Back to Journals » Journal of Pain Research » Volume 19
Comparative Safety Analysis of Hydromorphone and Morphone Sulfate: Evidence from the 2004–2024 FAERS
Received 7 August 2025
Accepted for publication 15 December 2025
Published 13 January 2026 Volume 2026:19 559014
DOI https://doi.org/10.2147/JPR.S559014
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Timothy Atkinson
Xiaohong Chen, Chunli Yang, Zhiying Lin
Jiangxi Provincial People’s Hospital, The First Affiliated Hospital of Nanchang Medical College, Nanchang, Jiangxi Province, 330006, People’s Republic of China
Correspondence: Zhiying Lin, Jiangxi Provincial People’s Hospital, The First Affiliated Hospital of Nanchang Medical College, Nanchang, Jiangxi Province, People’s Republic of China, Tel +86 0791 86896209, Email [email protected]
Background: Hydromorphone and morphine, as classic opioid drugs, are commonly used for postoperative analgesia and as adjuncts in the treatment of moderate to severe cancer pain and chronic pain. The lack of specific criteria and the complexity of their respective adverse events (AEs) make it difficult for clinical workers to make a decision.
Methods: This study utilized the FAERS database to compare the baseline risk of AEs between hydromorphone and morphine sulfate. AEs of opioid drugs “morphine” and “hydromorphone” were extracted from FAERS from 2004 to 2024. Non-proportional signal mining is performed by calculating the ratio of reports (ROR), proportional reporting ratio, Bayesian confidence propagation neural network, and empirical Bayesian geometric mean. Then they were filtered and mapped to a total of 25 types of AEs, including primary preference term (PT) signals and systemic organ categories.
Results: According to the FAERS database, Among totals of 44303 case reports related to two types of drug, 14902 reports were related to hydromorphone, 29401 reports were related to morphine sulfate. The statistical analysis results include 21890177 AEs reports in the FAERS database, of which 18282801 AEs reports are the “main analysis objects” of Hydromorphone and morphine. This study found that “psychological disorders” and “immune system disorders” are closely related to both drugs. But psychological disorders have the strongest correlation with Hydromorphone (ROR 6.33), while immune system disorders have the strongest correlation with morphine sulfate (ROR 8.41). The signal “General disorders and administrative site conditions” is more significantly associated with Hydromorphone. In addition, drug dependence is a common PT signal in both drugs, and prognosis should be closely monitored after treatment.
Conclusion: Prescription decision-making should be a comprehensive and balanced process. Our study identified potential new and unexpected AEs for Hydromorphone and morphine, providing valuable evidence for the safety research of Hydromorphone and morphine. Especially for prescribers of hydromorphone, clinical vigilance should extend beyond its known opioid-class effects to particularly raise awareness of two unexpected adverse events: for the immune related disorders and administration site reactions.
Keywords: hydromorphone, morphine, FAERS, adverse reactions, drug safety
Introduction
Opioids are one of the oldest known psychoactive drugs in the world and are listed by the World Health Organization (WHO) as drugs used for acute and cancer pain, as well as palliative care. In most countries/regions, the use of opioid drugs for non-medical purposes is illegal, but regulatory agencies, doctors, and dentists in North America have extended opioid prescription to a wide range of non-cancer pain conditions, from back pain to headaches to ankle sprains.1,2 Over time, opioid tolerance and opioid induced nociceptive sensitivity may lead to poor pain control and increased dosage, while the increase in prescription opioid drug dispensing is associated with an increase in opioid abuse and abuse related injuries.3,4 The data shows that when opioids are used as intraoperative drugs, adverse circulatory, respiratory and nervous system reactions in the perioperative period may lead to serious and even life-threatening side effects, increase the perioperative incidence rate and mortality, and increase the risk of postoperative drug abuse.3,5–10
Among them, hydromorphone and morphine are currently the two most commonly used opioid drugs for postoperative pain relief, with a wide range of usage. However, hydromorphone is usually considered a second-line drug for the treatment of acute and chronic pain with morphine, while oral morphine is recommended by the WHO as the preferred drug for chronic cancer pain relief.11–13 However, a large proportion of patients who use morphine do not experience sufficient pain relief, while switching to another opioid during this period can improve paincontrol, and reduce opioid related toxicity.13 Hydromorphone, due to its similar pharmacokinetic and pharmacodynamic characteristics to morphine, is popular among cancer patients, with non-toxic metabolites and flexible usage, and is often considered a substitute for morphine.14 Hydromorphone was introduced in the 1920s and is a semi-synthetic derivative of morphine with a potency approximately five to eight times that of morphine. It is easier to obtain clinically compared to morphine, but both have some common adverse effects including respiratory depression, nausea, vomiting, and itching.15,16 Based on the premise of good comparability in terms of analgesic effect and related side effects, hydromorphone is clinically rumored to be better at controlling pain than morphine with fewer side effects.17 However, a recent Cochrane systematic review database showed that the advantages of hydromorphone are still uncertain due to the lack of high-quality clinical studies.18 In another early randomized controlled trial, the cognitive ability of the hydromorphone group was poorer, but compared to the morphine group, anger, hostility, and emotions were better.14 These may be closely related to the differences and diversity in pharmacological properties of commonly used opioid drugs such as hydromorphone and morphine. Many studies have shown that the analgesic effects of hydromorphone and morphine are similar or have slight differences in advantages,16,19 leading to a difficult question of how these drugs differ in terms of pain relief andAEs when used at equivalent doses, which is also a common challenge that clinical doctors are facing.20
The multiple dimensions of public health issues, personal mental health, and quality of life issues caused by opioids determine that the use of opioid drugs must be regulated. However, the importance of opioid drugs cannot be replaced, especially morphine and hydromorphone. Therefore, how to use opioid drugs correctly is a topic that very worthy of our in-depth research. There is currently no consensus on the specific application scenarios and methods of these two drugs, as well as the criteria for when to adopt alternative treatments. The application of various analgesics currently proposed still belongs to the framework or coordinated research category, such as the concepts of opioid drug rotation and multimodal analgesia integrating non opioid analgesics.3,21–24 Although some of the conceptual methods proposed above have indeed played a certain role in reducing opioid use, conceptual and framework theories alone cannot be better applied in practice. Only more detailed scientific evidence can help promote further rational use of opioid drugs.
The Drug Alert Dataset and Database, FDA Adverse Event Reporting System (FAERS), launched in 1968, has collected a large amount of AEs data from various populations, locations, and drugs. Based on this database, signal mining of AEs is a mature technology. For example, in-depth research on the popular immune checkpoint inhibitors (ICIs) has found that ICIs are associated with five types of mental AEs.25 Combination therapy with ICIs is also an independent risk factor related to AEs such as interstitial lung disease, hypertension, and gastrointestinal bleeding.26 Studies have also found that tissue and organ toxicity associated with ICIs presented age and gender specificity.27 It is also possible to mine specific drug names that are prone to causing common drug-related AEs through this database, such as drugs related to allergic reactions. Research has found that the main drug categories related to systemic allergic reactions are antibiotics, monoclonal antibodies, nonsteroidal anti-inflammatory drugs, and acetaminophen, while the main drug categories related to allergic death are antibiotics, radiation contrast agents, and intraoperative drugs.25 Therefore, our research focuses on uncovering the potential effects of morphine and hydromorphone by mining the FAERS database and analyzing and comparing the differences between the two drugs, in order to provide reference for better clinical application of the two drugs.
This ambiguity underscores a pivotal clinical concern: whether the comparable analgesic profiles of hydromorphone and morphine sulfate mask significant differences in their potential for organ-specific harm, such as immune-related disorders associated with hydromorphone. To bridge this evidence gap, our study leverages the extensive FAERS database to perform the first comprehensive, real-world, comparative pharmacovigilance analysis of these drugs, with the goal of informing more precise and safer clinical utilization.
Methods
Data Selection
Data Source
In this study, AEs data related to Hydromorphone and morphine sulfate treatment were collected from the FAERS database. FAERS is a publicly accessible post market security monitoring database that has been releasing data quarterly since the first quarter of 2004. It collects AE reports submitted by healthcare professionals, pharmaceutical manufacturers, patients, and others. The FAERS database contains eight different files: demographic and management information (DEMO), drug information (DRUG), AEs (REAC), patient outcomes (OUTC), report source (RPSR), start and end dates of reported drugs (THER), indications for use (INDI), and ineffective reports (deleted). All documents can be accessed on the FDA website. Given that the data in FAERS is anonymous and publicly available, the requirement to obtain informed consent and approval from the Institutional Review Board is waived. This study downloaded ASCII report files from the FAERS database, covering the period from January 1, 2004 to June 31, 2024. Then use R Studio (version 4.2.2) to import and process the data.
Data Cleaning Process
The cleaning and mapping of drug names in FAERS is done by OpenDigil 2 (https://openvigil.sourceforge.net Visited in July 2024). It has a highly configurable search condition filter, which can be used to clean up data and obtain more accurate results in pharmacovigilance data mining.28 The specific selection process is shown in Figure 1.
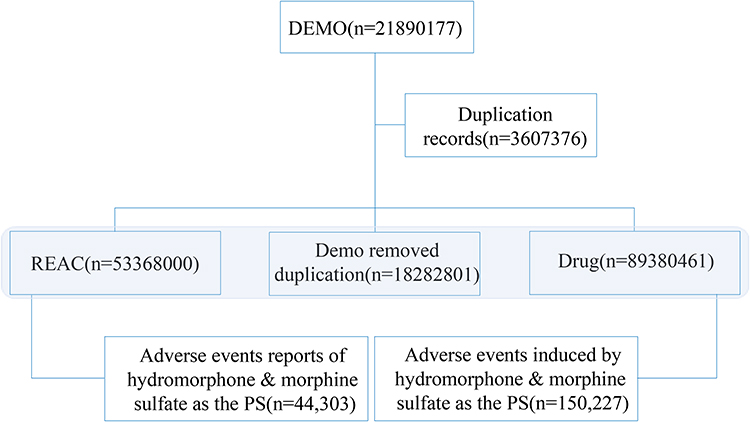 |
Figure 1 The process of selecting Hydromorphone and Morphine Sulfate from the FAERS database to turn off AEs. Abbreviations: DEMO, Demographic information; Drug, Drug information; REAC, Adverse events; PS, Main suspected drug records. |
Data Extraction and Analysis
For data with the same case ID in the DEMO table, we remove duplicate reports and only retain the latest report based on the date. After preprocessing, AEs in FAERS are encoded according to the preferred terms (PT) in the regulatory activity medical dictionary (MedDRA, version 25.0) and mapped to the system organ classification (SOC) level. The role codes for AEs are assigned by the reporter, including primary suspected drug (PS), secondary suspected drug (SS), concomitant drug, and interacting drug. To ensure the collection of drugs that are most likely to cause AEs during drug use, the analysis report is limited to drug records with “role_comd” as “PS” (primary suspected) in the DRUG file. The drug names were standardized using the Medex_UIMA_1.8.3 system. We used the latest version of MedDRA (25.0) to match PTs associated with Hydromorphone and morphine sulfate treatments for AEs and listed the corresponding SOC. We extracted AE related reports related to Hydromorphone and morphine sulfate, including clinical features such as patient age, reporting region, reporter, reporting date, route of administration, outcome, and time of AEs onset after administration.
