")
Back to Journals » Patient Preference and Adherence » Volume 17
Comparative Evaluation of Efficacy of Ketoprofen and Diclofenac Transdermal Patches with Oral Diclofenac Tablet on Postoperative Endodontic Pain- A Randomized Clinical Trial
Authors Porwal P, Shah N, Singh Rao A , Jain I, Maniangat Luke A, Shetty KP, Reda R , Testarelli L , Pawar AM
Received 15 May 2023
Accepted for publication 20 September 2023
Published 27 September 2023 Volume 2023:17 Pages 2385—2393
DOI https://doi.org/10.2147/PPA.S421371
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Jongwha Chang
Priya Porwal,1 Nimisha Shah,1 Ajay Singh Rao,1 Ihit Jain,2 Alexander Maniangat Luke,3,4 Krishna Prasad Shetty,3,4 Rodolfo Reda,5 Luca Testarelli,5 Ajinkya M Pawar6
1Department of Conservative Dentistry and Endodontics, K M Shah Dental College and Hospital, Sumandeep Vidyapeeth, Vadodara, Gujarat, India; 2Department of Dental Sciences, GBH American Hospital, Udaipur, Rajasthan, India; 3Department of Clinical Sciences, College of Dentistry, Ajman University, Ajman, United Arab Emirates; 4Centre of Medical and Bio-Allied Health Sciences Research (CMBAHSR), Ajman University, Ajman, United Arab Emirates; 5Section of Endodontics, Department of Oral and Maxillo-Facial Sciences, Sapienza University of Rome, Rome, Italy; 6Department of Conservative Dentistry and Endodontics, Nair Hospital Dental College, Mumbai, Maharashtra, India
Correspondence: Luca Testarelli, Section of Endodontics, Department of Oral and Maxillo-Facial Sciences, Sapienza University of Rome, Rome, Italy, Email [email protected] Alexander Maniangat Luke, Department of Clinical Sciences, College of Dentistry, Ajman University, Ajman, United Arab Emirates, Email [email protected]
Purpose: Evaluate the efficacy of transdermal patches containing ketoprofen and diclofenac sodium compared to oral diclofenac tablets in reducing post-endodontic pain after single-visit root canal therapy for teeth with symptomatic irreversible pulpitis.
Methods: A total of 78 eligible participants with symptomatic irreversible pulpitis and preoperative VAS scores of 4 or above were enrolled after obtaining ethical approval (SVIEC/ON/DENT/SRP/22064) and CTRI registration (CTRI/2022/07/044231). Exclusion criteria included pregnancy, lactation, fractured/cracked teeth, developmental anomalies, tooth pathology, or ongoing analgesic/NSAID use. After root canal treatment, participants were randomized into three groups using computer randomization. Groups A and B received transdermal patches with Ketoprofen and diclofenac sodium, respectively, applied to the right forearm for 24 hours, with an additional patch on the left forearm for the next day. Group C received four diclofenac sodium oral tablets, twice daily for two days. VAS scales were used to assess pain at 4, 8, 24, and 48 hours post-treatment. The VAS scores collected were tabulated and statistically analyzed using SPSS version 21 with (P < 0.05). Shapiro Wilk test and the Related Samples Friedman’s Two-Way Analysis of Variance by Ranks were used for statistical evaluation.
Results: Statistically significant reductions in mean postoperative pain scores were observed across all groups at all time points compared to preoperative scores. Notably, the Ketoprofen patch group exhibited superior performance compared to the diclofenac transdermal patch and oral diclofenac tablet groups at 48 hours, with statistical significance (p=0.047).
Conclusion: The present evidence substantiates the efficacy of transdermal patches containing diclofenac and ketoprofen in managing postoperative pain arising from symptomatic irreversible pulpitis in single-rooted teeth. By avoiding the use of oral NSAIDs, these patches provide effective pain relief while minimizing the risk of adverse effects, presenting a favorable option for patients.
