Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 15
Comparative Safety and Changes in Immunologic and Virologic Parameters of Dolutegravir versus Efavirenz-Based Antiretroviral Therapies Among HIV Patients: A Retrospective Cohort Study
Received 21 November 2022
Accepted for publication 7 April 2023
Published 27 April 2023 Volume 2023:15 Pages 173—190
DOI https://doi.org/10.2147/HIV.S396420
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Olubunmi Akindele Ogunrin
Melese Alemnew Ayal, Alemseged Beyene Berha
Department of Pharmacology and Clinical Pharmacy, School of Pharmacy, College of Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia
Correspondence: Alemseged Beyene Berha, Email [email protected]
Background: In combination with other two antiretroviral drugs, an efavirenz (EFV) or dolutegravir (DTG)-based regimen is the treatment of choice for human immunodeficiency virus (HIV) infection. This study aimed to determine the safety and changes in immunologic and virologic parameters of DTG compared with EFV-based ART as first-line HIV treatment among HIV patients.
Methods: A retrospective hospital-based cohort study was carried out from September 1, 2019 to August 30, 2020 at HIV clinics of three selected hospitals in North-West–East Ethiopia, Amhara Region. All HIV patients ≥ 3 years old, who had been on either DTG or EFV-based combination anti-retroviral therapy (cART), and had detectable viral load (VL) were included. Descriptive and multivariate Cox regression analyses were used.
Results: Overall, 990 HIV patients were included in the analysis (DTG n=694, EFV n=296). A VL of < 50 copies/mL was observed in 69% of patients in the DTG group and 66% in the EFV group (crude hazard ratio [CHR] =1.28, 95% CI: 1.08– 1.51; p=0.004). Out of the total, 289 (42%) of the patients in the DTG group reported adverse drug events (ADEs) compared with 147 (50%) in the EFV group (p=0.020). Younger age, opportunistic infections (OIs), bed-ridden condition, no prophylaxis for OIs, low baseline cluster of differentiation 4 (CD4) count, high baseline VL, poor adherence, and ADEs were predictors of poor survival, and younger age, OIs, low baseline CD4, DTG-based initial regimen, poor adherence with cART, naïve treatment history, and student job type were predictors of poor safety outcomes.
Conclusion: The DTG-based regimen demonstrates an improved viral suppression and CD4 cell recovery, and better safety profile compared with the EFV-based regimen for the treatment of HIV-infected patients. A baseline CD4+ T-cell count < 200 cells/mm3, OIs, and poor adherence with therapy were factors associated with poor survival and safety outcomes. HIV patients with these risk factors should be treated and monitored regularly.
Keywords: dolutegravir, efavirenz, human immunodeficiency virus, safety, survival
Background
Acquired immune deficiency syndrome (AIDS) is a human infectious disease with no cure. It is a stage of infection where advanced immunosuppression, progressive clinical deterioration, and opportunistic infections (OIs) occur. It leads to a fatal infection if left untreated with effective and safe medications.1,2 According to the global AIDS update in 2022, out of 38.4 million people living with human immunodeficiency virus (HIV), 28.7 million (75.5%) were accessing antiretroviral therapy (ART) in 2021, which is 1.7 times greater than in the 2015 report, when 17.1 million (49.4%) out of 34.6 million HIV patients were on ART.3
Although no curative medications are available, thanks to combination antiretroviral therapy (cART), fewer people are dying of HIV-related causes: 680,000 deaths were registered in 2020, down 77% from 2003 (3 million), which is the year in which the antiretroviral therapy (ART) service commenced in Ethiopia.4
Treatment with cART and prophylaxis for common OIs have improved the clinical condition of patients with HIV and decreased the complications of the disease.1 An ideal antiretroviral drug is expected to have long-term efficacy, long-term tolerability, a lack of drug–drug interaction, no food or timing restrictions, and a barrier to viral resistance.5 Moreover, the initial cART regimen is selected based on the drug’s safety, adherence of the patient, food requirements, drug interactions, degree of resistance, and comorbid conditions.6 The efficacy and safety of cART have largely improved with the arrival of newer and more convenient antiretroviral drug classes.7 Through semi-synthetic modification and new synthesis pathways, a number of novel, convenient, safer, and more suitable HIV drugs have been developed.8,9
The newly approved drug dolutegravir (DTG) is available in once-daily dosing for HIV patients, has a high genetic barrier to resistance, and is safer compared to non-DTG-based cART.10–15 It reduces the pill burden, has no significant drug interactions, does not require a booster, and has good absorption regardless of food intake.16–18 However, patients with viral mutations including Q148H/K/R plus G140S plus additional RAL mutations had a reduced response to DTG.10,19
As of September 2021, Ethiopia has reported a gradual decline in the number of people living with HIV (PLHIV), which was were estimated at 612,925 for the year 2021 and 609,349 in 2022; also, new adult HIV infections declined from 8772 to 8284 for the years 2021 and 2022, respectively.20 Of those patients receiving cART, only 51% were virally suppressed, owing to inadequate services, drug resistance, and adverse drug events (ADEs) from the available cART drugs.21
According to previous studies, DTG-based cART achieves a greater viral suppression compared with non-DTG-containing cART, particularly in patients with a high baseline viral load (VL) (>100,000 copies/mL) or ≤200 CD4+ T cells/mm3.22,23 A DTG-based regimen also showed improved safety compared with the regimen of EFV-based cART.14,24 A report from Amhara Region, Ethiopia, showed that the average incidence rate for the four years 2015–2018 was 6.9 per 1000 HIV patients, and it was highest in Dessie, Bahir Dar, and Gondar, in descending order.25
Inadequate adherence, non-disclosed HIV status, preexisting drug resistance, regimen complexity, side effects, advanced clinical stage, and suboptimal pharmacokinetics can lead to patient attrition, persistent viral replication, and the evolution of drug resistance.26–28 Studies on the comparative safety and survival rates of DTG versus EFV-based ART have been conducted in some countries.23,29–31 However, there is a paucity of data on the safety and survival rates of DTG and EFV-based ART regimens in Ethiopia. Thus, this study aimed to compare the safety and survival rates of DTG and EFV-based regimens for first-line HIV treatment among HIV patients in North-West–East Ethiopia, Amhara Region.
Methods
Study Areas
The study was conducted in the HIV treatment centers of three selected hospitals: Dessie Specialized Hospital (DSH), Debre Tabor Referral Hospital (DRH), and Felege Hiwot Comprehensive Specialized Hospital (FHCSH), Amhara Region, North-West–East Ethiopia. DRH was established in 1931 GC in South Gondar Zone, North-West Ethiopia. It is 99 km from Bahir Dar, which is the seat of the Regional Government of Amhara, and 667 km north of Addis Ababa. It has 214 beds and provides both outpatient and inpatient services to a catchment population of more than 2.7 million people. It provides a service for around 1866 HIV patients. FHCSH was founded in 1971 GC and is located in Bahir Dar, North-West Ethiopia. It serves a catchment population of about 10 million, including HIV patients, with 492 beds. Currently, it serves 6635 HIV patients. DSH was established in 1962 GC and is located in South Wollo Zone, North-Central Ethiopia. Dessie town is 397 km east of Addis Ababa. It is expected to provide a comprehensive service for a population of about 12 million, with 597 beds. It has 5466 HIV patients currently on treatment.
Study Design and Period
A hospital-based retrospective cohort study design was used to collect demographic and clinical data from the medical records of HIV-infected patients who had a follow-up at an HIV treatment center between September 1, 2019 and August 30, 2020. The study populations were all HIV patients with detectable (≥50 copies/mL) VL, aged ≥3 years, and who had been on either a DTG or an EFV-based cART regimen.
Data Collection Procedures and Instrument
After reviewing different published articles, treatment entries, follow-up forms, patient registers, and laboratory requests, a data extraction tool was prepared and used to collect demographic, clinical, immunologic, and laboratory data. Since secondary data were collected, only the English version of the tool was used.
Two pharmacists and four BSc nurses were recruited as data collectors by providing training about the data collection procedures from patient charts using a structured questionnaire. Data collectors and the principal investigator undertook all necessary preventive actions for coronavirus disease 2019 (COVID-19). The trained data collectors extracted socio-demographic characteristics as well as clinical data on safety and survival from the patient charts using structured questionnaires. The principal investigator supervised the overall data collection process and checked for data completeness on a daily basis.
The validity and reliability of the data collection tool were tested on 5% of the total sample size outside the study site before the actual data collection time. Any errors or doubts and incompleteness were corrected accordingly. The data were cleaned up rigorously before analysis.
Data Analysis and Interpretation
The data were entered and analyzed using SPSS version 26. The mean and standard deviation for continuous variables and the frequency and percentage for categorical variables were computed using descriptive statistics in SPSS to summarize the socio-demographic and relevant clinical characteristics of the study participants. Tables and charts were used to present statistically and/or clinically significant results. After checking the proportional hazards assumption using the log minus log graph and time-dependent Cox model, the variables in bivariate analysis with p-value ≤0.2 were further analyzed in multivariate Cox regression to control the effect of confounders. Survival rates in months, using the time interval between the dates of VL measurements, were estimated by Kaplan–Meier, and differences in survival rates were tested by the log-rank statistic.
