Back to Journals » ImmunoTargets and Therapy » Volume 14
Comparative Effectiveness and Safety of Molecular Targeted Therapy Plus PD-(L)1 with or without TACE in Unresectable Hepatocellular Carcinoma: A Retrospective Study
Authors Liu J, Wang Y, Cui L ![]() , Nie Y, Li C, Tan W
, Nie Y, Li C, Tan W ![]() , Li Y, Bai Y, Wan T, Hu B, Liu Z, Hu M, Wang M
, Li Y, Bai Y, Wan T, Hu B, Liu Z, Hu M, Wang M ![]() , Duan F
, Duan F ![]()
Received 10 October 2024
Accepted for publication 29 March 2025
Published 17 July 2025 Volume 2025:14 Pages 761—771
DOI https://doi.org/10.2147/ITT.S495451
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Sarah Wheeler
Jiangtao Liu,1,* Yan Wang,2,* Li Cui,2 Yan Nie,1 Chao Li,1 Wenle Tan,2 Ye Li,1 Yanhua Bai,1 Tao Wan,3 Bingyang Hu,3 Zhe Liu,3 Minggen Hu,3 Maoqiang Wang,2 Feng Duan2
1Department of Gastroenterology, Hainan Hospital of Chinese People’s Liberation Army (PLA) General Hospital, Sanya, Hainan, 572000, People’s Republic of China; 2Department of Interventional Radiology, Chinese People’s Liberation Army (PLA) General Hospital, Beijing, 100853, People’s Republic of China; 3Faculty of Hepato-Biliary-Pancreatic Surgery, Chinese People’s Liberation Army (PLA) General Hospital, Beijing, 100853, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Feng Duan, Email [email protected]
Objective: This study aims to compare the effectiveness and safety of TACE combined with molecular targeted therapy (MTT) plus Programmed death-ligand 1 (PD-(L)1) antibodies versus MTT plus PD-(L)1 antibodies for HCC patients.
Methods: Data from HCC patients who received either MTT plus PD-(L)1 (systemic therapy group) or TACE combined with MTT plus PD-(L)1 (combination therapy group) were retrospectively analyzed. The primary outcome was the objective reaction rate (ORR) at the initial assessment post-treatment initiation. Secondary outcomes included progressive free survival (PFS), overall survival (OS) and grade-3 or higher adverse events.
Results: A total of 222 HCC patients were included (109 in the systemic therapy group, 113 in the combination therapy group). Propensity score matching yielded 80 patients per group. The odds ratio for ORR in the combination therapy group was 1.29 (95% CI: 0.64– 2.60; p=0.479). Subgroup analysis revealed significantly higher ORR for patients with AFP≤ 200 ng/mL in the combination therapy group (OR=3.54, p=0.016). For patients without PVTT, the ORR odds were slightly higher with combination therapy (OR=5.33, p=0.068). Multivariate Cox regression analysis showed no significant differences in PFS (HR=0.68, p=0.131) or OS (HR=0.86, p=0.674) between the two groups. Higher baseline AFP (> 200 ng/mL) was associated with worse PFS (HR=1.68, p=0.012) and OS (HR=2.33, p=0.021). Surgical resection improved PFS (HR=0.42, p< 0.001) and OS (HR=0.31, p=0.004). Grade 3 or higher adverse events were more common in the combination therapy group (52% vs 15%, p< 0.0001).
Conclusion: No significant benefits were observed for combining TACE with MTT and PD-(L)1 in unresectable HCC patients. However, TACE may offer advantages for patients with AFP≤ 200 ng/mL or without PVTT.
