Back to Journals » Clinical Interventions in Aging » Volume 20
Comparative Effects of Minodronate and Alendronate on Low Back Pain in Postmenopausal Osteoporosis and Age Influence: A Head-to-Head, Randomized Clinical Trial
Authors Wang H, Liu H, Huang J, Meng X, Wang W, Xiao W, Liu D ![]() , Tao L
, Tao L ![]() , Song C
, Song C ![]()
Received 21 May 2025
Accepted for publication 5 November 2025
Published 27 November 2025 Volume 2025:20 Pages 2219—2230
DOI https://doi.org/10.2147/CIA.S541940
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Zhi-Ying Wu
Huan Wang,1 Hao Liu,1 Jie Huang,1 Xiuli Meng,2 Wei Wang,3 Wenhua Xiao,4 Dongyang Liu,5 Liyuan Tao,6 Chunli Song1
1Department of Orthopedics, Peking University Third Hospital, Beijing, People’s Republic of China; 2Pain Medicine Center, Peking University Third Hospital, Beijing, People’s Republic of China; 3Department of Obstetrics and Gynaecology, Peking University Third Hospital, Beijing, People’s Republic of China; 4Department of Endocrinology and Metabolism, Center of Reproductive Medicine, Peking University Third Hospital, Beijing, People’s Republic of China; 5Drug Clinical Trial Center, Peking University Third Hospital, Beijing, People’s Republic of China; 6Research Center of Clinical Epidemiology, Peking University Third Hospital, Beijing, People’s Republic of China
Correspondence: Chunli Song, Department of Orthopedics, Peking University Third Hospital, Beijing, China, 49# North Garden Road, Haidian District, Beijing, 100191, People’s Republic of China, Email [email protected]
Purpose: This study aimed to compare the analgesic efficacy of minodronate versus alendronate for postmenopausal osteoporosis-related low back pain and evaluate age-dependent treatment responses.
Methods: In this prospective, open-label randomized controlled trial, 72 postmenopausal women with osteoporosis were stratified by age (≥ 75 vs < 75 years) and allocated to 24-week treatment with daily minodronate (1 mg) or alendronate (10 mg). The primary endpoint was Visual Analogue Scale score changes from baseline to week 12. Secondary outcomes included age-stratified changes in lumbar spine and hip bone mineral density, along with serum bone turnover markers across different age groups (≥ 75 vs < 75 years).
Results: Both regimens demonstrated comparable analgesic efficacy, with significant within-group Visual Analogue Scale reductions (minodronate: 11.08± 1.52%; alendronate: 9.86± 1.29%; P< 0.01 for both) but no between-group difference (P=0.237). At week 24, comparable lumbar bone mineral density improvements were observed (minodronate: 2.42%, 95% CI 1.8– 3.1; alendronate: 4.84%, 95% CI 3.9– 5.7; P=0.103). Marked bone turnover markers suppression persisted in both arms (CTX: 46.14% vs 41.25%; P1NP: 44.82% vs 44.11%). Age-stratified analyses revealed comparable therapeutic responses across subgroups (P> 0.05). Safety profiles were similar, with adverse event rates of 29.7% (minodronate) versus 43.2% (alendronate) (P=0.10), predominantly mild upper gastrointestinal symptoms.
Conclusion: Both bisphosphonates demonstrated equivalent analgesic efficacy and comparable bone mineral density and biochemical effects, with age-independent responses. Safety profiles were similar, supporting clinical selection based on dosing convenience and gastrointestinal tolerance.
Trial Registration: ClinicalTrials.gov number: NCT05673980 (08/12/2022).
Plain Language Summary: This open-label trial demonstrated that minodronate and alendronate achieved comparable pain relief, bone mineral density improvement, and bone turnover markers suppression over 24 weeks, with similar safety profiles and age-independent efficacy. These findings support their equivalent analgesic and bone effects, guiding clinical selection based on dosing convenience and gastrointestinal tolerance.
Keywords: minodronate, alendronate, low back pain, bone mineral density, bone turnover markers, age
Introduction
Low back pain represents a prevalent clinical manifestation of osteoporosis,1 imposing substantial burdens on both quality of life and long-term health outcomes in affected individuals.2–4 The cause of the pain in osteoporosis patients is multifactorial, potentially involving vertebral fractures, muscle spasms, nerve compression, or degenerative changes in the spine.5 However, the specific mechanisms underlying osteoporosis-related low back pain remain incompletely understood, and further research is needed to elucidate these pathways. Moreover, pain further exacerbates bone loss.6 Pain relief greatly improves how patients feel, which is beneficial for increasing medication compliance in osteoporosis patients. Isphosphonates, a class of anti-osteoporosis drugs, have been reported to exhibit analgesic effects in some studies.7 The proposed mechanisms include inhibition of osteoclast activity, reduction of inflammatory cytokines, and modulation of nociceptive pathways.7,8 However, the exact analgesic mechanisms of bisphosphonates remain unclear, and further investigation is warranted to clarify their role in pain management.
With aging, osteoporosis has become an important public health problem worldwide. The prevalence of osteoporosis in women worldwide is 23.1%, whereas the incidence of osteoporosis among men worldwide is 11.7%.9 Owing to the coexistence of multiple diseases and the use of multiple drugs, the response of older people to anti-osteoporosis pharmacotherapies may be different from that of patients of other ages. In addition, the levels of bone turnover markers (BTMs), bone mineral density (BMD), fracture incidence and low back pain associated with osteoporosis also change with age.10–12 BMD can serve as a surrogate endpoint in clinical research on osteoporosis. BTMs are important diagnostic and therapeutic indicators for osteoporosis in clinical practice. BTMs include bone resorption markers and bone formation markers, and the changes in BTMs usually occur earlier than those in BMD. The International Council for Harmonization of Technical Requirements for Pharmaceutical for Human Use (ICH) guideline E7 emphasizes the importance of including older people in clinical trials, particularly those who are 75 years old or older.13 The organizations including the FDA have reiterated the urgent need for research and treatment of osteoporosis in such individuals.