In this study, the disproportionate analysis method used in pharmacovigilance research was employed for data mining, which evaluated the association between drugs and AEs through statistical methods such as the frequency ratio of the quadruple table (Table 1). We use this method to determine the potential association between Hydromorphone and morphine sulfate with AE, with the main analysis indicators including ROR PRR, The Information Component (IC) and Empirical Bayesian Geometric Mean (EBGM) are calculated using the Reported Ratio (ROR), Proportional Reporting Ratio (PRR), Bayesian Confidence Propagation Neural Network (BCPNN), and Multi Gamma Poisson Shrinker (MGPS) methods, respectively. ROR corrected the bias caused by the small number of reports, while PRR provided higher specificity. The calculation method of BCPNN is complex and has reduced sensitivity. In cases involving missing data, it can produce effective results; The implementation of MGPS can effectively reduce the influence of confounding factors, and this Bayesian analysis ensures the reliability and authenticity of FAERS data mining results.29 Table 2 provides a detailed introduction to the specific formulas and thresholds for the four algorithms mentioned above. Perform statistical analysis using Microsoft Excel 2016.
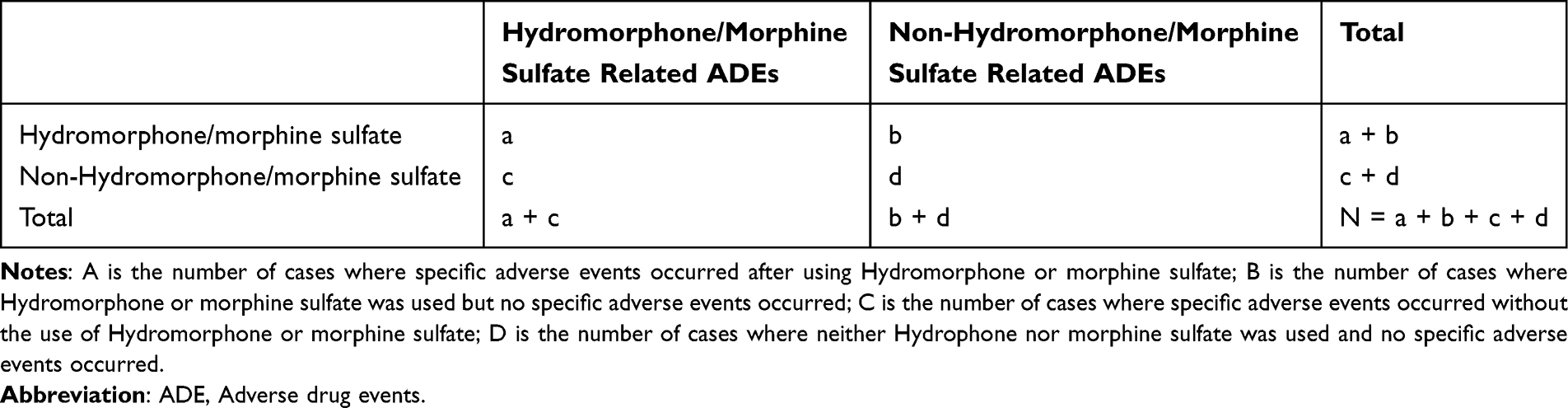 |
Table 1 Four-Grid Table for Signal Detection |
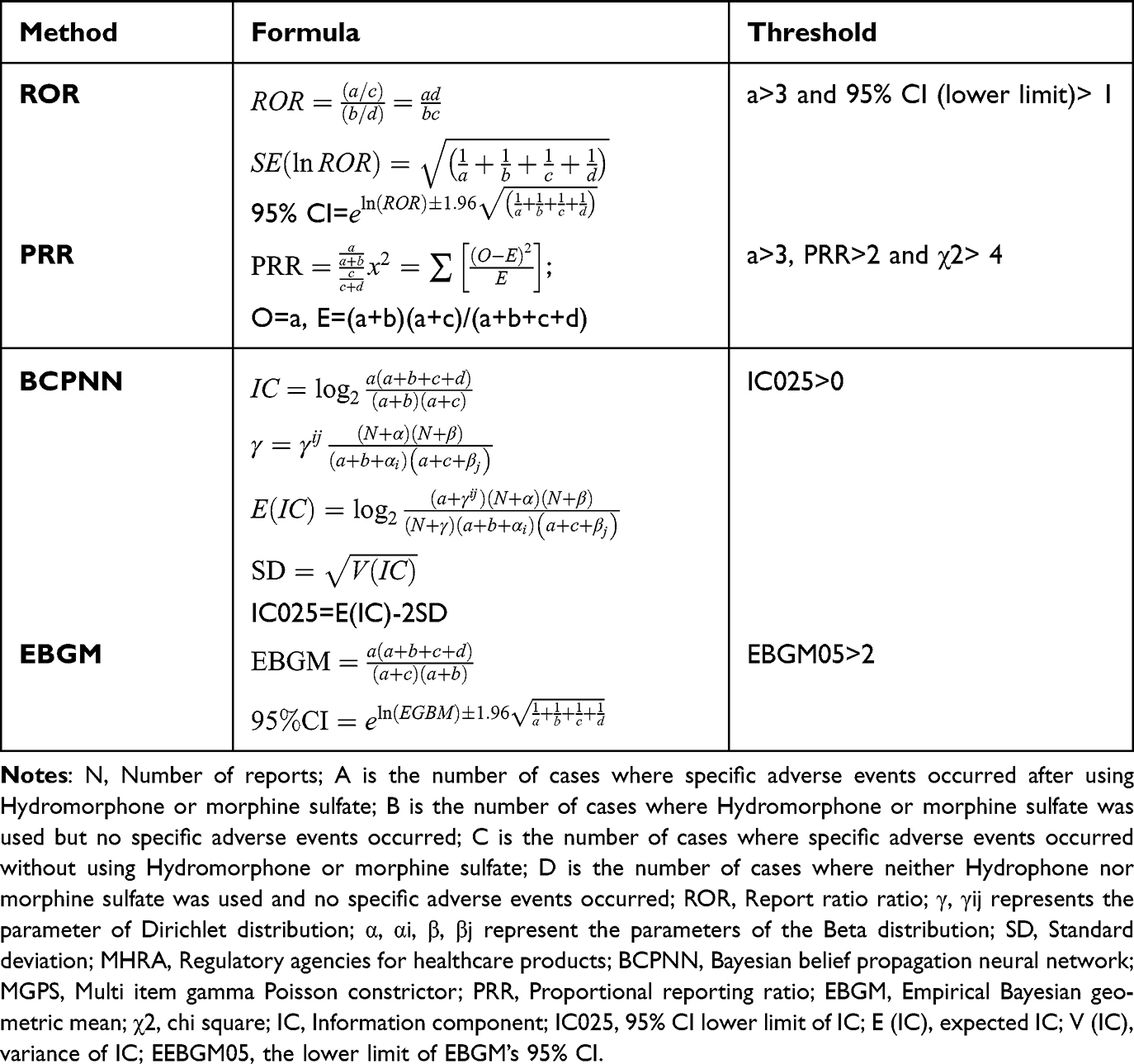 |
Table 2 Four Main Algorithms are Used to Evaluate the Correlation Between Hydromorphone and Morphine Sulfate and AE. This Includes ROR, PRR, BCPNN, and EBGM Methods, Formulas, and Thresholds |
Signal Filtering and Classification
PTs with a reporting frequency of ≥ 3 are included in the preliminary screening. We use MedDRA’s PTs and SOCs to encode, classify, and locate signals, with the aim of analyzing specific SOCs involved in AEs signals. The criteria for positive signal detection in ROR method: the number of reports is ≥ 3 and the lower limit of ROR 95% CI is>1; The criteria for positive signal detection in PRR method are: the number of reports is ≥ 3, PRR is ≥ 2, and the χ2 value is ≥ 4, all of which are valid simultaneously; The criteria for positive signal detection in BCPNN method: the 95% CI lower limit (IC025) of information components (IC) is greater than 0; The criteria for positive signal detection in MGPS method are: the lower limit of 95% confidence interval (EBGM05) of empirical Bayesian geometric mean (EBGM)>2, N>0. In this study, at least one of the four algorithms meets the criteria and can be considered as a positive signal for drug-related AEs; When all four algorithm criteria are met simultaneously, it indicates a strong correlation between AEs and drugs.
Data Limitations
The FAERS database contains incomplete and heterogeneous reports, with frequent missing information on indication, comorbidities, and concomitant medications. Because of these limitations, analyses restricted to single-suspect cases, indication-specific subgroups, or outcome-severity strata could not be reliably performed. Inconsistent reporting of seriousness and fatality further restricted stratified evaluations. These constraints are inherent to spontaneous reporting data and were considered when interpreting the results.
Software Workflow
Data cleaning steps such as duplicate removal and format adjustment were conducted in Excel. All statistical analyses—including calculation of ROR, PRR, IC, and EBGM—and all visualizations were performed entirely in R. Final table formatting was completed in Excel. This workflow ensures transparency and reproducibility of the analytic process.
Results
Basic Information on Hydromorphone and Morphine Sulfate Related AEs
According to the FAERS database, a total of 44303 reports related to two types of drug AEs were extracted between 2004 and 2024. Among them, 14902 reports were related to hydromorphone, involving 58532 AEs, with an average of 3.92 AEs per report; 29401 reports were related to morphine sulfate, involving 91695 AEs, with an average of 3.12 AEs per report. In terms of the average number of related AEs per person, the occurrence of AEs in hydromorphone is higher than in morphine sulfate. The clinical characteristics of specific drug-related AEs are detailed in Table 3.
