Back to Journals » Cancer Management and Research » Volume 18

Comparative Efficacy of Fosnetupitant and Fosaprepitant for Delayed Vomiting in Patients Receiving Irinotecan-Oxaliplatin Combination Chemotherapy: A Retrospective Propensity Score-Matched Study
Authors Maeda K ![]() , Kawada K, Hayashi T
, Kawada K, Hayashi T ![]() , Koyama S, Ishida T, Yoshioka T, Fukuda H, Horikawa I, Aizawa F, Niimura T, Yagi K, Goda M, Izawa-Ishizawa Y
, Koyama S, Ishida T, Yoshioka T, Fukuda H, Horikawa I, Aizawa F, Niimura T, Yagi K, Goda M, Izawa-Ishizawa Y ![]() , Ishizawa K
, Ishizawa K ![]()
Received 28 November 2025
Accepted for publication 1 May 2026
Published 4 June 2026 Volume 2026:18 579955
DOI https://doi.org/10.2147/CMAR.S579955
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Yong Teng
Kazuki Maeda,1,2 Kei Kawada,1,3 Toshinobu Hayashi,4 Sota Koyama,5 Tomoaki Ishida,6 Toshihiko Yoshioka,3 Hitoshi Fukuda,7 Io Horikawa,1,3 Fuka Aizawa,1,2 Takahiro Niimura,1,2 Kenta Yagi,8 Mitsuhiro Goda,9 Yuki Izawa-Ishizawa,10 Keisuke Ishizawa1– 3
1Department of Clinical Pharmacology and Therapeutics, Tokushima University Graduate School of Biomedical Sciences, Tokushima, Japan; 2Clinical Research Center for Developmental Therapeutics, Tokushima University Hospital, Tokushima, Japan; 3Department of Pharmacy, Tokushima University Hospital, Tokushima, Japan; 4Department of Pharmaceutical Sciences for Health Crisis Management, Faculty of Pharmaceutical Sciences, Fukuoka University, Fukuoka, Japan; 5Department of Clinical Pharmacy Practice Pedagogy, Tokushima University Graduate School of Biomedical Sciences, Tokushima, Japan; 6Department of Clinical Pharmacy, Nagoya City University Graduate School of Pharmaceutical Sciences, Nagoya, Japan; 7Department of Neurosurgery, Kochi Medical School, Kochi University, Kochi, Japan; 8Department of Pharmacy, Shimane University Hospital, Shimane, Japan; 9Department of Clinical Pharmacology and Therapeutics, Graduate School of Biomedical and Health Sciences, Hiroshima University, Hiroshima, Japan; 10Department of Health and Nutrition, Faculty of Human Life Science, Shikoku University, Tokushima, Japan
Correspondence: Kei Kawada, Department of Clinical Pharmacology and Therapeutics, Tokushima University Graduate School of Biomedical Sciences, 15-18-3 Kuramoto, Tokushima, 770-8503, Japan, Tel +81886337562, Email [email protected]
Purpose: Appropriate prevention of chemotherapy-induced nausea and vomiting (CINV) is essential for improving patients’ quality of life; however, no studies have compared neurokinin-1 receptor antagonists in regimens combining oxaliplatin and irinotecan. We aimed to compare the antiemetic efficacy of fosnetupitant and fosaprepitant in patients receiving FOLFIRINOX or FOLFOXIRI regimens.
Patients and Methods: We reviewed records of patients receiving FOLFIRINOX or FOLFOXIRI between April 1, 2018 and September 30, 2024 at Tokushima University Hospital. Eligible patients completed the first chemotherapy cycle, received standard triple antiemetic prophylaxis, and had complete nursing-recorded CINV follow-up data for days 1– 7. Patients were matched 1:1 using propensity scores for age, sex, alcohol consumption history, prior treatment, regimen, and chemotherapy doses. The primary objective was to compare the incidence of vomiting during the long-delayed phase (days 6– 7) between the fosnetupitant and fosaprepitant groups. The no-vomiting and no-nausea rates were compared using Fisher’s exact test, and the time to first vomiting using the Log rank test.
Results: After matching, data from 68 balanced patient pairs were analyzed. The fosnetupitant group had higher no-vomiting rates in the long-delayed phase (100% vs. 91.2%, p=0.028) and overall period (95.6% vs. 83.8%, p=0.045), compared with the fosaprepitant group. No significant intergroup difference was observed in the overall no-nausea rate (26.5% vs. 32.3%, p=0.573). With fosnetupitant, the time to first vomiting was longer (3/68 vs. 11/68, hazard ratio: 0.20, p=0.045), injection site reactions were fewer (0.0% vs. 19.1%, p< 0.001), and constipation and hiccup incidences were fewer (p> 0.05).
Conclusion: Despite the retrospective design, possible calendar-time confounding, and limited number of events, our results suggest that fosnetupitant offers better control of long-delayed and overall vomiting and a favorable safety profile, compared with fosaprepitant, in patients receiving FOLFIRINOX/FOLFOXIRI regimens. Infographic: Fosnetupitant vs. Fosaprepitant for vomiting prevention in FOLFIRINOX/FOLFOXIRI patients.Patients receiving FOLFIRINOX or FOLFOXIRI are shown. Propensity score-matched pairs (68 pairs) compare Fosnetupitant versus Fosaprepitant. Long-delayed vomiting (Days 6-7) results show 100 percent no vomiting with Fosnetupitant and 91.2 percent no vomiting with Fosaprepitant. The hazard ratio (HR) is 0.20 (0.05-0.56), Firth corrected. Firth’s penalized Cox regression analysis is mentioned.
