massachusetts Eye and Ear, Harvard Medical School, 243 Charles Street, Boston, MA, 02114, USA, Email [email protected]
Purpose: To compare outcomes of phacoemulsification and endocyclophotocoagulation with either dual blade goniotomy (PEcK) or two trabecular stents (ICE2).
Setting: Retrospective, nonrandomized comparative study from a level 3 triage center.
Methods: One hundred and seventy charts and a total of 1294 visits were reviewed following either PEcK or ICE2 from 2018 to 2022. One hundred and twenty-eight patients had PEcK and 42 underwent ICE2. Patients with less than 30 days of follow-up were excluded. The mean follow-up time was 505 ± 308 days. Two Kaplan–Meier curves (KM) assessed survival with ≤ baseline medications while maintaining (1) [GIC – Goal IOP Criteria] IOP ≤ goal IOP or (2) [PRC – Percent Reduction Criteria] IOP reduction ≥ 20% with 5 mmHg ≤ IOP ≤ 21 mmHg for at least two consecutive visits. IOP and medication burden reduction were compared using a paired t-test.
Results: Most patients were Caucasian (65%) and had mild-stage glaucoma (43%). The most common glaucoma type was primary open-angle glaucoma (58%). Average age was 72.2 years at the time of surgery. Mean preoperative IOP was 17.58 ± 4.98 mmHg on 3.00 ± 1.41 medications in PEcK and 15.36 ± 3.58 mmHg on 1.81 ± 1.11 medications in ICE2 (p = 0.015 for IOP; p < 0.001 for medications). Under GIC, the success rate was significantly higher in PEcK at POM6 (69% vs 46%, p < 0.001) and POY1 (63% vs 36%, p < 0.001). Under PRC, the success rate was significantly higher in PEcK at POM6 (73% vs 61%, p = 0.031) and POY1 (67% vs 50%, p = 0.028). Mean reductions at POY1 were 5.00 ± 4.31 mmHg on 1.35 ± 1.08 less medications after PEcK and 3.14 ± 2.83 mmHg on 1.01 ± 0.94 less medications after ICE2 (p < 0.001 at POY1 for IOP; p < 0.05 after POW6 for medications).
Conclusion: Both PEcK and ICE2 reduce medication and IOP from baseline, with PEcK having more favorable GIC and PRC success rates and greater IOP and medication reduction at 1 year.
Keywords: microinvasive glaucoma surgery, phacoemulsification, endocyclophotocoagulation, Kahook Dual Blade, iStent inject, surgical outcomes
Introduction
Microinvasive glaucoma surgeries (MIGS) have grown tremendously over the last decade. A 2016 Medicare review calculated a 426% increase in the total number of MIGS performed from 2012, which coincides with the first time surgical codes were assigned for these types of procedures.1 MIGS are favored in some patients over filtering and tube shunt surgeries for their superior safety profile.2,3 This high safety profile, however, is overshadowed by these procedures’ modest intraocular pressure (IOP) and medication-reducing effect, the reason they are better suited for patients with mild-to-moderate glaucoma. The potential for additive IOP-lowering and medication burden reduction without a significant increase in risk has led many surgeons to practice phacoemulsification in combination with one or more MIGS procedures.4 These combined MIGS (cMIGS) may result in more significant IOP and medication burden reduction than single MIGS (sMIGS), as suggested by some studies where cMIGS was more effective at reducing medication burden for at least 12 months.5
When phacoemulsification is performed in combination with endocyclophotocoagulation (ECP), a procedure that decreases aqueous production, the addition of a second, outflow-enhancing MIGS procedure may augment the overall IOP-lowering effect. Prior research has demonstrated greater reduction in both IOP and medication burden in the combinations of phacoemulsification/ECP/Kahook Dual Blade trabecular excision (New World Medical, Rancho Cucamonga, CA) (PEcK) and phacoemulsification/ECP/iStent inject (Glaukos Corporation, San Clemente, CA) (ICE2) compared to phacoemulsification/ECP alone.6–9 However, the relative effectiveness of PEcK and ICE2 remains unknown.
Methods
Overview
The Massachusetts General Brigham Institutional Review Board approved the study protocol. All research adhered to the Declaration of Helsinki and the Health Insurance Portability and Accountability Act.
