Back to Journals » Clinical Ophthalmology » Volume 19
Comparative Validation of MOPTIM MRT-200 Refraction Device with 2WIN and Retinomax
Authors Schumacher H, Garaygay G, Ayagalria A, Lauano BI, Marshall DM, Townley JR, Arnold RW ![]()
Received 19 June 2025
Accepted for publication 22 August 2025
Published 2 September 2025 Volume 2025:19 Pages 3153—3166
DOI https://doi.org/10.2147/OPTH.S545397
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Video abstract of “MOPTIM MRT-200 refraction device with 2WIN and retinomax” [545397]
Views: 134
Heidi Schumacher,1,2 Giancarlo Garaygay,1 Aana Ayagalria,1 Bryant Ikaika Lauano,1 Denise M Marshall,1,3 J Richard Townley,1,3 Robert W Arnold1
1Alaska Blind Child Discovery, Alaska Children’s EYE & Strabismus, Anchorage, Alaska, 99508, USA; 2Service High School, Anchorage, Alaska, USA; 3Anterior Segment Department, Eagle Eye Surgeons, Anchorage, Alaska, USA
Correspondence: Robert W Arnold, Alaska Blind Child Discovery, Alaska Children’s EYE & Strabismus, 3500 Latouche Street #280, Anchorage, Alaska, 99508, USA, Tel +19075611917, Email [email protected]
Background: Portable sphero-cylinder refraction is useful for remote medical missions and self-checking. A novel, inexpensive, handheld optical scope with an internal vision chart and adjustable diopter lens, called the Moptim MRT-200, was therefore validated.
Methods: Young, capable patients from a pediatric eye practice had dry refraction estimates with the Moptim MRT-200, Adaptica 2WIN photoscreener, and Monocular Retinomax compared with actual refined retinoscopy. Vector-converted sphero-cylinder refractions and the univariate ABCD Ellipsoid were used for comparison as well as monocular visual acuity.
Results: 206 racially diverse, high-risk refractive patients with median “Ellipsoid-Gap” of 3.5 had high correlation spherical equivalent and similar ABCD Ellipsoid comparing Moptim MRT-200, 2WIN and Retinomax (Kruskal Wallis X2(5) = 4.2, p = 0.52) however the 61 patients with blur associated with Ellipsoid gap over 5.0 had better refractive accuracy with 2WIN and Retinomax than Moptim MRT-200 (p < 0.001). Visual acuity with Moptim MRT-200 had a weak correlation (ICC.41 AND.47) and a Bland-Altman mean difference of approximately 1 logMAR line less fine than the actual phoropter refraction.
Conclusion: Precise sphero-cylinder estimation with the Moptim MRT-200 was too complex for lay screeners and many young patients, especially compared to 2WIN and Retinomax; however, rapid estimation of spherical refraction was feasible and valid.
Keywords: portable refraction, visual acuity, self-diagnosis, refractive comparison
Introduction
There are times when portable, non-expert refraction can be helpful. This can be checking your own eyes (self-refraction1) or testing on other subjects such as during remote medical missions.2 There are several types of portable autorefractors capable of estimating sphero-cylinder refraction. Some of them have been validated and compared3,4 (Table 1). Portable refraction can include viewing distant or near objects through labeled powered convex or concave trial lenses, particularly through certain portable skiascopy racks. Other methods include battery-powered, Safir method autorefractors that are lighter and hand-held unlike a large assortment of table-top autorefractors that utilize Hartmann-Shack Wavefront Aberrometry. Some hand-held also employ Hartmann-Shack technology. For the purposes of this study, devices that attach to a stand, such as typical mechanical or digital phoropters, or table-top electronic autorefractors, are not considered “portable”.
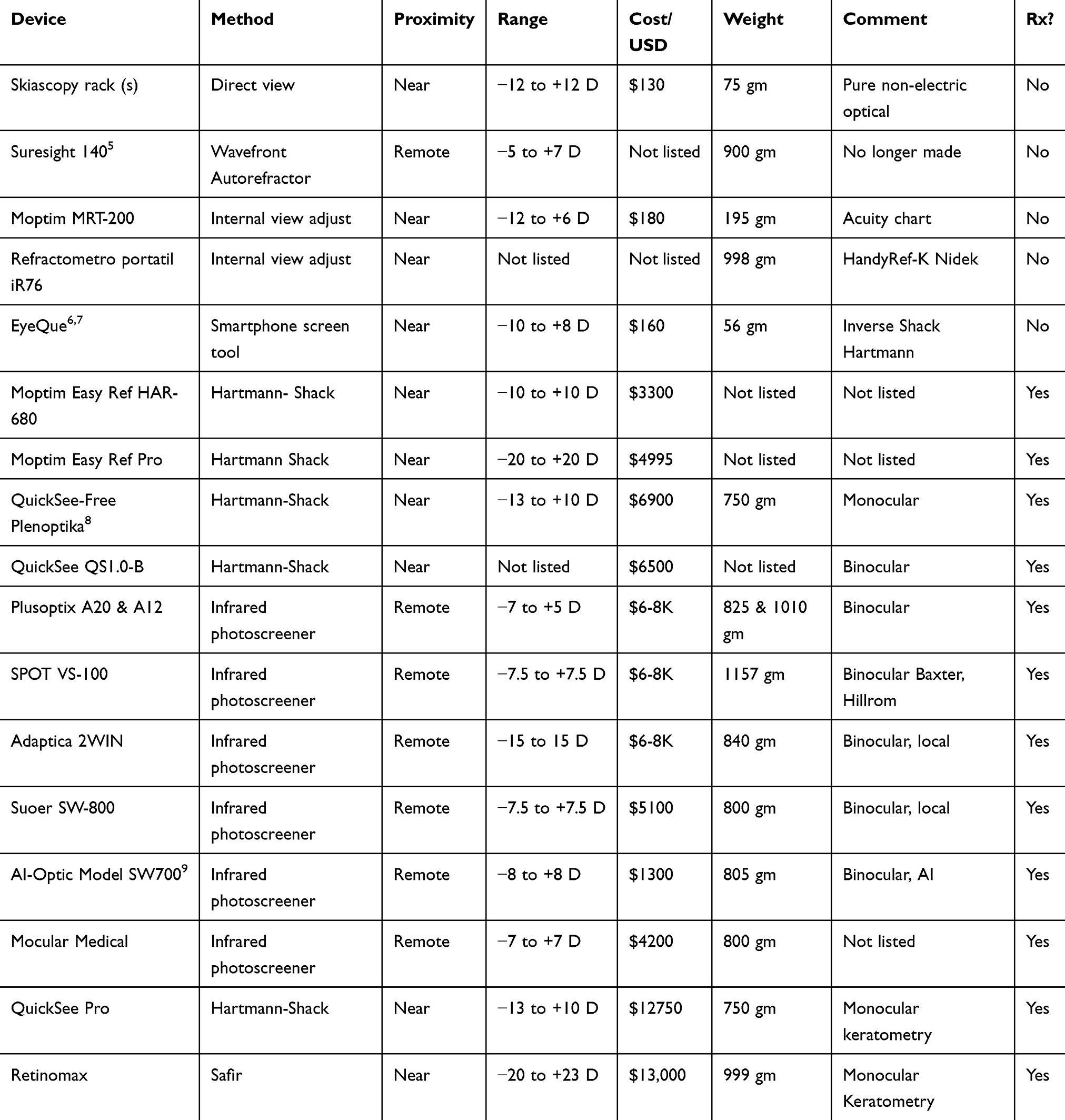 |
Table 1 Hand-Held, Portable Sphero-Cylinder Refraction Devices (2025). Range is Instrument’s capacity from Myopic to Hyperopic, Rx? Is Whether Output in Sphere, Cylinder and Axis; Yes or No |
These refracting devices are not to be confused with other hand-held Brix refractometers which are intended to determine the sugar content of fluids, lensometers that determine the refractive power of spectacles or contact lenses, or devices to determine inter-pupillary distance.
