Back to Journals » Journal of Inflammation Research » Volume 19
Comparative Prognostic Performance of SOFA2.0 and SOFA for 28-Day Mortality in Patients Developing Sepsis During ECMO Support
Authors Chen JY, Gu XL ![]() , Liu HY
, Liu HY ![]() , Li T, Yu YW
, Li T, Yu YW ![]() , Xu M
, Xu M
Received 10 March 2026
Accepted for publication 12 June 2026
Published 9 July 2026 Volume 2026:19 607506
DOI https://doi.org/10.2147/JIR.S607506
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Xin Du
Jia-Yi Chen,1,2,* Xiao-Ling Gu,3,* Hai-Yan Liu,4 Tong Li,5 Yong-Wei Yu,5 Mi Xu5
1Intensive Care Unit, Affiliated Hangzhou First People’s Hospital, School of Medicine, Westlake University, Hangzhou, Zhejiang, 310000, People’s Republic of China; 2Intensive Care Unit, Hangzhou Geriatric Hospital, Hangzhou, Zhejiang, 310022, People’s Republic of China; 3Intensive Care Unit, Taicang Affiliated Hospital of Soochow University, Taicang, Jiangsu, 215488, People’s Republic of China; 4Intensive Care Unit, The Second Affiliated Hospital of Henan University of Science and Technology, Luoyang, Henan, 471000, People’s Republic of China; 5Intensive Care Unit, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, Zhejiang, 310003, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yong-Wei Yu, Intensive Care Unit, The First Affiliated Hospital, Zhejiang University School of Medicine, No. 79 Qingchun Road, Hangzhou, Zhejiang, 310003, People’s Republic of China, Email [email protected] Mi Xu, Intensive Care Unit, The First Affiliated Hospital, Zhejiang University School of Medicine, No. 79 Qingchun Road, Hangzhou, Zhejiang, 310003, People’s Republic of China, Email [email protected]
Objective: The Sequential Organ Failure Assessment (SOFA) score is widely used to evaluate organ dysfunction in sepsis, but its performance may be affected in patients receiving extracorporeal membrane oxygenation (ECMO), where extracorporeal support and related therapies can alter physiologic parameters. An updated version, SOFA2.0, has been proposed to better reflect organ dysfunction in contemporary critical care. This study compared the prognostic performance of SOFA2.0 and traditional SOFA in patients who developed sepsis during ECMO support.
Methods: We conducted a single-center retrospective cohort study including adult patients who developed sepsis during ECMO support between January 2021 and December 2024. SOFA and SOFA2.0 scores were calculated at the time of Sepsis-3 diagnosis using the same clinical dataset. The primary outcome was 28-day mortality. Predictive performance was evaluated using receiver operating characteristic analysis, multivariable logistic regression, and reclassification metrics including net reclassification improvement (NRI) and integrated discrimination improvement (IDI).
Results: Fifty-three patients were included, with a median age of 54.0 years (IQR, 46.0– 61.0), 79.2% male patients, and a 28-day mortality rate of 67.9%. Both SOFA and SOFA2.0 scores were significantly higher in non-survivors than in survivors. SOFA2.0 demonstrated a numerically higher AUC than SOFA (0.765 [95% CI: 0.635– 0.896] vs. 0.719 [95% CI: 0.573– 0.865]), although the confidence intervals overlapped. Reclassification analysis showed positive continuous NRI (0.728) and IDI (0.071), indicating numerically favorable reclassification performance for SOFA2.0 compared with traditional SOFA. However, SOFA2.0 was not independently associated with mortality after multivariable adjustment.
Conclusion: In patients who developed sepsis during ECMO support, SOFA2.0 demonstrated comparable discriminatory performance to traditional SOFA, without clear evidence of superiority. Although SOFA2.0 showed numerically favorable discrimination and reclassification metrics, these findings should be interpreted cautiously given the limited sample size and single-center design.
Keywords: extracorporeal membrane oxygenation, sepsis, sequential organ failure assessment, SOFA 2 score, mortality
Introduction
Sepsis remains a leading cause of mortality among critically ill patients worldwide.1 The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3) define sepsis as life-threatening organ dysfunction caused by a dysregulated host response to infection, operationalized clinically as an acute increase in the Sequential Organ Failure Assessment (SOFA) score of ≥2 points.2 Since its incorporation into the Sepsis-3 framework, the SOFA score has served both as a diagnostic component and as a tool for prognostic risk stratification in general intensive care unit (ICU) populations.3
However, the performance of the traditional SOFA score may be challenged in patients receiving extracorporeal membrane oxygenation (ECMO).4 ECMO profoundly alters cardiopulmonary physiology and typically requires vasoactive agents, mechanical ventilation adjustments, and deep sedation.5 These factors may influence multiple SOFA domains, including respiratory, cardiovascular, and neurologic components, potentially limiting the score’s ability to reflect intrinsic organ dysfunction in this setting.6
Recently, an updated version of the SOFA score (SOFA2.0) has been proposed to better align organ dysfunction assessment with contemporary critical care practices.7 Compared with the original SOFA score, which has remained largely unchanged for nearly three decades, SOFA2.0 incorporates updated definitions of organ dysfunction, commonly used pharmacological and mechanical organ support therapies, and revised thresholds to better reflect current patterns of care and associated mortality risk; for example, SOFA2.0 incorporates contemporary vasopressor use and organ-support strategies into the assessment of organ dysfunction, aiming to improve prognostic relevance in modern critical care settings. These modifications may be particularly relevant in patients receiving ECMO support, in whom conventional physiologic parameters are frequently influenced by extracorporeal circulation and advanced organ support.7,8 Whether SOFA2.0 offers incremental prognostic value compared with the traditional SOFA score in patients who develop sepsis during ongoing ECMO support remains unknown, as evidence specifically addressing this population is currently lacking.