Surgical Technique
All procedures were performed in the Glaucoma Service at Massachusetts Eye and Ear. All patients received eye blocks, standard phacoemulsification by fellowship-trained glaucoma surgeons was followed by insertion of the ECP probe into the sulcus after it was properly expanded with cohesive viscoelastic and treatment of 120 to 270 of ciliary processes in continuous wave mode at a power of 0.25–0.55 Watts until observing whitening and shrinkage of ciliary processes. An additional corneal incision was created with a keratome to complete the treatment for a total of 300 to 360 in some cases. Standard phacoemulsification and ECP surgical techniques were described in a previous study by Nirappel et al.10 After rotating the patient’s head for visualization and inserting additional cohesive viscoelastic into the anterior chamber, the gonioscopy lens was placed onto the cornea. For PEcK, the KDB was introduced into the anterior chamber, and an ab-interno trabecular excision was performed. The KDB was passed through the trabecular meshwork (TM) and 3.5–5.0 clock hours of TM were excised in an inside-out fashion until two strips were formed. For ICE2, the first and second iStent inject were inserted into the nasal TM 2.0–3.0 clock hours apart.
Subsequently in both procedures, thorough removal of viscoelastic was done followed by injection of intracameral antibiotics (0.1 cc moxifloxacin or cefuroxime) and acetylcholine chloride intraocular solution (0.2cc). Dexamethasone was injected subconjunctivally. A drop of prednisolone and antibiotic were placed on the eye before it was patched and shielded. Unless there was a systemic contraindication, methylprednisolone (1 gram) was given intravenously, followed by a 6-day taper of oral methylprednisolone with an initial dose of 24 mg reduced by 4 mg daily.
Population
Subjects with known glaucoma and visually significant cataract were identified from surgical records at Massachusetts Eye and Ear between January 2018 and July 2022 and were included if the operative report confirmed having undergone PEcK or ICE2. Patients with 30 days or less of recorded follow-up were filtered out from our study population to avoid a bias caused by early failures. If an additional procedure was performed at the time of PEcK or ICE2, or if age was less than 18 years at the time of surgery, these patients were excluded. If a patient underwent surgery on both eyes, only the first eye was included.
Data Collection
A total of 1294 visits from 170 patient charts were reviewed following either PEcK or ICE2. Demographic data were gathered from the electronic medical records of study subjects and included age, gender, race/ethnicity, glaucoma type, and best-corrected visual acuity (BCVA). Baseline IOP was defined as the average of measurements made using Goldmann applanation tonometry on the last two visits prior to surgery. The baseline number of medications prescribed was recorded as the number of constituent agents if fixed-dose combination medications were used. Patients were assigned to mild, moderate, or severe glaucoma based on the American Academy of Ophthalmology Preferred Practice Pattern guidelines (ICD-10 Glaucoma Reference Guide).11 Prior history of ocular surgery or laser procedure in the operative eye was recorded. The goal IOP was a target set preoperatively that corresponded to a 20% IOP reduction from the level at which glaucoma progression was first reported.6 Postoperative data were collected from follow-up visits at postoperative day 1 (POD1), week 6 (POW6), month 3 (POM3), month 6 (POM6), year 1 (POY1), and month 18 (POM18) in agreement with the World Glaucoma Association’s Guidelines on Design and Reporting of Glaucoma Surgical Trials.12 Recorded measurements included IOP, BCVA, number of glaucoma medications, and presence of postoperative complications. If subjects required further glaucoma surgery, this was recorded.
Outcomes
Primary outcome measures were Kaplan–Meier survival curves based on goal and IOP reduction criteria. Two Kaplan–Meier curves (KM) assessed survival with ≤ baseline medications while maintaining (1) [GIC – Goal IOP Criteria] IOP ≤ goal IOP or (2) [PRC – Percent Reduction Criteria] IOP reduction ≥ 20% with 5 mmHg ≤ IOP ≤ 21 mmHg for at least two consecutive visits. IOP and medication burden reduction were compared using a paired t-test. Additionally, we examined the pattern of change in IOP and in the number of glaucoma medications over 18 months for each individual procedure and between PEcK and ICE2. Secondary outcomes included the pattern of change in Logarithm of the Minimum Angle of Resolution (logMAR) and the incidence of postoperative complications.
Statistical Analysis
This paper used the statistical analysis software package(s) R Studio Version 4.2.1. KM survival analyses were performed to calculate success probabilities subsequent to a 30-day postoperative grace period. P values were generated using Chi-squared tests to calculate the probability of achieving a 20% or greater reduction in IOP from preoperative measurements at any follow-up point and to check for significant differences in any baseline characteristics. T-tests were used to check for statistically significant changes from baseline for mean IOP and mean number of medications. We used the LogMAR representation of the Snellen Visual Acuities, substituting count fingers and hand motion with 2 for the former and 3 for the latter. No patients had no light perception or light perception. Our analysis was conducted in line with the analysis described by work done by Chang et al.13 Patients with 30 days or less of recorded follow-up were filtered out of our study population to avoid a bias caused by early failures. For all statistical tests, both t-tests and Chi-squared tests, a P < 0.05 was set for establishing significance.
