Back to Journals » Infection and Drug Resistance » Volume 19
Comparative Study of Confirmed versus Suspected Cases of Vibrio vulnificus Infection in Chaoshan District, Guangdong, China
Authors Liu YH, Fang SR, Chen W, Wu YF, Liu DK, Li T
Received 30 March 2026
Accepted for publication 19 May 2026
Published 26 May 2026 Volume 2026:19 613123
DOI https://doi.org/10.2147/IDR.S613123
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hazrat Bilal
Yu-Hua Liu,1 Shi-Rong Fang,1 Wen Chen,2 Yin-Feng Wu,1 De-Kun Liu,3 Tao Li1
1Department of Infectious Diseases, the First Affiliated Hospital of Shantou University Medical College, Shantou, 515041, People’s Republic of China; 2Department of Burns and Plastic Surgery, the First Affiliated Hospital of Shantou University Medical College, Shantou, 515041, People’s Republic of China; 3Department of Anesthesiology, the First Affiliated Hospital of Shantou University Medical College, Shantou, 515041, People’s Republic of China
Correspondence: Tao Li, Department of Infectious Diseases, The First Affiliated Hospital of Shantou University Medical College, No. 57 Changping Road, Shantou, 515041, People’s Republic of China, Tel +86 13502952306, Fax +86 754 88905225, Email [email protected] De-Kun Liu, Department of Anesthesiology, the First Affiliated Hospital of Shantou University Medical College, No. 57 Changping Road, Shantou, 515041, People’s Republic of China, Tel +86 15018802292, Fax +86 754 88905225, Email [email protected]
Objective: To compare the epidemiological, clinical, and laboratory data of patients with confirmed and suspected Vibrio vulnificus infection in Chaoshan District, Guangdong.
Methods: This retrospective study analyzed 25 confirmed cases and 23 suspected cases of V. vulnificus infection at the First Affiliated Hospital of Shantou University Medical College from January 2014 to December 2025. A confirmed case was defined by the presence of a positive result from culture and/or mNGS and a suspected case by the experience of a clear marine trauma followed by rapidly progressive soft tissue manifestations, but without etiological confirmation of V. vulnificus infection after exclusion of other infectious etiologies. The epidemiological history, early clinical manifestations, routine blood parameters, and in-hospital outcomes of the two groups were compared.
Results: The confirmed group had a greater severity of soft tissue infection (84.0% vs 26.0%, P< 0.01) and more involved sites (88.0% vs 47.8%, P< 0.01). The laboratory data indicated the confirmed group had more abnormalities in markers of tissue injury (creatinine kinase, lactate dehydrogenase), coagulation function (platelets, prothrombin time, international normalized ratio), liver function (aspartate transaminase, total bilirubin), renal function (serum creatinine), and lipid and nutritional markers (all P< 0.05). The confirmed group also had significantly higher rates of in-hospital mortality (32.0% vs 0%), multi-organ dysfunction syndrome (36.0% vs 0%), and surgical intervention (60.0% vs 30.4%), and a greater economic burden (all P< 0.001).
Conclusion: There are significant differences in the early clinical manifestations, routine blood parameters, and in-hospital outcomes for patients with confirmed and suspected V. vulnificus infection.