Patients supported with ECMO represent a particularly vulnerable population with substantial baseline organ dysfunction and high mortality.9 Several ECMO-specific prognostic tools, such as the Respiratory ECMO Survival Prediction score for respiratory failure and the Survival After Veno-Arterial ECMO score for refractory cardiogenic shock, have been developed to estimate survival in patients requiring ECMO support.10,11 However, these models are primarily designed for prognosis according to ECMO indication and pre-ECMO characteristics, rather than for dynamic assessment of infection-related organ dysfunction when sepsis develops during ongoing ECMO support. When sepsis occurs during ECMO support, distinguishing infection-related organ deterioration from ECMO-associated physiologic alterations becomes especially challenging.12,13 In this context, reassessment of organ dysfunction scoring systems is warranted.
Therefore, we conducted a retrospective comparative study to evaluate the prognostic performance of SOFA2.0 versus traditional SOFA at the time of Sepsis-3 diagnosis in patients who developed sepsis during ECMO support, using 28-day mortality as the primary outcome. We hypothesized that, by incorporating updated organ dysfunction definitions, contemporary organ-support therapies, and revised thresholds, SOFA2.0 may provide more clinically relevant risk stratification than the traditional SOFA score in this specific population.
Materials and Methods
Ethical Approval
This study was approved by the Ethics Committee of the First Affiliated Hospital, Zhejiang University School of Medicine (Approval No. 2025BIIT No.0961, approved in September 2025). Due to the retrospective observational design and the use of anonymized clinical data, the requirement for informed consent was waived by the Ethics Committee. All patient data were handled confidentially and anonymized prior to analysis. This study was conducted in accordance with the Declaration of Helsinki.
Study Design and Population
Study Participants
This single-center, retrospective cohort study consecutively included adult patients who received extracorporeal membrane oxygenation (ECMO) support in the Intensive Care Unit of the First Affiliated Hospital, Zhejiang University School of Medicine between January 2021 and December 2024, and who developed sepsis during ongoing ECMO support. Related investigations from this clinical cohort have previously been reported, including a study focusing on bleeding risk indicators during ECMO support.14
Sepsis was diagnosed according to the Sepsis-3 criteria, defined as suspected or confirmed infection accompanied by an acute increase in the Sequential Organ Failure Assessment (SOFA) score of ≥2 points from the pre-infection baseline (ΔSOFA ≥2).
Inclusion Criteria
- Aged between 18 and 70 years.
- ECMO support duration ≥ 24 hours after initiation.
- Sepsis that developed after ECMO initiation and during ongoing ECMO support.
- For patients who underwent more than one ECMO run during the study period, only the first ECMO run was included in the analysis.
Exclusion Criteria
- Missing data preventing calculation of SOFA or SOFA2.0 at the time of sepsis diagnosis.
- Missing data preventing determination of the pre-infection baseline SOFA required for ΔSOFA calculation.
- Transferred-in patients lacking sufficient pre-transfer data (eg., missing key physiologic/laboratory variables required for baseline SOFA assessment and sepsis adjudication) to adjudicate the first Sepsis-3 episode after ECMO initiation.
- Pregnancy or lactation.
Sepsis Identification and Index Time Definition
In our ICU, organ function parameters in ECMO-supported patients are routinely assessed daily, with standard laboratory testing performed between 05:00 and 05:30 and additional measurements obtained when clinically indicated. Sepsis screening was supported by automated electronic surveillance within the hospital information system and confirmed by clinician adjudication. For this study, the pre-infection baseline SOFA score was defined as the most recent routine daily SOFA assessment prior to fulfillment of Sepsis-3 criteria, typically derived from the preceding 05:00 evaluation, which may introduce potential misclassification bias due to the use of indirect estimation. The index time was defined as the first time point at which Sepsis-3 criteria were met after ECMO initiation during ongoing ECMO support. Both SOFA and SOFA2.0 scores were calculated at the index time using physiologic and laboratory measurements closest to, and not after, sepsis adjudication, with laboratory values anchored to the specimen collection timestamp rather than reporting time to minimize information bias.
SOFA and SOFA2.0 Assessment
At the index time of sepsis diagnosis, both the traditional SOFA score and SOFA2.0 score were retrospectively calculated using the same contemporaneous clinical and laboratory dataset, with SOFA2.0 calculated according to the definitions and scoring criteria described in the original development and validation studies.7,8 In our institution, ECMO-supported patients undergo routine daily laboratory assessment between 05:00 and 05:30, including arterial blood gas analysis. When Sepsis-3 criteria were fulfilled during this routine evaluation, the corresponding dataset was used for score calculation. In cases where sepsis was diagnosed later in the day due to new clinical deterioration, additional laboratory tests were obtained as clinically indicated, and score components were derived from measurements available at the time of adjudication; variables not remeasured were obtained from the most recent assessment prior to the index time. No post-index data were used. Patients with missing variables preventing complete calculation of either scoring system were excluded, and no data imputation was performed. A complete-case analysis approach was adopted to avoid introducing additional assumptions associated with imputation methods in this relatively small sample.