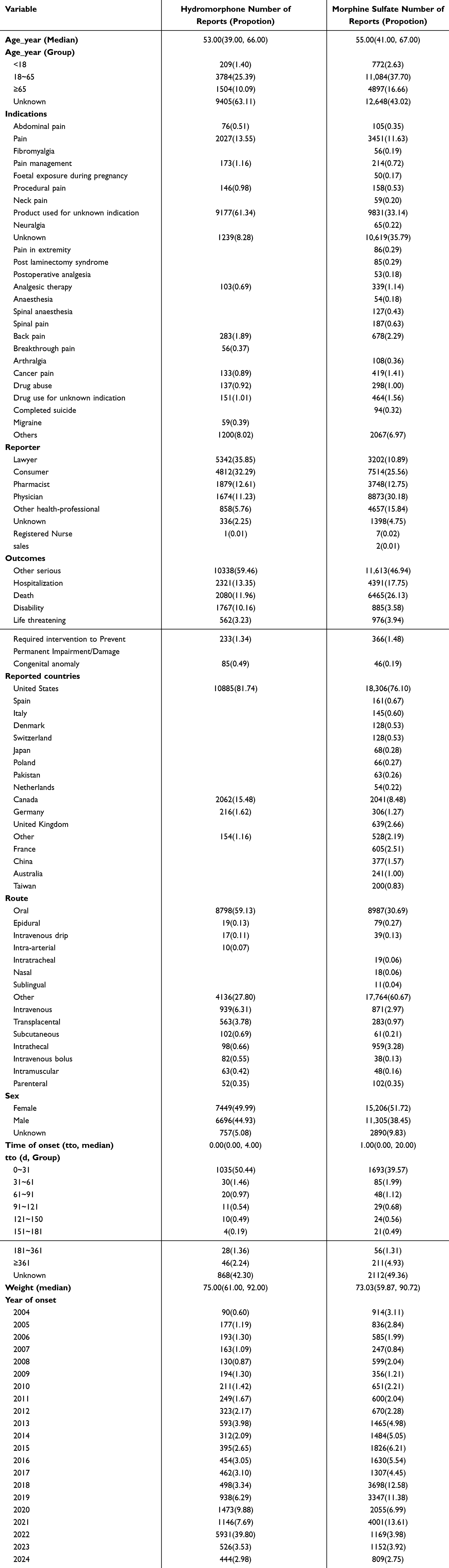 |
Table 3 Demographic Information on AEs with Hydromorphone and Morphine sulfate |
The age distribution results of all AEs related to Hydromorphone treatment showed that the median age of the reported population was 53 years old, with individuals between 18 and 65 years old reporting the most (25.39%), while individuals under 18 and over 65 years old reported the least (1.40%, 10.09%). Among them, the number of unknown reports is relatively high, which may result in the specific distribution of the population being “under the iceberg”. There are a total of 14 symptom indicators related to Hydromorphone treatment, including abdominal pain, pain, pain management, procedural pain, product used for unknown indication, unknown, analgesic therapy, back pain, breakthrough pain, cancer pain, drug abuse, drug use for unknown indication, migraine, and others. The types of reporters are Lawyer, Consumer, Pharmacist, Physician, Other health-professional, unknown, Registered Nurse, the number of reporters in each category, ranked from high to low, is 5342, 4812, 1879, 1674, 858, 336 and 1 respectively. The adverse outcomes include other serious, hospitalization, death, disability, life threatening, required intervention to Prevent Permanent Impairment/Damage And congenital anomaly. The number of people involved is 10338, 2321, 2080, 1767, 562, 233 and 85 respectively. The other serious category has the highest number of reported cases, as the lack of specific outcome information may affect the assessment of potential risk information for drug AEs. The most reported regions are from the United States (10885, 81.74%), followed by Canada (2062, 15.48%), followed by Germany (216, 1.62%) and other (154, 1.16%), with the proportion of reports from unknown regions being almost negligible. The number of AEs reported for this treatment was only 90 in 2004, and remained below 1000 from 2005 to 2019. It began to rise sharply from 2020, reaching a peak of 5931 cases in 2022, and then rapidly decreased to around 8.8% of the peak in the past two years.
The age distribution of all AEs related to morphine sulfate treatment showed a median age of 55 years. Among the segmented ages, the highest reported number of AEs between 18 and 65 years old was 11084 (37.70%), but the unknown population was more at 12648 (43.02%). Based on the existing epidemiological data of morphine sulfate treatment, it may not have a significant impact on the results. If other distribution forms are presented, it may affect the existing analysis. There are a total of 22 symptom indicators involved in AEs, of which 12 are the same as those of Hydromorphone treatment-related AEs, and the other 10 are fibromyalgia, foetal exposure during pregnancy, neck pain, neuralgia, pain in extremity, post laminectomy syndrome, anaesthesia, spinal anaesthesia, spinal pain, arthralgia, completed suicide; In addition, reports of two symptom indicators, namely migraine and breakthrough pain, were found in Hydromorphone, while morphine sulfate did not appear. Among the types of reporters, in addition to the 7 related to Hydromorphone, there is also an additional category called Sales. Among them, the number of reporters in the Physician category is the highest at 8873 (30.18%), followed by Consumers at 7514 (25.56%). The reporting area involves multiple countries, with an additional 13 reporting sources compared to Hydromorphone. From the perspective of time distribution, the number of annual cases of AEs related to this treatment remained stable between 2004 and 2012, staying below a thousand. The number of case reports continued to increase from 2013 until reaching its peak in 2021 (4001), and then began to decline. By 2024, it had dropped again to below a thousand.
The results of the drug intake route show that the main routes of the two drugs are similar, oral intake. Similarly, a large proportion of the intake routes for both drugs are unknown. Based on their distribution patterns, there will not be much impact on the comparison between the two drugs. In this regard, the two drugs have good comparability. The gender ratio can be well balanced in Hydromorphone AEs reports, with males (51.72%) slightly higher than females (38.45%) in morphine sulfate AEs. The median weight results showed that Hydromorphone AEs (75) and morphine stulfa AEs (73.03) cases were similar and had good comparability. In terms of onset time, the median duration of Hydromorphone AEs is 0 days, and the median duration of morphine stulfa AEs is 1 day, indicating that both drugs have a fast onset rate of AEs, and side effects should be closely monitored or monitored while taking them. Although both have the highest number of reported cases within 0–31 days, there are also longer periods of reported cases, such as 46 and 211 cases of Hydromorphone and morphine sulfate AEs with a duration of one year. The impact of this medication is profound, and after taking it, it is best to remember the specific information of the medication for close care of one’s own physical health. The highest age group of the two drugs is young people, which is consistent with the research of Manchikanti et al in 2010. The results of this study also show that the top two drugs are distributed in the United States. The above findings of Manchikanti et al may explain this phenomenon. The findings show that the United States population, which accounts for about 5% of the earth’s population, consumed about 80% of the world’s prescription opiate supply in the first decade of this century.30
Figure 2 illustrates the quarterly trend of the number of AEs per year. From the picture, it can be seen that there is no seasonal trend in the occurrence of AEs cases for both drugs. If the stable trend from the first quarter of 2004 to the end of the fourth quarter of 2012 is taken as the “baseline”, then from the first quarter of 2013 to the end of the fourth quarter of 2017, both drug-related AEs entered a period of “small fluctuations”, while from the first quarter of 2018 to the first quarter of 2023, they entered a period of “large fluctuations”. After that, the number of cases rapidly decreased and then stabilized until the end of the investigation year. Except for the period from the fourth quarter of 2020 to the fourth quarter of 2022, the peak number of drug-related AEs cases alternated between the two. In other time periods, the number of morphine sulfate AEs cases is higher than that of Hydromorphone AEs cases. Figure 3 shows the annual trend of AEs reports, from which it can be seen more clearly that the number of morphine stulfa morphine sulfate AEs cases has always been higher than that of Hydromorphone AEs, except for a sudden increase in Hydromorphone AEs cases in 2022, which is 1930 cases higher than the peak of 4001 cases of morphine sulfate AEs in 2021. Similar to the regions where Hydromorphone AEs are reported, the main reporting countries for morphine sulfate AEs are the United States (18306, 76.1%) and Canada (2041, 8.48%). This may be related to the significant increase in opioid prescriptions in countries such as the United States and Canada over the past two decades.1 But on the world map, there does not seem to be much difference (Figure 4), which may be due to the missing AEs report values of Hydromorphone for data in Africa, the Middle East, and some Southeast Asian regions, while the AEs report values of morphine sulfate are lower, and the source countries of many reports are unclear. The most important thing is that according to the descriptive analysis results of the database analysis, the United States and Canada basically account for the vast majority of drug reporting numbers. Therefore, the distribution maps of the two drugs in the map look similar and appear gray on the map.
