Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 18
Comparative Evaluation of Responsiveness of Insulin Counter-Regulatory Hormones and Insulin Resistance to Hypoglycemia in Newly Diagnosed Type 1 Diabetes Mellitus Man
Authors Zhou Y, Zhou J, Ma J ![]() , Yan R, Yuan L, Huang R, Shen Y, Ding B
, Yan R, Yuan L, Huang R, Shen Y, Ding B
Received 22 July 2025
Accepted for publication 10 November 2025
Published 21 November 2025 Volume 2025:18 Pages 4309—4317
DOI https://doi.org/10.2147/DMSO.S554306
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Ernesto Maddaloni
Yunting Zhou,1,* Junming Zhou,2,* Jianhua Ma,1,* Rengna Yan,1 Lu Yuan,1 Rong Huang,1 Yun Shen,1 Bo Ding1
1Department of Endocrinology, Nanjing First Hospital, Nanjing Medical University, Nanjing, People’s Republic of China; 2Department of Healthcare, Jinling Hospital, Medical School of Nanjing University, Nanjing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yun Shen, Department of Endocrinology, Nanjing First Hospital, Nanjing Medical University, Nanjing, Jiangsu, People’s Republic of China, Email [email protected] Bo Ding, Department of Endocrinology and Metabolism, Nanjing First Hospital, Nanjing Medical University, Nanjing, 210012, People’s Republic of China, Fax +862552887091, Email [email protected]
Aim: The mechanisms governing dynamic regulation of counterregulatory hormones in type 1 diabetes (T1DM) remain incompletely understood. To eliminate potential confounding effects of female sex hormones and menstrual cycle variations on insulin sensitivity and counter-regulatory hormone secretion, this study investigated the correlation between counter-regulatory hormone levels and insulin resistance in male patients with T1DM.
Research Design and Methods: From March 2022 to December 2022, 34 male patients with newly diagnosed T1DM and 8 male normal people without DM were included. Counter-regulatory hormone levels and clinical characteristics were collected. All the included T1DM subjects were treated with intensive insulin therapy by insulin pump for 1 week to achieve glycemic control, followed by using the hyperinsulinemic-hypoglycemic clamp to determine the steady-state glucose infusion rate, an indicator of insulin sensitivity. The chemiluminescent immunometric assay was also used to measure circulating counter-regulatory hormones, such as glucagon (GCG), insulin-like growth factor-1 (IGF-1), adrenocorticotropic hormone (ACTH), growth hormone (GH), and cortisol (Cor) at 0min and 30min during hyperinsulinemic-hypoglycemic test. Correlation analysis was conducted to investigate the relationship between insulin-stimulated glucose disposal rates (M value) and counter-regulatory hormone levels.
Results: The T1DM group exhibited lower fasting C-peptide levels than the normal group (p< 0.050). During the hypoglycemic clamp test and in the hypoglycemic state, the T1DM group showed a greater magnitude of increase in Cor and GH levels than the control group, whereas GCG displayed an opposite trend. Moreover, the M value was negatively correlated with ACTH, COR, and GH, and positively correlated with IGF-1 in male patients with newly diagnosed T1DM.
Conclusion: The current study demonstrates that inhibiting the upregulation of insulin counter-regulatory hormone levels contributes to impaired insulin regurgitator response during hypoglycaemia in newly man diagnosed T1DM patients. This study provides insight into the glycaemic control benefits of insulin counter-regulatory hormones, and insulin counter-regulatory hormone levels may serve as a potential biomarker for assessing the blood glucose control risk of T1DM.
Trial Registration: This trial is registered at ClinicalTrials.gov (CT.gov identifier: NCT05290207).
Keywords: counter-regulatory hormone levels, insulin resistance, hyperinsulinemic-hypoglycemic clamp, type 1 diabetes mellitus, insulin-stimulated glucose disposal rates
A Letter to the Editor has been published for this article.
Introduction
Diabetes mellitus is a metabolic disease characterized by insulin resistance and deficiency, which is one of the most severe public health challenges in the world.1 In China, the nationally representative survey reports that the estimated overall prevalence of diabetes has increased to 10.6%.2 Studies have demonstrated that type 1 diabetes mellitus (T1DM) accounts for about 5–10% of all DM patients and even represents 90% of all DM in childhood.3
T1DM is characterized by absolute insulin deficiency and dysregulated glucagon secretion.4 Since glycemic control is often accompanied by an increased risk of hypoglycemia, insulin alone is still a challenge for clinicians, although insulin replacement is the primary treatment for T1DM.5–7 Hypoglycemia is widely regarded as the primary limiting factor in optimizing glycemic targets.8 Concerns about hypoglycemia also bring about the failure to achieve glycemic control in T1DM patients.5,6 Counter-regulatory hormone responses to hypoglycemia, such as adrenocorticotropic hormone (ACTH), growth hormone (GH), and cortisol (Cor), have attracted many studies to explore its relationship with blood glucose regulation in the latest years.9–11 Numerous studies have found hypoglycaemic counter-regulation at normal blood glucose concentrations in well-controlled T2DM.12,13 The findings indicate that exaggerated ACTH, norepinephrine, and glucagon (GCG) responses to hypoglycemia compared to lean counterparts.14 However, the dynamic regulation of counter-regulatory hormones in T1DM is still unclear.