After a refraction is estimated, the level of corrected visual acuity is often of interest. Most table-top and hand-held automated autorefractors do not give a corrected visual acuity chart. On the other hand, chart visual can be estimated through a skiacopy rack for near or far.
The accepted method for comparison of two spectacle refractions is to vector convert the sphero-cylinder (plus- or minus cylinder notation) to J0, J45 and M (spherical equivalent) vector transformations10 each of which can be directly and linearly compared with regression and Bland Altman. On the other hand, two spectacles with exact match J0 might have widely disparate J45 or M and then result in much blur as a poor match. We previously developed the ABCD Ellipsoid method for univariate, blur-dependent comparison of two spectacle refractions.11,12 A highly matching spectacle such that the candidate spectacle only results in a one logMAR line blur (from 20/20 to 20/25) compared to the target yielding an “A” match or an ellipsoid value of 1.0 or less. A candidate spectacle blurring 3 logMAR lines compared to target would have an ellipsoid “B” match or value of 2.0. On the other hand, a different candidate spectacle blurring by 6 logMAR lines (from 20/20 to 20/80) would yield an ellipsoid “C” match with an ellipsoid value of 3.0.
We obtained the novel, small, portable autoscreening device Moptim MRT-200 (Version 1.0, Shenzhen Certainn Technology Co., Ltd., Shenzhen, China) and subjected it to refractive validation compared to the Adaptica 2WIN (version 5.5.0, Adaptica, Padua, Italy) infrared photoscreener and the Retinomax (Righton, Japan) monocular autorefractor (Figure 1) in a group of young patients from a subspecialty pediatric ophthalmology practice.
 |
Figure 1 The Retinomax, the Moptim MRT-200, and the Adaptica 2WIN are compared. |
Methods
Patients in this study had three dry refractions compared to their actual optimal refraction to determine relative refractive performance as well as a visual acuity comparison. The actual refraction utilized effective, non-pharmacologic techniques13,14 to relax accommodation without dilating the pupils and thus avoiding the recognized mydriatic degradation in best-corrected visual acuity.
This evaluation of screening tests has institutional review for the Alaska Blind Child Discovery by WCG (Study number 1365766) and is consistent with the Declaration of Helsinki and the Health Insurance Portability and Accountability Act (HIPAA). Parents and participants gave age-appropriate consent.
Ellipsoid Gap
The “Ellipsoid Gap” for a group of patients is defined as a univariate, sphero-cylinder comparison of their actual refraction to “optimal” plano-sphere “refraction” for right and left eyes utilizing the ABCD Ellipsoid method. Perfect optical match has a gap of zero, while high myopic astigmatism for all patients or high hyperopic astigmatism for older, minimally accommodating patients could have an Ellipsoid Gap of 10 units or greater. The Ellipsoid Gap is a unique, univariate method to define and quantify blur as a result of low- or high- sphero-cylinder refraction.
Patient Selection
From November 2024 through February 2025, non-routine eye patients in a sub-specialty pediatric ophthalmology/adult strabismus practice who were able to participate with phoropter refined retinoscopy as opposed to younger patients ideally refracted with SBARS skiascopy.14 These cooperative patients were invited to add Moptim MRT-200 self-adjusted refraction estimate to the other helpful refractive estimates, Adaptica 2WIN and Retinomax which were presented in random order. Patients could have strabismus, nystagmus, some degree of developmental delay as long as they could participate with gazing and communicating self-adjusted or assisted dialing of the Moptim MRT-200 device. For some patients, dial was assisted by the technician slowly turning the dial while the patient viewed the screen and said “stop” when the clearest image was first noted. Patients with or without strabismus had binocularity measured with the PDI Check autostereoscopic device. Some patients demonstrated sufficient understanding of spherical self-adjust that they took extra time attempting to also estimate cylinder magnitude and even axis with the Moptim MRT-200. Some patients had difficulty with fixation, alignment and pupil configuration thus failing to yield a binocular 2WIN refraction estimate. For some of them, the dominant single eye and then contralaterally patched non-preferred eye were measured using the monocular 2WIN function.
Two subsets of patients were selected for secondary comparison. For visual acuity, the group of patients with Ellipsoid Gap less than 2 had visual acuity compared. For sphero-cylinder refraction, a particularly blurred group with sufficiently high sphero-cylinder refractions that their Ellipsoid gap was greater than 5 had their refractions compared.
Actual Refraction and Refraction Estimates
These refractive estimating techniques are compared without cycloplegic drops to allow physiologic pupils. They are compared to actual refraction determined with accommodation relaxed with deliberate fogging and then refined in the phoropter to optimize visual acuity. Our fogging, accommodative relaxing techniques are known to relax more than 92% of hyperopia uncovered by cyclopentolate 1% drops.13
The Adaptica 2WIN (version 5.5.0) was used by manufacturer guidelines as adapted by ABCD during previous validation efforts. Most patients viewed the twinkling fixation lights with the audio attractant, but these were switched off if pupils were too small or if children with autism were upset by the noise. Plus-cylinder refractive estimate was recorded. If sufficient strabismus was present to not yield a binocular result, then monocular readings were attempted even with a No-Peeking eye patch over the sound eye. The 2WIN also reports pupil size and interpupillary distance.
The Retinomax was performed right eye, then left eye using the flower fixation target. Multiple readings were averaged, and a plus cylinder sphero-cylinder estimate plus keratometry for each eye was attempted and recorded.
The hand-held monocular self-sphere adjustable device (Moptim MRT-200) was used according to accompanying printed, translated directions and three YouTube videos. The instructions demonstrated how to estimate spherical refractive error or determine if a cylinder of greater to 1 diopter was present, but not specifically how to determine cylinder refractive error. The device is a hand-held scope with dimensions 4.7 × 5.5 × 18.5 cm weighing 195 grams powered by three disposable AAA batteries. A larger figure of the internal, illuminated tumbling E vision chart was generated and laminated highlighting the radial clock-hours for potential cylinder determination. The accompanying smart phone data storage application was not utilized.