Results
Baseline Characteristics
170 eyes of 170 patients were included, with 128 subjects who underwent PEcK and 42 who underwent ICE2 between January 2018 and July 2022 at MEE with an average study follow-up of 505 ± 308 days. Subjects had a mean age of 72.2 and were predominantly white (65%). A majority of patients had primary open-angle glaucoma (58%), were mild or moderate stage (75%), and were surgically naïve (90%). About one-third of patients (34%) had previously undergone a laser procedure, predominantly laser trabeculoplasty, on their operative eye. The PEcK cohort was more likely at baseline to have higher IOP (p = 0.02), a higher number of glaucoma medications (p < 0.01), and prior laser (p < 0.01). The PEcK group also consisted of a smaller proportion of patients with mild-to-moderate glaucoma compared to the ICE2 group (p < 0.001). In the PEcK group, a mean of 224 (±32) degrees of ciliary processes was treated with a mean power of 0.35 (±0.05) Watts. A mean of 4 clock hours of TM was excised. In the ICE2 group, a mean of 210 (±37) degrees of ciliary processes was treated with a mean power of 0.38 (±0.04) Watts of laser power. Demographic and baseline characteristics are summarized in Table 1
 |
Table 1 Baseline Demographics, Disease Characteristics, and Endocyclophotocoagulation Parameters in Both PEcK and ICE2 Cohorts |
Procedural and Comparative Efficacy
Two KM curves assessed survival with ≤ baseline medications while maintaining (1) [GIC – Goal IOP Criteria] IOP ≤ goal IOP or (2) [PRC – Percent Reduction Criteria] IOP reduction ≥ 20% with 5 mmHg ≤ IOP ≤ 21 mmHg for at least two consecutive visits (Figures 1 and 2). The survival probabilities at selected time points of interest are listed in Table 2. There were significant differences in the survival curves of PEcK and ICE2 groups under both goal IOP criteria (GIC) and percent reduction