Back to Journals » International Journal of Women's Health » Volume 17
Comparing Outcomes and Risks of Multiple Gestations: Assisted versus Spontaneous Conceptions
Authors Alarfaj RK ![]() , Alwahhabi A
, Alwahhabi A ![]() , Alshalan R
, Alshalan R ![]() , Alabdulkareem Y, Alabdulkareem D, Alkharouf F
, Alabdulkareem Y, Alabdulkareem D, Alkharouf F ![]()
Received 13 June 2025
Accepted for publication 17 October 2025
Published 8 November 2025 Volume 2025:17 Pages 4347—4357
DOI https://doi.org/10.2147/IJWH.S544868
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Rwan K Alarfaj,1,2 Aseel Alwahhabi,1,2 Renad Alshalan,1,2 Yara Alabdulkareem,1,2 Deamah Alabdulkareem,1,2 Feras Alkharouf2,3
1College of Medicine, King Saud bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia; 2King Abdullah International Medical Research Center (KAIMRC), Riyadh, Saudi Arabia; 3Obstetrics and Gynecology Department, Specialized Hospital for Women’s Health, Ministry of National Guard Health Affairs, Riyadh, Saudi Arabia
Correspondence: Aseel Alwahhabi, Email [email protected]
Background: Multiple gestations are increasingly prevalent worldwide, largely due to the rising use of Assisted Reproductive Technology (ART). Compared with singleton pregnancies, they are associated with substantially higher maternal and neonatal risks, including preterm birth, pregnancy complications, and adverse neonatal outcomes. However, regional data are limited, particularly from Saudi Arabia, where cultural, demographic, and healthcare system factors may uniquely influence these outcomes. Addressing this gap is essential to improve obstetric care, support patient counseling, and inform region specific health policies.
Objective: This study aimed to evaluate and compare maternal and neonatal outcomes in twin and triplet pregnancies conceived spontaneously versus via ART in Saudi Arabia.
Methods: A retrospective chart review was conducted at the Women’s Health Hospital, National Guard Hospital, Riyadh, covering the period from January 2022 to December 2023. Medical records of all twin and triplet pregnancies were reviewed. Data collected included maternal characteristics (age, BMI, gravida, parity, gestational age, complications) and neonatal outcomes (presentation, admission, birthweight, Apgar score).
Results: A total of 233 pregnancies were analyzed (222 twins, 11 triplets). The mean gestational age was 37.1 weeks for twins and 33.5 weeks for triplets. Most births occurred at late preterm gestation (> 32 weeks, 92.7%). Gestational diabetes mellitus (22.3%) and preterm birth (70.4%) were the most frequent complications. Triplet pregnancies were associated with earlier preterm deliveries, malpresentation, and a higher prevalence of ART use (30.5%). Cesarean delivery was the dominant mode of birth (88.8%). Neonatal admissions to NICU/ICN were mainly due to prematurity and neonatal respiratory distress syndrome. Independent predictors of ART included parity, chorionicity, amnionicity, and maternal morbidity.
Conclusion: Multiple gestations carry significant maternal and neonatal risks, with triplet pregnancies conceived via ART showing increased vulnerability to preterm birth, lower gestational age, and malpresentation. Cesarean section was the predominant delivery mode, and neonatal complications were largely related to prematurity. These findings underscore the need for targeted obstetric care in ART conceived multiple gestations and call for larger studies to inform clinical management and improve outcomes in Saudi Arabia.
Keywords: assisted reproductive technology, multiple pregnancy, spontaneous conception, maternal outcomes, neonatal outcomes, Saudi Arabia
Introduction
Multiple gestation is defined as a pregnancy in which a woman carries two or more fetuses in her womb.1 Recent data highlight that multiple pregnancies continue to be a significant global concern, with the vast majority being twin gestations rather than higher-order multiples. Large population studies show that between 2010 and 2015, the worldwide twinning rate reached about 12 per 1000 deliveries, which results in nearly 1.6 million twin births annually.2 More recent data indicate that in 2021, twin births accounted for 21.3 per 1000 live births, while triplet and higher-order births occurred at a rate of 80 per 100,000 live births.3 The prevalence distribution of multiple pregnancy varies by region, being highest in sub-Saharan Africa and lowest in East Asia.2 Triplet pregnancies occur in approximately 93 per 100,000 deliveries worldwide, with spontaneous triplets occurring in about 1 in 8000 pregnancies.4 The incidence of multiple pregnancies is rising due to factors like genetics, older maternal age, race, and increased use of assisted reproductive technology (ART).5 Multiple gestations carry high maternal risks, including gestational diabetes (GDM), preterm birth, hemorrhage, and preterm rupture of membranes (PROM), as well as neonatal morbidity and mortality6 which aligns with findings from the World Health Organization (WHO), which reported that maternal and neonatal mortality rates are significantly higher in multiple pregnancies worldwide. Twin pregnancies carry a much higher risk of severe maternal complications including postpartum hemorrhage, chronic hypertension, and even maternal death compared to singleton pregnancies, with the risk increasing by about 2.1 to 3.9 times.7 In China, these pregnancies are associated with higher risks of cesarean delivery, anemia, preterm labor, GDM, small for gestational age (SGA), low birthweight (LBW), and neonatal intensive care unit (NICU) admission.8 Similarly, in Turkey, cesarean delivery, anemia, hypertensive disorders, and GDM were common, with no triplets born after 34 weeks and most being SGA and LBW.9 A Swedish study on triplets reported 97% cesarean rates, all infants preterm, 34% SGA, and 92% needing neonatal care.10 Studies in Saudi Arabia provide insight into multiple gestation outcomes. Premature births and LBW infants were identified as the main contributors to perinatal deaths in twin pregnancies.11 A study conducted in the United States found that the rise in multiple gestations, mainly due to the increased use of ART, is associated with a corresponding rise in maternal and neonatal complications. This finding aligns with similar studies conducted in Turkey, China and