Keywords: antiemetics, chemotherapy-induced nausea and vomiting, FOLFIRINOX, FOLFOXIRI, moderate emetogenic chemotherapy
Introduction
Chemotherapy-induced nausea and vomiting (CINV) is a distressing adverse effect that impairs patients’ quality of life and limits adherence to therapy.1,2 Based on emetogenic risk, anticancer agents are categorized into highly emetogenic chemotherapy (HEC) and moderately emetogenic chemotherapy (MEC) regimens.3–6 Oxaliplatin and irinotecan are classified as MEC agents according to major international guidelines, including those of the American Society of Clinical Oncology (ASCO), Multinational Association of Supportive Care in Cancer/European Society for Medical Oncology (MASCC/ESMO), National Comprehensive Cancer Network (NCCN), and Japan Society of Clinical Oncology (JSCO).3–6 FOLFOXIRI and FOLFIRINOX regimens consist of three key chemotherapeutic agents commonly used in gastrointestinal cancers, namely, oxaliplatin, irinotecan, and 5-fluorouracil combined with leucovorin. These regimens are widely used in treating colorectal and pancreatic cancers, often in combination with molecular targeted agents. Although FOLFOXIRI and FOLFIRINOX are effective treatment options, they have also been reported to be associated with a higher incidence of CINV, compared with other anticancer agents classified as MEC.3–6 Moreover, owing to the prolonged emetogenic effect of these regimens, CINV often persists into the delayed phase.7 Although each component drug of these regimens is classified as MEC in the ASCO, MASCC/ESMO, NCCN and JSCO guidelines, their combination regimens are categorized as HEC in the JSCO guidelines.3 In HEC settings, guideline-concordant prophylaxis requires a three-drug regimen including a neurokinin-1 (NK1) receptor antagonist (RA), a serotonin type 3 (5-HT3) RA, and dexamethasone, with extended dexamethasone administration during the delayed phase. In contrast, for MEC, the use of an NK1-RA may be optional, depending on patient-related risk factors, and the duration of dexamethasone is often shorter. Therefore, how FOLFIRINOX and FOLFOXIRI are classified directly influences the indication for NK1-RA use and the optimal duration of dexamethasone, particularly in the delayed and long-delayed phases of CINV control. This wide variability complicates the establishment of prophylactic recommendations applicable to all anticancer agents classified as MEC.
Fosaprepitant, an NK1-RA, is a prodrug of aprepitant and is typically administered at a dose of 150 mg. In contrast, fosnetupitant is a prodrug of netupitant and is administered at a dose of 235 mg. Although both agents exert their antiemetic effects by blocking the NK1 receptor, mediated by substance P, they differ in their pharmacokinetic profiles, particularly in the half-life of their active metabolites. Aprepitant has a relatively short half-life of approximately 14 hours, whereas netupitant has a substantially longer half-life of approximately 70 hours. Fosnetupitant, a long-acting NK1-RA, has shown superior efficacy over fosaprepitant in controlling long-delayed CINV in cisplatin-based chemotherapy.8,9 However, prophylactic antiemetic strategies for FOLFIRINOX or FOLFOXIRI regimens are not standardized across international guidelines, and the comparative efficacy of fosaprepitant and fosnetupitant in this context has not been thoroughly investigated. Although prophylactic antiemetic therapy has led to marked improvements in the control of acute and delayed CINV, long-delayed CINV remains a clinical challenge. Failure to adequately manage CINV in this phase may negatively impact treatment adherence and continuation in subsequent chemotherapy cycles.
To address this knowledge gap, we aimed to compare the antiemetic efficacy of fosnetupitant and fosaprepitant in patients receiving FOLFIRINOX or FOLFOXIRI regimens using a propensity score-matched analysis in a real-world setting.
Materials and Methods
Study Design and Setting
This single-center, retrospective observational study was conducted at Tokushima University Hospital, Japan, between April 1, 2018, and September 30, 2024. Given that our institution includes both gastroenterology and gastrointestinal surgery departments, we anticipated sufficient case accrual for the study.
Ethical Considerations
The study protocol was approved by the Ethics Committee of Tokushima University Hospital (Approval No. 4633) and was conducted in accordance with the Ethical Guidelines for Medical and Biological Research Involving Human Subjects issued by the Japanese Ministry of Health, Labour and Welfare10 and the Declaration of Helsinki.11 Given the retrospective observational design of this study, the requirement for written informed consent was waived by the Ethics Committee. Instead, an opt-out approach was implemented by disclosing study information on the Tokushima University Hospital website prior to study commencement, thereby providing patients with the opportunity to decline participation.
Study Population
The study included patients who met the following criteria and received FOLFOXIRI for the treatment of colorectal cancer or FOLFIRINOX for the treatment of pancreatic cancer: 1) completed the first cycle of chemotherapy (the analysis was performed on a per-patient basis; the analysis was restricted to the first chemotherapy cycle to minimize the influence of prior-cycle nausea and vomiting and subsequent dose adjustments of anticancer agents or prophylactic antiemetic therapy); 2) received prophylactic antiemetic therapy, consisting of an NK1-RA, a 5-HT3RA, and dexamethasone; and 3) complete CINV follow-up records from days 1–7 after chemotherapy being available in the nursing records included in the electronic medical records. At our institution, the first treatment cycle is, in principle, conducted in an inpatient setting irrespective of the patient’s clinical status; therefore, hospitalized patients were included in this study. In the present study, the evaluation period was defined as days 1–7, and no additional monitoring was performed until the initiation of the subsequent chemotherapy cycle. Eligible patients were identified through electronic medical records based on injection records of oxaliplatin, irinotecan, fosaprepitant, or fosnetupitant.