criteria (PRC) (P < 0.05, Log rank test). Under the GIC, the cumulative probability of survival was 73.3% in the PEcK group and 60.6% in the ICE2 group at month 6 (P = 0.031), and 66.8% in the PEcK group and 36.4% in the ICE2 group at year 1 (P = 0.028). Under the PRC, the cumulative probability of survival was 69.0% in the PEcK group and 46.3% in the ICE2 group at month 6 (P < 0.001), and 63% in the PEcK group and 36.4% in the ICE2 group at year 1 (P < 0.001, Table 2).
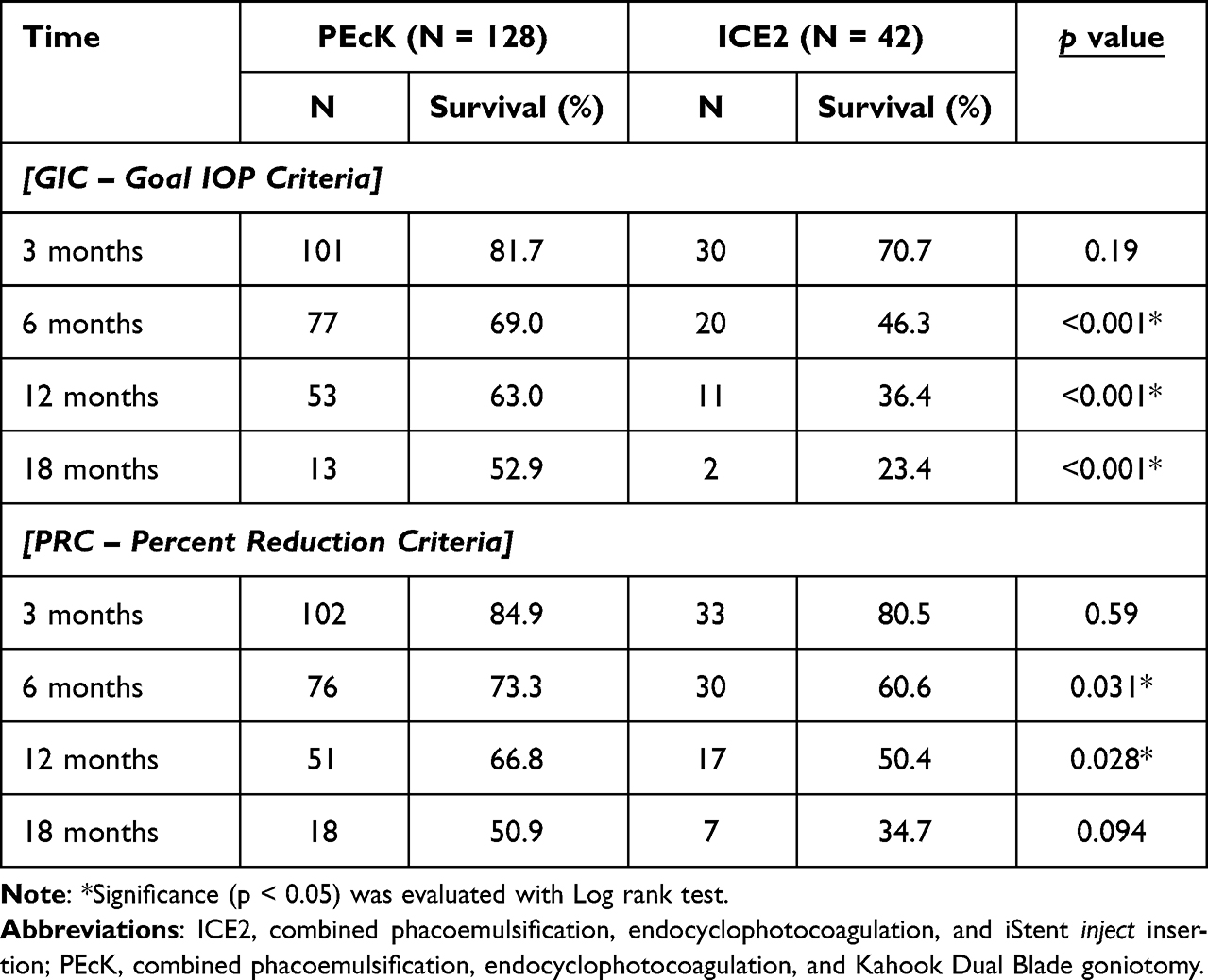 |
Table 2 Percentage of Patients in PEcK and ICE2 Groups That Achieved (1) [GIC – Goal IOP Criteria] IOP ≤ Goal IOP or (2) [PRC – Percent Reduction Criteria] IOP Reduction ≥ 20% with 5 mmHg ≤ IOP ≤ 21 mmHg for at Least Two Consecutive Visits at POM3, POM6, POM12 and POM18 |
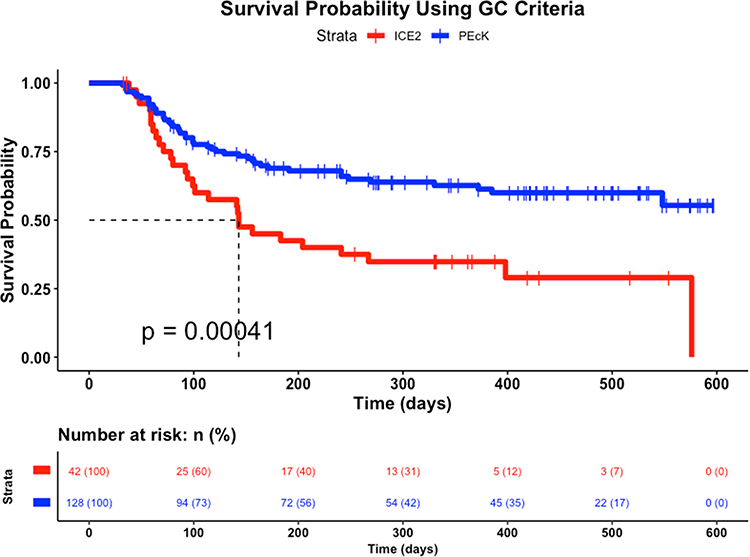 |
Figure 1 Survival comparison for PEcK vs ICE2 under [GIC – Goal IOP Criteria] with ≤ baseline medications while maintaining IOP ≤ goal IOP for at least two consecutive visits. |
 |
Figure 2 Survival comparison for PEcK vs ICE2 under [PRC – Percent Reduction Criteria] with ≤ baseline medications while maintaining IOP reduction ≥ 20% with 5 mmHg ≤ IOP ≤ 21 mmHg for at least two consecutive visits. |
A multivariate Cox Proportional Hazards (PH) model was constructed to account for differences in baseline IOP, baseline number of medications, glaucoma stage and prior history of laser procedure on the operative eye. Glaucoma type was not selected in the final Cox PH model to avoid overfitting. Higher baseline IOP was associated with an 18% and 15% reduced risk of failure under GIC (p < 0.001) and PRC (p < 0.001), respectively. A higher baseline number of medications was associated with a 17% reduced risk of failure under GIC (p = 0.048). Glaucoma stage and prior history of laser procedure were not a significant factor under both criteria.
