Back to Journals » Patient Preference and Adherence » Volume 19
Comparative Systematic Review of Telehealth Delivery Models, Intervention Content, and Outcomes in Heart Failure Care
Authors Sugiharto F ![]() , Trisyani Y
, Trisyani Y ![]() , Nuraeni A
, Nuraeni A ![]() , Abdullah KL
, Abdullah KL ![]()
Received 17 September 2025
Accepted for publication 16 December 2025
Published 30 December 2025 Volume 2025:19 Pages 4335—4352
DOI https://doi.org/10.2147/PPA.S568141
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Firman Sugiharto,1 Yanny Trisyani,2 Aan Nuraeni,2 Khatijah Lim Abdullah3
1Doctoral Program, Faculty of Nursing, Universitas Padjadjaran, Bandung, West Java, Indonesia; 2Department of Critical Care and Emergency Nursing, Faculty of Nursing, Universitas Padjadjaran, Bandung, West Java, Indonesia; 3School of Nursing, Faculty of Medical and Life Sciences, Sunway University, Bandar Sunway, Malaysia
Correspondence: Yanny Trisyani, Department of Critical Care and Emergency Nursing, Faculty of Nursing, Universitas Padjadjaran, Sumedang, West Java, Indonesia, Fax +620227795596, Email [email protected]
Background: Heart failure management remains challenging due to limited self-care and prevalent depressive symptoms, with telehealth emerging as an effective approach to strengthen disease management and enhance patients’ quality of life. However, studies that specifically explore models, intervention content, and the broader benefits of telehealth in HF management are still limited.
Purpose: This systematic review aimed to compare and synthesize different telehealth delivery models, intervention content, and associated outcomes in the management of patients with heart failure.
Methods: A systematic review was conducted in accordance with Cochrane and PRISMA guidelines. A comprehensive search was conducted across multiple databases, including PubMed, Scopus, EBSCOhost, Taylor & Francis, and Springer Nature, with a focus on randomised controlled trials (RCTs) published in English. The article selection process is based on title, abstract, full text, and eligibility criteria, including quality appraisal. Data analysis employed thematic synthesis and descriptive qualitative approaches to categorize interventions, content, and outcomes.
Results: The review included 28 studies, evaluating three main telehealth intervention models: (1) telemonitoring, (2) phone call support, and (3) smartphone and web-based applications. Intervention content included symptom and medication monitoring, patient education, empowerment for self-management, reminders and feedback, psychological and social support, and healthcare communication. The study outcomes were categorized into four themes, including clinical outcomes, physical and mental health outcomes, behavioral outcomes, and quality of life. Among these models, phone call support and reminder interventions were most often recommended as practical and feasible approaches, as they are easy to implement, and flexible.
Conclusion: This review highlights that while telehealth interventions consistently improve quality of life, their impact on mental health and long-term clinical outcomes remains variable. Integrating support models with phone calls and reminders into routine heart failure management may improve accessibility and continuity of care, particularly for patients requiring ongoing behavioral and emotional support.
Keywords: heart failure, telehealth, telemonitoring, telenursing, patient outcomes
Introduction
Heart failure (HF) is a global pandemic affecting approximately 64 million people worldwide.1 In the United States and Europe, >1 million hospitalizations are due to HF.2 In addition, a previous study reported that the combined average 30-day readmission rate from 18 countries was 13% (95% CI: 10%–16%) worldwide.3 HF is not only a health problem, but also a significant economic burden on the global health system.4 This condition reflects the significant challenges in managing HF, which not only increases the burden on global healthcare systems, but also worsens patients’ quality of life.
Higher hospitalisation, readmission, and mortality rates in HF patients are associated with poor levels of patient self-care.5–7 In addition, another challenge that also arises in HF patients is the high level of depressive symptoms. Depression is consistently associated with a poorer quality of life (QoL) in HF patients.8–10 Depression is common in HF patients and is closely associated with poor health-related quality of life (HRQoL). Depression affects a significant proportion of HF patients, with prevalence rates ranging from 21.5% to 65% across various studies and populations.9–11
Telehealth plays a crucial role in the management of HF patients. The American Heart Association (AHA) reported that telehealth has proven effective in enhancing the efficiency of information delivery, diagnosis, disease monitoring, and follow-up care conducted remotely, leading to significant advancements in cardiovascular disease management.12 In addition, telehealth innovations are an effective strategy for addressing depression and improving QoL in HF patients.13–17 Collaborative care models such as the Hopeful Heart Trial, which combines HF management with telephone depression care, significantly improve patients’ mood and QoL.18,19 Previous studies have used interactive tools and video-based CBT modules that can help patients change negative thought patterns, build self-efficacy, and adhere to treatment plans, directly addressing the impact of depression,18 which indirectly reduces the symptoms of depression.20–22 Additionally, telehealth facilitates regular communication between patients and healthcare providers, ensuring continuity of care.23 This approach not only improves clinical outcomes but also expands access to services, especially for patients and families living in remote areas, making it a practical and patient-centred strategy in managing heart failure.12,20
Although the effectiveness of telehealth in reducing hospitalisations, mortality, and improving self-care among HF patients has been widely demonstrated, existing reviews remain limited in scope. Previous reviews have focused on the benefits of telehealth for self-care in HF patients,24 as well as a nurse-led telecoaching intervention,25 without exploring existing models and content in telehealth.26,27 A comprehensive synthesis comparing these dimensions is still lacking. Addressing this gap, the present review aims to analyse and compare various telehealth delivery models, intervention contents, and their associated outcomes to provide a more integrated understanding of how telehealth can optimise HF management.
Exploring the various models and content used in telehealth is a crucial component in identifying best practices that can be applied in the care of HF patients. Without a thorough understanding of the telehealth models being implemented and the content being delivered, optimizing the use of telehealth to improve the quality of care and reduce readmission and mortality rates will be challenging to achieve. Although several studies have explored the specific benefits of telehealth, systematic reviews that provide a comprehensive analysis of the various approaches and types of content used in telehealth remain limited. This review aims to fill this gap by comparing and analyzing various telehealth interventions that have been implemented, as well as evaluating relevant content used to support HF patient management.
Materials and Methods
Study Design
This study employed a systematic review approach, following the Cochrane Handbook for Systematic Reviews of Interventions and conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.28,29 This review has been registered in PROSPERO with the ID number CRD420251050361.