Saudi Arabia, which also highlight heightened risks linked to multiple pregnancies.12 Additionally, a study conducted in Germany compared maternal factors and associated outcomes, it found that mothers with increased age and high BMI are more prone to spontaneous twin pregnancies, experiencing similar complications to those associated with ART from earlier studies, but with no significant increase in NICU admissions.13 In triplet pregnancies specifically in Saudi Arabia, preterm labor, anemia, and cesarean deliveries were common complications.14 Similarly, regionally, preterm labor was also the most frequent complication in another study, with neonatal issues primarily involving neonatal respiratory distress syndrome (NRDS).15 Moreover, locally, triplet pregnancies had shorter gestational lengths, higher cesarean rates, increased NICU admissions, and LBW, with neonatal complications including hyaline membrane disease, jaundice, and sepsis.1 Research on maternal and neonatal outcomes in multiple gestations in Saudi Arabia is crucial due to the rising incidence of multiple pregnancies and the significant maternal and neonatal risks involved. Understanding these risks highlights the need for region-specific prenatal planning, better prenatal care, and clear policies to guide assisted reproductive practices. Research in this area also plays a vital role in shaping targeted interventions that can lower morbidity and mortality rates while ensuring more efficient use of maternal and neonatal healthcare resources. Comparing twin and triplet gestations conceived spontaneously and via ART clarifies challenges, improves management and counseling, and enhances tailored healthcare practices. This study aims to compare outcomes between twin and triplet pregnancies and identify factors linked to adverse outcomes to improve management in Saudi Arabia.
Materials and Methods
This retrospective chart review was conducted on twin and triplet pregnancies from 1st of January 2022 to 31st of December 2023 at the Women’s Health Hospital, National Guard Health Affairs, Riyadh, Saudi Arabia. Initially, 286 patients were identified, but after excluding 53 cases due to miscarriage or termination (25 cases) and missing or inadequate information (28 cases), a total of 233 pregnancies that ended in live births were included in the analysis. The data were collected from medical records, focusing on maternal characteristics such as age, BMI, gravida, parity, abortions, history of previous Cesarean section, maternal comorbidities, mode of delivery, and the indication for Cesarean section. Pregnancy complications and gestational age at delivery were also recorded. Maternal morbidity was defined as the occurrence of any significant medical or pregnancy-related complications. For neonatal characteristics, the study included data on fetal presentation, birthweight, Apgar scores, neonatal admission status, cause of neonatal admission, and the length of neonatal hospital stay. Perinatal outcomes were assessed based on gestational age at birth, birthweight, Apgar scores, neonatal complications, and the need for NICU/ICN admission.
For statistical analysis, frequencies, and proportions (%) were reported for categorical variables, while medians (min-max) were used for continuous variables. Fisher’s exact test was used to compare maternal characteristics based on the number of fetuses due to the small sample size. Univariate (Fischer exact test) and multivariate analyses were performed to identify significant independent predictors of ART, with corresponding odds ratios and 95% confidence intervals. Gestational age was compared with infant characteristics using the Chi-square test. Also, the comparison of infantile characteristics and related factors was conducted using the McNemar test (categorical variables) and paired sample-test (continuous variables). Additionally, linear and multiple logistic regression analyses were conducted to assess factors influencing the length of hospital stay and premature birth in relation to maternal characteristics. A p-value of less than 0.05 was considered statistically significant. All data analyses were performed using SPSS version 21 (Armonk, New York, IBM Corporation).
All data collection followed strict confidentiality protocols to ensure patient privacy. The study was approved by the Institutional Review Board (IRB) of King Abdullah International Medical Research Center (KAIMRC) under approval number NRR24/028/4 and was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki. The requirement for informed consent was waived by the IRB due to the retrospective nature of the study, which involved anonymized data collected from existing medical records with no direct patient contact, in accordance with institutional policies and ethical guidelines.
Results
The study analyzed 233 birth records from January 2022 to December 2023, including 222 twin pregnancies (95.3%) and 11 triplet pregnancies (4.7%). Table 1 outlines the maternal characteristics, showing that 59.2% of the women were over 30 years old, with a similar proportion classified as obese (58.8%). Women with more than three pregnancies accounted for 37.3%, while those with more than one parity constituted 29.2%. Additionally, women who experienced more than one abortion represented 13.7%. The overall mean gestational age was 37.1 weeks (± 3.39), with twins having a mean of 37.3 weeks (± 3.32) and triplets having a mean of 33.5 weeks (± 2.88), with the difference being statistically significant (p < 0.001). Nearly all births (92.7%) occurred at late preterm gestation. A prior history of one C-section was reported by 15.9% of the women. The prevalence of assisted reproductive technology (ART) in the study population was 30.5%, and the most common mode of delivery was C-section (88.8%). Maternal morbidity was observed in 8.6% of cases. In addition, 78.5% of total pregnancies were dichorionic. A comparison of twins and triplets revealed that triplet pregnancies were significantly associated with early preterm births (p=0.029), the use of ART (p<0.001), and trichorionicity (p<0.001). However, no significant associations were identified between the number of fetuses and variables such as gender, BMI, gravida, parity, history of abortion, previous C-section, mode of delivery, or maternal morbidity (all p>0.05).