Results
Socio-Demographic, Clinical, and Laboratory Characteristics of Patients
Out of the 990 total study participants, 694 (70%) were taking a DTG-based regimen whereas 296 (30%) of them received an EFV-based regimen. An overall VL of <50 copies/mL was reported in 69% and 66% of the participants on the DTG and EFV-based regimens, respectively; and for patients with a baseline VL test exceeding 1000 copies/mL, this was decreased to a VL of <50 copies/mL in 38.0% in the DTG group and in 36.5% in the EFV group. Information on the patients who were enrolled and included in the study is depicted in Figure 1.
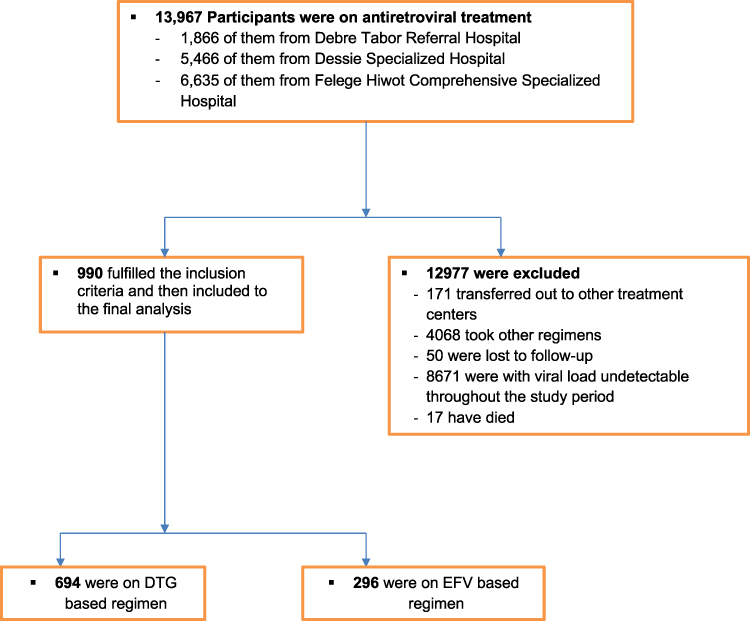 |
Figure 1 Schematic presentation of sampling procedure and technique in the evaluation of survival rate and safety outcome of DTG and EFV-based cART regimens among HIV-treated patients at DSH, DRH, and FHCSH, North-West–East Ethiopia, September 1, 2019 to August 30, 2020 (n=990). |
Demographic and clinical characteristics of patients at baseline were reasonably selected from the two treatment groups. The proportions of patients who were female, with initial VL ≥1000 copies/mL, baseline CD4+ T-cell count <200 cells/mm3, bed-ridden functional status, longer treatment duration, and young median age were higher in the EFV-based group compared to the DTG-based regimen. The baseline socio-demographic characteristics are shown in Table 1.
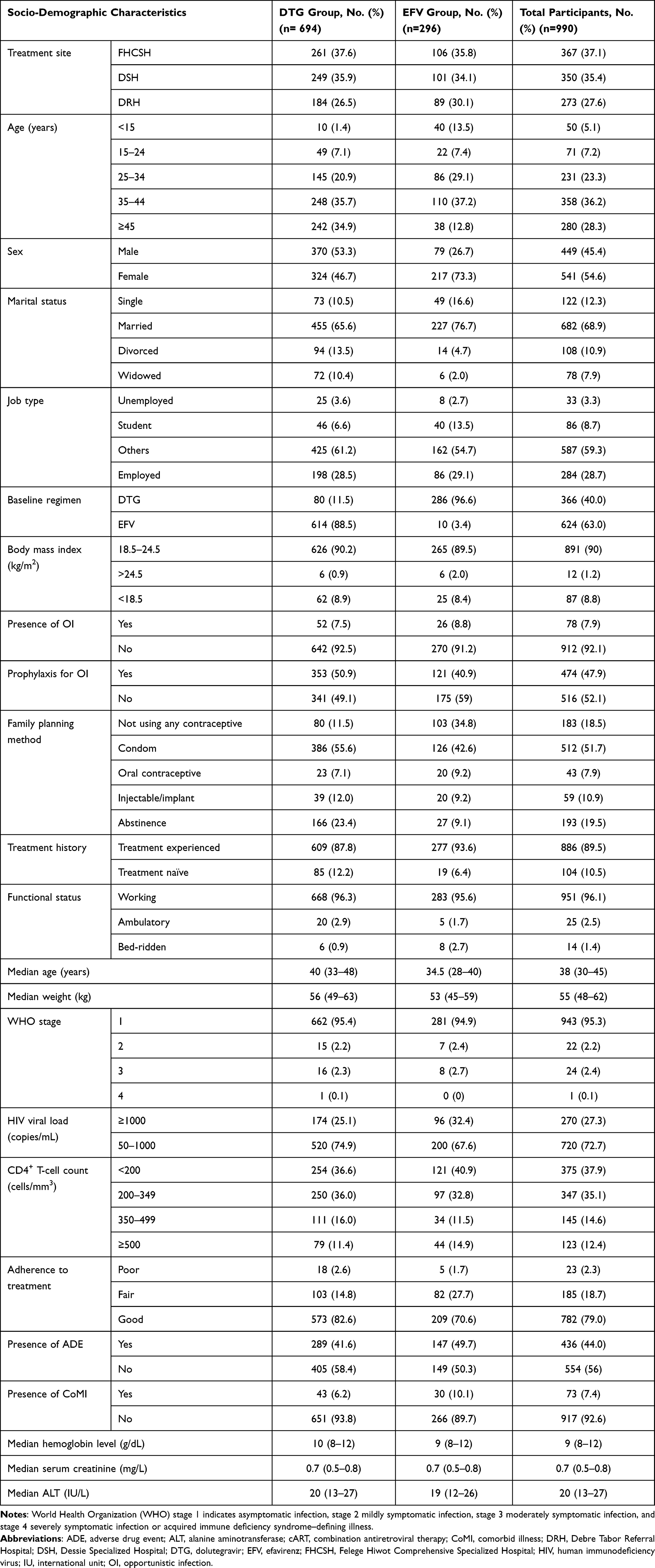 |
Table 1 Baseline Socio-Demographic and Clinical Characteristics of HIV Patients Treated with DTG and EFV-Based cART Regimens at DSH, DRH, and FHCSH, North-West–East Ethiopia, September 1, 2019 to August 30, 2020 (n=990) |
More than half (55%) of the participants resided in the hospital sub-city and 55% of them were female. The mean (SD) age of the participants was 38 (±13) years. The median baseline VL was 455 copies/mL and 270 (27%) of the participants had a baseline VL of ≥1000 copies/mL. The median CD4+ T-cell count was 235 cells/mm3, and 722 (73%) and 375 (38%) of the participants had a baseline CD4+ T-cell count of <350 and <200 cells/mm3, respectively. During the study period, 831 (95%) of the study participants were started with TDF + 3TC + EFV or DTG regimens compared to AZT or ABC + 3TC + EFV or DTG regimens.
Efficacy and Survival Rate
Since the ratio of events to hazards was small, the mean over the median survival was used to estimate the survival time (Table 2). The mean survival time using Kaplan–Meier analysis was 10.86 months (95% CI: 10.72–10.99). A significant (p=0.003) viral load reduction (VLR) was obtained in both regimen groups, with a higher reduction in the DTG group for a total of 636 out of 694 participants (91.6%) compared to the EFV-based regimen, 253 out of 296 participants (85.5%).