Outcome Definition
The primary outcome was 28-day all-cause mortality, defined as death from any cause within 28 days following the index time of sepsis diagnosis during ECMO support. A 28-day endpoint was selected because it is a commonly used and clinically relevant short-term outcome measure in sepsis and critical care research. Survival status was determined through review of electronic medical records and follow-up documentation, with no loss to follow-up. Patients alive at 28 days were considered survivors for outcome analysis.
Statistical Analysis
Continuous variables were expressed as medians with interquartile ranges (IQRs), and categorical variables were presented as frequencies and percentages. Comparisons between survivors and non-survivors were performed using the Mann–Whitney U-test for continuous variables and Fisher’s exact test for categorical variables.
The predictive performance of SOFA and SOFA2.0 for 28-day mortality was evaluated using receiver operating characteristic (ROC) curve analysis, with area under the curve (AUC) and 95% confidence intervals estimated by bootstrap resampling (2,000 iterations). Risk stratification was assessed using the median score of each scoring system as the cutoff value, which was chosen to provide a data-driven and unbiased threshold in the absence of established clinically validated cutoffs for this specific population, and sensitivity, specificity, Youden’s index, and crude odds ratios were calculated. Continuous net reclassification improvement (NRI) and integrated discrimination improvement (IDI) were computed based on logistic regression models including either SOFA or SOFA2.0 as a single predictor, using the improveProb function from the Hmisc package. The association between the two scoring systems was assessed using Spearman’s rank correlation coefficient, and agreement was further evaluated by Bland–Altman analysis. Univariable and multivariable logistic regression analyses were performed to assess the independent predictive value of SOFA2.0. Variables with P < 0.1 in univariable analysis and those considered clinically relevant were included in the multivariable model; a threshold of P < 0.1 was used for variable selection in order to avoid premature exclusion of potentially relevant predictors in this relatively small exploratory cohort, whereas a two-sided P < 0.05 was retained as the criterion for statistical significance in the final analyses. Given the limited number of outcome events, covariate selection was further constrained to reduce the risk of model overfitting, and the number of variables included in the final model was limited to maintain an appropriate event-to-variable ratio and to minimize potential collinearity. All statistical tests were two-sided, with P < 0.05 considered statistically significant. Statistical analyses were conducted using R software (version 4.4.0; R Foundation for Statistical Computing, Vienna, Austria), primarily with the pROC and Hmisc packages.
Results
Study Population
A total of 418 patients who received ECMO support between January 2021 and December 2024 were screened for eligibility. After applying the predefined inclusion and exclusion criteria, 53 patients who developed sepsis during ECMO support were included in the final analysis. The main reasons for exclusion included the absence of sepsis during ECMO support, insufficient ECMO duration, and missing data required for SOFA or SOFA2.0 calculation. The patient selection process is shown in Figure 1.
 |
Figure 1 Flowchart. |
The median age of the cohort was 54.0 years (IQR, 46.0–61.0), 42 patients (79.2%) were male, and the 28-day mortality rate was 67.9% (36/53) (Supplementary Table 1).
Baseline Characteristics and Association with Prognosis
Baseline characteristics of the study cohort stratified by survival status are presented in Table 1. No significant differences were observed between survivors and non-survivors in demographic variables including age, sex, and body mass index (all P > 0.05). In terms of disease severity, both SOFA and SOFA2.0 scores were significantly higher in non-survivors compared with survivors (SOFA: median 11.0 vs. 7.0, P = 0.014; SOFA2.0: median 16.0 vs. 9.0, P = 0.003), and the neurological subscore was also higher in the non-survivor group (median 3.0 vs. 0.0, P = 0.049). Regarding ECMO-related characteristics, the duration of ECMO support was significantly shorter in non-survivors (median 10.0 days vs. 24.0 days, P = 0.009). The distribution of ECMO configurations showed a trend toward statistical significance (P = 0.069), with ECPR observed exclusively among non-survivors. No significant differences were found between the two groups in infection-related variables, including the primary site of infection and blood culture positivity (all P > 0.05). Laboratory parameters, including platelet count, creatinine, and lactate levels, were also comparable between the two groups, although lactate showed a non-significant trend toward higher values in non-survivors.