Keywords: molecular targeted therapy, PD-(L)1, hepatocellular carcinoma, transarterial chemoembolization
Background
Primary liver cancer, including hepatocellular carcinoma (HCC), is a significant contributor to global cancer-related morbidity and mortality, ranking sixth and fourth, respectively.1,2 Unfortunately, over 50% of HCC patients receive a diagnosis at stage Barcelona Clinic Liver Cancer (BCLC)-C, according to the Barcelona Liver Cancer Criteria (BCLC), presenting a formidable challenge to treatment with an associated grim prognosis.3,4
The results of two Phase III global multicenter clinical trials, the SHARP and Oriental studies, have established the role of multi-target tyrosine kinase inhibitors (TKIs) in treating BCLC-C HCC.5,6 Although TKIs have served as first-line treatment for BCLC-C HCC for an extended period, their survival benefit remains limited.5–7 In recent years, immune checkpoint inhibitors (ICIs) such as programmed death-1 (PD-1) and programmed death-ligand 1 (PD-L1) antibodies, have demonstrated favorable efficacy and safety in Phase I and II clinical trials for BCLC-C HCC.8–11 However, large-scale clinical studies for BCLC-C HCC have failed to establish PD-(L)1 antibodies as superior to standard treatment.12,13
Given the limited success of PD-(L)1 monotherapy as a first-line treatment for HCC, researchers have shifted focus to combining PD-(L)1 antibodies with molecular targeted therapy (MTT) to enhance advanced HCC treatment. Recent randomized controlled trials have demonstrated the safety and efficacy of various combination regimens involving PD-(L)1 antibodies and MTT in treating BCLC-C stage HCC.14–16 The landmark IMbravel150 study highlighted that the combination of atezolizumab and bevacizumab (“T+A”) outperformed sorafenib monotherapy in terms of objective response rate (ORR), progression-free survival (PFS), and median overall survival (OS) for unresectable HCC.17,18 Following this study, clinical guidelines recommended the “T+A” combination regimen as a first-line treatment for BCLC-C stage HCC, while other systemic combination regimens were considered as second-line treatment options.19,20
Transarterial chemoembolization (TACE) is widely used for the treatment of HCC worldwide and is globally recognized as a standard treatment for BCLC-B stage liver cancer.20,21 In clinical practice, over 50% of BCLC-C stage liver cancer patients have undergone TACE treatment, which has demonstrated significant clinical benefit compared to standard treatment.22,23 Tumor necrosis induced by TACE treatment promotes the release of tumor-associated antigens and increases the mRNA expression level of PD-(L)1.24,25 Consequently, the combination of local TACE treatment and systemic therapy has garnered attention, offering hope for improved therapeutic outcomes for patients with unresectable liver cancer. Several single-arm studies indicate that the objective response rate of TACE combined with MTT plus PD-(L)1 ranges from 46.7 to 68.2%; with progression-free survival (PFS) and median overall survival (OS) durations of 8.5–13.3 months and 14.0–24.0 months, respectively.26–31 In comparative studies, recent retrospective cohort studies comparing the efficacy of TACE combined with MTT plus PD-(L)1 versus MTT plus PD-(L)1 have shown increased ORR and prolonged PFS and OS.31–33
This study aims to retrospectively extract patient data from the hospital information system of a tertiary referral center. Specifically, the study focuses on patients who received MTT plus PD-(L)1 antibodies and those who underwent TACE combined with MTT plus PD-(L)1 antibodies.
Materials and Methods
Patients
This retrospective cohort study received approval from the Ethics Committee of Chinese PLA General Hospital (Approval number: S2023-313-01) and was registered in the Chinese Clinical Trial Registry (Registration number: ChiCTR2300073556) before initiation. This study was conducted in accordance with the principles outlined in the Declaration of Helsinki. The search terms “liver cancer”, “primary hepatocellular carcinoma”, and “liver malignant tumor” were employed to retrieve cases from January 2020 to May 2023 within the hospital information system of the first medical center of PLA General Hospital. Subsequently, we reviewed the retrieved medical records, and based on the inclusion and exclusion criteria, screened HCC patients who received either MTT plus PD-1/PD-L1 (systemic therapy) or TACE combined with MTT plus PD-(L)1 (combination therapy).
Inclusion and Exclusion Criteria
Eligible patients met the following criteria: 1) newly diagnosed primary liver cancer with clinical or pathological diagnosis criteria; 2) BCLC-B or BCLC-C HCC without a baseline surgical index; 3) age between 18 and 75 years, of either sex; 4) received MTT plus PD-(L)1 or TACE combined with MTT plus PD-(L)1; 5) underwent dynamic contrast-enhanced MRI of the liver at baseline and follow-up; 6) underwent imaging and clinical evaluation at least once, 8~16 weeks post-treatment initiation. In this study, MTT plus PD-(L)1 referred to the simultaneous implementation of PD-(L)1 and MTT within a 2-week interval. TACE combined with MTT plus PD-(L)1 referred to the initiation of TACE therapy within 4 weeks of PD-(L)1 or MTT employing standard conventional TACE therapy in an “on-demand” mode, considering liver function and physical status. No restrictions were imposed on the order of TACE and MTT plus PD-(L)1 antibodies initiation. Exclusion criteria were: 1) any malignancy in other systemic systems; 2) severe vital organ insufficiency such as the heart, brain, and kidney; 3) Child-Pugh grade C liver function, massive ascites, hepatic encephalopathy, or bleeding from esophageal and gastric varices within 6 months pre-treatment; 4) previous treatment with TACE, ablation, targeted therapy, immunotherapy, radiation therapy, or surgery; 5) loss to follow-up after the first visit.
Study Indexes
Following patient selection, we recorded baseline laboratory indicators, clinical information, and survival data. Laboratory indicators included blood routine, biochemistry panel, coagulation, and alpha-fetoprotein. We analyzed dynamic contrast-enhanced MRI of the liver at baseline and the first evaluation post-treatment. Baseline imaging assessment included lesion diameter, lesion count, portal vein tumor thrombus, and extrahepatic metastasis. We recorded the portal vein tumor thrombus (PVTT) according to the Cheng classification,34 ranging from type 1 to type 4. We defined in the present study tumor without PVTT as PVTT-0. Liver tumor burden was classified according to the “Up-to-7” criteria, with exceeding defined as a maximum diameter of intrahepatic tumors (cm) + number of lesions greater than or equal to 7.34 Tumor treatment response was assessed using mRECIST criteria,35 including complete response (CR), partial response (PR), stable disease (SD), and disease progression (PD). Treatment information included drug type, name, dose, administration cycle, number of TACE procedures, and whether surgery was performed. Adverse events were recorded based on the common terminology criteria for adverse events (CTCAE) version 5.0.36 Survival information was extracted from patient records, hospitalization records, and telephone follow-up information. Survival information of patients lost to follow-up was censored according to the time of the last visit or hospitalization in survival analysis.
