Back to Journals » Cancer Management and Research » Volume 11
Comparative performance of inflammation-based prognostic scores in patients operated for intrahepatic cholangiocarcinoma
Authors Lin J, Fang T, Zhu M, Xu X, Zhang J, Zheng S, Jing C, Zhang M, Liu B, Zhang B
Received 22 December 2018
Accepted for publication 10 May 2019
Published 30 October 2019 Volume 2019:11 Pages 9107—9119
DOI https://doi.org/10.2147/CMAR.S198959
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Antonella D'Anneo
Jiajia Lin,1,* Tingting Fang,1,* Mengxuan Zhu,1,* Xin Xu,1 Juan Zhang,1 Susu Zheng,1 Chuyu Jing,1 Meixia Zhang,1 Binbin Liu,1 Boheng Zhang1,2
1The Liver Cancer Institute, Zhongshan Hospital, Fudan University, Shanghai 200032, People’s Republic of China; 2Center for Evidence-Based Medicine, Fudan University, Shanghai 200032, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Boheng Zhang; Binbin Liu
The Liver Cancer Institute, Zhongshan Hospital, Fudan University, 180 Fenglin Road, Xuhui District, Shanghai 200032, People’s Republic of China
Tel +86 216 403 8038
Fax +86 216 403 8038
Email [email protected]; [email protected]
Objective: Prognostic performance of inflammation-based prognostic scores, including the Glasgow Prognostic Score (GPS), modified Glasgow Prognostic Score (mGPS), neutrophil to lymphocyte ratio (NLR), platelet to lymphocyte ratio (PLR), lymphocyte to monocyte ratio (LMR), Prognostic Index (PI) and Prognostic Nutritional Index (PNI) has been explored in patients with varied types of cancer, though little data is available in intrahepatic cholangiocarcinoma (ICC). This study sought to evaluate the impact of systemic inflammation on the overall survival (OS) of ICC patients, and to identify more optimal prognostic indices.
Patients and methods: The prognostic power of all the scores mentioned above was compared in 123 patients underwent curative surgery for ICC using Kaplan–Meier curves, COX regression models and the receiver operating characteristics (ROC) curves. The results were validated in a cohort of 95 ICC patients.
Results: Multivariate analysis identified LMR as the only independent inflammation-based predictor for OS in the training cohort (P=0.007, HR 2.082, 95% CI 1.218–3.558). More importantly, the combined score of LMR and pTNM designated the inflammation-based pathological stage (IPS) outperformed other established scores in terms of discriminatory ability, monotonicity and homogeneity in the training and validation cohorts.
Conclusion: This study reveals that preoperative LMR is an independent predictor of OS in ICC patients after hepatectomy, and the IPS can be applied as a novel prognostic indicator in these patients.
Keywords: inflammation-based prognostic score, the lymphocyte to monocyte ratio, intrahepatic cholangiocarcinoma, prognostic marker, staging system
Introduction
In the last three decades, having witnessed a marked increase in incidence1 as well as mortality rates2 globally, intrahepatic cholangiocarcinoma (ICC) remains the second most frequent primary liver cancer after hepatocellular carcinoma (HCC). Surgical resection is considered the only choice of potentially curative treatment for patients with operable ICC. Unfortunately, the surgical outcome is grim even after curative-intent resection, as the median survival period after hepatic resection is only 12.2 months.3 However, reports on the predictors of survival are relatively scarce.
Inflammation associated factors, such as hepatobiliary flukes, primary sclerosing cholangitis (PSC), chronic hepatitis B/C infection and hepatolithiasis are known to be risk factors for ICC. They cause chronic biliary inflammation and increased cellular turnover.4 Moreover, the presence of systemic inflammation negatively correlates with prognosis of cancer patients.5,6
Previous studies have elucidated that preoperative inflammation-based prognostic scores are predictive of survival in patients with malignancies7–10 including ICC.11–13 These prognostic indices include the Glasgow Prognostic Score (GPS) and modified Glasgow Prognostic Score (mGPS) based on the serum concentrations of CRP and albumin, the Prognostic Index (PI) based on CRP concentration and white blood cell count, the neutrophil to lymphocyte ratio (NLR), the platelet to lymphocyte ratio (PLR), the lymphocyte to monocyte ratio (LMR), and the Prognostic Nutritional Index (PNI) based on albumin concentration and lymphocyte count. To our knowledge, no study has assessed the prognostic value of all these scores for ICC patients. In the present study, we compared the prognostic ability of these scores as well as pathological staging systems among patients who underwent radical resection for ICC to identify more optimal prognostic predictors for these patients.
Materials and methods
Patients
Medical records of ICC patients who underwent potentially curative hepatectomy at the Liver Cancer Institute of Zhongshan Hospital (Fudan University, Shanghai, China) between 2010 and 2014 were retrospectively reviewed. Curative hepatectomy was defined as the complete removal of all macroscopic tumor nodules with clear microscopic margins and no residual tumors as indicated by CT scan at one month after surgery. Only patients pathologically confirmed to have primary intrahepatic cholangiocarcinoma were enrolled in this study. Patients who underwent preoperative therapies like transarterial chemoembolization, radiofrequency ablation, or percutaneous ethanol injection and those who showed clinical evidence of infection or other inflammatory conditions were excluded. Patients with a history of other malignancies were also excluded. Finally a total of 218 patients with ICC were included and then randomly divided into two groups, termed the training cohort and validation cohort (123 and 95 patients, respectively). The pathological stage was classified according to the AJCC 7th edition.14 Blood samples were obtained 1–3 days before surgery for measurement of white blood cell count, neutrophil, lymphocyte, platelet (Plt), monocyte count, CRP, albumin, alkaline phosphatase (ALP), total bilirubin and other laboratory data relevant to this study.
This study complied with the standards of the Declaration of Helsinki and the current ethical guidelines, and was approved by the Zhongshan Hospital Ethics Committee. All data were analyzed and displayed anonymously, thus the identity of the study participants is concealed. Written informed consent for the use of clinicopathtological data for study purpose was obtained from participants on admission.
Follow-up and postoperative treatment
According to our routine follow-up procedure, patients were followed up monthly during the first postoperative year and every 3 months thereafter. Tumor markers, such as the CA19-9 and liver ultrasonography were assessed at each visit. A computed tomography (CT) scan of the abdomen was performed every 6 months. Bone scan or magnetic resonance imaging (MRI) was used when needed. If recurrence was suspected, additional investigations, such as hepatic angiography and positron emission tomography-computed tomography (PET-CT) were performed. Patients with confirmed ICC recurrence received further treatment, if the recurrent tumor was localized, a second liver resection, radiofrequency ablation (RFA), or percutaneous ethanol injection (PEI) was suggested. If the recurrent tumor was multiple or diffused, patients were suggested to take transcatheter arterial chemoembolization (TACE) or chemotherapy; as for lymph node or bone metastasis, external radiotherapy was recommended. Overall survival (OS) was defined as the interval between the date of resection and the date of death or the last follow-up.
Statistical analysis
Continuous variables are presented as medians and ranges. Categorical variables are presented as numbers and percentages. Comparisons between groups were performed using the Student's unpaired t-test or Mann–Whitney U test for continuous or ordinal variables, while Chi square test or Fisher’s exact test was adopted for categorical variables, as appropriate. The overall survival rates were calculated using the Kaplan–Meier method, and differences in the survival rates between two groups were compared by the log-rank test. Backward stepwise multivariate Cox proportion analysis was performed to determine the influence of factors on OS which were significant in the univariate analysis.
A binary logistic regression model was fitted, and the regression coefficients derived from the model were used to create a new staging system as a composite score for LMR and pTNM, termed the inflammation-based pathological stage (IPS). To evaluate the discriminatory ability of each score, receiver operating characteristics (ROC) curves were generated, and the areas under the curve (AUC) were measured. The optimal cutoff was determined by ROC analysis. The monotonicity of each score was evaluated with the linear trend chi-square test, whereas the homogeneity of prognostic prediction across categories was measured using the likelihood ratio test as described in a previous study.15 The construction of the inflammation-based prognostic scores and their optimal cutoff values are shown in Table 1. Statistical analyses were performed using the SPSS statistical software package, version 17.0 (IBM SPSS Inc.,Chicago, IL, USA), at a significance level of P less than 0.05.