Figure 1 shows that the most common pregnancy complication was GDM (22.3%), followed by Preterm Premature Rupture of Membranes (PPROM) (10.3%) and preeclampsia (4.3%), while preterm birth as the major antenatal complication (70.4%), followed by Intrauterine Growth Restriction (IUGR) (9%) and Selective Intrauterine Growth Restriction (SIUGR) (4.7%).
Figure 2 illustrates that the most common maternal comorbidity was thyroid disease (12.9%), followed by asthma (5.2%) and cholecystectomy (3.9%). However, unremarkable medical history was seen in (59.7%).
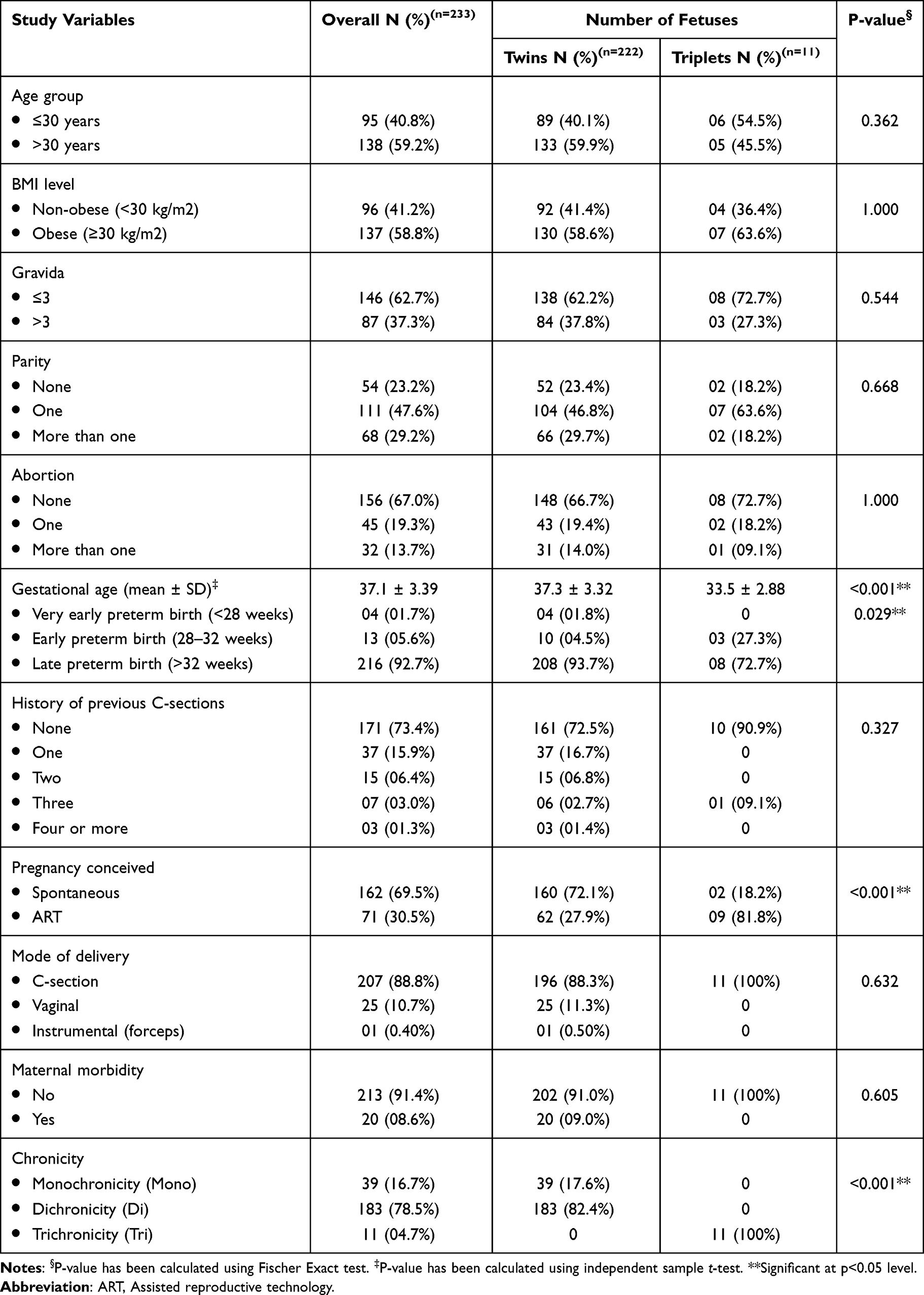 |
Table 1 Maternal Characteristics in Relation to the Number of Fetuses |
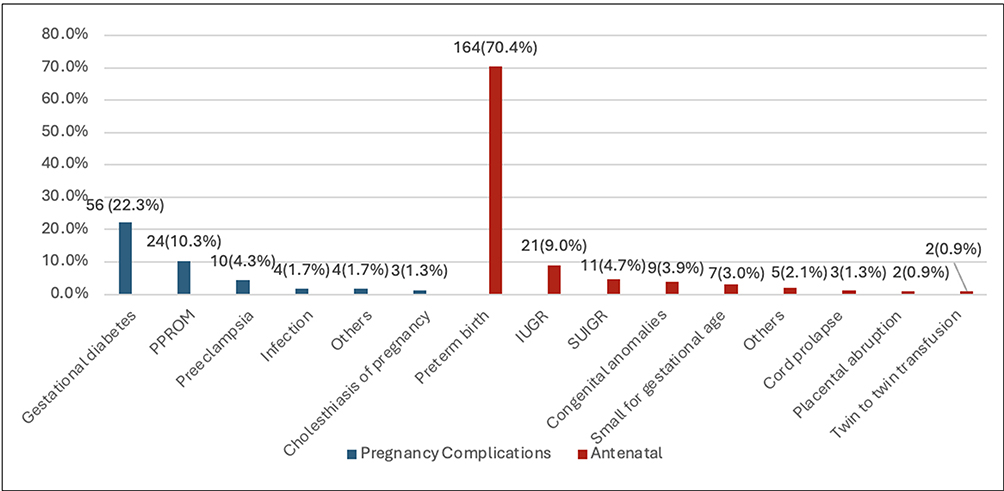 |