Keywords: Vibrio vulnificus, soft tissue infection, suspected case, metagenomic next-generation sequencing
Introduction
Vibrio vulnificus infection is an acute and severe disease caused by infection with V. vulnificus, a Gram-negative bacterium that occurs in marine environments. Patients with a V. vulnificus infection that has progressed to V. vulnificus-necrotizing soft tissue infection (Vv-NSTI), have a mortality rate of about 50% and their care is associated with significant public health costs.1 V. vulnificus infection is more common in individuals with underlying health conditions, such as chronic liver disease, diabetes, or an immunocompromised status. Globally, over 95% of fatal V. vulnificus infections occur in subtropical regions, including the Chaoshan region of Guangdong, China. V. vulnificus infections show a clear seasonal peak from March to November, particularly in the warm summer months when seawater temperatures rise and seafood consumption increases. Recent regional evidence from Asia quantified this burden. In particular, a 2024 systematic review and meta-analysis reported a 10% prevalence of seafood-borne V. vulnificus, with oysters as a major source,2 and another 2024 meta-analysis reported concerning patterns of antimicrobial resistance among Asian seafood isolates.3 Furthermore, a 2025 South Korean study highlighted the substantial health and economic impact of infections associated with raw oyster consumption.4
Early identification and timely intervention by a multidisciplinary treatment (MDT) team are critical to the survival of these patients. V. vulnificus infection is often diagnosed in individuals with a history of seafood-related puncture or seawater exposure through a wound. These patients develop rapidly progressing skin redness, swelling, pain, and necrotizing soft tissue infection (NSTI) of the extremities.5 Microbial culture is the gold standard for the etiological diagnosis of V. vulnificus infection. However, traditional culture methods are time-consuming, and the overall rate of positive culture in patients with confirmed infection is approximately 30% to 40%.6 Metagenomic next-generation sequencing (mNGS) has become a valuable adjunctive tool for the identification of infectious pathogens.7 The increasing use of mNGS may partially overcome the limitation of the low rate of culture positivity, but its role in distinguishing confirmed from suspected V. vulnificus infections in routine practice remains unclear.
No studies have yet compared patients who have confirmed V. vulnificus infection with those who have suspected V. vulnificus infection. In clinical practice, many patients are managed as having suspected V. vulnificus infection without microbiological confirmation, yet it is unclear whether their early clinical features and prognoses differ from those of confirmed cases. In this study, we define confirmed cases as those with microbiological evidence of V. vulnificus (culture and/or mNGS), and suspected cases as those with epidemiological exposure and typical soft tissue manifestations but no etiological confirmation. This retrospective study compared the epidemiological history, early clinical symptoms and key laboratory parameters (within 6 h of emergency department presentation or admission), treatment measures, and clinical outcomes of groups with confirmed and suspected V. vulnificus infection. We aim to identify clinical and laboratory indicators associated with confirmed V. vulnificus infection and poor outcomes to enable the earlier recognition and risk stratification of high-risk patients.
Materials and Methods
Study Subjects
This retrospective comparative study enrolled patients with confirmed trauma-related infection who were hospitalized at the First Affiliated Hospital of Shantou University Medical College (Guangdong, China) between January 2014 and December 2025. The inclusion criteria for the confirmed V. vulnificus infection group (n = 25) were: (1) marine trauma within 7 days before symptom onset; (2) rapidly progressive soft tissue manifestations (eg, erythema, swelling, bullae, NSTI); and (3) a positive bacterial culture or mNGS result from wound tissue or blood. The inclusion criteria for the suspected V. vulnificus infection group (n = 23) were: (1) marine trauma within 7 days before symptom onset; (2) rapidly progressive soft tissue manifestations as described above; (3) no etiological confirmation of V. vulnificus; and (4) exclusion of other infectious etiologies (eg, Aeromonas, Streptococcus, Staphylococcus, V. alginolyticus) based on routine culture or mNGS when available. The exclusion criteria for both groups were: (1) age <16 years; (2) chronic soft tissue infection or pressure ulcer prior to trauma; (3) incomplete or missing medical records affecting outcome assessment; or (4) transfer from another hospital with initiation of antibiotic therapy >24 h before admission.
This study was approved by the Ethics Committee of the First Affiliated Hospital of Shantou University Medical College (Approval No. B-2026-052) and adhered to the principles outlined in the Declaration of Helsinki. Written informed consent was waived due to the retrospective nature of the study. Patient data were anonymized and kept confidential in accordance with ethical guidelines.
Medical records were reviewed, and clinical information on demographics, epidemiology, physical examination findings, presenting symptoms, laboratory parameters, antibiotics, surgical treatment, and outcomes were analyzed.