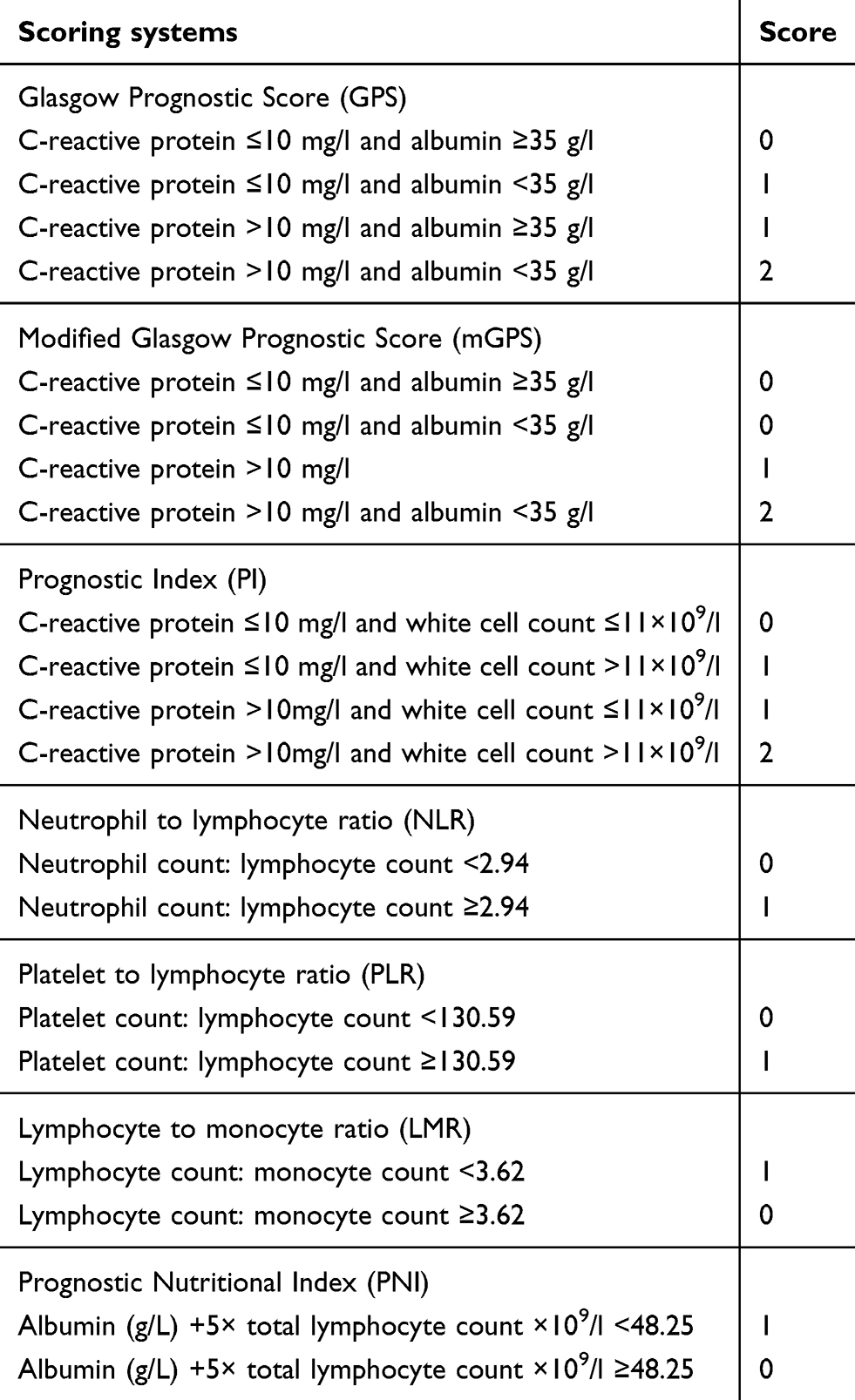 |
Table 1 Definition of inflammation-based prognostic scores |
Results
Clinicopathologic profile of patients
The detailed baseline characteristics of patients in the training and validation cohorts are summarized in Table 2. Overall, there were no significant differences between the two cohorts with respect to all clinicopathological and demographic data as well as inflammation-based prognostic scores. Among the 218 patients enrolled in the study, 124 (56.9%) were male. A total of 57 (46.3%) patients in the training set and 45 (47.4%) patients in the validation set died at the end of observation (March 2016). The median OS of the training cohort was 11.6 months (range 2.0–62.2 months) while that of the validation cohort was 16.8 months (range 1.3–62.7 months). No significant difference in OS between the two groups was noted.
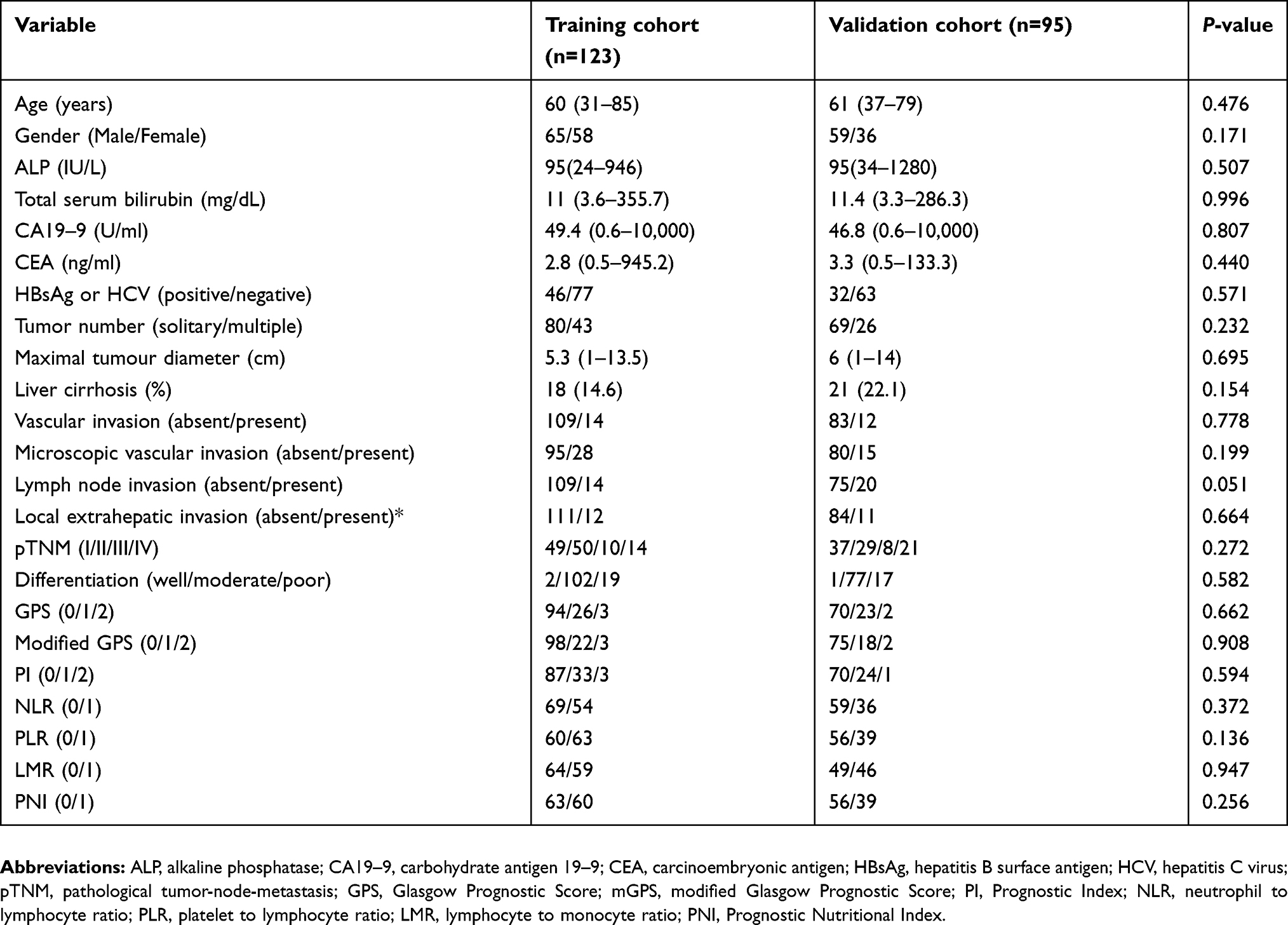 |
Table 2 Clinicopathtological characteristics of the patients in two cohorts |
Univariate and multivariate analyses of prognostic factors for OS
In the training set, univariate analysis revealed that ALP (P=0.039), CA19-9 (P=0.031), CEA (P=0.013), multiple nodules (P<0.001), maximal tumor diameter (P=0.040), vascular invasion (P=0.016), lymph node invasion (P=0.006), pTNM stage (P=0.001), the GPS (P=0.027), mGPS (P=0.025), PI (P=0.020), NLR (P=0.004), PLR (P=0.009), LMR (P=0.005) and the PNI (P=0.023) were risk factors for inferior overall survival. Multivariate analysis identified pTNM (P=0.001, HR 1.557, 95% CI 1.200–2.022) and the LMR (P=0.007, HR 2.082, 95% CI 1.218–3.558) as independent risk factors for poorer OS as shown in Table 3.