Sample Size and Sampling
A total of 190 eligible patients who received FOLFOXIRI or FOLFIRINOX at Tokushima University Hospital between April 1, 2018 and September 30, 2024 were included in the study. The sample size was determined based on the number of consecutive, eligible patients available during the study period.
Study Procedures
Modified FOLFOXIRI and modified FOLFIRINOX were administered at identical doses (oxaliplatin, 85 mg/m2; irinotecan, 150 mg/m2; leucovorin, 200 mg/m2; and 5-fluorouracil, 2400 mg/m2, as a continuous infusion without a bolus) according to institutional standards. All patients received a standardized antiemetic regimen consisting of palonosetron (0.75 mg), dexamethasone (9.9 mg, 6.6 mg, or 3.3 mg), and either fosaprepitant (150 mg) or fosnetupitant (235 mg).3–6 In the fosaprepitant group, fosaprepitant was diluted in 250 mL of normal saline and administered intravenously at 500 mL/h, starting 60 minutes before chemotherapy and completed 30 minutes prior to chemotherapy. Subsequently, palonosetron and dexamethasone diluted in 100 mL of normal saline were administered intravenously at 200 mL/h until immediately before chemotherapy. In the fosnetupitant group, fosnetupitant was diluted in 100 mL of normal saline and administered intravenously at a rate of 200 mL/h, starting 30 minutes before chemotherapy, together with palonosetron and dexamethasone.
All included patients received prophylactic antiemetic therapy and chemotherapy in accordance with the predefined regimens, and thus adherence-related concerns were unlikely. The palonosetron dose of 0.75 mg represents the approved and routinely used standard dose in Japanese clinical practice at the time of the study.12 The dexamethasone dosage was predetermined according to each regimen: 6.6 mg for FOLFOXIRI and 9.9 mg for FOLFIRINOX. A dose reduction to 3.3 mg was implemented in one patient; however, the reason for this adjustment was not documented in the medical records. Beyond day 1, dexamethasone was not incorporated into the regimen as part of prophylactic antiemetic therapy but was used in the same manner as other rescue medications, according to patients’ symptoms. In addition to dexamethasone, dopamine receptor antagonists, such as metoclopramide and prochlorperazine, were used as rescue antiemetics, and olanzapine was also administered based on the physicians’ clinical judgment.
Data Collection
Data on the following variables were retrospectively obtained from electronic medical records: demographic characteristics (age, sex, history of alcohol consumption, and smoking history), doses of oxaliplatin and irinotecan, cancer type, chemotherapy regimen, prior treatment history, antiemetic agents used and their doses, the presence of nausea, presence of vomiting, time to onset of vomiting, and adverse events (injection site reactions [ISRs], constipation, and hiccups). Nausea was assessed using daily nursing records based on patient-reported symptoms documented in the electronic medical records, regardless of severity. In routine inpatient practice at our institution, nursing assessments are conducted at least three times a day, and additional evaluations are performed as needed, in response to patients’ symptoms. Vomiting was defined as any documented emetic episode.
Rescue antiemetic use was not included as an outcome because, in routine clinical practice, it is often administered as a part of patient management, and its accurate and consistent capture is difficult in a retrospective review of electronic medical records. Therefore, instead of using the standard CINV endpoint of a complete response (defined as no emesis and no rescue medication use), we adopted single-outcome definitions of “no nausea” and “no vomiting.”
ISRs were defined as the presence of any symptoms at the infusion site, including pain, erythema, swelling, induration, or phlebitis. They were assessed during infusion and within 24 hours of drug administration, and cases were identified from nursing free-text notes in the electronic medical records. ISRs were graded according to the Common Terminology Criteria for Adverse Events (CTCAE) version 5.0. Owing to the retrospective nature of the study, we could not definitively determine whether ISRs were caused by the study drug.
Outcomes
Efficacy Endpoints
The primary endpoint was predefined as the proportion of patients with no vomiting during the long-delayed phase (days 6–7), based on prior evidence suggesting that emesis associated with platinum-based combination chemotherapy may extend beyond day 5.8,9 The secondary endpoints were the proportions of patients with no vomiting during the acute phase (day 1), delayed phase (days 2–5), and overall period (days 1–7), as well as those of patients with no nausea during the acute phase (day 1), delayed phase (days 2–5), long-delayed phase (days 6–7), and overall period (days 1–7) and the time to the first vomiting episode.
Safety Endpoints
Secondary (safety) endpoints were the incidence of ISR, constipation, and hiccups from days 1–7.13
Statistical Analysis
Propensity Score Matching
Propensity scores were estimated using a logistic regression model to mitigate the effect of cofounders and enhance comparability effects. Accordingly, 1:1 propensity score matching was used. Covariates included in the propensity score model were age, sex, history of alcohol consumption, prior chemotherapy, regimen, and administered doses of oxaliplatin and irinotecan. Matching was performed using the nearest-neighbor method with a caliper width of 0.2 standard deviations of the logit of the propensity score.
