Back to Journals » OncoTargets and Therapy » Volume 11
Comparative study of clinical efficacy using three-dimensional and two-dimensional laparoscopies in the treatment of distal gastric cancer
Authors Liu JG, Zhou HT, Qin HQ, Ru HM, Huang JH, Liang SY, Mo XW, Tang WZ
Received 8 October 2017
Accepted for publication 13 December 2017
Published 11 January 2018 Volume 2018:11 Pages 301—306
DOI https://doi.org/10.2147/OTT.S153520
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ingrid Espinoza
Jungang Liu,1,* Haitao Zhou,2,* Haiquan Qin,1 Haiming Ru,1 Jiahao Huang,1 Siyuan Liang,1 Xianwei Mo,1 Weizhong Tang1
1Department of Gastrointestinal Surgery, Affiliated Tumor Hospital of Guangxi Medical University, Nanning, Guangxi Zhuang Autonomous Region, 2Department of Colorectal Surgery, Tumor Hospital of Chinese Academy of Medical Sciences, Beijing, China
*These authors contributed equally to this work
Background: Three-dimensional (3D) laparoscopy has the advantages and characteristics of more radical procedures in the treatment of gastric cancer. The objective of this research was to investigate the short-term efficacy and safety of 3D laparoscopic procedures in the treatment of advanced distal gastric cancer.
Methods: We retrospectively analyzed the clinical data of 124 patients treated with 3D and two-dimensional (2D) laparoscopic D2 lymphadenectomy for distal gastric cancer at the China Academy of Medical Sciences Cancer Hospital and the Affiliated Cancer Hospital of Guangxi Medical University from January 2014 to January 2015. The effects on operative time, bleeding, hospitalization time, complications, and the number of lymph nodes removed were analyzed.
Results: The difference between the general data of the two groups was not statistically significant (P>0.05). In analysis of the subgroups, the number of lymph nodes removed in the 3D laparoscopic group was significantly higher than in the 2D laparoscopic group ([2.52±1.88] vs [2.22±1.80], P=0.001; [2.22±1.80] vs [1.47±1.99], P=0.019). However, the differences among the total number of lymph nodes removed, operative time, intraoperative blood loss, intraoperative complications, postoperative complications, postoperative recovery time, and postoperative hospital stay were not statistically significant.
Conclusion: 3D laparoscopic-assisted radical gastrectomy for distal advanced gastric cancer is safe and feasible.
Keywords: laparoscopic gastrectomy, D2 lymphadenectomy, gastric neoplasm, imaging, 3D laparoscopy
Introduction
Laparoscopic procedures for early gastric cancer were first reported by Kitano et al1 in 1994. Since then, laparoscopic gastrectomy for cancer has been used worldwide because of its remarkable advantages of being a minimally invasive procedure and having a radical effect similar to that of open procedures.2–7 Perigastric vascular anatomy is complicated, and often a wide range of gastric cancer lymph nodes must be removed. However, lymphoscintigrams are displayed as planar images in two-dimensional (2D) laparoscopic procedures. Therefore, performing perigastric lymphadenectomy can be difficult, requiring surgeons who have extensive experience in procedures and excellent operating skills. With the development of the laparoscopic technique, three-dimensional (3D) laparoscopy has overcome the shortcomings of traditional laparoscopic procedures and now provides surgeons with 3D visions. Generally, 3D laparoscopy has the advantages and characteristics of radical gastric cancer procedures. This study aimed to investigate the feasibility and short-term effects of 3D laparoscopic-assisted radical gastrectomy for distal advanced gastric cancer.
Methods
Patients
This study was approved by the Institution Review Board of Guangxi Medical University, and written informed consent was obtained from each patient. The clinical data were collected from patients treated with 3D and 2D laparoscopic D2 lymphadenectomy for distal gastric cancer in the Chinese Academy of Medical Sciences Cancer Hospital and the Affiliated Cancer Hospital of Guangxi Medical University from January 2014 to January 2015. All the patients underwent gastroscopy before surgery, and their pathological diagnosis was adenocarcinoma of the stomach. They also underwent chest X-ray and abdominal and pelvic computerized tomography staging. The inclusion criteria were as follows: 1) 20–70 years of age; 2) preoperative imaging showing no distant metastasis; 3) tumor diameter <10 cm; 4) no major blood vessels fused or encased by lymph node metastasis and/or tumor not extensively infiltrated with surrounding tissues and organs; 5) signed patient informed consent; and 6) patient able to tolerate surgical treatment under normal circumstances. The exclusion criteria included the following: 1) distant metastasis; 2) presence of underlying diseases that would make the patient intolerant of a laparoscopic pneumoperitoneum; 3) previous abdominal procedures; 4) previous malignant tumors; 5) previous radiotherapy or chemotherapy; 6) dysfunction of coagulation, hypoproteinemia, anemia, or diabetes mellitus; and 7) refusal to sign informed consent. Pathological staging was based on the staging criteria for gastric cancer published in the 2016 American Joint Committee on Cancer Staging Manual, 8th edition.