From limited English-language details of method, we developed specific techniques for which the following details are added in addition to the Video Abstract (https://youtu.be/auQ-On82VpA). The Moptim MRT-200 device consists of a single on-off button, a small external illuminated LCD screen with refractive error in 0.25 diopter steps starting with +6.00 and going all the way to −12 by turning a dial on the opposite end as the eyepiece with multipurpose attached covering cap. Inside the device is a high-resolution eye chart with optotype tumbling E representing visual acuity ranging from logMAR 0.5 (20/63) to −0.4 (20/8). To the left side of the 10-line charts is 20/20 notation while the notation to the right side is logMAR. To the left to the Tumbling E charts are two images of houses which come into focus while reducing plus sphere by rotating the dial, with the upper image of a house coming into focus before the lower image of a house. All around the houses and Tumbling E charts are clock dials to assist in being aware of astigmatism axis. Patients were oriented by viewing our external, large laminated clear view of the internal Moptim MRT-200 chart.
The device was turned on and after several seconds the LCD screen shows some Mandarin language. Then the dial is turned fully counter-clockwise until +6.00 appears. The patient views through the viewing screen of the Moptim MRT-200 covering the non-tested eye with the loose covering eyepiece cap. The rotary diopter dial is slowly turned clockwise either by the patient, or “assisted” by the tester if manual coordination was not sufficient. The patient was instructed to look for the two houses and to either tell, or stop turning the dial, when the top house just begins to be clearly viewed. The dial was then turned counterclockwise and then gradually clockwise until the top house just appeared clearest. The screen diopter measure was recorded for that eye and the patient asked which line of Tumbling E optotypes the smallest “E” shapes were readable. Then the same technique was repeated for the left eye.
If the patient was particularly aware and capable of the methods, we attempted to determine sphero-cylinder refraction with the Moptim MRT-200. The patient was shown the printed, enlarged image of the internal eye chart and oriented to the concept of the clock dial. Then the right eye was tested with the left cap-covered and the dial turned manually until the top house became clear. Then the dial was counterclockwise, then slowly clockwise from +6.00 toward minus clockwise until the first clock hour designation was determined clearest or boldest. The chart dial clock hour was recorded with the corresponding diopter reading from the dial-adjusted LCD screen. Then the patient viewed again, turning the dial further clockwise until the orthogonal clock-hour was the most bold/clear. The second clear dial clock hour, and its corresponding diopter clock hour was recorded. The smallest Tumbling E visible was also recorded for that eye and then attention was repeated for the left eye starting back at the +6.00 diopter from the fully counterclockwise dial. Demonstration of the three different refractive devices and the actual refraction are shown on the video abstract for this article (VIDEO: https://youtu.be/auQ-On82VpA).
Estimation of astigmatism spectacle took a calculation of what number of cylinder refraction degrees each eye had in the plus configuration with the clock hour first noted bold/clear and converted to degrees by the following formula:
Degrees for Spectacles = Function of Patient-Reported Clock Hours (Decimal)
Degrees = (180/π)*acos(cos((π/6)*(hours-9))) (if trigonometric function uses radians).
One patient with moderately high astigmatism performed test re-Test sphero-cylinder refractive estimates with Moptim MRT-200. These were then compared to the actual, refined refraction in the right and left eyes.
Refractive comparison is done on all completed patients and again on those with sufficiently high refractive error to score a blurry Ellipsoid Gap of each eye greater than 5.0 chosen since these individuals generally would qualify for disability due to vision impairment.
Patients were tested for their best, dry phoropter corrected monocular visual acuity on a calibrated M&S visual acuity system using HOTV optotypes. This was then compared to their Moptim MRT-200 tumbling E visual acuity reporting the smallest line they could resolve the shapes of the tumbling E. Visual acuity was also compared in a subset of the patients with minimal refractive error determined by the Ellipsoid Gap less than 2.0.
Sample Size Estimation
Given a mean ABCD-Ellipsoid of 2.0 and a standard deviation of 1.5, with alpha of 0.05 and power of 0.8, the ability to detect a difference of 0.5 would take a sample size of at least 142 patients (two-tailed).
Data Analysis
Patient characteristics are reported as proportions and typical appropriate descriptive statistics with attention directed to whether data distributions are normal by Shapiro–Wilk and/or the Kolmogorov–Smirnov test. Data are then compared with t-Test and/or Wilcoxon Ranked Sum test.
Results
Attempts at the three dry refraction estimates compared to phoropter, fogged, then refined actual refraction were completed by 219 patients of whom 209 were less than 19 years old and 55 had strabismus and/or nystagmus. The mean ± S.D. age was 11.2 ± 7.1 years and 120 were female. The racial/ethnic mix was Asian 16, Black 27, Hispanic 24, Middle East 1, Alaska Native 22, Pacific Islander 28 and White 101. Developmental delay (autism, attention deficit hyperactivity disorder, Down Syndrome, prematurity, cerebral palsy) was present in 58.
There was a difference in ability for devices to yield a refractive estimate based on severity of refractive error, pupil configuration, ocular alignment and/or patient cooperation. 2WIN did not yield a refraction estimate in one eye of 4 and both eyes in 8 while only 1 young patient could not provide any estimate with Moptim MRT-200 and a Retinomax gave a reading in all patients. All three devices could be compared in 206 patients.
For patients who had a refractive estimate from each device compared to actual refraction, vector components J0, J45 and spherical equivalent M have Intra Class correlations (ICC) and Bland Altman (BA) analysis statistics shown in Table 2 and Bland Altman graphs shown in Figure 2.
