Back to Journals » Patient Preference and Adherence » Volume 20
Comparative Systematic Review of Home-Based and Center-Based Cardiac Rehabilitation of Delivery Models and Outcomes
Authors Karisa P ![]() , Sylviana N
, Sylviana N ![]() , Syamsunarno MRAA, Fitria N
, Syamsunarno MRAA, Fitria N ![]() , Tiksnadi BB, Setiawan S
, Tiksnadi BB, Setiawan S
Received 7 December 2025
Accepted for publication 5 February 2026
Published 19 February 2026 Volume 2026:20 581645
DOI https://doi.org/10.2147/PPA.S581645
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Putri Karisa,1 Nova Sylviana,2,3 Mas Rizky Anggun Adipurna Syamsunarno,2 Nita Fitria,3,4 Badai Bhatara Tiksnadi,5 Setiawan Setiawan2,3
1Doctoral Program in Medical Science, Faculty of Medicine, Universitas Padjadjaran, Bandung, West Java, Indonesia; 2Department of Biomedical Sciences, Faculty of Medicine, Universitas Padjadjaran, Bandung, West Java, Indonesia; 3Center of Sport Science, Wellness, and Longevity, Graduate School, Universitas Padjadjaran, Bandung, West Java, Indonesia; 4Department of Fundamental Nursing, Biomedical Division, Faculty of Nursing, Universitas Padjadjaran, Sumedang, West Java, Indonesia; 5Department of Cardiology and Vascular Medicine, Hasan Sadikin General Hospital-Universitas Padjadjaran, Bandung, West Java, Indonesia
Correspondence: Nova Sylviana, Department of Biomedical Sciences, Faculty of Medicine, Universitas Padjadjaran, Jalan Raya Bandung-Sumedang, Km. 21 Jatinangor, Sumedang, West Java, 45363, Indonesia, Tel +62-022-84288888, Fax +62-022-2036549, Email [email protected]
Aim: Center-based cardiac rehabilitation (CBCR) is a cornerstone of secondary prevention, yet participation remains limited due to access constraints and adherence barriers. Home-based cardiac rehabilitation (HBCR) has evolved from conventional telephone- and logbook-supported programs to technology-assisted telerehabilitation. However, the extent to which specific delivery models translate into clinical and patient-centered benefits remains unclear.
Purpose: To compare HBCR and CBCR delivery models and outcomes, and to evaluate whether variation in HBCR delivery approaches is associated with differences in functional capacity, adherence, quality of life, and cardiovascular risk factors.
Patients and Methods: A PRISMA 2020-guided systematic review of randomized controlled trials compared HBCR with Phase II/III CBCR. Risk of bias was assessed using RoB 2. Outcomes were synthesized narratively, and random-effects meta-analyses (inverse-variance) were conducted where data were sufficiently comparable for VO2peak, 6-minute walk distance (6MWD), and adherence.
Results: Fourteen trials (2002– 2023), including 1,085 participants (22– 242 per study), were included. HBCR delivery clustered into traditional programs (exercise prescription with telephone/logbook follow-up) and technology-assisted models (web/app platforms, wearable monitoring, and/or video-supported supervision). Overall risk of bias was low in six trials, some concerns in seven, and high in one; concerns were most commonly related to randomization, while outcome measurement was consistently low risk. Meta-analysis favored HBCR for VO2peak at follow-up (MD 0.68 mL·kg− 1·min− 1, 95% CI 0.06– 1.29; I2=4%), whereas 6MWD showed no between-setting difference (MD − 6.77 m, 95% CI − 55.06 to 41.52; I2=61%). Adherence modestly favored HBCR (MD 3.24 sessions, 95% CI − 0.10 to 6.58; I2=70%). HRQoL and cardiovascular risk factors were generally comparable.
Conclusion: HBCR yields outcomes comparable to CBCR, with small advantages in VO2peak and adherence, supporting the scalability of HBCR, particularly technology-assisted models, to expand rehabilitation access and uptake.
Keywords: cardiac rehabilitation, center-based CR, delivery models, home-based CR, telerehabilitation
Introduction
Improving access to effective cardiac rehabilitation directly advances good health and well-being by strengthening prevention and management, and by reducing mortality from Cardiovascular disease (CVD). CVD remains the leading cause of death and disability worldwide, accounting for nearly 20 million deaths annually.1 Exercise-based cardiac rehabilitation (CR) is a cornerstone of secondary prevention and improves survival, functional capacity, and quality of life.2,3 Current guidelines recommend CR for a broad range of eligible patients, including those following acute coronary syndrome or myocardial infarction, after percutaneous coronary intervention or coronary artery bypass grafting, and for selected heart failure populations.4 Clinically, CR is delivered across phased care (Phase I inpatient, Phase II early outpatient/supervised, and Phase III/IV long-term maintenance), and incorporates core components such as structured exercise training, patient education, cardiovascular risk factor management, psychosocial support, and long-term lifestyle counseling.4,5 However, participation in traditional center-based CR (CBCR) remains low, with only 20–30% of eligible patients enrolling.6 Barriers are multifactorial and include access and system constraints (distance, facility availability, costs/coverage), as well as patient-level factors such as comorbidities, competing responsibilities, and psychosocial concerns.7,8 These barriers contribute to suboptimal engagement and may compromise clinical outcomes.4
Home-based cardiac rehabilitation (HBCR) has emerged as an alternative that offers greater flexibility and may reduce logistical burden while supporting family involvement, features that can facilitate adherence and sustained behavior change. Prior systematic reviews generally report comparable outcomes between HBCR and CBCR for exercise capacity and cardiovascular risk factors,9,10 and telerehabilitation-based CR appears safe and effective in improving cardiorespiratory fitness compared with usual care or CBCR.11–14 Nonetheless, many reviews pool heterogeneous HBCR delivery models and comparators and often prioritize composite outcomes (eg, mortality or rehospitalization), limiting inference regarding which delivery approaches best support functional capacity and patient-centered outcomes.10,15,16 In addition, variability in exercise dose, program duration, and reporting of intervention components hinders translation into scalable program design.17,18
Importantly, HBCR also faces engagement challenges, including low self-motivation and concerns about exercising without direct supervision.19 This has driven the adoption of technology-assisted delivery (eg, mobile apps, remote monitoring, and structured telecoaching) to enhance feedback, safety, and adherence.11,20,21 Thus, HBCR with a telehealth approach appears to be an innovative rehabilitation model that is feasible and effective compared to conventional CR in hospitals.11,14,20 However, it remains unclear whether different HBCR delivery models, traditional (eg, logbooks and telephone follow-up) versus technology-assisted (eg, apps or real-time telemonitoring), produce different effects on functional capacity and patient-centered outcomes.21 Therefore, this systematic review aimed to (1) compare HBCR versus CBCR on functional capacity, adherence, quality of life, and cardiovascular risk factors, and (2) evaluate whether HBCR delivery models influence these outcomes, to inform clinically effective and acceptable CR program design in home-based and digital care settings.
Materials and Methods
Study Design
This study followed the PRISMA 2020 guidelines for reporting systematic reviews.22 The comprehensive study protocol has been registered on the PROSPERO platform (registration number: CRD420251059819).
Search Strategy
Electronic databases, including PubMed, Cochrane Central Register of Controlled Trials (CENTRAL), and Scopus, were used to identify primary studies in any language. Data retrieval from the databases during June–August 2025 (strategy provided in Supplementary material, Table S1). In the article search process, we used three general concepts to identify medical subject headings (MeSH): “home-based therapy”, “center-based”, and “cardiac rehabilitation”. All keywords used the Boolean operator OR to identify the same concept, and AND to link concepts. Three reviewers (PK, NS, NF) independently searched each database. If there were differences of opinion, they were resolved through discussion with other reviewers (MRAAS, BBT, SS).
Eligibility Criteria
Three independent reviewers selected relevant articles in this review according to the PRISMA guidelines. The research question and eligibility criteria were developed using the PICOT framework (P: Population, I: Intervention, C: Comparison, O: Outcome, T: Study type). The population (P) of this study was adult patients (≥18 years) with cardiovascular disease, both in centers/hospitals and at home/in the community. Eligible participants were required to have a clinician-diagnosed cardiac condition consistent with guideline-indicated cardiac rehabilitation populations, including coronary artery disease/chronic coronary disease (eg, post–acute coronary syndrome or myocardial infarction, post–percutaneous coronary intervention or coronary artery bypass grafting, and/or stable angina), and selected heart failure populations (HFrEF/HFpEF) as defined by each trial’s inclusion criteria. Where applicable, diagnosis definitions (eg, LVEF thresholds, NYHA class, or procedure-based eligibility such as post–atrial fibrillation ablation) were extracted as reported by the original trials.
The intervention (I) was a home-based exercise rehabilitation program, either structured, supervised, or semi-supervised. The comparison (C) is a center-based exercise rehabilitation program, which is a structured program conducted in a hospital, clinic, or rehabilitation center under direct supervision. The primary outcomes were functional capacity measures (VO2peak) and the 6-minute walk distance (6MWD). In addition to statistical significance, we planned to interpret functional capacity findings against minimal clinically important difference (MCID) benchmarks to enhance clinical interpretability. Secondary outcomes include quality of life (QoL), adherence, and clinical risk. The type of studies (T) included were all randomized controlled trials (RCTs). Publications were excluded if the full text was unavailable, and studies that were not intervention studies (eg, reviews or meta-analyses) were excluded. To address clinical risk and comorbidity, we included trials recruiting clinically stable participants suitable for outpatient Phase II/III rehabilitation; trials exclusively enrolling unstable/high-risk patients requiring continuous monitoring or with exercise contraindications were excluded, consistent with established cardiac rehabilitation risk-stratification frameworks (eg, markedly reduced LVEF, complex ventricular arrhythmias, unstable angina, or recent decompensation). We also excluded populations with major mobility/movement disorders or severe comorbidities that precluded safe participation in exercise training (as defined in the original trials’ exclusion criteria). There were no publication year restrictions to ensure a comprehensive review of relevant studies.