Eligibility Criteria
In this review, three independent reviewers selected relevant articles according to the PRISMA guidelines (see Figure 1). The development of research questions and eligibility criteria was based on the PICOT framework. The population (P) of interest consisted of heart failure. The intervention (I) studied was telehealth, encompassing telemedicine and telenursing. The comparator (C) was standard care or usual care; the outcome (O) focused on health outcomes, including readmissions, mortality, self-efficacy, self-care, quality of life, knowledge, depression, anxiety, and other relevant measures. The study type (T) included in this review was restricted to randomized controlled trials (RCTs).
 |
Figure 1 PRISMA Flow Diagram adapted from Page MJ, McKenzie JE, Bossuyt PM et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. Creative Commons.28 |
 |
Figure 2 Risk of Bias Assessment. |
 |
Figure 3 Number of Studies Based on Country. |
 |
Figure 4 Delivery Models, Contents, and Outcomes of Telehealth. Abbreviations: HF, Heart Failure; FU, Follow-Up; BP, Blood Pressure; HR, Heart Rate; ECG, Electrocardiogram; SpO2, Peripheral Capillary Oxygen Saturation. |
Studies were eligible for inclusion if they were full-text, published in English, and employed an RCT design to evaluate the effectiveness of telehealth in managing patient with heart failure. Publications were excluded if the full text was unavailable, if the language was not English, or if the study was secondary research. No publication year limits were applied in this review to ensure a comprehensive inclusion of all relevant randomized controlled trials on telehealth interventions for heart failure patients. This approach was chosen to capture the evolution and longitudinal trends of telehealth technologies and intervention designs over time, considering the rapid and continuous advancement of digital health innovations in HF management.
Search Strategy
Identification of articles was conducted systematically through six main databases and search engine: EBSCOhost, PubMed, Scopus, Taylor and Francis, Springer Nature, and Sage Journal. The keywords used in the search process included: “heart failure or cardiac failure or CHF or chronic heart failure or congestive heart failure AND telenursing or telehealth or e-nursing or digital nursing AND clinical outcomes or patient outcomes or client outcomes”. The Boolean operators “AND” and “OR” were used to refine or broaden the search results and effectively capture relevant literature across various databases.
In addition to database searching, hand searching was also conducted. Hand searching refers to the manual process of reviewing reference lists of relevant articles, journals, or conference proceedings to identify additional studies that may not have been retrieved through electronic databases. This approach was used to ensure a more comprehensive identification of eligible studies for inclusion in the review.
Study Selection and Quality Appraisal
The authors (FS and AN) independently screened the studies according to the predefined eligibility criteria. During the initial selection phase, duplicates were identified and removed using Mendeley Reference Manager. Next, the titles, abstracts, and full texts of the articles were evaluated for their relevance to the research topic, with the inclusion and exclusion criteria applied. In the final stage, all authors conducted a detailed review of each selected article using the Joanna Briggs Institute (JBI) critical appraisal checklist to evaluate the quality of the studies.30 This tool was selected because it is a globally recognized instrument specifically designed for evaluating RCTs, and its standardized framework promotes consistency across reviewers, thereby enhancing the transparency of the appraisal process.
For quality assessment, articles with a RCT design were evaluated using 13 criteria. Each item provided four response options: Yes, No, Not Applicable, and Unclear. A score of 1 was assigned for each “Yes” response, while all other responses received a score of 0. Studies that obtained a JBI score below 75% were excluded from the review. Discrepancies in the assessment results were discussed among the authors. However, no disagreements occurred regarding the suitability of the selected studies for inclusion.
Assessment of Risk of Bias in Included Studies
Two reviewers (FS and AN) independently assessed the Risk of Bias (RoB) for RCT studies included in this review analysis using the Cochrane Risk of Bias (RoB) 2.0 tool. RCTs consist of five RoB domains, including (1) randomisation process, (2) deviation from the intended intervention, (3) missing outcome data, (4) outcome measurement, and (5) selection of reported outcomes.31 RoB is defined as “high”, “low”, or “some concern”, or “no information” for each domain. Discrepancies in the assessment results were then discussed, and a review by all authors determined the decision.
Data Extraction and Analysis
In this review, data from the selected studies were extracted and examined using tables that consolidated all relevant findings related to the research topic. Data extraction was performed by two reviewers (FS and AN) and subsequently reviewed by others reviewers (YT and KLA). The extraction table contained important study characteristics and interventions, and the data were analyzed thematically through an exploratory descriptive approach. The analysis process started with organising and presenting the extracted data in a table format based on the reviewed articles. Each finding was then thoroughly analysed and described in accordance with the extracted information. To ensure accuracy and minimise the risk of errors during data extraction, the authors conducted a final review of all included studies.
Results
Study Selection
The study selection process adhered to the PRISMA 2020 guidelines. An initial search across six major databases (PubMed, Springer Nature, Scopus, EBSCOhost, Taylor and Francis, and Sage Journal) yielded 14,185 records. Following the removal of 2,768 duplicates, 11,417 studies remained for title and abstract screening. Of these, 11,321 were excluded for not meeting the predefined eligibility criteria. Consequently, 96 full-text articles were retrieved for further assessment. Forty-three articles could not be accessed in full, leaving 53 for eligibility evaluation. At this stage, 32 studies were excluded due to heterogeneous study populations, inappropriate study designs, irrelevant interventions, or publication in languages other than English. In parallel, manual hand searching identified seven additional studies, all of which met the eligibility criteria. In total, 28 studies were included in the final systematic review.
Quality Appraisal and Risk of Bias of Included Studies
The results of the article quality analysis using the JBI showed that almost all the analysed studies had a good methodology (see Table S1). This is evidenced by the majority of studies scoring 13/13, indicating that they met almost all the criteria for reducing the risk of bias. However, several aspects were answered with “No” or “Unclear” in several studies, indicating potential methodological issues. An aspect that showed uncertainty was participant blinding (participants were blind to treatment assignment), where several studies did not provide clear information about whether participants were aware of the treatment they received.17,32–40 Additionally, one study also showed an “Unclear” response to the outcome assessors’ blindness to treatment assignment criteria.37
The risk of bias analysis also found that almost all studies were classified as low-risk (see Figure 2). Overall, although most studies scored high with a low risk of bias, it is important to pay attention to studies that show concerns in several domains. Domains such as deviation from the intended intervention and inconsistent outcome measurements warrant further scrutiny, as these may indicate issues with intervention implementation or the validity of the outcomes being measured. Therefore, although the majority of these studies demonstrated high quality and reliability, a more in-depth evaluation of studies with concerns in specific domains is crucial to ensure the credibility and relevance of their findings in a broader context.