Figure 1 Pregnancy complications and antenatal complications. |
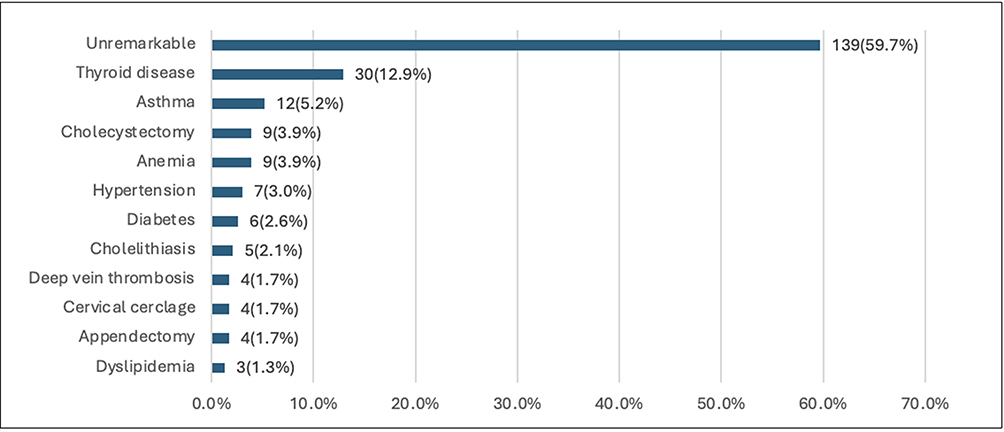 |
Figure 2 Maternal comorbidity. |
Table 2 shows that triplets were likelier to have a breech presentation (p=0.006), while twins were likelier to be admitted to NICU/ICN due to NRDS (p=0.038). There were no significant differences between the characteristics of twins and triplets in relation to admission or other causes of admission (all p>0.05).
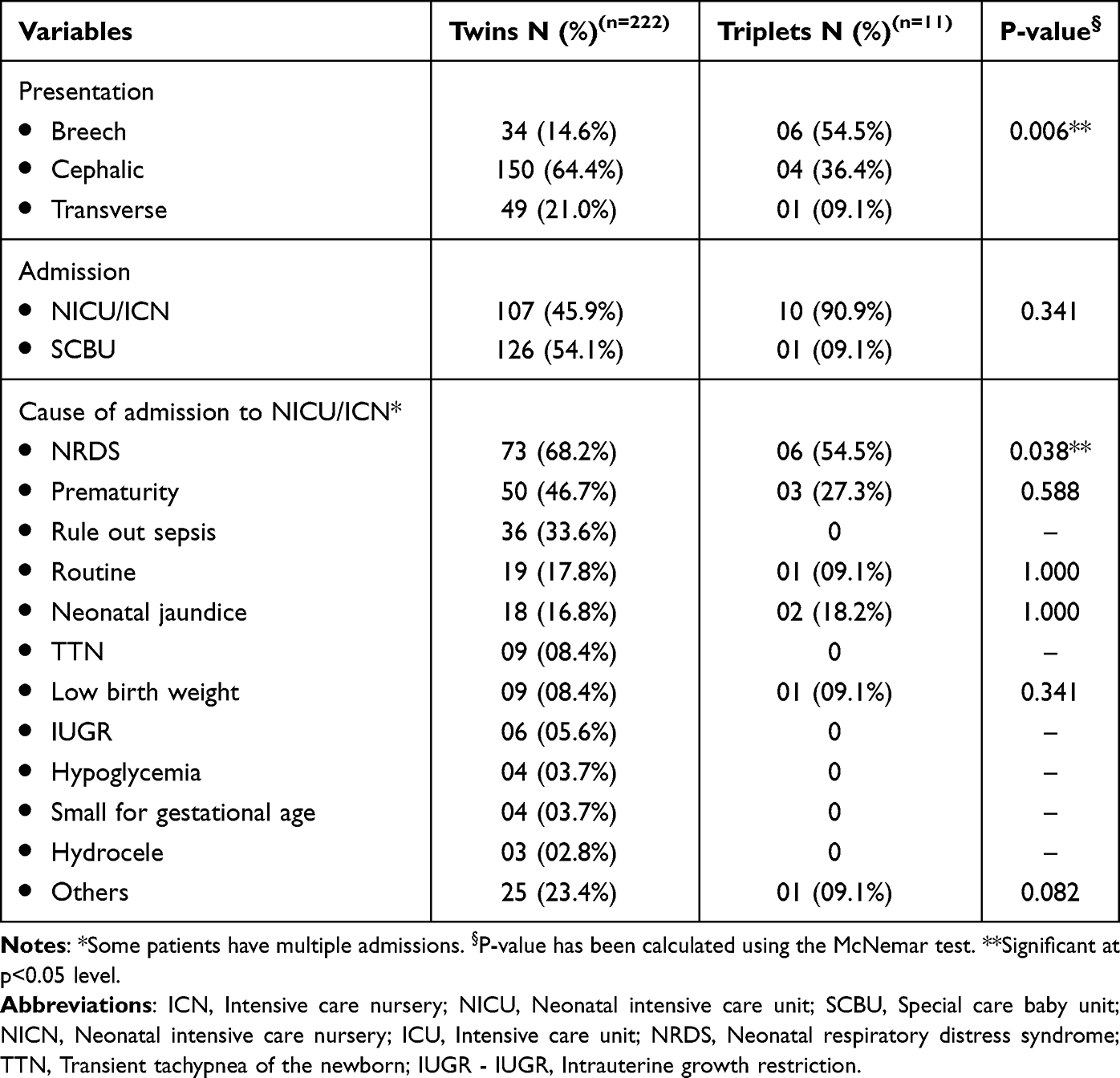 |
Table 2 Infantile Characteristics: Categorical Variables |
As presented in Table 3, there were no significant differences between twins and triplets in terms of birthweight, Apgar scores, or length of hospital stay (all p > 0.05).