Comparative Analyses
Comparative analyses were conducted to evaluate the differences between the fosnetupitant and fosaprepitant groups. Categorical variables, such as the no-vomiting rate and incidence of ISRs, were compared using Fisher’s exact test. Continuous variables, including age, were analyzed using the Mann–Whitney U-test. For the primary binary outcome, the risk difference between groups was calculated with corresponding 95% confidence intervals (CIs). The time to first vomiting was assessed using Kaplan–Meier survival analysis and compared between the groups using the Log rank test.14 Because of the small number of vomiting events, a Cox proportional-hazards model with Firth’s penalized likelihood correction was applied to reduce small-sample bias and the potential overestimation of treatment effects. In this model, the time to first vomiting was specified as the dependent variable and the treatment group (fosnetupitant vs. fosaprepitant) as the independent variable. The hazard ratios (HRs) and 95% CIs were estimated accordingly.15 The proportional-hazards assumption was not grossly violated upon graphical assessment. All statistical analyses were performed using EZR (version 1.68), a graphical user interface for R designed for medical statistics.16 A two-sided p-value <0.05 was considered statistically significant.
Results
Participant Selection
Following propensity score matching, 68 matched pairs (136 patients) were included in the analysis (Table 1). Baseline characteristics, including age, sex, history of alcohol consumption, prior chemotherapy exposure, and administered doses of oxaliplatin and irinotecan, were confirmed to be well-balanced between the two groups.
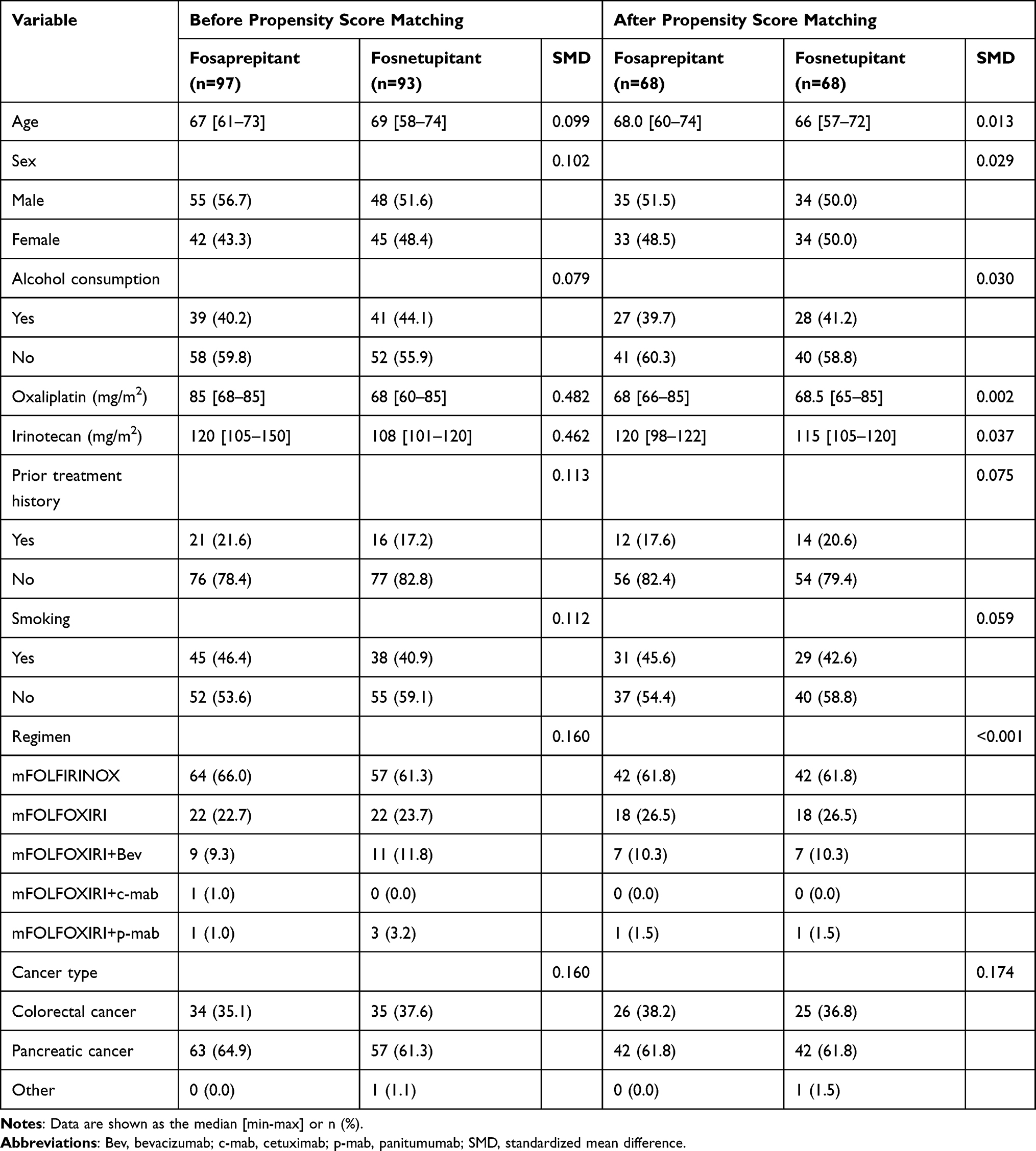 |
Table 1 Baseline Characteristics of the Study Participants |
Efficacy: Incidence of No Vomiting and No Nausea
After matching, the incidence of no vomiting during the long-delayed phase (days 6–7) was significantly higher in the fosnetupitant group (100%) than in the fosaprepitant group (91.2%) (p = 0.028), with a risk difference of 8.8% (95% CI, 2.1% to 15.6%). Over the entire study period (days 1–7), the no-vomiting rate was significantly higher in the fosnetupitant group than in the fosaprepitant group (95.6% vs. 83.8%, p = 0.045) (Table 2), corresponding to a risk difference of 11.8% (95% CI, 1.7% to 21.8%). Although the acute no-nausea rate was lower in the fosaprepitant group than in the fosnetupitant group, the long-delayed and overall no-nausea rates were higher in the fosaprepitant group; however, none of these differences were significant (Table 3).