One month after the operations, postoperative recovery of the patients was assessed by telephone follow-up calls and clinical follow-ups.
Methods
The 3D group used the Olympus HD 3D laparoscopic surgery system, and both the surgeons and assistants wore 3D glasses. The 2D group used the Olympus HD laparoscopic procedures system. The two groups used the same surgical method.8 Tracheal intubation and intravenous injections of medications were performed to achieve anesthesia, and the patients were positioned supine. A five-trocar technique was used. Pneumoperitoneum pressure was maintained at 12–15 mmHg, and distal gastrectomy was performed according to the location of the tumor. Standard D2 lymphadenectomy was performed according to the lymph node stations and dissection range stipulated by the 14th edition of the Japanese Gastric Cancer Treatment Protocol.9 For patients with distal gastrectomy, the anastomosis was conducted using either using Billroth I or Billroth II anastomosis.
The observation index included the total number of lymph node dissections and the number of lymph nodes in subgroup 1, subgroup 3, subgroup 4d, subgroup 4sa, subgroup 4sb, subgroup 6, subgroup 7, subgroup 8a, subgroup 9, subgroup 11p, and subgroup 12a. The pathological results were final. The operative time, amount of bleeding, and postoperative complications were observed and recorded.
Data analysis
Statistical data were analyzed using SPSS version 24.0 (SPSS Inc., Chicago, IL, USA). The independent sample t-test was used to compare the means of the two groups. Enumeration data were verified by the χ2 test, and P<0.05 was considered statistically significant.
Results
General data
The Affiliated Cancer Hospital of Guangxi Medical University introduced the 3D laparoscopic system in October 2014. Prior to that, patients would undergo 2D laparoscopic procedures. This study enrolled 124 patients, including 60 cases from the 3D laparoscopic group and 64 cases from the 2D laparoscopic group. The detailed clinical data of the two groups of patients are shown in Table 1.
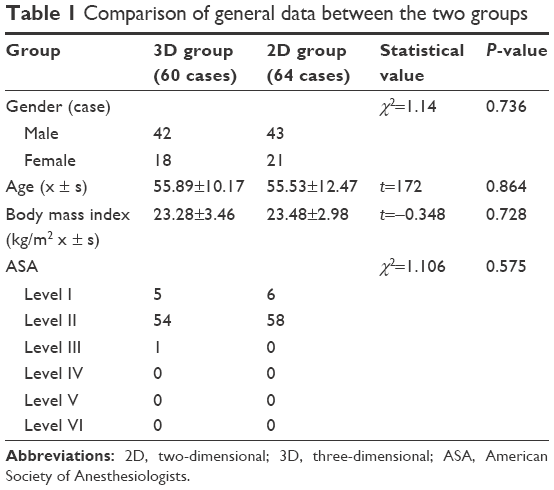 | Table 1 Comparison of general data between the two groups |
Operation
The mean operative time for the 3D laparoscopic group was 181.03±36.76 min, and for the 2D laparoscopic group it was 191.47±47.19 min. No significant difference was found between the two groups (P=0.171) with regard to operative time. The amount of bleeding in the 3D laparoscopic group was 160.83±150.66 mL, while in the 2D group it was 170.31±147.49 mL. No statistical difference was observed between the two groups (P=0.724). The 3D laparoscopic group reported one case of pancreatic injury, and the 2D laparoscopic group reported one case of splenic artery injury, one case of common hepatic artery injury, and one case of portal vein injury. Although no statistical difference (P=0.341) was found between groups, it seemed that complications tended to be less in the 3D laparoscopic group. No significant difference was observed between the two groups (P=0.396). Details of the intraoperative data are shown in Table 2.