Study Selection, Data Analysis, and Data Extraction
Three reviewers (PK, NS, NF) independently screened the studies according to the eligibility criteria. All the studies were downloaded from the databases, and duplicates were identified using Mendeley Reference Manager. Next, all studies were evaluated for relevance to the research topic based on their titles and abstracts. Then, after obtaining the full-text versions of all identified studies, one of the reviewers collected relevant full-text. The three reviewers also independently assessed the full text for inclusion using predefined criteria. In the final stage, all included studies will be evaluated using the Risk of Bias 2 (ROB2) tool to assess the quality of the resulting studies. The included studies will be extracted using Google Forms, and the results will be presented in a table that includes demographic characteristics and key results in the study. In addition, we extracted trial-reported diagnostic inclusion criteria and key exclusion criteria (including high-risk features and major comorbidities) to characterize the clinical risk profile of included participants. Any disagreements will be resolved through consensus with other reviewers (MRAAS, BBT, SS).
Risk of Bias Assessment
Two reviewers (PK and NS) independently assessed the risk of bias for the included studies. The included randomized controlled trials were appraised using the Cochrane Risk of Bias tool for randomized trials (RoB 2) across five domains: (1) bias arising from the randomization process, (2) bias due to deviations from intended interventions, (3) bias due to missing outcome data, (4) bias in measurement of the outcome, and (5) bias in selection of the reported result. For each domain, judgments followed RoB 2 guidance and signaling questions and were rated as “low risk of bias”, “some concerns”, or “high risk of bias”. An overall risk-of-bias judgment was derived according to the RoB 2 algorithm. Domain-level judgments were recorded in a structured spreadsheet and subsequently visualized using RobVis to generate both the traffic-light plot and the weighted summary plot. If any discrepancies are found, we will discuss them with all authors to reach a decision.
Data Synthesis
Given clinical and methodological heterogeneity across trials (eg, outcome definitions, measurement instruments, follow-up duration, intervention components, and reporting formats), we primarily conducted a narrative synthesis. For each outcome domain (functional capacity, adherence, health-related quality of life, and cardiovascular risk factors), we tabulated study characteristics, measurement tools, and between-group findings (HBCR vs CBCR), and summarized the direction of effects and statistical significance as reported. Trials were additionally grouped by HBCR delivery model (traditional vs technology-assisted) to compare patterns qualitatively. Where outcomes were sufficiently comparable and reported with available variance estimates, we performed random-effects meta-analyses (inverse-variance). Pooled effects are presented as mean differences (MDs) with 95% confidence intervals, and heterogeneity was assessed using I2 and the Chi2 test. Outcomes were not pooled when instruments, definitions, follow-up windows, or reporting were too heterogeneous or variance data were incomplete; these were summarized narratively and detailed in Supplementary Tables S2–S4. To support clinical interpretability of functional capacity, we applied published MCID benchmarks (VO2peak: 1 mL/kg/min; 6MWD: ~25 m) as interpretive thresholds.15,23 MCID appraisal used study-level mean change from baseline (post–baseline) when baseline and follow-up data were available; where SD of change was not reported, mean change was presented and missing variance was indicated. MCID values were used as benchmarks rather than definitive cut-points, and we did not estimate the proportion achieving MCID due to lack of individual-level data.
Results
Study Selection
A comprehensive search of various databases identified a large number of studies. Specifically, the initial search yielded 2510 studies. Of these, 873 studies were excluded due to duplication, leaving 1637 studies for screening. Fifty-eight studies were selected based on criteria outlined in their titles and abstracts. However, only 48 studies were assessed for eligibility after excluding 10 studies that could not be retrieved. Finally, 14 studies met the inclusion criteria and were included in the analysis (See Figure 1).
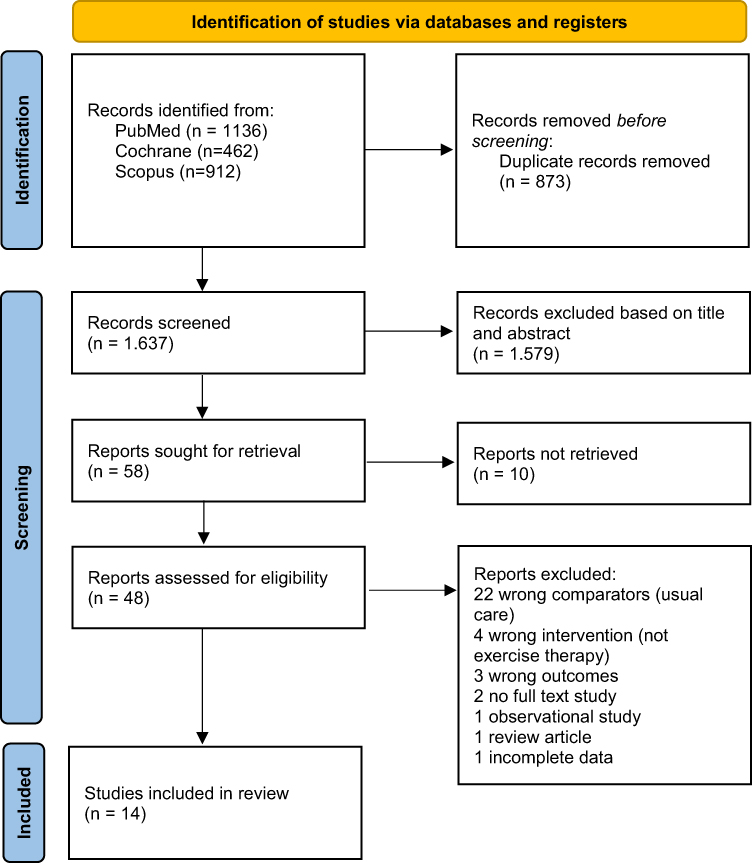 |
Figure 1 PRISMA flowchart of the study selection process. Notes: Adapted from Page MJ, McKenzie JE, Bossuyt PM et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021; 372:n71. |
Risk of Bias Assessment in Included Studies
Across the 14 included trials, the overall RoB 2 judgment was low risk in six studies,24–29 some concerns in seven studies,20,30–35 and high risk in one study36 (Figure 2). Overall, the evidence base was therefore dominated by trials rated as low risk or some concerns, with only a single study judged high risk. At the domain level, the most frequent source of “some concerns” was the randomization process (Domain 1), suggesting potential limitations in reporting or in the conduct of allocation procedures across several trials. Deviations from intended interventions (Domain 2) contributed additional concerns in a smaller subset of studies, whereas missing outcome data (Domain 3) was judged low risk in nearly all trials, with “some concerns” observed in only one study. Measurement of the outcome (Domain 4) was consistently rated low risk across all studies, suggesting outcome ascertainment was unlikely to be a major driver of bias. Concerns related to the selection of the reported result (Domain 5) were uncommon overall. However, this domain drove the single high-risk study, underscoring the need for cautious interpretation when conclusions rely heavily on studies with concerns in Domain 1 and/or Domain 5.
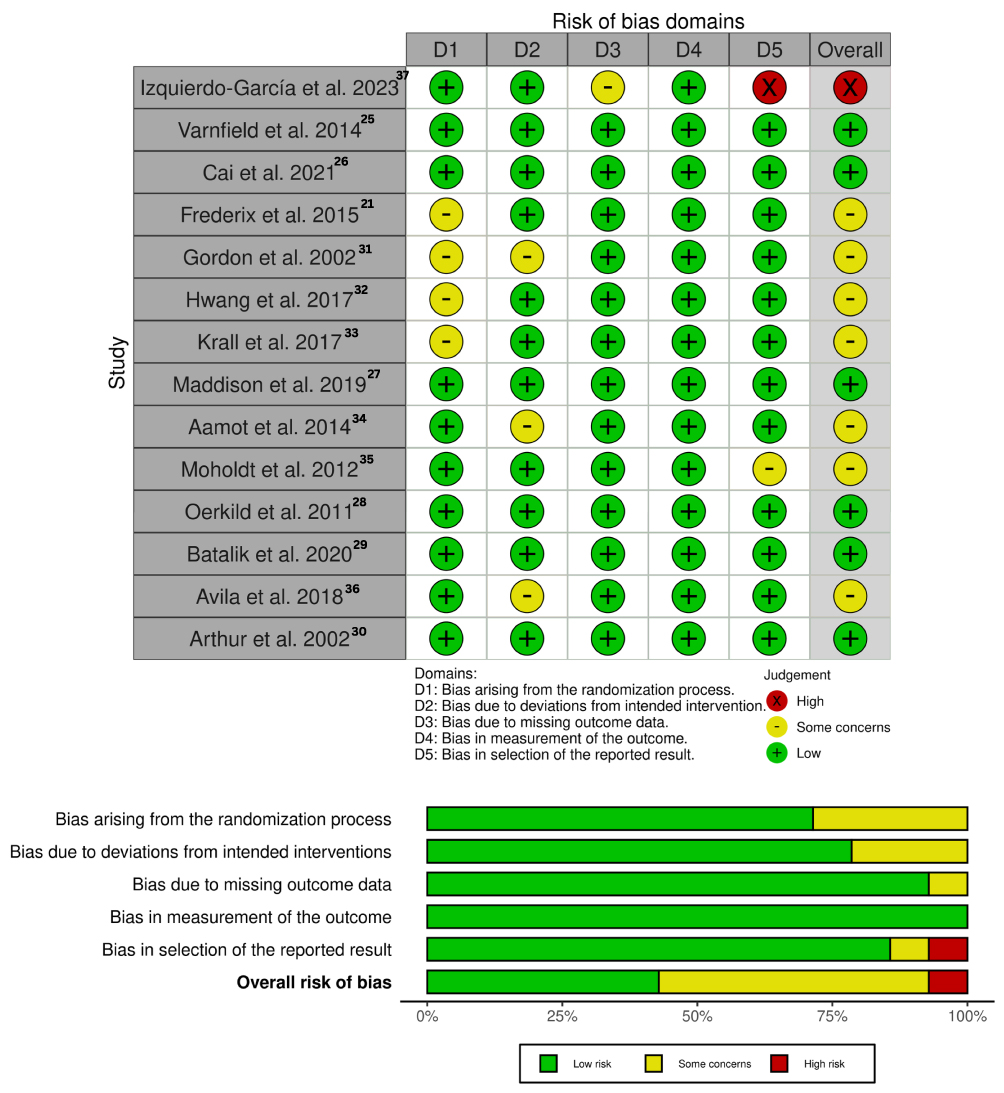 |
Figure 2 Summary of risk of bias. |
Characteristics of Included Studies
The included studies were conducted between 2002 and 2023 and comprised 14 randomized controlled trials, with sample sizes ranging from 22 to 242 participants (total n=1,249). The smallest trial was conducted by Izquierdo-García et al (n=22),36 while the largest was Arthur et al (n=242).29 Across trials, participant age generally reflected an older adult CR population: most studies enrolled participants with mean ages in the mid-50s to early-60s. Sex distribution was consistently male-predominant across the evidence base. Most trials enrolled predominantly men (often >75% male). All studies were conducted in high-resource settings, including Australia (n=2),24,31 Belgium (n=2),20,35 Norway (n=2),33,34 and each study (n=1) conducted in Canada,29 China,25 Czech Republic,28 Spain,36 Netherland,32 New Zealand,26 Denmark,27 and USA.30
In terms of clinical characteristics, most participants were patients with stable coronary artery disease, including post-myocardial infarction, post-CABG surgery, or percutaneous revascularization procedures, and patients with low to moderate risk acute coronary syndrome.24,26–30,32–34 Several studies specifically recruited heart failure patients with preserved ejection fraction,20,31,35,36 while others included patients after atrial fibrillation ablation.25 All studies compared home-based exercise therapy programs with phase II/III center-based cardiac rehabilitation, and generally reported that baseline characteristics between HBCR and CBCR groups were comparable in terms of age, gender, and cardiovascular diagnosis profile.20,24–29,31–36 The characteristics of this study are summarized in Table 1.