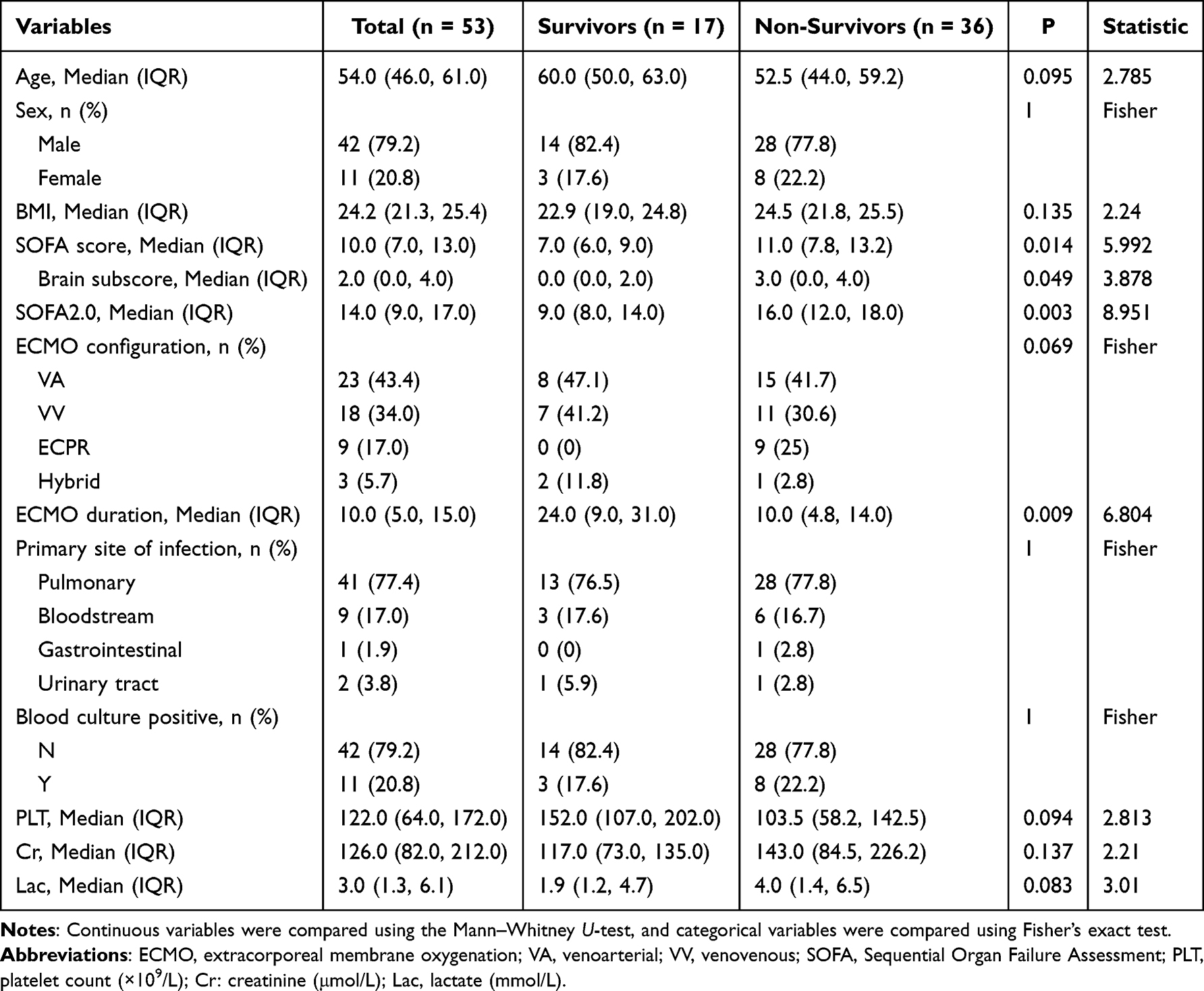 |
Table 1 Baseline Characteristics of Survivors and Non-Survivors |
Distribution Characteristics of SOFA and SOFA2.0 Scores
The distributions of SOFA and SOFA2.0 scores stratified by survival status are illustrated in Figure 2A and B. Both scoring systems showed higher score distributions in non-survivors compared with survivors. Overall, SOFA2.0 exhibited a wider distribution range than the traditional SOFA score, reflecting its expanded scoring scale. These distribution patterns visually illustrate differences between survivors and non-survivors but should be interpreted as descriptive findings rather than definitive evidence of discriminatory performance.
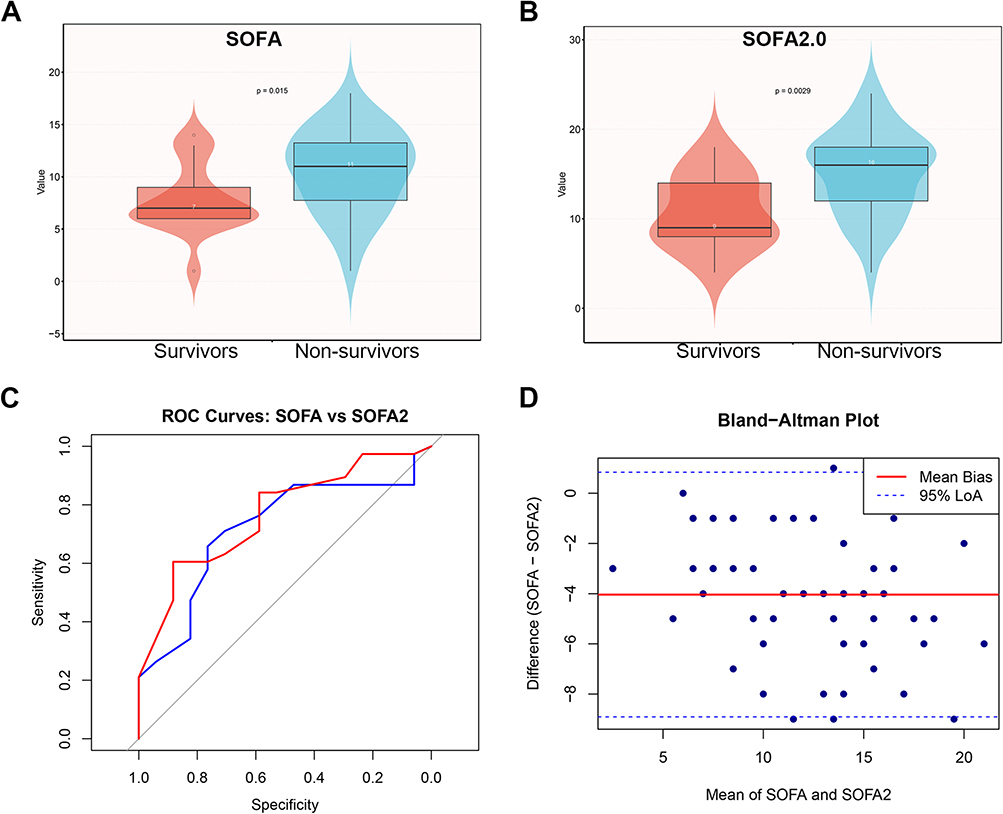 |
Figure 2 Comparative performance of SOFA and SOFA2.0 for 28-day mortality prediction in patients who developed sepsis during ECMO support (n = 53). (A) Box plots of SOFA scores stratified by survival status. (B) Box plots of SOFA2.0 scores stratified by survival status. (C) Receiver operating characteristic (ROC) curves for SOFA and SOFA2.0 scores, with area under the curve (AUC) and 95% confidence intervals for prediction of 28-day mortality. (D) Bland–Altman agreement analysis between SOFA and SOFA2.0 scores, showing mean difference and limits of agreement. Group comparisons were performed using the Mann–Whitney U-test. A two-sided P < 0.05 was considered statistically significant. |