Minodronate is the third generation of bisphosphonate,14 which has a low incidence of adverse reactions. A ten-year real-world study results revealed the lowest incidence of minodronate-related osteonecrosis of the jaw (ONJ) and typical femoral fractures (AFFs).15 Minodronate does not undergo metabolism or transformation within the body and is excreted primarily unchanged through the kidneys.16 With age, renal function declines, particularly in individuals older than 75. Bisphosphonate is not inherently nephrotoxic, however, it may cause renal function impairment in patients with preexisting renal dysfunction.17 Alendronate and zoledronate have been investigated in elderly populations, providing valuable reference for the use of bisphosphonates in the geriatric group.18,19 Currently, the effect of minodronate has not been previously studied in the older osteoporosis population, making it crucial to evaluate the impact of age on the efficacy and safety of minodronate. This study aimed to compare the analgesic efficacy of minodronate versus alendronate for postmenopausal osteoporosis-related low back pain and evaluate age-dependent treatment responses.
Materials and Methods
Study Design
The aim of this study was to compare the efficacy of minodronate and alendronate in the treatment of low back pain in postmenopausal osteoporosis patients (Minodronate vs Alendronate Pain Study, “MAPS”), while also evaluating the effects of these treatments on BMD and BTMs across different age groups. This was a head-to-head, single-center, randomized, open-label controlled trial with a duration of 24 weeks. The participants were randomly allocated to receive either minodronate or alendronate. The trial was structured into two distinct phases, each lasting 12 weeks. In the first phase, minodronate or alendronate was administered once daily for 12 weeks. In the second phase, all the subjects stopped minodronate or alendronate for 12 weeks.
This study has been registered in a clinical trial registry (clinicaltrial.gov, ID: NCT05673980 on 08/12/2022). Ethical approval for the study protocol was granted by the Peking University Third Hospital Medical Science Research Ethics Committee, with approval number M2022828. The study was conducted in accordance with the principles of the Declaration of Helsinki. The study protocol adheres to the CONSORT 2010 checklist of information to include when reporting a randomised trial. The trial protocol is available at “Efficacy and safety of minodronate in the treatment of postmenopausal osteoporosis with low back pain: a single-centre, randomized and open-label controlled trial. (DOI: 10.1186/s13063-024-8364-7)”.17 Prior to their participation, each subject enrolled in the study provided their written informed consent.
Participants
Postmenopausal women aged >50 years diagnosed with osteoporosis were prospectively enrolled. The trial was initiated on January 1, 2023, with recruitment concluding on April 11, 2024, yielding a final cohort comprising 80 participants. Using a stratified randomization protocol, subjects were allocated in a 1:1 ratio to receive either daily oral minodronate (1 mg/day) or alendronate (10 mg/day). Age-based stratification ensured proportional representation, with participants aged≥75 years and those aged <75 years assigned at a 1:2 allocation ratio to maintain demographic balance across treatment arms.
The study’s inclusion criteria were as follows: postmenopausal women with chronic low back pain (≥3 months duration), a VAS score exceeding 30 mm, and sufficient vitamin D status (serum 25-hydroxyvitamin D>20 ng/mL). The exclusion criteria included secondary osteoporosis, prior use of medications influencing bone metabolism, and the presence of any conditions that could confound bone metabolism assessments. Eligible subjects meeting these criteria were invited to participate in the trial.
The participants in the study were administered either oral administration of alendronate or minodronate daily for a period of 12 weeks, after which drug administration was discontinued. Throughout the trial, a total of 5 in-person follow-up visits were planned. Back pain was evaluated using 100 mm VAS scores (0 = no pain, 100 = worst pain possible). The patients’ VAS scores were recorded via weekly telephone follow-ups over a 12-week period. Vital signs, BTMs, serum calcium, and serum phosphorus were measured during the screening period, on day 1, and in weeks 8, 12 and 24. Blood parameters, liver function, renal function, electrocardiogram results and BMD were monitored during the screening period and at weeks 12 and 24. The safety assessment was mainly based on the occurrence of gastrointestinal adverse reactions after oral administration.
Randomization and Study Interventions
The participants were randomly assigned to different treatment groups by local investigators utilizing a randomization envelope system, which effectively concealed the allocation sequence. A series of random numbers was generated using SPSS software. These random numbers, along with their corresponding serial numbers, were used to determine the assignment of subjects to either the minodronate or alendronate group, ensuring that the allocation process was both opaque and unbiased.
The participants were administered a daily oral dose of either minodronate or alendronate in the morning over a 12-week treatment period. All the subjects received supplementary oral calcium carbonate and vitamin D3 (containing 600 mg of calcium and 125 IU of vitamin D3) after dinner, which was maintained throughout the entire study duration to ensure consistent calcium and vitamin D3 supplementation. If any subjects were to experience a sudden exacerbation of low back pain with a VAS score of 70 or higher, they would uniformly receive rescue medication (acetaminophen) for treatment, and the duration of pain relief treatment would not exceed 5 days.
Outcome Assessment
The primary endpoint was VAS score changes from baseline to week 12. Secondary outcomes included age-stratified changes in lumbar spine and hip BMD, along with serum BTMs across different age groups (≥75 vs <75 years).
Sample Size Calculation and Power
This was an exploratory study with a small sample size. The number of participants was determined based on a randomized controlled trial published in the Journal of Bone and Mineral Metabolism in 2013.20 In this study, a 1:1 design method was adopted to estimate the sample size required by the T test of two independent samples, and α=0.05, 1-β=0.90, considering a 10% loss to follow-up rate. A total of 72 patients were included in the alendronate group and the minodronate group, of whom 24 were in the older subgroup and 48 were in the very senior subgroup.
Statistical Analysis
Statistical Analysis Datasets
There were three statistical analysis datasets, including intention-to-treat (ITT) sets, per-protocol (PP) sets and safety sets. All the subjects included in this study were included in the ITT analysis sets. The PP sets were used for sensitivity analysis. Primary and secondary outcomes were analyzed according to ITT and PP principles. In addition, all the subjects who received treatment were included in the safety sets, which were used in the analysis of vital signs, laboratory tests and adverse effects (AEs).