 |
Table 2 No-Vomiting Rate in the Fosnetupitant and Fosaprepitant Groups |
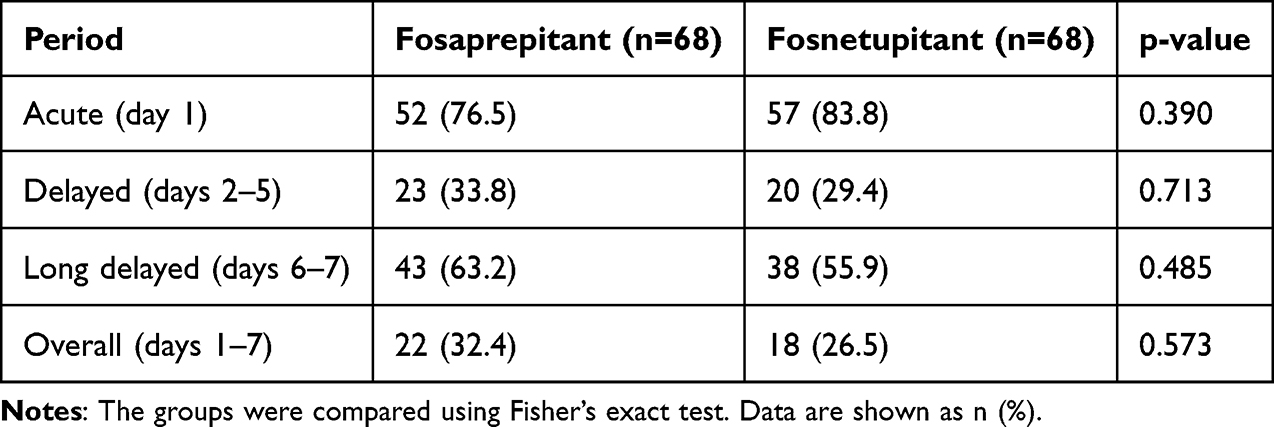 |
Table 3 No-Nausea Rate in the Fosnetupitant and Fosaprepitant Groups |
Time to First Vomiting Episode
The time to the first vomiting episode was significantly longer in the fosnetupitant group than in the fosaprepitant group (3/68 vs. 11/68, p = 0.045). In the Firth-corrected Cox model, the HR for vomiting in the fosnetupitant group compared with that in the fosaprepitant group was 0.20 (95% CI, 0.05–0.56) (Figure 1). Because of the small number of vomiting events, the median time to first vomiting could not be estimated in either group. During the 7-day observation period, vomiting occurred in 4.4% and 16.2% of patients in the fosnetupitant and fosaprepitant groups, respectively.
 |
Figure 1 Time to vomiting occurrence. Kaplan–Meier curves comparing the fosaprepitant and fosnetupitant groups. The hazard ratios (HRs) and 95% confidence intervals (CIs) were estimated using a Firth penalized Cox proportional-hazards model, and the differences between the groups were assessed using the Log rank test. Numbers below the plot indicate the cumulative number of vomiting events at each time point. The plus (+) symbols indicate censored observations (i.e., patients without events at the last follow-up) in each group. |
Safety Profile
In the safety evaluation, the incidence of ISRs was significantly lower in the fosnetupitant group than in the fosaprepitant group (0.0% vs. 19.1%, p<0.001), corresponding to a risk difference of −19.1% (95% CI, −28.5% to −0.1%). All ISR events were of grades 1 or 2, and no grade 3 or higher events were observed. The incidences of constipation and hiccups were lower in the fosnetupitant group than in the fosaprepitant group; however, these differences were not significant (Table 4).