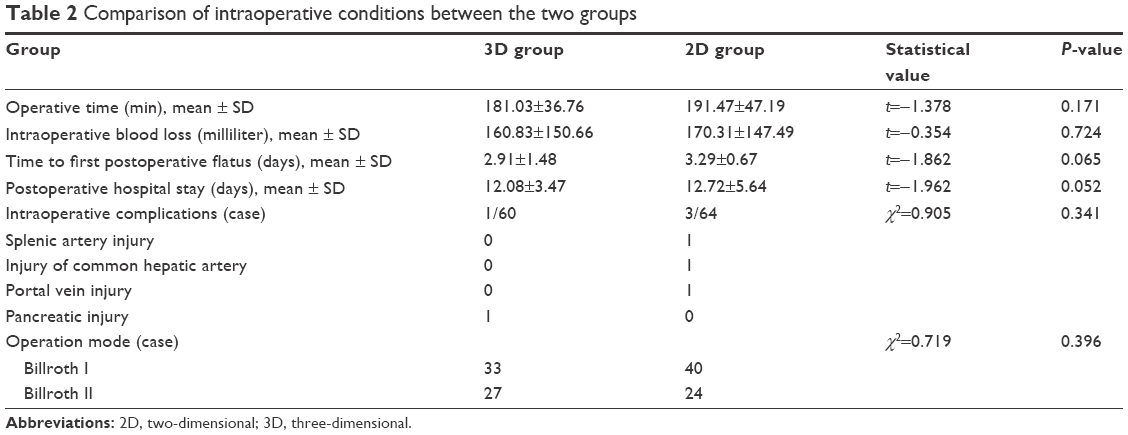 | Table 2 Comparison of intraoperative conditions between the two groups |
Postoperative recovery and postoperative complications
The patients in the 3D and 2D laparoscopic groups started to pass gas 2.91±1.48 days and 3.29±0.67 days after their operations, respectively. No statistical difference was found between the two groups (P=0.065). The length of hospital stay was 12.08±3.47 days and 12.72±5.64 days for the 3D and 2D laparoscopic groups, respectively, and no statistically significant difference was observed (P=0.052).
Postoperative gastroparesis occurred in one patient from the 3D laparoscopic group and one patient from the 2D laparoscopic group. These patients were relieved after conservative treatment and were discharged 24 days and 22 days after the operations, respectively. In the 3D laparoscopic group, pancreatic leakage occurred in one patient, and it was cured 10 days after octreotide treatment. In the 2D laparoscopic group, one patient had postoperative intraperitoneal bleeding, and one patient had duodenal and duodenal anastomotic leakage. They were cured at 10 and 19 days after conservative treatment, respectively. Although there was an increase in the number of postoperative complications observed in the 2D laparoscopic group compared with the 3D laparoscopic group, no statistically significant difference was found between the two groups. The details of postoperative recovery are shown in Table 3.
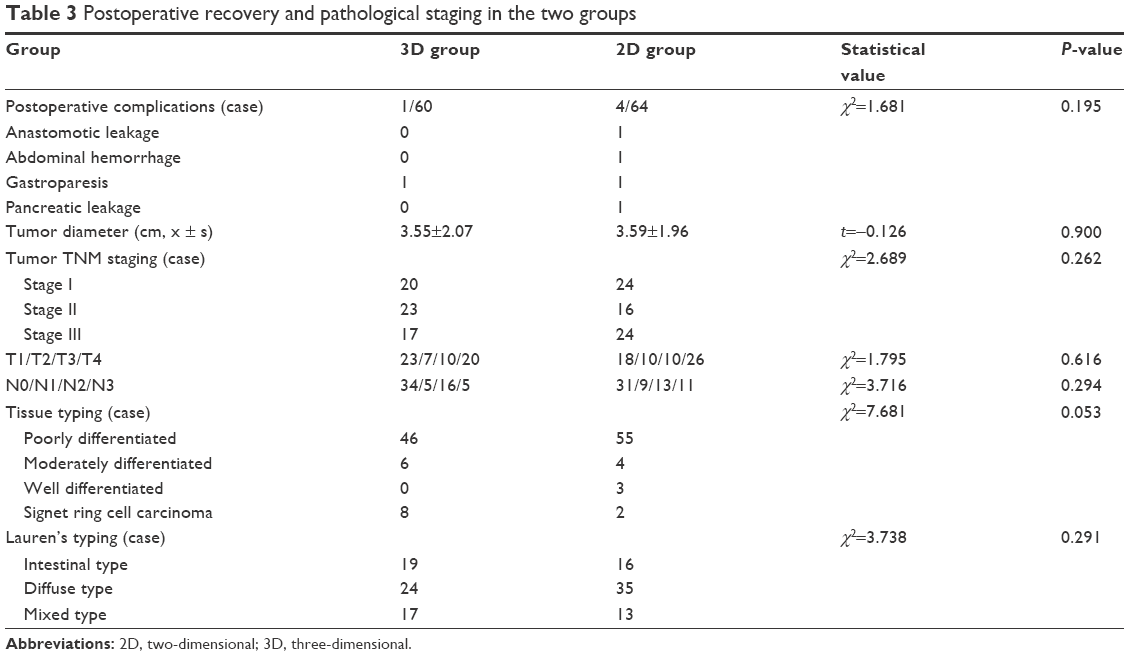 | Table 3 Postoperative recovery and pathological staging in the two groups |
Postoperative pathological staging
No statistically significant difference was found in T staging and N staging between the two groups (Table 3). The average number of lymph nodes detected in each patient in the 3D laparoscopic group was 37.36±14.78, and in the 2D laparoscopic group it was 33.03±12.65. No statistically significant difference was observed between the two groups (P=0.081). The average number of positive lymph nodes detected in lymph node-positive patients in the 3D laparoscopic group was 3.32±6.42 and in the 2D laparoscopic group was 5.00±8.57. No statistically significant difference was found between the two groups (P=0.221). However, analysis of the subgroups revealed that the number of lymph nodes in subgroup 11p and subgroup 8a of the 3D laparoscopic group was 2.22±1.80 and 2.52±1.88, respectively, and in the 2D laparoscopic group it was 1.47±1.99 and 1.48±1.43, respectively. Significantly statistical differences were found between the two groups (P=0.019 and P=0.001, respectively) for these two subgroups. For the remaining groups, 1, 3, 4d, 4sa, 4sb, 5, 6, 7, 9, and 12a, there was no statistically significant difference found in the number of lymph nodes between any two of them (P>0.05) (Table 4).