Characteristics of Studies
The studies analyzed had various characteristics, including location, design, population, and participant demographics of the HF studies. Studies were conducted in various countries, including the United States, Australia, Germany, Poland, Iran, Canada, and several other countries (see Figure 3). All study designs used were RCTs, which are considered the most credible method for evaluating medical interventions.
The sample sizes in these studies varied, ranging from studies involving as few as nine participants in each group to those with more than 800 participants. The study with the largest sample size was conducted in the United States, with 826 participants in the intervention group and 827 in the control group.34 This large study allows for greater insight into the effectiveness of the intervention in a larger and more diverse group of patients. In addition, the study with the smallest sample size was conducted in the USA, with only 9 participants per group in a pilot study focused on heart failure patients with NYHA II–III.41
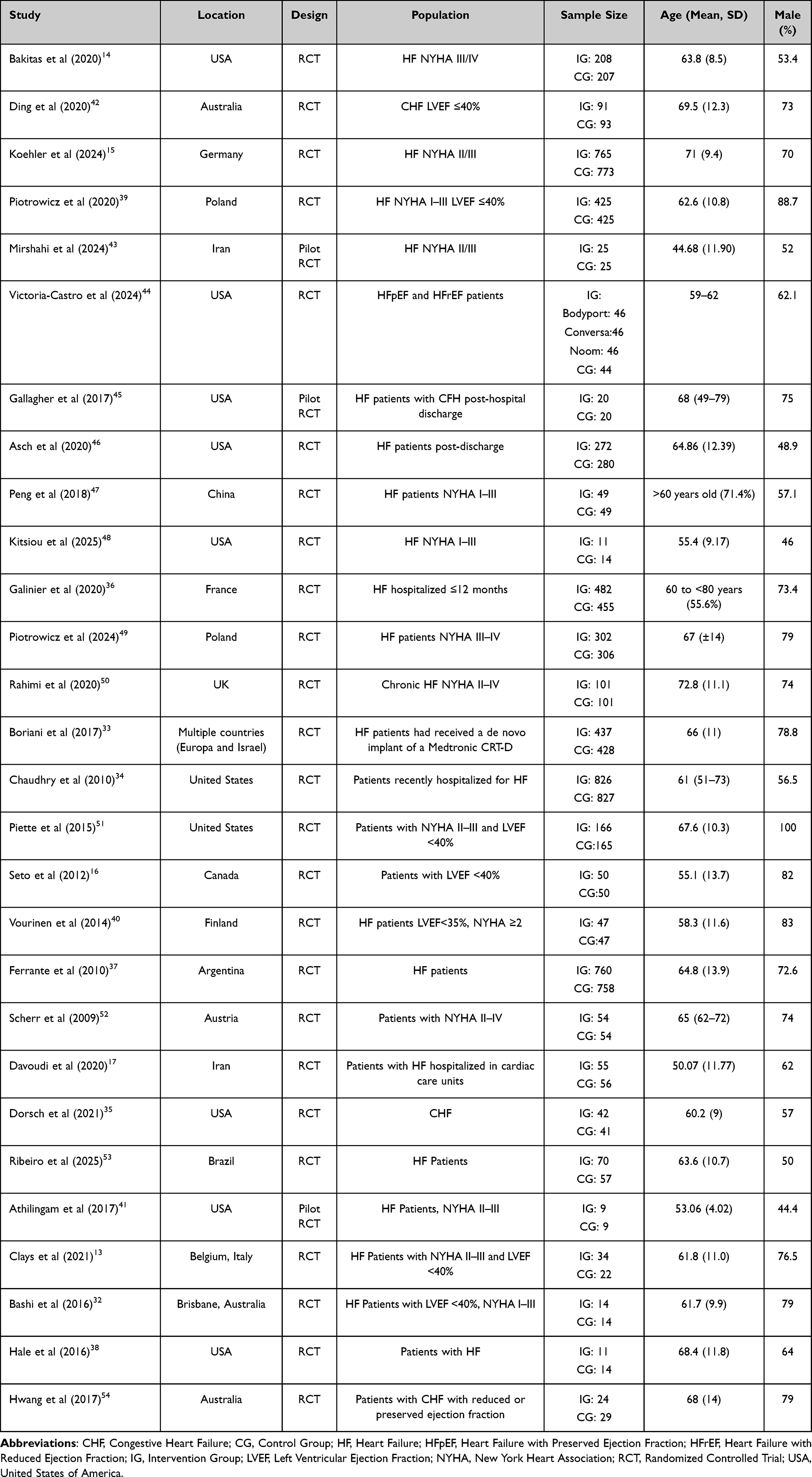 |
Table 1 Characteristics of Studies |
Characteristics of Participants
Most of the studies involved patients with NYHA stage II–IV heart failure, which includes moderate to severe conditions (See Table 1). In these studies, participants were mostly elderly patients, with many studies involving an average age of between 60 and 70 years, which is representative of the typical heart failure population worldwide. For example, a study in Australia involved participants with an average age of 69.5 years,42 while a study in Poland had an average age of 62.6 years.39 The gender distribution in most of these studies showed a preponderance of males, although there was variation between studies. For example, in a US study, the proportion of males reached 100%, while in some other studies in the USA and Canada, the percentage of males was around 50–75%.
Analysis of Delivery Models in Telehealth
Thematic analysis approach was used to categorize the delivery methods. First, descriptions of intervention delivery across all included RCTs were extracted into a data matrix. Two of the researchers (FS and AN) coded the descriptions according to mode of delivery (eg, remote monitoring devices, telephone, mobile applications). Codes with conceptual overlap were then clustered together by the two researchers and any disagreement was resolved by discussion. Lastly through iterative comparison of delivery characteristics to ensure the themes emerged inductively from the data. Three recurring themes were identified: (1) telemonitoring, (2) phone call support and reminders, and (3) mobile applications and web-based systems.
Telemonitoring is a remote health monitoring method that enables medical personnel to continuously monitor a patient’s condition in real-time using technological devices. In addition, telephone calls in the context of telehealth are an approach in which communication between the patient and the healthcare provider is conducted via telephone. Finally, mobile applications and web-based systems serve as telehealth platforms, enabling patients to monitor their health conditions independently. An application installed on a smartphone or internet-based web portal allows patients and healthcare workers to monitor patients.