Multivariable Logistic Regression Analysis
Multivariable logistic regression analysis was performed to evaluate the independent association between SOFA2.0 and mortality (Table 2). In univariable analysis, higher SOFA2.0 scores were significantly associated with increased mortality risk (OR = 1.24, 95% CI: 1.07–1.44, P = 0.005). However, after adjustment for renal subscore, antithrombin III level, and platelet count at 24 hours, the association between SOFA2.0 and mortality was no longer statistically significant (adjusted OR = 1.01, 95% CI: 0.47–2.18, P = 0.974). None of the other variables included in the model demonstrated an independent association with mortality.
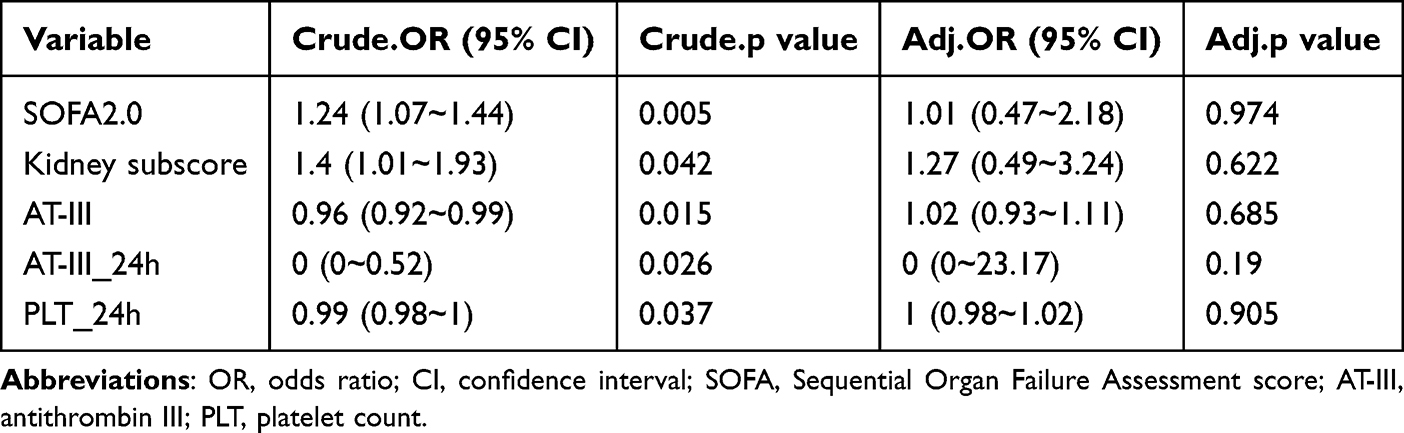 |
Table 2 Logistic Multivariate Analysis |
ROC Curve Analysis (SOFA vs. SOFA2.0)
Receiver operating characteristic (ROC) curve analysis was performed to evaluate the discriminatory performance of SOFA and SOFA2.0 for mortality prediction (Figure 2C and Table 3). The area under the curve (AUC) for SOFA2.0 was 0.765 (95% CI: 0.635–0.896), which was numerically higher than that of SOFA (AUC: 0.719, 95% CI: 0.573–0.865). However, the confidence intervals overlapped, suggesting comparable discriminatory ability between the two scoring systems. The modest numerical difference between the AUC values should therefore be interpreted cautiously and does not establish clear superiority of SOFA2.0 over the traditional SOFA score.