In pathophysiology, decreased β-cell function (BCF) and insulin resistance (IR) are the two main factors involved in DM. The interaction of pancreatic BCF with IR plays an important role in the pathogenesis of T1DM and T2DM.15 While the insulin-stimulated glucose disposal rate (M value) is a well-established metric for assessing insulin sensitivity in T2DM, emerging evidence highlights heterogeneity in insulin sensitivity among T1DM patients.16 At present, the relationship between counter-regulatory hormone levels during hypoglycemia and insulin resistance in T1DM patients remains controversial. Therefore, this study aims to explore the differences in insulin counter-regulatory hormones during hypoglycemia between T1DM patients and normal people. The hypoglycemic clamp test were used to evaluate whether the M value affects counter-regulatory hormones in response to hypoglycemia in T1DM patients in our study.
Patients and Methods
Study Design and Population
According to the Declaration of Helsinki guidelines, this study protocol was approved by the Institutional Ethical Committee of Nanjing First Hospital in January, 2022 (Approval Number. KY20220124-07). This trial is also registered at ClinicalTrials.gov (ClinicalTrials.gov ID: NCT05290207). The written informed consent was provided by all patients. In this study, male, drug-naive patients aged 18–60 years with newly diagnosed T1DM were recruited. The WHO 1999 diagnostic criteria were used as the basis for the diagnostic criteria of diabetes.17 The WHO 1999 and 2019 diabetes diagnostic criteria differ in core indicators and diagnostic methods. For the first time, HbA1c ≥6.5% was included as one of the diagnostic criteria for diabetes in WHO 2019 Criteria. However, the applicability of HbA1c may be limited by factors such as anemia and hemoglobinopathies, requiring integration with clinical judgment. So we use the WHO 1999 criteria in our study. The first patient enrollment for this study occurred in March 2022. The exclusion criteria were (a) patients with secondary hypogonadism, (b) patients with acute infection or stress, (c) patients with acute complications of diabetes, (d) patients with serious systemic disease or any other condition that is considered unsuitable for this study, and (e) patients who used systemic SAIDs or any medication that may affect testosterone levels in the past 3 months. Finally, a total of 48 eligible male T1DM patients admitted to Nanjing First Hospital between March and December 2022 were included.
Experimental Procedures
Anthropometric parameters including blood pressure, height, weight and age were recorded. Blood samples of all patients were gathered after overnight fasting. Body mass index (BMI) was measured as weight divided by the square of height (kg/m2). The standard enzymatic assay was used to analyze liver and renal functions including creatinine (Cr), albumin (Alb), aspartate aminotransferase (AST), alanine aminotransferase (ALT), and lipid profiles such as apolipoprotein B (ApoB), apolipoprotein A1 (ApoA1), low-density lipoprotein (LDL), high-density lipoprotein (HDL), triglyceride (TG), and total cholesterol (TC). The chemiluminescent immunometric assay and high-performance liquid chromatography assay were used to measure fasting C-peptide (FCP) and glycated hemoglobin (HbA1c), respectively. The chemiluminescent immunometric assay was also used to measure circulating counter-regulatory hormones, such as glucagon (GCG), IGF-1, GH, Cor, and ACTH, which were collected at 0 and 30 minutes during hyperinsulinemic-hypoglycemic test.
Insulin Sensitivity Assessment
All participants underwent intensive insulin therapy via insulin pump for 1 week to achieve glycemic control, defined as >80% of fasting blood glucose (FBG) readings ≤7.0 mmol/L and 2-hour postprandial glucose ≤11.1 mmol/L, monitored via flash glucose monitoring (FGM). The insulin pump was stopped 12 hours before the start of the clamp, and the hyperinsulinemic-hypoglycemic clamp was used to evaluate insulin sensitivity.18 After an overnight fast, patients reported to the laboratory at 8:00 AM. Intravenous catheters were placed in the left antecubital fossa for insulin/glucose infusion and in the right antecubital fossa for blood sampling. A primed continuous insulin infusion (9 pmol/kg/min) was administered for 30 minutes, supplemented with potassium chloride (5 mmol/h) to prevent hypokalemia. Plasma glucose levels were monitored every 5 minutes, with a controlled reduction rate (~0.08 mmol/min) until a hypoglycemic nadir (2.9 ± 0.1 mmol/L) was achieved and stabilized using a modified glucose clamp technique.19,20 There were no Serious Adverse Events (SAEs) were reported during the course of this study. Counter-regulatory hormones were sampled at 0 and 30 minutes during hypoglycemia. Insulin sensitivity was quantified as the glucose infusion rate (GIR, mg/kg/min) during the final 30 minutes of steady-state hypoglycemia (M value).21
Statistical Analysis
Categorical variables were presented as the percentage (%). Continuous variables were described as the mean ± SE or median. The characteristics of patients in different treatment groups were compared using the χ2 test for categorical variables and one-way variance (ANOVA) for continuous variables. The correlation was detected by Spearman correlation coefficient. A non-parametric test was used when the data distribution was skewed. All statistical analyses were conducted using GraphPad Prism 6.0 and SPSS 22.0. P<0.05 was considered statistically significant.