The PEcK and ICE2 procedures resulted in significant patterns of IOP and medication reduction from baseline (all P < 0.001) up to 18 months. At POM6, mean IOP reduction was 5.12 ± 4.57 mmHg on 1.47 ± 1.10 less medications after PEcK, and 2.67 ± 2.09 mmHg on 0.84 ±0.85 less medications after ICE2 (p = 0.09 for IOP; p < 0.01 for medications). At POY1, mean IOP reduction was 5.00 ± 4.31 mmHg on 1.35 ± 1.08 less medications after PEcK, and 3.14 ± 2.83 mmHg on 1.01 ± 0.94 less medications after ICE2 (p < 0.01 for IOP; p = 0.03 for medications). The PEcK procedure had higher IOP reduction than the ICE2 procedure at all postoperative timepoints. This difference only trended toward statistical significance at POM3 (p = 0.06) and POM6 (p = 0.09) but was statistically significant at POY1 (P < 0.001) and POY1.5 (P = 0.006). The mean reduction in medications was significantly greater in the PEcK group compared to the ICE2 group up to POY1, but similar to the ICE2 group at POY1.5 (p = 0.93). Mean LogMAR BCVA was significantly improved from baseline up to POY1 in both groups. There were no between-group differences in the pattern of visual acuity improvement at any time point. Mean IOP and mean medication reduction at selected time points of interest are listed in Table 3.
 |
Table 3 Mean Intraocular Pressure (IOP) and Mean Medication Reduction at Postoperative Week 6, Months 3, 6, 12, and 18 in Both PEcK and ICE2 Cohorts |
Postoperative Complications
Postoperative corneal edema and anterior segment inflammation (AC grade of 1+ cells or greater based on the Standardization of Uveitis Nomenclature criteria) rates were comparable between both groups and resolved within 3 months in most cases. Early postoperative hyphema and microhyphema (up to 1 month post-op) were significantly more common (P = 0.007) in the PEcK group but resolved within 3 months in 96.5% of cases. The number of persistent hyphema and microhyphema cases present at any time point beyond month 3 was similar between both groups (p > 0.99). By the end of follow-up time, lens heme was present in 4.8% of PEcK cases versus none of the ICE2 cases; this difference, however, did not attain statistical significance. There was a single case of cystoid macular edema (CME) in a patient who underwent ICE2 and no patients experienced endophthalmitis. Additional surgical intervention was pursued within 12 months for 5 PEcK subjects (6% of total eyes), who had higher baseline IOP (25.83 ± 9.55) and medication burden (3.83 ± 0.98). None of the ICE2 patients required additional surgical intervention. The interventions included three Baerveldt Glaucoma Implants, one Ahmed Glaucoma Implant, and one trabeculectomy. Postoperative complications and procedures are summarized in Table 4.
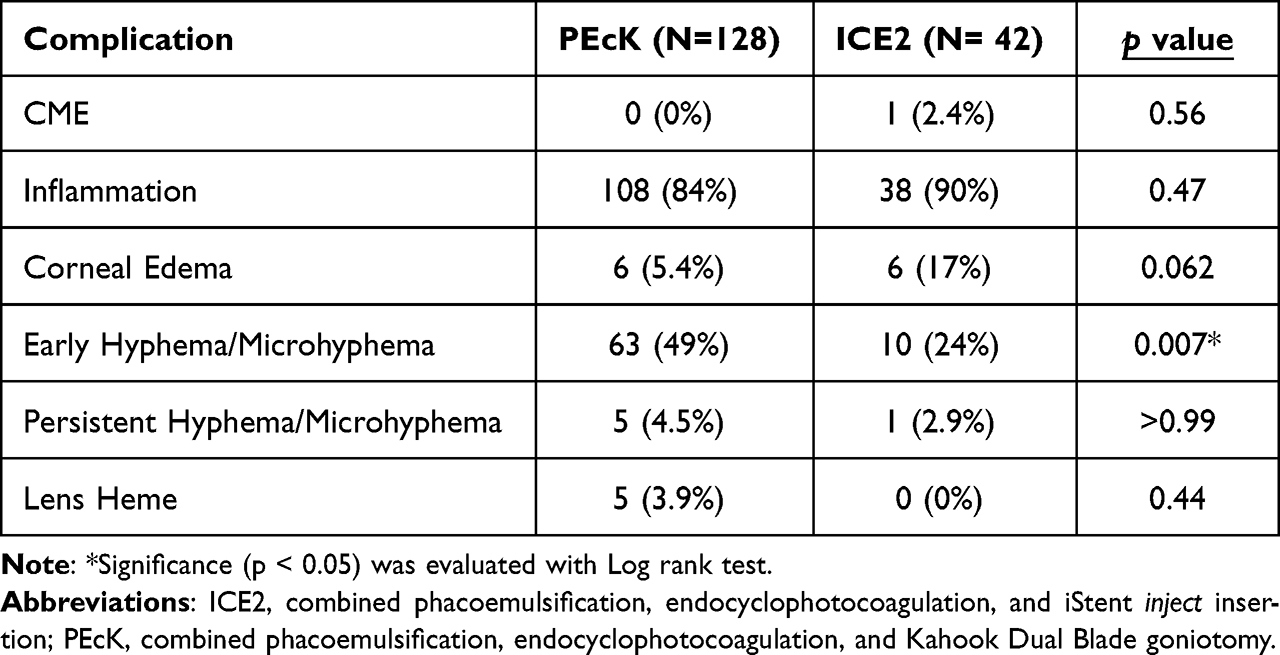 |
Table 4 Postoperative Complications in Both PEcK and ICE2 Cohorts |
Discussion
Patients who underwent either PEcK or ICE2 experienced significant reductions in both IOP and medication burden throughout 18 months. Our study compares the IOP-lowering and medication-reducing effects of PEcK versus ICE2 in a population with predominantly mild-to-moderate glaucoma. We demonstrate for the first time that PEcK results in greater patterns of IOP and medication burden reduction than ICE2, as well as more favorable KM survival estimates, at various time points within the 18-month follow-up period.