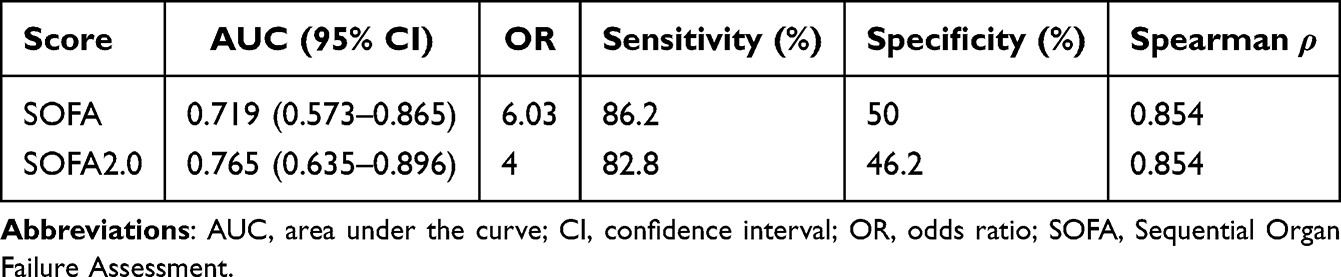 |
Table 3 Spearman Correlation Coefficients and Sensitivity Analysis for SOFA and SOFA2.0 |
Using the median score as the cutoff value, patients with higher SOFA scores had an odds ratio (OR) of 6.03 for mortality, whereas the corresponding OR for SOFA2.0 was 4.00. SOFA demonstrated slightly higher sensitivity than SOFA2.0 (86.2% vs. 82.8%), while specificity was modest for both scores (50.0% vs. 46.2%).
Correlation and Agreement Between Scores
The correlation and agreement between SOFA and SOFA2.0 scores were further evaluated (Table 3 and Figure 2D). Spearman correlation analysis demonstrated a strong positive correlation between the two scoring systems (ρ = 0.854), indicating consistent patient risk ranking. Bland–Altman analysis showed a mean bias of −4.0 points (95% limits of agreement: −8.6 to −0.4), suggesting that SOFA scores were systematically lower than SOFA2.0 scores while maintaining acceptable agreement between the two methods.
Reclassification Analysis (NRI and IDI)
To further compare the reclassification performance of SOFA2.0 and SOFA, continuous net reclassification improvement (NRI) and integrated discrimination improvement (IDI) analyses were performed (Table 4). The continuous NRI was 0.728, indicating improved risk reclassification when SOFA2.0 was used instead of SOFA. In addition, the IDI was 0.071, suggesting improved separation of predicted mortality risk between survivors and non-survivors. These findings indicate numerically favorable reclassification performance for SOFA2.0 compared with the traditional SOFA score; however, the interpretation of NRI and IDI should be approached with caution, as these metrics remain subject to methodological debate.
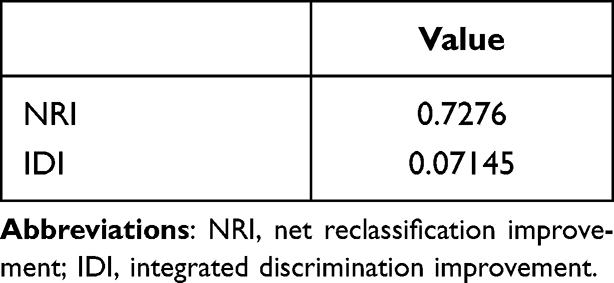 |
Table 4 Continuous Net Reclassification Improvement (NRI) and Integrated Discrimination Improvement (IDI) |
Discussion
In this retrospective cohort of patients who developed sepsis during ECMO support, both the traditional SOFA score and the updated SOFA2.0 score demonstrated the ability to discriminate 28-day mortality risk. SOFA2.0 showed a numerically higher AUC and favorable reclassification metrics, including positive NRI and IDI values. However, given the overlapping confidence intervals, lack of independent association in multivariable analysis, and the exploratory nature of the study, these findings should be interpreted as indicating broadly comparable prognostic performance rather than clear superiority over the conventional SOFA score. SOFA2.0 did not remain independently associated with mortality after adjustment in multivariable analysis, which may be attributable to the limited sample size, potential collinearity between organ dysfunction variables, and the complex influence of ECMO-related support on physiologic parameters. In addition, the shorter duration of ECMO support observed in non-survivors may partly reflect survivorship bias, as patients who died earlier inherently had less time to receive prolonged support.
Several factors may explain why SOFA2.0 did not demonstrate independent prognostic significance in the multivariable model. In ECMO-supported populations, mortality is often strongly influenced by the underlying indication for ECMO and baseline disease severity.15–17 Patients receiving ECMO frequently present with severe cardiopulmonary failure or require extracorporeal support after cardiac arrest, conditions that may dominate outcome determination.9,18 In addition, the extensive use of organ support therapies during ECMO, including circulatory support, renal replacement therapy, and deep sedation, may modify physiologic parameters incorporated into organ dysfunction scores.19,20 This may weaken the direct relationship between measured organ dysfunction and underlying disease severity, thereby affecting the prognostic performance of conventional scoring systems. Consequently, the measured organ dysfunction at a single time point may not fully reflect the overall physiologic reserve of these critically ill patients. The observed shorter ECMO duration in non-survivors should be interpreted cautiously, as it likely reflects survivorship bias, with early mortality leading to shorter support duration rather than a protective effect of prolonged ECMO.
Early identification of patients at increased risk of mortality is particularly important in the ECMO setting, where clinical deterioration may occur rapidly and management decisions often need to be made under significant time pressure.21 However, the clinical utility of SOFA2.0 should not be overstated. Because this study assessed both scores at a single index time point, the analysis may not fully capture dynamic changes in organ dysfunction after sepsis onset. Therefore, prognostic assessment in ECMO-supported patients should remain multifactorial and incorporate the underlying indication for ECMO, ECMO-related physiologic alterations, and the trajectory of organ dysfunction.22–24 In this context, SOFA2.0 should be regarded as a supplementary risk-stratification tool rather than a standalone determinant of clinical decision-making.