The Kaplan‒Meier survival curve and Log rank test were used to analyze the primary outcomes and secondary outcomes. The generalized linear mixed model was used to control the baseline imbalance and central effect, and the different centers were set as fixed effects. Quantitative data are expressed as the mean ± standard deviation, and a t test was used to compare the data. For comparisons between groups, all hypothesis tests were two-sided (α=0.05, unless otherwise specified). P<0.05 was considered statistically significant. The confidence intervals for all tests were 95%.
Investigations were conducted to assess changes in the VAS score, BTMs and BMD, including a comparison of the number of subjects who showed significant changes from baseline using χ2 tests and an assessment of the difference in mean values with t tests.
All the statistical analyses were conducted using SPSS 26.0 (IBM, Armonk, NY, USA) and R 4.2.2 software (www.r-project.org).
Results
Baseline Characteristics and Follow-Up
A total of 108 subjects were screened in this study, and a total of 80 subjects signed informed consent forms. 40 subjects were randomly assigned to receive minodronate, and 40 subjects were assigned to receive alendronate. The full analysis set consisted of 37 subjects in the minodronate group and 37 subjects in the alendronate group. Among these subjects, 74 subjects completed the 24-week treatment of the trial. During the trial period, no patients initiated the use of rescue medication (acetaminophen). The results show no significant differences between the ITT and PP analyses. Efficacy analyses were performed on the ITT population (74 subjects). The flow chart of this trial is shown in Figure 1.
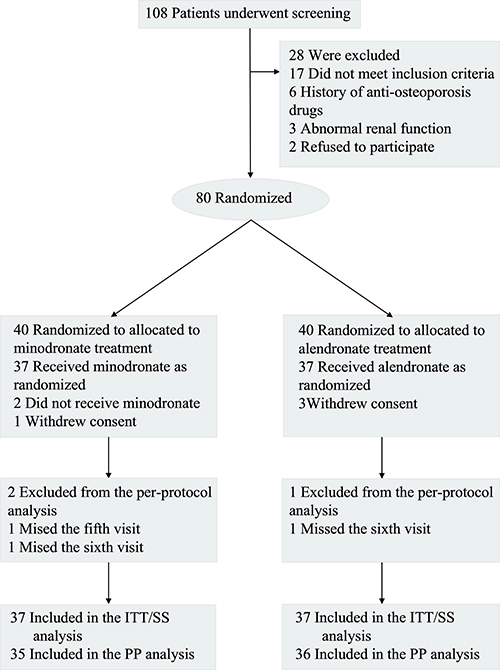 |
Figure 1 Study flow chart. |
There were no significant differences between the two groups in terms of age, time since menopause, body mass index (BMI), VAS scores, BMD, CTX, P1NP, Ca or P. The median age was 66.52 years in this population. The baseline demographic and clinical characteristics are presented in Tables 1 and S1.
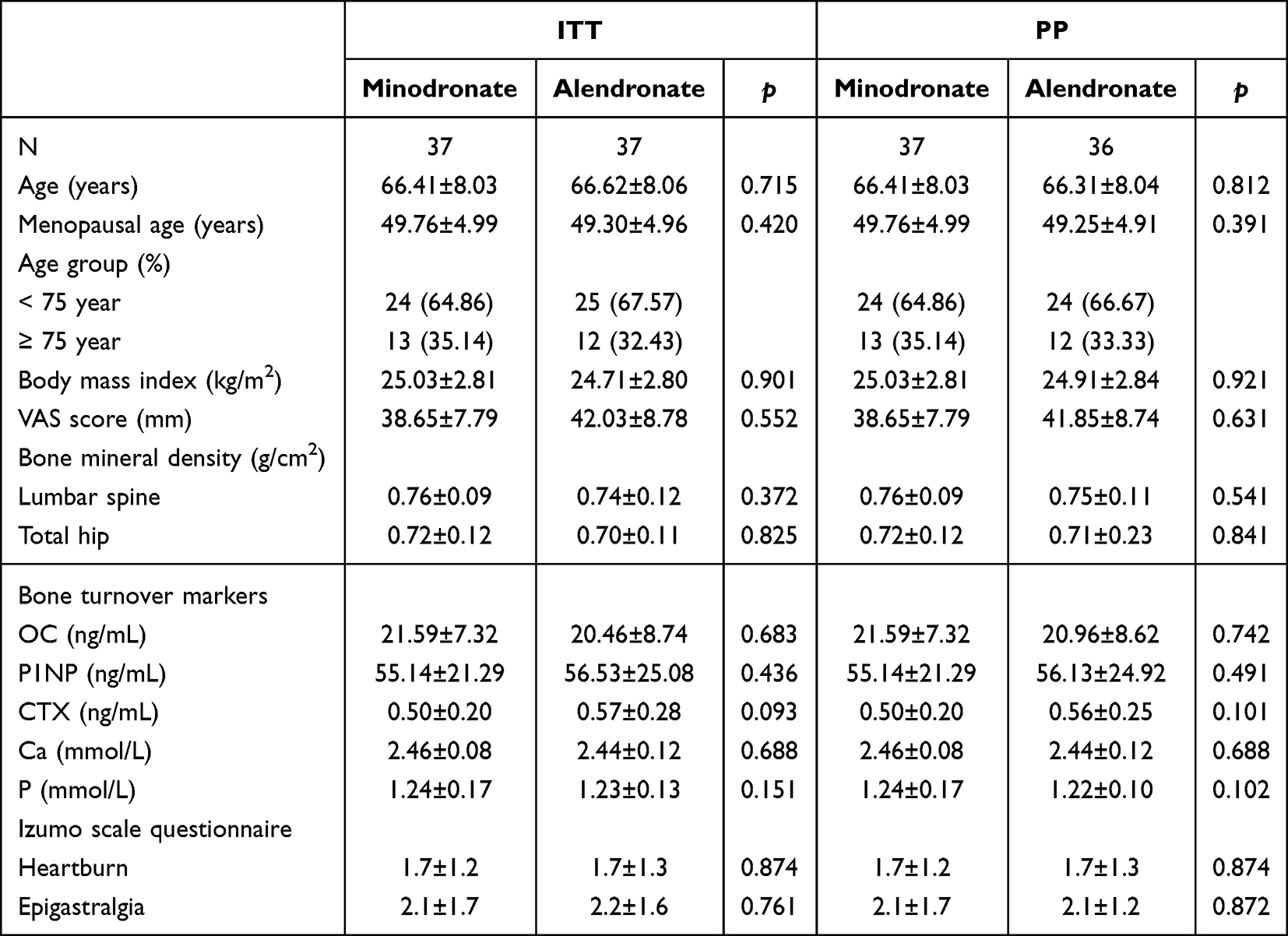 |
Table 1 Baseline Characteristics of the Patients |
VAS Scores
The minodronate group demonstrated earlier onset of pain reduction, with significant decreases in VAS scores emerging at Week 2, followed by progressive improvement in a time-dependent manner. By Week 4, this group achieved a 10% reduction from baseline VAS scores, a magnitude attained one week later (Week 5) in the alendronate group. At the 12-week endpoint, minodronate-treated subjects exhibited a mean VAS reduction of 11.08 mm (95% CI: 9.2–12.9) from baseline, compared to 9.86 mm (95% CI: 8.1–11.6) in the alendronate group. While both interventions showed significant within-group improvements, comparative analysis revealed no statistically significant between-group differences in VAS scores at any timepoint. Notably, minodronate consistently outperformed in reducing VAS scores from baseline across all measurement intervals, as shown by the temporal trajectories in Figure 2 and detailed in the longitudinal data of Table S2.