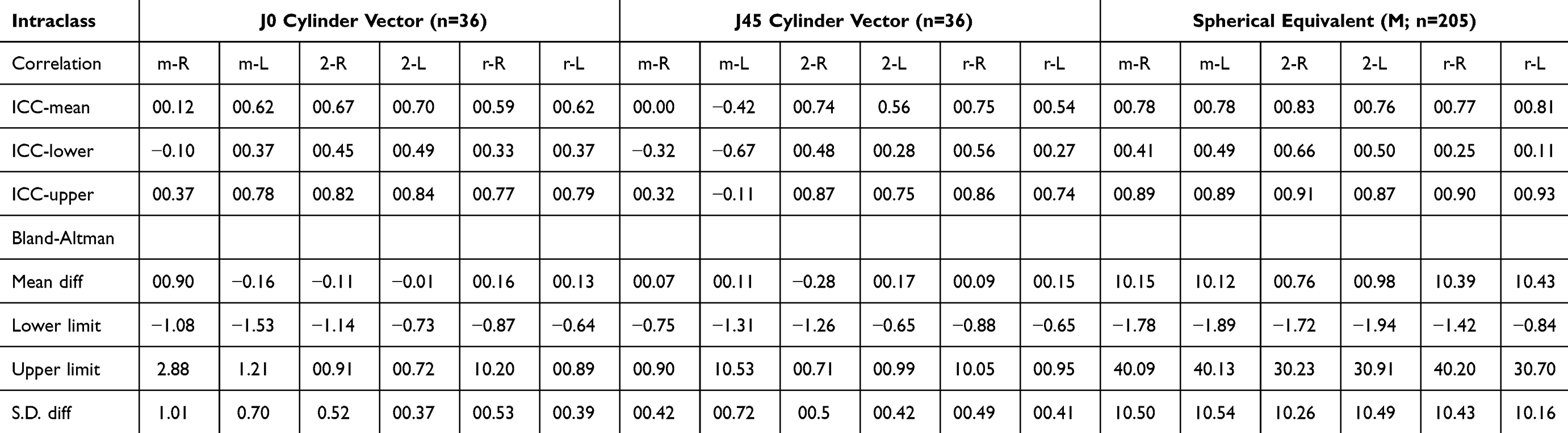 |
Table 2 Bland-Altman and Correlation Statistics for Comparison of Sphero-Cylinder Vector Transformations J0, J45 and M for the Three Devices Moptim MRT-200 (M), the Adaptica 2WIN (2) and the Retinomax (R) for Right (R) and Left (L) Eyes in 206 Patients. ICC Is Intraclass Correlation with Mean, Lower Limit and Upper Limit Listed. Bland Altman Mean Difference, with Lower and Upper Limits and Also the Standard Deviation of the Difference |
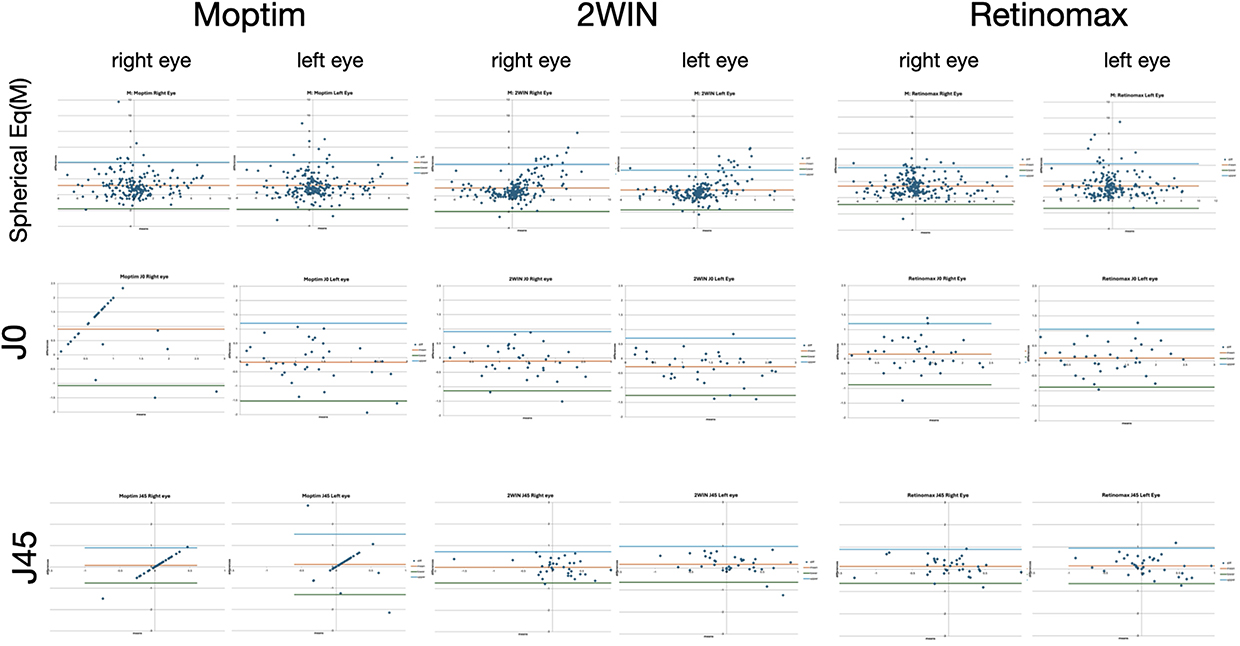 |
Figure 2 Bland Altman plots comparing vector transformed sphero-cylinder dry refractions by three hand-held devices (Moptim) MRT-200, Adaptica 2WIN and Righton Retinomax to actual, refined phoropter refraction on 206 capable, young patients. |
The ABCD Ellipsoid was used as a univariate method to compare refractions, the descriptive statistics of which are shown in Table 2. The “Ellipsoid-Gap” compared actual dry refraction candidate refractions to a plano sphere target for all patients as a means of comparing the refractive error severity of this cohort of subspecialty pediatric ophthalmology cooperative youth and young adult strabismic patients.
For right/left eyes, the “Ellipsoid Gap” for our 206 patients with data from all three devices, medians were 3.60/3.38, interquartile ranges IQR1: 1.58/1.51, IQR3: 8.00/7.61, means 5.10±4.3/5.13±4.5 and maximums 17.1/17.6. There were 61 particularly blurred patients with Ellipsoid Gap greater than 5.0 while 41 other patients had their Ellipsoid gap or less than 2.0. The right eye was tested first. The ellipsoid gap for Moptim MRT-200 did not correlate with age for right eye (r(217) = 0.08, p = 0.22) but reached significant correlation for the left eyes (r(217) – 0.17, p = 0.01). The Ellipsoid Gap can be viewed on the right sides of Figures 3 and 4.