Theme I: Telemonitoring
In the context of telemonitoring, more than half of the reviewed studies (n=10) have been conducted using technology to remotely monitor patient health conditions.15,16,33,36,38,39,42,45,50,54 The technologies used vary, including Bluetooth scales, tablets, Android apps, mobile phones, ECG devices, and wireless sensors. Systems used typically involve devices connected to a cellular network or the internet, allowing patient health data to be sent in real-time to healthcare providers for further monitoring. Monitoring is carried out on various aspects of the patient’s health to ensure their condition remains under control. Aspects that are monitored include body weight, vital signs (blood pressure, heart rate, breathing, and SpO2), ECG (Electrocardiogram), daily symptoms experienced by the patient, as well as medication compliance and reminders with a wireless system.
Theme II: Phone Call Support and Reminders
On the theme of telephone calls, five studies have utilised telephone technology to provide support and monitor patient health.14,34,37,43,53 Some aspects that are monitored include coping, namely the patient’s ability to deal with stress and their health problems. Bakitas et al (2020) utilised telephone calls to support patients in self-care, symptom management, and making critical life decisions in challenging situations.14 In addition, Mirshahi et al (2024) expanded the use of technology by combining phone calls, WhatsApp, and SMS for case discussions and providing palliative care education, allowing for more flexible communication between patients, families, and medical staff.43 The use of phone calls is also for symptom monitoring, including weight reporting and depression monitoring in patients with a telephone-based interactive voice response system.34 This system provides automated support, providing feedback based on patient-reported data.34 Two other studies used this phone call system as a medication reminder, self-care, and lifestyle instructions related to managing patient conditions effectively.37,53
Theme III: Smartphone App and Web-Based
The majority of studies (n=13) utilized iOS- and Android-based mobile applications, as well as web-based platforms, to support patient health monitoring.13,17,32,35,40,41,44,46–48,51,52,55 This technology allows patients to independently monitor their health and connect with medical providers. Furthermore, these apps enable patients to receive reminders, education, and support directly from medical professionals.
Several studies have used iOS and Android-based mobile applications. Previous studies have developed iOS/Android-based mobile applications to record biometrics and support patient-doctor communication, education, monitoring, live coaching, and peer support groups44 WeChat and QQ have been utilised for physical exercise programs and health education,47 as well as for vital signs monitoring and lifestyle management in heart failure patients.51,48 Other studies have developed applications for symptom monitoring, reminders, and physical exercise for heart failure patients17,35,41 Clays et al (2021) developed a web-based application that utilises wearable sensors to monitor physical health and provide psychological support.13
On the other hand, web-based systems are also used for patient health monitoring.32,46,51,55 Piotrowicz et al (2024) and Bashi et al (2016) used a web-based platform for specialist doctor consultations, symptom monitoring, and education for heart failure patients.32,55 Asch et al (2022) used a web-based system to support patient behaviour and ensure daily adherence,46 while Piette et al (2015) developed mobile and web applications for self-management, alerts, and automated feedback.51 These systems demonstrate how mobile applications and web-based platforms can be used in an integrated manner to improve patient health management.
Analysis of Content in Telehealth
An analysis of various studies found six categories of content in telehealth. These categories include (I) daily monitoring of symptoms and medication adherence,15–17,32–35,37,39–42,44–46,48,50–53 (II) Patients education,13,14,17,35–37,41,43,44,47,50,54,55 (III) Patient empowerment for self-management,13,14,32,38,39,41,46,47,53 (IV) Reminders and feedback,17,36,38,51,52 (V) Psychological and social support,16,43,46,54 and (VI) Communication with health workers.32,33,40,44 For more details, see Figure 4 and Table 2.
 |
Table 2 Characteristics of Intervention, Delivery Model, Content, and Summary of Results |
The Outcomes of Telehealth in Managing Heart Failure
Telehealth interventions have been shown to provide benefits in managing patients with heart failure, particularly in terms of remote monitoring and support for self-management (see Table 2 and Figure 4). General outcomes of implementing telehealth in patients with heart failure are categorised into four themes: (I) clinical outcomes, (II) physical and mental health outcomes, (III) behavioural outcomes, and (IV) quality of life. In clinical outcomes, telehealth can reduce mortality and readmission rates15,37–39,52,53 Additionally, in physical and mental health outcomes, the use of telehealth can improve physical function,44 knowledge,32,41 and reduce anxiety and depression.13 Then, on the behavioural outcomes theme, telehealth can improve self-care,16,32,41,55 compliance in monitoring symptoms and medications,42,48,51,54 self-efficacy and health belief.32,48 Lastly, the use of telehealth can also improve quality of life.14–17,35,38,39,43,47,55
Based on the studies analyzed, several also reported insignificant outcomes. Several studies also reported that the use of telehealth did not significantly reduce readmission, mortality, and emergency department visit rates,16,33–36,46 no change in self-care,13,40 QoL and physical well-being,13,35,41,44 cannot reduce anxiety and depression,14,41,47 and compliance in HF patient restrictions.45
Discussion
HF management remains a significant challenge in healthcare globally.56,57 Although conventional medical care plays an important role, many HF patients still face difficulties in monitoring their condition, adhering to treatment, and self-managing symptoms. In this context, telehealth interventions offer an innovative and promising approach to addressing these problems.15,50,51
Based on the results of this review, it is evident that telehealth interventions have significant potential to improve the health outcomes of HF patients, with a focus on enhancing self-care, reducing hospitalisation rates, and enhancing the quality of life for patients. From the 28 studies analysed, there were three themes of telehealth interventions: telemonitoring, phone call support, and technology-based mobile/web applications. These three categories offer distinct yet complementary benefits in patient management. Thematic analysis revealed that all three telehealth models have significant potential to improve clinical outcomes, physical and mental health, behavioral outcomes, and quality of life among HF patients.
Telemonitoring, as one of the main models, has shown high effectiveness in monitoring patient conditions in real-time.15,16,33,36,38,39,42,45,50,54 The technology used allows for the direct transmission of biometric data such as blood pressure, weight, and blood oxygenation level (SpO2) to healthcare providers, allowing for immediate intervention in the event of any irregularities in the patient’s vital signs or symptoms. The use of this technology also provides benefits in detecting changes in patient conditions earlier, leading to faster and more appropriate treatment adjustments.58 As a result, several studies have shown that telemonitoring can reduce hospitalization rates and improve patients’ quality of life.15,16,50 In addition, this model also supports increased adherence to self-care, which is an important factor in managing HF effectively.16,38 On the other hand, four other studies reported contrasting findings where telemonitoring-based interventions were unable to reduce readmission, hospitalization, and mortality rates in HF patients.16,33,36,39 Therefore, although telemonitoring shows great potential in monitoring patient conditions in real-time, the differences in results found in these studies highlight the importance of considering certain factors that may influence the effectiveness of a given intervention including patient characteristics, level of technological literacy, healthcare system support, and integration with multidisciplinary care teams.