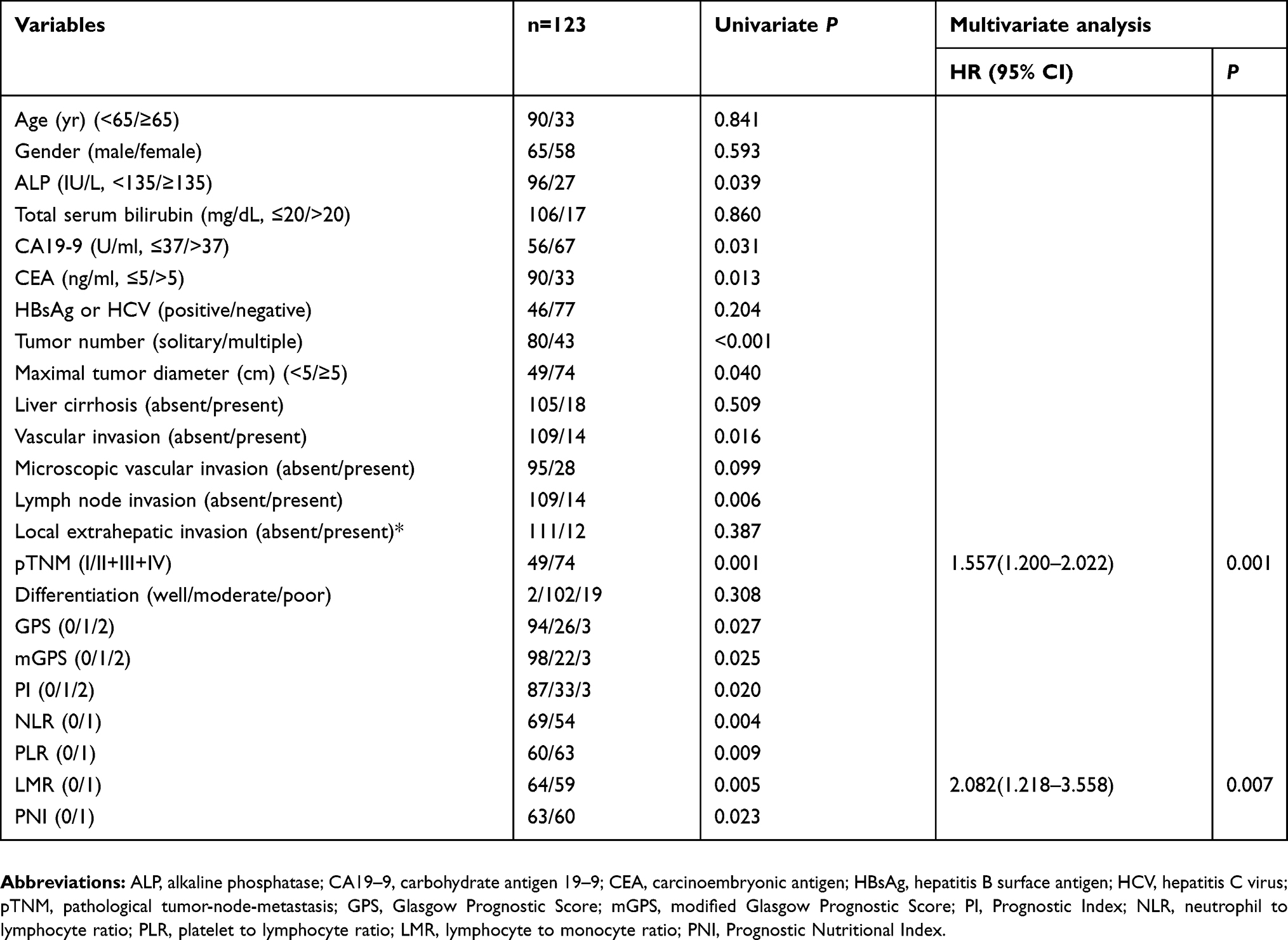 |
Table 3 Univariate and multivariate analyses of prognostic factors |
Comparative prognostic performance of scoring systems
The relationship between the prognostic scores and overall survival in the training set is shown in Figure 1. Higher levels of GPS, mGPS, NLR, PLR, LMR, PNI and pTNM were associated with reduced OS, although PI displayed marginal significance for predicting survival (P=0.055). A combination score of LMR and pTNM, designated inflammation-based pathological stages (IPS) was constructed as shown in Table 4. Patients were grouped into three categories according to their IPS stages, which resulted in significant differences in OS between all adjacent strata. Compared with patients staged IPSⅠ, those with IPS Ⅱ in the training set were 2.641 times more likely to end up with inferior OS. For patients with IPS Ⅲ, the relative hazard ratio was 4.955 (Table 4). In the validation set, only the PI, LMR, pTNM and the IPS were significantly related to overall survival rates (see Figure S1). Stepwise increase in IPS was accompanied with rise in hazard ratio in validation cohort.
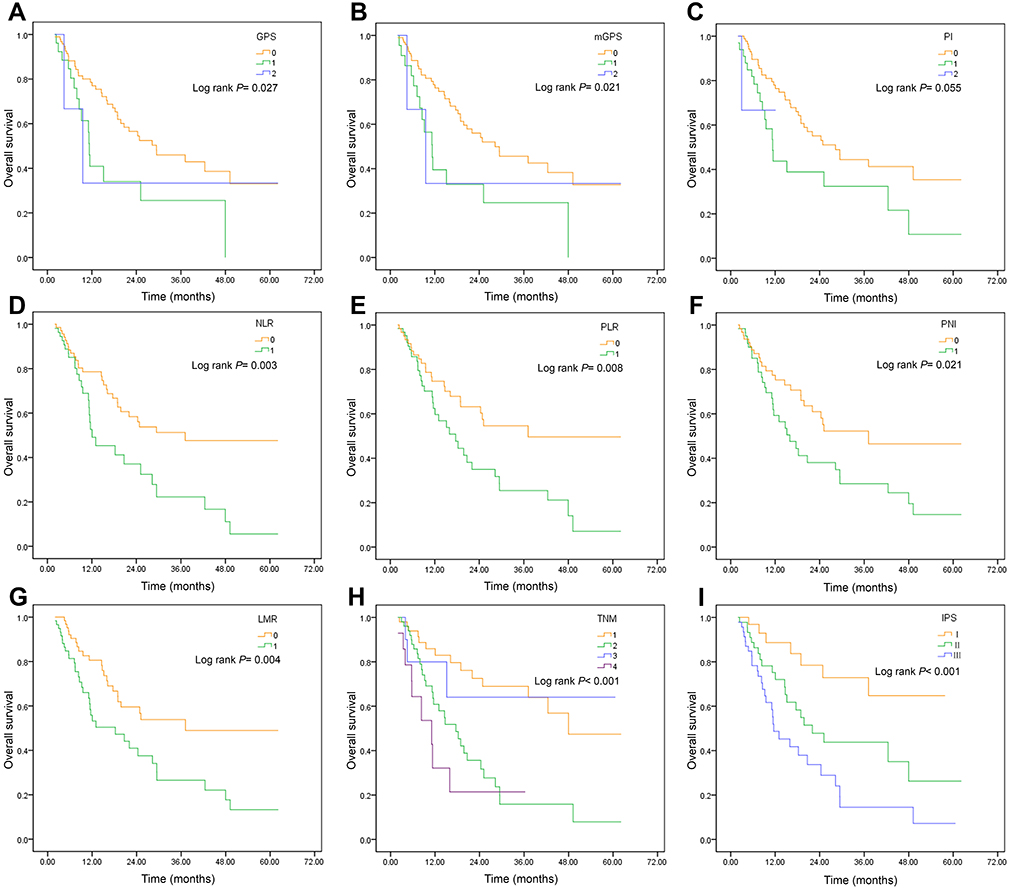 |
Figure 1 Kaplan–Meier overall survival curves for ICC patients undergoing curative hepatectomy stratified by inflammation-based prognostic scores and staging systems in the training cohort. (A) GPS; (B) mGPS; (C) PI; (D) NLR; (E) PLR; (F) PNI; (G) LMR; (H) pTNM; (I) IPS. Abbreviations: GPS, Glasgow Prognostic Score; mGPS, modified Glasgow Prognostic Score; PI, Prognostic Index; NLR, neutrophil lymphocyte ratio; PLR, platelet (Plt) lymphocyte ratio; PNI, Prognostic Nutritional Index; LMR, lymphocyte monocyte ratio; pTNM, pathological tumor-node-metastasis; IPS, inflammation-based pathological stage. |
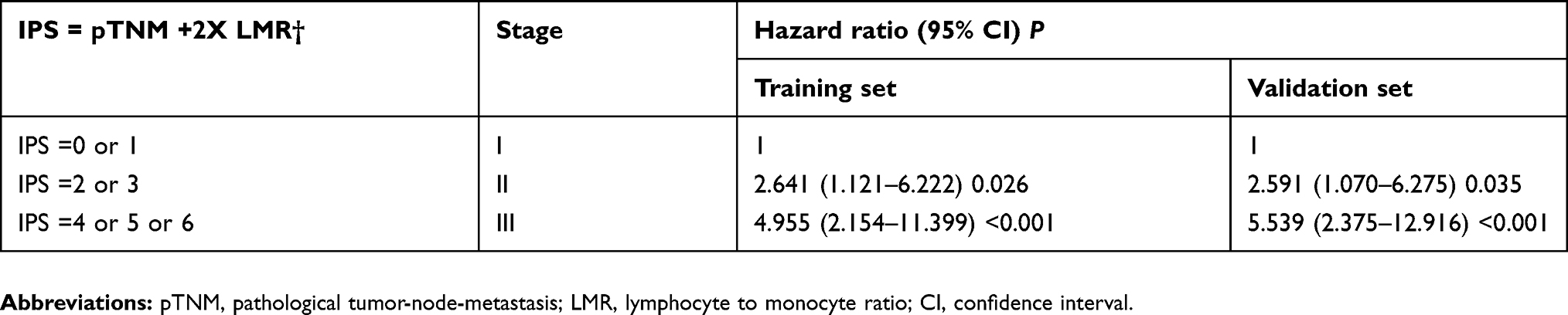 |