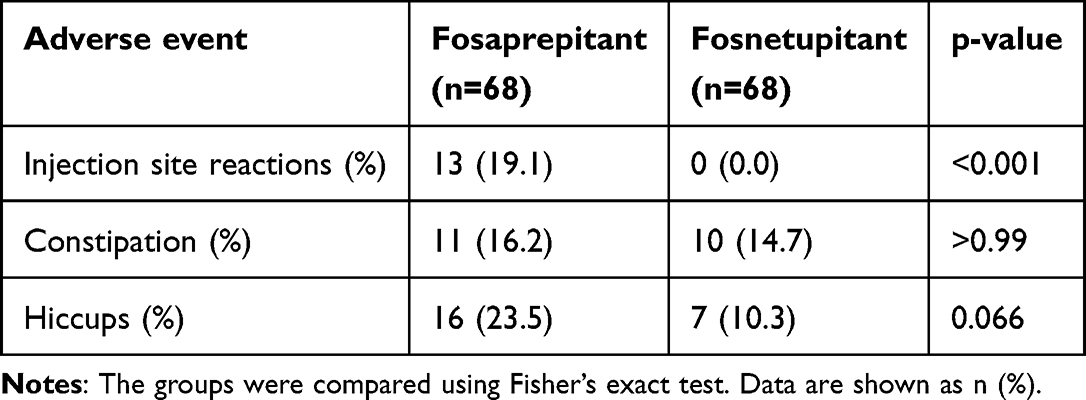 |
Table 4 Incidence of Adverse Events in the Fosnetupitant and Fosaprepitant Groups |
Discussion
In this single-center, retrospective propensity score-matched study, we compared the antiemetic efficacy and safety of fosnetupitant and fosaprepitant in patients receiving FOLFIRINOX or FOLFOXIRI regimens. Although these regimens are generally classified as MEC, they are frequently associated with a high emetogenic risk.3–6 Consequently, inconsistencies in MEC/HEC classification have been reported, with differing recommendations among the ASCO, NCCN, JSCO, and MASCC/ESMO guidelines.17 Our findings demonstrated that fosnetupitant was associated with a lower incidence of delayed vomiting (particularly in the long-delayed phase [days 6–7]) and ISRs, compared with fosaprepitant. Collectively, these results suggest that fosnetupitant may offer improved control of vomiting during the long-delayed and overall phases, with a potentially more favorable safety profile in the context of FOLFIRINOX or FOLFOXIRI treatment.
Both fosnetupitant and fosaprepitant exert antiemetic effects via inhibition of NK1 receptors, mediated by substance P. The observed differences in long-delayed efficacy may be partly attributable to pharmacokinetic differences between their active metabolites. Aprepitant, the active metabolite of fosaprepitant, has a half-life of approximately 14 hours, whereas netupitant, the active metabolite of fosnetupitant, has a substantially longer half-life of approximately 70 hours.9,18–20 This prolonged exposure may contribute to sustained antiemetic effects in multi-day emetogenic regimens, such as FOLFIRINOX and FOLFOXIRI. Nevertheless, given the observational design of this study, alternative explanations—including temporal changes in clinical practice patterns and documentation—cannot be excluded. No significant difference in the nausea incidence was observed between the two groups, whereas vomiting was significantly lower with the use of fosnetupitant. This finding is consistent with the known pharmacologic profile of NK1-RAs, which tend to exert stronger effects on vomiting than on nausea.21–23
In this study, all patients received palonosetron at the approved Japanese dose of 0.75 mg, consistent with standard clinical practice.12,24 Although the recommended dose in international guidelines is 0.25 mg, similar efficacy between the two doses has been reported.25
The sustained suppression of vomiting by fosnetupitant observed in the long-delayed phase in this study is consistent with the findings of previous studies on cisplatin-based HEC regimens.8,9,21 Triplet antiemetic prophylaxis with a 5-HT3RA, dexamethasone, and an NK1-RA is beneficial in cisplatin-based HEC or FOLFIRINOX contexts. For instance, Hishida-Sadaka et al7 reported that triple antiemetic therapy was effective in reducing delayed-phase CINV in patients undergoing FOLFIRINOX for pancreatic cancer, although they did not directly compare the NK1-RA types Additionally, Inano et al8 and Inui et al9 demonstrated the association between lower delayed-phase CINV and fosnetupitant compared with fosaprepitant or aprepitant in cisplatin-based chemotherapy Our findings build upon those observations by demonstrating that fosnetupitant may also provide enhanced protection in oxaliplatin-irinotecan combination regimens, especially in the long-delayed phase, which is typically underrepresented in conventional CINV trials that are focused only on to the first 120 hours after chemotherapy.26
From a safety perspective, ISRs occurred more frequently in the fosaprepitant group than those in the fosnetupitant group in this study, a trend also reported previously.27 Although oral NK1-RAs may avoid concerns about ISRs, intravenous administration offers notable clinical advantages, given that other antiemetics are administered intravenously simultaneously and that CINV may compromise oral intake.28–30 Investigating optimal prophylactic antiemetic strategies for FOLFOXIRI and FOLFIRINOX regimens is important, as primary prophylaxis may be effective against refractory and anticipatory CINV, and it may also affect the maintenance of the chemotherapy dose intensity in patients with gastrointestinal cancers.31,32
Our findings have clinically significant implications, as they demonstrate the comparative efficacy of fosnetupitant versus fosaprepitant in the context of FOLFOXIRI or FOLFIRINOX regimens via propensity score matching, thereby addressing a critical gap in the current antiemetic literature. However, they should be interpreted in light of some study limitations. First, its retrospective nature potentially introduced biases owing to documentation variability and the reliance on clinician-recorded CINV events. Second, although propensity score matching balanced the observed confounders, unmeasured variables, including psychological distress or dietary factors, might still have affected the outcomes. Third, nausea, being inherently subjective, was not quantitatively assessed using validated patient-reported outcome measures, which limits the interpretability of nausea-related endpoints. In addition, because rescue antiemetic use was not systematically captured, complete responses (defined as no emesis and no rescue medication use) could not be evaluated. Therefore, the present findings cannot be directly compared with those of randomized controlled trials in which a complete response was the primary endpoint. Furthermore, the single-center, retrospective design of the study may limit the generalizability of the findings, as institutional treatment protocols, documentation quality, and patient characteristics may differ across centers. Therefore, prospective, multicenter studies are needed to confirm the reproducibility of these findings and enhance their generalizability across diverse clinical settings. Fourth, the number of vomiting events was limited, which may have reduced statistical power. Although a Firth-corrected Cox proportional-hazards model was applied to mitigate small-sample bias, the limited number of events warrants cautious interpretation of the stability and precision of the HR estimates. Fifth, the propensity score model did not incorporate several potential confounders related to CINV, including a history of motion sickness, prior CINV, baseline anxiety, opioid use, baseline constipation, access to rescue antiemetics, performance status, and kidney and liver function. Sixth, because fosnetupitant was introduced later in the study period, temporal changes in supportive care practices or antiemetic management strategies may have influenced the observed differences. Therefore, the present findings could not establish causality, and the observed differences may partly reflect temporal changes in supportive care practices or documentation patterns rather than intrinsic differences between the two NK1-RAs. In addition, secondary endpoints were not adjusted for multiplicity and should therefore be interpreted as exploratory. The findings from the secondary analyses require confirmation in adequately powered prospective studies.