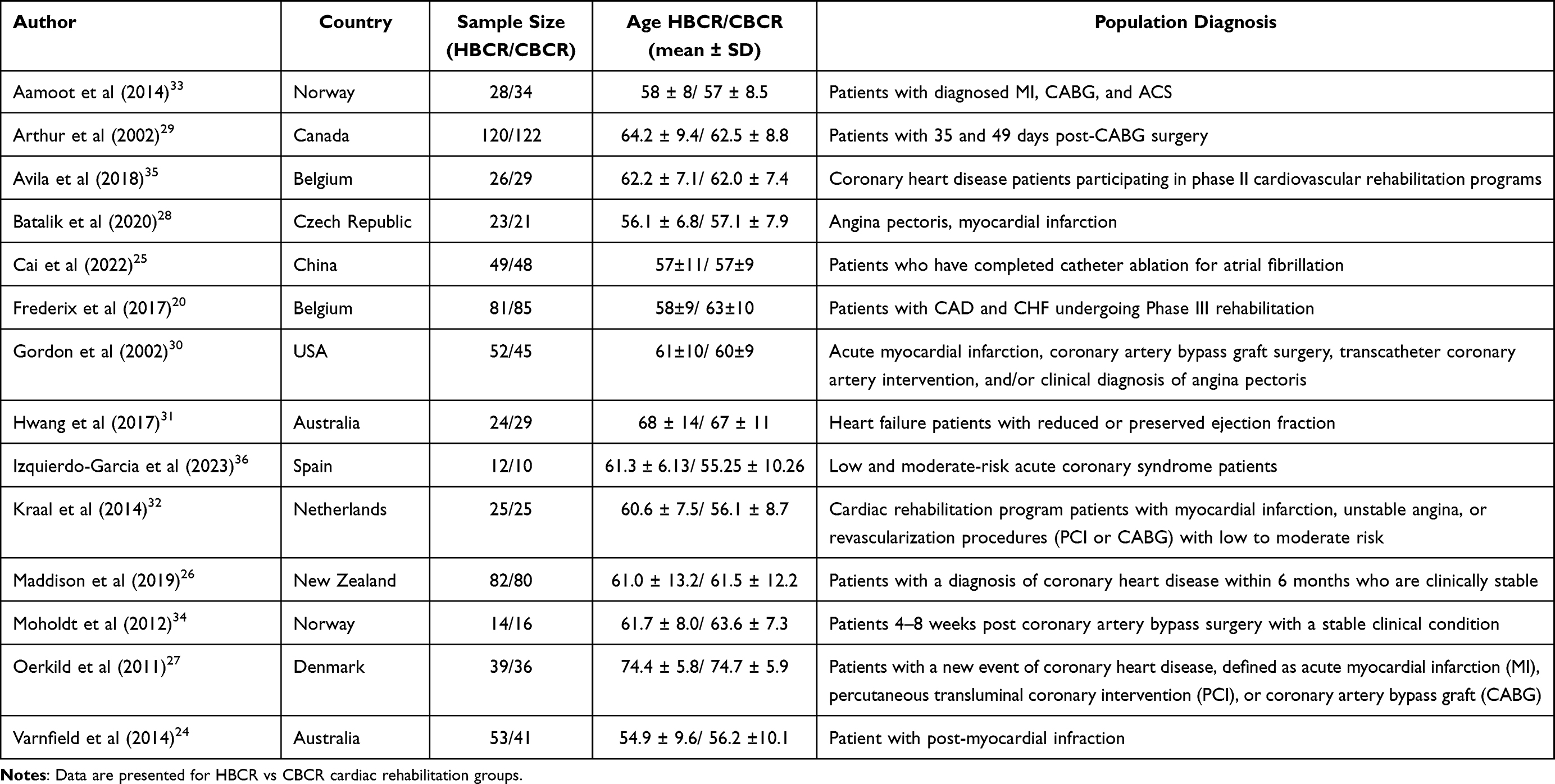 |
Table 1 Characteristics of Studies |
Analysis of Delivery Models in Home-Based Cardiac Rehabilitation
The experimental groups in the thirteen studies received HBCR as an intervention, while CBCR served as the control. Table 2 shows the content of the intervention model provided in each study. The core content of this intervention includes exercise dosage and various intervention models for administering HBCR. In general, the intervention is divided into two types: traditional and technology-assisted HBCR. Three studies revealed that traditional HBCR was administered by rehabilitation doctors who prescribed exercise doses to patients in terms of frequency, intensity, and type of exercise. Rehabilitation was then carried out at home and followed up by telephone by physiotherapists and rehabilitation officers. In contrast, the other ten studies used technology to conduct follow-ups, record physical progress, and guide exercise rehabilitation. For more details, see Table 2 and Figure 3.