Outcome Definitions
The primary outcome was the incidence of multiple organ dysfunction syndrome (MODS), defined as a total Sequential Organ Failure Assessment (SOFA) score exceeding 5 at any time within the first 7 days after admission. The secondary outcomes were in-hospital mortality, length of hospital stay, and economic burden. Economic burden was defined as the total direct hospitalization costs (in Chinese Yuan, RMB) that were billed to the patient, including medication, laboratory tests, imaging, surgical procedures, and intensive care unit fees. Indirect costs, such as lost productivity or post-discharge rehabilitation, were excluded.
Statistical Analyses
SPSS software (version 25.0) was used for statistical analysis. Continuous variables were first tested for normality. Normally distributed data are presented as mean ± standard deviation (mean ± SD), and non-normally distributed data as median with interquartile range (M [IQR]). For baseline comparisons of the two groups, an independent sample t-test was applied when the data in both groups were normally distributed and the variances were homogeneous; otherwise, the Wilcoxon rank-sum test was applied. Categorical variables are presented as frequencies and percentages, and were analyzed using the Pearson chi-square test or Fisher’s exact test (for small sample sizes). A two-tailed α of 0.05 was considered statistically significant.
Results
Basic Demographic Characteristics, Epidemiology, and Early Clinical Manifestations
All confirmed cases and suspected cases were admitted between March 2014 and November 2025 and were diagnosed with trauma-related infection. There were 25 cases with microbiologically confirmed V. vulnificus infection, and 23 controls with suspected but not confirmed V. vulnificus infection (Table 1). In the confirmed cases, the median age was 67.0 years (IQR:49.5, 75.5), 96.0% (24/25) were male, 72% (18/25) had a history of marine trauma (eg, fish stabs, shrimp stabs, crab pincer injuries), 8.0% (2/25) had a