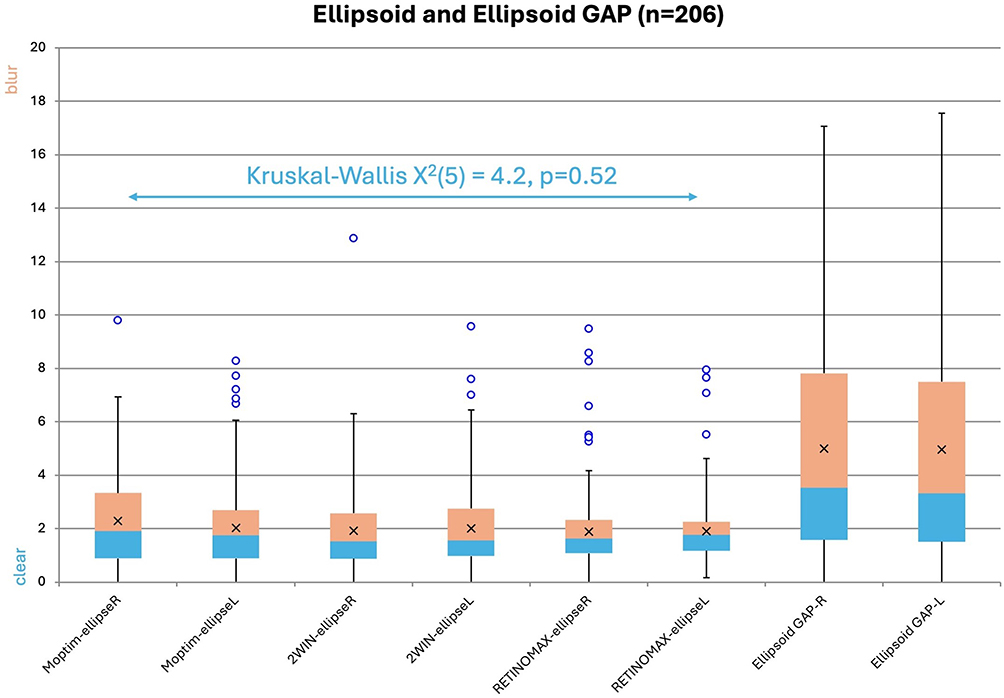 |
Figure 3 The ABCD Ellipsoid for right and left eyes for (Moptim) MRT-200, Adaptica 2WIN and Righton Retinomax compared to actual refraction for 206 capable young patients. At the far right is the Ellipsoid Gap showing the degree of uncorrected refractive blur for this cohort. In the box plots, x marks the mean. |
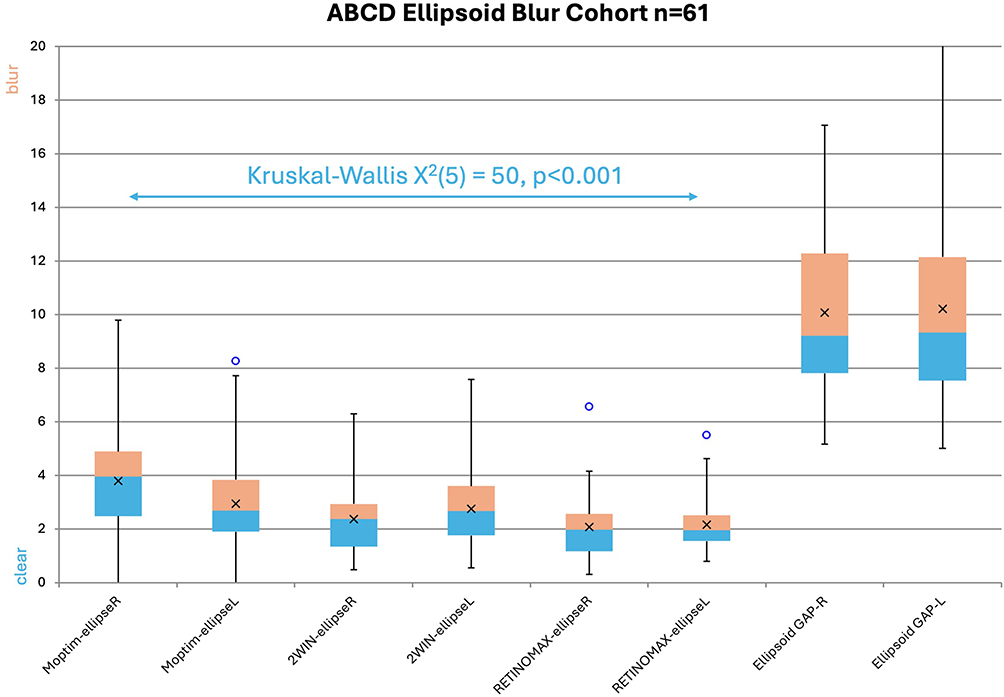 |
Figure 4 The ABCD Ellipsoid for right (R) and left (L) eyes for (Moptim) MRT-200, Adaptica 2WIN and Righton Retinomax compared to actual refraction for 61 capable, high refractive error young patients. At the far right is the Ellipsoid Gap showing the high degree (>5.0) of uncorrected refractive blur for this special cohort. In the box plots, x marks the mean. |
The ABCD Ellipsoid was also used to compare each of the three refractive devices with actual refraction (Table 3). For all 206 patients, the median ABCD Ellipsoid comparing device to actual refraction did not differ (Kruskal–Wallis X2(5) = 4.2, p = 0.52). Patients with more profound refractive error but able to get a reading on 2WIN, Retinomax and Moptim MRT-200 (n = 61) had much larger Ellipsoid Gap with an ABCD ellipsoid range from 5 to 21; these high refractive error patients are then separately compared (Figure 4). For these particularly sphero-cylinder blurred patients, the 2WIN and Retinomax outperformed the Moptim MRT-200 (Kruskal–Wallis X2(5) = 50, p < 0.001).
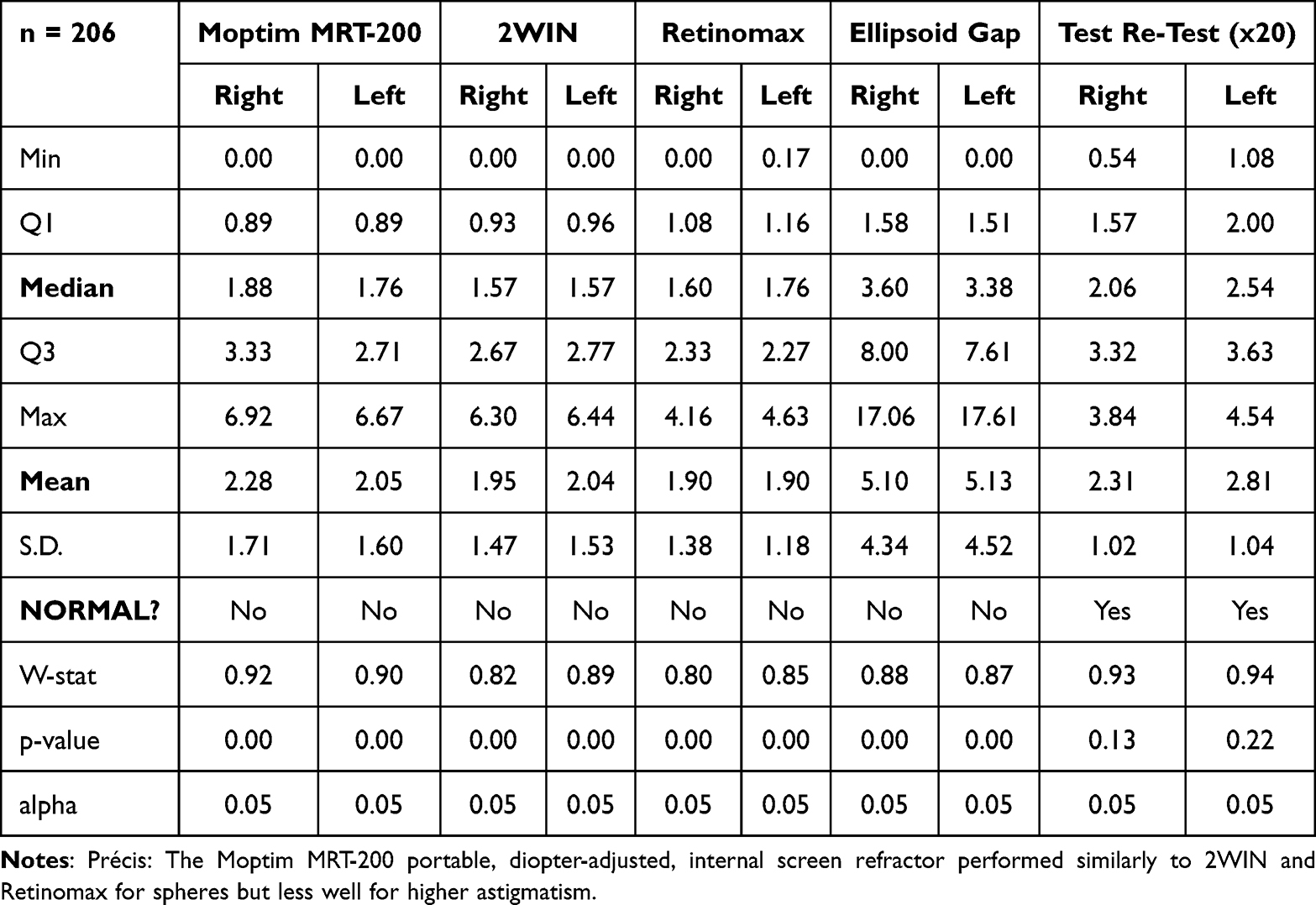 |
Table 3 ABCD Ellipsoid Metrics Compared. The ABCD Ellipsoid Is a Univariate Combination of the Three Vector Transformations J0, J45 and M Separated on the Basis of Induced Blur. The Ellipsoid Gap is Defined as the ABCD Ellipsoid Between a Given Spectacle Refraction and Plano Sphere. Q1 and Q3 are Interquartile Ranges Around the Median and S.D Is Standard Deviation. The W-stat and p-value are related to the Shapiro–Wilk Test for Normality of the Data Distribution. Test Retest is Repeated Refraction Estimate for One Subject with Ellipsoid Gap of 5.25 Right Eye and 3.74 Left Eye |