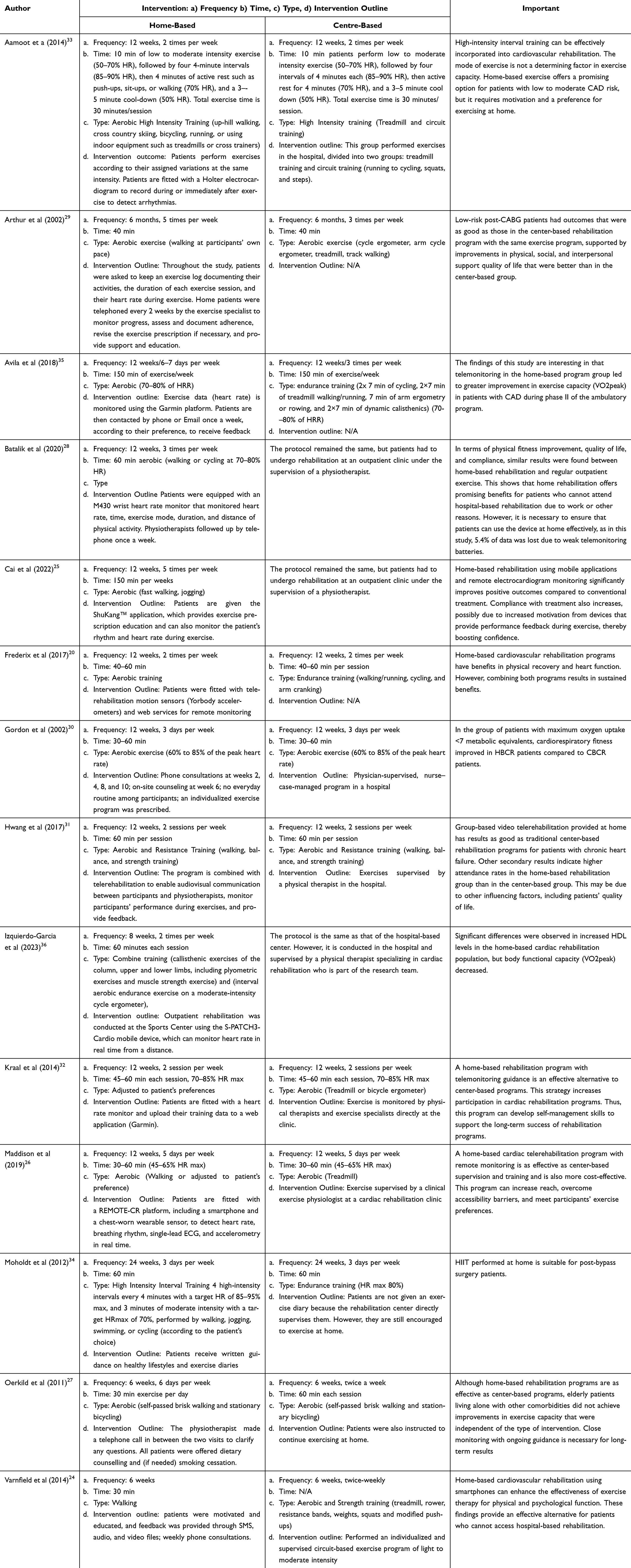 |
Table 2 Intervention Model |
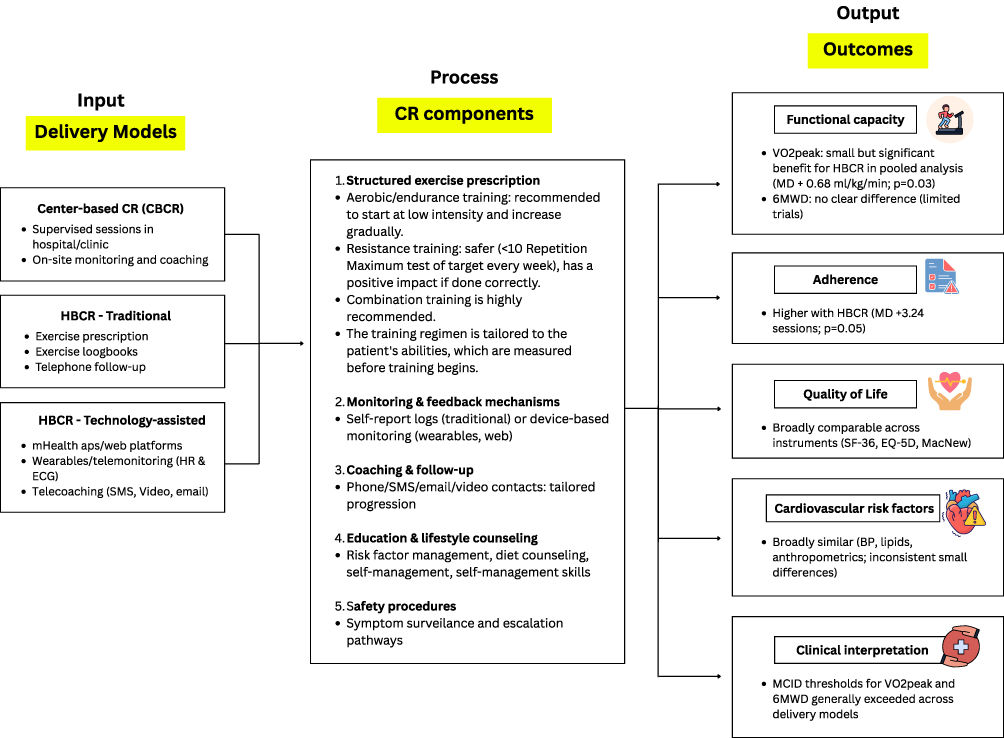 |
Figure 3 Logic model of delivery interventions, CR components, and outcomes. |
Theme I: Conventional HBCR Programs with Telephone and Logbook Support
Several trials featured relatively low-tech HBCR models that relied on written exercise prescriptions, heart rate targets, and self-reported exercise logs, combined with telephone follow-ups. The studies by Arthur et al and Gordon et al provided aerobic exercise five times per week for six months to post-CABG patients, with daily logbooks and weekly phone calls, resulting in equivalent physical capacity and quality-of-life outcomes, and even better results in some other domains compared to center-based rehabilitation.29,30 Including a group given high-intensity interval training (HIIT), it showed comparable functional capacity improvements between home- and center-based rehabilitation.33,34 Oerkild et al used a combination of walking exercises, exercise diaries, and phone calls, finding that the home-based program was not inferior to the center-based program in elderly patients despite comorbidities and more limited response capacity.27 This theme suggests that with systematic educational support and telephone follow-up, conventional home-based models can replicate the physiological benefits of center-based programs, particularly in low- to moderate-risk patients.27,29,33
Theme II: Web-Based and Platform-Supported Telerehabilitation
The use of web platforms and telemonitoring has been widely used for home-based cardiac rehabilitation programs. Avila et al used a heart-rate monitor connected to the Garmin platform, providing 150 minutes/week of exercise for 12 weeks.35 Frederix et al combined the Yorbody accelerometer with web services to monitor daily physical activity and structured exercise sessions, finding that web-based home-based programs had the same results as center-based programs.20 Another delivery model, telemonitoring with exercise data uploaded to a website application, has also been shown to maintain VO2peak and promote the development of long-term self-management skills.32 However, it should be noted that the use of telemonitoring requires reliable technology and accurate use to minimize data loss.28
Theme III: Smartphone Application and SMS-Based mHealth Models
Smartphone and SMS-based mHealth technology combines digital monitoring with promising multimodal education. Varnfield et al developed a home-based program that integrates smartphones via SMS, audio, and video, along with weekly telephone consultations, resulting in clinical and psychological improvements comparable to those of conventional rehabilitation.24 Cai et al designed a 12-week program using mobile applications and wearable devices to record activity and cardiovascular parameters, reporting increased patient confidence and engagement.25 The same system was given to patients with coronary heart disease, using the REMOTE-CR platform, which is a combination of a smartphone application and a multi-sensor chest patch (single-lead ECG, respiration, accelerometer), resulting in an improvement in exercise capacity comparable to center-based rehabilitation after 12 weeks of training.26 This pattern indicates a transition to an app-based cardiac telerehabilitation model, where supervision, goal setting, and feedback are transferred mainly to mobile devices, with less frequent but targeted clinician contact.24–26
Theme IV: Video-Based and Real-Time Sensor-Guided Telerehabilitation
Video-based supervision and real-time sensors are a home-based approach with the highest level of interaction. Hwang et al reported a 12-week group-based video telerehabilitation program with synchronous supervision by a physical therapist. This study found that home-based CR can improve functional capacity and quality of life comparable to in-person training in hospitals.31 Another study using heart rate monitoring devices that can send real-time data remotely during training sessions found that this approach improved VO2 peak and metabolic parameters, such as HDL.36 Other mHealth devices that combine ECG/accelerometer sensors with real-time feedback via an app can form a spectrum of sensor-guided telerehabilitation models that mimic the supervised training experience in a clinic.25,26 Overall, these models emphasize the integration of real-time monitoring, audiovisual feedback, and two-way interaction, which enable individualized exercise dosing, early detection of safety issues, and the potential for increased adherence in patients at higher risk or with intensive supervision needs.25,26,31,36
Analysis of Exercise Dose (FITT Principle) Between HBCR and CBCR Programs
In all included clinical trials, the prescribed exercise dose for the home-based group was deliberately adjusted to match that of the center-based cardiac rehabilitation (CR) group, based on the FITT principle (Frequency, Intensity, Time, Type). Most studies asked both groups to exercise 3 to 5 times per week for 6–24 weeks, with session durations of 30–60 minutes, and target intensities in the moderate to high range (eg, 45–85% HRmax or approximately 70–80% HRR, or RPE 11–15). In some clinical trials, the center-based group performed 2–3 supervised sessions per week. In contrast, the home-based group was instructed to perform the same number of structured sessions plus unsupervised walking or daily physical activity, so that the total weekly volume of the home-based group was sometimes slightly higher.20,24,26,28,32,35 Only a few studies allowed for a clearly lower frequency or duration in the home-based group due to practical limitations, but generally remained within the exercise dose range recommended by CR guidelines.27,29,33
In terms of intensity, rehabilitation centers use direct heart rate measurements and/or exercise test results (CPET/ETT) to adjust target zones during supervised sessions. In contrast, home-based programs use a combination of heart rate monitors, pedometers/accelerometers, and RPE scales to achieve similar intensities.20,24–26,28,31,32,35,36 In HIIT studies, the interval protocols used at home were identical to those given in the hospital (eg, 4×4 minutes of high-intensity with active intervals), so the main difference was only in the location and method of supervision.33,34 Several trials showed that telemonitoring and digital devices helped patients maintain the desired intensity zone at home, with HR/activity data reviewed periodically and prescriptions adjusted as needed.20,24–26,28,32
The Outcomes of Intervention in Cardiovascular Rehabilitation
Physical Outcome
Across the included trials, physical function outcomes were synthesized using random-effects meta-analysis. For VO2peak, 12 trials were pooled and showed a small but statistically significant difference favoring HBCR at follow-up (MD 0.68 mL·kg−1·min−1, 95% CI 0.06 to 1.29; p=0.03), with low heterogeneity (τ2=0.05; χ2=11.41, df=11, p=0.41; I2=4%), indicating largely consistent effects across studies. For 6-minute walk distance (6MWD), 2 trials contributed data and the pooled estimate showed no statistically significant between-group difference (MD −6.77 m, 95% CI −55.06 to 41.52; p=0.78), with moderate heterogeneity (χ2=2.58, df=1, p=0.11; I2=61%), reflecting variability between the small number of available studies. Individual trial estimates and study weights are presented in Figure 4.