Another intervention model is phone call support and reminder. This model also makes a significant contribution to improving the management of HF patients.14,34,37,43,53 Through phone calls, patients receive not only educational support regarding treatment and symptom management but also much-needed emotional support.14,34,37,43,53 However the results of this review found that the outcome of interventions in this category is still controversial. Two studies reported that this telephone-based intervention can reduce readmissions and hospitalisations by 1 to 3 years,37,53 However, other studies have shown no significant difference.34 In addition, QoL was also reported in both studies with different results.14,43 This may occur due to differences in content and other additional media in the intervention that influence the outcome in each study. Therefore, it is necessary to consider other aspects of content and delivery methods to increase the effectiveness of the intervention.
Mobile applications and web-based platforms have also proven to be beneficial models in the management of HF patients.13,17,32,35,40,41,44,46–48,51,52,55 This technology gives patients the opportunity to monitor their condition independently, receive medication reminders, and receive education related to managing their disease.17,35,47,51 However, differences in results were also found in studies that implemented interventions with this model. Several studies have reported that mobile and web-based application interventions can improve QoL or HR-QoL,17,35,47,48,55 In addition, an increase in patients’ self-care abilities was also observed in the studies by Athilingam et al (2017),41 Bashi et al (2016),32 and Piotrowicz et al (2024).55 Meanwhile, the other two studies did not experience any differences in self-care before and after the intervention.13,35 Then, the decrease in hospitalisation rates was only in the study of Scher et al (2009), three other studies reported no significant differences in the results of mortality, readmission, and hospitalisation rates of HF patients.35,40,46
The results of the thematic analysis show that the three telehealth models, such as telemonitoring, phone call support and reminders, and smartphone app/web-based, basically have similar core content. The core content of telehealth encompasses symptom monitoring, patient education, empowerment for self-management, provision of reminders and feedback, psychosocial support, and communication with healthcare professionals. These similarities emphasise that telehealth is built on the same foundation, namely, facilitating monitoring, increasing health literacy, strengthening self-care skills, and providing both emotional and clinical support. However, further analysis shows that the telemonitoring model tends to have a broader and more detailed content coverage than the other two models. Under the theme of “daily monitoring of symptoms and adherence,” telemonitoring consistently includes more comprehensive clinical parameters, such as daily weight, vital signs and daily reporting and medication adherence. This may be explained by the differences in the design of telemonitoring systems, and phone-based approaches as phone-based approaches depend on self-reporting while telemonitoring enables more continuous data. The diversity of monitored indicators provides an advantage in the early detection of deterioration in patient conditions, allowing for faster intervention to prevent rehospitalisation.
The phone call support and reminders model offers a simple approach, with a core strength in providing interpersonal support through basic monitoring (weight, symptoms, and medication adherence), education, and follow-up reminders, reinforced by two-way interaction with healthcare professionals or peer support to enhance motivation, adherence, and daily problem-solving.37,53 This model is easy to implement, flexible, and low-cost, making it suitable for moderate-risk patients who need behavioral reinforcement and emotional support.14,34,37,43,53 Meanwhile, smartphone apps and web-based offer flexibility and personalized interventions with similar content, but with a greater emphasis on self-management aspects.32,46,51,55 The content in this model includes digital education features, live coaching, and online peer support; Its advantages lie in easy access, real-time feedback, and integration of lifestyle modules, although its effectiveness is highly dependent on digital literacy and consistency of use, making it more suitable for younger, technology-savvy, and highly motivated patients in self-care.
All three telehealth models have similar core content, but there are important differences in the duration of follow-up use. Studies using the phone call support and reminders model have examined the longest intervention period, ranging between 12 weeks to 3 years, compared to telemonitoring (30 days to 24 months) and smartphone app/web-based (23 days to 12 months). This difference suggests that telephone-based interventions tend to be easier to sustain in the long term because they do not require specialised equipment or high digital literacy, but instead rely on relatively simple, flexible, and low-cost interpersonal communication. This also shows that phone call support is more feasible to implement widely, especially in the context of health systems with limited resources. Conversely, although telemonitoring and smartphone-based apps have proven effective in the short to medium term, limitations in cost, device availability, and patient adherence to the technology are factors that limit their long-term sustainability. Therefore, this aspect of follow-up duration reinforces the view that phone call support can be a more sustainable telehealth strategy, particularly for patients with chronic monitoring needs and long-term behavioral support requirements.
Despite the overall evidence supporting the benefits of telehealth interventions in HF management, findings across studies remain heterogeneous, with several trials reporting neutral or even negative outcomes. For instance, several RCTs studies reported that no significant differences in mortality, hospitalization, or physical well-being compared with standard care.33,39,50 Similarly, Chaudhry et al (2010)34 found that a telemonitoring-based system did not reduce readmission or mortality rates, while Victoria-Castro et al (2024) and Asch et al (2022) also demonstrated limited effects on QoL and readmissions.44,46 However, a recent meta-analysis including 17 RCTs reported that telemonitoring was effective in reducing the number of patients readmitted to the hospital compared with usual care strategies.59 These variability in outcomes may be due to the differences in patient populations (eg, age, digital literacy, severity of HF), the design of the platforms (such as whether they are interactive feedback versus being primarily self-management tools), and the duration and intensity of the interventions.
The factors supporting the success of telehealth interventions are diverse. Accessibility to technology is crucial, especially for patients living in remote areas or with limited access to technological devices.60–62 Studies show that difficulties in accessing or using technology can hinder the effectiveness of telehealth interventions, even though the technology offers many benefits.61,63,64 In addition, patient involvement is also a determining factor in the success of this intervention.41,44,65 Patients who have high levels of engagement in telehealth programs tend to show better outcomes, both in terms of symptom management and treatment adherence.41 Therefore, it is important for healthcare professionals to ensure that patients feel supported and involved in their care process, whether through regular communication, reminders, or providing motivation.