wound exposed to seafood or seawater, and the remaining 20.0% (5/25) had no clear evidence of marine trauma. In the control group, the median age was 60.0 years (IQR:50.0, 70.0), 78.3% (18/23) were male, and all patients had a history of marine trauma (including fish stabs, shrimp stabs, crab pincer injuries, and fish hook wounds). The two groups had no significant differences in age, sex, or epidemiological characteristics (P > 0.05). Analysis of early clinical manifestations (within 6 h of emergency department presentation or admission) indicated the confirmed cases had greater percentages of patients with of severe soft tissue infection (84.0% vs 26.0%, P < 0.01) and patients with 2 or more involved sites (88.0% vs 47.8%, P < 0.01).
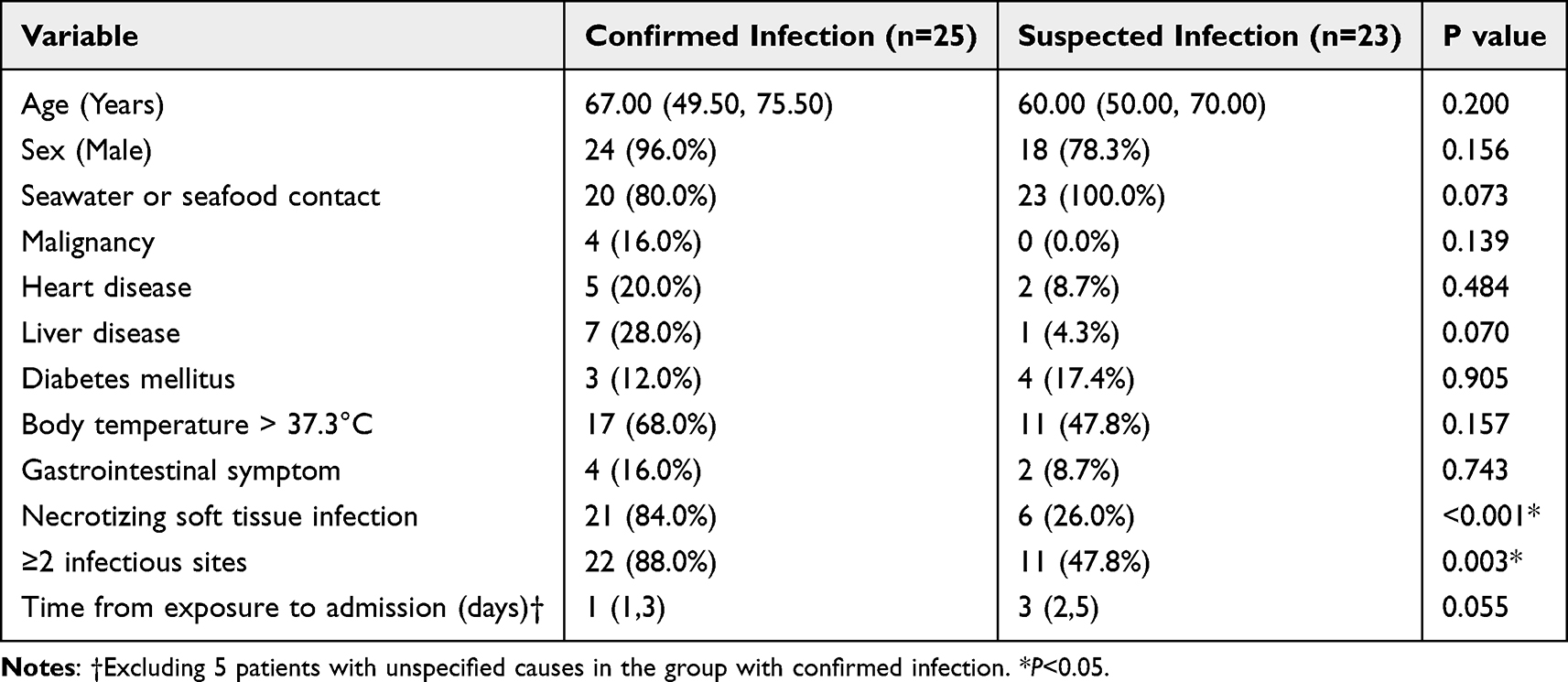 |
Table 1 Baseline Demographic and Clinical Characteristics of Patients with Confirmed and Suspected Vibrio vulnificus Infection |
Key Laboratory Parameters
We also compared the baseline laboratory findings of the two groups, which were recorded at admission (Table 2). These groups had no significant differences in the white blood cell count (WBC), percentage of neutrophils (NE%), C reactive protein (CRP), sodium (Na), glucose (Glu), or triglycerides (TG). In contrast, the confirmed group had clinical parameters indicative of more severe infection and multi-organ involvement. Specifically, the markers of tissue injury (creatinine kinase [CK], lactate dehydrogenase [LDH]), coagulation (platelets [PLT], prothrombin time [PT], international normalized ratio [INR]), liver function (aspartate aminotransferase [AST], total bilirubin [Tbil]), and renal function (serum creatinine [Cr]) were worse in the confirmed cases (all P < 0.05). The lipid profile (high-density lipoprotein [HDL], low-density lipoprotein [LDL], total cholesterol [TC]) and nutritional markers (total protein [TP], albumin [Alb]) were also lower in the confirmed cases (all P < 0.05). These results indicate the confirmed cases had a more severe disease state.