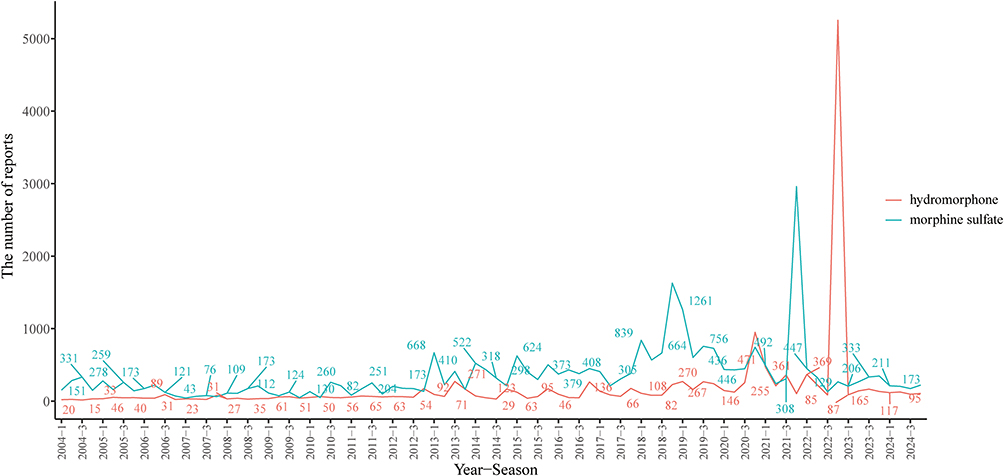 |
Figure 2 Quarterly line chart of counts related to Hydromorphone AE and morphine sulfate AEs. |
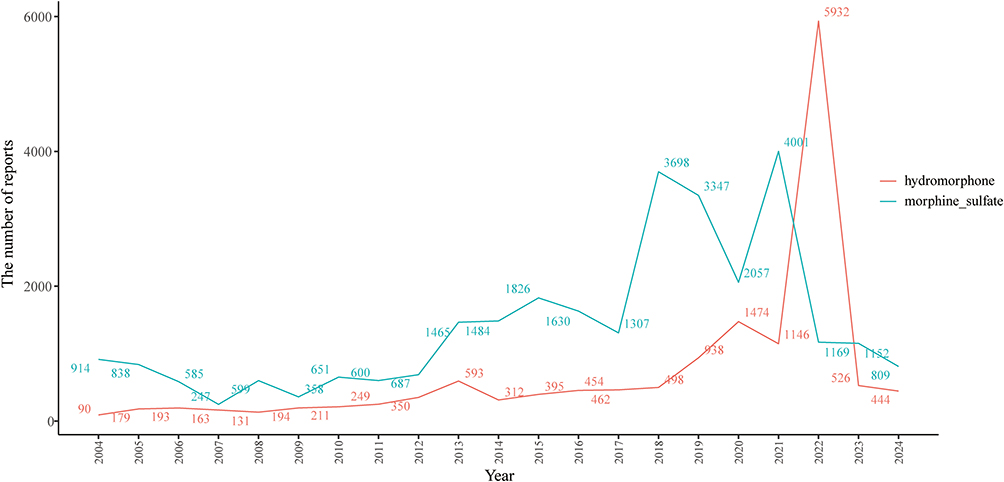 |
Figure 3 Count annual line graph related to Hydromorphone AEs and morphine sulfate AEs. |
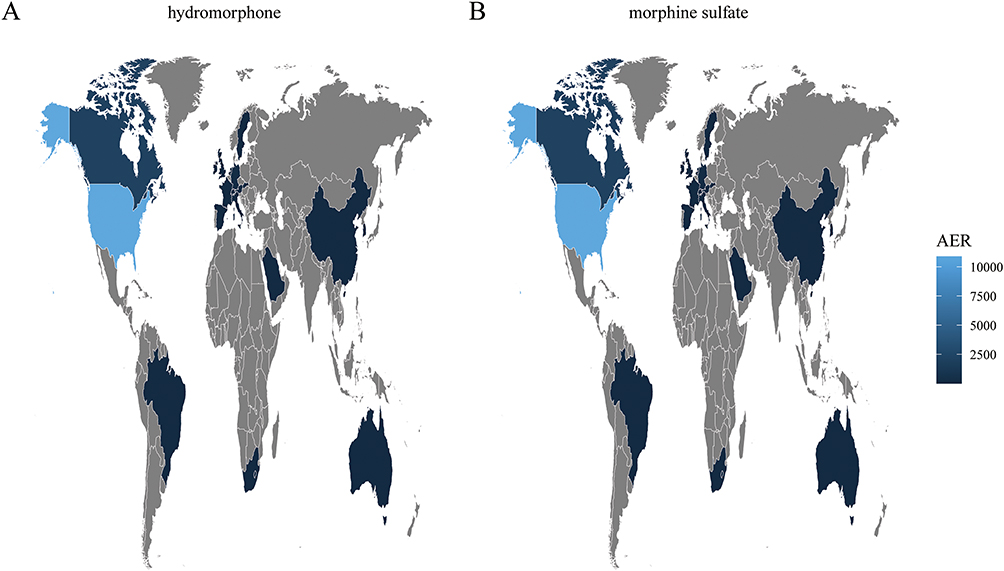 |
Figure 4 The brighter blue shadow indicates that the region (such as the United States) has a higher reported AEs value and is the highest area for this indicator. On the contrary, gray indicates areas with fewer reports. The dark blue regions (such as some European, South American, and Asian countries) indicate moderate levels of AEs reported. Given that both drugs appear to have high AEs values in North America (especially the United States), some South American countries, Australia, East Asia (such as China), and some European countries. For data in Africa, the Middle East, and some Southeast Asian regions, although Hydromorphone’s AEs report values are missing, morphine sulfate’s AEs report values are relatively low, so they all appear gray on the map. In addition, many of the source countries of the reports are unclear, so the figures (A and B) look similar. (A) Hydromorphone. (B) morphine sulfate. |
Signal Mining of Hydromorphone and Morphone Sulfate Related AEs
Analysis by SOC Level
Table 2 provides a detailed introduction to the specific formulas and thresholds for the four algorithms mentioned (ROR, PRR, BCPNN, and EBGM). All AEs were identified and classified into 25 System Organ Classification (SOC) categories. For detailed information on all SOC signals, please refer to Table 4. In this study, the positive signal standard thresholds of four algorithms were used to analyze the four most relevant AEs systems for Hydromorphone treatment, which were psychological disorders (n=16453, ROR 6.33, PRR4.83, IC 2.27, EBGM 4.81), immune system disorders (n=951, ROR 1.43, PRR 1.42, IC0.5, EBGM 1.42), injury, poisoning, and procedural complexes (n=7315, ROR 1.33, PRR 1.29, IC 0.37, EBGM 1.29), and general disorders and administrative site conditions. Conditions (n=12633, ROR 1.26, PRR 1.21, IC 0.27, EBGM 1.21). Among them, psychological disorders simultaneously meet all four algorithm standards, therefore their correlation is the strongest. In addition, although the signal strength of neurological system disorders (4260 cases), gastrointestinal disorders (3414 cases), respiratory, thoracic, and median disorders (2230 cases), investigations (2133 cases), musculoskeletal and connected tissue disorders (1688 cases), and skin and subcutaneous tissue disorders (1308 cases) may not be as strong as the aforementioned systems, their large number of reports are worth closely monitoring.
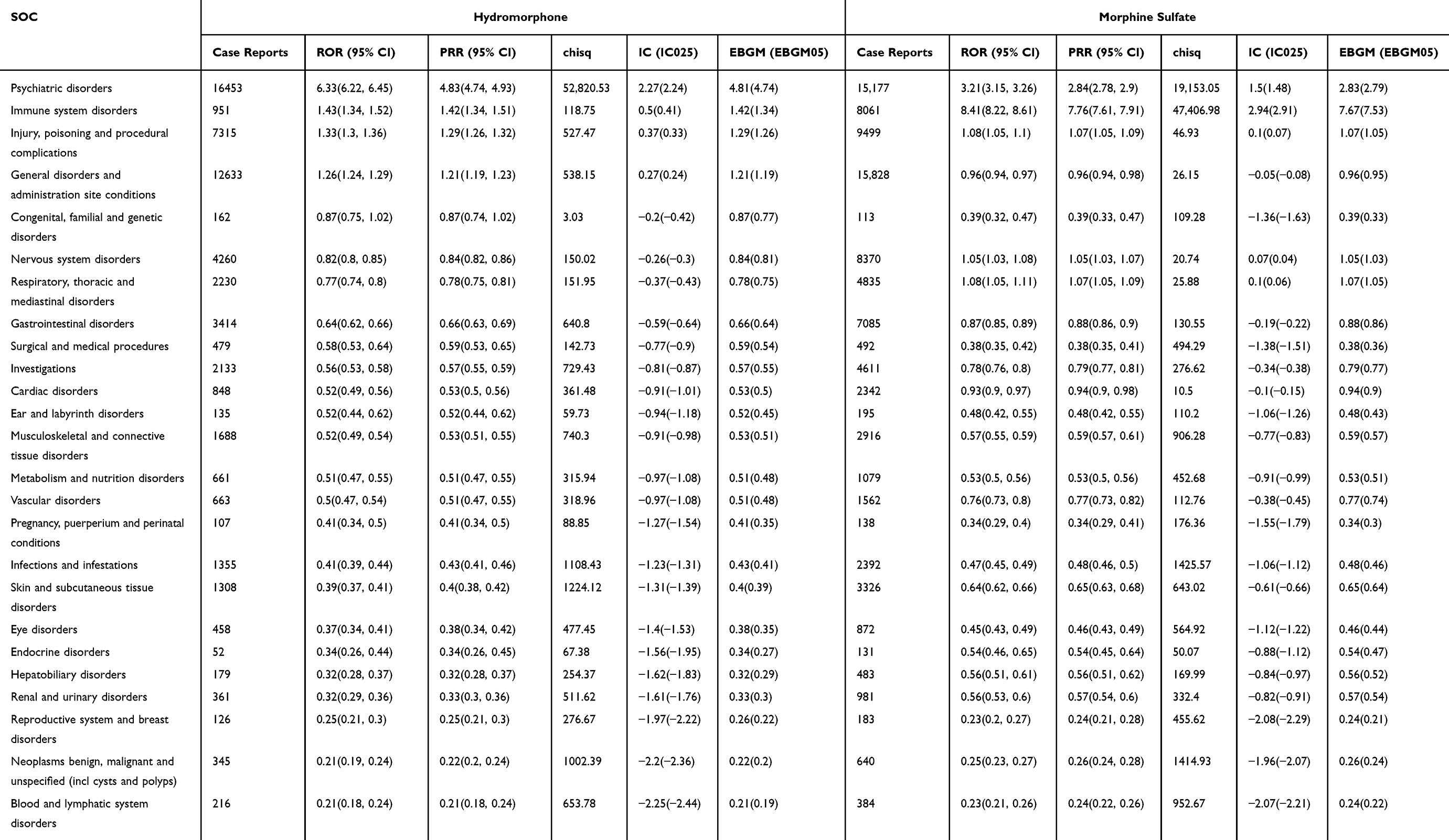 |
Table 4 SOC Systems Related to Hydromorphone and Morphine Sulfate |
For morphine sulfate related AEs systems, there are psychological disorders (n=15177, ROR 3.21, PRR2.84, IC 1.5, EBGM 2.83), immune system disorders (n=8061, ROR 8.41, PRR 7.76, IC 2.94, EBGM 7.67), and exception, poisoning and procedural complications (n = 9499, ROR 1.08, PRR 1.07, IC 0.1, EBGM 1.07). Among them, psychological disorders and immune system disorders both meet four algorithm standards, but immune system disorders have the strongest correlation (ROR 8.41). Although these findings are inconsistent with the warnings on drug labels,31 this new result is necessary to identify the issues with the drug and further expand the dimensions of drug research. Similarly, there are also a large number of reported cases of general disorders and administrative site conditions (15828 cases), neurological system disorders (8370 cases), gastrointestinal disorders (7085 cases), respiratory, thoracic and median disorders (4835 cases), investigations (4611 cases), and skin and subcutaneous tissue disorders (3326 cases) that require further monitoring.
Combining Figure 5, among these system signals, psychological disorders, immune system disorders, and injury, Poisoning and procedural complications are associated with both Hydromorphone and morphine sulfate drug treatments. The difference is that Hydromorphone is not only associated with the three system signals mentioned above, but also with general disorders and administrative site conditions, which are related to its treatment. There is an additional treatment-related AEs compared to morphone sulfate. Compared to Hydromorphone, which has only one strongly correlated AEs, morphine sulfate has an additional strongly correlated AEs, namely immune system disorders.