Conclusion
Fosnetupitant was associated with a lower incidence of long-delayed vomiting and fewer ISRs, compared with fosaprepitant, in patients receiving FOLFIRINOX or FOLFOXIRI regimens. Given its pharmacologic profile and clinical benefits, fosnetupitant is a promising NK1-RA in FOLFIRINOX or FOLFOXIRI regimens. The findings of this study support the optimization of antiemetic prophylaxis in such regimens. Nausea and rescue medication use are difficult to accurately capture in retrospective studies. Therefore, prospective studies in which patient diaries or the patient-reported outcomes version of the CTCAE, with a complete response as the endpoint, are used are warranted to validate these findings and guide future antiemetic strategies.
Abbreviations
5-HT3, serotonin type 3; ASCO, American Society of Clinical Oncology; CI, confidence interval; CINV, chemotherapy-induced nausea and vomiting; CTCAE, Common Terminology Criteria for Adverse Events; ESMO, European Society for Medical Oncology; HEC, high emetogenic chemotherapy; HR, hazard ratio; ISR, injection site reaction; JSCO, Japan Society of Clinical Oncology; MASCC, Multinational Association of Supportive Care in Cancer; MEC, moderate emetogenic chemotherapy; NCCN, National Comprehensive Cancer Network; NK1-RA, neurokinin-1 receptor antagonist.
Data Sharing Statement
The data analyzed in this study can be obtained from the corresponding author upon reasonable request.
Acknowledgments
We sincerely thank all the members of the Department of Clinical Pharmacology and Therapeutics, Graduate School of Biomedical Sciences, Tokushima University for their kind support and helpful contributions to this research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors declare that no funds, grants, or other support were received for this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Gupta K, Walton R, Kataria SP. Chemotherapy-induced nausea and vomiting: pathogenesis, recommendations, and new trends. Cancer Treat Res Commun. 2021;26:100278. doi:10.1016/j.ctarc.2020.100278
2. Hesketh PJ. Chemotherapy-induced nausea and vomiting. N Engl J Med. 2008;358(23):2482–11. doi:10.1056/NEJMra0706547
3. Japanese Society of Clinical Oncology (JSCO) Antiemetic Guidelines; 2023. Available from: http://www.jsco-cpg.jp/antiemetic-therapy/.
4. Herrstedt J, Clark-Snow R, Ruhlmann CH, et al. MASCC and ESMO guideline update for the prevention of chemotherapy- and radiotherapy-induced nausea and vomiting. ESMO Open. 2024;9(2):102195. doi:10.1016/j.esmoop.2023.102195
5. Hesketh PJ, Kris MG, Basch E, et al. Antiemetics: ASCO guideline update. J Clin Oncol. 2020;38(24):2782–2797.
6. NCCN clinical practice guidelines in oncology: antiemesis. ver2.2025. Available from: https://www.nccn.org/login.
7. Hishida-Sadaka S, Iihara H, Ohata K, et al. Efficacy and safety of 5HT3RA, DEX, and NK1RA for the prevention of FOLFIRINOX-induced nausea and vomiting in patients with pancreatic cancer: a retrospective cohort study. Support Care Cancer. 2023;31(12):657.
8. Inano H, Morimoto Y, Kitagawa K, et al. Comparing the efficacy of fosnetupitant, an NK1 receptor antagonist in CDDP-based regimens, with that of fosaprepitant and aprepitant: a retrospective observational study. Biol Pharm Bull. 2024;47(3):692–697. doi:10.1248/bpb.b23-00819
9. Inui N, Toi Y, Yoneshima Y, et al. Pooled analysis of studies evaluating fosnetupitant and risk factors for cisplatin-induced nausea and vomiting during the extended overall phase. Adv Ther. 2023;40(11):4928–4944. doi:10.1007/s12325-023-02648-1
10. Japanese Ministry of Health. Labour and welfare. ethical guidelines for medical and biological research involving human subjects; 2021. Available at: Available from: https://www.mhlw.go.jp.