Keywords: diclofenac transdermal patch, ketoprofen transdermal patch, oral analgesics, topical NSAIDs
Introduction
Managing pain can be difficult and is often used to evaluate the clinician’s skill in endodontic practice. Unfortunately, many people perceive root canal therapy as a painful experience, which can lead to patients opting for tooth extraction instead of endodontic treatment.1,2
Significant efforts have been made to create medications that can effectively treat pain. One important group of drugs that has been used for centuries to alleviate pain are Non-steroidal Anti-inflammatory Drugs (NSAIDs). In dentistry, commonly used non-narcotic painkillers include aspirin, diclofenac sodium, ketoprofen, ibuprofen, and paracetamol. These drugs work by inhibiting the enzymes COX-1 and COX-2, which are crucial for the production of prostaglandins and are responsible for their effectiveness in reducing pain.3
Despite their effectiveness in pain and inflammation management, NSAIDs pose serious risks such as small-intestinal ulceration, GI tract bleeding, renal complications like acute (ARF) and chronic (CRF) renal failure, cardiovascular complications and electrolyte imbalance, particularly in patients with underlying systemic conditions and those taking multiple medications. Combining NSAIDs with other pain relievers can exacerbate gastric discomfort and lead to potentially dangerous interactions with other drugs. Thus, minimizing polypharmacy is crucial to prevent adverse consequences.4–7
The topical administration of NSAIDs is considered a revolutionary solution to tackle the difficulties posed by conventional drug delivery methods. Topical delivery involves directly applying the medication to the skin, eyes, nose, or mucous membranes to treat localized conditions, avoiding problems associated with oral administration, such as hepatic first-pass metabolism, gastric pH variations, and plasma level fluctuations.8 Topical medications can come in the form of ointments, gels, lotions, transdermal patches, and sprays. Both transdermal and topical routes of analgesics provide a non-invasive mode of administration that offers numerous benefits, including high efficacy and a favorable adverse effects profile. The transdermal route is particularly promising as it delivers medication painlessly with minimal side effects, resulting in excellent patient compliance.9 Through the use of lipid-based solutions, drugs can passively diffuse through the skin over an extended period, achieving the desired therapeutic effects. Transdermal drug delivery eliminates the fear of needles and associated complications, making it an appealing option for patients.10
The market offers various transdermal patches containing NSAIDs, such as ketoprofen, diclofenac and piroxicam. Among these, diclofenac is a commonly used NSAID as an analgesic and anti-inflammatory agent following dental treatments.11 Diclofenac, being an organic acid, has the ability to dissolve in lipids and its salts can dissolve in water at neutral pH. These characteristics make it possible for the drugs to easily permeate through cell membranes. Ketoprofen is another leading NSAID available, in patch and gel forms. In addition to inhibiting cyclooxygenase (COX), ketoprofen stabilizes lysosomal membranes and antagonizes bradykinin action leading pain control for a prolonged period.12
Due to the limited literature on the efficacy of transdermal patches in pain management. Specifically, the study focuses on comparing the pain-relieving efficacy of diclofenac and ketoprofen transdermal patches to the conventional oral diclofenac tablet in patients suffering from symptomatic irreversible pulpitis. This is an important area of investigation as current pain management techniques may not be effective for all patients and alternative methods may be necessary. The null hypothesis indicated that there will be no difference in the pain-relieving efficacy of diclofenac and ketoprofen transdermal patches to the conventional oral diclofenac tablet in patients suffering from symptomatic irreversible pulpitis. The primary objective of the study was to assess the pain-relieving efficacy of the transdermal patches in comparison to oral diclofenac tablet which is considered as a positive control group and as a secondary objective the study also aimed to record any adverse effects experienced by patients due to drugs given.
Materials and Methods
Ethical Statement
Institutional ethical committee approval was obtained (SVIEC/ON/DENT/SRP/22064) by K.M. Shah Dental College and Hospital, Sumandeep Vidyapeeth, Gujarat which was in accordance with the Declaration of Helsinki, prior to initiation of the study. The trial was registered on CTRI (CTRI/2022/07/044231) and informed consent was obtained from the patients.
Patient Enrolment
Patients in the age group of 18 to 65 years of age, who were ambulant and medically healthy (ASA I or II),13 requiring non-surgical root canal treatment diagnosed as symptomatic irreversible pulpitis with or without apical periodontitis having preoperative VAS score more than 4 indicated for single visit endodontics were included in the study. Patients meeting any of the following conditions were excluded from participation: Patients who have previously used analgesics or non-steroidal anti-inflammatory drugs within 24 hours prior to procedure. People who have a hypersensitivity or allergic reaction to the drug diclofenac. Patients with a history of hypertension or underlying heart disease. Pregnant or breast-feeding as it may affect fetal development or lactation. People with visibly broken or cracked teeth. Persons with dental development abnormalities that may affect study results. Patients with closed pulpitis characterized by the absence of clinical signs of pulpal inflammation.