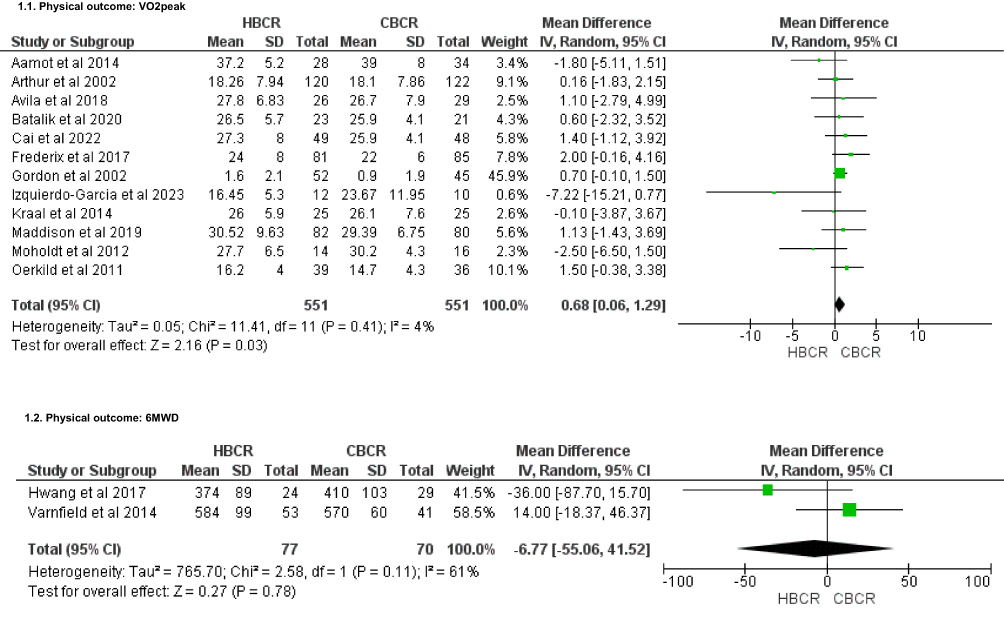 |
Figure 4 Forest plot of physical outcomes HBCR and CBCR. |
Adherence
Five trials were pooled to examine adherence using a random-effects model. Overall, adherence was higher in home-based CR than in centre-based CR, with a pooled mean difference of 3.24 sessions (95% CI −0.10 to 6.58; p=0.06). Between-study heterogeneity was substantial (τ2=9.87; χ2=13.39, df=4, p=0.01; I2=70%), indicating variability in effect magnitude across studies, although most individual estimates favored home-based programs (Figure 5).
 |
Figure 5 Forest plot of adherence outcomes HBCR and CBCR. |
Quality of Life
Nine trials reported health-related quality of life (HRQoL) using various generic and disease-specific instruments, including the SF-36, EQ-5D, and the MacNew Heart Disease questionnaire (Supplementary File: Table S3). Across these studies, between-group differences at follow-up were generally minor and did not consistently favour either HBCR or CBCR. Several trials reported slightly higher scores in one or more domains for the home-based group. For example, Arthur et al and Kraal et al observed numerically higher physical, social, and/or total MacNew scores in home-based participants. In contrast, Avila et al reported higher physical and social functioning scores in the home-based arm.29,32,35 In contrast, some domains or instruments slightly favoured centre-based rehabilitation, such as higher general health or mental health scores in the centre-based group in Avila et al35 marginally higher EQ-5D index values in Maddison et al and Varnfield et al,24,26 and small advantages in selected domains for centre-based participants in Aamot et al and Moholdt et al33,34 Because these differences were generally modest and inconsistent across domains and instruments, the evidence indicates that home-based CR yields HRQoL outcomes broadly comparable to those achieved with CBCR programs.
Cardiovascular Risk Factor
Seven trials reported a range of cardiovascular risk factor outcomes, including resting heart rate, blood pressure, anthropometric indices, carotid intima–media thickness, and lipid profiles (Supplementary File: Table S4). Across these studies, HBCR and CBCR showed broadly similar risk factor profiles at follow-up, with only minor, inconsistent differences between groups. Several trials reported modest advantages for home-based CR on selected parameters. For example, Avila et al found lower carotid intima-media thickness, body fat, and hip circumference in the HBCR with CBCR, while Aamot et al and Oerkild et al observed slightly lower resting heart rate and/or blood pressure values in home-based participants.27,33,35 Varnfield et al reported numerically lower total cholesterol, LDL cholesterol, and triglycerides, as well as a smaller abdominal circumference, in the home-based group.24 Conversely, other trials showed small advantages for CBCR in specific risk markers, such as lower systolic blood pressure and LDL cholesterol in Izquierdo-Garcia et al and Maddison et al, or higher HDL cholesterol in Moholdt et al and Varnfield et al.24,26,34,36 Given the heterogeneity of measures and the modest magnitude of between-group differences, the overall evidence indicates that both HBCR and CBCR achieve comparable control of major cardiovascular risk factors, with no consistent pattern indicating superiority of one setting over the other.
Discussion
This systematic review found a slight, significant difference in functional capacity improvement (VO2peak) between HBCR and CBCR (MD 0.68 mL·kg−1·min−1, 95% CI 0.06 to 1.29; p=0.03), whereas no between-setting difference was observed for 6MWD (MD −6.77 m, 95% CI −55.06 to 41.52; p=0.78). When placed in context, our findings are broadly consistent with the Cochrane evidence base, which has repeatedly concluded that home-based and centre-based CR yield similar outcomes for exercise capacity and other key endpoints up to 12 months, with no clear evidence of superiority for either setting.9,10,37 The small VO2peak advantage observed in our pooled analysis may differ from Cochrane’s “exercise capacity” synthesis for several reasons: Cochrane typically pools multiple exercise-capacity metrics using standardized mean differences across a broader set of comparisons, whereas our quantitative synthesis focused on trials reporting VO2peak in comparable units and timepoints. In addition, a larger proportion of newer HBCR trials incorporate technology-enabled monitoring and feedback, which may influence engagement and dose delivery, potentially contributing to small differences in fitness outcomes. This finding provides new insight as it contradicts with Cochrane previous studies that revealed comparable effects on VO2peak in both HBCR and CBCR groups.9,10 We hypothesize that this finding is consistent with greater adherence in the HBCR group than in the CBCR group (MD 3.24 sessions, 95% CI −0.10 to 6.58; p=0.06). The integration of home-based exercise rehabilitation with information technology has expanded the possibilities of HBCR, including wearable devices and cloud-based data delivery, which enable real-time monitoring of exercise data and provide exercise guidance.28,32,38–41 In this review, the studies included in the adherence assessment all used a telerehabilitation approach integrated into the HBCR program.25,26,28,31,32 It was found that rehabilitation integrated with innovative wearable devices has been shown to improve low adherence.42 Similar findings were obtained that the introduction of technologies such as virtual reality and augmented reality can bring virtual sports coaches into real environments to provide real-time movement instructions and feedback to improve adherence.43,44
Although not all HBCR studies improved functional capacity compared to CBCR (eg, Izquierdo-Garcia et al36 and Oerkild et al),27 it is important to note that we found no evidence of differences in effectiveness between HBCR delivery (Supplementary File: Figure S1). Conventional, telehealth, or hybrid delivery methods can effectively improve acceptance and adherence by allowing people to perform CR exercise in more accessible locations. However, the average change in VO2peak substantially exceeded the clinically important difference associated with a reduction in mortality risk (1 mL/kg/min).45,46 All exercise delivery models exceeded the minimum clinically important difference (MCID), except for one study with conventional telephone follow-up28 and one study with an HBCR group-based intervention36 which require further research (Supplementary File: Table S2). The small number of comparisons indicates that this should be interpreted with caution. However, comparable results across delivery methods suggest that the impact of accessibility barriers on CR participation rates may be being overcome.47
The HBCR program is implemented not only to promote exercise and encourage sustained adherence, but also to instill confidence and empower patients to manage their own cardiac rehabilitation.48 Thus, the CR program can support sustained physical, physiological, and psychological cardiac rehabilitation in the long term, resulting in improved quality of life.49 In principle, exercise CR can reduce oxidative stress, improve endothelial progenitor cell function, enhance ventricular remodeling, and regulate inflammation.50 This mechanism dilates the coronary arteries and forms collateral circulation, increases blood flow and myocardial energy supply by enlarging the lumen area of collateral vessels and increasing myocardial capillary density, thereby reducing risk factors such as improvements in systolic blood pressure, maximum heart rate, and lipid profile.11,51 This may also be because HBCR has a higher total weekly volume due to the flexibility of the exercise.52 However, the effectiveness and safety of using telerehabilitation need to be validated by doctors and professional rehabilitation practitioners for exercise prescriptions.53
Exercise intensity is a consideration when prescribing the exercises. The studies included in this research were 45–85% HRmax or approximately 70–80% HRR, or RPE 11–15, which, according to the guidelines of the European Association of Preventive Cardiology/European Society of Cardiology (EAPC/ESC). The American College of Sports Medicine (ACSM) includes the low- to high-intensity range.53 The ACSM states that strenuous exercise increases the risk of acute cardiac death and acute myocardial infarction in patients with atherosclerotic disease, especially in those who are not regularly active.54 Therefore, high-intensity exercise is indicated for asymptomatic, stable patients with low-risk revascularization of coronary artery disease who do not have residual high-risk coronary artery disease lesions or exercise-induced arrhythmias.40,55 However, this differs from high-intensity interval training (HIIT), which is known to increase peak oxygen uptake and 6MWD compared to moderate-intensity continuous training (MICT).37,56 However, these findings must be within the appropriate target range, where MICT must be performed at 55%–69% of maximum heart rate, oxygen uptake at 40%–59% of peak oxygen uptake, and rate of perceived exertion (RPE) between 11 and 13. During high-intensity interval training, heart rate should be 85%–95% of maximum heart rate, oxygen uptake should be 80%–90% of peak oxygen uptake, and RPE should be 15–18.37,57 Certainly, the exercise prescription must be adjusted to meet the progression requirements to enhance the patient’s exercise adaptation and help improve cardiorespiratory function, muscle strength, flexibility, and endurance, thereby improving overall fitness.33,38,41,58 Regardless of the type of exercise, it is a crucial stage of rehabilitation to improve cardiovascular health; however, a combination of aerobic exercise and muscle strengthening is more recommended to reduce the incidence of side effects and improve body composition, strength, and heart function.59