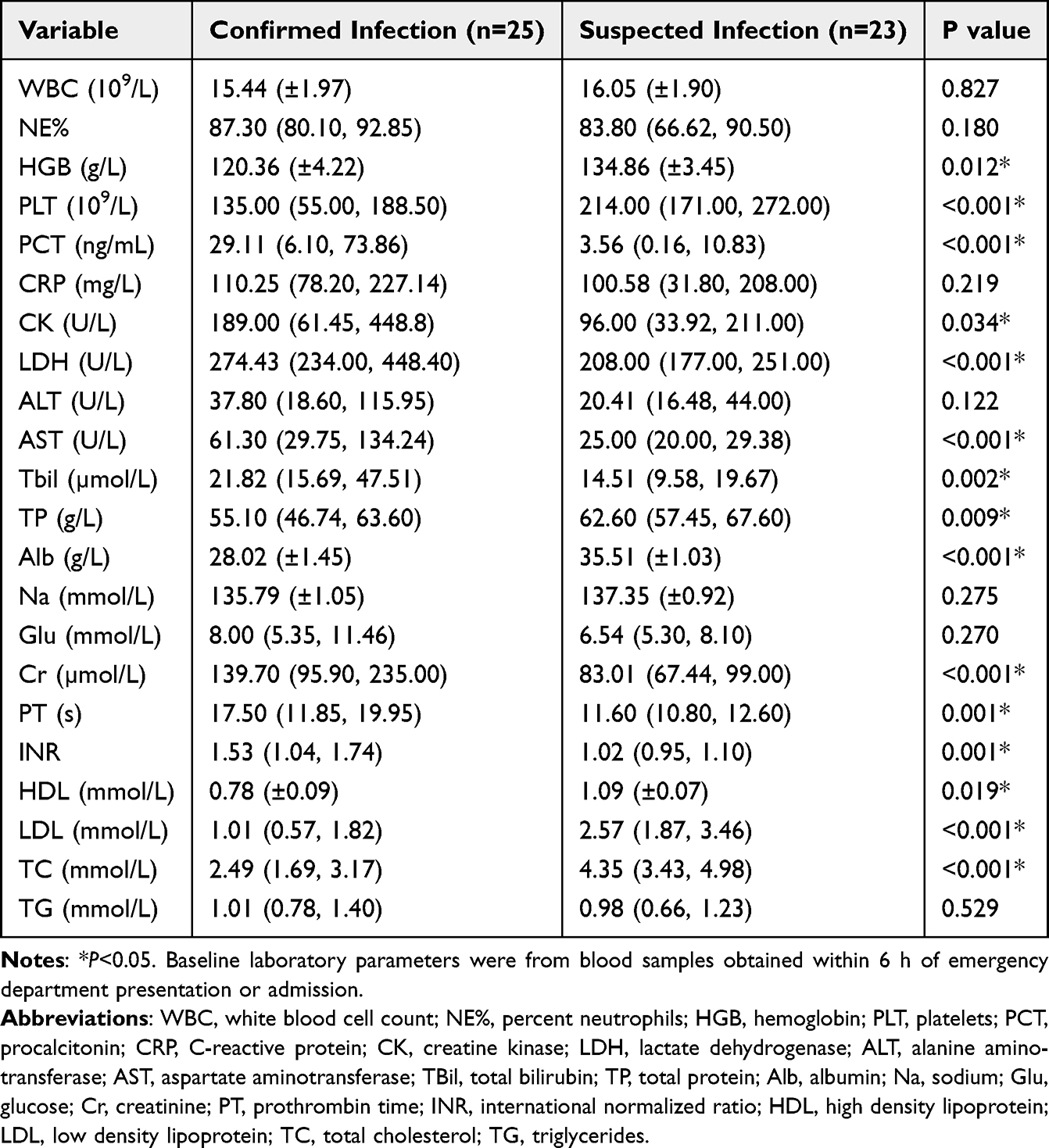 |
Table 2 Baseline Laboratory Characteristics of Patients with Confirmed and Suspected Vibrio vulnificus Infection |
Patient Outcomes
We performed pathogen cultures for all 48 patients and mNGS for 10 patients (Table 3). In the 25 confirmed cases, 15 patients were positive by culture only, 8 were positive by mNGS only, and 2 were positive by both methods. In the suspected cases, all 23 patients had negative culture results and none of the patients received testing by mNGS. All 48 patients received standard antibiotic therapy, which consisted of piperacillin-tazobactam, imipenem, or a third-generation cephalosporin alone or combined with a fluoroquinolone.