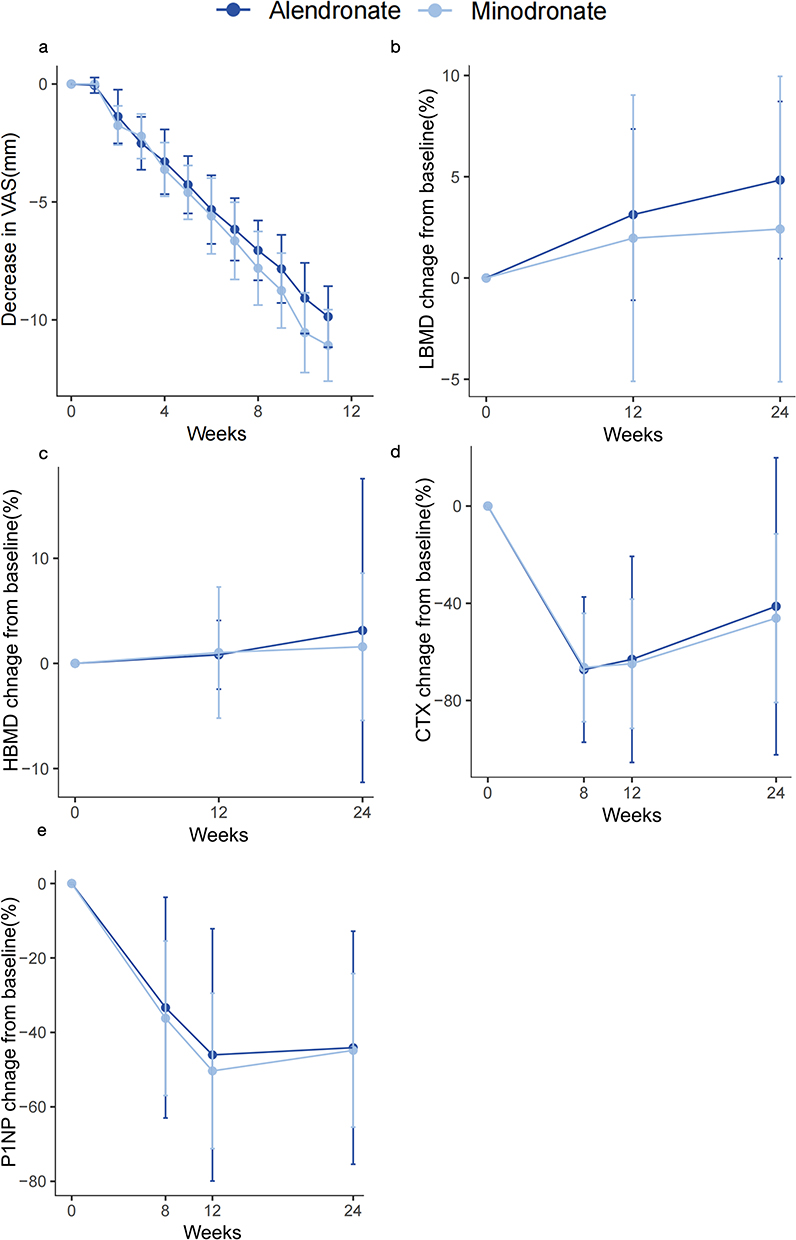 |
Figure 2 Changes in Pain VAS Scores, LBMD, HBMD, CTX, and P1NP from baseline in the minodronate and alendronate groups using Intention-to-Treat Analysis. (a) Changes in Pain VAS Scores from baseline in the minodronate and alendronate groups. (b) Changes in LBMD from baseline in the minodronate and alendronate groups. (c) Changes in HBMD from baseline in the minodronate and alendronate groups. (d) Changes in CTX from baseline in the minodronate and alendronate groups. (e) Changes in P1NP from baseline in the minodronate and alendronate groups. Light blue represents the minodronate group, and dark blue represents the alendronate group. |
BMD
Following 12 weeks of treatment, the minodronate group exhibited lumbar spine and hip BMD increases of 2.02% and 1.03%, respectively, from baseline. Comparatively, the alendronate group showed greater lumbar gains (3.13%) but marginally lower hip improvements (0.81%). Notably, both therapies demonstrated sustained efficacy through a 12-week post-treatment observational period. Minodronate displayed progressive BMD accrual, achieving cumulative increases of 2.42% (lumbar) and 1.58% (hip) at week 24, whereas alendronate maintained its lumbar improvement (3.13%) with attenuated hip gains (0.81%) relative to baseline. The BMD change from baseline (Figure 2 and Table S3) and the values of BMD (Figure S1) confirm these differential patterns of skeletal response.