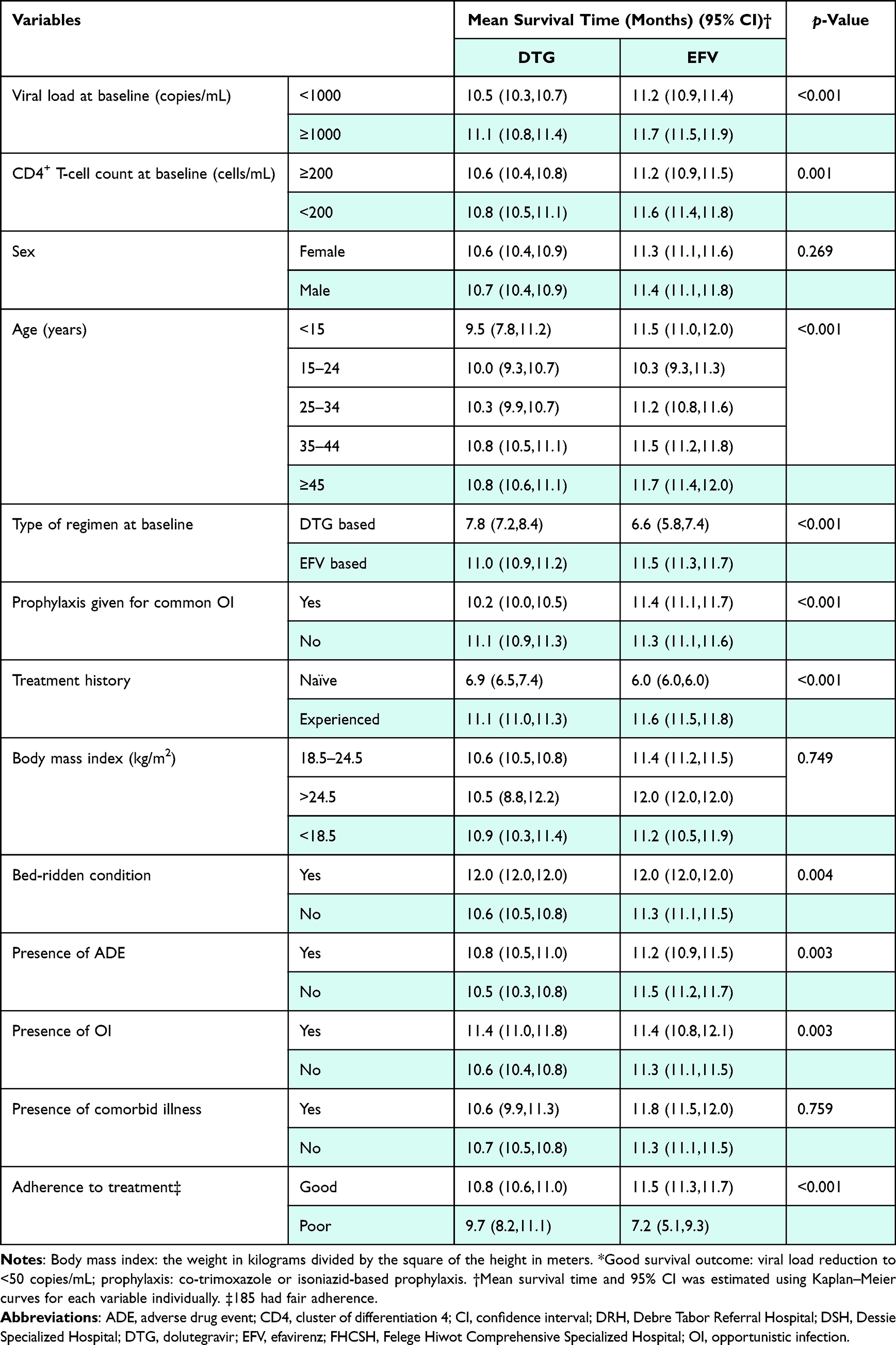 |
Table 2 Kaplan–Meier Analysis of Good Survival Outcome* and Associated Factors for DTG Compared to EFV-Based Regimen Among HIV Patients in DSH, DRH, and FHCSH, North-West–East Ethiopia, from September 1, 2019 to August 30, 2020 (n=990) |
On the basis of Kaplan–Meier analysis (Figure 2), the average time to achieve VL <200 copies/mL and <50 copies/mL was 10.43 months (95% CI: 10.26–10.60) and 10.65 months (95% CI: 10.48–10.81) in the DTG group, while it was 11.23 months (95% CI: 11.11–11.49) and 11.35 months (95% CI: 11.160–11.53) in the EFV group, respectively.
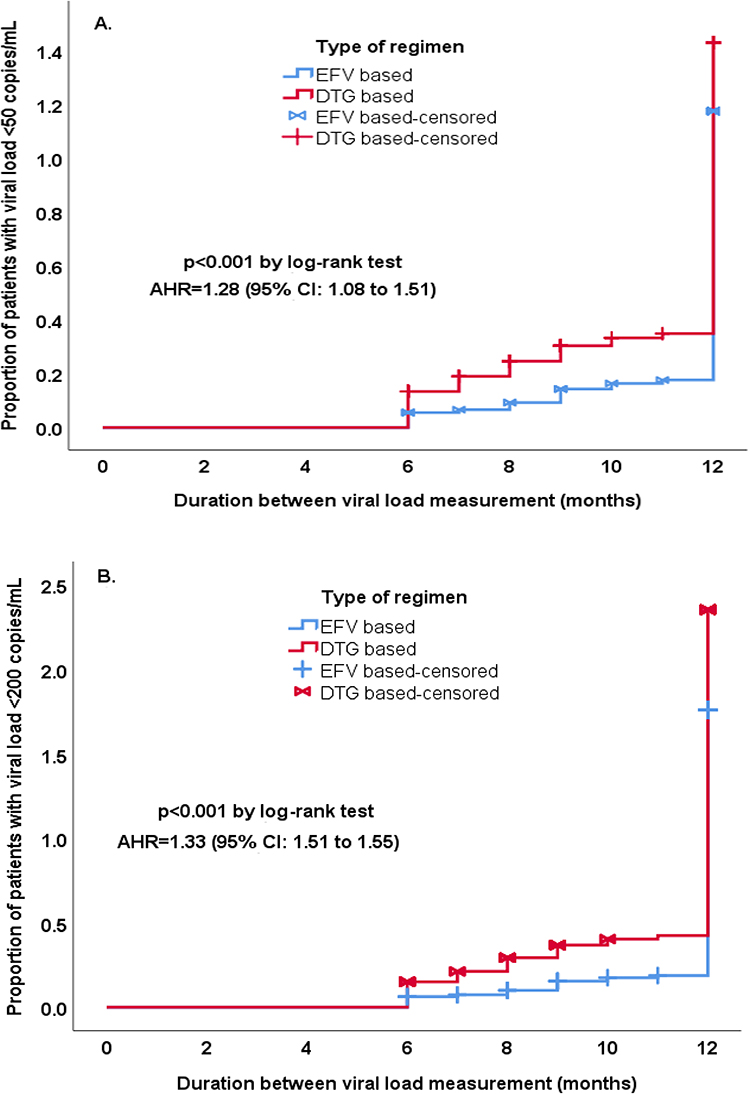 |
Figure 2 Proportion of patients with viral load <50 copies/mL and <200 copies/mL at final measurement. Kaplan–Meier plots of time from baseline to the final HIV viral load measurement value of (A) <50 copies/mL and (B) <200 copies/mL at FHCSH, DRH, and DSH, North-West–East Ethiopia, September 1, 2019 to August 30, 2020 (n=990). |
There were significant differences in VLR of <50 copies/mL between the two treatment groups: a total of 479 of 694 participants (69%) in the DTG group and 196 of 296 participants (66%) in the EFV group showed a VLR of <50 copies/mL. The difference between the two regimen groups was 3 percentage points (crude hazard ratio [CHR]=1.28, 95% CI: 1.08–1.51; p=0.004).
The median change from baseline in the VL during the study period was higher in the EFV treatment group, at 465 copies/mL (interquartile range [IQR] 176 to 1533) than in the DTG-based regimen, with 364 copies/mL (IQR 174 to 879). Among those patients with a baseline VL of ≥1000 copies/mL, a total of 66 out of 174 participants (38.0%) in the DTG group and 35 out of 96 participants (36.5%) in the EFV group had an undetectable VL, with a difference of 1.5 percentage points (adjusted hazard ratio [AHR]=0.45, 95% CI: 0.37–0.56; p<0.001).
A significantly higher number of patients reached a final VL threshold of <200 copies/mL in the DTG group (601 out of 694 participants [87%]) compared to the EFV group (237 out of 296 participants [80%]), with a risk difference of 7 percentage points (AHR=1.33, 95% CI: 1.15–1.55; p<0.001).
The difference in the numbers of women showing VL suppression <50 copies/mL between the DTG group (236 of 324 [73%]) compared with the EFV group (143 of 217 [66%]) was not statistically significant (p=0.422). Among those patients with a higher baseline VL (≥1000 copies/mL), 37% of them reached a VL of <50 copies/mL in the two regimen groups. A higher proportion of patients had virologic failure (VL of >1000 copies/mL) in the EFV group than in the DTG-based regimen (8 out of 296 [2.70%] vs 11 out of 694 [1.59%]).
The median change from baseline in the CD4+ T-cell count at one year was higher in the DTG group than in the EFV group (increase of 139 cells/mm3 [IQR 69 to 202] vs 100 cells/mm3 [IQR −35 to 164]). This change in CD4+ T-cell count between the two treatment groups was significant (p<0.001), with a higher mean score for DTG (M=117) than for EFV (M=67), and the mean difference of 50 (95% CI: 29–71).
There was a significant difference (p<0.041) in the number of participants who had a final CD4+ T-cell count of ≥200 cells/mm3 in the DTG group (646 out of 694 participants [93%]) compared with the EFV group (256 out of 296 [87%]), with a difference of 6 percentage points (AHR=1.162, 95% CI: 1.01–1.34). There was a significant difference in the mean score (p<0.001) for female participants who had a CD4+ T-cell count increase between the DTG group (M=124) and EFV group (M=60). The magnitude of the differences was higher in the DTG group, with a mean difference of 64 (95% CI: 3.86–90.54).
Safety and Tolerability
The safety profile of the DTG-based regimen was favorable compared to the EFV-based regimen. The number of HIV patients who had events of WHO stage 3 or higher was 10 out of 694 participants (1.44%) in the DTG group and seven out of 296 participants (2.36%) in the EFV group (p=0.140).
A greater, but non-significant, average weight gain was observed in the DTG group than in the EFV group (0.39 kg vs 0.32 kg), with a mean difference of 0.07 kg (p=0.647). Similarly, the mean weight change was non-significantly higher (p=0.819) in female patients of both regimen groups; 0.48 in DTG and 0.30 in the EFV-based regimen (95% CI: −0.004 to 0.145). A DTG-induced weight gain was observed more in participants who had a low body mass index (BMI <18.5 kg/m2) at the baseline of the study (AHR=1.33, 95% CI: 1.01–1.75; p=0.043), while a high BMI at baseline (>24.5 kg/m2) was protective against weight gain (AHR= 0.82, 95% CI: 0.34–1.97; p=0.651).