Medical history was taken in the outpatient department as a part of initial screening process which assessed the blood pressure, blood sugar, body temperature and any other systemic conditions and allergies of all the patients and mentioned the same on patient’s case history sheet and only those patients who were medically fit and had blood pressure levels below 140/90 mmHg were considered for the study. Signs and symptoms of the patients were carefully recorded including history and type of pain, sleep disturbances, aggravating and relieving factors.
To achieve a comprehensive examination, the clinical assessment of each tooth included numerous crucial characteristics. Examining the tooth for symptoms of carious lesions, evaluating for tenderness upon percussion, and carrying out pre-operative tests to determine the tooth’s responsiveness were all part of the procedure. The cold test was intended solely to check for any delayed or absent reaction in compared to a healthy tooth on the contrary side. Furthermore, intraoral periapical radiographs were used to identify radiolucency, suggesting probable pulp and dentin involvement, with or without periapical radiolucency. The study’s inclusion criteria were patients with a Peri Apical Index score (PAI) of ≤ 2 on radiographic findings.14–16
Randomization and Allocation
A single endodontist with clinical experience in endodontics carried out the root canal treatment on all patients. A research assistant who was not involved in the treatment allocated patients randomly using a permutation block method and stratified by gender. The patient codes were generated by a computer software using https://www.randomizer.org/ and were concealed in 3 opaque envelopes After the completion of treatment, the envelopes were opened in sequence using the SNOSE method (sequentially numbered opaque sealed envelopes) to assign patients to any one out of the three groups and the allocation ratio was kept to be 1:1:1. Group I received two transdermal ketoprofen patches (Ketoplast plus patch, 30mg. Zuventus Healthcare Ltd., Mumbai, Maharashtra, India) to use once a day. Group Il received 2 transdermal diclofenac patches (Sandor Diclo-Touch, 100 mg, Sandor Medicaids Pvt. Ltd., Hyderabad, Telangana, India) to use once a day. Group IlI patients received four oral diclofenac tablets (Voveran 50mg, Novartis India Ltd., Mumbai, Maharashtra, India) twice daily for 48 hours which was considered as a control group (gold standard) as diclofenac is claimed to be more effective than ibuprofen and is a commonly prescribed NSAID to relieve postoperative pain in dentistry.11
A dental nurse, who was blinded to the group allocation, assessed postoperative pain using the Visual Analogue Scale (VAS) as the co-investigator 2. The study was conducted in a double-blinded manner, and neither the principal investigator nor co-investigator 2 was aware of the group allocation. Patients could not be blinded in the study due to difference in physical forms of the study drugs.
Sample Size Calculation
Sample size calculation was done according to the research conducted by Mangal et al, 2020.17 The study considered a mean difference in delta E of 0.57 between three groups, with a 5% alpha error and 90% power. Additionally, a clinically significant difference of 0.5 units was taken into account. Based on these factors, a sample size required for each group was 22. To compensate for potential dropout or a lack of response during follow-up, four additional samples were included per group. Therefore, a total of 26 samples were included per group (Figure 1).
 |
Figure 1 The PRIRATE 2020 flowchart. |
Treatment Protocol
The clinical procedure involved a conventional inferior alveolar and long buccal nerve block for mandibular teeth or infiltration anesthesia for maxillary teeth using 1.8 mL 2% lignocaine with 1: 200,000 epinephrine (Aquacaine plus, Aqua Fine Injecta Pvt. Ltd., Pune, Maharashtra, India) followed by assessment of subjective and objective symptoms of anesthetic success. Caries excavation and access cavity preparation with an Endo access bur was done. (Dentsply Tulsa, Tulsa, OK, USA). Composite wall build-up was done in cases with missing walls using nano-hybrid composite (3M ESPE Filtek Z350, Seefeld, Bayern, Germany) in case of class II carious lesion. Rubber dam isolation of the concerned tooth was done. Canals were debrided using hand K files (Mani Inc, Tochigi-Ken, Japan) and working length was determined using apex locator (root ZX mini, J Morita corp. Tokyo, Japan) followed by irrigation with normal saline and 5.25% sodium hypochlorite solution (Prime Dental Products Pvt Ltd, Mumbai, Maharashtra, India). Further chemo-mechanical preparation was done using rotary files (EdgeEndo NiTi rotary files, Henry Schien, Gillingham, Kent) After chemo-mechanical preparation subsequent master gutta percha was inserted to working length, tug back was checked and master cone radiograph was taken for confirmation followed by obturation with AH plus epoxy resin (Maillefer Dentsply, Konstanz, Germany) sealer with gutta percha using lateral condensation technique. Following root canal treatment, post endodontic restoration was done using composite and fiber reinforced composite (Ever X posterior, GC, Medak, Telangana, India) was used in cases of extensive tooth structure loss. After endodontic treatment, the patient was provided with the respective study drug in the form of either a tablet or a patch placed on the right forearm. Patients were provided with a chart of 4 VAS scales which they were instructed to fill at four-time intervals at 4h, 8h, 24h, and 48h and were advised to record any side effects like gastric irritation, vomiting, diarrhea, nausea, dizziness, and local irritation due to the allotted drug. The VAS scores were recorded by CI-2 on the next visit at the end of two days.