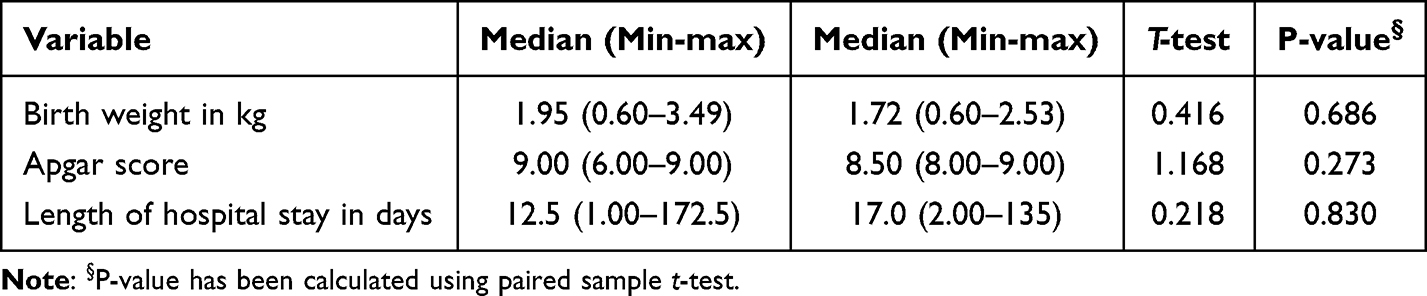 |
Table 3 Infantile Characteristics: Continuous Variables - Median (Min–Max) Measures |
Univariate analysis shows that parity (p=0.001), chorionicity (p<0.001), amnionicity (p=0.001), maternal morbidity (p=0.010), thyroid disease (p=0.001), and asthma (p=0.031) were identified as the influencing factors of pregnancy conceived, while age, BMI, gravida, abortion, gestational age, history of previous Cesarean section, mode of delivery, and antenatal complications were not relevant factors of a pregnancy conceived (p>0.05) (Table 4).
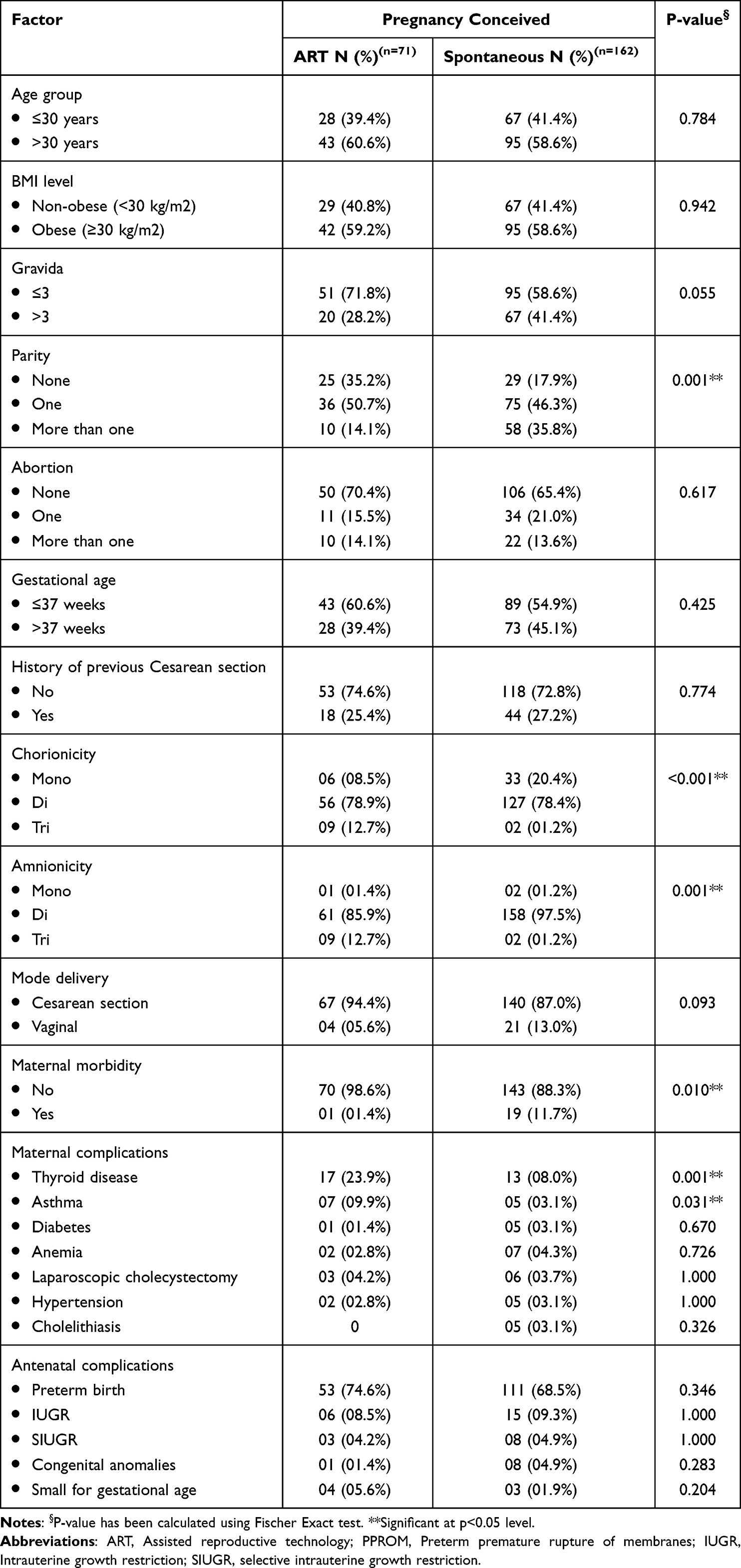 |
Table 4 Univariate Analysis to Determine the Influencing Factors of Pregnancy Conceived(n=233) |
A multivariate regression analysis was subsequently performed in Table 5 to determine the significant independent predictor of ART. Based on the results, it was found that compared to women who had no parity, women who had a single parity had a decreased chance of having ART by almost (93%) (AOR=0.065; 95% CI=0.017–0.244; p<0.001) and reduced chance of (84%) among women with multiple parities (AOR=0.155; 95% CI=0.050–0.475; p=0.001). Also, women with maternal morbidity had reduced rates of having ART by almost 91% compared to women without maternal morbidity (AOR=0.093; 95% CI=0.012–0.719; p=0.023). However, compared to women who had monochorionicity, women with dichorionicity were at least 26.5 times higher in women who conceived by ART (AOR=26.480; 95% CI=4.453–157.5; p<0.001) and 10.53 times higher among women who had trichorionicity (AOR=2.161–51.36; p=0.004). Further, compared to women who had monoamnionicity, women with triamnionicity had an increased chance of having ART by at least 12.1 times higher (AOR=12.136; 95% CI=2.500–58.92; p=0.002). In addition, mothers with thyroid diseases were higher in women who underwent ART (AOR=3.375; 95% CI=1.520–7.494; p=0.003).
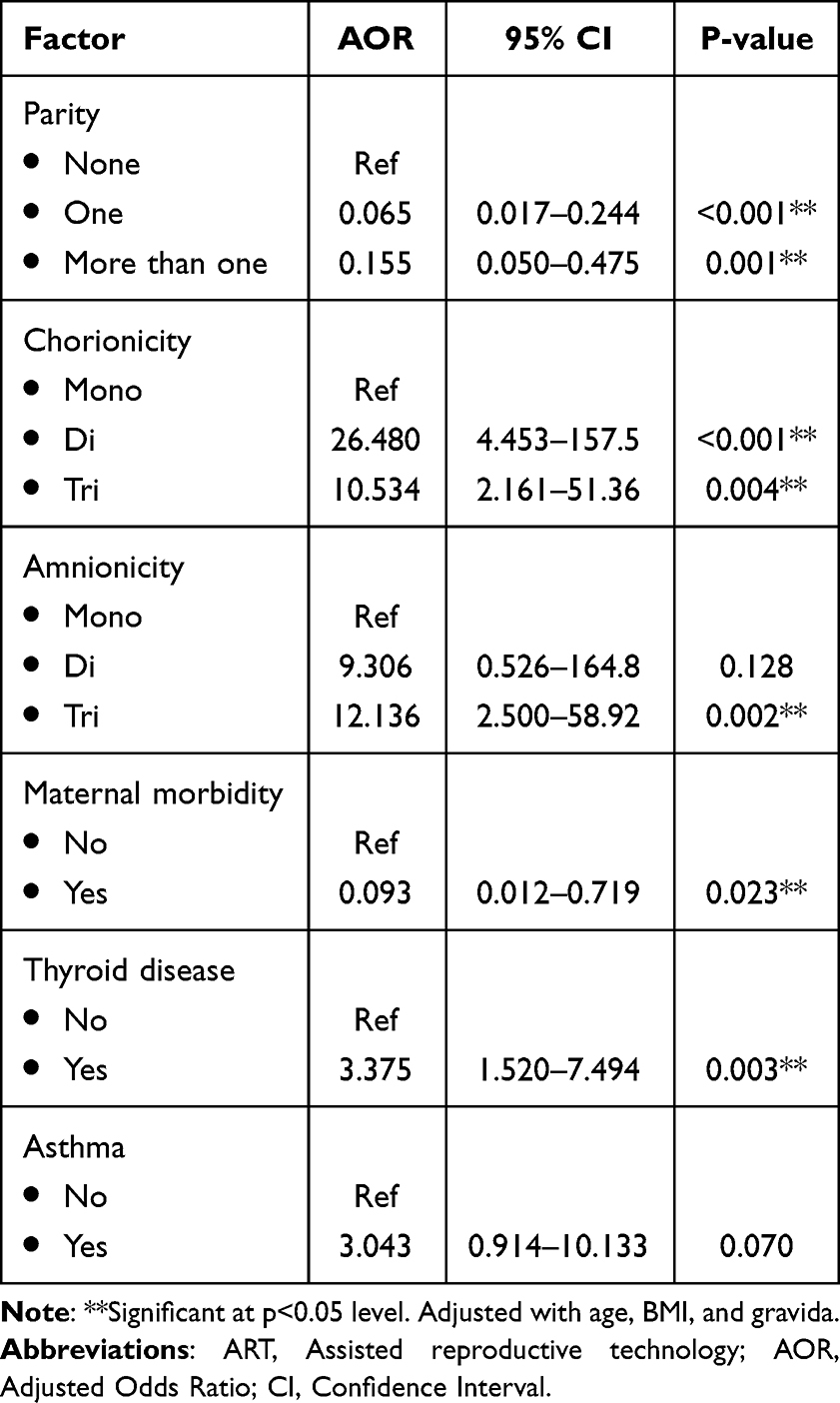 |
Table 5 Multivariate Regression Analysis to Determine the Significant Independent Predictor of ART(n=233) |
Discussion
This study examined maternal and neonatal outcomes in multiple pregnancies via ART and spontaneous conception. Triplets had lower gestational age, breech presentation, and were often conceived via ART. Consistent with AlBasri et al, who stated that twin births were associated with a longer gestational age, while triplet births were associated with a shorter duration.1 The mean gestational age in this study was longer for both twins (37.3 ± 3.32 weeks) and triplets (33.5 ± 2.88 weeks) compared to Albasri et al, who reported 36.0 ± 3.05 weeks for twins and 32 ± 3.81 