Although it was not significant (p=0.376), the proportion of patients who experienced ADEs was higher in the EFV group than the DTG group (147 of 296 [49.70%] vs 289 of 694 [41.64%]). Diarrhea (9.0%), insomnia (6.1%), and nausea (5.5%) were the most common ADEs in the DTG group, while diarrhea (12.5%), nausea (8.8), and insomnia (7.8%) were most common in the EFV group (Table 3).
 |
Table 3 Frequencies of Adverse Drug Events Experienced by HIV Patients Treated with DTG or EFV-Based Regimens at DSH, DRH, and FHCSH, North-West–East Ethiopia, from September 1, 2019 to August 30, 2020 (n=990) |
Adherence to treatment was better in the DTG group than for EFV-based regimens: 573 of 694 participants (83%) on the DTG-based regimen versus 209 out of 296 (71%) on the EFV-based regimen had good adherence (p<0.001).
HIV patients who took the EFV-based regimen non-significantly (p=0.109) experienced more disease complications during treatment compared to patients treated with the DTG-based regimen (11% vs 6%). Cardiovascular (9%), cancer (8%), and neurologic (8%) complications were common with EFV, and cancer (11%), cardiovascular (7%), and metabolic (6%) complications in the DTG-based regimen. The mean increase in serum creatinine was significantly higher in the EFV group (0.34) compared to the DTG group (0.30), with a mean difference of 0.04 (95% CI: −0.03 to 0.10; p=0.036), while the mean increase in ALT was 4.25 and 3.86, respectively, for the DTG and EFV-based regimens, with a mean difference of 0.389 (95% CI: −1.12 to 1.90; p=0.613). The average decrease in hemoglobin level in the EFV group was non-significantly (p=0.355) larger than that in the DTG group: 0.31 versus 0.29, with a mean difference of 0.02 (95% CI: −0.05 to 0.08).
Predictors of Survival Rate
A bivariate analysis using the Cox regression model was used to assess the predictors associated with poor survival outcome. The variables at a significance level of p<0.2 in the bivariate Cox regression model were age 25–34 years, sex, presence of OIs, bed-ridden functional status, occurrence of ADE, prophylaxis for common OIs, poor adherence to treatment, residence, and initial laboratory values of VL ≥1000 copies/mL and CD4+ T-cell count <200 cells/mm3. Level of education, job type, presence of comorbid illness, type of regimen, and BMI were not statistically significant predictors in the bivariate Cox analysis to fit the multivariate test. All of the variables that were predictors for poor survival outcome at the 0.2 significance level in the bivariate Cox regression analysis were included in the final multivariate Cox regression analysis (Table 4). According to the multivariate Cox regression model, HIV patients in the age group 25–34 years had 32% less risk for poor survival rate compared to patients ≥45 years old (AHR=0.68, 95% CI: 0.48–0.96; p=0.027). Those patients with bed-ridden functional status were at almost two times increased risk of poor survival outcome compared to the working group (AHR=1.98, 95% CI: 1.05–3.73; p=0.035). In addition, patients who experienced ADEs showed about 37% greater risk of poor survival outcome than those not experiencing ADEs (AHR=1.37, 95% CI: 1.10–1.71; p=0.005). Patients with OIs had a 68% greater risk (AHR=1.68, 95% CI: 1.21–2.34; p=0.002) and prophylaxis given for common OIs resulted in a 53% lower risk for poor survival rates (AHR=0.47, 95% CI: 0.37–0.60; p<0.001) compared to patients without OIs and no prophylaxis, respectively. Patients with baseline CD4+ T-cell count <200 cells/mm3 were at almost 1.5 times (AHR=1.46, 95% CI: 1.17–1.83; p=0.001) and those with baseline VL ≥1000 copies/mL at nearly three times (AHR=2.97, 95% CI: 2.38–3.72; p<0.001) increased risk of poor survival compared to those with a baseline CD4 count of ≥200 cells/mm3 and VL of <1000 copies/mL, respectively. Poor treatment adherence also increased the risk of poor response (VLR ≥50 copies/mL) by more than two times (AHR=2.25, 95% CI: 1.23–4.11; p=0.009) compared to patients with good adherence. On the other hand, the variables of participant sex and residence were not statistically significant as predictors for poor survival outcome.
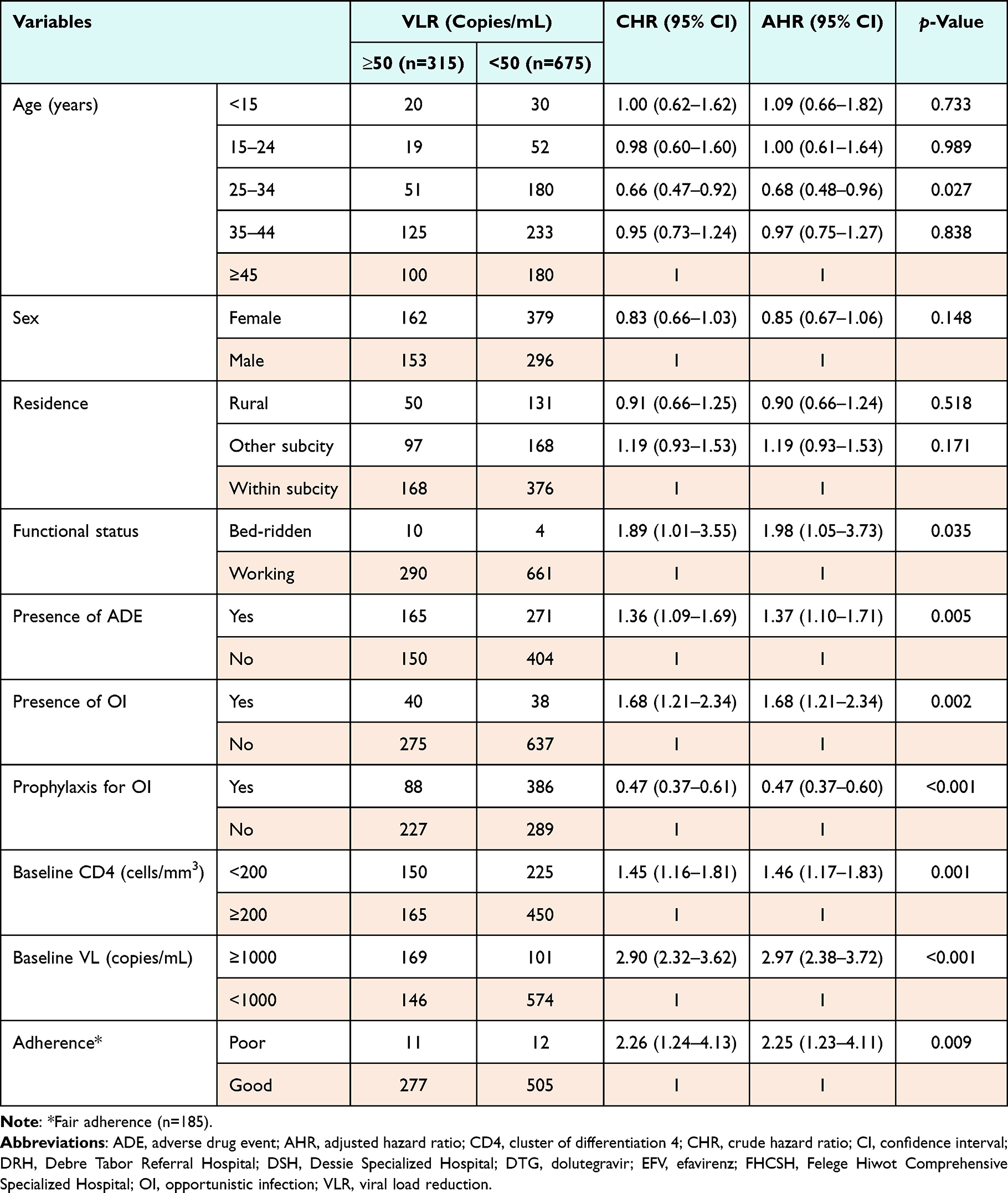 |
Table 4 Bivariate and Multivariate Cox Regression Analysis of Predictors Associated with Viral Load Reduction to ≥50 Copies/mL Among HIV Patients Treated with DTG and EFV-Based Regimens at DSH, DRH, and FHCSH, North-West–East Ethiopia, from September 1, 2019 to August 30, 2020 (n=990) |
Predictors of Safety
Of the total participants, 458 (46%) took at least two other drugs concomitantly with the cART regimen. Reasons or switching regimens were the introduction of a new drug (DTG-based regimen) in 595 patients (92.1%), toxicity/side effect in 25 (3.9%), drug stockouts in 11 (1.7%), forgetfulness in eight (1.2%), too ill in four (0.6%), and felt better in three patients (0.5%) (p<0.001).