Results
Baseline Characteristics
In this study, 34 male patients with newly diagnosed T1DM and 8 healthy controls were included. Clinical characteristics of the participants are summarized in Table 1. Using a glucose infusion rate (GIR) threshold of 5.700 mg/(kg·min) for insulin sensitivity stratification,16 participants were categorized into T1DM (n=34) and control (n=8) groups. The two groups were well matched in the history of hypertension, BMI, and age (all p > 0.05). The HbA1c level was higher in the T1DM group than in the normal group (p = 0.0012). The Fasting C-peptide level was lower in the T1DM group than in the normal group (p < 0.0001). There was no significant difference in ApoA1/ApoB, ApoB, ApoA1, LDL, HDL, TG, TC, Cr, AST, and ALT between the two groups (all p > 0.05).
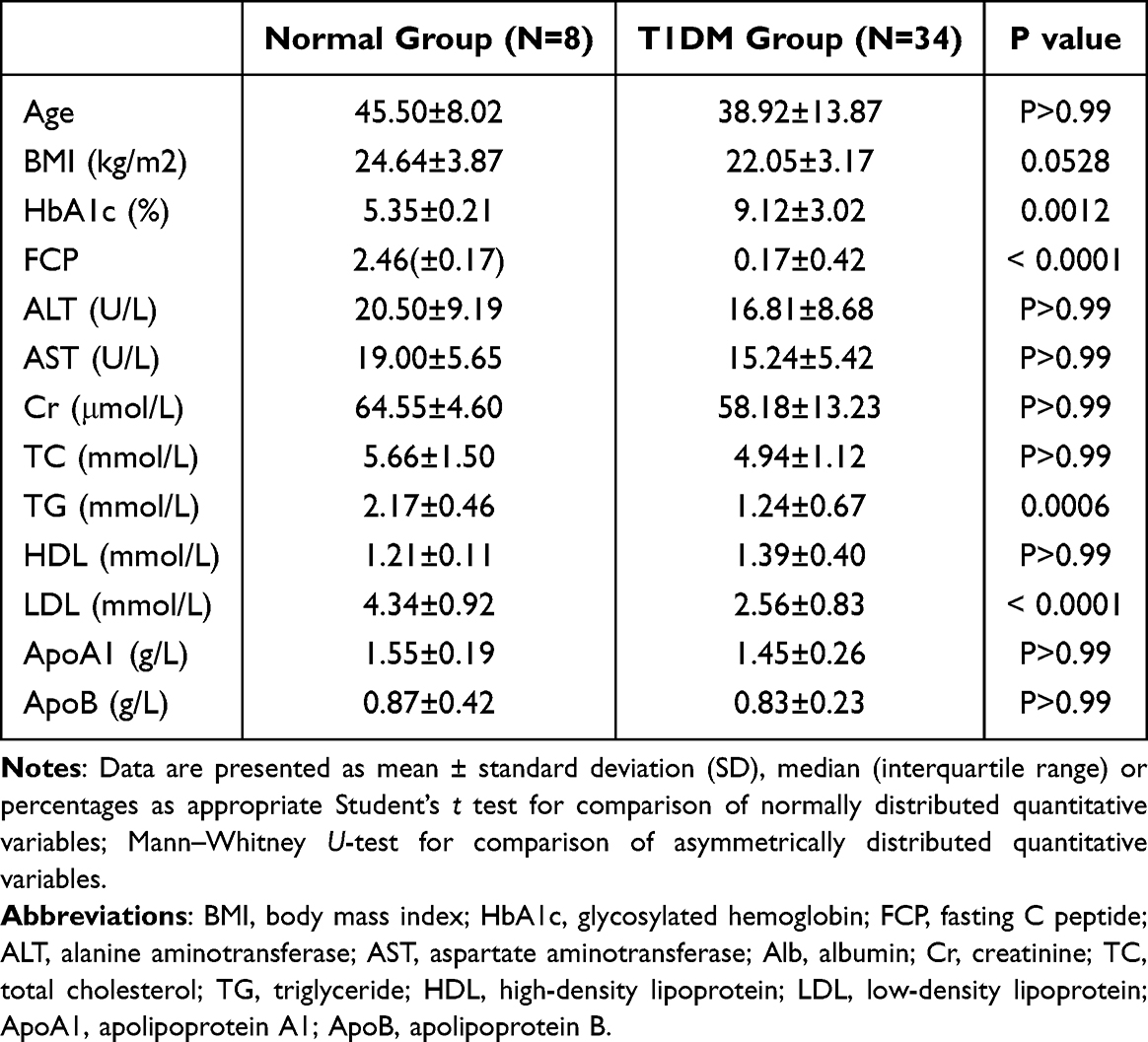 |
Table 1 Characteristics of Clinical Characteristics of Study Patients |
Circulating Counter-Regulatory Hormone Levels Between Groups
Counter-regulatory hormone, including ACTH, Cor, GH, IGF-1 and glucagon (GCG), profiles are presented in Table 2. At the beginning of hypoglycemic clamp test, the T1DM group had lower GH levels than the normal group (p = 0.0041) and had higher IGF-1 levels than the normal group (p = 0.0016). There was no difference in ACTH, Cor, and GCG between the two groups (all p > 0.050). Following 30 minutes of hypoglycemia, the T1DM group displayed reduced GCG responses (P = 0.0014) but elevated Cor (P = 0.0041) and GH (P = 0.0123) levels relative to controls. ACTH levels remained comparable between groups post-clamp (P > 0.05).