Several variables were analyzed by multi-variable analysis against the Moptim MRT-200 ABCD Ellipsoid: age, gender, race, developmental delay, ABCD Ellipsoid for 2WIN and Retinomax and the Ellipsoid Gap for those n = 197 capable patients less than 20 years old. For right eye Moptim MRT-200 was only significantly influenced by Ellipsoid Gap (p < 0.001). For the left eye Moptim MRT-200 was mildly influenced by Retinomax (p = 0.08) but mainly influenced by ABCD Ellipsoid for 2WIN (p < 0.001) and Ellipsoid Gap (p < 0.001).
For the one moderately-high sphero-cylinder subject performing test re-Test twenty times with the Moptim MRT-200, the Ellipsoid Gap was 5.25 for right eye and 3.74 for the left eye. The right eye/left eye ABCD Ellipsoid of each Moptim MRT-200 compared with actual refraction had median 2.06/2.54, IQR1 1.57/2.00, IQR3 3.32/3.63, and since normally distributed, mean ± S.D.: 2.31±1.02/2.81±1.04 (Figure 5).
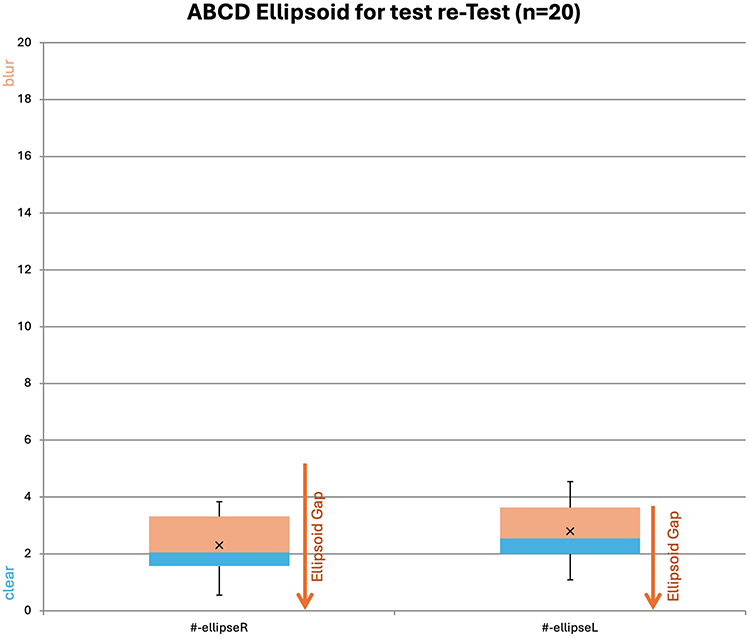 |
Figure 5 ABCD-Ellipsoid number values (#) for right (R) and left (L) eyes comparing twenty repeated Moptim MRT-200 sphero-cylinder estimates of refractive error compared to actual refraction for one astigmatic subject. The arrows indicated the Ellipsoid Gap degree of uncorrected blur for this subject. |
Visual acuity (Tumbling E recognition) with user-optimized dial on the Moptim MRT-200 was compared to best corrected, patch-insured monocular visual acuity with actual refraction using a calibrated M&S system and isolated HOTV optotypes. With the Moptim MRT-200, the patient either noted the adjacent value or the numeric sequence of Tumbling E optotype lines as the “smallest size they could still see.” Visual acuity converted to logMAR is compared with Bland Altman plots for all completed patients (n = 175) and for those with refractive error near plano sphere (n = 41) are compared in Figure 6. Box plots of compared logMAR visual acuity are shown in Figure 7. The correlation of visual acuity between Moptim MRT-200 and refined phoropter M&S chart was only an Intra Class Correlation of 0.41 right eye and 0.47 left eye. The MRT-200 near acuity was about 1 logMAR line less fine than actual M&S distance visual acuity.