The SOFA score is widely used for organ dysfunction assessment in critically ill patients, including those with sepsis.2,25 However, the predictive performance of SOFA may vary across different clinical contexts, particularly in ECMO-supported populations, where extracorporeal circulation and associated therapies can substantially influence physiologic parameters used in organ dysfunction assessment.6,12,13 In ECMO-supported patients, several physiologic variables included in the SOFA score can be influenced by extracorporeal circulation and concurrent therapies, which may reduce the direct relationship between measured organ dysfunction and clinical outcomes.26–28 The updated SOFA2.0 score was proposed to improve the assessment of organ dysfunction in contemporary critical care settings. Our findings suggest that although SOFA2.0 demonstrated numerically favorable discrimination and reclassification metrics, its overall prognostic performance in patients who developed sepsis during ECMO support was broadly comparable to that of the traditional SOFA score.
Several limitations of this study should be acknowledged. First, this was a single-center retrospective study with a relatively small sample size, which may limit the generalizability of the findings to other clinical settings. Second, as a regional ECMO referral center, our institution receives a substantial proportion of patients transferred from other hospitals after ECMO initiation due to clinical deterioration or management challenges. This referral pattern may result in a cohort with higher baseline severity and may partially explain the relatively high mortality observed in this study, which should therefore be interpreted in the context of a high-risk referral population. In addition, ECMO type and underlying indications were not included in the multivariable model due to sample size constraints, which may have introduced residual confounding. Finally, although efforts were made to standardize data collection and score calculation, residual confounding inherent to observational studies cannot be completely excluded. In addition, given the limited sample size, the robustness of multivariable modeling and cutoff-based stratification should be interpreted with caution, and further validation in larger cohorts is required. Furthermore, the exclusion of patients with missing data without imputation may have introduced selection bias and reduced statistical power. Moreover, the absence of statistically significant differences in baseline characteristics between survivors and non-survivors should be interpreted with caution, as the limited sample size may have reduced the power to detect subtle between-group differences.
In patients who developed sepsis during ECMO support, both SOFA and SOFA2.0 demonstrated discriminatory ability for 28-day mortality. Although SOFA2.0 showed numerically favorable discrimination and reclassification metrics, no clear superiority over the traditional SOFA score was demonstrated. Furthermore, SOFA2.0 did not remain independently associated with mortality after multivariable adjustment. These findings should be interpreted as exploratory given the limited sample size and single-center design, and SOFA2.0 should be regarded as a supportive risk-stratification tool rather than a standalone predictor for clinical decision-making. Further validation in larger multicenter cohorts is warranted.
Data Sharing Statement
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
Consent for Publication
All listed authors consent to the submission, and all data are used with the consent of the person generating the data.
Acknowledgments
Thanks to Zhejiang University Press for the language revision of our manuscript.
Author Contributions
Jia-Yi Chen: Conceptualization, Data curation, Investigation, Formal analysis, Visualization, Writing-original draft. Xiao-Ling Gu: Data curation, Investigation, Formal analysis, Writing-review & editing. Hai-Yan Liu: Funding acquisition, Investigation, Data curation, Writing-review & editing. Tong Li: Investigation, Resources, Writing-review & editing. Yong-Wei Yu: Conceptualization, Methodology, Supervision, Project administration, Writing-review & editing. Mi Xu: Methodology, Supervision, Writing-review & editing.
All authors have agreed on the journal to which the article has been submitted; reviewed and approved all versions of the manuscript; and agree to take responsibility and be accountable for the contents of the article.
Funding
This work was supported by the 2024 Public Welfare Research Guidance Project in the Field of Agriculture and Social Development (Grant No. 20241029Y088).
Disclosure
The authors declare that they have no competing interests.
References
1. Rudd KE, Johnson SC, Agesa KM, et al. Global, regional, and national sepsis incidence and mortality, 1990-2017: analysis for the Global Burden of Disease Study. Lancet. 2020;395:200–10. doi:10.1016/S0140-6736(19)32989-7
2. Seymour CW, Liu VX, Iwashyna TJ, et al. Assessment of clinical criteria for sepsis: for the third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA. 2016;315:762–774. doi:10.1001/jama.2016.0288
3. Do SN, Dao CX, Nguyen TA, et al. Sequential Organ Failure Assessment (SOFA) score for predicting mortality in patients with sepsis in vietnamese intensive care units: a multicentre, cross-sectional study. BMJ Open. 2023;13(e064870):e064870. doi:10.1136/bmjopen-2022-064870
4. Lambden S, Laterre PF, Levy MM, Francois B. The SOFA score-development, utility and challenges of accurate assessment in clinical trials. Critical Care. 2019;23:374. doi:10.1186/s13054-019-2663-7