Evaluation Criteria
Patients were asked to describe the intensity of pain on the VAS scale at 4h, 8h, 24h and 48h postoperatively on VAS scale (Figure 2).
 |
Figure 2 VAS scale employed in the current study. |
Statistical Analysis
The VAS scores collected were tabulated and statistically analyzed using SPSS version 21 (IBM Corp., Armonk, NY, USA) with (P < 0.05) and 95% confidence interval.
Normality of the data was assessed using Shapiro Wilk test and it was found that the data was not normally distributed (p<0.05). Thus, non-parametric test was applied for testing the hypothesis. Mean and standard deviation were computed for descriptive analysis.
Independent Samples Kruskal–Wallis Test was used to compare the three groups in terms of mean pain scores at preoperative and post-operative at four-time intervals at 4h, 8h, 24h and 48h (inter-group analysis). To compare the preoperative and post-operative VAS scores in each group Related Samples Friedman’s Two-Way Analysis of Variance by Ranks was used indicating the reduction in pain scores at 4h, 8h, 24h and 48h time interval (intra-group analysis).
Results
Of the 78 patients enrolled, 26 patients were allocated to each group, consisting of 41 males and 37 females, 50 maxillary and 28 mandibular teeth. 37 patients belonged to the age group of 18–40 years, 41 patients belonged to the age group of 40–60 years (Table 1). As there were dropouts (Group A = 1, Group B = 3 and Group C = 3), modified intention-to-treat analysis using the last observation carried forward approach. Mean preoperative score was 5.69±1.46, 5.65±1.16, 5.84±1.46 in group A, B and C respectively (Figure 3). However, there was no significant difference in pre-operative VAS score (p = 0.918).
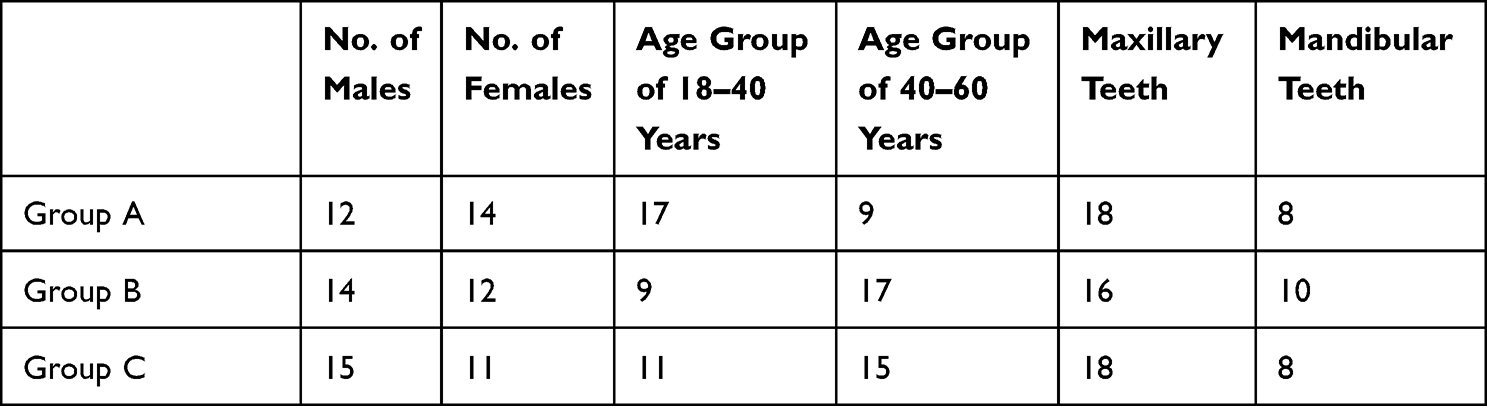 |
Table 1 Demographic Data for the Study Participants Included in the Trial |
 |
Figure 3 Comparison of VAS score at different time interval in the 3 groups. |
The study found statistically significant difference in the mean preoperative and postoperative scores in all the three groups at all-time intervals (p < 0.001). Comparing the parameters 4h, 8h, 24h between the three groups revealed no significant difference (p value of 0.622, 0.239, 0.336 respectively) (Figure 3). Among the three experimental groups, group A (ketoprofen patch) performed better than group B (diclofenac patch) and C (diclofenac tablet) at 48 hours which was statistically significant (p=0.047). The lowest mean pain values were observed in Group A (0.11±0.32), followed by Group C (0.61±0.89) and Group B (0.65±1.29) at the end of 48 hours (Table 2). None of the patients in the transdermal group (A & B) reported any adverse effects and 10 out of 23 patients reported of a gastric discomfort (Table 3).