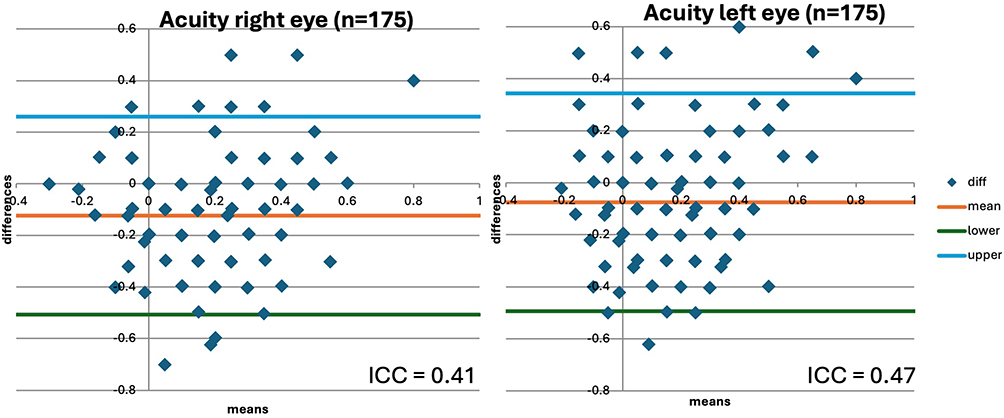 |
Figure 6 Bland Altman analysis of visual acuity comparing the Moptim MRT-200 internal Tumbling E chart to the actual phoropter refined refraction and HOTV optotypes on a calibrated distance M&S screen. On the right are comparisons for 41 subjects with minimal refractive error represented by Ellipsoid gap less than 2.0. |
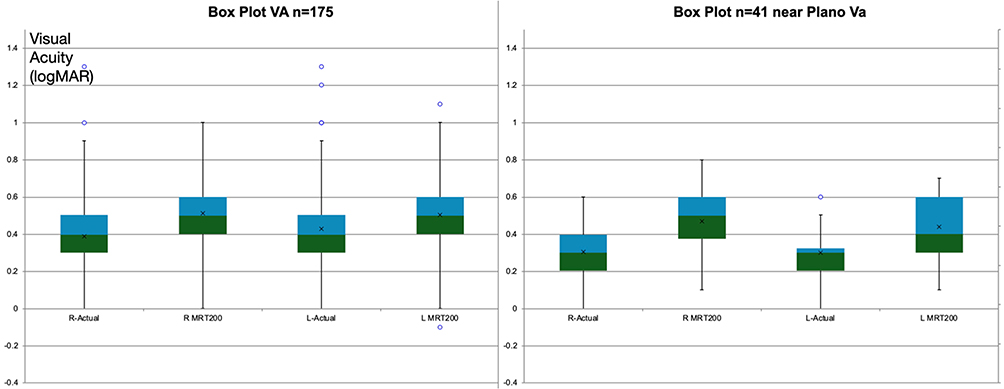 |
Figure 7 Box plots showing medians and interquartile ranges for logMAR visual acuity comparing the internal Tumbling E chart in the Moptim (MRT-200) with phoropter refined actual refraction and a distance HOTV on the M&S system. The left shows all 175 comparable patients while the right shows 41 patients with minimal refractive error such that Ellipsoid Gap was less than 2.0. |
Discussion
We compared an inexpensive, lightweight device with other state-of-the-art photoscreening and wavefront autorefractors seeking the ability to estimate sphero-cylinder refractive error in young people. To our knowledge, this is the first peer-reviewed comparison with other state-of-the-art pediatric refraction devices. The Chinese Moptim MRT-200 performed well in some ways, and less well in others, but appears to have merit for certain pediatric eye clinics and remote outreach eye clinics.
We used not only the three recognized, reliable15 and repeatable16 sphero-cylinder vector transformations but also the univariate, blur-related ABCD ellipsoid.12 Expensive, table-top autorefractors can be very accurate,17,18 while less expensive devices have also been compared19–21 with many endorsing Retinomax and QuickSee. Autorefractors may substitute well for subjective refraction in certain instances.22 Many studies only address cycloplegic refraction whereas dry refraction enhanced by fogging23 can yield immediate better visual acuity.24 In younger children, cycloplegic Retinomax reduces the over-accommodation we also observed with our near devices and it was utilized in the landmark MEPEDS and BPEDS studies.25 The intermediate-distance infrared photoscreeners are capable of giving precise sphero-cylinder refractions4,26 and they have also performed well compared to the Retinomax.12 Therefore our use of 2WIN and Retinomax for comparison with a new refractive device is appropriate and contemporary.
The Moptim MRT-200 requires much understanding by the screener, and cooperation by the patient to obtain and sphero-cylinder estimation. On the other hand, it allows rapid observation of a wide range of spherical refractive error to get a substantially blurred patient in reasonably refinable range. It is even possible to place a known, additional concave or convex trial lens over the device to estimate a much wider range of high spherical refraction. To estimate spherical refractive error, the Moptim MRT-200 was as quick as the 2WIN or Retinomax (usually about 5–10 seconds per eye). On the other hand, the explanation of internal eye chart clock-hours, slow diopter dial turning and explanation of observed changes took much longer to estimate sphero-cylinder refraction (over two minutes per eye even for test re-Test).
Despite our refractionist’s effort, these young patients still tended to over-accommodate during dry refraction especially with the near proximity tools Retinomax and Moptim MRT-200. The remote, 1-meter distant 2WIN elicited less accommodation, especially when the twinkling fixation lights were dimmed on the device. We noted that on their left (second) eyes with Moptim MRT-200, the accuracy of refraction by ellipsoid match was correlated with age. Symmetric extra accommodation of 1–3 diopters is often tolerated well by young children unless accompanied by accommodative esotropia, however it can produce asthenopia in older patients.
The Moptim MRT-200 internal visual acuity chart was somewhat confusing for American children. With respect to ceiling and floor optotype presentation, the Moptim MRT-200 showed extremely fine logMAR −0.4 resolution, but probably should add a much coarser logMAR ≥1.0 option also. The Tumbling E optotype is recognized internationally but children often confuse left and right, so an “up” a “down” and an “E” orientation in random order might simplify the chart. The logMAR designations adjacent to each row were also confusing and might be better to just label with the logMAR designation or international 6-meter denominator for international use.
Advantages and Limitations of the Moptim MRT-200: The device is sturdy and portable with easily obtained AAA batteries. It can estimate sphero-cylinder refraction and visual acuity. It is fairly simple to estimate spherical equivalent refraction. The cost less than $200 USD is an advantage. The disadvantages are the potential for over accommodation and a complex process to determine cylinder power and axis. The format and labelling of visual acuity Tumbling E chart require some explanation, also.
This study has several strengths including a diverse selection of young patients including race, ethnicity, developmental delay and wide amblyopia/strabismus mix. The three refractive devices and the confirmation were under similar dry conditions but attempting to limit over-accommodation. Visual acuity was compared with gold-standard monocular distance acuity. Conventional J0, J45 and spherical equivalent were compared, but also the newer ABCD univariate ellipsoid method which for the first ime is utilized to quantify uncorrected refractive error blur. Limitations of the study include testing within an eye exam room rather than in a remote mission environment. We did not have each patient identify the orientation of Each Tumbling E but rather asked them the smallest line they could see. Patients unable to complete one or more refractive tests were noted but excluded from final analysis. Certain aspects of age and developmental delays were not quantified to allow correlation of all factors.
Conclusion
The Moptim MRT-200 is affordable, portable and sturdy. It would not replace a 2WIN or Retinomax for remote mission precise sphero-cylinder lay refraction. Though not simple to understand with respect to its internal acuity chart and astigmatism estimation, the Moptim MRT-200 could be useful for lay- or eye doctor quick estimation of a wide range of spherical refractive error.
Clinical Trials Registry
Data Access: https://www.abcd-vision.org/references/MRT-200%20De-ID.pdf
Abbreviations
ABCD, Alaska Blind Child Discovery; Acos, arc cosine; BA, Bland Altman; Cos, cosine; D, diopter; E, Tumbling E optotype; HIPAA, Health insurance portability and accountability act; HOTV, bilaterally symmetric, non-copyrighted visual acuity optotypes; ICC, intra class correlation; IQR, interquartile range; J0 and J45, vector transformations of sphero-cylinder refraction; logMAR, acuity notation the logarithm of the minimum angle of resolution; M, spherical equivalent (sphere plus ½ cylinder); M&S, brand of visual acuity monitor system developed by Joe Marino; SBARS, school bus accommodation relaxing skiascopy; S.D., standard deviation; W-stat, Shapiro Wilks statistic for normality of data.