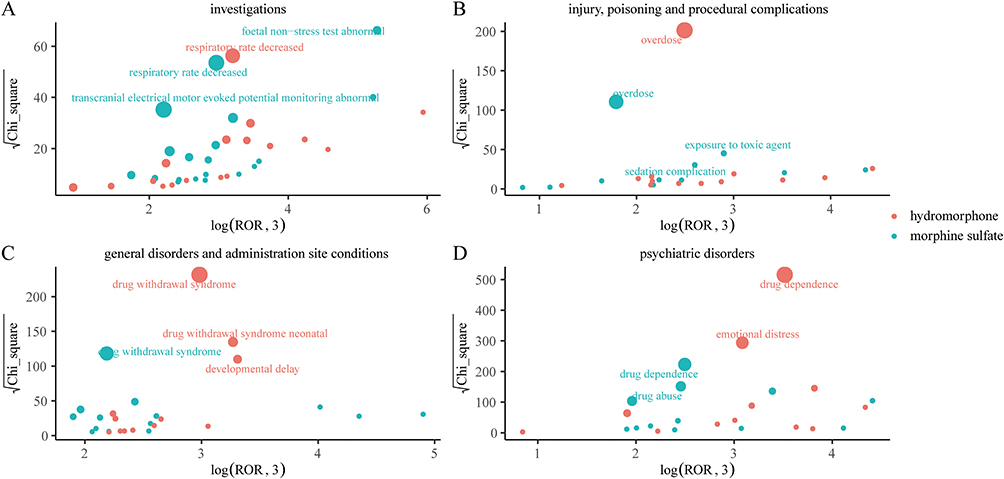 |
Figure 5 The most relevant preferred terms in the classification of the most important system organs in Figure 5. Hydrophorphon and morphine sulfate. (A) 1Vestigatlons is abnormal. (B) 1nlury, polsoning and proceduracompications. (C) general disorders and administration site conditions. (D) psychiatric disorders. |
Analysis by PT Level
After screening, a total of 416 preferred words (PT) met the positive signal criteria of ROR, PRR, BCPNN, and EBGM algorithms and were classified as AEs signals related to two drug treatments. Among them, 214 PTs were associated with Hydromorphone treatment, and similarly, 285 PTs were associated with morphine sulfate treatment. Supplementary Table 1 provides detailed information on all PT signals. In a single PT, with ROR value as a reference, the three signals of Hydromorphone treatment are very prominent: antasthmatic drug level (ROR 683.12), foreign body embolism (ROR 277.23), coccygectomy (ROR248.41) And the Malignant Continental Nerve Neoplastic (ROR 165.61). However, these signals were only reported in 3–7 cases, so their clinical significance is still unclear. In addition, although the signal intensity of drug dependence (6925 cases), pain (3903 cases), emotional distress (3423 cases), drug withdrawal syndrome (2340 cases), and drug hypersensitivity (654 cases) is not as high as the aforementioned PTs, their reported numbers far exceed other PTs and are more common in previous clinical cases and research reports.32,33 Therefore, when citing them in clinical practice, attention should be paid to observation and dosage consideration. In contrast, for morphological sulfate, the strongest PT signals are anatomical complexity neonatural (ROR 348.62), fossil non stress test abnormal (ROR 329.84), transcranial electrical motor evolved potential monitoring abnormal (ROR 309.9), infusion site granule (ROR 217.9), and substance dependence (ROR 127.02). Except for a slightly higher number of substance dependence reports at 107, the number of other strongly correlated reports is very low. The PT with the highest reported number of adverse events (AEs) treated with morphine sulfate is drug hypersensitivity (7364 cases), followed by drug dependence (3926 cases). Drug dependence is related to both drug treatments and has a higher number of reports. Therefore, close attention to the occurrence of this type of AEs during clinical medication can improve patients’ happiness with drug treatment. Of course, in experimental research, attention can also be paid to the specific details related to the occurrence of AEs and medication, in order to provide scientific basis for better drug treatment.
Grouping by Age
To investigate the effects of two drug combination regimens on different age groups, we conducted age stratified analysis on all reports. The detailed information and results of all groups are provided in Supplementary Table 2 of the supplementary materials.
For patients receiving Hydromorphone treatment, 61, 107, and 102 PT were found in the age groups of under 18 years old, 18–65 years old, and over 65 years old, respectively. Among them, retro orbital neoplasma (ROR 778.85), malignant cranial nerve neoplasma (ROR 667.58), and postoperative ileus (ROR 351.31) are the three most prominent signals in the age group under 18 years old. Drug dependence is the most commonly reported AEs (33 cases), followed by toxicity to various agents (26 cases). After retro orbital neoplasty, potent opioid drugs such as hydromorphone are often used for pain relief, and the use of hydromorphone may reflect more on its application in treating these tumor related pains rather than directly causing tumor development. Rare malignant cranial nerve neoplasms in children, such as brainstem gliomas or nerve sheath tumors, often accompany severe neuropathic pain. Hydromorphone is often used for pain management in such patients due to its potent and central nervous system pain management properties.34–37 Therefore, high ROR values may reflect the frequency of use of hydromorphone in these specific clinical contexts, rather than its carcinogenicity. Postoperative ileus is a common adverse event (AEs) of opioid drugs, especially in pediatric postoperative analgesia, which requires more attention. In the age group of 18–65 years old, antagonistic drug level (ROR 1201.6) is the most significant signal, followed by human immunodeficiency virus transmission (ROR 961.33), while drug dependence once again becomes the most common condition (380 cases). Most opioid drugs undergo two-stage liver metabolism, during which new metabolites are produced and coupled with other molecules in the body. Some anti-asthma drugs (such as theophylline) may interact with intermediate products of hydromorphone metabolism through the hepatic enzyme metabolism pathway, affecting drug.38–40 The relationship between human immunodeficiency virus transmission and opioid use can be explained by some studies, as opioid use is associated with increased frequency of sexual activity related to transmission, while injection drug use is associated with annual new HIV cases and multiple outbreaks in recent years.41–44 In the age group of 65 and above, endometritis (ROR 605.58) showed significantly higher signal intensity than other PTs during sexual activity and injection of opioid drugs, followed by opposition positive (ROR 252.29) and urticaria thermal (ROR 232.92). The reports on endometritis and opioid drugs only involve the role of delta opioid receptors in mediating the inhibitory effect of endogenous opioid drugs on endometritis,45 which is inconsistent with our research results. It is possible that the data entry, disease coding, or case classification steps in FAERS were not strictly followed according to the standards, resulting in slight discrepancies with actual reports. Opposites positive may be due to slow metabolism in the elderly, resulting in high drug concentrations during testing. The most frequently reported types of PT are irresponsible to stimulation (81 cases), depressed level of consciousness (69 cases), respiratory rate decreased (53 cases), and staging (50 cases). Among the population of unknown age groups, the strongest signal is related to palliative sex (ROR 192.35), followed by self esteem infected (ROR 65.16) and neonatal hydropathy (ROR 61.86). The strongly correlated PT signals in patients of unknown age group are different from those in other age groups, indicating that the age distribution of this group may not have a significant tendency, and may be close to the distribution of known age groups. Considering the large number of reported cases in this group, conclusions should not be drawn without considering relevant information when conducting analysis and discussion. It should be analyzed as a separate group.
For patients treated with morphine sulfate, 45, 28, and 9 PTs were found in the age groups of under 18 years old, 18–65 years old, and over 65 years old, respectively. Infant regression (ROR 553.16), respiratory paradox (ROR 368.77), and acute chest syndrome (ROR 166.95) are particularly prominent PT signals in the age group under 18 years old. It is worth noting that in this age group, there were also significant reports of overdose (90 cases), somnolence (68 cases), and toxicity to various agents (66 cases). Morphine is an opioid drug and one of the most commonly used analgesics in neonatal intensive care units (NICUs). It is mainly metabolized in the liver, and newborns are a unique group in terms of drug, metabolism, elimination, and clinical effects. Their “symptomatic organs” and drug action sites are in the developmental stage, and their liver and kidney clearance rates are relatively low. The concentration of morphine in their plasma is significantly higher than that of other age groups, and critically ill newborns may experience reduced metabolism and morphine clearance rates due to impaired liver and kidney function. Renal dysfunction can prolong its half-life and may lead to toxicity caused by drug accumulation, including excessive sedation, respiratory depression, etc.46 In the 18–65 age group, although there were only three reports, the signal intensity of infusion site granuloma (ROR 223.86), substance dependence (ROR 142.4), and injection site granuloma (ROR 125.96) was significantly higher than other PT signals. Drug hypersensitivity remained the most common condition (2759 cases), drug abuse (1037 cases), and drug dependence (388 cases). Granuloma formation is a commonly reported AEs in morphine therapy, but there is currently no clear report on which administration method is most likely to form granulomas.47,48 Our results suggest that administration methods such as injection or infusion may be associated with the formation of morphine related granulomas. In the age group over 65 years old, hypogonadism male (ROR 259.6) has the strongest signal, followed by anterior spinal art syndrome (ROR 133.81) and injection site granulosa (ROR 101.96). But drug hypersensitivity had the highest number of reports (2077 cases), followed by overdose (189 cases) and toxicity to various agents (189 cases). The top three PT signals with unknown age group signal strength are anatomical complex neonatal (ROR 1793.73), transcranial electrical motor evolved potential monitoring abnormal (ROR 797.34), and foetal non stress test abnormal (ROR 483.2).
In summary, it is found that there are relatively more reports of unknown age groups in both drug treatment regimens. Although most of the strongly correlated PT signals found in each group have corresponding evidence to confirm, there are still some signal results that do not have scientific basis. This may be related to the lack of rigor in FAERS data. However, all PT signals with strong correlation obtained should be taken seriously in practical applications, which is crucial for monitoring the dynamic evaluation of drug toxicity.
Grouping by Gender
The detailed information on the gender differences between the two drug treatment regimens can be found in Supplementary Table 3. Combining Figure 6, 101 PT signals were detected in the treatment of hydromorphone among female genders, among which the signal intensities of palmative staging (ROR 577.76), foreign body embedding (ROR 481.48), coccygeology (ROR 577.76), and rest regime (ROR 296.3) were the strongest, while drug dependence (3026), emotional distress (1626 cases), and overdose (1317 cases) had the highest frequencies; In male gender, a total of 102 PT signals were detected, including antagonistic drug level (ROR 708.63), foreign body embedding (ROR 425.18), analogic drug level (ROR 193.26), and malignant cranial nerve neovascularization (ROR 166.74), with drug dependence (3813 cases), pain (1927 cases), and overdose (1864 cases) having the highest frequency. In the pattern observed in morphine sulfate treatment, the number of PT signals observed in both female and male genders was 100. Among them, the highest signal intensity observed in females is foetal megacyst (ROR 228.99), catheter site granule (ROR 174.47), and observational procedure complexity (ROR 146.56), while in males it is infusion site granule (ROR 219.66), injection site granule (ROR 133.1), and catheter site granule (ROR 92.67). The highest frequency PT signals were in female drug hypersensitivity (5372 cases) and male drug dependence (2233 cases).