Implication for Practice
The results of this review indicate that telehealth interventions have great potential in improving the management of HF patients. Evidence supports the importance of integrating technologies, such as telemonitoring, phone support, and mobile and web-based applications, into daily clinical practice to improve patient self-care, reduce hospitalisations, and enhance patient quality of life. Therefore, healthcare practitioners should consider implementing telehealth interventions tailored to the specific needs of HF patients, particularly for elderly patients and those with multiple comorbidities. In addition, given the positive results related to reduced mortality rates, hospitalisations, and increased self-care behaviour, the integration of telehealth into the HF patient care system is a strategic step that needs to be prioritised.
Strengths and Limitations of the Study
There are several advantages to this review. This study has a significant strength in its application of a rigorous methodology, involving 28 RCTs, which is the most valid research method for assessing the effectiveness of an intervention. Additionally, the diversity of study populations and locations enables these findings to be applied to various groups of HF patients worldwide. Next, this review successfully identified and evaluated various delivery models and content in telehealth interventions, which provided valuable insights for further development in healthcare practice.
This study presents robust findings. However, several limitations should be noted. First, heterogeneity in the types of interventions, as well as the characteristics of the patient population, makes it difficult to generalize the findings to the entire HF patient population. In addition, some of the included studies exhibited methodological weaknesses, such as a lack of clarity regarding blinding procedures, which could introduce bias into the study results. Another limitation is the lack of long-term follow-up in many studies, which reduces understanding of the lasting impact of telehealth interventions on patient clinical outcomes.
Conclusion
Telehealth interventions including telemonitoring, phone call support and reminders, and mobile or web-based applications demonstrate substantial potential in optimizing the management of patients with HF. While telemonitoring appears most effective in comprehensive, high-resource settings where continuous monitoring and data integration are feasible, simpler approaches such as nurse-led phone call support and reminder systems may be more applicable in resource-limited contexts. This review highlights that although many interventions show reductions in hospital readmissions and improvements in self-care and QoL, outcome variability remains evident across different models and populations. These inconsistencies underscore the need for greater standardization of intervention content, sustained engagement strategies, and integration into existing health systems. Future research should prioritize evaluating long-term effectiveness, addressing digital literacy barriers, and exploring scalable, cost-effective models to ensure equitable access and sustainable implementation of telehealth in heart failure care.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lippi G, Sanchis-Gomar F. Global epidemiology and future trends of heart failure. AME Med J. 2020;5(Ci):2–7. doi:10.21037/amj.2020.03.03
2. Ambrosy AP, Fonarow GC, Butler J, et al. The global health and economic burden of hospitalizations for heart failure: lessons learned from hospitalized heart failure registries. J Am Coll Cardiol. 2014;63(12):1123–1133. doi:10.1016/j.jacc.2013.11.053
3. Foroutan F, Rayner DG, Ross HJ, et al. Global Comparison of Readmission Rates for Patients With Heart Failure. J Am Coll Cardiol. 2023;82(5):430–444. doi:10.1016/j.jacc.2023.05.040
4. Wei C, Heidenreich PA, Sandhu AT. The economics of heart failure care. Prog Cardiovasc Dis. 2024;82:90–101. doi:10.1016/j.pcad.2024.01.010
5. Sahebi A, Mohammad-Aliha J, Ansari-Ramandi M, Naderi N. Investigation the relationship between self-care and readmission in patients with chronic heart failure. Res Cardiovasc Med. 2015;4(1). doi:10.5812/cardiovascmed.25472
6. Ghorbanzadeh M, Khosravirad Z, Rostamzadeh M, et al. The Efficacy of Self-care Behaviors, Educational Interventions, and Follow-up Strategies on Hospital Readmission and Mortality Rates in Patients with Heart Failure: self-care Behaviors in Heart Failure Patients. Galen Med J. 2023;12. doi:10.31661/gmj.v12i.3116
7. Freedland KE, Skala JA, Steinmeyer BC, Chen L, Carney RM, Rich MW. Longitudinal Relationships Between Heart Failure Self-care and All-Cause Hospital Readmissions. J Cardiovasc Nurs. 2024;39(3):279–287. doi:10.1097/JCN.0000000000001059
8. Aggelopoulou Z, Fotos NV, Chatziefstratiou AA, Giakoumidakis K, Elefsiniotis I, Brokalaki H. The level of anxiety, depression and quality of life among patients with heart failure in Greece. Appl Nurs Res. 2017;34:52–56. doi:10.1016/j.apnr.2017.01.003
9. Bekelman DB, Havranek EP, Becker DM, et al. Symptoms, Depression, and Quality of Life in Patients With Heart Failure. J Card Fail. 2007;13(8):643–648. doi:10.1016/j.cardfail.2007.05.005
10. Mulugeta H, Sinclair PM, Wilson A. Prevalence of depression and its association with health-related quality of life in people with heart failure in low- and middle-income countries: a systematic review and meta-analysis. PLoS One. 2023;18(3 March):1–17. doi:10.1371/journal.pone.0283146
11. AbuRuz ME. Anxiety and depression predicted quality of life among patients with heart failure. J Multidiscip Healthc. 2018;11:367–373. doi:10.2147/JMDH.S170327
12. Takahashi EA, Schwamm LH, Adeoye OM, et al. An Overview of Telehealth in the Management of Cardiovascular Disease: a Scientific Statement from the American Heart Association. Circulation. 2022;146(25):E558–68. doi:10.1161/CIR.0000000000001107
13. Clays E, Puddu PE, Luštrek M, et al. Proof-of-concept trial results of the HeartMan mobile personal health system for self-management in congestive heart failure. Sci Rep. 2021;11(1):1–10. doi:10.1038/s41598-021-84920-4
14. Bakitas MA, Dionne-Odom JN, Ejem DB, et al. Effect of an Early Palliative Care Telehealth Intervention vs Usual Care on Patients with Heart Failure: the ENABLE CHF-PC Randomized Clinical Trial. JAMA Intern Med. 2020;180(9):1203–1213. doi:10.1001/jamainternmed.2020.2861
15. Koehler F, Koehler J, Bramlage P, et al. Impact of telemedical management on hospitalization and mortality in heart failure patients with diabetes: a post-hoc subgroup analysis of the TIM-HF2 trial. Cardiovasc Diabetol. 2024;23(1):1–9. doi:10.1186/s12933-024-02285-0
16. Seto E, Leonard KJ, Cafazzo JA, Barnsley J, Masino C, Ross HJ. Mobile phone-based telemonitoring for heart failure management: a randomized controlled trial. J Med Internet Res. 2012;14(1):1–14.