On the bivariate Cox regression, covariates such as age groups 15–24 and 35–44 years old, poor adherence, DTG-based initial regimen, OIs, naïve treatment history, bed-ridden functional status, baseline VL ≥1000 copies/mL, baseline CD4 count <200 cells/mm3, and student job type were found to be significant predictors for the occurrence of ADEs at p<0.2, and these were candidates for multivariable Cox regression (Table 5). Participant sex, marital status, family planning method, presence of comorbid illness, BMI, and prophylaxis for common OIs were not found to be predictors of ADEs, so they were not tailored to multivariate analysis. During multivariable Cox regression, the age group 15–24 years was at more than two times (AHR=2.21, 95% CI: 1.60–3.05; p<0.001) increased risk and the age group 35–44 years was at 31% decreased risk (AHR=0.69, 95% CI: 0.53–0.89; p=0.004) for the occurrence of ADE compared to those aged ≥45 years. Poorly adherent patients had about 3.5 times greater risk for experiencing ADE than patients with good adherence (AHR=3.49, 95% CI: 2.13–5.70; p<0.001). Patients taking the DTG-based regimen at baseline were at almost three times higher risk for ADE compared to patients who took the EFV-based baseline regimen (AHR=2.85, 95% CI: 1.98–4.09; p<0.001). Moreover, patients infected with OIs had a 56% greater risk associated with the development of ADEs than non-infected patients (AHR=1.56, 95% CI: 1.17–2.09; p=0.003). Treatment-naïve HIV patients at baseline were at more than 10.5 times increased risk of developing ADEs than treatment-experienced patients (AHR=10.56, 95% CI: 7.21–15.48; p<0.001). The chance of developing ADEs in patients with baseline CD4 count <200 cells/mm3 was increased by 21% compared to those with ≥200 cells/mm3 (AHR=1.21, 95% CI: 1.01–1.47; p=0.045). Student job type, which increases the risk by more than two times (AHR=2.12, 95% CI: 1.55–2.90; p<0.001), was also identified as an independent predictor of cART-related ADEs at the p<0.05 significance level. Variables of functional status and baseline VL were not statistically significant predictors for treatment safety.
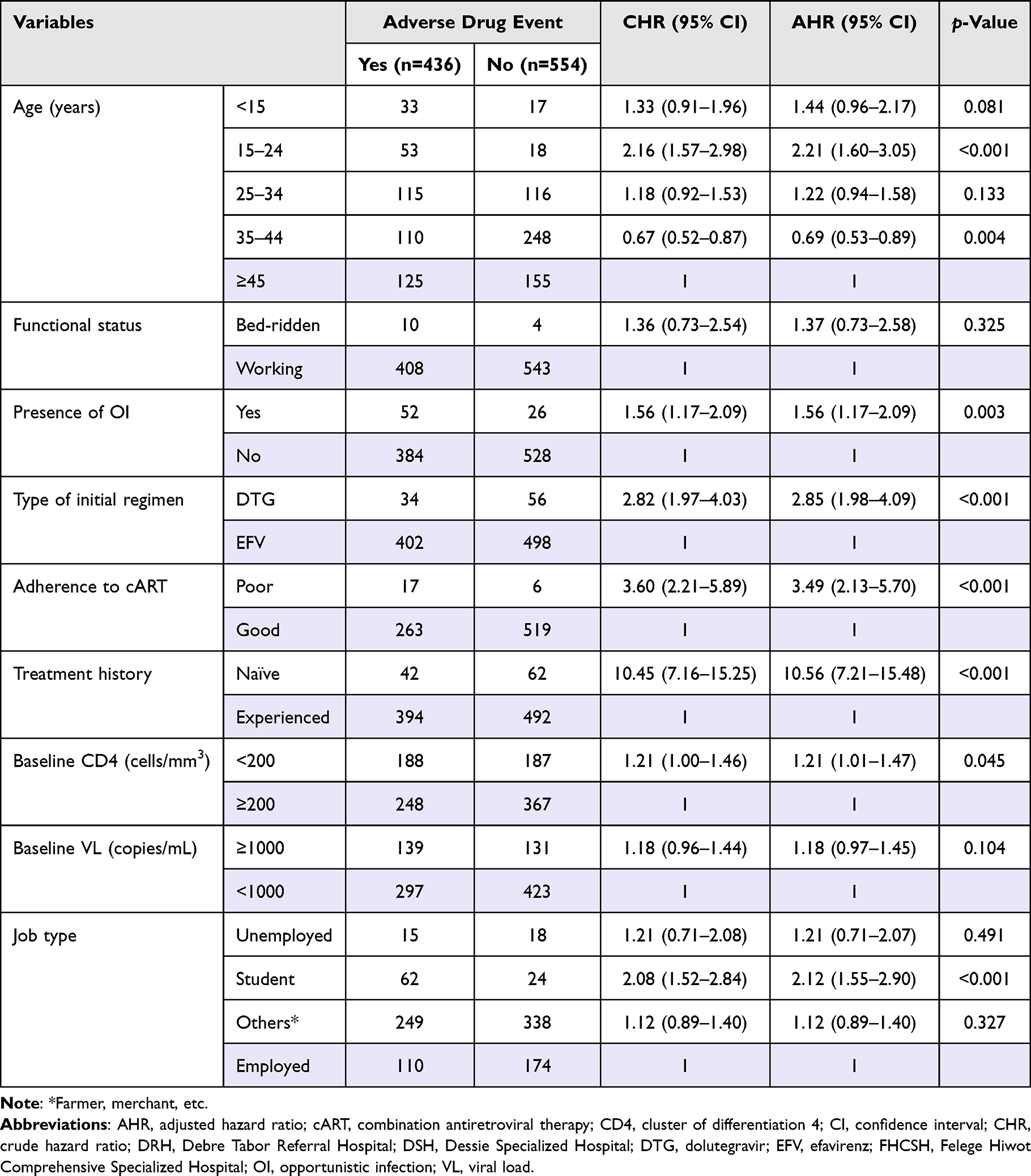 |
Table 5 Bivariate and Multivariate Cox Regression Analysis of Predictors Associated with the Occurrence of Adverse Drug Events Among HIV Patients Treated with EFV and DTG-Based Regimens at DSH, DRH, and FHCSH, North-West–East Ethiopia, September 1, 2019 to August 30, 2020 (n=990) |
At any given time, HIV patients with comorbid illness had a more than 13 times higher risk of developing a treatment complication (AHR=13.42, 95% CI: 8.52–21.15; p<0.001) than those who had no comorbid condition. A unit change in the total number of drugs taken during treatment increases the chance of experiencing ADEs by 22% (AHR=1.22, 95% CI: 1.11–1.34; p<0.001) and complications by 83% (AHR=1.83, 95% CI: 1.60–2.09; p<0.001). For each g/dL increase in blood hemoglobin level, there was an increase in survival of about 5% (AHR=1.05, 95% CI: 1.01–1.09; p=0.013).
Discussion
This study aimed to assess the survival rate and safety profile of DTG-based regimens compared to EFV-based antiretroviral therapy. Among the 990 study participants, 315 (32%) and 436 (44%) had poor VL outcome and low safety profile, respectively. Moreover, the survival rate and safety results from this 48-week retrospective study were poorer compared with other similar studies conducted for the same duration.32–35 Unlike the many reference trials discussed here, the demographics, type of patients (ART-exposed and ART-naïve HIV-infected patients), and clinical characteristics at baseline were not balanced between the treatment groups. The proportion of patients who were female, with initial VL ≥1000 copies/mL, baseline CD4+ T-cell count <200 cells/mm3, bed-ridden functional status, longer treatment duration, and young median age were higher in the EFV-based compared to the DTG-based regimen. This is because DTG-based regimens are not recommended for pregnant and breast-feeding mothers, females of child-bearing age without a consistent contraceptive method, children younger than 10 years, and unstable patients, according to Ethiopian HIV treatment guidelines.36
There are many controversies regarding the use of DTG for pregnant women among studies, including those released after the Ethiopian HIV treatment guidelines had been published. Some articles found adverse birth outcomes, especially neural tube defects, from DTG-based regimens, whereas in other studies adverse birth outcomes were similar among pregnant women who initiated both EFV and DTG-based regimens.29,37 DTG-based regimens are reported to have better survival and lower overall HIV transmission than EFV-based regimens, and are recommended for all adults regardless of pregnancy or child-bearing potential, because of their public health benefits and cost effectiveness.29,38,39
The survival rates in the current study, based on the proportion of participants who had reduced VL <50 copies/mL in both regimen groups (69% in DTG and 66% in EFV), were lower compared to those in previous studies.14,35,40–42 The higher survival rate achieved by previous studies may be due to the higher socio-economic status of patients, the availability of baseline resistance screening, the type of nucleoside reverse transcriptase inhibitor (NRTI), a more frequent and extended follow-up schedule, and the awareness of patients being followed by data collectors. The survival rate was also lower for a VL threshold of <200 copies/mL: 86.6% and 80.07% of the participants in the DTG and EFV groups, respectively, compared to the 2019 study by Charles Kouanfack and Bassega in Cameroon.35 The discrepancy could be due to the naïve participants’ treatment history and lower baseline immune status in the reference trial, as indicated in other studies.14,35,37 In the present study, treatment-naïve HIV patients comprised only 104 participants (10.5%), and about 38% had CD4 <200 cells/mm3, whereas in the Cameroon study, all patients were treatment naïve and 33% had a baseline CD4+ cell count of <200 cells/mm3.
The average time taken to achieve VLR <50 copies/mL by DTG was shorter compared to the EFV-based regimen (10.65 months in DTG and 11.35 months in EFV). This finding is similar to the results from a clinical trial from 2015 (28 vs 84 days)14 and a randomized study conducted for 3 years (4 months).40 However, the time taken to reach this endpoint was too long in both regimen groups in this study. This was probably due to the VL measurement being carried out a maximum of two times in our study, while it was more frequent in the previous trial and randomized study.