weeks for triplets (p < 0.001). Similarly, the triplet mean was slightly higher than Lambers et al’s 32.3 weeks and Nasseri et al’s 30.92 ± 3.8 weeks, indicating better outcomes.1,6,16 A total of 78.5% of pregnancies were dichorionic, with triplet pregnancies associated with trichorionicity. Similarly, Sever et al also noted twins were mostly dichorionic diamniotic, and triplets trichorionic triamniotic, showing a comparable chorionicity distribution.9 Nearly all births (92.7%) occurred at late preterm gestation (>32 weeks), with no triplets born before 28 weeks. In contrast, Sever et al reported a higher proportion of twin pregnancies delivered before 25 weeks compared to triplet pregnancies, suggesting fewer extremely preterm births in this study.9
Our study revealed that NRDS and prematurity were the most common complications among infants, with NRDS showing significant variation between twins and triplets (p=0.038). This finding contrasts with Su et al, which reported SGA and LBW as the most common neonatal complications in multiple pregnancies.8 Similarly, Mitsiakos et al found no significant differences between triplets and singletons in primary outcomes, with no notable variation in the prevalence of severe neonatal morbidities.17 Maternal/neonatal characteristics (age, BMI, gravida, parity, abortion, Cesarean history, delivery mode, morbidity, NICU/ICN admission, birthweight, Apgar score, and hospital stay) did not differ between twins and triplets (p>0.05). This contrasts with Nasseri et al, who reported significantly higher rates of cesarean delivery and mean maternal age in triplets than in twins, as well as lower Apgar scores in triplets.16 Previous reports show that ART use and delayed pregnancy at advanced ages may be linked to multiple pregnancies.18 Age was not a factor for ART in our study. However, our regression model showed increasing chorionicity and amnionicity predicted ART, while increasing parity and maternal morbidity were predictive for spontaneous conceptions. This corroborates the reports of Arian et al, suggesting that the proportion of early adverse maternal outcomes and complications (both medical and obstetric) was significantly higher in the ART group, even after adjusting for multiple potential confounders.19 A systematic review and meta-analysis by Marleen et al documented that ART twins face a higher risk of preterm birth, pregnancy hypertension, GDM, and cesarean section compared to non-ART twins. ART twins also have increased neonatal risks, including congenital malformations, birthweight discordance, RDS, and NICU admission, with at least (25%) higher risk than non-ART twins.20 However, a study conducted in Saudi Arabia reported no significant differences in congenital malformations between twins conceived through ART and those conceived naturally.21