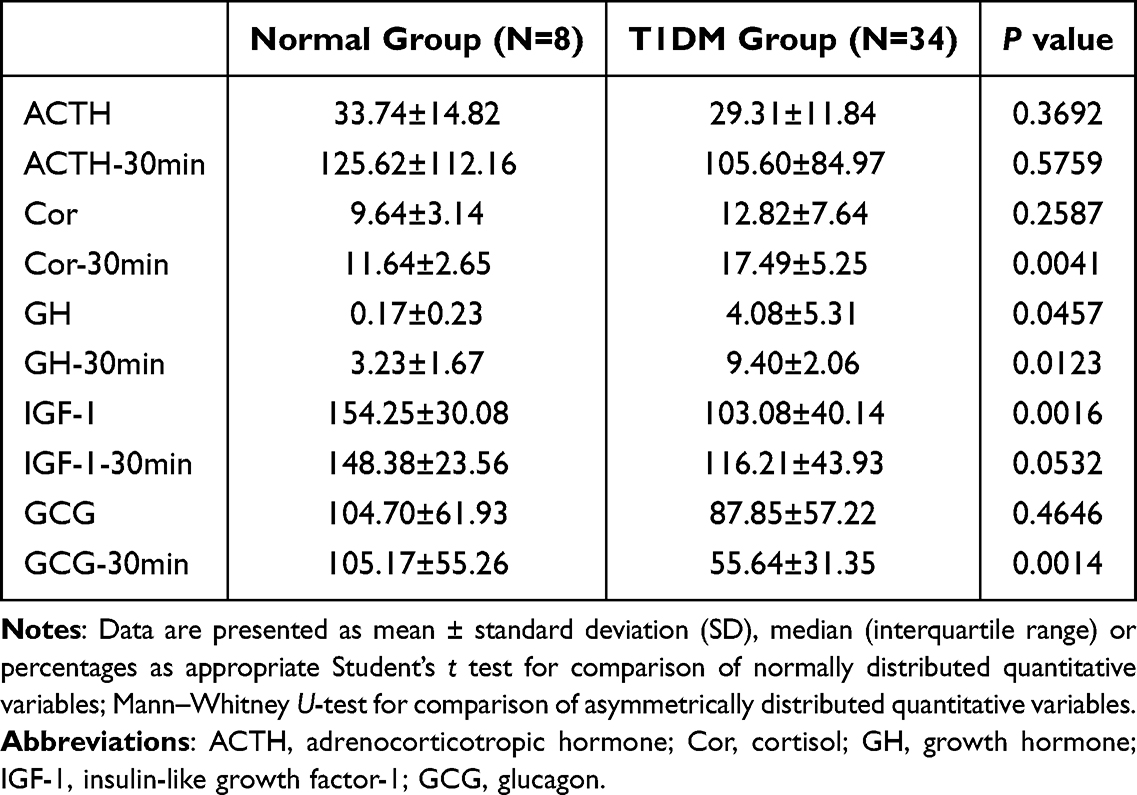 |
Table 2 Circulating Counter-Regulatory Hormones Levels Between Groups |
Linear Correlation Between Changes in Counter-Regulatory Hormone Levels and M Value in Male Patients with T1DM
The observed changes in counter-regulatory hormone levels and insulin resistance were validated in patients using Spearman correlation analysis. M value was negatively related to ΔACTH (r= −0.3055, p = 0.0303), ΔCor (r =- 0.2869, p = 0.0132), ΔGH (r = −0.2098, p = 0.0366), while M value was positively associated with ΔIGF-1 (r = 0.2838, p = 0.1894), instead of ΔGCG (r = 0.0089, p = 0.0478) (Figure 1). To address potential confounding by diabetes duration and metabolic parameters, multivariate linear regression models were constructed. ACTH and GH were excluded due to their upstream regulatory roles in IGF-1 and Cor secretion, which could introduce multicollinearity. After adjusted for Age, T1DM duration, BMI and HbA1c, M value was not independently correlated with IGF-1 and Cor levels (date not shown).