A lower number of HIV patients in both regimen groups (1.6% of participants in the DTG group and 2.7% in the EFV group) had virologic failure. This finding deviated from the findings of other studies (international study 2.3% and 2.9%; Johannesburg, South Africa 14% and 19%; and Italy 6.6% and 4.8%, respectively).14,41,43,44 The higher virologic failure in the reference studies resulted from their better study design, study set-up, follow-up period, time of ART initiation, and treatment history, as stated in a 2019 study from Germany.45 In addition, the proportion of patients who had a VL of <1000 copies/mL at baseline was 73%, but all patients in the reference study had a baseline VL of ≥1000 copies/mL. However, the level of treatment failure in the DTG group (1.6%) was higher compared to the Cameroon study (<1%).35 This may be due to the higher baseline CD4+ T-cell count and use of TDF-based NRTIs in their patients, as supported by a study from Italy.44 Treatment failure for the EFV group (2.7%) was also higher compared with that found in a clinical trial in West Central Europe (2.2%), in 2020.46 This may be because of the larger sample size, the higher median baseline CD4, and the higher level of significance, together with the different study set-up and design in the European study. This was also supported by a study from Italy.44
Even though it was not statistically significant, VL suppression of <50 copies/mL in women (73% in DTG and 66% in EFV-based regimens) was less than reported in other comparative studies.14,35,41 The observed differences may be due to a higher proportion of women being treatment experienced, as treatment history was a predictor for VLR in a study from Germany.45 The lower socio-economic status of our study participants, which may lead to difficulties accessing HIV treatment and inadequate counseling, could be another possible issue to be considered.
The median increase in CD4+ T-cell counts from baseline was 138.5 cells/mm3 in DTG and 100 cells/mm3 in the EFV treatment group. This is far lower than the findings of other studies (Cameroon 178 and 150; international study 220 and 190; SINGLE study 267 and 208; SPRING-1 study 338 and 301; and Spain 325 and 281, respectively).14,35,40,42,43,47 This may be due to the higher baseline immune status of the study patients. Likewise, the longer follow-up period, rapid initiation of ART, naïve treatment history, robust methodology, and the study set-ups may play a role in this variation. A higher level of non-adherence associated with treatment and prophylaxis, a higher prevalence of OIs and lower prophylaxis coverage, poor nutritional condition, low socio-economic level, and low educational background in our study participants could also have an impact on the observed inconsistencies, as previously reported in a study from Southern Ethiopia.48
In the present study, patients with bed-ridden functional status were at almost two times increased risk of poor survival outcome compared to working groups. Patients who experienced ADEs and OIs also showed about 37% and 68% greater risk of poor survival outcome, respectively. The 25–34 year age group had 32% and patients given prophylaxis for common OIs had 53% protective effect for survival compared to patients ≥45 years old and without prophylaxis, respectively. Patients with a baseline CD4+ T-cell count <200 cells/mm3 were at almost 1.5 times and those with baseline VL ≥1000 copies/mL were at nearly three times increased risk of poor survival compared to those with a baseline CD4 of ≥200 cells/mm3 and a VL <1000 copies/mL, respectively. Poor treatment adherence also increased the risk of poor response (VLR ≥50 copies/mL) by more than two times compared to patients with good adherence. The findings are in line with other studies.48,49 In addition, the lower CD4 and higher VL at baseline as independent predictors of poor survival rate were comparable to studies elsewhere.14,35,37,44,48 Nevertheless, this result totally deviates from the findings from a study in South Africa.41 The discrepancy may be due to their better study design and baseline patient characteristics, nutritional status, healthcare system, resources allocated, and study settings, with various healthcare professionals’ expertise and hospitals’ infrastructure.
The survival rate of HIV patients in the presence of OIs in DTG was similar to the EFV-based regimen. In contrast to this result, the VLR achieved by DTG was lower than on the EFV-based regimen (75% vs 84%) in patients co-infected with tuberculosis, in a clinical trial conducted in seven countries.43 This could be due to the drug–drug interactions of DTG with rifampicin and the different baseline VL of the two regimen groups, as noted in other studies.35,50 On the other hand, the younger age group somewhat increased the risk of poor survival rate compared to older patients. This is supported by a study from South Africa, in which older patients achieved a higher VLR compared to younger ones.41 There was also a lower virologic reduction in the age group of <18 years in a cohort from the USA compared to patients ≥18 years old in other studies.14,42,51 In contrast to this, in a trial from North America, Europe, and Australia, with age groups divided at 50 years, VLR by older patients was lower than in younger patients.14 This may be due to their better study design, extended study period, higher comorbid condition, and lower immune status.
On the issue of safety, the incidence of ADEs was lower in both regimen groups in this study (49.7% in EFV and 41.6% in the DTG group) compared to previous studies (SPRING study 62% and 55%; and SINGLE study 54.7% and 24.2%, respectively).14,40,41 The reasons for patients developing few ADEs may be related to inadequate follow-up time and frequency. In this study, the follow-up schedule was too short and the frequency of detecting ADEs was common since starting the treatment in a few months. The present study revealed that being treatment naïve had about 10 times the risk of having ADEs compared to treatment-experienced patients, and neuropsychiatric ADEs were the most frequent reasons for regimen change in HIV treatment. This is similar to the findings of a study from Italy.52 The prevalence of diarrhea, nausea, headache, fatigue, and insomnia was similarly high in DTG-based regimens compared with a study conducted in the USA and Canada in 2017.53 The incidence of psychiatric disorders, such as insomnia, anxiety, and depression, was lower than in a study from North America, Europe, and Australia.14 Such variations could be due to the lack of a standardized method for identifying, assessing, classifying, and recording ADEs in our study participants. In this study, there were no abnormal laboratory values or severe ADEs that led to treatment discontinuation. This result is in contrast to the findings of a study conducted at 34 sites in France, Germany, Italy, Russia, Spain, and the USA.40 This may be due to our poor and less restricted follow-up, besides the differences in institutional laboratory services.
The percentages of participants who had WHO stage ≥3 events, which were 1.44% in the DTG and 2.36% in the EFV group, were low in this study compared with those in the study conducted in Cameroon (5.2% and 5.9%).35 Patients in this study were clinically stable at baseline (97.5% of participants were in stages I and II) and virally suppressed. This good baseline patient condition may be the reason for their attaining non-advanced WHO clinical stages.
The risk of ADEs in the age groups 15–24 and 35–44 years was increased more than twice and decreased by 31%, respectively, compared to age ≥45 years. Being younger in age and having a student job type also increased the risk of cART-related ADEs by more than two times. In contrast to this result, younger age was protective in a study from Italy.52 The difference may be due to only severe ADEs being recorded. In addition, they had a higher proportion of treatment-naïve patients and TDF-based NRTI regimens, as noted in a study from Aksum, Ethiopia.54
Poorly adherent patients had about 3.5 times greater risk of experiencing ADEs than patients with good adherence. Patients taking the DTG-based regimen at baseline were at almost three times higher risk of ADEs compared to patients who took the EFV-based baseline regimen. Moreover, patients infected with OIs had a 56% greater risk of developing ADEs than non-infected patients, but these results were not significant or protective factors for developing ADEs in Aksum, Ethiopia (0.72, 95% CI: 0.45–1.14).54 A possible reason for this discrepancy may be that the study from Aksum counted only severe forms of ADE and had half the sample size of this study. The chance of developing ADEs in patients with baseline CD4 count <200 cells /mm3 was increased by 21% compared to those with ≥200 cells/mm3, whereas baseline CD4 was not significant in a study from Italy.52 This may be due to their longer study time, and better study setting and design.
The average body weight gain (0.39 kg in DTG and 0.32 kg in EFV) was non-significant and was much lower than in studies conducted elsewhere.34,35,55 Being treatment naïve was reported as a significant predictor of weight gain in previous studies34,55 while more of the participants in this study were treatment experienced. In addition, this may be due to the poor lifestyle and nutritional status of these study participants.
Type of baseline regimen was not a predictor of survival rate in the current study, whereas it was a significant predictor in a cohort study from Italy.44 This may be due to the larger sample size, type of NRTI used, strong study method, and better study setting in the Italian study.
Limitations of the Study
As the study design was retrospective, not all of the required information could be traced from the patient charts, and the sample size was also relatively small for generalizability. Moreover, potentially confounding factors, such as the duration of ART before switching, were not examined. Since the study was based on secondary data, it is difficult to ascertain both the survival and safety outcomes of DTG compared to EFV-based regimens. There may also be differences in the measurement of each study variable across health professionals, which could result in the underestimation or overestimation of safety and survival outcomes. As per the standard, the VL measurement schedules took a minimum of two times per-year, however in this study setting the VL measurement schedules took longer (≥12 months), due to this the patients may reach an endpoint (VL <50 copies/mL) lately to determine the difference in survival rate. Predictors such as blood glucose level, nutritional status, and vital signs were not included as they were not fully documented on the patient register and, as a result, they were totally left out from the analysis.
Conclusion
The DTG-based regimen showed an improved safety, viral suppression ,and CD4 cell recovery profile compared with the EFV-based regimen for the treatment of HIV-infected patients. Age from 15 to 24 years, presence of OIs, increased total number of drugs, type of initial regimen being DTG, poor treatment adherence, naïve treatment history, low baseline CD4+ T-cell count (<200 cells/mm3), and being a student were predictors of poor safety outcomes, whereas age 35–44 years was a protective factor.