Complications are common in multiple pregnancy. In our study, GDM and PPROM were the most reported pregnancy complications, while preterm birth was the most prominent antenatal complication. Prematurity was the leading cause of NICU/ICN admission. Other neonatal complications were NRDS, suspected sepsis, and neonatal jaundice. Supporting this, a study in Western Saudi Arabia found preterm birth, GDM, and PROM were the most common pregnancy complications, while hyaline membrane disease, neonatal jaundice, and sepsis were the leading infant complications.1 A systematic review in Italy found that assisted conception of monochorionic twins did not increase the risk of hypertensive disorders, preterm delivery, or twin-twin transfusion syndrome; however, it was associated with a higher risk of cesarean section and neonatal death.22
Conclusion
Women with triplets, who conceived via ART, had heightened risk of lower gestational age and malpresentation. Triplet pregnancies were associated with earlier preterm births, a higher prevalence or ART use, and trichorionicity. The overall mean gestational age was notably lower in triplets compared to twins. Additionally, most pregnancies resulted in late preterm births, with C-section being the most common mode of delivery. The most prominent pregnancy complication was GDM, while preterm birth was the most frequent antenatal complication. In addition, despite the normal Apgar score ranges, NRDS and prematurity were the main reasons behind NICU/ICN admission. These same reasons were also the main factors influencing longer hospital stays. Education about the risks of twin pregnancies in women seeking ART is essential, as pregnancy complications are frequent. Therefore, strict monitoring during pregnancy is pivotal in the management of women with multiple gestation. Limitations of this study are attributed to the small sample size and the nature of the study design; however, it is one of the first studies in Saudi to report on outcomes of twin and triplet pregnancies. This establishes the need for more studies with larger sample sizes and more robust methodology.
Abbreviations
ART, Assisted Reproductive Technology; GDM, Gestational Diabetes Mellitus; NRDS, Neonatal Respiratory Distress Syndrome; NICU/ICN, Neonatal Intensive Care Unit/Intermediate Care Nursery.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that there are no conflicts of interest to this study.