The PEcK procedure, to the best of our knowledge, has only been reported in two prior retrospective studies.6,9 At 12 months following PEcK, mean IOP was decreased by 5.1 mmHg on 1.6 fewer medications in 53 subjects previously described in our prior study comparing PEcK to phacoemulsification/ECP/first generation single-stent iStent (ICE1).6 These 12-month differences are similar in magnitude to those reported in 21 subjects by Izquierdo et al (5.52 mmHg decrease, 1.2 fewer medications).9 In our study, mean IOP was reduced by 5.00 mmHg on 1.35 fewer medications in 128 subjects, which appears to conform with the above two studies.
For ICE2, 12-month mean IOP was decreased by 3.14 mmHg on 1.01 fewer medications. Only Pantalon et al have previously studied the outcomes of ICE2 in a population with higher baseline IOP (19.97 mmHg) and comparable medication number (2.22), reporting that 12-month mean IOP was decreased by 6.92 mmHg on 0.98 fewer medications.8 Our study demonstrates that ICE2 is also effective in patients with lower baseline IOP.14 Additionally, the 12-month differences following ICE2 reported in this study suggest that the second-generation two-stent iStent inject may better decrease IOP and medication burden than ICE1, when compared to our prior study in a comparable population (1.4 mmHg decrease, 0.76 fewer medications).6 Comparison with Ferguson et al, which is the only other study that reports on ICE1, is limited by substantially different study populations, given the higher baseline IOP (21.49 mmHg), which may have led to a higher 12-month IOP reduction (7.14 mmHg).7
PEcK demonstrated significantly greater patterns of IOP and medication reductions at various time points throughout the 18-month follow-up period. This difference could potentially be attributable to the larger opening in the TM created by ab interno trabeculectomy with the KDB compared to the two iStents.7 However, the PEcK group also had significantly greater IOP and number of medications at baseline compared to the ICE2 group. And though we constructed a multivariate Cox proportional hazards to account for these differences, the observations relating to IOP and medication reduction must be interpreted with caution.
PEcK had significantly higher efficacy at maintaining IOP ≤ goal IOP with ≤ baseline medications (GIC). Survival probability utilizing the GIC criteria was 63% and 36% at POY1 for the PEcK and ICE2 cohorts, respectively (p < 0.001). ICE2 procedures showed significantly lower efficacy than PEcK at maintaining IOP reduction ≥ 20% with 5 mmHg ≤ IOP ≤ 21 mmHg with ≤ baseline medications (PRC), with survival probabilities of 67% and 50% at POY1, for the PEcK and ICE2 cohorts, respectively (p < 0.001). As previously mentioned, higher baseline IOP was associated with greater posttreatment reductions in IOP under both success criteria, and higher baseline number of medication was associated with greater posttreatment reductions in medications under GIC. This may suggest that patients with higher baseline IOP were more likely to achieve a ≥20% reduction and maintain ≤ goal IOP. However, in the multivariate Cox adjusted KM curves, the differences in survival between the two groups were maintained. This supports a significant difference in survival between the two cohorts and suggests that PEcK has more favorable success rates compared to ICE2 based on our survival criteria.