Success in CR programs is not determined solely by exercise prescriptions but also by other core components that are multidisciplinary and comprehensive, including patient assessment, physical activity counseling, diet and nutrition counseling, risk factor control, patient education, psychosocial management, and vocational advice.60 Our studies primarily involve the integration of CR programs with the use of technological tools such as telerehabilitation, telemonitoring, and telecoaching remotely. The use of telehealth in patient assessment and monitoring during CR programs is considered adequate because it includes digital health solutions, questionnaires, communication, psychosocial support, and even vital parameters measured by patients using sensors.61 However, there are CR components that still require face-to-face contact with health workers, such as blood tests and exercise tests, before patients are given the freedom to exercise at home according to the prescribed exercise regimen. In addition, the CR program must support long-term lifestyle changes.62 A long-term follow-up program on the FIT@Home CBA test in coronary heart disease patients found a decrease in physical activity after 4 years of cardiac rehabilitation in both the CBCR and HBCR programs. However, if a stronger focus is placed on behavioral change combined with longer monitoring, HBCR is actually more effective than CBCR.20,63,64 A Phase III CR trial showed that combining CBCR with HBCR using telerehabilitation for 9 months resulted in a greater increase in VO2 peak than CBCR alone.20 Similarly, virtual education in CR can improve patients’ understanding of their disease, increase self-confidence and self-management, facilitate behavioral change, and improve psychosocial health through family involvement in care.65
In addition to HBCR, delivered through an exercise program with remote monitoring, virtual reality (VR) technology has recently been introduced and has been shown to increase exercise capacity compared with the usual care group.66 Unlike HBCR, which can be carried out with any exercise according to the patient’s wishes and the prescribed exercise regimen, the use of VR in CR is generally packaged in the form of exergames or video games that require rigorous physical exercise.67 However, exergames have only been tested on two populations of cardiac patients (coronary artery bypass surgery and heart failure patients).68 Integrating them into HBCR programs poses serious challenges because they require a high level of technological expertise, even though they have been shown to increase energy expenditure, motor function, and well-being.69,70 To date, VR-based CR research has primarily been integrated into CBCR programs, so our study did not detect any effects of this intervention. In the future, the effects of VR-based CR on HBCR with CBCR should be explored, and the effectiveness of VR in improving cardiac function, quality of life, and patient compliance should be considered.66
Until now, it remains unclear which patients are optimal candidates for HBCR. A recent study shows that patients who are not recommended for HBCR include the elderly, those with low levels of education, those with lower exercise capacity, and those who have undergone coronary artery bypass surgery.71 Ideally, digital technology should be applicable and personalized according to the needs of each subgroup. However, it is important to note that exercise requirements need to be adjusted, so traditional exercise testing is still necessary, regardless of patient preferences and digital competence.72 For example, in CHF patients with lower exercise capacity, nutritional counseling should include advice on fluid and salt intake. Another obstacle is the cost of implementing HBCR.73 Even in developed countries such as those in Europe, reimbursement for telehealth HBCR interventions is not available due to the relatively high cost of the technology.74–76 However, there is ample research evidence that HBCR improves patient cost-efficiency and increases participation and control of cardiovascular risk factors, resulting in cost savings for society.77 Essentially, this redesign must actively involve patients and stakeholders (health workers, government support, and hospitals) in the development of behavioral change interventions.78 Thus, in the future, research on CR should not only focus on the effects of interventions, but also on how their implementation affects the quality of care services.
Strengths and Limitations
This review has several strengths. We included only randomised controlled trials directly comparing home- and centre-based CR, thereby reducing confounding and enhancing internal validity. We examined a broad range of clinically relevant outcomes, including functional capacity, adherence, HRQoL, and cardiovascular risk factors, and we conducted prespecified subgroup analyses by delivery model within HBCR. Nevertheless, several limitations should be acknowledged. There was important clinical and methodological heterogeneity across trials in programme duration, patient populations, and measurement instruments; accordingly, outcomes that were not sufficiently comparable were synthesised narratively rather than pooled, and the small number of trials contributing to some endpoints (particularly 6MWD and adherence) limited precision and power to detect small differences. Most studies had short- to medium-term follow-up, restricting inference regarding longer-term outcomes such as hospitalisation and mortality, consistent with gaps noted in prior evidence syntheses. In addition, key intervention descriptors, including exercise intensity progression and behavioural/core components of CR (eg, education, psychosocial support, risk-factor counselling) were inconsistently reported, precluding a more granular assessment of “dose–adherence” mechanisms and implementation fidelity. The evidence base was also predominantly male, limiting sex-specific inference and generalisability to women, who experience persistent disparities and distinct barriers to CR access and completion; future trials should prioritise sex-disaggregated reporting and delivery strategies tailored to women’s needs.79 Finally, few trials reported multivariable analyses to identify determinants of HBCR “success” (eg, predictors of adherence or functional response), so we could not synthesise patient- or system-level factors associated with better outcomes; addressing this gap will require adequately powered pragmatic trials with prespecified predictor/moderator analyses and standardised reporting.9
Conclusion
This systematic review summarizes that home-based cardiac rehabilitation (HBCR), delivered through both traditional and technology-assisted models, achieves functional and patient-centered outcomes that are broadly comparable to center-based cardiac rehabilitation (CBCR) across varied cardiac populations and program designs; pooled analyses showed a slight advantage for HBCR in VO2peak and modestly higher adherence, while 6-minute walk distance, health-related quality of life, and cardiovascular risk factors were generally similar between settings with minor and inconsistently directed differences. These findings support HBCR as a credible, scalable pathway to expand participation in evidence-based secondary prevention, particularly for patients facing travel, cost, scheduling, or psychosocial barriers to facility-based programs. Future research should shift from asking whether HBCR can match CBCR to determining which HBCR components drive benefit, for whom, and under what implementation conditions, through adequately powered pragmatic trials that directly compare delivery models (eg, low-tech vs platform-based vs real-time supervised telerehabilitation), include longer follow-up to assess durability and clinical events, and standardize reporting of exercise dose (FITT), intervention components, and adherence metrics. Studies should also pre-specify clinically meaningful thresholds (MCID) and responder analyses, consistently report change scores and variance to enable pooling, and integrate risk-of-bias considerations into interpretation, while addressing equity and access in low- and middle-income settings, evaluating cost-effectiveness and health-system capacity, and applying implementation science to challenges such as digital literacy, technology reliability, privacy, and sustainable staffing; harmonized core outcome sets spanning functional capacity, patient-reported outcomes, safety, and participation will further enable delivery-model-specific meta-analyses and better inform policy and program design at scale.
Acknowledgments
UNPAD funds this publication charge through the Indonesian Endowment Fund for Education (LPDP) on behalf of the Indonesian Ministry of Higher Education, Science and Technology, managed under the EQUITY program (Contract No. 4303/B3/DT.03.08/2025 and 3927/UN.6.RKT/HK.07.00/2025), and PMDSU Scholarship Batch VIII for PK (Contract No. 1662/UN6.3.1/PT/00.2025).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Stark BA, DeCleene NK, Desai EC, et al. Global, regional, and national burden of cardiovascular diseases and risk factors in 204 countries and territories, 1990-2023. JACC. 2025:S0735109725074285. doi:10.1016/j.jacc.2025.08.015.