The DTG-based regimen improved the survival rate over the EFV-based regimen in the treatment of HIV-infected patients. Bed-ridden functional status, poor treatment adherence, high baseline VL, low baseline CD4+ T-cell count, lower baseline hemoglobin level, presence of ADEs, and presence of OIs were predictors of poor survival outcomes, whereas age 25–34 years and prophylaxis for common OIs improved the survival rate.
Recommendations
It would be better to conduct such a study prospectively, with an extended period and repeated measures of important indicators. Policy makers should revise the guidelines and researchers need to review the efficacy and safety of DTG for pregnant mothers and young children. Local health bureaus, in collaboration with other stakeholders, need to work continually to improve patient adherence to their cART and OI prophylaxis and treatment. Health institutions need to strengthen their data recording and record-keeping practices, as well as patient follow-up. Moreover, more attention should be given to clinically unstable patients who have low CD4 counts and high VL measurements.
Abbreviations
ABC, abacavir; ADE, adverse drug event; AHR, adjusted hazard ratio; AIDS, acquired immune deficiency syndrome; ART, antiretroviral therapy; cART, combination antiretroviral therapy; CD4, cluster of differentiation 4; CHR, crude hazard ratio; DTG, dolutegravir; EFV, efavirenz; HIV, human immunodeficiency virus; NRTI, nucleoside reverse transcriptase inhibitor; OI, opportunistic infection; 3TC, lamivudine; TDF, tenofovir; VL, viral load; VLR, viral load reduction; WHO, World Health Organization.
Data Sharing Statement
All relevant data are included in the article and uploaded as supporting information files. Extra data can be accessed upon reasonable request to the corresponding author. This paper is based on the thesis of Melese Alemnew. It has been published on the institutional website.56
Ethics Approval and Consent to Participate
In accordance with the Declaration of Helsinki (1964), ethical approval was obtained from the Ethics Review Committee of the School of Pharmacy, College of Health Sciences, Addis Ababa University, through a letter reference number of ERB/SOP/202/09/2020. The School of Pharmacy Ethical Review Committee and the three hospitals’ quality assurance departments and HIV focal person to access patients’ data waived the requirement for informed consent. All methods were carried out in accordance with the relevant guidelines and regulations. Only numerical identifications were used as a reference. The confidentiality and anonymity of the subjects was maintained by not recording identifying details, such as names or any other personal identifiers.
Acknowledgments
We would like to express our gratitude to all data collectors and support staff working in the medical record rooms of Dessie Specialized Hospital (DSH), Debre Tabor Referral Hospital (DRH), and Felege Hiwot Comprehensive Specialized Hospital (FHCSH), and patients and family members who provided information during data collection. Finally, we would like to thank our friends for their valuable technical support.
Author Contributions
Both authors have made a substantial contribution to the work reported, be it in conception, design, conduct, acquisition of data, analysis and interpretation, or all of these; both have participated in drafting, revising, or critically reviewing the article; both have given final approval of the version to be published; they have agreed to submit the article to the journal; and they have agreed to take responsibility for all aspects of the work.
Funding
The study was conducted with the financial support of Addis Ababa University.
Disclosure
The authors declare that they have no competing interests.
References
1. Sax PE, Kuritzkes DR. HIV essentials. Jones & Bartlett Learning; 2017. Available from: https://www.amazon.com/HIV-Essentials-2017-Paul-Sax/dp/1284124703.
2. Lu D, Lu T, Wu H, Che J. Challenges for HIV/AIDS therapy. Adv Pharmacoepidemiol Drug Saf. 2013;2(4):e120.
3. UNAIDS. Fact sheet - latest global and regional statistics on the status of the AIDS epidemic; 2022.
4. WHO. HIV fact sheet; 2020. Available from: https://www.who.int/news-room/fact-sheets/detail/hiv-aids.
5. Pau AK, Clifford Lane H. Guidelines for the use of antiretroviral agents in adults and adolescents living with HIV. Panel on Antiretroviral Guidelines for Adults and Adolescents; 2018.
6. Jason J, Schafer JMC, Elizabeth M, et al. HIV pharmacotherapy: the pharmacist’s role in care and treatment. In: American Society of Health-System Pharmacists. Elsevier; 2018.
7. Kanters S, Vitoria M, Doherty M, et al. Comparative efficacy and safety of first-line antiretroviral therapy for the treatment of HIV infection: a systematic review and network meta-analysis. Lancet HIV. 2016;3(11):e510–e520. doi:10.1016/S2352-3018(16)30091-1
8. Federal Ministry of Health. Implementation Manual for DTG Rollout and ART Optimization in Ethiopia. Ethiopia: Federal Ministry of Health; 2019.
9. Fantauzzi A, Turriziani O, Mezzaroma I. Potential benefit of dolutegravir once daily: efficacy and safety. HIV AIDS. 2013;5:29–40.
10. Dow DE, Bartlett JA. Dolutegravir, the second-generation of Integrase Strand Transfer Inhibitors (INSTIs) for the treatment of HIV. Infect Dis Ther. 2014;3(2):83–102. doi:10.1007/s40121-014-0029-7
11. Kandel CE, Walmsley SL. Dolutegravir - a review of the pharmacology, efficacy, and safety in the treatment of HIV. Drug Des Devel Ther. 2015;9:3547–3555. doi:10.2147/DDDT.S84850
12. Vitoria M, Hill A, Ford N, et al. The transition to dolutegravir and other new antiretrovirals in low- and middle-income countries – what are the issues? HIV Global Hepatitis Program. 2018;32(12):1551–1561.
13. Cruciani M, Malena M. Combination dolutegravir-abacavir-lamivudine in the management of HIV/AIDS: clinical utility and patient considerations. Patient Prefer Adherence. 2015;9:299–310. doi:10.2147/PPA.S65199
14. Walmsley SL, Antela A, Clumeck N, et al. Dolutegravir plus abacavir/lamivudine for the treatment of HIV-1 infection in antiretroviral therapy-naive patients: week 96 and week 144 results from the SINGLE randomized clinical trial. Brief Rep. 2015;70:515–519.
15. Dehority W, Abadi J, Wiznia A, Viani RM. Use of integrase inhibitors in HIV-infected children and adolescents. Drugs. 2015;75(13):1483–1497. doi:10.1007/s40265-015-0446-2
16. Bruzzese E, Lo Vecchio A, Smarrazzo A. Dolutegravir-based anti-retroviral therapy is effective and safe in HIV-infected paediatric patients. Ital J Pediatr. 2018;44(1):37. doi:10.1186/s13052-018-0469-x
17. Fourati S, Charpentier C, Amiel C. Cross-resistance to elvitegravir and dolutegravir in 502 patients failing on raltegravir: a French national study of raltegravir-experienced HIV-1-infected patients. J Antimicrob Chemother. 2015;70(5):1507–1512. doi:10.1093/jac/dku535
18. Miller M, Liedtke MD, Rathbun RC, Lockhart SM. The role of dolutegravir in the management of HIV infections. Infect Drug Resist. 2015;19. doi:10.2147/IDR.S58706
19. Saladini F, Giannini A, Boccuto A, et al. Comparable in vitro activities of second-generation HIV-1 integrase strand transfer inhibitors (INSTIs) on HIV-1 clinical isolates with INSTI resistance mutations. Antimicrob Agents Chemother. 2019;64(1):e01717–01719. doi:10.1128/AAC.01717-19
20. Ethiopian Public Health Institute. HIV Related Estimates and Projections in Ethiopia for the Year 2021–2022. Addis Ababa: Ethiopian Public Health Institute; 2022.
21. UNAIDS/WHO/UNICEF UWaWHCIT. HIV country profile-Ethiopia. In: Global AIDS Monitoring. UNAIDS/WHO/UNICEF UWaWHCIT; 2017.
22. Cruciani M, Parisi SG, De Socio GV. Dolutegravir based antiretroviral therapy compared to other combined antiretroviral regimens for the treatment of HIV-infected naive patients: a systematic review and meta-analysis. PLoS One. 2019;14(9):e0222229. doi:10.1371/journal.pone.0222229
23. Snedecor SJ, Radford M, Kratochvil D, Grove R, Punekar YS. Comparative efficacy and safety of dolutegravir relative to common core agents in treatment-naive patients infected with HIV-1: a systematic review and network meta-analysis. BMC Infect Dis. 2019;19(1):484. doi:10.1186/s12879-019-3975-6
24. Walmsley SL, Antela A, Clumeck N. Dolutegravir plus abacavir–lamivudine for the treatment of HIV-1 infection. N Engl J Med. 2013;369(19):1807–1818. doi:10.1056/NEJMoa1215541
25. Worku ED, Asemahagn MA, Endalifer ML. Epidemiology of HIV infection in the Amhara Region of Ethiopia, 2015 to 2018 surveillance data analysis. HIV AIDS. 2020;12:307–314.