BTMs
At the 12-week treatment endpoint, minodronate induced reductions in bone resorption (CTX: 64.88%, 95% CI: 68.2 to 61.6) and bone formation (P1NP: 50.35%, 95% CI: 53.1 to 47.6) relative to baseline. Alendronate demonstrated comparable suppression (CTX: 63.09%, P1NP: 46.04%), with overlapping confidence intervals indicating no significant between-group differences. Both therapies exhibited sustained biochemical suppression during the 12-week post-treatment follow-up (Week 24). Minodronate maintained greater attenuation of bone turnover (CTX: 46.14%, P1NP: 44.82%) compared to alendronate (CTX: 41.25%, P1NP: 44.11%), though intergroup comparisons remained statistically non-significant. The changes in baseline CTX and P1NP modulation are detailed in Figure 2 and Table S3, with the concentrations provided in Figure S2.
The Impact of Age on BTMs and BMD
In the minodronate-treated cohort, participants aged ≥75 years (older subgroup) demonstrated lumbar spine and hip BMD increases of 0.44% and 1.31%, respectively, at Week 12, whereas those aged <75 years (senior subgroup) exhibited greater lumbar gains (2.91%) but reduced hip improvements (0.88%). In contrast, alendronate-treated participants showed no significant inter-subgroup differences in lumbar or hip BMD changes. The analysis revealed no statistically significant age-dependent disparities in lumbar BMD response to either therapy at weeks 12 or 24. However, pooled analysis across treatment arms identified a consistent trend: participants aged ≥75 years exhibited numerically greater lumbar BMD increments from baseline compared to senior counterparts (mean difference: 1.2%, P = 0.13). Age-stratified BMD values are detailed in Figure S3.
Both minodronate and alendronate induced significant reductions in serum CTX and P1NP levels across all age groups, with initial decreases observed as early as week 8 of treatment (Figure S4). These biomarkers remained persistently suppressed throughout the treatment period, demonstrating sustained pharmacodynamic effects that persisted even after drug discontinuation. Age-related differences in treatment response were specifically noted in CTX reduction at week 8, with the senior group showing greater suppression compared to the older cohort (69.60±17.66% vs 60.58±28.99% reduction from baseline, respectively; P=0.036). However, this age-dependent variation was transient, as subsequent time points revealed no significant age-related differences in either CTX or P1NP levels. Figures 3 and S4 comprehensively illustrates the effects of aging on multiple clinical parameters, including VAS scores, BMD changes, and bone turnover marker dynamics. The data demonstrate that while age influenced early treatment response magnitude, it did not substantially affect the duration of biochemical suppression achieved through bisphosphonate therapy.
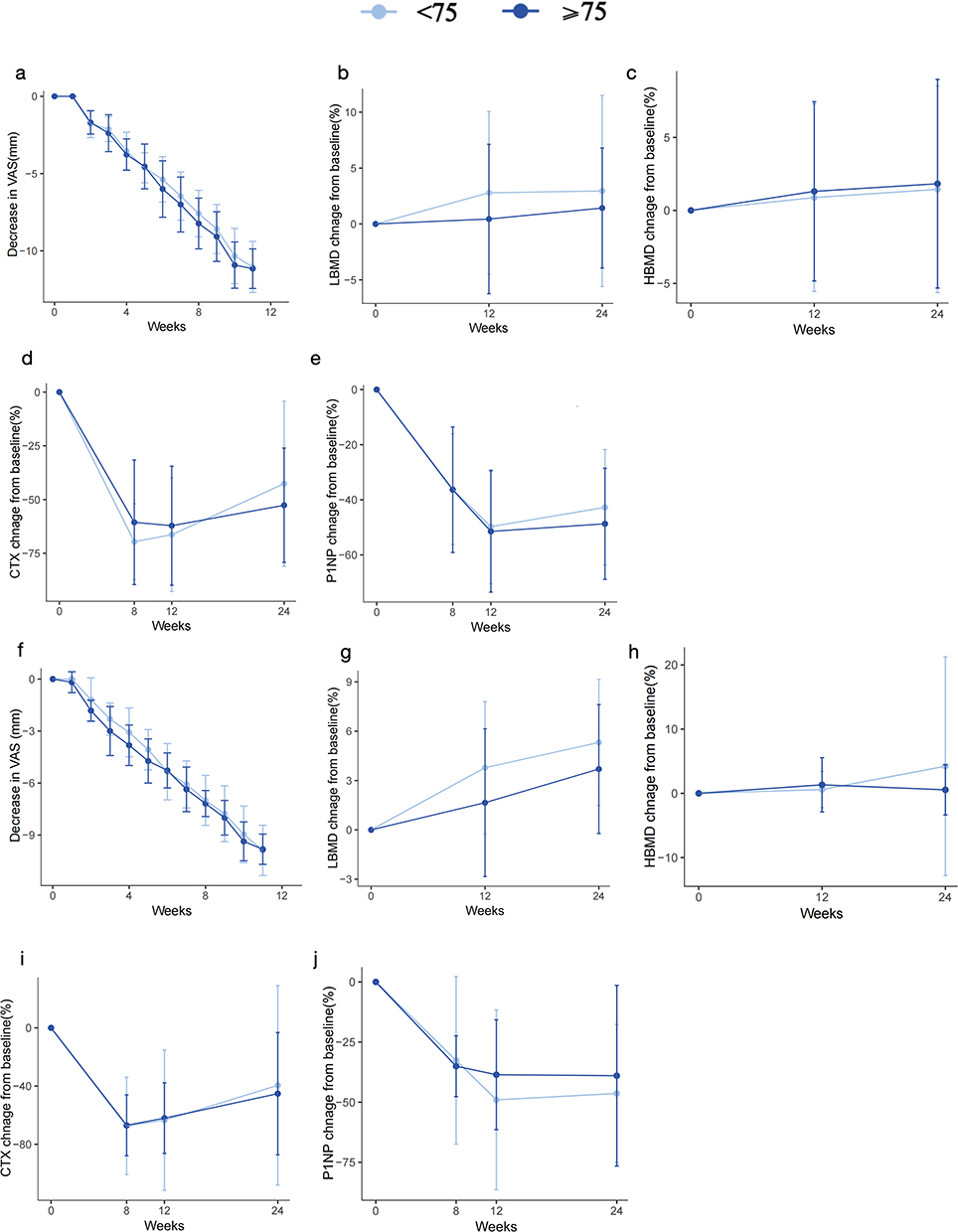 |
Figure 3 Effect of age on VAS, BMD, and BTMs in the minodronate and alendronate groups using Intention-to-Treat Analysis. (a–g) The effect of age on VAS, BMD, and BTMs in the minodronate group. (f–j) The effect of age on VAS, BMD, and BTMs in the alendronate group. Light blue represents the senior group, and dark blue represents the older group. |
Adverse Events
Both minodronate and alendronate demonstrated favorable safety profiles, with no serious adverse events reported during the trial period. Gastrointestinal tolerability in the minodronate group remained comparable to baseline levels throughout treatment. A comparative safety analysis revealed distinct adverse event patterns: the minodronate group exhibited lower incidence rates of nausea (5.4% vs 10.8%), vomiting (0% vs 5.4%), and constipation (2.7% vs 5.4%) relative to the alendronate group. However, both therapies showed similar rates of belching (8.1% vs 13.5%), dizziness (8.1% vs 5.4%), tachycardia (2.7% vs 2.7%), and diarrhea (2.7% vs 5.4%). The complete safety data, including adverse event frequencies and intergroup comparisons, are detailed in Table 2.