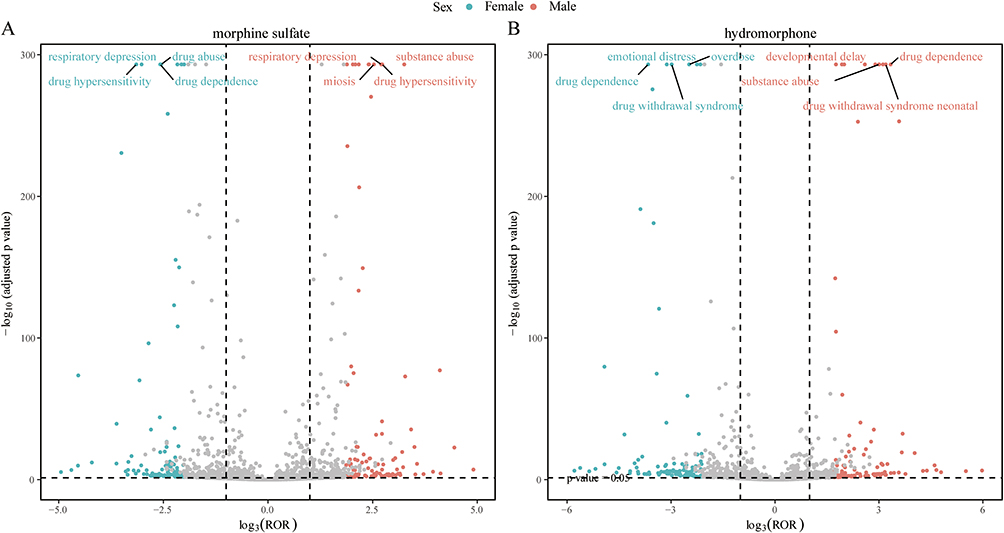 |
Figure 6 Volcanic plot of PT signals of Hydromorphone and morphine sulfate related AEs grouped by gender. (A) morphine sulfate related AEs. (B) hydromorphone related AEs. |
Analysis of Onset Time
Among all AEs reports, a total of 6331 reports included the time of occurrence of AEs. After excluding inaccurate or missing onset times and reports of unknown gender, there were 1184 and 2167 reports corresponding to the occurrence time of hydromorphone and morphine sulfate AEs, respectively. The median onset times were 51.50 days (44.00, 61.70) and 52.00 days (43.00, 64.00), respectively. Interestingly, Figure 7 indicates that for both drug combinations, the majority of AEs in males and females occur within the first month of treatment, highlighting the necessity for early monitoring and proactive intervention. In addition, AEs may still occur up to one year after the start of drug treatment, indicating that continuous monitoring of potential AEs throughout the entire treatment period and even up to one year after treatment is essential.
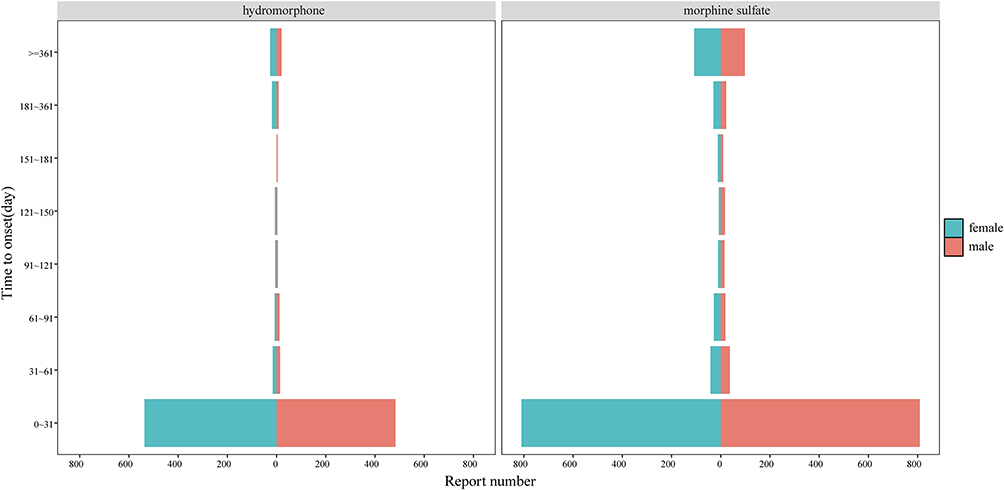 |
Figure 7 Differences in the onset time of AEs between males and females. |
Discussion
Currently, most research on the analgesic effects of morphine and hydromorphone is focused on clinical cohorts, and from the research results, it is not yet possible to draw a conclusion on which drug is better. Our research focuses on big data mining and analysis through the largest FDA pharmacovigilance database, aiming to evaluate and compare two drugs from the perspective of drug-related AEs, in order to provide supplementary information and provide another reference direction for clinical workers. Through asymmetric analysis, our results show that psychological disorders, immune system disorders, injury, poisoning, and procedural complexes are associated with Hydromorphone and morphine sulfate therapy at the SOC level. In addition, Hydromorphone therapy related SOC signals also involve general disorders and administrative site conditions. At the PT signal level, the strongest PT signal intensities (calculated according to ROR) related to Hydromorphone treatment are at the antagonistic drug level, foreign body embedding, coccygectomy, and malignant cranial nerve neovascularization. The highest number of AEs reported for Hydromorphone treatment are drug dependence, pain, emotional distress, drug withdrawal syndrome, and drug hypersensitivity. The corresponding PT signals with the highest intensity related to morphine sulfate therapy are anaesthetic complex neonatural foetal non-stress test abnormal, transcranial electrical motor evoked potential monitoring abnormal, infusion site granuloma And substance dependence. The most reported cases related to it are drug hypersensitivity and drug dependence. It should be noted that the number of reported cases of strongly correlated PT signals in these two drugs is relatively low, and the highest number of cases is only substance dependence related to morphine sulfate treatment (107 cases). Therefore, the impact of quantity alone is not comprehensive enough, and AEs with numerical advantages must be combined to be convincing. Therefore, it is scientific to comprehensively interpret the AEs with the highest strength and number of drugs. For example, a recent FAERS study on tuberculosis treatment drugs used this analysis strategy to conduct a more comprehensive discussion on drug AEs.49 Although Hydromorphone and morphine sulfate treatment-related AEs have high similarities in SOC, there are specific differences in the PT signal level. For example, both SOC levels are strongly correlated with psychological disorders, but at the PT signal level, Hydromorphone related PT signals show drug dependence and emotional distress, while morphine sulfate treatment-related PT signals show substance dependence and drug dependence. However, the SOC name corresponding to each PT signal with high drug correlation did not appear in the SOC level analysis results column, such as the foreign body embedding and foreign body embedding corresponding to the SOC name investigations in the PT signals related to Hydromorphone therapy and the antasthmatic drug level and foreign body embedding in the PT signals related to morphine sulfate.
When stratifying the population distribution by age and gender, it is known that the age group in a given location has a larger proportion, which may cause bias in the research results and analysis. However, the results of the analysis and discussion based on literature research still have some reference significance. Although age specificity has not been clearly determined, some PT signals have clear age distinctions such as infant sex and hypogonadism male, and can be explained to some extent by existing research or common sense. At the same time, many positive PT signals identified in this population distribution stage, such as injection site granuloma and infusion site granuloma, have been confirmed by multiple studies to be related to medication.47,48 Therefore, in clinical or basic practice, attention should be paid to distinguishing this signal and further experimental research may lead to new discoveries. According to the analysis of the onset time results, regardless of gender, drug-related AEs mostly occur within the first month, followed by a relatively high number of AEs occurring after one year compared to other times except for the first month. Considering the prevalence and long-term nature of drug addiction side effects caused by opioid drugs, there is reason to suspect that those lasting longer than a year are likely due to the effects of opioid abuse. The SOC signal strongly correlated with both drugs, namely psychological disorders, is closely synchronized with drug abuse. Therefore, it is necessary to be vigilant about the dosage and duration of opioid drugs, prevent opioid addiction, and strictly control the prescription of opioid drugs, which may be an effective public health measure.50,51 The most intense occurrence of AEs occurs within the first month after drug treatment, so it is necessary to closely monitor the patient’s condition after drug treatment in order to detect and treat patients affected by side effects as early as possible and save the prognosis of opioid use patients.
Opioid drugs exert their effects in the human body mainly through the mediation of opioid.52 Currently, there are three main opioid receptors that have been cloned and characterized, including mu opioid receptor (MOR), delta opioid receptor (DOR), and kappa opioid receptor (KOR), as well as a type called nociceptive receptor (NOPR), all of which belong to the G protein coupled receptor (GPCR) family.53,54 Opioid drugs form a vast regulatory network by interacting with opioid receptors, which in turn interact extensively with other signaling molecules.55
Psychological disorders are a heterogeneous group of brain diseases, including depression, bipolar disorder, schizophrenia, drug addiction, post-traumatic stress disorder, anxiety and mood disorders, as well as various neurological disorders such as Parkinson’s disease, Huntington’s disease, and Alzheimer’s disease. In most cases, there is a lack of clear boundaries, and there is a large amount of symptom heterogeneity within the disease and symptom overlap between diseases.53 Almost all mental illnesses are associated with dysfunction of dopaminergic signaling mediated by the corticospinal and nigrostriatal dopamine (DA) systems. Compounds acting on this system, such as antidepressants and antipsychotics, can be used clinically to treat negative emotional states and other symptoms in psychiatric patients.56–58 KORs and their hypothesized endogenous ligand dynorphin (DYNs) are enriched and regulate neurotransmitters in the aforementioned DA brain regions.59,60 Research has also shown that the KORs system plays a role in driving aversion, negative emotional states, stress-induced motivational behavior and cognitive changes, as well as pseudopsychotic effects. KOR agonists can induce behavioral effects associated with various psychiatric disorders, including depression, schizophrenia, drug addiction, and bipolar disorder.61 Our analysis results found that psychological disorders are AEs strongly correlated with both Hydrorphone and morphine sulfate, which may be related to the KORs system in the body. If patients with psychological disorders need to use opioid drugs in clinical practice, it is necessary to consider the individualized medication risks of Hydromorphone and morphine and find alternative methods.
Since 1975, a large amount of strong literature has been accumulated to support the conclusion that opioid drugs regulate immune responses. In the vast majority of cases, these studies indicate that opioid drugs have immunosuppressive effects. However, with the publication of a paper in 2005, the hypothesis was proposed that opioid drugs have pro-inflammatory effects.62 Morphine is also considered an important release agent of histamine in human mast cells, showing significant activity against mast cells, whose activation often causes allergic reactions.63 Morphine first reduces the proliferation ability of macrophage progenitor cells and lymphocytes, then reduces the number of reactive macrophages to infection by inhibiting their recruitment into tissues, and finally activates the μ receptor, leading to insensitivity of chemokine receptors on macrophages. In addition, morphine also inhibits the phagocytic ability of macrophages, which overall reduces their ability to resist invading pathogens in vitro and in vivo.64 Long term morphine treatment can also weaken adaptive immune responses, such as impairing T cell function, altering cytokine expression, inhibiting T cell apoptosis and altering T cell differentiation, and reducing B cell function through μ receptors. However, there is almost no evidence to confirm the immunosuppressive effect of morphine in early clinical patients.65 However, hydromorphone, which is also an opioid drug, does not have immunosuppressive effects. This was confirmed in a comparative study evaluating the immunosuppressive effects of several opioid drugs on male Swiss mice. Morphine impaired spleen cell proliferation, NK cell activity, and IL-2 production, while hydromorphone treatment did not have a significant effect.66 Although many cell and animal experiments have shown that opioid drugs induce immune suppression in adaptive and innate immune systems, a definitive conclusion cannot be drawn due to the lack of relevant clinical and epidemiological evidence. This is also consistent with our analysis results, that is, morphine and hydromorphone, as opioid drugs, are associated with immune system disorders in their treatment. Among them, morphine treatment has a strong correlation, but further clinical and large-scale epidemiological evidence is needed to verify whether AEs are directly caused by drugs. However, in clinical practice, patients with immune system diseases should still be cautious when using morphine and hydromorphone for treatment.