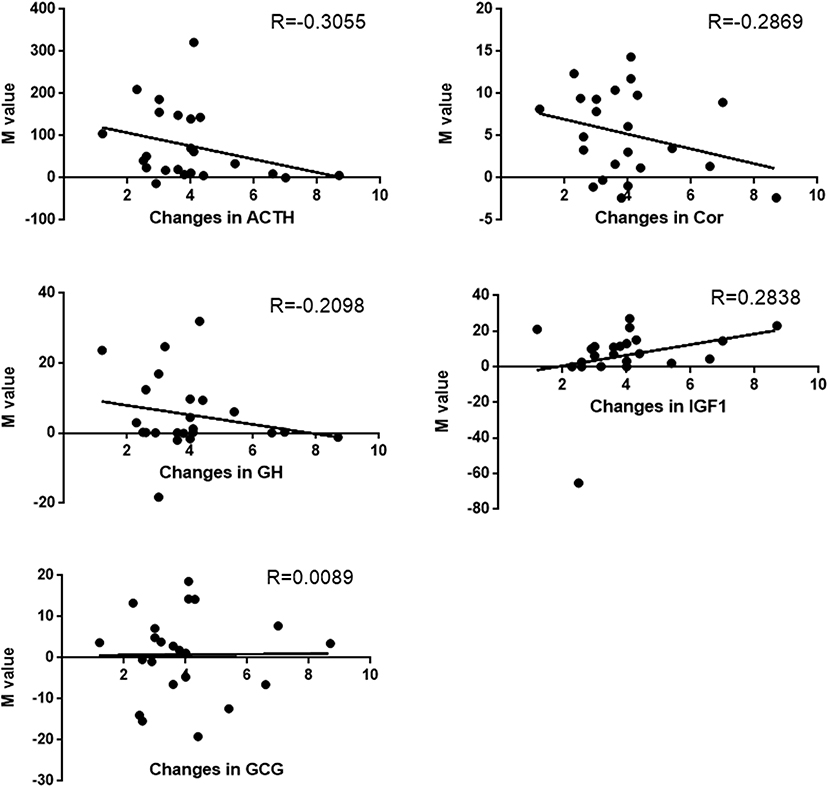 |
Figure 1 Correlation between changes in counter-regulatory hormone levels and M value in male patients with T1DM in linear regression. |
Discussion
In the present study, insulin counter-regulatory hormones were first examined in response to hypoglycemia in male patients with newly diagnosed T1DM and normal people. Key findings demonstrate that the T1DM group had a significantly higher multiple of Cor and GH elevation than the normal group in the hypoglycemic state during the hyperinsulinemic-hypoglycemic clamp test, which is an oppositive trend in GCG. Furthermore, insulin sensitivity (quantified as the M value) showed significant negative correlations with changes in adrenocorticotropic hormone (ΔACTH), ΔCor, and ΔGH, while displaying a nonsignificant positive association with ΔIGF-1 in male patients with newly diagnosed T1DM.
It was found that T1DM patients exhibited lower levels of ACTH, IGF-1, and GCG, and showed higher trends in GH and Cor at the beginning of the hypoglycemic clamp. Some studies have shown that the basic GH level in T1DM patients is normal or elevated, which is related to the negative feedback regulation of IGF-1 in the hypothalamus and pituitary.22,23 The various insulin counter-regulatory hormones mentioned above, such as Cor, GH, and ACTH, are mainly regulated by the central nervous system. In contrast, GCG is primarily regulated by glucose levels in the islet environment and also regulated by the central nervous system through counter-regulatory hormones and the autonomic nervous system.24–26 Some studies have found that the function of glucagon secretion is impaired with the prolongation of the T1DM course, which is closely related to blood glucose fluctuations, especially hypoglycaemia.27,28 After 30 minutes of the hypoglycemic clamp test, the results indicated that ACTH in T1DM patients showed no significant changes, Cor increased significantly, but GCG decreased significantly. This is consistent with previous findings. Previous studies have shown that even though the glucagon response to hypoglycemia has been weakened during the first year of T1DM, the adrenergic response has not been weakened, which suggests that the mechanism for the loss of insulin counter-regulatory hormones is different.29,30 This may explain the drastic decline in GCG. The study also showed that the average peak ACTH level of insulin-induced hypoglycemia was 3.5 times higher than the baseline level. This is also consistent with our findings.31 In premenopausal women with obesity, the ACTH-Cor relationship is characterized by reduced efficacy and sensitivity, which explains the absence of elevated serum Cor concentrations despite elevated plasma ACTH levels.32,33 The key finding is not just that these defects exist, but that they are already present and functionally significant at the clinical onset of the disease. It shows the entire counter-regulatory system is dysregulated from the very beginning, which is a significant pathophysiological insight. By studying drug-naive patients as new T1DM patients during the honeymoon phase, the study removes the confounding effects of long-term insulin therapy, chronic complications, and beta-cell exhaustion. This allows for a clearer view of the intrinsic hormonal dysregulation at play in early T1DM.
Our results showed that during the hypoglycemia test in T1DM patients, M values were negative correlated with ΔACTH, ΔCor, and ΔGH. Specifically, some studies showed cor (via ACTH stimulation) antagonizes insulin action by upregulating hepatic gluconeogenesis through increased expression of enzymes such as phosphoenolpyruvate carboxykinase (PEPCK) and glucose-6-phosphatase, thereby elevating blood glucose levels.34 Additionally, cor reduces peripheral glucose uptake in skeletal muscle and adipose tissue by downregulating GLUT4 transporters and impairing insulin receptor signalling.35 It also stimulates lipolysis, increasing free fatty acids (FFAs), which inhibit insulin signaling via lipid intermediates like diacylglycerols and ceramides that disrupt IRS-1/PI3K-Akt pathways.36 GH exhibits dual effects: while acute exposure may transiently mimic insulin-like actions, chronic elevation induces insulin resistance. GH promotes lipolysis, raising FFAs that interfere with muscle glucose uptake and enhance hepatic glucose production.37 Furthermore, GH activates JAK-STAT signaling pathways, inducing suppressor of cytokine signaling (SOCS) proteins that inhibit insulin receptor substrates (IRS) and PI3K-Akt signalling-critical for GLUT4 translocation-while also increasing hepatic glucose output via gluconeogenesis and glycogenolysis.38 Collectively, these hormones may antagonize insulin by amplifying hepatic glucose production, suppressing peripheral glucose uptake, and impairing insulin signaling through lipolysis, transcriptional modulation, and intracellular pathway interference, ultimately contributing to reduced M values during hypoglycemia.