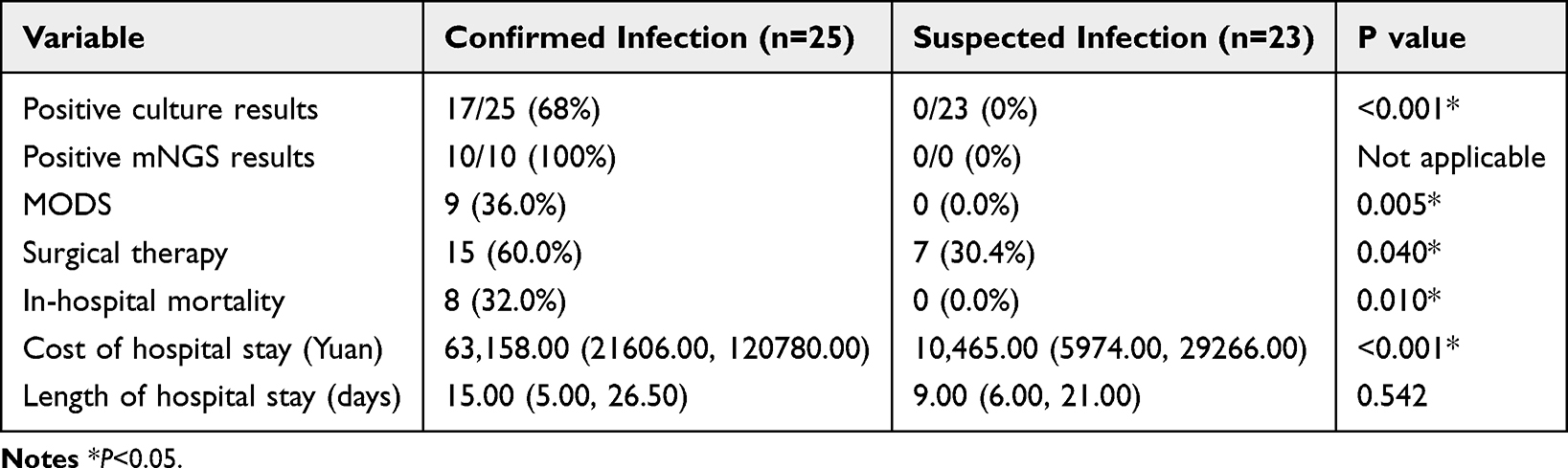 |
Table 3 Outcomes of Patients with Confirmed and Suspected Vibrio vulnificus Infection |
The confirmed cases had significantly higher rates of in-hospital mortality (32.0% vs 0%, P = 0.01), multiple organ dysfunction syndrome (MODS, 36.0% vs 0%, P = 0.005), and surgical intervention (60.0% vs 30.4%, P = 0.04), and a greater economic burden (63,158 vs 10,465 yuan, P < 0.001).
Discussion
Patients with V. vulnificus infection present with fever and with localized limb erythema, swelling, and pain. Many clinicians are unfamiliar with this disease because of its relative rarity, and this can lead to delayed diagnosis. Early identification of skin and soft tissue involvement is essential for timely intervention and surgical debridement.8 In our study, each patient with suspected V. vulnificus infection had an epidemiological history and signs of limb inflammation that suggested infection by this pathogen. The suspected and confirmed groups had comparable age, gender, and underlying diseases, but the confirmed group had more severe soft tissue infection and a greater involvement of multiple sites.
Previous reports compared patients with NSTI caused by V. vulnificus and other pathogens (eg, Staphylococcus aureus or Aeromonas species).9,10 Another matched-pair cohort study demonstrated that Vv-NSTI was associated with greater in-hospital mortality,11 consistent with our findings. Our group with confirmed infection had more pathological laboratory parameters and worse clinical outcomes. Thus, in the absence of etiological confirmation, a diagnostic strategy that considers epidemiological exposure with clinical and laboratory findings may be a reliable adjunctive tool for identifying patients at high risk of V. vulnificus infection. Specific laboratory parameters, particularly those indicative of tissue injury, abnormal coagulation, liver dysfunction, renal dysfunction, dyslipidemia, and poor nutritional status, might be most useful for early risk stratification in clinical practice.