5. Lee HJ, Ko BS, Ryoo SM, et al. Modified cardiovascular SOFA score in sepsis: development and internal and external validation. BMC Med. 2022;20:263. doi:10.1186/s12916-022-02461-7
6. Spinelli E, Mauri T, Carlesso E, et al. Time-Course of physiologic variables during extracorporeal membrane oxygenation and outcome of severe acute respiratory distress syndrome. ASAIO. 2020;66:663–670. doi:10.1097/MAT.0000000000001048
7. Moreno R, Rhodes A, Ranzani O, et al. Rationale and methodological approach underlying the development of the Sequential Organ Failure Assessment (SOFA)-2 score: a consensus statement. JAMA Network Open. 2025;8:e2545040. doi:10.1001/jamanetworkopen.2025.45040
8. Ranzani OT, Singer M, Salluh JIF, et al. Development and validation of the sequential organ failure assessment (SOFA)-2 score. JAMA. 2025;334:2090–2103. doi:10.1001/jama.2025.20516
9. Rajsic S, Treml B, Jadzic D, et al. Extracorporeal membrane oxygenation for cardiogenic shock: a meta-analysis of mortality and complications. Ann Intens Care. 2022;12(93):93. doi:10.1186/s13613-022-01067-9
10. Schmidt M, Bailey M, Sheldrake J, et al. Predicting survival after extracorporeal membrane oxygenation for severe acute respiratory failure. The Respiratory Extracorporeal Membrane Oxygenation Survival Prediction (RESP) score. Am J Respir Crit Care Med. 2014;189:1374–1382. doi:10.1164/rccm.201311-2023OC
11. Schmidt M, Burrell A, Roberts L, et al. Predicting survival after ECMO for refractory cardiogenic shock: the survival after veno-arterial-ECMO (SAVE)-score. Eur Heart J. 2015;36:2246–2256. doi:10.1093/eurheartj/ehv194
12. Lee DG, Sobieszczyk MJ, Barsoumian AE, Marcus JE. The utility of sepsis scores for predicting blood stream infections in extracorporeal membrane oxygenation. Perfusion. 2024;39:921–926. doi:10.1177/02676591231168644
13. Marcus JE, Shah A, Peek GJ, MacLaren G. Nosocomial infections in adults receiving extracorporeal membrane oxygenation: a review for infectious diseases clinicians. Clin Infectious Dis. 2024;79:412–419. doi:10.1093/cid/ciae120
14. Xu M, Xu H, Yu YW, Pan XY, Jin JJ, Li T. Prolonged thromboelastography r time and thrombocytopenia as early warning indicators of bleeding in ECMO patients who developed sepsis during support: a Retrospective Cohort Study. Infect Drug Resist. 2026;19:576614. doi:10.2147/IDR.S576614
15. Combes A, Peek GJ, Hajage D, et al. ECMO for severe ARDS: systematic review and individual patient data meta-analysis. Intensive Care Med. 2020;46:2048–2057. doi:10.1007/s00134-020-06248-3
16. Shaefi S, Brenner SK, Gupta S, et al. Extracorporeal membrane oxygenation in patients with severe respiratory failure from COVID-19. Intensive Care Med. 2021;47:208–221. doi:10.1007/s00134-020-06331-9
17. Treml B, Breitkopf R, Bukumirić Z, Bachler M, Boesch J, Rajsic S. ECMO Predictors of mortality: a 10-year referral centre experience. J Clin Med. 2022;11:1224. doi:10.3390/jcm11051224
18. Vakil D, Soto C, D’Costa Z, et al. Short-term and intermediate outcomes of cardiogenic shock and cardiac arrest patients supported by venoarterial extracorporeal membrane oxygenation. J Cardiothoracic Surg. 2021;16(290). doi:10.1186/s13019-021-01674-w
19. Ronco C, Ricci Z, Husain-Syed F. From multiple organ support therapy to extracorporeal organ support in critically ill patients. Blood Purification. 2019;48:99–105. doi:10.1159/000490694
20. Fleming GM, Askenazi DJ, Bridges BC, et al. A multicenter international survey of renal supportive therapy during ECMO: the Kidney Intervention During Extracorporeal Membrane Oxygenation (KIDMO) group. ASAIO J. 2012;58:407–414. doi:10.1097/MAT.0b013e3182579218
21. Yang X, Lin Y, Tang A, et al. Tough choices: the experience of family members of critically ill patients participating in ECMO treatment decision-making: a descriptive qualitative study. BMC Med Inf Decis Making. 2025;25:65. doi:10.1186/s12911-025-02876-1
22. Pladet LCA, Barten JMM, Vernooij LM, et al. Prognostic models for mortality risk in patients requiring ECMO. Intensive Care Med. 2023;49:131–141. doi:10.1007/s00134-022-06947-z
23. Giordano L, Francavilla A, Bottio T, et al. Predictive models in extracorporeal membrane oxygenation (ECMO): a systematic review. Syst Rev. 2023;12:44. doi:10.1186/s13643-023-02211-7
24. Pladet L, Luijken K, Fresiello L, et al. Clinical decision support for extracorporeal membrane oxygenation: will we fly by wire? Perfusion. 2023;38:68–81. doi:10.1177/02676591231163688
25. Probst L, Schalk E, Liebregts T, et al. Prognostic accuracy of SOFA, qSOFA and SIRS criteria in hematological cancer patients: a retrospective multicenter study. J Intensive Care. 2019;7:41. doi:10.1186/s40560-019-0396-y
26. Veraar C, Schwarz S, Thanner J, et al. Transient perioperative inflammation following lung transplantation and major thoracic surgery with elective extracorporeal support: a prospective observational study. Ann Translat Med. 2021;9:385. doi:10.21037/atm-20-4771
27. Li WZ, Zhou XM, Su W, et al. Pediatric sequential organ failure assessment for predicting outcomes in ECMO-bridged pediatric heart transplant recipients: experience from the largest pediatric heart transplant center in China. Front Med. 2025;12:1631616. doi:10.3389/fmed.2025.1631616
28. Chen H, Yu RG, Yin NN, Zhou JX. Combination of extracorporeal membrane oxygenation and continuous renal replacement therapy in critically ill patients: a systematic review. Critical Care. 2014;18:675. doi:10.1186/s13054-014-0675-x
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.