Table 4 Construction of the inflammation-based pathological stage (IPS) |
To assess the discriminatory capacity of each scoring system, receiver operating characteristic curves were constructed for survival status at 12-month, 18-month and 24-month follow-up. The area under the ROC curve (AUC) was calculated and compared, as shown in Table 5. The IPS had the highest AUC value at 12-months (0.699), 18-months (0.676) and 24-months (0.669) follow-up in comparison with other inflammation-based prognostic indices and the pTNM in the training set. This conclusion was furthere verified in the validation cohort. The IPS had an AUC value of 0.737, 0.713, 0.717 at 12-month, 18-month and 24-month follow-up, respectively, as shown in Table S1. The IPS with the highest χ2 according to the linear trend test and the LR test was considered to have the best monotonicity and homogeneity, although pTNM stage appeared to have higher homogeneity in the training group as shown in Table 6 and Table S2.
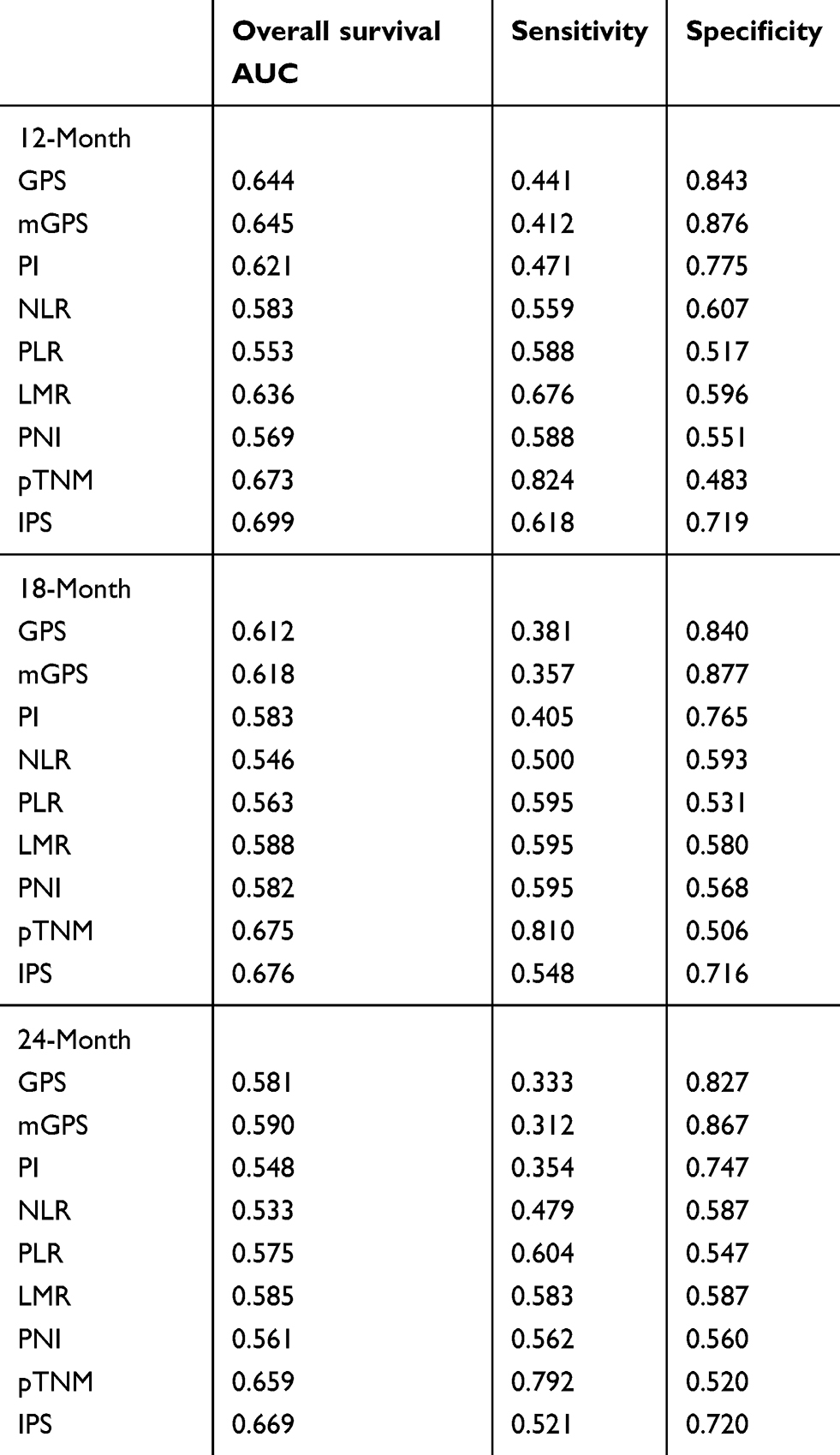 |
Table 5 Comparison of the AUC between inflammation-based prognostic scores in the training cohort |
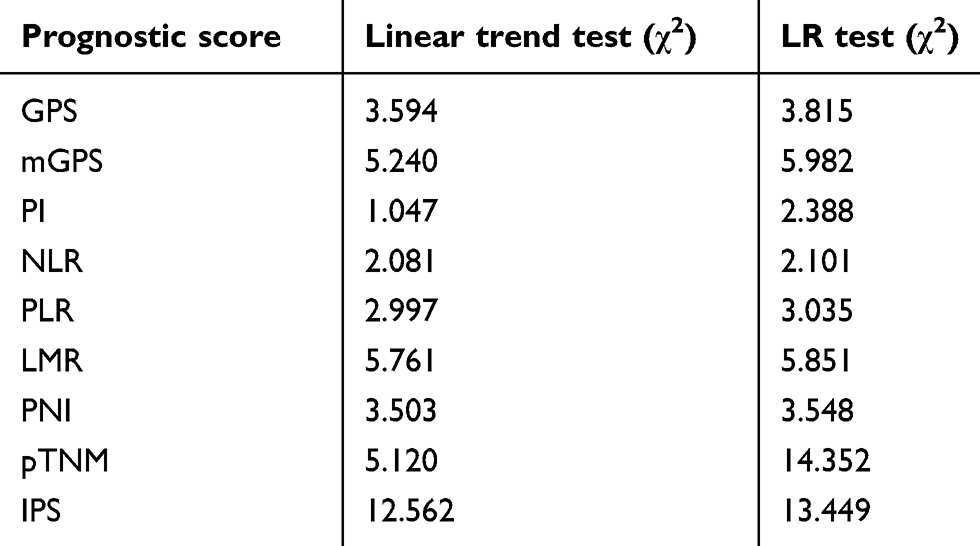 |
Table 6 Evaluation of monotonicity and homogeneity of scoring systems in the training cohort |
Relationship between clinicopathological factors and the IPS
Several clinicopathological features were compared among the three groups with different level of IPS in the training cohort (Table 7). Those with the same elements that constituted pTNM or LMR including tumor number, maximal tumor diameter, lymph node invasion, vascular invasion, local extrahepatic invasion, PI, NLR, PLR and PNI were not compared. It turned out that patients with higher ALP, CEA, microscopic vascular invasion, elevated GPS and modified GPS were more likely to have advanced stages of IPS.