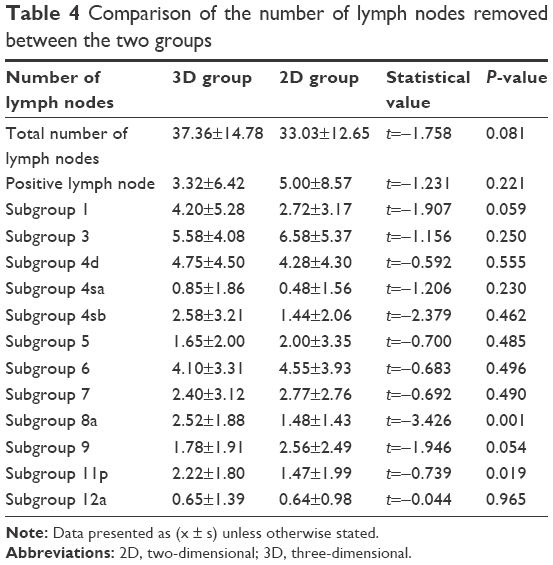 | Table 4 Comparison of the number of lymph nodes removed between the two groups |
Discussion
Gastric cancer, which has the second highest morbidity and mortality rates of any cancer, is one of the most common forms of malignant tumors in China.10 Surgery is an important treatment for gastric cancer, and D2 lymphadenectomy has been used as the standard surgery for advanced gastric cancer. With the progress of minimally invasive techniques, laparoscopic gastrectomy for advanced cancer has been performed worldwide. The advantages and safety of minimally invasive procedures have been recognized in previous research.11–14 Some believe that the long-term effects are similar to those of open radical gastrectomy.14–16
Laparoscopic gastrectomy for advanced cancer must follow the same principle of radically resecting the tumor followed in traditional open procedures. The main, and often the most difficult, goal of this procedure is lymph node dissection. The 2D laparoscopy usually poses some difficulty for beginners in identifying anatomical structures, judging distances between tissues, and finding and separating tissues at the anatomical level because of the lack of stereoscopic vision. Laparoscopic gastrectomy for advanced cancer is difficult because gastric blood supply is abundant, there are many layers of anatomy, and the gastric lymph nodes are complexly distributed. With the progress of science and technology, 3D laparoscopy has made up for the deficiencies of traditional 2D laparoscopy to a certain extent. Compared with its 2D counterpart, 3D laparoscopic surgery has a higher magnification of the local surgical field and gives a better stereoscopic vision and sense of anatomical structure, thus making it easier and more precise to grasp tissue, dissect, separate tissues, stop blood, and ligate vessels. It reduces the difficulty of surgery; the damage to the surrounding vessels, organs, and tissues; and the amount of bleeding during surgery.17 During the dissection of lymph nodes, vessels are well organized in the 3D field of vision. Specifically, 3D laparoscopic surgery allows surgeons to control the operating space and avoid accidental damage to blood vessels when dissecting perivascular adipose tissues.