 |
Table 2 Intra- and Inter-Group Comparison of Mean VAS Score for Pain in the Three Groups |
 |
Table 3 Inter-Group Comparison for the Occurrence of Adverse Effects |
Discussion
Dental care is often associated with pain by patients, and poorly managed pain during dental treatment causing them to avoid or postpone treatment. The management of post-endodontic pain has been an area of constant research, with better formulations and methods continuously replacing outdated ones. The present study was conducted to evaluate and compare the effectiveness of transdermal patches of ketoprofen and diclofenac sodium with oral diclofenac tablet on post-endodontic pain reduction following single-visit root canal therapy in symptomatic irreversible pulpitis. Based on the results of the study the null hypothesis was partially rejected. All the three groups (Group A – ketoprofen patch, Group B – diclofenac sodium patch, and Group C – oral diclofenac tablet) had a statistical significant reduction in post-endodontic pain compared to pre-operative pain levels (p < 0.001). However, the ketoprofen patch showed the highest reduction in pain at 48 hours which was statistically significant compared to the other two groups, followed by the diclofenac sodium patch and the oral diclofenac tablet. These findings suggest that transdermal patches of ketoprofen and diclofenac sodium can provide effective pain relief in post-endodontic pain.
The results of this study align with earlier research carried out by Murugan et al,18 who examined the efficacy of oral and transdermal diclofenac for managing pain in patients with symptomatic irreversible pulpitis after single-visit root canal therapy. The study concluded that transdermal diclofenac patches are more effective than oral diclofenac tablets in controlling pain following single-visit root canal treatment.
Our study revealed that the use of a ketoprofen patch resulted in superior pain control compared to both diclofenac patch and diclofenac tablet, as indicated by lower mean visual analog scores. These findings are consistent with previous studies by Bhargava et al,19 and Krishna and Nataraj20 who also observed similar results when comparing the efficacy of the two patches following different surgical procedures. A recent systematic review and meta-analysis by Mason et al,21 concluded that transdermal diclofenac patches are used to treat sports-related injuries.