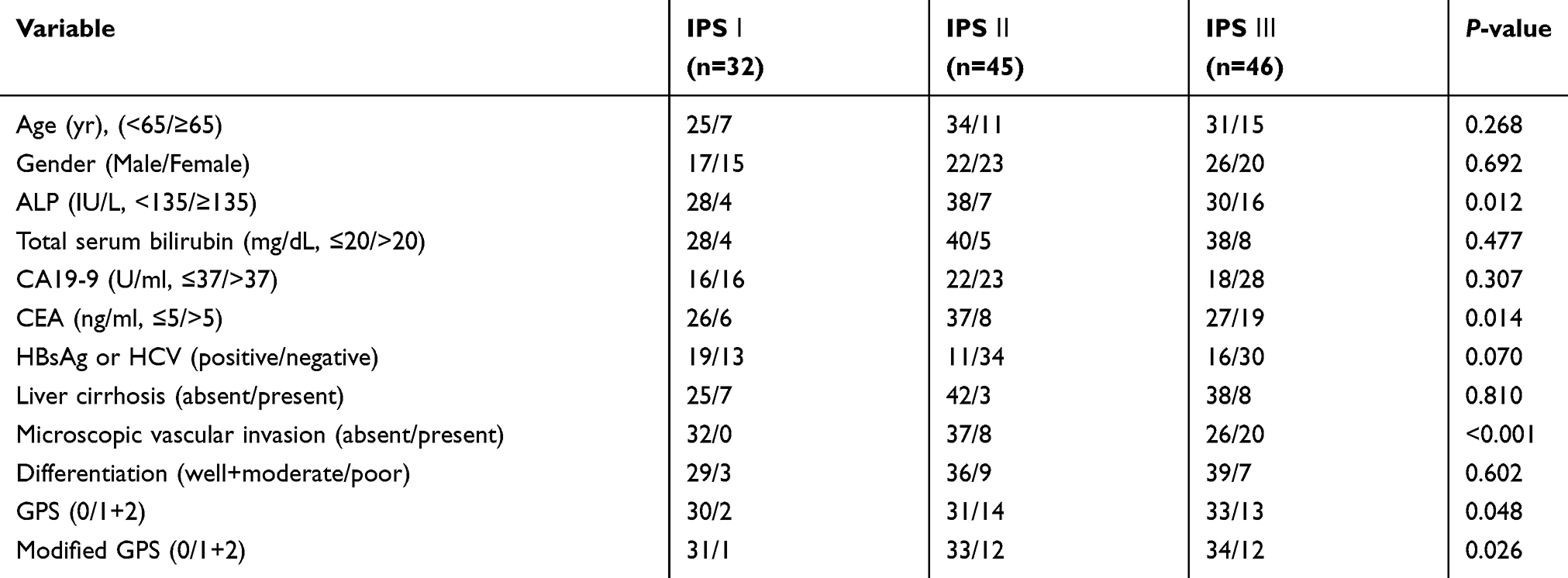 |
Table 7 Clinicopathtological characteristics of the patients grouped according to IPS in the training cohort |
Similar conclusions were drawn in the validation cohort; in which the aforementioned factors were significantly associated with advanced IPS level in this set (Table S3).
Discussion
In the present study, we have demonstrated that inflammation-based prognostic scores such as GPS, mGPS, PI, NLR, PLR, LMR and PNI are associated with dismal prognosis in ICC patients underwent radical surgery. Besides, we report for the first time that LMR is an independent prognostic predictor of OS in these patients. Based on this finding, we generated a novel inflammation-based prognostic score named the IPS, which proved to be more effective in stratifying the prognosis of patients with operable ICC.
Several lines of evidence indicate that inflammation acts much like “fertilizer” for the growth of malignancies. Inflammation is observed after activation of almost all common oncogenes including Myc and Ras16,17 and “is demonstrably capable of fostering the development of incipient neoplasias into full-blown cancers”.18 Both local and systemic inflammatory responses are evident in the progression of human cancer.19,20 For intrahepatic cholangiocarcinoma, a previous study from our institution have validated that ICC cells are likely to recruit more neutrophils to the tumor foci through overexpressed CXCL5.21 Lin et al from Sun Yat-sen University Cancer Center demonstrated a significant association between high levels of serum CRP and adverse cancer-specific survival (P=0.001) and recurrence-free survival (P<0.001)22 in ICC. To assess the level of systemic inflammation in an effective way, several inflammation-based prognostic scores such as GPS,23 mGPS,24 PI,25 NLR,26–28 PLR,29–31 PNI32-34 and LMR have been proposed in the recent decade. The prognostic power of these indices has been demonstrated in various types of malignancies including liver and bile duct neoplasm.7,9
However, few studies have looked into the prognostic ability of inflammation-based scores in patients with intrahepatic cholangiocarcinoma. Gomez et al reported, for the first time, that ICC patients with an elevated preoperative NLR (>5) had significantly shorter overall survival after hepatic resection.11 Similarly, Chen et al found that high NLR (≥2.49) showed notable correlation with early recurrence and poor overall survival in ICC patients.12 The same research group confirmed that high level of PLR (≥123) might be a significant prognostic factor in ICC patients; PLR values greater than 123 reflected strong correlation with early recurrence and worse OS.13 In the present study, the prognostic significance of elevated PLR was only observed in the training set. However, PLR did not exert any significant effect on OS in the validation cohort, possibly due to limited cohort size.
In our comparative analysis of prognostic scores, the prognostic power of LMR, which had been tested by previous investigators, was also validated. Stotz et al demonstrated that elevated preoperative LMR was an independent predictor of increased TTR and OS in patients with stage II and III colon cancer.35 Lin and colleagues illustrated that the LMR was a significant prognostic factor for OS and DFS in patients receiving curative surgery for hepatocellular carcinoma.36 Consistent with their conclusion, Wu et al stated that a high LMR may predict favorable OS and RFS in surgically treated HCC patients.37 In our study, we demonstrated for the first time that patients with increased pretreatment LMR (≥3.62) exhibited longer overall survival after hepatectomy for ICC. To the best of our knowledge, the prognostic performance of all these established inflammation-based prognostic scores has never been studied in a comparative fashion in intrahepatic cholangiocarcinoma. Our study not only confirmed the prognostic value of the GPS, mGPS, NLR, PLR, PNI, LMR and the PI but also highlighted the prominent prognostic value of LMR for operable ICC patients.
Components of these inflammation-based prognostic scores included in the present study comprise majority of the immune cells. Both innate and acquired immune cells play critical roles in the initiation, invasive growth and metastasis of cancer. Innate immune cells including macrophages, neutrophils, and mast cells are largely responsible for inflammatory reactions.38 In tumor sites, macrophages (and monocytes) create an inflammatory environment that is mutagenic and growth-promoting during tumor initiation. As tumors progress, they promote angiogenesis, enhance tumor cell migration, invasion and suppression of anti-tumor immunity.39 Macrophages at the tumor periphery can also foster local invasion by supplying matrix-degrading enzymes such as metalloproteinases and cysteine cathepsin proteases.18
The adaptive immune cells (B and T cells), however, can be tumor-suppressing. They carry out cancer immunosurveillance, recognize transformed cells and destroy them, resulting in a return to normal physiological tissue.40 A major subset of tumors shows evidence of a T cell–infiltrated phenotype. The presence of activated CD8+ T cells both within the tumor and in the peritumor microenvironment has been reported to indicate positive prognosis.41,42 Therefore, it is conceivable that higher LMR, as a compound outcome of increased peripheral blood lymphocytes and diminished monocytes, indicates favorable prognosis.