Both procedures were found to be effective at restoring vision and were safe, with a low incidence of complications. The greater incidence of early postoperative hyphema after PEcK may limit its applicability in monocular patients or those who are intolerant to transient periods of blurry vision. This disadvantage, however, may be outweighed by the procedure’s greater efficacy, especially in more moderate-to-severe glaucoma patients who require substantial IOP and medication lowering but who are opposed to or may wish to postpone filtering surgery.
This study may be limited by its retrospective design, relatively small sample size for the ICE2 group, and patient attrition over time. There is also a risk of selection bias, as the choice of the procedure (ICE2 vs PEcK) and reinstating medications was made at each surgeon’s discretion. Although the risk of selection bias cannot be eliminated, it may be attenuated by the makeup of surgeons performing the cases. These surgeons do not routinely share patients or collaborate on cases. Finally, follow-up duration was limited, and we cannot at the time comment on the longer-term success of either procedure. However, given the popularity of MIGS and the practice trends toward combining different MIGS as well as the paucity of comparative data regarding cMIGS, our data provide a reasonable and novel comparison between PEcK and ICE2. These data could be utilized in future studies for power and sample-size calculations.
Conclusion
Overall, we demonstrate that both PEcK and ICE2 procedures reduce IOP and medication number from baseline and up to 12 months post-op, with PEcK having significantly greater IOP control and medication burden reduction, as well as more favorable GIC and PRC survival rates. Although the larger opening in the TM created during PEcK was associated with a significantly higher rate of early hyphema and microhyphema, this may be outweighed by the procedure’s greater efficacy especially in moderate-to-severe glaucoma patients. Additional studies that prospectively examine larger cohorts over longer follow-up are needed to fully investigate these cMIGS procedures, although we realize that performing these prospective studies may not be cost-effective, which we believe further augments the value of the data we have presented.
What Was Known
- Combining multiple microinvasive glaucoma procedures (cMIGS) with different mechanisms to lower intraocular pressure (IOP) may be a safe and effective therapeutic approach in patients undergoing phacoemulsification.
- Both phacoemulsification/endocyclophotocoagulation/Kahook Dual Blade goniotomy (PEcK) and phacoemulsification/endocyclophotocoagulation/two-stent iStent inject (ICE2) have greater efficacy than phacoemulsification/endocyclophotocoagulation alone.
- Understanding the relative efficacies of different MIGS combinations is integral to clinical decision-making, but the relative effectiveness of PEcK versus ICE2 is uncertain.
What This Paper Adds
- Both PEcK and ICE2 lead to significant patterns of reduction in IOP and medication burden throughout 12 months, supplementing the evidence that combination MIGS procedures are effective.
- PEcK appears to confer significantly greater IOP and medication reduction than ICE2, as well as more favorable GIC and PRC survival rates.
Data Sharing Statement
De-identified data are available upon reasonable request to corresponding authors.
Acknowledgments
The authors are grateful to Mr. and Mrs. Charles and Anne Gifford (Concord, Massachusetts, USA), Mr. and Mrs. Joseph and Cathey S. Leitch (Charleston, South Carolina, USA), as well as the Sinskey Foundation (Los Angeles, California, USA) for their generous donations that supported this research. Meeting presentation at The European Society of Cataract and Refractive Surgeons, Messe Wien Exhibition and Congress Center, Vienna, Austria, September 8–12, 2023.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or for-profit sectors.
Disclosure
D. Solá-Del Valle received financial support from Allergan, an AbbVie company, for giving lectures related to the XEN Gel Stent in 2021, a device that is unrelated to this study. The authors report no other conflicts of interest in this work.