References
1. AlBasri SF, Shouib GM, Bajouh OS, Nasrat HA, Ahmad E, AlGreisi FM. AlGreisi FM: maternal and neonatal outcomes in twin and triplet gestations in Western. Saudi Arabia Saudi Med J. 2017;38:657–661. doi:10.15537/smj.2017.6.17699
2. Monden C, Pison G, Smits J. Twin peaks: more twinning in humans than ever before. Hum Reprod. 2021;36(6):1666–1673. doi:10.1093/humrep/deab029
3. Horon I, Martin JA. Changes in twin births in the United States,2019-2021. Natl Vital Stat Rep. 2022;71(9):1–11. PMID: 36595468.
4. Bernal Claverol M, Ruiz Minaya M, Aracil Moreno I, et al. Maternal, perinatal and neonatal outcomes of triplet pregnancies according to chorionicity: a systematic review of the literature and meta-analysis. J Clin Med. 2022;11(7):1871. PMID: 35407479; PMCID: PMC8999732. doi:10.3390/jcm11071871
5. Kulkarni AD, Jamieson DJ, Jones HW Jr, Kissin DM, Gallo MF, Macaluso M. Adashi EY: fertility treatments and multiple births in the United States. N Engl J Med. 2013;369:2218–2225. doi:10.1056/NEJMoa1301467
6. Lambers DS, Allen J, Gottula J, Devaiah CG, Habli M. Habli M: the maternal impact, health burden, and postpartum sequela in triplet pregnancies: a retrospective cohort. Am J Perinatol. 2020;38(S 01):e256–e261. doi:10.1055/s-0040-1709489
7. Santana Danielly S, Cecatti José G, Surita Fernanda G. Twin pregnancy and severe maternal outcomes: the world health organization multicountry survey on maternal and newborn health. Obstetrics Gynecol. 2016;127(4):631–641. doi:10.1097/AOG.0000000000001338
8. Su RN, Zhu WW, Wei YM, Wang C, Feng H, Lin L. Yang HX: maternal and neonatal outcomes in multiple pregnancy: a multicentre study in the Beijing population. Chin Med J. 2015;128:197–202. doi:10.4103/0366-6999.149206
9. Sever B. Ekin A: outcomes of multiple pregnancies: results of a perinatology clinic in a tertiary health center. J Health Sci Med. 2023;6:561–565. doi:10.32322/jhsm.1262414
10. Ekström MM, Tiblad E, Norman M, Stephansson O, Granfors M. Granfors M: maternal, pregnancy and neonatal outcomes in triplet pregnancies in Sweden - a nationwide cohort study. Ups J Med Sci. 2023;128:1–8. doi:10.48101/ujms.v128.9473
11. Algwiser A, Al Sultan S, Mesleh RA. Ayoub H: twin pregnancies: incidence and outcome—Riyadh Armed Forces Hospital experience. J Obstet Gynaecol. 1999;19:587–593. doi:10.1080/01443619963789
12. Duffy CR. Duffy CR: multifetal gestations and associated perinatal risks. NeoReviews. 2021;22:734–746. doi:10.1542/neo.22-11-e734
13. Schubert J, Timmesfeld N, Noever K, Arabin B. Challenges for better care based on the course of maternal body mass index, weight gain and multiple outcome in twin pregnancies: a population-based retrospective cohort study in Hessen/Germany within 15 years. Arch Gynecol Obstet. 2020;301:161–170. doi:10.1007/s00404-020-05440-6
14. Al-Suleiman SA, Al-Jama FE, Rahman J, Rahman MS. Rahman MS: obstetric complications and perinatal outcome in triplet pregnancies. J Obstet Gynaecol. 2006;26:200–204. doi:10.1080/01443610500508295
15. Al-Sunaidi M. Al-Shahrani MS: fetomaternal and neonatal outcome of triplet pregnancy. Promising Results Saudi Med J. 2011;32:685–688.
16. Nasseri F, Azhir A. Azhir A: the neonatal outcome in twin versus triplet and quadruplet pregnancies. J Res Med Sci. 2009;14:7–12.
17. Mitsiakos G, Gialamprinou D, Chatziioannidis I, et al. Are neonatal outcomes of triplet pregnancies different from those of singletons according to gestational age? J Perinat Med. 2021;49(1145–1153):1145–1153. doi:10.1515/jpm-2020-0558
18. Adashi EY. Adashi EY: seeing double: a nation of twins from sea to shining sea. Am J Obstet Gynecol. 2016;214:311–313. doi:10.1016/j.ajog.2016.01.185
19. Arian SE, Erfani H, Yadav GS, Clark S, Gibbons WE, Shamshirsaz AA. Shamshirsaz AA: neonatal and maternal outcomes among twin pregnancies stratified by mode of conception in the United States. Fertil Steril. 2021;116:514–521. doi:10.1016/j.fertnstert.2021.03.032
20. Marleen S, Kodithuwakku W, Nandasena R, et al. Maternal and perinatal outcomes in twin pregnancies following assisted reproduction: a systematic review and meta-analysis involving 802,462 pregnancies. Hum Reprod Update. 2024;30:309–322. doi:10.1093/humupd/dmae002
21. Al-Fifi S, Al-Binali A, Al-Shahrani M, Shafiq H, Bahar M, Almushait M. Eskandar M: congenital anomalies and other perinatal outcomes in ICSI vs. naturally conceived pregnancies: a comparative study. J Assist Reprod Genet. 2009;26:377–381. doi:10.1007/s10815-009-9329-3
22. Wang M, Chai J. Comparison of outcomes of monochorionic twin pregnancies conceived by assisted reproductive technology vs. spontaneous conceptions: a systematic review and meta-analysis. Front Pediatr. 2022;10:962190. doi:10.3389/fped.2022.962190
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.