As for the injury, The association between poisoning and procedural complications and two drug treatments has also been demonstrated in previous studies by scholars. For example, observational results have shown that opioid therapy can have negative effects on stem cells, thereby affecting cell healing and regeneration processes, resulting in reduced or even abnormal healing of damaged tissues.67–69 Other systemic AEs, including gastrointestinal, urogenital, respiratory, cardiovascular, neurological, and skin itching, can be caused by opioid therapy.38 However, the reactions of general disorders and administrative site conditions are only related to Hydromorphone treatment, which suggests that we need to balance drug efficacy and specific AEs when selecting analgesic regimens.
Considering the strong correlation between psychological disorders and both drug treatments, and the strong correlation between immune system disorders and morphine sulfate treatment, with a lower correlation with Hydromorphone, it is recommended to avoid using morphine for full course treatment in patients with fragile or disordered immune systems in clinical practice. If possible, these two drugs should be avoided as much as possible. Patients with obvious signals of general disorders and administrative site conditions should avoid using Hydromorphone, as it is positively correlated with Hydromorphone and not with morphone-sulfate at the SOC level. And injury, The signals of poisoning and procedural complexes are related to both types of drug therapy, and caution should be exercised when using both drugs or choosing alternative analgesic modes in patients with corresponding underlying diseases.
Although pharmacovigilance research is crucial for monitoring the safety of drugs after they are marketed and the corresponding FAERS database analysis methods are mature, they do have some limitations. In fact, many ADRs may not be reported correctly or have incomplete information, resulting in biased analysis results. And although this study conducted stratified descriptive analysis based on population distribution, considering that the data did not have strict control or experimental groups, and there was a lack of strict comparability between the two drug groups, the Hydromorphone and morphine drug data mainly reflected some prominent signal values at the overall level, and the extrapolation performance was limited. The causal relationship evaluation always lacked completeness, and further clinical observation and research were needed to determine whether there was a biological causal relationship. Therefore, these results should be interpreted with caution. With the progress of the times and the continuous development of medicine, many models have emerged to measure patient medication and patient drug AEs, such as population econometric models that fully consider patient characteristics to explain population trends and pharmacokinetic and pharmacodynamic data variability.70 There are also population exposure response models to evaluate the effectiveness of naloxone in treating opioid induced constipation in adults with chronic non cancer pain.71 With the continuous development and maturity of artificial intelligence technology, deploying big data models using artificial intelligence in the entire process of data collection, organization, and analysis not only requires rapid response but also ensures certain accuracy. Future research could consider using more rigorous prospective studies combined with large-scale artificial intelligence models to more accurately assess the safety risks of Hydromorphone and morphine.
Signals identified in this study were interpreted in the context of known pharmacological mechanisms and compared with existing literature. Biological plausibility was carefully considered to ensure that observed associations are consistent with current understanding. It is important to note that these signals do not imply causal relationships but should be regarded as risk alerts that warrant further investigation.
Conclusion
Our research suggests that at certain levels of SOCs and PTs, Hydromorphones and Variants have equal safety risks, particularly in terms of psychological disorders and immune system disorders. However, for patients with more obvious signals of general disorders and administrative site conditions, morphine may be more suitable than Hydromorphone. In addition, for drug dependence, which is a common PT signal in different age groups of the two drugs, the prognosis should be closely monitored after drug treatment, and public health monitoring capabilities should be strengthened if conditions permit. Some PT signals that have been screened and supported by research theories need more attention, and further experiments and research are needed to determine the reliability of these signals. This study is subject to several inherent limitations of the FAERS database, including missing data, confounding by concomitant medications, and inability to stratify by indication or outcome severity. Despite the limitations of FAERS database analysis, our study still provides some clues for reference in elucidating the key aspects of Hydromorphone and morphine security.
Data Sharing Statement
The data sets used during the current study are available from the corresponding author on a reasonable request. The datasets generated for this study can be found at https://www.fda.gov/drugs/fdas-adverse-event-reporting-system-faers/fda-adverse-event-reporting-system-faers-public-dashboard.
Ethics Approval and Consent to Participate
In accordance with the “Ethical Review Measures for Life Science and Medical Research Involving Humans” (issued on February 18, 2023, by the People’s Republic of China), this study complies with Article 32, Items 1 and 2, and falls under the category of research that does not require ethical review. The relevant provisions are as follows:
Article 32, Item 1: Research that does not involve human samples, data, or personal privacy, and where there is no direct intervention or collection of sensitive information from individuals, does not require ethical approval.
Article 32, Item 2: Research conducted using publicly available anonymized data or de-identified biological samples, and where no new interventions are made on participants, does not require ethical approval.
Therefore, this study does not require ethical review approval.
Disclosure
The authors declare that they have no competing interests.
References
1. Louisa D, Jason G, Jack S, et al. Global patterns of opioid use and dependence: harms to populations, interventions, and future action. Lancet. 2019;394(10208):1560–22. doi:10.1016/S0140-6736(19)32229-9
2. Keith H, Shover Chelsea L, Andrews Christina M, et al. Responding to the opioid crisis in North America and beyond: recommendations of the Stanford-Lancet Commission. Lancet. 2022;399(10324):555–604. doi:10.1016/S0140-6736(21)02252-2
3. Colvin Lesley A, Fiona B, Hales Tim G. Perioperative opioid analgesia-when is enough too much? A review of opioid-induced tolerance and hyperalgesia. Lancet. 2019;393(10180):1558–1568. doi:10.1016/S0140-6736(19)30430-1
4. Maosha D, Xiaoke D, Min C, et al. Strong opioids-induced cardiac, neurologic, and respiratory disorders: a real-world study from 2004 to 2023 based on FAERS. Naunyn Schmiedebergs Arch Pharmacol. 2024;397(6):4105–4121. doi:10.1007/s00210-023-02844-4
5. Abuse Substance. Key substance use and mental health indicators in the United States: results from the 2019 National Survey on Drug Use and Health. 2020.
6. Glare P, Aubrey KR, Myles PS. Transition from acute to chronic pain after surgery. Lancet. 2019;393(10180):1537–1546. doi:10.1016/S0140-6736(19)30352-6
7. Jiang X, Orton M, Feng R, et al. Chronic opioid usage in surgical patients in a large academic center. Ann Surg. 2017;265(4):722–727. doi:10.1097/SLA.0000000000001780
8. Johnson SP, Chung KC, Zhong L, et al. Risk of prolonged opioid use among opioid-naïve patients following common hand surgery procedures. J Hand Surg Am. 2016;41(10):947–57.e3. doi:10.1016/j.jhsa.2016.07.113
9. Santa Cruz Mercado A, Liu R, Bharadwaj KM, et al. Association of intraoperative opioid administration with postoperative pain and opioid use. JAMA Surg. 2023;158(8):854–864. doi:10.1001/jamasurg.2023.2009
10. Tricco AC, Parker A, Hezam A, et al. Controlled-release hydromorphone and risk of infection in adults: a systematic review. Harm Reduct J. 2023;20(1):60. doi:10.1186/s12954-023-00788-9
11. Sarhill N, Walsh D, Nelson KA. Hydromorphone: pharmacology and clinical applications in cancer patients. Support Care Cancer. 2001;9(2):84–96. doi:10.1007/s005200000183
12. Quigley C. Hydromorphone for acute and chronic pain. Cochrane Database Syst Rev. 2002;1:Cd003447.
13. Murray A, Hagen NA. Hydromorphone. J Pain Symptom Manage. 2005;29(5 Suppl):S57–66. doi:10.1016/j.jpainsymman.2005.01.007
14. Rapp SE, Egan KJ, Ross BK, et al. A multidimensional comparison of morphine and hydromorphone patient-controlled analgesia. Anesth Analg. 1996;82(5):1043–1048. doi:10.1097/00000539-199605000-00029
15. Shannon R, David S, Matthew C, et al. Hydromorphone versus morphine: a historical cohort study to evaluate the quality of postoperative analgesia. Can J Anaesth. 2021;68(2):226–234. doi:10.1007/s12630-020-01849-4
16. Yihang L, Xinying Y, Shuang L, et al. Effectiveness and safety of hydromorphone compared to morphine for postoperative analgesia: a systematic review and meta-analysis. Pain Physician. 2024;27(8):469–478. doi:10.36076/ppj.2024.7.469
17. Konrad M, Albert D, Erik O, et al. Morphine and hydromorphone effects, side effects, and variability: a crossover study in human volunteers. Anesthesiology. 2023;139(1):16–34. doi:10.1097/ALN.0000000000004567
18. Xianzheng Z, Jiang Z, Jun L, et al. Patient Controlled Subcutaneous Analgesia of Hydromorphone Versus Morphine to Treat Moderate and Severe Cancer Pain: a Randomized Double-Blind Controlled Trial. J Pain Symptom Manage. 2024;67(1):50–58. doi:10.1016/j.jpainsymman.2023.09.018
19. Sarah S, Charles G, Trottier Evelyne D, et al. Morphine or hydromorphone: which should be preferred? A systematic review. Arch Dis Child. 2021;106(10):1002–1009. doi:10.1136/archdischild-2020-319059
20. Hoon S, Joo GT. Side effect profiles of different opioids in the perioperative setting: are they different and can we reduce them? Br J Anaesth. 2019;123(3):266–268. doi:10.1016/j.bja.2019.06.009
21. Gedda C, Nygren J, Garpenbeck A, et al. Multimodal analgesia bundle and postoperative opioid use among patients undergoing colorectal surgery. JAMA Network Open. 2023;6(9):e2332408. doi:10.1001/jamanetworkopen.2023.32408
22. Carron M, Tamburini E, Linassi F, et al. Efficacy of nonopioid analgesics and adjuvants in multimodal analgesia for reducing postoperative opioid consumption and complications in obesity: a systematic review and network meta-analysis. Br J Anaesth. 2024;133(6):1234–1249. doi:10.1016/j.bja.2024.08.009
23. Knotkova H, Fine PG, Portenoy RK. Opioid rotation: the science and the limitations of the equianalgesic dose table. J Pain Symptom Manage. 2009;38(3):426–439. doi:10.1016/j.jpainsymman.2009.06.001
24. Mercadante S. Opioid rotation for cancer pain: rationale and clinical aspects. Cancer. 1999;86(9):1856–1866. doi:10.1002/(SICI)1097-0142(19991101)86:9<1856::AID-CNCR30>3.0.CO;2-G
25. Yu RJ, Krantz MS, Phillips EJ, et al. Emerging causes of drug-induced anaphylaxis: a review of anaphylaxis-associated reports in the FDA adverse event reporting system (FAERS). J Allergy Clin Immunol Pract. 2021;9(2):819–29.e2. doi:10.1016/j.jaip.2020.09.021
26. T G, Jiang A, Zhou C, et al. Adverse reactions associated with immune checkpoint inhibitors and bevacizumab: a pharmacovigilance analysis. Int J Cancer. 2023;152(3):480–495. doi:10.1002/ijc.34332
27. Yang F, Shay C, Abousaud M, et al. Patterns of toxicity burden for FDA-approved immune checkpoint inhibitors in the United States. J Exp Clin Cancer Res. 2023;42(1):4. doi:10.1186/s13046-022-02568-y
28. Zhang W, Chen M, Cai X, et al. Detection and analysis of signals of adverse events of memantine based on the US food and drug administration adverse event reporting system. Expert Opin Drug Saf. 2024;23(5):617–625. doi:10.1080/14740338.2024.2338251
29. Gao H, Zhai X, Y H, et al. Pharmacovigilance study of the association between progestogen and depression based on the FDA adverse event reporting System (FAERS). Sci Rep. 2025;15(1):1302. doi:10.1038/s41598-025-85826-1
30. Laxmaiah M, Bert F, Hary A, et al. Therapeutic use, abuse, and nonmedical use of opioids: a ten-year perspective. Pain Physician. 2010;13(5):401–435.