In addition to V. vulnificus, various other bacterial species (eg, Aeromonas spp., Shewanella spp., Mycobacterium marinum, and Streptococcus suis) can cause superficial soft tissue and invasive systemic infections following marine-related wounds or seawater exposure.12–14 A study of soft tissue infections from fish spike wounds found that normal commensal bacteria (eg, methicillin-resistant Staphylococcus aureus, Enterobacter cloacae, Clostridium spp.) are more commonly isolated than marine pathogens.15 These studies demonstrate the microbiological diversity and complexity of post-exposure infections. In the Chaoshan region, V. vulnificus infection is an uncommon seawater-related disease, so clinicians must consider this species along with a broad spectrum of other potential pathogens.16 Failure to recognize and treat V. vulnificus infection in a timely manner can lead to severe morbidity or death.2 Given the considerable heterogeneity and risk of misclassification among “suspected” cases and our lack of adjustment for confounders, such as comorbidities and timing of treatment, caution is needed when attributing infections to V. vulnificus without microbiological confirmation. If possible, future studies should incorporate microbiological confirmation, clinical phenotyping, and multivariable adjustments.
All patients with confirmed or suspected V. vulnificus infection were admitted from March 2014 to November 2025, but 14 of the confirmed cases occurred in 2024 or 2025, and 8 were identified by mNGS only. mNGS became available at our institution in 2017, so this may account for the greater number of cases during more recent years.7,17 Due to the limitations of identifying V. vulnificus and other pathogens by culture—suboptimal timing of sample collection, prior use of antibiotics, and suboptimal culture conditions—there is a high probability of false negatives. Consequently, some suspected but undiagnosed cases in this study could be attributed to V. vulnificus. Future multicenter prospective cohort studies should better define the actual pathogens in a “suspected group” by combining molecular techniques (such as PCR and mNGS) with rigorous clinical assessment. Furthermore, combating neglected zoonotic diseases, such as V. vulnificus infection, also necessitates a broader integrated “One Health” approach.18 As with other zoonoses, this approach promotes coordinated, multisectoral strategies that consider human, animal, and environmental health and includes improved surveillance, data sharing between public health and veterinary sectors, and preventive measures.
Conclusions
In conclusion, this study provides preliminary evidence for the early identification and risk stratification of patients with V. vulnificus infection. Our findings demonstrate that early clinical features (severe soft tissue involvement, multiple affected sites) and specific laboratory markers (particularly those indicative of tissue injury, coagulation dysfunction, impaired liver and renal function, dyslipidemia, and poor nutritional status) reliably distinguished confirmed cases from suspected cases. However, this was a single-center study with a relatively small sample size, and statistical matching of the confirmed and suspected groups was not possible. Our results suggest that further large studies are warranted for confirmation. Specifically, future multicenter cohorts using standardized molecular diagnostics are necessary to validate the markers identified in this study and to more fully characterize the heterogeneity of patients with clinically suspected V. vulnificus infection. In addition, given the local custom of eating raw marinated seafood in Chaoshan, it is necessary to strengthen public awareness and education regarding V. vulnificus infection.
Data Sharing Statement
The datasets generated and analyzed in the present study are available from the corresponding author, Tao Li, upon reasonable request.
Ethics Approval and Informed Consent
This study was approved by the Ethics Committee of the First Affiliated Hospital of Shantou University Medical College (Approval No. B-2026-052) and adhered to the principles outlined in the Declaration of Helsinki. Written informed consent was waived due to the retrospective nature of the study. Patient data were anonymized and kept confidential in accordance with ethical guidelines.
Acknowledgments
We thank Medjaden Inc. for scientific editing of this manuscript.