Clinicopathological predictors have proved to be suboptimal in identifying high-risk patients. But recent evidence underscored the discriminatory power of combined prognostic index of the clinicopathological predictors like staging systems and the inflammation based indices. Pinato et al proposed a new prognostic score based on a combination of mGPS and CLIP scores. They found that the predictive accuracy of the combined score (c score 0.7, 95% CI 0.6–0.8) appeared to be superior to that of the CLIP score alone (c score 0.6, 95% CI 0.5–0.7).43 Kinoshita and co-workers also elucidated that when GPS was combined with the CLIP system to form a new prognostic system, named inflammation-based CLIP, better prognostic accuracy was achieved compared to GPS or CLIP alone.44 Unlike hepatocellular carcinoma, there are barely established staging systems for ICC. The most commonly used staging system for ICC is the TNM classification system. In this study, we verified the prognostic power of the inflammation-based pathological stage (IPS). It seems that the IPS is superior to the pTNM staging system and the inflammation-based indices alone in terms of discriminatory power (large differences in prognosis between different stages), homogeneity (small differences in prognosis between patients in the same stage) and monotonicity (mortality of patients increased significantly with the increase of staging). Kaplan–Meier curve revealed that patients with advanced IPS stages, even in the same pTNM stage of ICC when undergoing operation, got inferior overall survival rates. The stratification of prognosis according to the IPS stages was definitive, which totally outperformed the traditional pTNM staging system. In addition, IPS scores were strongly linked to tumor markers including ALP, CEA, and aggressive pathological characteristics like microscopic vascular invasion, all of which reflect poor prognosis. This indicates that more intense follow-up or prophylactic postoperative treatment such as chemotherapy, radiotherapy and transcatheter arterial chemoembolization (TACE) is needed for patients with advanced IPS stages.
In summary, this study reveals that the GPS, mGPS, NLR, PLR, PNI, LMR and the PI possess high prognostic value for OS in operable ICC. LMR was identified as the only independent predictor of OS among those inflammation-based scores. Besides, a novel and powerful inflammation-based prognostic index termed the IPS was established. Given the retrospective, small size and single institution-based nature of this study, certain limitations regarding this prognostic analysis should be acknowledged. Therefore, the findings of this study should be independently validated through prospective multicentric large cohort studies in the future.
Acknowledgments
This work is supported by the National Natural Science Foundation of China (Grant No. 81173391), Shanghai Municipal Commission of Health and Family Planning (ZY3-CCCX-3-2004) and Zhongshan Hospital Science Foundation (2018ZSQN35). The funding sources did not have any role in study design, data collection and analysis, decision to publish.
Disclosure
Dr Boheng Zhang reports grants from National Natural Science Foundation of China, Shanghai Municipal Commission of Health and Family Planning, during the conduct of the study. Dr Jiajia Lin reports grant from Zhongshan Hospital Science Foundation, during the conduct of the study. The authors declare no other conflicts of interest in this work.
References
1. Shaib YH, Davila JA, McGlynn K, El-Serag HB. Rising incidence of intrahepatic cholangiocarcinoma in the United States: a true increase? J Hepatol. 2004;40:472–477. doi:10.1016/j.jhep.2003.11.030
2. Patel T. Worldwide trends in mortality from biliary tract malignancies. BMC Cancer. 2002;2:10. doi:10.1186/1471-2407-2-10
3. Zou S, Li J, Zhou H, et al. Mutational landscape of intrahepatic cholangiocarcinoma. Nat Commun. 2014;5:5696. doi:10.1038/ncomms6696
4. Bridgewater J, Galle PR, Khan SA, et al. Guidelines for the diagnosis and management of intrahepatic cholangiocarcinoma. J Hepatol. 2014;60:1268–1289. doi:10.1016/j.jhep.2014.01.021
5. Hashimoto K, Ikeda Y, Korenaga D, et al. The impact of preoperative serum C-reactive protein on the prognosis of patients with hepatocellular carcinoma. Cancer-Am Cancer Soc. 2005;103:1856–1864.
6. McMillan DC, Canna K, McArdle CS. Systemic inflammatory response predicts survival following curative resection of colorectal cancer. Br J Surg. 2003;90:215–219. doi:10.1002/bjs.4038