Our results also showed the IGF-1 secretion response was significantly impaired in during the hypoglycemia test in T1DM patients. It can be speculated that this is because glucagon independent of insulin action induces a decrease in biologically active IGF-1 levels by regulating IGFBP-1 and IGFBP-2 levels, which is the mechanism by which glucagon induces GH secretion.39 Therefore, severe damage to GCG further leads to abnormal secretion of IGF-1. Meanwhile, it was found that compared with the normal group, the GH level was significantly elevated in T1DM patients at 0 min of the hypoglycemic clamp test, but the GH reactivity was decreased in T1DM patients at 30 min of the hypoglycemic clamp test. As we know, two endocrine systems are the insulin and GH/IGF-I axis which are interconnected at many levels. IGF-I production can be regulated by insulin, acting on the GH receptor or at a post-receptor site. The increased GH level may be due to a reduction in feedback inhibition or an alteration in hypothalamic/pituitary control. The former may, in turn, result from a low level of IGF-I, a reduction in the availability of IGF-I to relevant receptors, or an increase in the level of inhibitors.40 The normal individuals included in this study had a higher level of IGF-1 compared to T1DM patients, and it can be thus speculated that this may also be a contributing factor to this outcome.
Given the close association between M values and insulin counter-regulatory hormones in T1DM patients, longitudinal studies are required to explore how changes in insulin counter-regulatory hormone levels occur, especially in T1DM patients predisposed to these conditions. Moreover, there is a significantly negative linear correlation between M values and ACTH, Cor and GH, while a positive linear correlation between M values and IGF-1. These results demonstrate that changes in insulin counter-regulatory hormone levels may contribute to the increased insulin sensitivity in T1DM patients. After adjusted for Age, T1DM duration, BMI and HbA1c, M value was not independently correlated with IGF-1 and Cor levels by multivariate linear regression models. This state triggers the very counter-regulatory hormone responses we measured, meaning that the significant correlations we observed between ΔACTH, ΔCor, ΔGH, and the M-value are, in part, a reflection of this integrated stress response. This difference may be due to multiple factors. Firstly, this is a cross-sectional study that failed to draw a causal role for insulin counter-regulatory hormones in the pathogenesis of insulin resistance. The male-only focus controls for female hormonal variation but means the results are not applicable to females with T1DM. Secondly, this study was conducted in a singer center and with a small number of patients due to the high cost and complexity of the hyperinsulinemic-hypoglycemic clamp, thus limiting the power of our results to some extent. Data from cross-sectional study in a single center, while valuable, also has other limitations such as geographic bias, selection bias, institutional practices, recall bias, reproducibility issues, Unmeasured Confounders and so on, which can affect the generalizability, reliability, and applicability of research findings. The Thirdly, blood samples for 30 min into the hypoglycemic state were collected due to the financial resources of this study, possibly missing peak GCG secretion. Catecholamine, Cor and GH should also be observed if the blood glucose level is 2.2 mmol/L for more than 2 hours. However, in this study, it is risky and challenging from an ethical perspective.
Conclusion
In conclusion, the current study demonstrates that the abnormal insulin counter-regulatory hormone levels may contribute to an impaired insulin response during hypoglycaemia in patients with men newly diagnosed T1DM. This preliminary study provides a detailed pathophysiological snapshot, confirming that counter-regulatory hormone dysregulation and its correlation with insulin resistance are present at the diagnosis of T1DM in men. While the cross-sectional nature and limited sample size prevent causal inferences, the strong correlations between the stress hormone axis and metabolic function establish a foundation for future research. These findings highlight the need to explore whether this early hormonal milieu influences the long-term clinical course of the disease.
Data Sharing Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Compliance with Ethics Guidelines
Each participant provided written informed consent. This study protocol was approved by the Institutional Ethical Committee of Nanjing First Hospital in accordance with the Declaration of Helsinki guidelines (KY20220124-07). This trial is registered at Clinical Trials.gov (CT.gov identifier: NCT05290207).
Author Contributions
Y.Z, J.Z and J.M share co-first authorship. Y.Z: Data curation and Writing-original draft, J.Z: Data curation and Formal analysis, J.M: Methodology and Supervision, R.Y: Data curation, Y.L: Software and Formal analysis, R.H: Validation, Y.S: Visualization and Writing-review & editing. B.D: Conceptualization and Methodology. All authors took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
This work and Rapid Service Fee were supported by the Project supported by 2024 Nanjing Health Technology Development Special Fund (YKK24114), the National Key R&D Program of China (No. 2018YFC1314100), the In-Hospital Program of Jinling Hospital (To Jm Z, No. 2024JCYJQN095), the Postdoctoral Science Foundation of Nanjing 2024 (No. 2458, to Yt.Z), Jiangsu Innovative and Enterpreneurial Talent Program (No.JSSCBS20211546, to Yt.Z), and Future Science and Technology Talent Program of Nanjing First Hospital (to Yt.Z), the National Nature Science Foundation of China (NSFC-82402486).