Consent Statement
All individuals in the video abstract gave consent to share their images for educational purposes.
Disclosure
Dr. Arnold coordinates the Alaska Blind Child Discovery which has received discounted vision screening technology from several vendors. Dr. Arnold is a board member and patent holder in PDI Check which makes vision screening games for autostereoscopic screens. Dr. Arnold is an investigator and protocol developer for the Pediatric Eye Disease Investigator Group. The authors report no other conflicts of interest in this work.
References
1. Kós AFdSN, Bernardo Kaplan Moscovici 2,Cesar Vilar1, MAPDC, Maíra Gomes Barbosa Da Silva1,Maurício Agne Neuwald1, ALDM, Jonathan Clive Lake1, Antonio Francisco Pimenta Motta5, Patrick Frensel de Moraes Tzelikis 1 PCC, Larissa Gouvea7, Walton Nosé2, Wilson Takashi Hida 1. Comparison of self-test refraction, autorefraction, and subjective refraction. Clin Ophthalmol. 2025;19:1085–1092. doi:10.2147/OPTH.S510850
2. Martin SJ, Htoo HE, Hser N, Arnold RW. Performance of two photoscreeners enhanced by protective cases. Clin Ophthalmol. 2020;14:1427–1435. doi:10.2147/OPTH.S251451
3. Samanta A, Shetty A, Nelson PC. Better one or two? A systematic review of portable automated refractors. J Telemed Telecare. 2022;28(6):404–411. doi:10.1177/1357633X20940140
4. Liu Z, Pazo E, Ye H, Yu C, Xu L. Comparing school-aged refraction measurements using the 2WIN-S portable refractor in relation to cycloplegic retinoscopy: a cross-sectional study. J Ophthalmol. 2021;2021:8. doi:10.1155/2021/6612476
5. Lang D, Leman R, Arnold AW, Arnold RW. Validated portable pediatric vision screening in the Alaska Bush. A VIPS-like study in the Koyukon. Alaska Med. 2007;49(1):2–15.
6. Sapiens N, Korani H, Serri J. Refraction Measurements Comparison between the EyeQue VisionCheck and Autorefractor and Phoropter Refraction. IOVS. 2024; 65(7): 609.
7. Sapiens N, O’Neal P. Accuracy measurement of an at-home refraction measurement device. Opt Eng. 2022;61(12):121805. doi:10.1117/1.OE.61.12.121805
8. Loayza A, Lewis A, Chamberlin S, Trivedi R, Wolf B, Peterseim MM. Evaluation of the Plenoptika QuickSee free portable autorefractor in schools in the Gambia. J Pediatr Ophthalmol Strabismus. 2025;62(2):122–127. doi:10.3928/01913913-20241105-03
9. Arnold RW. Comparative validation of plusoptix and AI-optic photoscreeners in children with high amblyopia risk factor prevalence. Clin Ophthalmol. 2022;16:2639–2650. doi:10.2147/OPTH.S378777
10. Miller JM. Clinical applications of power vectors. Optom Vis Sci. 2009;86(6):599–602. doi:10.1097/OPX.0b013e3181a6a211
11. Arnold RW, Beveridge JS, Martin SJ, Beveridge NR, Metzger EJ, Smith KA. Grading sphero-cylinder spectacle similarity. Clin Optomet. 2021;13:23–32. doi:10.2147/OPTO.S289770
12. Arnold R, Martin SJ, Beveridge JR, et al. Ellipsoid spectacle comparison of plusoptix, retinomax and 2WIN autorefractors. Clin Ophthalmol. 2021;15:3637–3648. doi:10.2147/OPTH.S326680
13. Schaafsma JD, Arnold RW. Pre-cycloplegic exam benefit of photoscreening and accommodation-relaxing skiascopy. Clin Ophthalmol. 2024;18:833–846. doi:10.2147/OPTH.S454430
14. Arnold AW, Arnold SL, Sprano JH, Arnold RW. School bus accommodation-relaxing skiascopy. Clin Ophthalmol. 2019;13:1841–1851. doi:10.2147/OPTH.S219031
15. Goss DA, Grosvenor T. Reliability of refraction--a literature review. J Am Optom Assoc. 1996;67(10):619–630.
16. Padhy D, Bharadwaj SR, Nayak S, Rath S, Das T. Does the accuracy and repeatability of refractive error estimates depend on the measurement principle of autorefractors? Transl Vis Sci Technol. 2021;10(1):2. doi:10.1167/tvst.10.1.2
17. Ghadimi H, Nikdel M, Suh DW. Comparison of photorefraction by Plusoptix A12 and cycloplegic autorefraction in children. BMC Ophthalmol. 2024;24(1):179. doi:10.1186/s12886-024-03459-w
18. Wang D, Jin N, Pei RX, et al. Comparison between two autorefractor performances in large scale vision screening in Chinese school age children. Int J Ophthalmol. 2020;13(10):1660–1666. doi:10.18240/ijo.2020.10.22
19. Joseph S, Varadaraj V, Dave SR, et al. Investigation of the accuracy of a low-cost, portable autorefractor to provide well-tolerated eyeglass prescriptions: a randomized crossover trial. Ophthalmology. 2021;128(12):1672–1680. doi:10.1016/j.ophtha.2021.05.030
20. Agarwal A, Bloom DE, deLuise VP, Lubet A, Murali K, Sastry SM. Comparing low-cost handheld autorefractors: a practical approach to measuring refraction in low-resource settings. PLoS One. 2019;14(10):e0219501. doi:10.1371/journal.pone.0219501
21. Sopeyin A, Young BK, Howard MA. 2020 evaluation of portable vision screening instruments. Yale J Biol Med. 2021;94(1):107–114. doi:10.1016/S0161-6420(96)30753-7
22. Orr PR, Cramer LD, Hawkins BS, Bressler NM. Manifest refraction versus autorefraction for patients with subfoveal choroidal neovascularization. Invest Ophthalmol Vis Sci. 2001;42(2):447–452.
23. Musa MJ, Zeppieri M. Principles and technique of fogging during subjective refraction. StatPearls. 2023.
24. Mimouni M, Zoller L, Horowitz J, Wygnanski-Jaffe T, Morad Y, Mezer E. Cycloplegic autorefraction in young adults: is it mandatory? Graefes Arch Clin Exp Ophthalmol. 2016;254(2):395–398. doi:10.1007/s00417-015-3246-1
25. Varma R, Deneen J, Cotter S, et al. The multi-ethnic pediatric eye disease study: design and methods. comparative study multicenter study research support, N.I.H. extramural research support, non-U.S. gov’t. Ophthalmic Epidemiol. 2006;13(4):253–262. doi:10.1080/09286580600719055
26. Jorge J, Fernandes P. Comparison of the Plusoptix A16 and vision screener V100. Front Ophthalmol. 2024;4:1414417. doi:10.3389/fopht.2024.1414417
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.