7. Kinoshita A, Onoda H, Imai N, et al. Comparison of the prognostic value of inflammation-based prognostic scores in patients with hepatocellular carcinoma. Br J Cancer. 2012;107:988–993. doi:10.1038/bjc.2012.354
8. Pinato DJ, Shiner RJ, Seckl MJ, Stebbing J, Sharma R, Mauri FA. Prognostic performance of inflammation-based prognostic indices in primary operable non-small cell lung cancer. Brit J Cancer. 2014;110:1930–1935. doi:10.1038/bjc.2014.145
9. Okuno M, Ebata T, Yokoyama Y, et al. Evaluation of inflammation-based prognostic scores in patients undergoing hepatobiliary resection for perihilar cholangiocarcinoma. J Gastroenterol. 2016;51:153–161. doi:10.1007/s00535-015-1103-y
10. Wang D, Luo H, Qiu M, et al. Comparison of the prognostic values of various inflammation based factors in patients with pancreatic cancer. Med Oncol. 2012;29:3092–3100. doi:10.1007/s12032-012-0226-8
11. Gomez D, Morris-Stiff G, Toogood GJ, Lodge JPA, Prasad KR. Impact of systemic inflammation on outcome following resection for intrahepatic cholangiocarcinoma. J Surg Oncol. 2008;97:513–518. doi:10.1002/jso.21001
12. Chen Q, Yang L, Li X, et al. The elevated preoperative neutrophil-to-lymphocyte ratio predicts poor prognosis in intrahepatic cholangiocarcinoma patients undergoing hepatectomy. Tumor Biol. 2015;36:5283–5289. doi:10.1007/s13277-015-3188-6
13. Chen Q, Dai Z, Yin D, et al. Negative impact of preoperative platelet-lymphocyte ratio on outcome after hepatic resection for intrahepatic cholangiocarcinoma. Medicine. 2015;94:e574. doi:10.1097/MD.0000000000000874
14. Edge SB BD CCFA. AJCC Cancer Staging Manual.
15. Ueno S. Discrimination value of the new western prognostic system (CLIP score) for hepatocellular carcinoma in 662 Japanese patients. HEPATOLOGY. 2001;34:529–534. doi:10.1053/jhep.2001.27219
16. Soucek L, Lawlor ER, Soto D, Shchors K, Swigart LB, Evan GI. Mast cells are required for angiogenesis and macroscopic expansion of Myc-induced pancreatic islet tumors. Nat Med. 2007;13:1211–1218. doi:10.1038/nm1649
17. Sparmann A, Bar-Sagi D. Ras-induced interleukin-8 expression plays a critical role in tumor growth and angiogenesis. Cancer Cell. 2004;6:447–458. doi:10.1016/j.ccr.2004.09.028
18. Hanahan D, Weinberg RA. Hallmarks of cancer: the next generation. Cell. 2011;144:646–674. doi:10.1016/j.cell.2011.02.013
19. Roxburgh CS, Salmond JM, Horgan PG, Oien KA, McMillan DC. Comparison of the prognostic value of inflammation-based pathologic and biochemical criteria in patients undergoing potentially curative resection for colorectal cancer. Ann Surg. 2009;249:788–793. doi:10.1097/SLA.0b013e3181a3e738
20. Canna K, McArdle PA, McMillan DC, et al. The relationship between tumour T-lymphocyte infiltration, the systemic inflammatory response and survival in patients undergoing curative resection for colorectal cancer. Br J Cancer. 2005;92:651–654. doi:10.1038/sj.bjc.6602419
21. Zhou SL, Dai Z, Zhou ZJ, et al. CXCL5 contributes to tumor metastasis and recurrence of intrahepatic cholangiocarcinoma by recruiting infiltrative intratumoral neutrophils. Carcinogenesis. 2014;35:597–605. doi:10.1093/carcin/bgt397
22. Lin ZY, Liang ZX, Zhuang PL, et al. Intrahepatic cholangiocarcinoma prognostic determination using pre-operative serum C-reactive protein levels. BMC Cancer. 2016;16:792. doi:10.1186/s12885-016-2827-7
23. Forrest LM, McMillan DC, McArdle CS, Angerson WJ, Dunlop DJ. Evaluation of cumulative prognostic scores based on the systemic inflammatory response in patients with inoperable non-small-cell lung cancer. Br J Cancer. 2003;89:1028–1030. doi:10.1038/sj.bjc.6601242
24. Proctor MJ, Morrison DS, Talwar D, et al. An inflammation-based prognostic score (mGPS) predicts cancer survival independent of tumour site: a Glasgow Inflammation Outcome Study. Br J Cancer. 2011;104:726–734. doi:10.1038/sj.bjc.6606087
25. Proctor MJ, Morrison DS, Talwar D, et al. A comparison of inflammation-based prognostic scores in patients with cancer. A Glasgow Inflammation Outcome Study. Eur J Cancer. 2011;47:2633–2641. doi:10.1016/j.ejca.2011.03.028
26. Mano Y, Shirabe K, Yamashita Y, et al. Preoperative neutrophil-to-lymphocyte ratio is a predictor of survival after hepatectomy for hepatocellular carcinoma. Ann Surg. 2013;258:301–305. doi:10.1097/SLA.0b013e318297ad6b
27. Jung J, Park SY, Park S, Park J. Prognostic value of the neutrophil-to-lymphocyte ratio for overall and disease-free survival in patients with surgically treated esophageal squamous cell carcinoma. Tumor Biol. 2015;37:7149–7154. doi:10.1007/s13277-015-4596-3