Ma et al18 and Hong et al19 reported their experiences in 3D laparoscopic D2 lymphadenectomy for distal gastric cancer and found no significant difference between the operative time, intraoperative blood loss, number of lymph node dissections, and postoperative complication rates between the procedure and those of 2D laparoscopic D2 lymphadenectomy for distal gastric cancer. In this study, unlike in the 2D group, less intraoperative bleeding was found in the 3D group patients, and the operative time was shorter. However, no significant difference was found (P=0.724) between the two groups. The 3D vision was provided by 3D laparoscopy, which enabled the surgeons to locate the lymph nodes accurately. The spatial distribution of blood vessels and the anatomic relation between blood vessels were clear. Therefore, the operative time was shorter, and the intraoperative bleeding was less. The time to the first postoperative flatus was reduced in the 3D group patients, and their intestinal function recovered more quickly than patients in the 2D group. However, no significant difference was observed (P=0.065) between the two groups.
One case of intraoperative pancreatic injury occurred in the 3D group, and one case of splenic artery injury, one case of common hepatic artery injury, one case of portal vein injury, and one case of colon injury occurred in the 2D group. The intraoperative and postoperative complications that occurred in the 3D group were less than those that occurred in the 2D group. Although this result was not statistically significant, these values in the 3D group were decreased.
The 3D laparoscopy provides a surgeon with good stereoscopic vision and a sense of anatomical structure to reduce intraoperative damage to surrounding vessels, organs, and tissues. The range of lymph node dissection and the number of lymph nodes detected are important indicators of performance in laparoscopic gastrectomy for cancer. In this study, compared with the 2D group, there was no significant difference found (P=0.081) between the number of lymph nodes (60 cases) removed by 3D laparoscopy and the number (64 cases) removed by 2D laparoscopy. The number of lymph nodes removed in the two groups was greater than 15, which met the requirements of the 2017 National Comprehensive Cancer Network guidelines for the pathological staging of gastric cancer. This result shows that 3D laparoscopic D2 lymphadenectomy for distal gastric cancer is an effective way to treat this cancer.
The subgroup analysis showed that the number of lymph nodes removed by 3D laparoscopy in subgroups 11p and 8a was greater than that removed by 2D laparoscopy and that the difference was significant (P<0.05). The difficulty in removing lymph nodes may be significantly reduced during surgery by the advantages of the 3D laparoscopic surgery system. Especially in subgroups 11p and 8a, the effect of lymphadenectomy using 3D laparoscopy is better than that using 2D laparoscopy.
Conclusion
In conclusion, 3D laparoscopic-assisted radical gastrectomy for distal gastric cancer is safe and feasible. It has an efficacy similar to that of 2D laparoscopic surgery as well as a minimally invasive effect. The 3D laparoscopic gastrectomy tends to increase the number of lymph nodes removed in subgroups and reduce the incidence of intraoperative and postoperative complications. As the study was retrospective and the sample size limited, the effects of 3D laparoscopic-assisted radical gastrectomy for distal gastric cancer need to be further studied using multicenter, prospective, and randomized controlled clinical trials.