17. Davoudi M, Ghezeljeh TN, Aghouee FV. Effect of a Smartphone-Based App on the Quality of Life of Patients With Heart Failure: randomized Controlled Trial. JMIR Nurs. 2020;3(1):1–12.
18. Fezza GC, Sansone S, Nolan RP. Therapeutic components of digital counseling for chronic heart failure. Front Psychiatry. 2022;13(October):1–8. doi:10.3389/fpsyt.2022.888524
19. Herbeck Belnap B, Anderson A, Abebe KZ, et al. Blended collaborative care to treat heart failure and comorbid depression: rationale and Study Design of the Hopeful Heart Trial. Psychosom Med. 2019;81(6):495–505. doi:10.1097/PSY.0000000000000706
20. Silva-Cardoso J, Juanatey JRG, Comin-Colet J, Sousa JM, Cavalheiro A, Moreira E. The Future of Telemedicine in the Management of Heart Failure Patients. Card Fail Rev. 2021;7:2–6. doi:10.15420/cfr.2020.32
21. Tedeschi A, Palazzini M, Trimarchi G, et al. Heart Failure Management through Telehealth: expanding Care and Connecting Hearts. J Clin Med. 2024;13(9):2592. doi:10.3390/jcm13092592
22. Kaihara T, Scherrenberg M, Intan-Goey V, et al. Efficacy of digital health interventions on depression and anxiety in patients with cardiac disease: a systematic review and meta-Analysis. Eur Hear J - Digit Heal. 2022;3(3):445–454. doi:10.1093/ehjdh/ztac037
23. Masterson Creber R, Dodson JA, Bidwell J, et al. Telehealth and Health Equity in Older Adults with Heart Failure: a Scientific Statement from the American Heart Association. Circ Cardiovasc Qual Outcomes. 2023;16(11):E000123. doi:10.1161/HCQ.0000000000000123
24. Ersananda A, Prasetya H, Ichsan B. A Meta Analysis: effectiveness of Telemedicine to Improve Self-Care in Patients with Hearth Failure. J Heal Policy Manag. 2024;9(1):119–130.
25. Imanuel Tonapa S, Inayati A, Sithichoksakulchai S, Daryanti Saragih I, Efendi F, Chou FH. Outcomes of nurse-led telecoaching intervention for patients with heart failure: a systematic review and meta-analysis of randomised controlled trials. J Clin Nurs. 2022;31(9–10):1125–1135. doi:10.1111/jocn.16025
26. Wang C, Ba Y, Ni J, Huang R, Du X. Role of Telemedicine Intervention in the Treatment of Patients with Chronic Heart Failure: a Systematic Review and Meta-analysis. Anatol J Cardiol. 2024;28(4):177–187. doi:10.14744/AnatolJCardiol.2023.3873
27. Zhu Y, Gu X, Xu C. Effectiveness of telemedicine systems for adults with heart failure: a meta-analysis of randomized controlled trials. Heart Fail Rev. 2020;25(2):231–243. doi:10.1007/s10741-019-09801-5
28. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:1–11.
29. Riley RD, Moons KGM, Snell KIE, et al. A guide to systematic review and meta-analysis of prognostic factor studies. BMJ. 2019;364. doi:10.1136/bmj.k4597
30. Joanna Briggs Institute (JBI). JBI’s critical appraisal tools [Internet]. 2022. Available from: https://jbi.global/critical-appraisal-tools.
31. Strene JAC, Page JSMRGE, Blencowe NS, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:1–8.
32. Bashi N, Windsor C, Douglas C. Evaluating a Web-Based Self-Management Intervention in Heart Failure Patients: a Pilot Study. JMIR Res Protoc. 2016;5(2):e116. doi:10.2196/resprot.5093
33. Boriani G, Da Costa A, Quesada A, et al. Effects of remote monitoring on clinical outcomes and use of healthcare resources in heart failure patients with biventricular defibrillators: results of the MORE-CARE multicentre randomized controlled trial. Eur J Heart Fail. 2017;19(3):416–425. doi:10.1002/ejhf.626
34. Chaudhry SI, Mattera JA, Curtis JP, et al. Telemonitoring in Patients with Heart Failure. N Engl J Med. 2010;363(24):2301–2309. doi:10.1056/NEJMoa1010029
35. Dorsch MP, Farris KB, Rowell BE, Hummel SL, Koelling TM. The Effects of the ManageHF4Life Mobile App on Patients with Chronic Heart Failure: randomized Controlled Trial. JMIR mHealth uHealth. 2021;9(12):e26185. doi:10.2196/26185
36. Galinier M, Roubille F, Berdague P, et al. Telemonitoring versus standard care in heart failure: a randomised multicentre trial. Eur J Heart Fail. 2020;22(6):985–994. doi:10.1002/ejhf.1906
37. Ferrante D, Varini S, MacChia A, et al. Long-term results after a telephone intervention in chronic heart failure: DIAL (Randomized trial of phone intervention in chronic heart failure) follow-up. J Am Coll Cardiol. 2010;56(5):372–378. doi:10.1016/j.jacc.2010.03.049
38. Hale TM, Jethwani K, Kandola MS, Saldana F, Kvedar JC. A remote medication monitoring system for chronic heart failure patients to reduce readmissions: a two-arm randomized pilot study. J Med Internet Res. 2016;18(5):e91. doi:10.2196/jmir.5256
39. Piotrowicz E, Pencina MJ, Opolski G, et al. Effects of a 9-Week Hybrid Comprehensive Telerehabilitation Program on Long-term Outcomes in Patients with Heart Failure: the Telerehabilitation in Heart Failure Patients (TELEREH-HF) Randomized Clinical Trial. JAMA Cardiol. 2020;5(3):300–308. doi:10.1001/jamacardio.2019.5006
40. Vuorinen AL, Leppänen J, Kaijanranta H, et al. Use of home telemonitoring to support multidisciplinary care of heart failure patients in Finland: randomized controlled trial. J Med Internet Res. 2014;16(12):e282. doi:10.2196/jmir.3651
41. Athilingam P, Jenkins B, Johansson M, Labrador M. A mobile health intervention to improve self-care in patients with heart failure: pilot randomized control trial. JMIR Cardio. 2017;1(2):e3. doi:10.2196/cardio.7848
42. Ding H, Jayasena R, Chen SH, et al. The effects of telemonitoring on patient compliance with self-management recommendations and outcomes of the innovative telemonitoring enhanced care program for chronic heart failure: randomized controlled trial. J Med Internet Res. 2020;22(7):1–12. doi:10.2196/17559
43. Mirshahi A, Bakitas M, Khoshavi M, et al. The impact of an integrated early palliative care telehealth intervention on the quality of life of heart failure patients: a randomized controlled feasibility study. BMC Palliat Care. 2024;23(1):1–13. doi:10.1186/s12904-024-01348-z
44. Victoria-Castro AM, Martin ML, Yamamoto Y, et al. Impact of Digital Health Technology on Quality of Life in Patients With Heart Failure. JACC. 2024;12(2):336–348. doi:10.1016/j.jchf.2023.09.022
45. Gallagher BD, Moise N, Haerizadeh M, Ye S, Medina V, Kronish IM. Telemonitoring Adherence to Medications in Heart Failure Patients (TEAM-HF): a Pilot Randomized Clinical Trial. J Card Fail. 2017;23(4):345–349. doi:10.1016/j.cardfail.2016.11.001
46. Asch DA, Troxel AB, Goldberg LR, et al. Remote Monitoring and Behavioral Economics in Managing Heart Failure in Patients Discharged from the Hospital: a Randomized Clinical Trial. JAMA Intern Med. 2022;182(6):643–649. doi:10.1001/jamainternmed.2022.1383
47. Peng X, Su Y, Hu Z, et al. Home-based telehealth exercise training program in Chinese patients with heart failure A randomized controlled trial. Med. 2018;97(35).