Disclosure
The authors declare that there is no conflict of interest.
References
1. International Diabetes Federation. IDF virtual congress 2023. Diabet Res Clin Pract. 2023;198:110632. doi:10.1016/j.diabres.2023.110632
2. Wang L, Gao P, Zhang M, et al. Prevalence and ethnic pattern of diabetes and prediabetes in China in 2013. JAMA. 2017;317(24):2515–2523. doi:10.1001/jama.2017.7596
3. Dong C, Wu G, Li H, et al. Type 1 and type 2 diabetes mortality burden: predictions for 2030 based on Bayesian age-period-cohort analysis of China and global mortality burden from 1990 to 2019. J Diabetes Investig. 2024;15(5):623–633. doi:10.1111/jdi.14146
4. Kramer CK, Borgono CA, Van Nostrand P, et al. Glucagon response to oral glucose challenge in type 1 diabetes: lack of impact of euglycemia. Diabetes Care. 2014;37(4):1076–1082. doi:10.2337/dc13-2339
5. Davis HA, Spanakis EK, Cryer PE. Hypoglycemia During Therapy of Diabetes, in Endotext. Feingold KR. Editors. South Dartmouth (MA):2000.
6. Cryer PE. Hypoglycemia: still the limiting factor in the glycemic management of diabetes. Endocr Pract. 2008;14(6):750–756. doi:10.4158/EP.14.6.750
7. Chen S, Lu J, Peng D, et al. Incidence rate and risk factors for hypoglycemia among individuals with type 1 diabetes or type 2 diabetes in China receiving insulin treatment. Diabet Res Clin Pract. 2023;206:110987. doi:10.1016/j.diabres.2023.110987
8. Leelarathna L, Little SA, Walkinshaw E, et al. Restoration of self-awareness of hypoglycemia in adults with long-standing type 1 diabetes: hyperinsulinemic-hypoglycemic clamp substudy results from the HypoCOMPaSS trial. Diabetes Care. 2013;36(12):4063–4070. doi:10.2337/dc13-1004
9. Tripyla A, Herzig D, Reverter-Branchat G, et al. Counter-regulatory responses to postprandial hypoglycaemia in patients with post-bariatric hypoglycaemia vs surgical and non-surgical control individuals. Diabetologia. 2023;66(4):741–753. doi:10.1007/s00125-022-05861-9
10. Sanchez-Rangel E, Deajon-Jackson J, Hwang JJ. Pathophysiology and management of hypoglycemia in diabetes. Ann N Y Acad Sci. 2022;1518(1):25–46. doi:10.1111/nyas.14904
11. Espes D, Liljeback H, Hill H, et al. GABA induces a hormonal counter-regulatory response in subjects with long-standing type 1 diabetes. BMJ Open Diabetes Res Care. 2021;9(1):e002442. doi:10.1136/bmjdrc-2021-002442
12. Nathan DM, Group DER. The diabetes control and complications trial/epidemiology of diabetes interventions and complications study at 30 years: overview. Diabetes Care. 2014;37(1):9–16. doi:10.2337/dc13-2112
13. Bengtsen MB, Stoy J, Rittig NF, et al. A human randomized controlled trial comparing metabolic responses to single and repeated hypoglycemia in type 1 diabetes. J Clin Endocrinol Metab. 2020;105(12):e4699–e4711. doi:10.1210/clinem/dgaa645
14. Weaver JU, Kopelman PG, McLoughlin L, et al. Hyperactivity of the hypothalamo-pituitary-adrenal axis in obesity: a study of ACTH, AVP, beta-lipotrophin and cortisol responses to insulin-induced hypoglycaemia. Clin Endocrinol. 1993;39(3):345–350. doi:10.1111/j.1365-2265.1993.tb02375.x
15. Vladu M, Clenciu D, Efrem IC, et al. Insulin resistance and chronic kidney disease in patients with type 1 diabetes mellitus. J Nutr Metab. 2017;2017:6425359. doi:10.1155/2017/6425359
16. Tang X, Yan X, Zhou H, et al. Associations of insulin resistance and beta-cell function with abnormal lipid profile in newly diagnosed diabetes. Chin Med J. 2022;135(21):2554–2562. doi:10.1097/CM9.0000000000002075
17. Alberti KG, Zimmet PZ. Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: diagnosis and classification of diabetes mellitus provisional report of a WHO consultation. Diabet Med. 1998;15(7):539–553. doi:10.1002/(SICI)1096-9136(199807)15:7<539::AID-DIA668>3.0.CO;2-S
18. Qian X, Wang H, Yang G, et al. Pioglitazone improved insulin sensitivity and first phase insulin secretion among obese and lean people with diabetes: a multicenter clamp study. Diabetes Ther. 2018;9(2):815–826. doi:10.1007/s13300-018-0401-9
19. Amiel SA, Tamborlane WV, Simonson DC, et al. Defective glucose counterregulation after strict glycemic control of insulin-dependent diabetes mellitus. N Engl J Med. 1987;316(22):1376–1383. doi:10.1056/NEJM198705283162205