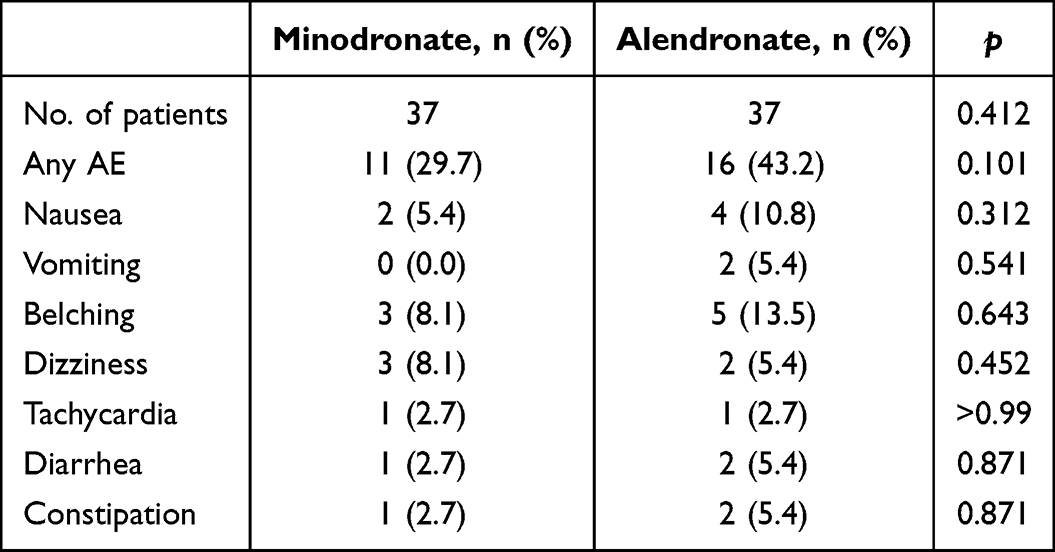 |
Table 2 The Adverse Effect of Two Group |
Discussion
Our findings show that both minodronate and alendronate can effectively reduce low back pain and suppress bone turnover in postmenopausal osteoporosis patients. The results of the endpoints show no significant differences between the ITT and PP analyses. Although the minodronate group had greater numerical improvements in pain relief than the alendronate group, the intergroup difference was not statistically significant.These findings align with previous studies indicating bisphosphonates can quickly relieve pain in osteoporosis patients.21 The observed analgesic effects, particularly the rapid pain reduction within the first treatment phase, hold clinical relevance regardless of intergroup differences.
While both agents increased lumbar BMD, the numerically greater gain with alendronate (4.84% vs 2.42%) suggests potential differential effects on bone formation, warranting further investigation. Notably, sustained BMD improvement persisted after 12-week discontinuation, consistent with bisphosphonates’ prolonged skeletal retention.22 A 5-year extended observational study of alendronate in the United States revealed that alendronate remained effective even after discontinuation, with a sustained increase in lumbar BMD and a sustained reduction in fracture risk.23,24 The significant decrease in BTMs further confirms the effective suppression of bone resorption by both drugs. Minodronate and alendronate both had long-term inhibitory effects on CTX and P1NP, which is consistent with their known effects on reducing bone turnover and fracture risk.
Osteoporosis patients often experience back pain, which may be related to osteoclast-mediated bone resorption.25 Excessive osteoclast activity activates acid-sensing ion channel protein ASIC-3 and transient receptor potential vanilloid subtype 1 (TRPV1), acidifying the local microenvironment. This lowers the local tissue pH, heightens nociceptor sensitivity, and thus causes pain.26 Minodronate is 10–100 times more active for the inhibition of bone resorption than alendronate is,27 which may account for the superior improvement in VAS scores observed with minodronate compared to alendronate.
Minodronate effectively inhibits farnesyl pyrophosphate synthase. It has a lower affinity for bone matrix hydroxyapatite at both neutral and acidic pH levels, suggesting reduced binding to the bone matrix hydroxyapatite.28,29 In vitro studies have demonstrated that, compared with the elution time of alendronate, the relative elution time ratio order was as follows: zoledronic acid = alendronate > risedronate > minodronate.28,29 In vivo studies have shown that after intravenous injection in rats, alendronate has the highest percentage of skeletal retention within 24 hours, whereas minodronate has the lowest percentage of skeletal retention.29 These studies collectively suggest that minodronate resides in bone tissue for a shorter duration and binds to bone matrix hydroxyapatite to a lesser extent in circulation. Following a 12-week discontinuation of bisphosphonate therapy, our findings demonstrated a significant increase in BTMs, with minodronate showing a greater increase than alendronate, suggesting a quicker clearance of minodronate from the body. Although minodronate deposits less in the skeleton, its lower affinity allows for more effective release during bone resorption, thereby exerting potent antiresorptive activity in vivo.