48. Kitsiou S, Gerber BS, Buchholz SW, Kansal MM, Sun J, Pressler SJ. Patient-Centered mHealth Intervention to Improve Self-Care in Patients With Chronic Heart Failure: Phase 1 Randomized Controlled Trial. J Med Internet Res. 2025;27.
49. Piotrowicz K, Krzesiński P, Galas A, et al. Health-related quality of life and self-care in heart failure patients under telecare—insights from the randomized, prospective, controlled AMULET trial. Front Public Health. 2024;12(September):1–10.
50. Rahimi K, Nazarzadeh M, Pinho-Gomes AC, et al. Home monitoring with technology-supported management in chronic heart failure: a randomised trial. Heart. 2020;106(20):1573–1578. doi:10.1136/heartjnl-2020-316773
51. Piette JD, Striplin D, Marinec N, et al. A mobile health intervention supporting heart failure patients and their informal caregivers: a randomized comparative effectiveness trial. J Med Internet Res. 2015;17(6):e142. doi:10.2196/jmir.4550
52. Scherr D, Kastner P, Kollmann A, et al. Effect of home-based telemonitoring using mobile phone technology on the outcome of heart failure patients after an episode of acute decompensation: randomized controlled trial. J Med Internet Res. 2009;11(3):1–12. doi:10.2196/jmir.1252
53. Ribeiro EG, Brant LCC, Rezende LC, et al. Effect of Telemedicine Interventions on Heart Failure Hospitalizations: a Randomized Trial. J Am Heart Assoc. 2025;14(6):e036241. doi:10.1161/JAHA.124.036241
54. Hwang R, Bruning J, Morris NR, Mandrusiak A, Russell T. Home-based telerehabilitation is not inferior to a centre-based program in patients with chronic heart failure: a randomised trial. J Physiother. 2017;63(2):101–107. doi:10.1016/j.jphys.2017.02.017
55. Piotrowicz K, Krzesiński P, Galas A, et al. Health-related quality of life and self-care in heart failure patients under telecare—insights from the randomized, prospective, controlled AMULET trial. Front Public Health. 2024;12(September):1–11.
56. Sapna F, Raveena F, Chandio M, et al. Advancements in Heart Failure Management: a Comprehensive Narrative Review of Emerging Therapies. Cureus. 2023;15(10):e46486. doi:10.7759/cureus.46486
57. Shahim B, Kapelios CJ, Savarese G, Lund LH. Global Public Health Burden of Heart Failure: an Updated Review. Card Fail Rev. 2023;9:e11. doi:10.15420/cfr.2023.05
58. Rebolledo Del Toro M, Herrera Leaño NM, Barahona-Correa JE, Muñoz Velandia OM, Fernández ÁDG, Peña ÁA G. Effectiveness of mobile telemonitoring applications in heart failure patients: systematic review of literature and meta-analysis. Heart Fail Rev. 2023;28(2):431–452. doi:10.1007/s10741-022-10291-1
59. Masotta V, Dante A, Caponnetto V, et al. Telehealth care and remote monitoring strategies in heart failure patients: a systematic review and meta-analysis. Hear Lung. 2024;64(December 2023):149–167. doi:10.1016/j.hrtlng.2024.01.003
60. Moehr J, Schaafsma J, Anglin S, Pantazi S, Grimm N, Anglin S. Success factors for telehealth - A case study. Int J Med Inform. 2006;75(10–11):755–763. doi:10.1016/j.ijmedinf.2005.11.001
61. Bradford N, Caffery L, Smith A. Telehealth services in rural and remote Australia: a systematic review of models of care and factors influencing success and sustainability. Rural Remote Health. 2016;16(4):4268.
62. Rangachari P, Mushiana S, Herbert K. A Narrative Review of Factors Historically Influencing Telehealth Use across Six Medical Specialties in the United States. Int J Environ Res Public Health. 2021;18(9):4995. doi:10.3390/ijerph18094995
63. Gajarawala SN, Pelkowski JN. Telehealth Benefits and Barriers. J Nurse Pract. 2021;17(2):218–221. doi:10.1016/j.nurpra.2020.09.013
64. Adams RB, Nelson VR, Holtz BE. Barriers for Telemedicine Use Among Nonusers at the Beginning of the Pandemic. Telemed reports. 2021;2(1):211–216. doi:10.1089/tmr.2021.0022
65. Victoria-Castro AM, Martin M, Yamamoto Y, et al. Pragmatic randomized trial assessing the impact of digital health technology on quality of life in patients with heart failure: design, rationale and implementation. Clin Cardiol. 2022;45(8):839–849. doi:10.1002/clc.23848
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Differential Effects of Telehealth on Psychological Outcomes in Heart Failure: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
Sugiharto F, Trisyani Y, Nuraeni A, Abdullah KL
Therapeutics and Clinical Risk Management 2026, 22:617167
Published Date: 30 June 2026