2. Owen O, O’Carroll V. The effectiveness of cardiac telerehabilitation in comparison to centre-based cardiac rehabilitation programmes: a literature review. J Telemed Telecare. 2024;30(4):631–21. doi:10.1177/1357633X221085865
3. Ades PA, Keteyian SJ, Wright JS, et al. Increasing cardiac rehabilitation participation from 20% to 70%: a road map from the million hearts cardiac rehabilitation collaborative. Mayo Clin Proc. 2017;92(2):234–242. doi:10.1016/j.mayocp.2016.10.014
4. Thomas RJ, Beatty AL, Beckie TM, et al. Home-based cardiac rehabilitation: a scientific statement from the American Association of Cardiovascular and Pulmonary Rehabilitation, the American Heart Association, and the American College of Cardiology. Circulation. 2019;140(1). doi:10.1161/CIR.0000000000000663
5. Brown EC, Franklin BA, Regensteiner JG, Stewart KJ. Effects of single bout resistance exercise on glucose levels, insulin action, and cardiovascular risk in type 2 diabetes: a narrative review. J Diabetes Complications. 2020;34(8):107610. doi:10.1016/j.jdiacomp.2020.107610
6. Peters AE, Keeley EC. Trends and predictors of participation in cardiac rehabilitation following acute myocardial infarction: data from the behavioral risk factor surveillance system. J Am Heart Assoc. 2018;7(1):e007664. doi:10.1161/JAHA.117.007664
7. Sukul D, Seth M, Barnes GD, et al. Cardiac rehabilitation use after percutaneous coronary intervention. J Am Coll Cardiol. 2019;73(24):3148–3152. doi:10.1016/j.jacc.2019.03.515
8. Neubeck L, Freedman S, Briffa T, Bauman A, Redfern J. Four-year follow-up of the choice of health options in prevention of cardiovascular events randomized controlled trial. Eur J Cardiovasc Prev Rehabil. 2011;18(2):278–286. doi:10.1097/HJR.0b013e32833cca66
9. McDonagh ST, Dalal H, Moore S, et al. Home-based versus centre-based cardiac rehabilitation. cochrane heart group. Cochrane Database Syst Rev. 2023;2023(10). doi:10.1002/14651858.CD007130.pub5
10. Anderson L, Sharp GA, Norton RJ, et al. Home-based versus centre-based cardiac rehabilitation. cochrane heart group. Cochrane Database Syst Rev. 2017;2017(10). doi:10.1002/14651858.CD007130.pub4
11. Zhong W, Fu C, Xu L, et al. Effects of home-based cardiac telerehabilitation programs in patients undergoing percutaneous coronary intervention: a systematic review and meta-analysis. BMC Cardiovasc Disord. 2023;23(1):101. doi:10.1186/s12872-023-03120-2
12. Antoniou V, Davos CH, Kapreli E, Batalik L, Panagiotakos DB, Pepera G. Effectiveness of home-based cardiac rehabilitation, using wearable sensors, as a multicomponent, cutting-edge intervention: a systematic review and meta-analysis. J Clin Med. 2022;11(13):3772. doi:10.3390/jcm11133772
13. Li L, Ringeval M, Wagner G, Paré G, Ozemek C, Kitsiou S. Effectiveness of home-based cardiac rehabilitation interventions delivered via mHealth technologies: a systematic review and meta-analysis. Lancet Digit Health. 2025;7(4):e238–e254. doi:10.1016/j.landig.2025.01.011
14. Stefanakis M, Batalik L, Antoniou V, Pepera G. Safety of home-based cardiac rehabilitation: a systematic review. Heart Lung. 2022;55:117–126. doi:10.1016/j.hrtlng.2022.04.016
15. Tegegne TK, Rawstorn JC, Nourse RA, Kibret KT, Ahmed KY, Maddison R. Effects of exercise-based cardiac rehabilitation delivery modes on exercise capacity and health-related quality of life in heart failure: a systematic review and network meta-analysis. Open Heart. 2022;9(1):e001949. doi:10.1136/openhrt-2021-001949
16. Promwong W, Meenongwah J, Kenbubpha K, Suyasa IGPD. Effectiveness of home-based cardiac rehabilitation programs on health outcomes of persons with heart failure: an umbrella review. Belitung Nurs J. 2025;11(5):517–527. doi:10.33546/bnj.3994
17. He X, Wang J, Ye L, Xu L, Gao J. Effects of cardiac rehabilitation on cardiac function and cardiovascular adverse events in coronary heart disease patients following percutaneous coronary intervention: a systematic review and meta-analysis of randomized controlled trials. Rev Cardiovasc Med. 2025;26(9):39926. doi:10.31083/RCM39926
18. Pagliari C, Isernia S, Rapisarda L, et al. Different models of cardiac telerehabilitation for people with coronary artery disease: features and effectiveness: a systematic review and meta-analysis. J Clin Med. 2024;13(12):3396. doi:10.3390/jcm13123396
19. Brito J, Aguiar-Ricardo I, Alves Da Silva P, et al. Home-based cardiac rehabilitation - the real barriers of programs at distance. Eur J Prev Cardiol. 2021;28(Supplement_1):
20. Frederix I, Solmi F, Piepoli MF, Dendale P. Cardiac telerehabilitation: a novel cost-efficient care delivery strategy that can induce long-term health benefits. Eur J Prev Cardiol. 2017;24(16):1708–1717. doi:10.1177/2047487317732274
21. Van MRFR, Houben VJG, Rikken SAOF, Gómez-Doblas JJ, Lozano-Torres J, van ‘t Hof AWJ. Cardiac (tele)rehabilitation in routine clinical practice for patients with coronary artery disease: protocol of the REHAB + trial. Front Cardiovasc Med. 2024;11:1387148. doi:10.3389/fcvm.2024.1387148
22. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. doi:10.1136/bmj.n71
23. Gremeaux V, Troisgros O, Benaïm S, et al. Determining the minimal clinically important difference for the six-minute walk test and the 200-meter fast-walk test during cardiac rehabilitation program in coronary artery disease patients after acute coronary syndrome. Arch Phys Med Rehabil. 2011;92(4):611–619. doi:10.1016/j.apmr.2010.11.023
24. Varnfield M, Karunanithi M, Lee CK, et al. Smartphone-based home care model improved use of cardiac rehabilitation in postmyocardial infarction patients: results from a randomised controlled trial. Heart. 2014;100(22):1770–1779. doi:10.1136/heartjnl-2014-305783
25. Cai C, Bao Z, Wu N, et al. A novel model of home-based, patient-tailored and mobile application-guided cardiac telerehabilitation in patients with atrial fibrillation: a randomised controlled trial. Clin Rehabil. 2022;36(1):40–50. doi:10.1177/02692155211032372
26. Maddison R, Rawstorn JC, Stewart RAH, et al. Effects and costs of real-time cardiac telerehabilitation: randomised controlled non-inferiority trial. Heart. 2019;105(2):122–129. doi:10.1136/heartjnl-2018-313189
27. Oerkild B, Frederiksen M, Hansen JF, Simonsen L, Skovgaard LT, Prescott E. Home-based cardiac rehabilitation is as effective as centre-based cardiac rehabilitation among elderly with coronary heart disease: results from a randomised clinical trial. Age Ageing. 2011;40(1):78–85. doi:10.1093/ageing/afq122
28. Batalik L, Dosbaba F, Hartman M, Batalikova K, Spinar J. Benefits and effectiveness of using a wrist heart rate monitor as a telerehabilitation device in cardiac patients: a randomized controlled trial. Medicine (Baltimore). 2020;99(11):e19556. doi:10.1097/MD.0000000000019556
29. Arthur HM, Smith KM, Kodis J, Mckelvie R. A controlled trial of hospital versus home-based exercise in cardiac patients. Med Sci Sports Exerc. 2002;34(10):1544–1550. doi:10.1097/00005768-200210000-00003
30. Gordon NF, English CD, Contractor AS, et al. Effectiveness of three models for comprehensive cardiovascular disease risk reduction. Am J Cardiol. 2002;89(11):1263–1268. doi:10.1016/S0002-9149(02)02323-8
31. Hwang R, Bruning J, Morris NR, Mandrusiak A, Russell T. Home-based telerehabilitation is not inferior to a centre-based program in patients with chronic heart failure: a randomised trial. J Physiother. 2017;63(2):101–107. doi:10.1016/j.jphys.2017.02.017
32. Kraal JJ, Peek N, Van Den Akker-Van Marle ME, Kemps HM. Effects of home-based training with telemonitoring guidance in low to moderate risk patients entering cardiac rehabilitation: short-term results of the FIT@Home study. Eur J Prev Cardiol. 2014;21(2_suppl):26–31. doi:10.1177/2047487314552606
33. Aamot IL, Forbord SH, Gustad K, et al. Home-based versus hospital-based high-intensity interval training in cardiac rehabilitation: a randomized study. Eur J Prev Cardiol. 2014;21(9):1070–1078. doi:10.1177/2047487313488299
34. Moholdt T, Bekken Vold M, Grimsmo J, Slørdahl SA, Wisløff U. Home-based aerobic interval training improves peak oxygen uptake equal to residential cardiac rehabilitation: a randomized, controlled trial. PLoS One. 2012;7(7):e41199. doi:10.1371/journal.pone.0041199
35. Avila A, Claes J, Goetschalckx K, et al. Home-based rehabilitation with telemonitoring guidance for patients with coronary artery disease (short-term results of the TRiCH study): randomized controlled trial. J Med Internet Res. 2018;20(6):e225. doi:10.2196/jmir.9943
36. Izquierdo-García J, Arranz–Escudero A, Tello De Meneses R, et al. Efficacy of a cardiac rehabilitation program in a municipal sports center compared to the hospital program: randomized controlled trial eCARCEX. An Sist Sanit Navar. 2023;46(3):e1050. doi:10.23938/ASSN.1050
37. Taylor JL, Holland DJ, Keating SE, et al. Short-term and long-term feasibility, safety, and efficacy of high-intensity interval training in cardiac rehabilitation: the FITR heart study randomized clinical trial. JAMA Cardiol. 2020;5(12):1382. doi:10.1001/jamacardio.2020.3511
38. Ma J, Ge C, Shi Y, et al. Chinese home-based cardiac rehabilitation model delivered by smartphone interaction improves clinical outcomes in patients with coronary heart disease. Front Cardiovasc Med. 2021;8:731557. doi:10.3389/fcvm.2021.731557
39. Nkonde-Price C, Reynolds K, Najem M, et al. Comparison of home-based vs center-based cardiac rehabilitation in hospitalization, medication adherence, and risk factor control among patients with cardiovascular disease. JAMA Netw Open. 2022;5(8):e2228720. doi:10.1001/jamanetworkopen.2022.28720
40. Claes J, Cornelissen V, McDermott C, et al. PATHway-I: feasibility, acceptability and clinical effectiveness of a technology enabled cardiac rehabilitation platform. A randomized controlled trial. J Med Internet Res. doi:10.2196/14221
41. Song Y, Ren C, Liu P, Tao L, Zhao W, Gao W. Effect of smartphone-based telemonitored exercise rehabilitation among patients with coronary heart disease. J Cardiovasc Transl Res. 2020;13(4):659–667. doi:10.1007/s12265-019-09938-6
42. Zhao Y, Li J, Tao C, Ding R. Research hotspots and trends of cardiopulmonary exercise test: visualization analysis based on citespace. Med Nov Technol Devices. 2022;16:100191. doi:10.1016/j.medntd.2022.100191
43. Qian J, McDonough DJ, Gao Z. The effectiveness of virtual reality exercise on individual’s physiological, psychological and rehabilitative outcomes: a systematic review. Int J Environ Res Public Health. 2020;17(11):4133. doi:10.3390/ijerph17114133
44. Plante TG, Aldridge A, Bogden R, Hanelin C. Might virtual reality promote the mood benefits of exercise? Comput Hum Behav. 2003;19(4):495–509. doi:10.1016/S0747-5632(02)00074-2
45. Keteyian SJ, Brawner CA, Ehrman JK, Ivanhoe R, Boehmer JP, Abraham WT. Reproducibility of peak oxygen uptake and other cardiopulmonary exercise parameters. Chest. 2010;138(4):950–955. doi:10.1378/chest.09-2624
46. Corrà U, Mezzani A, Bosimini E, Giannuzzi P. Prognostic value of time-related changes of cardiopulmonary exercise testing indices in stable chronic heart failure: a pragmatic and operative scheme. Eur J Cardiovasc Prev Rehabil. 2006;13(2):186–192. doi:10.1097/01.hjr.0000189807.22224.54
47. Bakhshayeh S, Sarbaz M, Kimiafar K, Vakilian F, Eslami S. Barriers to participation in center-based cardiac rehabilitation programs and patients’ attitude toward home-based cardiac rehabilitation programs. Physiother Theory Pract. 2021;37(1):158–168. doi:10.1080/09593985.2019.1620388
48. Saensoda S, Pokpalagon P, Chaiviboontham S. The effects of a home-based cardiac rehabilitation program via the line application on functional capacity and quality of life among open-heart surgery patients: a quasi-experimental study. Healthcare. 2025;13(9):1051. doi:10.3390/healthcare13091051
49. Zheng Y, Zhou LF, Qin SW, Guo J, Qin BY. The impact of home cardiac rehabilitation on quality of life and psychological well-being in patients with coronary heart disease: a randomized controlled study. Med Sci Monit Int Med J Exp Clin Res. 2024;30e942803. doi:10.12659/MSM.942803
50. Fiuza-Luces C, Santos-Lozano A, Joyner M, et al. Exercise benefits in cardiovascular disease: beyond attenuation of traditional risk factors. Nat Rev Cardiol. 2018;15(12):731–743. doi:10.1038/s41569-018-0065-1
51. Hu Y, Ding K, Wu G, Li X, Li J, Shang Z. The effect of technology-based home cardiac rehabilitation on risk factor modifications in coronary heart disease patients. a systematic review and meta-Analysis. Rev Cardiovasc Med. 2024;25(2):59. doi:10.31083/j.rcm2502059
52. Bravo-Escobar R, González-Represas A, Gómez-González AM, et al. Effectiveness and safety of a home-based cardiac rehabilitation programme of mixed surveillance in patients with ischemic heart disease at moderate cardiovascular risk: a randomised, controlled clinical trial. BMC Cardiovasc Disord. 2017;17(1):66. doi:10.1186/s12872-017-0499-0
53. Xue D, Yu Z, Jianchao L, et al. Effectiveness, safety and adherence of home-based exercise rehabilitation in patients with coronary heart disease patients: a systematic review. Med Nov Technol Devices. 2025;26:100361. doi:10.1016/j.medntd.2025.100361
54. Thompson PD, Franklin BA, Balady GJ, et al. In Collaboration With the American College of Sports Medicine. Exercise and acute cardiovascular events: placing the risks into perspective: a scientific statement from the American Heart Association Council on Nutrition, Physical Activity, and Metabolism and the Council on Clinical Cardiology. Circulation. 2007;115(17):2358–2368. doi:10.1161/CIRCULATIONAHA.107.181485.