Safety considerations further distinguish these agents. Minodronate’s attenuated hydroxyapatite binding correlates with reduced skeletal deposition, potentially lowering risks of osteonecrosis of the jaw (ONJ) and atypical fractures.30 Minodronate’s lower affinity for bone means it deposits less, likely explaining its lower adverse reaction rate. Due to this characteristic, minodronate may permit a shorter drug holiday prior to tooth extraction. Data from the Japanese Adverse Drug Event Report database showed that minodronate had the lowest incidence of osteonecrosis of the jaw among all bisphosphonates.15 This characteristic advantage may permit shorter drug holidays prior to dental procedures, particularly beneficial for elderly patients with comorbid dental conditions.
Age-stratified analyses revealed consistent therapeutic responses across geriatric subgroups. Additionally, the levels of hormones, particularly estrogen and testosterone, decrease with age, and play a critical role in maintaining bone density and metabolism, resulting in impaired osteoblast function and enhanced osteoclast activity.31 Furthermore, the older population often experiences nutritional deficiencies, particularly in calcium and vitamin D, which adversely affect bone formation and mineralization.32 These factors contribute to a low turnover state of bone metabolism in the older population, increasing the risk of osteoporosis. Minodronate can reduce the expression of BTMs rapidly. In our study, there was a swift decline in CTX following minodronate administration, particularly at the 8th week, where the decrease was more pronounced in the minodronate group, especially among the older population. These findings suggest that minodronate may have a significant effect on bone turnover rates in the older population, particularly in the early stages of treatment. Osteoclasts facilitate bone resorption by creating an acidic environment within the resorption lacunae, which dissolves the hydroxyapatite crystals in the bone matrix.33 Minodronate has the lowest affinity for bone matrix hydroxyapatite among all bisphosphonates at acidic pH values, implying that it can be more readily released from the bone matrix during bone resorption, thereby exerting potent antiresorptive activity in vivo.34 This mechanism may help explain the rapid suppression of the bone turnover rate in elderly patients by minodronate.
Our study only focused on female osteoporosis patients, which restricts the generalizability of our findings to other demographics. Also, strict inclusion criteria led to a study group with few medical comorbidities and a limited fracture history, causing a low fracture incidence during the trial. This narrow demographic scope and low fracture event rate may limit the wider application of our results, and should be taken into account when interpreting the study outcomes.
Conclusions
Minodronate and alendronate showed equivalent efficacy in improving BMD, reducing bone turnover markers (CTX, P1NP), and alleviating pain (VAS scores), with no significant intergroup differences. Age did not influence therapeutic outcomes. Both agents exhibited comparable safety profiles consistent with bisphosphonate class effects.
Data Sharing Statement
The data underlying this article will be shared upon reasonable request to the corresponding author.
Acknowledgments
The authors would like to express sincere thanks to all patients who participated in the study. We would like to acknowledge Tasly Pharmaceutical Group Co.,Ltd. and Beijing Research Association for Chronic Diseases Control and Health Education for supporting this research project.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Key Research and Development Program (Grant number 2021YFC2501700) and the National Natural Science Foundation of China (Grant number 82330078, 82272554).
Disclosure
Huan Wang, Hao Liu, Jie Huang, Xiuli Meng, Wei Wang, Wenhua Xiao, Dongyang Liu, Liyuan Tao and Chunli Song declare that they have no conflict of interest.
References
1. Pickering ME, Javier RM, Malochet S, Pickering G, Desmeules J. Osteoporosis treatment and pain relief: a scoping review. Eur J Pain. 2024;28(1):3–20. doi:10.1002/ejp.2156
2. Cortet B, Chauvin P, Feron JM, et al. Fragility fractures in France: epidemiology, characteristics and quality of life (the EPIFRACT study). Arch Osteoporos. 2020;15(1):46. doi:10.1007/s11657-019-0674-2
3. Nawrat-Szołtysik A, Miodońska Z, Piejko L, et al. Assessment of quality of life and pain severity in older men with osteoporosis: cross-sectional study. Int J Environ Res Public Health. 2021;19(1):18. doi:10.3390/ijerph19010018
4. Yoon SP, Lee SH, Ki CH, et al. Quality of life in patients with osteoporotic vertebral fractures. Asian Spine J. 2014;8(5):653–658. doi:10.4184/asj.2014.8.5.653
5. Iwata S, Hashizume H, Yoshimura N, et al. Osteoporosis, spinal degenerative disorders, and their association with low back pain, activities of daily living, and physical performance in a general population. Sci Rep. 2024;14(1):15860. doi:10.1038/s41598-024-64706-0
6. Rizou S, Chronopoulos E, Ballas M, Lyritis GP. Clinical manifestations of osteoarthritis in osteoporotic and osteopenic postmenopausal women. J Musculoskelet Neuronal Interact. 2018;18(2):208–214.
7. Tzschentke TM. Pharmacology of bisphosphonates in pain. Br J Pharmacol. 2021;178(9):1973–1994. doi:10.1111/bph.14799
8. Wong R, Wiffen PJ. Bisphosphonates for the relief of pain secondary to bone metastases. Cochrane Database Syst Rev. 2002;2002:CD002068.