20. Mikeladze M, Hedrington MS, Joy N, et al. Acute effects of oral dehydroepiandrosterone on counterregulatory responses during repeated hypoglycemia in healthy humans. Diabetes. 2016;65(10):3161–3170. doi:10.2337/db16-0406
21. Jiang LL, Wang SQ, Ding B, et al. The effects of add-on exenatide to insulin on glycemic variability and hypoglycemia in patients with type 1 diabetes mellitus. J Endocrinol Invest. 2018;41(5):539–547. doi:10.1007/s40618-017-0765-0
22. Kinsley BT, Widom B, Utzschneider K, et al. Stimulus specificity of defects in counterregulatory hormone secretion in insulin-dependent diabetes mellitus: effect of glycemic control. J Clin Endocrinol Metab. 1994;79(5):1383–1389. doi:10.1210/jcem.79.5.7962332
23. Press M, Tamborlane WV, Thorner MO, et al. Pituitary response to growth hormone-releasing factor in diabetes: failure of glucose-mediated suppression. Diabetes. 1984;33(8):804–806. doi:10.2337/diab.33.8.804
24. Watts AG, Donovan CM. Sweet talk in the brain: glucosensing, neural networks, and hypoglycemic counterregulation. Front Neuroendocrinol. 2010;31(1):32–43. doi:10.1016/j.yfrne.2009.10.006
25. McCrimmon RJ, Evans ML, Fan X, et al. Activation of ATP-sensitive K+ channels in the ventromedial hypothalamus amplifies counterregulatory hormone responses to hypoglycemia in normal and recurrently hypoglycemic rats. Diabetes. 2005;54(11):3169–3174. doi:10.2337/diabetes.54.11.3169
26. Routh VH. Glucosensing neurons in the ventromedial hypothalamic nucleus (VMN) and hypoglycemia-associated autonomic failure (HAAF). Diabetes Metab Res Rev. 2003;19(5):348–356. doi:10.1002/dmrr.404
27. Li K, Song WJ, Wu X, et al. Associations of serum glucagon levels with glycemic variability in type 1 diabetes with different disease durations. Endocrine. 2018;61(3):473–481. doi:10.1007/s12020-018-1641-1
28. Farhy LS, Chan A, Breton MD, et al. Association of basal hyperglucagonemia with impaired glucagon counterregulation in type 1 diabetes. Front Physiol. 2012;3:40. doi:10.3389/fphys.2012.00040
29. Arbelaez AM, Xing D, Cryer PE, et al. Blunted glucagon but not epinephrine responses to hypoglycemia occurs in youth with less than 1 yr duration of type 1 diabetes mellitus. Pediatr Diabetes. 2014;15(2):127–134. doi:10.1111/pedi.12070
30. Sherr J, Xing D, Ruedy KJ, et al. Lack of association between residual insulin production and glucagon response to hypoglycemia in youth with short duration of type 1 diabetes. Diabetes Care. 2013;36(6):1470–1476. doi:10.2337/dc12-1697
31. Grzywa M. Serum somatomedin activity and growth hormone level in obese men: dependence on degree of obesity and hyperlipidemia. Exp Clin Endocrinol. 1986;88(3):325–333. doi:10.1055/s-0029-1210613
32. Praveen EP, Sahoo JP, Kulshreshtha B, et al. Morning cortisol is lower in obese individuals with normal glucose tolerance. Diabetes Metab Syndr Obes. 2011;4:347–352. doi:10.2147/DMSO.S23915
33. Jessop DS, Dallman MF, Fleming D, et al. Resistance to glucocorticoid feedback in obesity. J Clin Endocrinol Metab. 2001;86(9):4109–4114. doi:10.1210/jcem.86.9.7826
34. Zhou PZ, Zhu YM, Zou GH, et al. Relationship between glucocorticoids and insulin resistance in healthy individuals. Med Sci Monit. 2016;22:1887–1894. doi:10.12659/MSM.895251
35. Beaupere C, Liboz A, Feve B, et al. Molecular mechanisms of glucocorticoid-induced insulin resistance. Int J Mol Sci. 2021;22(2):623. doi:10.3390/ijms22020623
36. Petersen MC, Shulman GI. Mechanisms of Insulin Action and Insulin Resistance. Physiol Rev. 2018;98(4):2133–2223. doi:10.1152/physrev.00063.2017
37. Huang Z, Huang L, Waters MJ, et al. Insulin and growth hormone balance: implications for obesity. Trends Endocrinol Metab. 2020;31(9):642–654. doi:10.1016/j.tem.2020.04.005
38. Liu W, Wang X. Research advances on Suppressor of Cytokine Signaling 3 (SOCS3) in animal carbohydrate and lipid metabolism processes. Pak J Biol Sci. 2022;25(12):1100–1108. doi:10.3923/pjbs.2022.1100.1108
39. Sarem Z, Bumke-Vogt C, Mahmoud AM, et al. Glucagon decreases IGF-1 bioactivity in humans, independently of insulin, by modulating its binding proteins. J Clin Endocrinol Metab. 2017;102(9):3480–3490. doi:10.1210/jc.2017-00558
40. Holly JM, Amiel SA, Sandhu RR, et al. The role of growth hormone in diabetes mellitus. J Endocrinol. 1988;118(3):353–364. doi:10.1677/joe.0.1180353
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.