55. Hansen D, Abreu A, Ambrosetti M, et al. Exercise intensity assessment and prescription in cardiovascular rehabilitation and beyond: why and how: a position statement from the secondary prevention and rehabilitation section of the european association of preventive cardiology. Eur J Prev Cardiol. 2022;29(1):230–245. doi:10.1093/eurjpc/zwab007
56. Terada T, Cotie LM, Tulloch H, et al. Sustained effects of different exercise modalities on physical and mental health in patients with coronary artery disease: a randomized clinical trial. Can J Cardiol. 2022;38(8):1235–1243. doi:10.1016/j.cjca.2022.03.017
57. Pattyn N, Beulque R, Cornelissen V. Aerobic interval vs. continuous training in patients with coronary artery disease or heart failure: an updated systematic review and meta-analysis with a focus on secondary outcomes. Sports Med. 2018;48(5):1189–1205. doi:10.1007/s40279-018-0885-5
58. Bushman BA. Developing the P (for Progression) in a FITT-VP Exercise Prescription. ACSMS Health Fit J. 2018;22(3):6–9. doi:10.1249/FIT.0000000000000378
59. Marzolini S, Oh PI, Brooks D. Effect of combined aerobic and resistance training versus aerobic training alone in individuals with coronary artery disease: a meta-analysis. Eur J Prev Cardiol. 2012;19(1):81–94. doi:10.1177/1741826710393197
60. Ambrosetti M, Abreu A, Corrà U, et al. Secondary prevention through comprehensive cardiovascular rehabilitation: from knowledge to implementation. 2020 update. A position paper from the secondary prevention and rehabilitation section of the european association of preventive cardiology. Eur J Prev Cardiol. 2021;28(5):460–495. doi:10.1177/2047487320913379
61. Scherrenberg M, Wilhelm M, Hansen D, et al. The future is now: a call for action for cardiac telerehabilitation in the COVID-19 pandemic from the secondary prevention and rehabilitation section of the European Association of Preventive Cardiology. Eur J Prev Cardiol. 2021;28(5):524–540. doi:10.1177/2047487320939671
62. Bock BC, Carmona-Barros RE, Esler JL, Tilkemeier PL. Program participation and physical activity maintenance after cardiac rehabilitation. Behav Modif. 2003;27(1):37–53. doi:10.1177/0145445502238692
63. Claes J, Buys R, Avila A, Cornelis N, Goetschalckx K, Cornelissen VA. Lifelong changes in physical activity behaviour through phase II cardiac rehabilitation? Still steps to take! Eur J Prev Cardiol. 2021;28(7):e17–e19. doi:10.1177/2047487320929451
64. Lunde P, Bye A, Bergland A, Grimsmo J, Jarstad E, Nilsson BB. Long-term follow-up with a smartphone application improves exercise capacity post cardiac rehabilitation: a randomized controlled trial. Eur J Prev Cardiol. 2020;27(16):1782–1792. doi:10.1177/2047487320905717
65. Kaihara T, Falter M, Scherrenberg M, et al. The impact of dietary education and counselling with a smartphone application on secondary prevention of coronary artery disease: a randomised controlled study (the TeleDiet study). Digit Health. 2023;9:20552076231164101. doi:10.1177/20552076231164101
66. Zhang M, Liu S, Xiong X, et al. Effectiveness of virtual reality in cardiac rehabilitation patients for exercise capacity and negative emotions: a systematic review and meta-analysis. Medicine. 2024;103(49):e40812. doi:10.1097/MD.0000000000040812
67. Gao Z, Pope Z, Lee JE, et al. Impact of exergaming on young children’s school day energy expenditure and moderate-to-vigorous physical activity levels. J Sport Health Sci. 2017;6(1):11–16. doi:10.1016/j.jshs.2016.11.008
68. Jaarsma T, Klompstra L, Ben Gal T, et al. Effects of exergaming on exercise capacity in patients with heart failure: results of an international multicentre randomized controlled trial. Eur J Heart Fail. 2021;23(1):114–124. doi:10.1002/ejhf.1754
69. Verheijden Klompstra L, Jaarsma T, Strömberg A. Exergaming in older adults: a scoping review and implementation potential for patients with heart failure. Eur J Cardiovasc Nurs. 2014;13(5):388–398. doi:10.1177/1474515113512203
70. Cacciata M, Stromberg A, Lee JA, et al. Effect of exergaming on health-related quality of life in older adults: a systematic review. Int J Nurs Stud. 2019;93:30–40. doi:10.1016/j.ijnurstu.2019.01.010
71. Brouwers RWM, Brini A, Kuijpers RWFH, Kraal JJ, Kemps HMC. Predictors of non-participation in a cardiac telerehabilitation programme: a prospective analysis. Eur Heart J - Digit Health. 2022;3(1):81–89. doi:10.1093/ehjdh/ztab105
72. Brouwers RWM, Scherrenberg M, Kemps HMC, Dendale P, Snoek JA. Cardiac telerehabilitation: current status and future perspectives. Neth Heart J Mon J Neth Soc Cardiol Neth Heart Found. 2024;32(1):31–37. doi:10.1007/s12471-023-01833-9
73. Frederix I, Caiani EG, Dendale P, et al. ESC e-cardiology working group position paper: overcoming challenges in digital health implementation in cardiovascular medicine. Eur J Prev Cardiol. 2019;26(11):1166–1177. doi:10.1177/2047487319832394
74. Brouwers RWM, Van Der Poort EKJ, Kemps HMC, Van Den Akker-van Marle ME, Kraal JJ. Cost-effectiveness of cardiac telerehabilitation with relapse prevention for the treatment of patients with coronary artery disease in the Netherlands. JAMA Netw Open. 2021;4(12):e2136652. doi:10.1001/jamanetworkopen.2021.36652
75. Shields GE, Wells A, Doherty P, Heagerty A, Buck D, Davies LM. Cost-effectiveness of cardiac rehabilitation: a systematic review. Heart. 2018;104(17):1403–1410. doi:10.1136/heartjnl-2017-312809
76. Batalik L, Filakova K, Sladeckova M, Dosbaba F, Su J, Pepera G. The cost-effectiveness of exercise-based cardiac telerehabilitation intervention: a systematic review. Eur J Phys Rehabil Med. 2023;59(2). doi:10.23736/S1973-9087.23.07773-0
77. Frederix I, Vandijck D, Hens N, De sutter J, Dendale P. Economic and social impact of increased cardiac rehabilitation uptake and cardiac telerehabilitation in Belgium – a cost–benefit analysis. Acta Cardiol. 2018;73(3):222–229. doi:10.1080/00015385.2017.1361892
78. Kok G, Gottlieb NH, Peters GJY, et al. A taxonomy of behaviour change methods: an Intervention Mapping approach. Health Psychol Rev. 2016;10(3):297–312. doi:10.1080/17437199.2015.1077155
79. Coutinho T, Khadanga S, Adedinsewo D, et al. Cardiac rehabilitation in women: a scientific statement from the American Heart Association. Circulation. 2025;152(19). doi:10.1161/CIR.0000000000001379
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.