11. World Medical Association. World medical association declaration of helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194. doi:10.1001/jama.2013.281053
12. Segawa Y, Aogi K, Inoue K, et al. A Phase II dose-ranging study of palonosetron in Japanese patients receiving moderately emetogenic chemotherapy, including anthracycline and cyclophosphamide-based chemotherapy. Ann Oncol. 2009;20(11):1874–1880. doi:10.1093/annonc/mdp243
13. Navari RM, Aapro M. Antiemetic prophylaxis for chemotherapy-induced nausea and vomiting. N Engl J Med. 2016;374(14):1356–1367. doi:10.1056/NEJMra1515442
14. Kaplan EL, Meier P. Nonparametric estimation from incomplete observations. J Am Stat Assoc. 1958;53(282):457–481. doi:10.1080/01621459.1958.10501452
15. Heinze G, Schemper M. A solution to the problem of monotone likelihood in Cox regression. Biometrics. 2001;57(1):114–119. doi:10.1111/j.0006-341X.2001.00114.x
16. Kanda Y. Investigation of the freely available easy-to-use software “EZR” for medical statistics. Bone Marrow Transplant. 2013;48(3):452–458. doi:10.1038/bmt.2012.244
17. Razvi Y, Chan S, McFarlane T, et al. ASCO, NCCN, MASCC/ESMO: a comparison of antiemetic guidelines for the treatment of chemotherapy-induced nausea and vomiting in adult patients. Support Care Cancer. 2019;27(1):87–95. doi:10.1007/s00520-018-4464-y
18. Pharmaceuticals and Medical Devices Agency (PMDA) for searching drug information in Japan (Fosaprepitant). Available from: https://www.info.pmda.go.jp/go/pack/2391405D1039_1_01/?view=frame&style=XML&lang=ja.
19. Pharmaceuticals and Medical Devices Agency (PMDA) for searching drug information in Japan (Fosnetupitant). Available from: https://www.info.pmda.go.jp/go/pack/2391406A1029_1_02/?view=frame&style=XML&lang=ja.
20. Spinelli T, Calcagnile S, Giuliano C, et al. Netupitant PET imaging and ADME studies in humans. J Clin Pharmacol. 2014;54(1):97–108. doi:10.1002/jcph.198
21. Hata A, Okamoto I, Inui N, et al. Randomized, double-blind, Phase III study of fosnetupitant versus fosaprepitant for prevention of highly emetogenic chemotherapy-induced nausea and vomiting: CONSOLE. J Clin Oncol. 2022;40(2):180–188. doi:10.1200/JCO.21.01315
22. Saito H, Yoshizawa H, Yoshimori K, et al. Efficacy and safety of single-dose fosaprepitant in the prevention of chemotherapy-induced nausea and vomiting in patients receiving high-dose cisplatin: a multicentre, randomised, double-blind, placebo-controlled Phase 3 trial. Ann Oncol. 2013;24(4):1067–1073. doi:10.1093/annonc/mds541
23. Andrews PLR, Golding JF, Sanger GJ. An assessment of the effects of neurokinin1 receptor antagonism against nausea and vomiting: relative efficacy, sites of action and lessons for future drug development. Br J Clin Pharmacol. 2023;89(12):3468–3490. doi:10.1111/bcp.15852
24. Maemondo M, Masuda N, Sekine I, et al. A phase II study of palonosetron combined with dexamethasone to prevent nausea and vomiting induced by highly emetogenic chemotherapy. Ann Oncol. 2009;20(11):1860–1866. doi:10.1093/annonc/mdp195
25. Bria E, Lesser M, Raftopoulos H, et al. Using two meta-analysis methods to determine whether common dose differences affect efficacy with the serotonin antagonist (5-HT) palonosetron: an individual patient data (IPD) meta-analysis and an abstracted data (AD) meta-analysis of 1947 patients entered into the 8 doubleblinded randomized clinical trials (RCTs). Support Care Cancer. 2009;17(872):02–007.
26. Chow R, Yin LB, Baqri W, et al. Prevalence and predictors of long-delayed (> 120 h) Chemotherapy-induced nausea and vomiting (CINV)-a systematic review and individual patient data meta-analysis. Support Care Cancer. 2023;31(8):505. doi:10.1007/s00520-023-07978-y
27. Nakata A, Hashimoto N, Narita Y, et al. Safety of a short-term infusion of fosnetupitant in patients with gastrointestinal and breast cancer: a prospective study. Oncologist. 2025;30(2):oyae223. doi:10.1093/oncolo/oyae223
28. Luo WT, Chang CL, Huang TW, Gautama MSN. Comparative effectiveness of netupitant-palonosetron plus dexamethasone versus aprepitant-based regimens in mitigating chemotherapy-induced nausea and vomiting: a meta-analysis of randomized controlled trials. Oncologist. 2025;30(2):oyae233. doi:10.1093/oncolo/oyae233
29. Navari RM, Schwartzberg LS. Evolving role of neurokinin 1-receptor antagonists for chemotherapy-induced nausea and vomiting. Onco Targets Ther. 2018;11:6459–6478. doi:10.2147/OTT.S158570
30. Matsuura K, Tsurutani J, Inoue K, et al. A phase 3 safety study of fosnetupitant as an antiemetic in patients receiving anthracycline and cyclophosphamide: CONSOLE-BC. Cancer. 2022;128(8):1692–1698. doi:10.1002/cncr.34088
31. Kim JE, Jang JS, Kim JW, et al. Efficacy and safety of aprepitant for the prevention of chemotherapy-induced nausea and vomiting during the first cycle of moderately emetogenic chemotherapy in Korean patients with a broad range of tumor types. Support Care Cancer. 2017;25(3):801–809. doi:10.1007/s00520-016-3463-0
32. Parisi A, Giampieri R, Mammarella A, et al. Primary versus secondary antiemetic prophylaxis with NK1 receptor antagonists in patients affected by gastrointestinal malignancies and treated with a doublet or triplet combination regimen including oxaliplatin and/or irinotecan plus fluoropyrimidines: a propensity score matched analysis. Front Oncol. 2022;12:935826. doi:10.3389/fonc.2022.935826
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.