Author Contributions
Each author made a significant contribution to this study that consisted of study conception, study design, study execution, acquisition of data, analysis and interpretation of data, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Kim JS, Lee EG, Chun BC. Epidemiologic characteristics and case fatality rate of Vibrio vulnificus infection: analysis of 761 cases from 2003 to 2016 in Korea. J Korean Med Sci. 2022;37:e79. doi:10.3346/jkms.2022.37.e79
2. Tanveer M, Ntakiyisumba E, Won G. Prevalence and risk factors of seafood-borne Vibrio vulnificus in Asia: a systematic review with meta-analysis and meta-regression. Front Microbiol. 2024;15:1363560. doi:10.3389/fmicb.2024.1363560
3. Tanveer M, Ntakiyisumba E, Won G. Revealing antimicrobial resistance profile and associated factors of Vibrio vulnificus isolated from clinical, environmental, and seafood samples across Asia: a systematic review and meta-analysis. Heliyon. 2024;10:e40334. doi:10.1016/j.heliyon.2024.e40334
4. Tanveer M, Ntakiyisumba E, Kim B, Won G. Estimating risk, disease burden, and economic impact of Vibrio vulnificus infection associated with raw oyster consumption in South Korea. Appl Food Res. 2025;5:100820. doi:10.1016/j.afres.2025.100820
5. Baker-Austin C, Oliver JD. Vibrio vulnificus: new insights into a deadly opportunistic pathogen. Environ Microbiol. 2018;20:423–7. doi:10.1111/1462-2920.13955
6. Burillo A, Bouza E. Use of rapid diagnostic techniques in ICU patients with infections. BMC Infect Dis. 2014;14:593. doi:10.1186/s12879-014-0593-1
7. Li X, Wang C, Guo Z, et al. Enhancing Vibrio vulnificus infection diagnosis for negative culture patients with metagenomic next-generation sequencing. Front Cell Infect Microbiol. 2023;13:1210919. doi:10.3389/fcimb.2023.1210919
8. Hong GL, Lu CJ, Lu ZQ, et al. Surgical treatment of 19 cases with vibrio necrotising fasciitis. Burns. 2012;38:290–295. doi:10.1016/j.burns.2011.04.013
9. Tsai YH, Wen-Wei Hsu R, Huang KC, Huang TJ. Comparison of necrotizing fasciitis and sepsis caused by Vibrio vulnificus and Staphylococcus aureus. J Bone Joint Surg Am. 2011;93:274–284. doi:10.2106/JBJS.I.01679
10. Tsai YH, Hsu RW, Huang TJ, et al. Necrotizing soft-tissue infections and sepsis caused by Vibrio vulnificus compared with those caused by Aeromonas species. J Bone Joint Surg Am. 2007;89:631–636. doi:10.2106/JBJS.F.00580
11. Chang CY, Wu KH, Wu PH, et al. In-hospital mortality associated with necrotizing soft tissue infection due to Vibrio vulnificus: a matched-pair cohort study. World J Emerg Surg. 2022;17:28. doi:10.1186/s13017-022-00433-z
12. Finkelstein R, Oren I. Soft tissue infections caused by marine bacterial pathogens: epidemiology, diagnosis, and management. Curr Infect Dis Rep. 2011;13:470–477. doi:10.1007/s11908-011-0199-3
13. Yu M, Wang X, Yan A. Microbial profiles of retail Pacific Oysters (Crassostrea gigas) from Guangdong Province, China. Front Microbiol. 2021;12:689520. doi:10.3389/fmicb.2021.689520
14. Diaz JH, Lopez FA. Skin, soft tissue and systemic bacterial infections following aquatic injuries and exposures. Am J Med Sci. 2015;349:269–275. doi:10.1097/MAJ.0000000000000366
15. Collins H, Lee KM, Cheng PT, Hulme S. Soft tissue infections from fish spike wounds: normal commensal bacteria are more common than marine pathogens. ANZ J Surg. 2018;88:E40–E44. doi:10.1111/ans.13850
16. Chen LC, Zhu HJ, Zhou ZY, Ke YJ, Chen CW. Laboratory analysis on 4 cases of sporadic Vibrio vulnificus infection in Shantou City. Chin J Infect Control. 2016;15:272–276.
17. Wang Q, Miao Q, Pan J, et al. The clinical value of metagenomic next-generation sequencing in the microbiological diagnosis of skin and soft tissue infections. Int J Infect Dis. 2020;100:414–420. doi:10.1016/j.ijid.2020.09.007
18. Meurer IR. The importance of medical knowledge about Q Fever in the context of timely diagnosis and treatment and the use of the one health approach in combating this and other neglected zoonotic diseases [Letter]. Infect Drug Resist. 2025;18:5007–5008. doi:10.2147/IDR.S567142
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.