28. Shimada H, Takiguchi N, Kainuma O, et al. High preoperative neutrophil-lymphocyte ratio predicts poor survival in patients with gastric cancer. Gastric Cancer. 2010;13:170–176. doi:10.1007/s10120-010-0554-3
29. Koh C, Bhoo-Pathy N, Ng K, et al. Utility of pre-treatment neutrophil–lymphocyte ratio and platelet–lymphocyte ratio as prognostic factors in breast cancer. Brit J Cancer. 2015;113:150–158. doi:10.1038/bjc.2015.183
30. Zhang Y, Jiang C, Li J, Sun J, Qu X. Prognostic significance of preoperative neutrophil/lymphocyte ratio and platelet/lymphocyte ratio in patients with gallbladder carcinoma. Clin Transl Oncol. 2015;17:810–818. doi:10.1007/s12094-015-1310-2
31. Jiang N, Deng J, Liu Y, Ke B, Liu H, Liang H. The role of preoperative neutrophil–lymphocyte and platelet–lymphocyte ratio in patients after radical resection for gastric cancer. Biomarkers. 2014;19:444–451. doi:10.3109/1354750X.2014.926567
32. Chan AWH, Chan SL, Wong GLH, et al. Prognostic Nutritional Index (PNI) predicts tumor recurrence of very early/early stage hepatocellular carcinoma after surgical resection. Ann Surg Oncol. 2015;22:4138–4148. doi:10.1245/s10434-015-4516-1
33. Pinato DJ, North BV, Sharma R. A novel, externally validated inflammation-based prognostic algorithm in hepatocellular carcinoma: the prognostic nutritional index (PNI). Br J Cancer. 2012;106:1439–1445. doi:10.1038/bjc.2012.92
34. Okamura Y, Ashida R, Ito T, Sugiura T, Mori K, Uesaka K. Preoperative neutrophil to lymphocyte ratio and prognostic nutritional index predict overall survival after hepatectomy for hepatocellular carcinoma. World J Surg. 2015;39:1501–1509. doi:10.1007/s00268-015-2982-z
35. Stotz M, Pichler M, Absenger G, et al. The preoperative lymphocyte to monocyte ratio predicts clinical outcome in patients with stage III colon cancer. Brit J Cancer. 2013;110:435–440. doi:10.1038/bjc.2013.785
36. Lin Z. Lymphocyte-to-monocyte ratio predicts survival of patients with hepatocellular carcinoma after curative resection. World J Gastroentero. 2015;21:10898. doi:10.3748/wjg.v21.i38.10898
37. Wu S, Lin Y, Ye H, Li F, Xiong X, Cheng N. Lymphocyte to monocyte ratio and prognostic nutritional index predict survival outcomes of hepatitis B virus-associated hepatocellular carcinoma patients after curative hepatectomy. J Surg Oncol. 2016;114:202–210. doi:10.1002/jso.24297
38. Szabo G, Mandrekar P, Dolganiuc A. Innate immune response and hepatic inflammation. Semin Liver Dis. 2007;27:339–350. doi:10.1055/s-2007-991511
39. Qian BZ, Pollard JW. Macrophage diversity enhances tumor progression and metastasis. Cell. 2010;141:39–51. doi:10.1016/j.cell.2010.03.014
40. Dunn GP, Old L, Schreiber RD. The immunobiology of cancer immunosurveillance and immunoediting. Annu Rev Immunol. 2004;21:137–148.
41. Hamanishi J, Mandai M, Iwasaki M, et al. Programmed cell death 1 ligand 1 and tumor-infiltrating CD8+ T lymphocytes are prognostic factors of human ovarian cancer. Proc Natl Acad Sci U S A. 2007;104:3360–3365. doi:10.1073/pnas.0611533104
42. Galon J. Type, density, and location of immune cells within human colorectal tumors predict clinical outcome. SCIENCE. 2006;313:1960–1964. doi:10.1126/science.1129139
43. Pinato DJ, Stebbing J, Ishizuka M, et al. A novel and validated prognostic index in hepatocellular carcinoma: the inflammation based index (IBI). J Hepatol. 2012;57:1013–1020. doi:10.1016/j.jhep.2012.06.022
44. Kinoshita A, Onoda H, Imai N, et al. The glasgow prognostic score, an inflammation based prognostic score, predicts survival in patients with hepatocellular carcinoma. BMC Cancer. 2013;13:52. doi:10.1186/1471-2407-13-52
Supplemantary materials
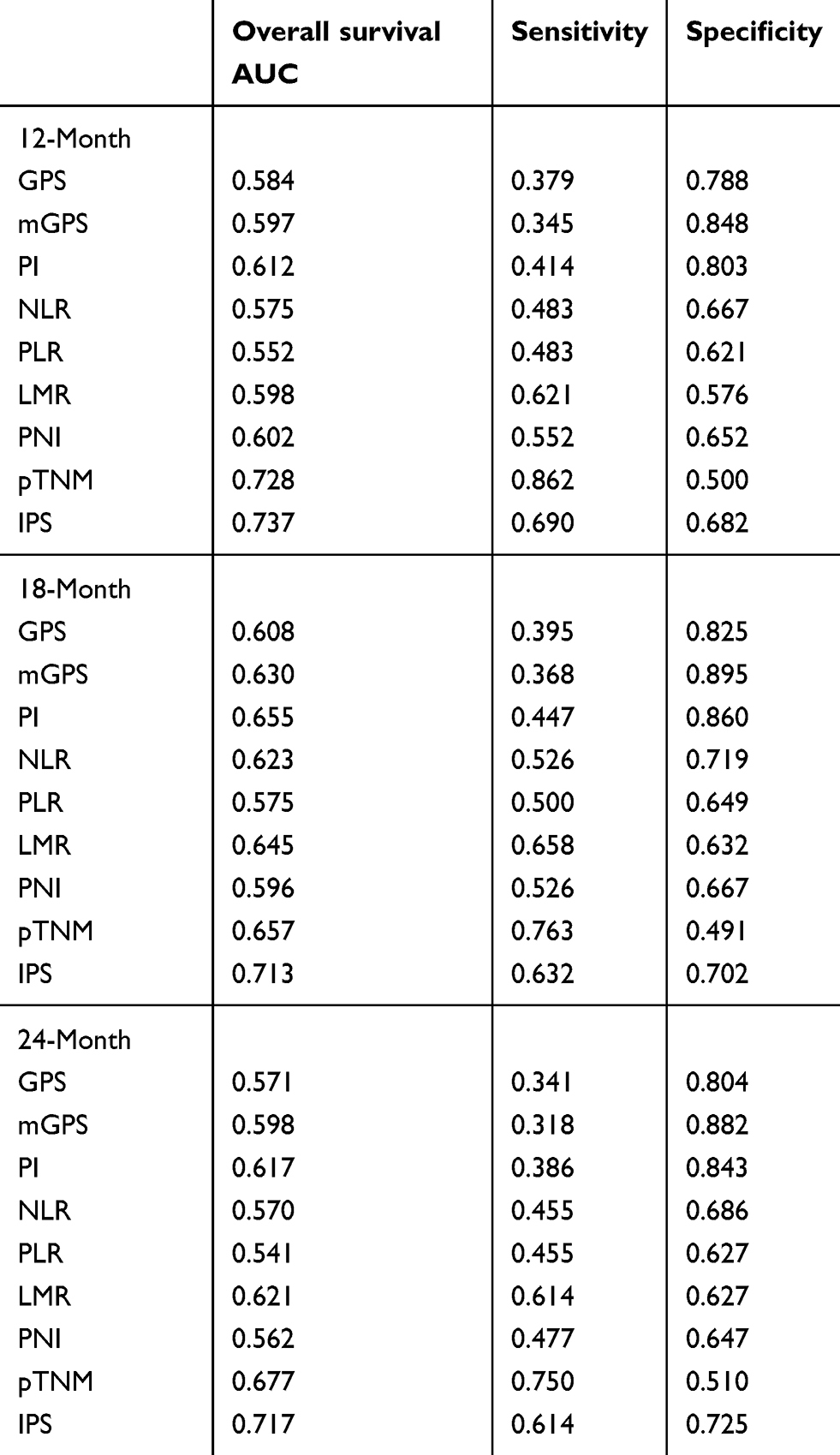 |
Table S1 Comparison of the AUC between between inflammation-based prognostic scores in the validation cohort |
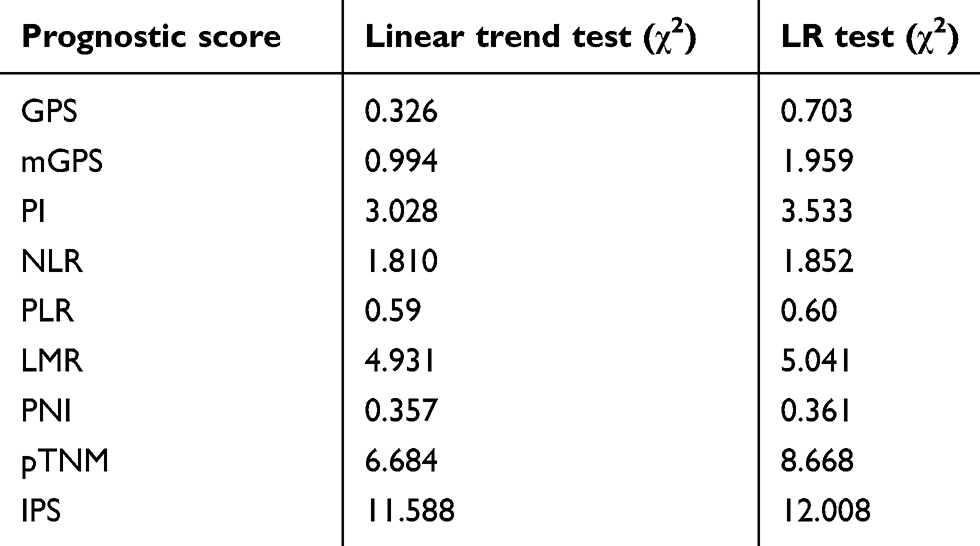 |
Table S2 Evaluation of monotonicity and homogeneity of scoring systems in the validation cohort |
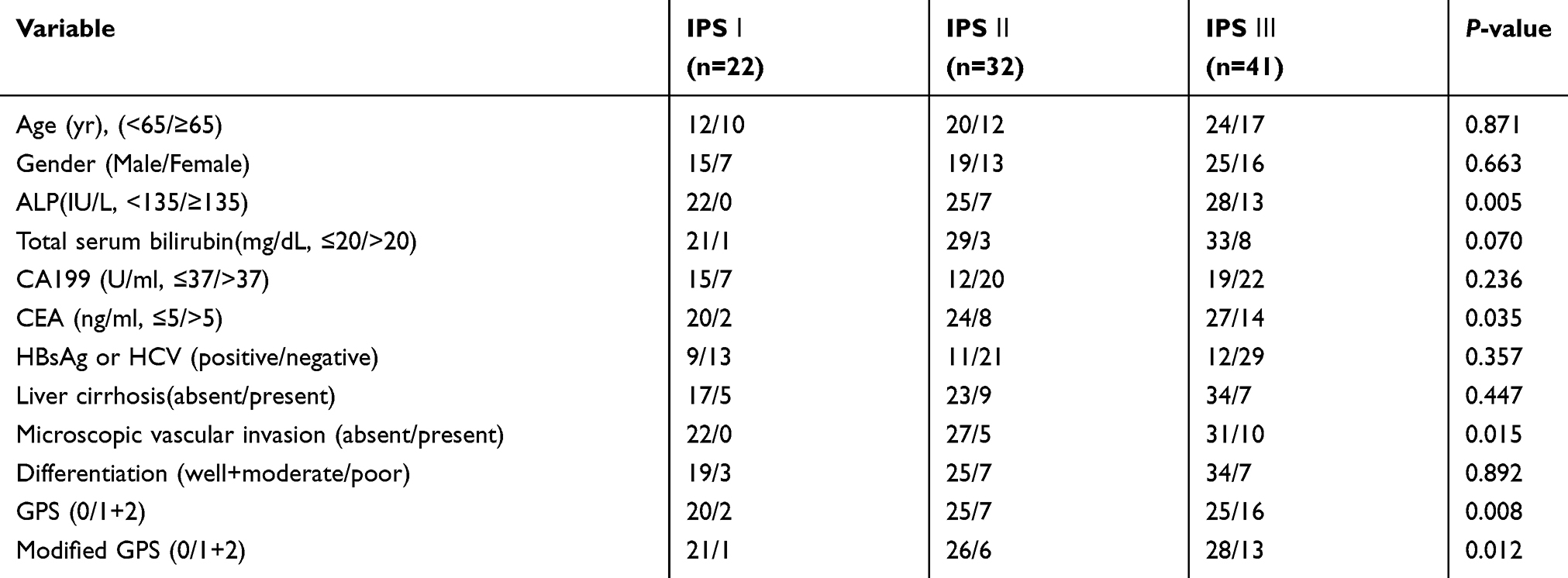 |
Table S3 Clinicopathtological characteristics of the patients grouped according to the IPS in the validation cohort |
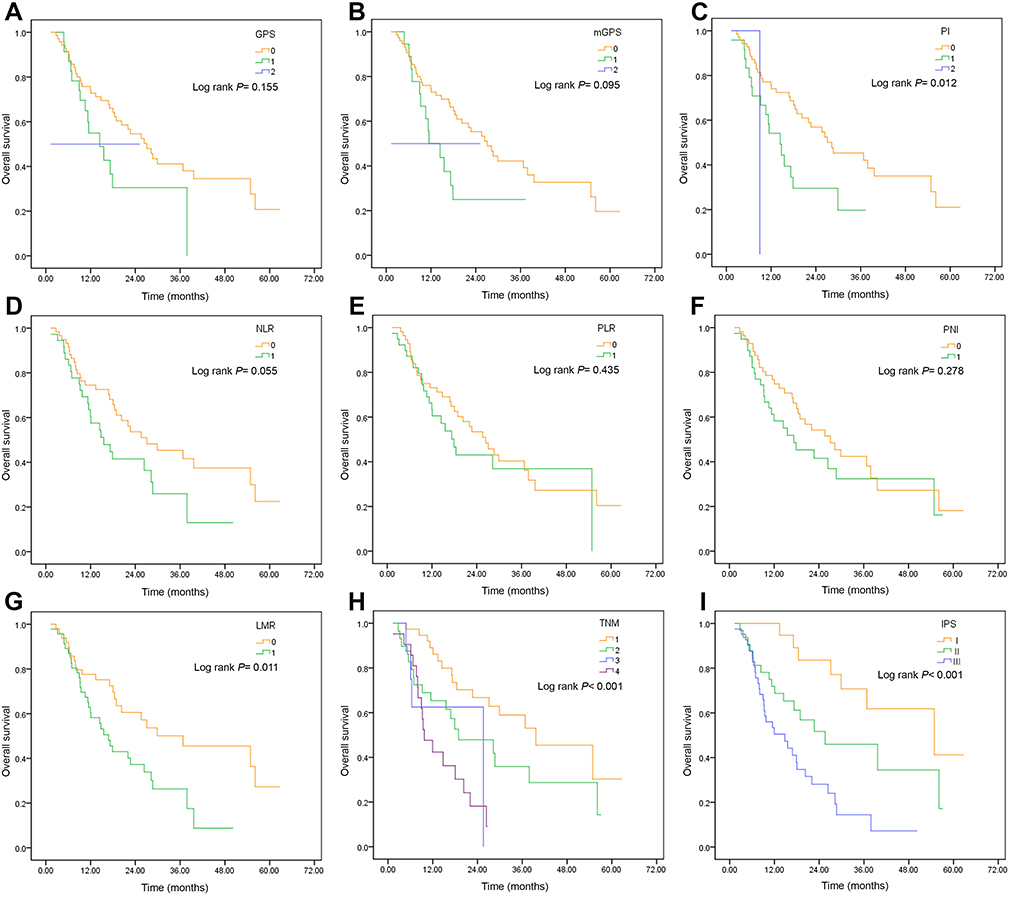 |
Figure S1 Kaplan–Meier overall survival curves for ICC patients undergoing curative hepatectomy stratified by inflammation-based prognostic scores and staging systems in the validation cohort. (A) GPS; (B) mGPS; (C) PI; (D) NLR; (E) PLR; (F) PNI; (G) LMR; (H) pTNM; (I) IPS. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.