Author contribution
JGL, HTZ, XWM, and WZT designed this manuscript. JGL, HTZ, HQQ, HMR, JHH, and SYL collected the data and JGL and HTZ analyzed the data. JGL wrote this manuscript. JGL, XWM, and WZT edited the final manuscript. All authors gave final approval of this submission. All authors contributed toward data analysis, drafting and critically revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Kitano S, Iso Y, Moriyama M, Sugimachi K. Laparoscopy-assisted Billroth I gastrectomy. Surg Laparosc Endosc. 1994;4(2):146–148. | ||
Han HS, Kim YW, Yi NJ, Fleischer GD. Laparoscopy-assisted D2 subtotal gastrectomy in early gastric cancer. Surg Laparosc Endosc Percutan Tech. 2003;13(6):361–365. | ||
Kim HH, Hyung WJ, Cho GS, et al. Morbidity and mortality of laparoscopic gastrectomy versus open gastrectomy for gastric cancer: an interim report – a phase III multicenter, prospective, randomized Trial (KLASS Trial). Ann Surg. 2010;251(3):417–420. | ||
Haverkamp L, Brenkman HJ, Seesing MF, et al. Laparoscopic versus open gastrectomy for gastric cancer, a multicenter prospectively randomized controlled trial (LOGICA-trial). BMC Cancer. 2015;15:556. | ||
Nakamura K, Katai H, Mizusawa J, et al. A phase III study of laparoscopy-assisted versus open distal gastrectomy with nodal dissection for clinical stage IA/IB gastric Cancer (JCOG0912). Jpn J Clin Oncol. 2013;43(3):324–327. | ||
Kong J, Wu SD, Su Y, Fan Y. Single incision versus conventional laparoscopic resection in gastrointestinal stromal tumors: a retrospective cohort analysis at a single tertiary care center. Onco Targets Ther. 2014;7:995–999. | ||
Liu G, Jian F, Wang X, Chen L. Fast-track surgery protocol in elderly patients undergoing laparoscopic radical gastrectomy for gastric cancer: a randomized controlled trial. Onco Targets Therapy. 2016;9:3345–3351. | ||
Sciences CAoM. Division of laparoscopic and endoscopic surgery. Guidelines for laparoscopic surgery for gastric cancer (2016 Edition). Chinese J Digest Surgery. 2016;(15):851–857. | ||
Xiang H. Important changes in the Japanese protocol for the treatment of gastric cancer, Fourteenth Edition. Chinese J Pract Surg. 2010;4(30):241–246. | ||
Chen W, Zheng R, Baade PD, et al. Cancer statistics in China, 2015. CA Cancer J Clin. 2016;66(2):115–132. | ||
Parisi A, Nguyen NT, Reim D, et al. Current status of minimally invasive surgery for gastric cancer: A literature review to highlight studies limits. Int J Surg. 2015;17:34–40. | ||
Son T, Kwon IG, Hyung WJ. Minimally invasive surgery for gastric cancer treatment: current status and future perspectives. Gut Liver. 2014;8(3):229–236. | ||
Haverkamp L, Ruurda JP, Offerhaus GJ, Weijs TJ, van der Sluis PC, van Hillegersberg R. Laparoscopic gastrectomy in Western European patients with advanced gastric cancer. Eur J Surg Oncol. 2016;42(1):110–115. | ||
Chen XZ, Hu JK, Yang K, Wang L, Lu QC. Short-term evaluation of laparoscopy-assisted distal gastrectomy for predictive early gastric cancer: a meta-analysis of randomized controlled trials. Surg Laparosc Endosc Percutan Tech. 2009;19(4):277–284. | ||
Zeng YK, Yang ZL, Peng JS, Lin HS, Cai L. Laparoscopy-assisted versus open distal gastrectomy for early gastric cancer: evidence from randomized and nonrandomized clinical trials. Ann Surg. 2012;256(1):39–52. | ||
Vinuela EF, Gonen M, Brennan MF, Coit DG, Strong VE. Laparoscopic versus open distal gastrectomy for gastric cancer: a meta-analysis of randomized controlled trials and high-quality nonrandomized studies. Ann Surg. 2012;255(3):446–456. | ||
McLachlan G. From 2D to 3D: the future of surgery? Lancet. 2011;378(9800):1368. | ||
Junjun M, Lu Z, Zhou HX. Clinical curative effect of laparoscopic radical resection of 3D. Chinese J Digest Surgery. 2015;3(14):192–194. | ||
Qiang H, Yong W, Jianjun W. 3D laparoscopic clinical application in radical gastrectomy for gastric cancer. Chinese Med J. 2014;30(94):2375–2376. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.