9. Salari N, Ghasemi H, Mohammadi L, et al. The global prevalence of osteoporosis in the world: a comprehensive systematic review and meta-analysis. J Orthop Surg Res. 2021;16(1):609. doi:10.1186/s13018-021-02772-0
10. Miyagi M, Inoue G, Murata K, et al. Factors associated with pain-related disorders and gait disturbance scores from the Japanese orthopedic association back pain evaluation questionnaire and oswestry disability index in patients with osteoporosis. Arch Osteoporos. 2021;17(1):1. doi:10.1007/s11657-021-01045-x
11. von Friesendorff M, McGuigan FE, Wizert A, et al. Hip fracture, mortality risk, and cause of death over two decades. Osteoporos Int. 2016;27(10):2945–2953. doi:10.1007/s00198-016-3616-5
12. Klotz U. Pharmacokinetics and drug metabolism in the elderly. Drug Metab Rev. 2009;41(2):67–76. doi:10.1080/03602530902722679
13. van Riet-Nales DA, Hussain N, Sundberg KAE, et al. Regulatory incentives to ensure better medicines for older people: from ICH E7 to the EMA reflection paper on quality aspects. Int J Pharm. 2016;512(2):343–351. doi:10.1016/j.ijpharm.2016.05.001
14. Ito M, Sone T, Fukunaga M. Effect of minodronic acid hydrate on Hip geometry in Japanese women with postmenopausal osteoporosis. J Bone Miner Metab. 2010;28(3):334–341. doi:10.1007/s00774-009-0138-7
15. Nakamura M, Umetsu R, Abe J, et al. Analysis of the time-to-onset of osteonecrosis of jaw with bisphosphonate treatment using the data from a spontaneous reporting system of adverse drug events. J Pharm Health Care Sci. 2015;1(1):34. doi:10.1186/s40780-015-0035-2
16. Zhou Y, He X, Li H, et al. Pharmacokinetics and tolerability of minodronic acid tablets in healthy Chinese subjects and food and age effects on the pharmacokinetics. Clin Ther. 2015;37(4):869–876. doi:10.1016/j.clinthera.2015.01.015
17. Ott SM, Drueke T, Elder G, et al. Renal function and bisphosphonate safety. J Bone Miner Res. 2008;23(3):453–454. doi:10.1359/jbmr.071028
18. Greenspan SL, Perera S, Ferchak MA, Nace DA, Resnick NM. Efficacy and safety of single-dose zoledronic acid for osteoporosis in frail elderly women: a randomized clinical trial. JAMA Intern Med. 2015;175(6):913–921. doi:10.1001/jamainternmed.2015.0747
19. Cecilia D, Jódar E, Fernández C, Resines C, Hawkins F. Effect of alendronate in elderly patients after low trauma Hip fracture repair. Osteoporos Int. 2009;20(6):903–910. doi:10.1007/s00198-008-0767-z
20. Yoshioka T, Okimoto N, Okamoto K, Sakai A. A comparative study of the effects of daily minodronate and weekly alendronate on upper gastrointestinal symptoms, bone resorption, and back pain in postmenopausal osteoporosis patients. J Bone Miner Metab. 2013;31(2):153–160. doi:10.1007/s00774-012-0393-x
21. Matsumoto T, Hagino H, Shiraki M, et al. Effect of daily oral minodronate on vertebral fractures in Japanese postmenopausal women with established osteoporosis: a randomized placebo-controlled double-blind study. Osteoporos Int. 2009;20(8):1429–1437. doi:10.1007/s00198-008-0816-7
22. Fink HA, MacDonald R, Forte ML, et al. Long-term drug therapy and drug discontinuations and holidays for osteoporosis fracture prevention: a systematic review. Ann Intern Med. 2019;171(1):37–50. doi:10.7326/M19-0533
23. Black DM, Cummings SR, Karpf DB, et al. Randomised trial of effect of alendronate on risk of fracture in women with existing vertebral fractures. Fracture Intervention Trial Research Group. Lancet. 1996;348:1535–1541.
24. Black DM, Schwartz AV, Ensrud KE, et al. Effects of continuing or stopping alendronate after 5 years of treatment: the Fracture Intervention Trial Long-term Extension (FLEX): a randomized trial. JAMA. 2006;296(24):2927–2938. doi:10.1001/jama.296.24.2927
25. Mediati RD, Vellucci R, Dodaro L. Pathogenesis and clinical aspects of pain in patients with osteoporosis. Clin Cases Miner Bone Metab. 2014;11(3):169–172.
26. Catalano A, Martino G, Morabito N, et al. Pain in osteoporosis: from pathophysiology to therapeutic approach. Drugs Aging. 2017;34(10):755–765. doi:10.1007/s40266-017-0492-4
27. Dunford JE, Thompson K, Coxon FP, et al. Structure-activity relationships for inhibition of farnesyl diphosphate synthase in vitro and inhibition of bone resorption in vivo by nitrogen-containing bisphosphonates. J Pharmacol Exp Ther. 2001;296(2):235–242. doi:10.1016/S0022-3565(24)38786-5
28. Ebetino FH, Hogan AM, Sun S, et al. The relationship between the chemistry and biological activity of the bisphosphonates.Bone. 2011;49:20–33
29. Lawson MA, Ebetino FH, Mazur A, et al. The pharmacological profile of a novel highly potent bisphosphonate, OX14 (1-Fluoro-2-(Imidazo-[1,2-α]Pyridin-3-yl)-Ethyl-Bisphosphonate). J Bone Miner Res. 2017;32(9):1860–1869. doi:10.1002/jbmr.3138
30. Papapetrou PD. Bisphosphonate-associated adverse events. Hormones. 2009;8(2):96–110. doi:10.14310/horm.2002.1226
31. Niwczyk O, Grymowicz M, Szczęsnowicz A, et al. Bones and hormones: interaction between hormones of the hypothalamus, pituitary, adipose tissue and bone. Int J Mol Sci. 2023;25(1):24. doi:10.3390/ijms25010024
32. Rizzoli R, Biver E, Brennan-Speranza TC. Nutritional intake and bone health. Lancet Diabetes Endocrinol. 2021;9(9):606–621. doi:10.1016/S2213-8587(21)00119-4
33. Coxon FP, Thompson K, Roelofs AJ, Ebetino FH, Rogers MJ. Visualizing mineral binding and uptake of bisphosphonate by osteoclasts and non-resorbing cells. Bone. 2008;42:848–860.
34. Matsumoto T, Endo I. Minodronate. Bone. 2020;137:115432. doi:10.1016/j.bone.2020.115432
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Efficacy and Safety of Generic Alendronate for Osteoporosis Treatment
Jarusriwanna A, Malisorn S, Tananoo S, Areewong K, Rasamimongkol S, Laoruengthana A
Orthopedic Research and Reviews 2024, 16:85-91
Published Date: 22 February 2024
Synergistic Efficacy of Calcitriol Combined with Denosumab versus Calcitriol Alone in Postmenopausal Osteoporosis: A Retrospective Cohort Study
Li X, Hu M, Shen Y
International Journal of Women's Health 2026, 18:599348
Published Date: 22 May 2026