The reason for the superior pain control offered by the ketoprofen patch over the diclofenac patch and tablet can be attributed to various factors. While diclofenac only inhibits COX-1 and COX-2 to reduce prostaglandin synthesis, ketoprofen inhibits both COX and the lipoxygenase pathway of the arachidonic acid cascade, thus reducing the synthesis of leukotrienes. Moreover, ketoprofen effectively inhibits bradykinin and stabilizes lysosomal membranes to prevent osmotic damage and decrease inflammatory reactions. Although ketoprofen is more potent than diclofenac, its limited use in clinical practice could be due to the unavailability of the ketoprofen patch compared to the diclofenac patch. Nonetheless, ketoprofen administered as traits dermal medication supersedes diclofenac in terms of efficacy.22
However, the oral administration of NSAIDs can cause a number of side effects. Like gastric discomfort, ulceration and bleeding, cardiovascular complications, allergic reactions, drowsiness, nausea and vomiting.23
Transdermal patches deliver drugs through the skin and into the bloodstream. They work by using a combination of adhesive layers and permeable membranes to control the release of medication over a period of time. When a transdermal patch is applied to the skin, the drug in the patch dissolves or is dispersed in a matrix or reservoir that is in contact with the skin. The drug molecules then diffuse through the skin’s layers and into the bloodstream, bypassing the digestive system and liver metabolism that can alter the medication’s efficacy.24
The transdermal route of drug delivery has several advantages, including sustained release of the drug, better patient compliance, and minimal side effects. However, transdermal drug delivery has certain limitations such as the possibility of skin irritation, inability to deliver macromolecular agents and ionic drugs, and unsuitability for patients in shock or with low peripheral blood flow.25
Regarding safety, 10 out of the 23 patients who took oral diclofenac experienced gastric discomfort, whereas none of the patients who used the transdermal patch reported any local or systemic discomfort. Research conducted by Agarwal et al,26 found that using a diclofenac patch to reduce venous cannulation resulted in a localized red rash at the application site of the patch. However, in the current study, positive results may have been achieved because the diclofenac patch was applied to different sites each time. In a review on the use of topical NSAIDs, Mason et al,21 emphasized the safety of diclofenac patches.
Furthermore, the study has some limitations. The sample size was relatively small, and the study was conducted on patients with a specific diagnosis of symptomatic irreversible pulpitis. The results may not be generalizable to other types of endodontic cases or to patients with different diagnosis.
Conclusion
Transdermal patches of ketoprofen and diclofenac sodium can be effective in reducing post-endodontic pain after single-visit root canal treatment in symptomatic irreversible pulpitis. To validate the results of this study, further research using bigger sample sizes and a variety of diagnoses is necessary.
Data Sharing Statement
The raw data will be provided if requested from the corresponding author.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Nivethithan T, Raj JD. Endodontic pain-cause and management: a review. Int J Pharm Sci. 2015;6(7):2723.
2. Keiser K, Hargreaves KM. Building effective strategies for the management of endodontic pain. Endod Topics. 2002;3(1):93–105. doi:10.1034/j.1601-1546.2002.30109.x
3. Smith EA, Marshall JG, Selph SS, Barker DR, Sedgley CM. Nonsteroidal anti-inflammatory drugs for managing postoperative endodontic pain in patients who present with preoperative pain: a systematic review and meta-analysis. J Endod. 2017;43(1):7–15. doi:10.1016/j.joen.2016.09.010
4. Mitragotri S. Breaking the skin barrier. Adv Drug Deliv Rev. 2004;5(56):555–556. doi:10.1016/j.addr.2003.10.022
5. Mathews L, Roy A. Management of pain using transdermal patches-a review. Asian J Pharm Clin Res. 2016;9(6):32–35. doi:10.22159/ajpcr.2016.v9i6.13775
6. Musu M, Finco G, Antonucci R, et al. Acute nephrotoxicity of NSAID from the foetus to the adult. Eur Rev Med Pharmacol Sci. 2011;15(12):1461–1472.