26. Paul E, Sax CJC, Daniel R. HIV Essentials.
27. Abebe Moges N, Olubukola A, Micheal O, Berhane Y. HIV patients retention and attrition in care and their determinants in Ethiopia: a systematic review and meta-analysis. BMC Infect Dis. 2020;20(1):439. doi:10.1186/s12879-020-05168-3
28. Alemseged Abdissa A, D. Y, Fonager J, et al. Drug resistance in HIV patients with virological failure or slow virological response to antiretroviral therapy in Ethiopia. BMC Infect Dis. 2014;14(1):181. doi:10.1186/1471-2334-14-181
29. Zash R, Jacobson DL, Diseko M, et al. Comparative safety of dolutegravir-based or efavirenz-based antiretroviral treatment started during pregnancy in Botswana: an observational study. Lancet Global Health. 2018;6(7):e804–e810. doi:10.1016/S2214-109X(18)30218-3
30. Kanters S, Vitoria M, Zoratti M, et al. Comparative efficacy, tolerability and safety of dolutegravir and efavirenz 400mg among antiretroviral therapies for first-line HIV treatment: a systematic literature review and network meta-analysis. EClinicalMed. 2020;28:100573. doi:10.1016/j.eclinm.2020.100573
31. Nickel K, Halfpenny NJ, Snedecor SJ, Punekar YS. Comparative efficacy, safety and durability of dolutegravir relative to common core agents in treatment-naïve patients infected with HIV-1: an update on a systematic review and network meta-analysis. BMC Infect Dis. 2021;21(1):1–11.
32. Zhong M, Li M, Qi M, et al. A retrospective clinical study of dolutegravir-versus efavirenz-based regimen in treatment-naïve patients with advanced HIV infection in Nanjing, China. Front Immunol. 2023;13:7927. doi:10.1038/s41467-022-35607-5
33. Chan P, Yoon B, Colby D, et al. Immunological, cognitive, and psychiatric outcomes after initiating efavirenz-and dolutegravir-based antiretroviral therapy during acute human immunodeficiency virus infection. Clin Infect Dis. 2023;76(3):e718–e726.
34. Bourgi K, Rebeiro PF, Turner M, et al. Greater weight gain in treatment naïve persons starting dolutegravir-based antiretroviral therapy. Clin Infect Dis. 2020;70:1267–1274.
35. Charles Kouanfack MM-E, Bassega PO. Dolutegravir-based or low-dose efavirenz–based regimen for the treatment of HIV-1. N Engl J Med. 2019;381(9):816–826.
36. FMoH E. National Consolidated Guidelines for Comprehensive HIV Prevention, Care and Treatment. Federal Ministry of Health; 2018.
37. Kintu K, Malaba TR, Nakibuka J, et al. Dolutegravir versus efavirenz in women starting HIV therapy in late pregnancy (DolPHIN-2): an open-label, randomised controlled trial. Lancet HIV. 2020;7:e332–e339.
38. Dugdale CM, Ciaranello AL, Bekker LG. Risks and benefits of dolutegravir- and efavirenz-based strategies for South African women with HIV of child-bearing potential: a modeling study. Ann Intern Med. 2019;170(9):614–625. doi:10.7326/M18-3358
39. Phillips AN, Venter F, Havlir D, et al. Risks and benefits of dolutegravir-based antiretroviral drug regimens in sub-Saharan Africa: a modelling study. Lancet HIV. 2019;6(2):e116–127. doi:10.1016/S2352-3018(18)30317-5
40. Hans-Ju¨rgen Stellbrink H-J, Reynes J, Lazzarin A. Dolutegravir in antiretroviral-naive adults with HIV-1: 96-week results from a randomized dose-ranging study. AIDS. 2013;27(11):1771–1778. doi:10.1097/QAD.0b013e3283612419
41. Venter WDF, Sokhela S, Simmons B. Dolutegravir with emtricitabine and tenofovir alafenamide or tenofovir disoproxil fumarate versus efavirenz, emtricitabine, and tenofovir disoproxil fumarate for initial treatment of HIV-1 infection (ADVANCE): week 96 results from a randomised, Phase 3, non-inferiority trial. Lancet HIV. 2020;7(10):e666–e676. doi:10.1016/S2352-3018(20)30241-1
42. Van Lunzen J, Maggiolo F, Arribas JR. Once daily dolutegravir (S/GSK1349572) in combination therapy in antiretroviral-naive adults with HIV: planned interim 48 week results from SPRING-1, a dose-ranging, randomised, phase 2b trial. Lancet Infect Dis. 2012;12(2):111–118. doi:10.1016/S1473-3099(11)70290-0
43. Allan R, Tenorio BG, Talarico CL, et al. Plasma dolutegravir-based antiretroviral therapy for patients coinfected with tuberculosis and human immunodeficiency virus: a multicenter, noncomparative, open-label, randomized trial. Clin Infect Dis. 2020;70(4):549–556.
44. Gianotti N, Lorenzini P, Cozzi-Lepri A, et al. Durability of different initial regimens in HIV-infected patients starting antiretroviral therapy with CD4+ counts <200 cells/mm3 and HIV-RNA >5 log10 copies/mL. J Antimicrob Chemother. 2019;74(9):2732–2741. doi:10.1093/jac/dkz237
45. Brehm TT, Franz M, Hufner A, et al. Safety and efficacy of elvitegravir, dolutegravir, and raltegravir in a real-world cohort of treatment-naive and -experienced patients. Medicine. 2019;98(32):e16721. doi:10.1097/MD.0000000000016721
46. Neesgaard B, Mocroft A, Zangerle R, et al. Virologic and immunologic outcomes of treatment with integrase inhibitors in a real-world setting: the RESPOND cohort consortium. PLoS One. 2020;15(12):e0243625. doi:10.1371/journal.pone.0243625
47. Blanco JR, Alejos B, Moreno S. Impact of dolutegravir and efavirenz on immune recovery markers: results from a randomized clinical trial. Clin Microbiol Infect. 2018;24(8):900–907. doi:10.1016/j.cmi.2017.11.016
48. Abuto W, Abera A, Gobena T, Dingeta T, Markos M. Survival and predictors of mortality among HIV positive adult patients on highly active antiretroviral therapy in public hospitals of Kambata Tambaro Zone, Southern Ethiopia: a retrospective cohort study. HIV AIDS. 2021;13:271–281.
49. Siedner MJ, Moorhouse MA, Simmons B, et al. Reduced efficacy of HIV-1 integrase inhibitors in patients with drug resistance mutations in reverse transcriptase. Nat Commun. 2020;11(1). doi:10.1038/s41467-020-19801-x
50. Mehtani NJ, Puryear S, Pham P, Dooley KE, Shah M. Infectious diseases learning unit: understanding advances in the treatment of latent tuberculosis infection among people with human immunodeficiency virus. Open Forum Infect Dis. 2021;8(8):ofab319. doi:10.1093/ofid/ofab319
51. Wiznia AAC, Fenton T. Dolutegravir in 6--12 year old HIV infected children: 48--week results from IMPAACT P1093. Pediatr Infect Dis J. 2015;34(11):1207.
52. Mondi A, Cozzi-Lepri A, Tavelli A, et al. Effectiveness of dolutegravir-based regimens as either first-line or switch antiretroviral therapy: data from the Icona cohort. J Int AIDS Soc. 2019;22(1):e25227. doi:10.1002/jia2.25227
53. Benoît Trottier JEL, Lake JE, Logue K, et al. Dolutegravir/abacavir/lamivudine versus current ART in virally suppressed patients (STRIIVING): a 48-week, randomized, non-inferiority, open-label, phase IIIb study. Antivir Ther. 2017;22(4):295–305. doi:10.3851/IMP3166
54. Gebremeskel TG, Gebreyowhans D, Abrha Gesesew H, Ward PR. Incidence and predictors of severe adverse drug reaction among patients on antiretroviral therapy in Tigray, Ethiopia: a retrospective cohort study. HIV AIDS. 2021;13:641–649. doi:10.2147/HIV.S310419
55. Taramasso L, Bonfanti P, Ricci E, et al. Factors associated with weight gain in people treated with dolutegravir. Open Forum Infect Dis. 2020;7(6):ofaa195. doi:10.1093/ofid/ofaa195
56. Alemnew M. Comparative Safety and Survival Rate of Dolutegravir with Efavirenz Based Antiretroviral Therapies for First-Line HIV Treatment Among Patients in Amhara Region, Ethiopia: Retrospective Cohort Study. AAU Institutional Repository; 2022.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Phase IV Study on Safety, Tolerability and Efficacy of Dolutegravir, Lamivudine, and Tenofovir Disoproxil Fumarate in Treatment Naïve Adult Indian Patients Living with HIV-1
Dravid A, Morkar D, Prasad D, Ramapuram JT, Patel KV, Naik KS, Bhrusundi M, Kulkarni M, Hegde S, Anuradha S, Nageswaramma S, Madan S, Jayaprakash T, Kulkarni V
Pragmatic and Observational Research 2022, 13:75-84
Published Date: 10 August 2022
Weight and BMI Changes Following Initiation of Emtricitabine/Tenofovir Alafenamide Co-Formulated with Darunavir or Co-Administered with Dolutegravir in Overweight or Obese, ART-Naïve People Living with HIV-1
Donga P, Emond B, Rossi C, Bookhart BK, Lee J, Caron-Lapointe G, Wei F, Lafeuille MH
ClinicoEconomics and Outcomes Research 2023, 15:579-591
Published Date: 24 July 2023
Amphotericin B Colloidal Dispersion is Efficacious and Safe for the Management of Talaromycosis in HIV-Infected Patients: Results of a Retrospective Cohort Study in China
Liu M, Yang H, Liu Q, He K, Yuan J, Chen Y
Infection and Drug Resistance 2024, 17:5581-5593
Published Date: 14 December 2024