References
1. Rathi S, Andrews CA, Greenfield DS, Stein JD. Trends in glaucoma surgeries performed by glaucoma subspecialists versus nonsubspecialists on medicareBeneficiaries from 2008 through 2016. Ophthalmology. 2021;128(1):30–38. doi:10.1016/j.ophtha.2020.06.051
2. Sng CCA, Barton K. Minimally Invasive Glaucoma Surgery. Springer Nature; 2021. doi:10.1007/978-981-15-5632-6
3. Birnbaum FA, Neeson C, Solá-Del Valle D. Microinvasive glaucoma surgery: an evidence-based review. Semin Ophthalmol. 2021;36(1–2):1–15. doi:10.1080/08820538.2021.1903513
4. Pillunat LE, Erb C, Jünemann AG, Kimmich F. Micro-invasive glaucoma surgery (MIGS): a review of surgical procedures using stents. Clin Ophthalmol. 2017;11:1583–1600. doi:10.2147/OPTH.S135316
5. Mai DD, Ingram Z, Oberfeld B, Solá-Del Valle D. Zoe Ingram, Blake Oberfeld & David Solá-Del Valle (2023) combined microinvasive glaucoma surgery – a review of the literature and future directions. Semin Ophthalmol. 2023;38(6):529–536. doi:10.1080/08820538.2023.2181665
6. Klug E, Chachanidze M, Nirappel A, et al. Outcomes of phacoemulsification and endoscopic cyclophotocoagulation performed with dual blade ab interno trabeculectomy or trabecular micro-bypass stent insertion. Eye. 2021;36(2). doi:10.1038/s41433-021-01475-4
7. Ferguson TJ, Swan R, Sudhagoni R, Berdahl JP. Microbypass stent implantation with cataract extraction and endocyclophotocoagulation versus microbypass stent with cataract extraction for glaucoma. J Cataract Refract Surg. 2017;43(3):377–382. doi:10.1016/j.jcrs.2016.12.020
8. Pantalon AD, Barata ADDO, Georgopoulos M, Ratnarajan G. Outcomes of phacoemulsification combined with two iStent inject trabecular microbypass stents with or without endocyclophotocoagulation. Br J Ophthalmol. 2020;104(10):1378–1383. doi:10.1136/bjophthalmol-2019-315434
9. Izquierdo JC, Agudelo N, Rubio B, et al. Combined phacoemulsification and 360- degree endocyclophotocoagulation with and without a kahook dual blade in patients with primary open-angle glaucoma. Clin Ophthalmol. 2021;15:11–17. doi:10.2147/OPTH.S282440
10. Nirappel A, Klug E, Neeson C, et al. Transscleral vs endoscopic cyclophotocoagulation: safety and efficacy when combined with phacoemulsification. BMC Ophthalmol. 2023;23(1):129. doi:10.1186/s12886-023-02877-6.
11. Gedde SJ, Vinod K, Wright MM, et al. primary open-angle glaucoma preferred practice pattern®. Ophthalmology. 2021;128(1):71–P150. doi:10.1016/j.ophtha.2020.10.022
12. Shaarawy TM, Sherwood MB, Grehn F, Editors. WGA Guidelines on Design and Reporting of Glaucoma Surgical Trials. Amsterdam, the Netherlands: Kugler Publications; 2009.
13. Chang EK, Gupta S, Chachanidze M, Miller JB, Chang TC, Solá-Del Valle DA. Combined pars plana glaucoma drainage device placement and vitrectomy using a vitrectomy sclerotomy site for tube placement: a case series. BMC Ophthalmol. 2021;21(1):106. doi:10.1186/s12886-021-01872-z.
14. Chang EK, Gupta S, Chachanidze M, Hall N, Chang TC, Solá-Del Valle D. Safety and efficacy of microinvasive glaucoma surgery with cataract extraction in patients with normal-tension glaucoma. Sci Rep. 2021;11(1):8910. doi:10.1038/s41598-021-88358-6.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Multicenter Effectiveness and Disease Stability Through 3 Years After iStentTrabecular Micro-Bypass with Phacoemulsification in Glaucoma and Ocular Hypertension
Clement C, Howes F, Ioannidis A, Shiu M, Manning D, Lusthaus JA, Skalicky SE, Goodwin TW
Clinical Ophthalmology 2022, 16:2955-2968
Published Date: 1 September 2022
Comparison of Efficacy of Combined Phacoemulsification and iStent Inject versus Combined Phacoemulsification and Hydrus Microstent
Chee WK, Yip VCH, Tecson IO, Chua CH, Ang BCH, Kee AR, Hu JY, Kan TCJ, Yip LWL
Clinical Ophthalmology 2023, 17:1151-1159
Published Date: 14 April 2023
Impact of Surgical Sequence on Outcomes of Combined Phacoemulsification and Kahook Dual Blade KDB Goniotomy: A 1-Year Prospective Comparative Study
Mechleb N, Nemr A, Tomey K, Cherfan DG, Cherfan G, Dorairaj S, Abdelmassih Y, Khoueir Z
Clinical Ophthalmology 2026, 20:593122
Published Date: 25 May 2026