7. Zadsirjan S, Toghrolian A, Zargar N, Nuvvula S. Analgesic efficacy of ketoprofen transdermal patch versus ibuprofen oral tablet on postendodontic pain in patients with irreversible pulpitis: a randomized clinical trial. Pain Res Manag. 2023;2023:1–10. doi:10.1155/2023/8549655
8. Guilherme VA, Ribeiro LN, Tofoli GR, Franz-Montan M, de Paula E, de Jesus MB. Current challenges and future of lipid nanoparticles formulations for topical drug application to oral mucosa, skin, and eye. Curr Pharma Des. 2017;23(43):6659–6675. doi:10.2174/1381612823666171122103849
9. Zaid Alkilani A, McCrudden MT, Donnelly RF. Transdermal drug delivery: innovative pharmaceutical developments based on disruption of the barrier properties of the stratum corneum. Pharmaceutics. 2015;7(4):438–470. doi:10.3390/pharmaceutics7040438
10. Jeong WY, Kwon M, Choi HE, Kim KS. Recent advances in transdermal drug delivery systems: a review. Biomater Res. 2021;25(1):1–5. doi:10.1186/s40824-021-00226-6
11. Gazal G, Al-Samadani KH. Comparison of paracetamol, ibuprofen, and diclofenac potassium for pain relief following dental extractions and deep cavity preparations. Saudi Med J. 2017;38(3):284–291. doi:10.15537/smj.2017.3.16023
12. Dheeraj M, Johar S, Mahajan P, Jandial T, Chauhan S, Gupta K. Comparative evaluation of the efficacy of two modes of delivery of diclofenac for the management of post-endodontic pain: a randomized controlled clinical trial. J Pharm Biol Sci. 2023;15(6):1283–1286. doi:10.4103/jpbs.jpbs_119_23
13. Saklad M. Grading of patients for surgical procedures. Anesthesiology. 1941;2(3):281–284. doi:10.1097/00000542-194105000-00004
14. Trope M, Delano EO, Orstavik D. Endodontic treatment of teeth with apical periodontitis: single vs. multivisit treatment. J Endod. 1999;25(5):345–350. doi:10.1016/S0099-2399(06)81169-6
15. Vera J, Siqueira JF, Ricucci D, et al. One- versus two-visit endodontic treatment of teeth with apical periodontitis: a histobacteriologic study. J Endod. 2012;38(8):1040–1052. doi:10.1016/j.joen.2012.04.010
16. Ørstavik D, Kerekes K, Eriksen HM. The periapical index: a scoring system for radiographic assessment of apical periodontitis. Dental Traumatol. 1986;2(1):20–34. doi:10.1111/j.1600-9657.1986.tb00119.x
17. Mangal S, Mathew S, Murthy BS, Hegde S, Dinesh K, Ramesh P. The efficacy of transdermal and oral diclofenac for post-endodontic pain control: a randomised controlled trial. Ind J Dent Res. 2020;31(1):53–56. doi:10.4103/ijdr.IJDR_167_17
18. Murugan B, Kumar SA, Krishnappan Srinivasan NA, Kumar EP, Lakshmi N. A randomized clinical trial on oral and transdermal diclofenac on controlling postoperative endodontic pain. Group. 2022;1(3.70):0–67.
19. Bhargava D, Thomas S, Beena S. Comparison between efficacy of transdermal ketoprofen and diclofenac patch in patients undergoing therapeutic extraction—a randomized prospective split mouth study. J Maxillofac Surg. 2019;77(10):1998–2003. doi:10.1016/j.joms.2019.04.007
20. Krishna R, Nataraj MS. Efficacy of a single dose of a transdermal diclofenac patch as pre-emptive postoperative analgesia: a comparison with intramuscular diclofenac. South Afr J Anaesth Analg. 2012;18(4):194–197. doi:10.1080/22201173.2012.10872852
21. Mason L, Moore RA, Edwards JE, Derry S, McQuay HJ. Topical NSAIDs for chronic musculoskeletal pain: systematic review and meta-analysis. BMC Musculoskelet Disord. 2004;5(1):1–8. doi:10.1186/1471-2474-5-28
22. Esparza F, Cobián C, Jiménez JF, García-Cota JJ, Sánchez C, Maestro A; Working group for the acute pain study of SETRADE. Topical ketoprofen TDS patch versus diclofenac gel: efficacy and tolerability in benign sport related soft-tissue injuries. Br J Sports Med. 2007;41(3):134–139. doi:10.1136/bjsm.2006.030239
23. Moore N, Pollack C, Butkerait P. Adverse drug reactions and drug–drug interactions with over-the-counter NSAIDs. Ther Clin Risk Manag. 2015;11:1061–1075. doi:10.2147/TCRM.S79135
24. Park H, Otte A, Park K. Evolution of drug delivery systems: from 1950 to 2020 and beyond. J Control Release. 2022;342:53–65. doi:10.1016/j.jconrel.2021.12.030
25. Al Hanbali OA, Khan HM, Sarfraz M, Arafat M, Ijaz S, Hameed A. Transdermal patches: design and current approaches to painless drug delivery. Acta Pharmaceutica. 2019;69(2):197–215. doi:10.2478/acph-2019-0016
26. Agarwal A, Dhiraaj S, Kumar A, Singhal V, Singh U. Evaluation of a diclofenac transdermal patch for the attenuation of venous cannulation pain: a prospective, randomised, double‐blind, placebo‐controlled study. Anaesthesia. 2006;61(4):360–362. doi:10.1111/j.1365-2044.2006.04538.x
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.