31. Alexandra S. FDA Announces Stronger Warnings for Opioid Painkillers. 2016.
32. Kaye AD, Dufrene K, Cooley J, et al. Neuropsychiatric effects associated with opioid-based management for palliative care patients. Curr Pain Headache Rep. 2024;28(7):587–594. doi:10.1007/s11916-024-01248-0
33. Grenald SA, Largent-Milnes TM, Vanderah TW. Animal models for opioid addiction drug discovery. Expert Opin Drug Discov. 2014;9(11):1345–1354. doi:10.1517/17460441.2014.966076
34. Stannard C, Gaskell H, Derry S, et al. Hydromorphone for neuropathic pain in adults. Cochrane Database Syst Rev. 2016;2016(5):Cd011604. doi:10.1002/14651858.CD011604.pub2
35. Pillay Smiley N, Alden T, Hartsell W, et al. Severe radiation necrosis successfully treated with bevacizumab in an infant with low-grade glioma and tumor-associated intractable trigeminal neuralgia. Pediatr Blood Cancer. 2016;63(9):1671–1673. doi:10.1002/pbc.26055
36. Klepstad P, Borchgrevink P, Hval B, et al. Long-term treatment with ketamine in a 12-year-old girl with severe neuropathic pain caused by a cervical spinal tumor. J Pediatr Hematol Oncol. 2001;23(9):616–619. doi:10.1097/00043426-200112000-00013
37. Delavallee M, Rooijakkers H, Koerts G, et al. Motor cortex stimulation in a three-year-old child with trigeminal neuropathic pain caused by a malignant glioma in the cerebellopontine angle: case report. Neurosurgery. 2011;69(2):E494–6. doi:10.1227/NEU.0b013e318218cf6f
38. Martin WR. Pharmacology of opioids. Pharmacol Rev. 1983;35(4):283–323. doi:10.1016/S0031-6997(25)06637-2
39. Yang Y, Wu P, Guo J, et al. Circadian time-dependent effects of experimental colitis on theophylline disposition and toxicity. Br J Pharmacol. 2024;181(19):3743–3759. doi:10.1111/bph.16440
40. Robson RA, Miners JO, Matthews AP, et al. Characterisation of theophylline metabolism by human liver microsomes. Inhibition and immunochemical studies. Biochem Pharmacol. 1988;37(9):1651–1659. doi:10.1016/0006-2952(88)90423-6
41. Feelemyer JP, Richard E, Khan MR, et al. Does the association between stimulant use and high risk sexual behavior vary by injection drug use, sexual minority status, or HIV infection status? A meta-analysis. AIDS Behav. 2023;27(9):2883–2890. doi:10.1007/s10461-023-04012-4
42. Tookes H, Bartholomew TS, Geary S, et al. Rapid identification and investigation of an HIV risk network among people who inject drugs -Miami, FL, 2018. AIDS Behav. 2020;24(1):246–256. doi:10.1007/s10461-019-02680-9
43. Lyss SB, Buchacz K, Mcclung RP, et al. Responding to outbreaks of human immunodeficiency virus among persons who inject drugs-United States, 2016-2019: perspectives on recent experience and lessons learned. J Infect Dis. 2020;222(Suppl 5):S239–s49. doi:10.1093/infdis/jiaa112
44. Prevention centers for disease control and HIV and injection drug use.
45. Cui L, Cai H, Sun F, et al. Beta-endorphin inhibits the inflammatory response of bovine endometrial cells through δ opioid receptor in vitro. Dev Comp Immunol. 2021;121:104074. doi:10.1016/j.dci.2021.104074
46. Donato J, Rao K, Lewis T. Pharmacology of common analgesic and sedative drugs used in the neonatal intensive care unit. Clin Perinatol. 2019;46(4):673–692. doi:10.1016/j.clp.2019.08.004
47. Allen JW, Horais KA, Tozier NA, et al. Time course and role of morphine dose and concentration in intrathecal granuloma formation in dogs: a combined magnetic resonance imaging and histopathology investigation. Anesthesiology. 2006;105(3):581–589. doi:10.1097/00000542-200609000-00024
48. Vadera S, Harrop JS, Sharan AD. Intrathecal granuloma and intramedullary abscess associated with an intrathecal morphine pump. Neuromodulation. 2007;10(1):6–11. doi:10.1111/j.1525-1403.2007.00081.x
49. Wei S, He C, Xie X, et al. Which fluoroquinolone is safer when combined with bedaquiline for tuberculosis treatment: evidence from FDA adverse event reporting system database from 2013 to 2024. Front Pharmacol. 2024;15:1491921. doi:10.3389/fphar.2024.1491921
50. Ciucă Anghel DM, Nițescu GV, Tiron AT, et al. Understanding the mechanisms of action and effects of drugs of abuse. Molecules. 2023;28(13):4969. doi:10.3390/molecules28134969
51. Schatzberg AF. Opioids in psychiatric disorders: back to the future? Am J Psychiatry. 2016;173(6):564–565. doi:10.1176/appi.ajp.2015.15101354
52. Wang Y, Zhuang Y, Diberto JF, et al. Structures of the entire human opioid receptor family. Cell. 2023;186(2):413–27.e17. doi:10.1016/j.cell.2022.12.026
53. Tejeda HA, Bonci A. Dynorphin/kappa-opioid receptor control of dopamine dynamics: implications for negative affective states and psychiatric disorders. Brain Res. 2019;1713:91–101. doi:10.1016/j.brainres.2018.09.023
54. Katrin A, Poornima B, Bond Richard A, et al. Adrenoceptors (version 2019.4) in the IUPHAR/BPS guide to pharmacology database. IUPHAR/BPS Guide Pharmacol CITE. 2019;2019(4):2633.
55. Bian JM, N W, Su RB, et al. Opioid receptor trafficking and signaling: what happens after opioid receptor activation? Cell Mol Neurobiol. 2012;32(2):167–184. doi:10.1007/s10571-011-9755-5
56. Berke JD. What does dopamine mean? Nat Neurosci. 2018;21(6):787–793. doi:10.1038/s41593-018-0152-y
57. Broyd A, Balzan RP, Woodward TS, et al. Dopamine, cognitive biases and assessment of certainty: a neurocognitive model of delusions. Clin Psychol Rev. 2017;54:96–106. doi:10.1016/j.cpr.2017.04.006
58. Mccutcheon R, Abi-Dargham A, Howes OD. Schizophrenia, dopamine and the striatum: from biology to symptoms. Trends Neurosci. 2019;42(3):205–220. doi:10.1016/j.tins.2018.12.004
59. Shippenberg TS. The dynorphin/kappa opioid receptor system: a new target for the treatment of addiction and affective disorders? Neuropsychopharmacology. 2009;34(1):247. doi:10.1038/npp.2008.165
60. Chavkin C, James IF, Goldstein A. Dynorphin is a specific endogenous ligand of the kappa opioid receptor. Science. 1982;215(4531):413–415. doi:10.1126/science.6120570
61. Tejeda HA, Shippenberg TS, Henriksson R. The dynorphin/κ-opioid receptor system and its role in psychiatric disorders. Cell Mol Life Sci. 2012;69(6):857–896. doi:10.1007/s00018-011-0844-x
62. Eisenstein TK. The role of opioid receptors in immune system function. Front Immunol. 2019;10:2904. doi:10.3389/fimmu.2019.02904
63. Baldo BA, Pham NH. Opioid toxicity: histamine, hypersensitivity, and MRGPRX2. Arch Toxicol. 2023;97(2):359–375. doi:10.1007/s00204-022-03402-2
64. Plein LM, Rittner HL. Opioids and the immune system - friend or foe. Br J Pharmacol. 2018;175(14):2717–2725. doi:10.1111/bph.13750
65. Roy S, Ninkovic J, Banerjee S, et al. Opioid drug abuse and modulation of immune function: consequences in the susceptibility to opportunistic infections. J Neuroimmune Pharmacol. 2011;6(4):442–465. doi:10.1007/s11481-011-9292-5
66. Sacerdote P, Manfredi B, Mantegazza P, et al. Antinociceptive and immunosuppressive effects of opiate drugs: a structure-related activity study. Br J Pharmacol. 1997;121(4):834–840. doi:10.1038/sj.bjp.0701138
67. Martin JL, Koodie L, Krishnan AG, et al. Chronic morphine administration delays wound healing by inhibiting immune cell recruitment to the wound site. Am J Pathol. 2010;176(2):786–799. doi:10.2353/ajpath.2010.090457
68. Coluzzi F, Scerpa MS, Centanni M. The effect of opiates on bone formation and bone healing. Curr Osteoporos Rep. 2020;18(3):325–335. doi:10.1007/s11914-020-00585-4
69. Barlass U, Dutta R, Cheema H, et al. Morphine worsens the severity and prevents pancreatic regeneration in mouse models of acute pancreatitis. Gut. 2018;67(4):600–602. doi:10.1136/gutjnl-2017-313717
70. Välitalo P, Ranta VP, Hooker AC, et al. Population pharmacometrics in support of analgesics studies. Acta Anaesthesiol Scand. 2014;58(2):143–156. doi:10.1111/aas.12253
71. Al-Huniti N, Xu H, Zhou D, et al. Population exposure-response modeling supported selection of naloxegol doses in Phase III studies in patients with opioid-induced constipation. CPT Pharmacometrics Syst Pharmacol. 2017;6(10):705–711. doi:10.1002/psp4.12229
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.