Outcome Measurements
The primary outcome was the objective reaction rate (ORR) at the initial assessment post-treatment initiation. Secondary outcomes included progressive free survival (PFS), overall survival (OS) and grade-3 or higher adverse events (according to CTCAE definitions). ORR was defined as the proportion of CR plus PR cases relative to the total. PFS was defined as the time from treatment initiation to disease progression or death from any cause, whichever occurred first. OS was defined as the duration from treatment initiation to death from any cause.
Statistical Methods
Measurement data were summarized as median and interquartile range (IQR), while categorical data were presented as frequency and percentage. Continuous variables were compared using the independent t-test or Mann–Whitney U-test, depending on their distribution. The Chi-square test or Fisher’s exact test was applied for categorical variables.
Propensity score matching (PSM) was employed to balance potential confounders in comparing the overall response rate (ORR) between the two groups. Propensity scores were estimated using logistic regression, with treatment type (combination vs systemic therapy) as the dependent variable and clinically relevant covariates (eg, sex, age, hepatitis infection, AFP levels, “Up-to-7” criteria, PVTT classification, extrahepatic metastasis, and BCLC stage) as independent variables. A 1:1 nearest-neighbor matching algorithm with a caliper of 0.2 of the standard deviation of the logit of the propensity score was used without replacement. Covariate balance before and after matching was assessed using standardized mean difference (SMD), with an SMD < 0.1 indicating adequate balance.
Post-matching, odds ratios (ORs) for ORR were compared between groups. Subgroup analyses were conducted for sex, age (>65 years), AFP levels (>200 ng/mL), PVTT classification, extrahepatic metastasis, BCLC stage, and “Up-to-7” criteria.
Progression-free survival (PFS) and overall survival (OS) were compared using the Log rank test, and multivariate Cox proportional hazards models were employed to identify independent prognostic factors. Covariates included treatment group, age, sex, AFP levels, viral hepatitis status, extrahepatic metastasis, “Up-to-7” criteria, BCLC stage, PVTT classification, and surgical resection. Statistical significance was defined as p < 0.05, and all analyses were conducted using R software (version 4.2.2).
Results
Overall results
The study finally included 222 cases of HCC, comprising 109 cases in the systemic therapy group and 113 cases in the TACE combination therapy group. No significant differences were observed in the distribution of sex, mean age, viral hepatitis, TBIL, MELD score, CPS grade, AFP levels, and extra-hepatic metastasis between the therapy groups. However, there were statistically significant differences in the presence of PVTT and BCLC-class.
The median follow-up time was 15.1 months overall, with 18.6 months in the systemic therapy group and 13.2 months in the combination therapy group. The mean time from baseline to the first evaluation was 102 days in the systemic therapy group and 129 days in the combination therapy group. The mean number of TACE procedures before the first evaluation was 1.9 in the combination therapy group. The mean treatment cycle before evaluation was 4.7 in the systemic therapy group and 5.4 in the combination therapy group. The mean total cycle was 14.9 in the systemic therapy group and 19.3 in the TACE combination therapy group.
All PD-(L)1 agents included atezolizumab, sintilimab, pembrolizumab, teplizumab, tirelizumab, and camrelizumab. MTT agents included bevacizumab, lenvatinib, sorafenib, donafenib, and apatinib. In the systemic therapy group, the top three MTT plus PD-(L)1 combinations were sintilimab plus lenvatinib (87/109, 79.8%), atezolizumab plus bevacizumab (6/109, 5.5%), and pembrolizumab plus lenvatinib (5/109, 4.6%). In the TACE combination therapy group, the top three combinations were sintilimab plus lenvatinib (42/113, 40.8%), atezolizumab plus bevacizumab (17/113, 15.0%), and sintilimab plus bevacizumab (5/113, 4.4%).
A significant difference in the rate of surgical resection was observed between the two groups (p-value: <0.001), with a higher rate in the systemic therapy group (62%) compared to the combination therapy group (12%).
Objective Response Rate
Table 1 describes the baseline characteristics and their balance before and after PSM. The post-matching results indicate that PSM successfully balanced the baseline covariates between the combining therapy and systemic therapy groups, creating a total of 80 patients received systemic therapy, and a matched cohort of 80 patients received TACE combining therapy (Figure 1).
 |
Table 1 Baseline Covariates Before and After Matching |
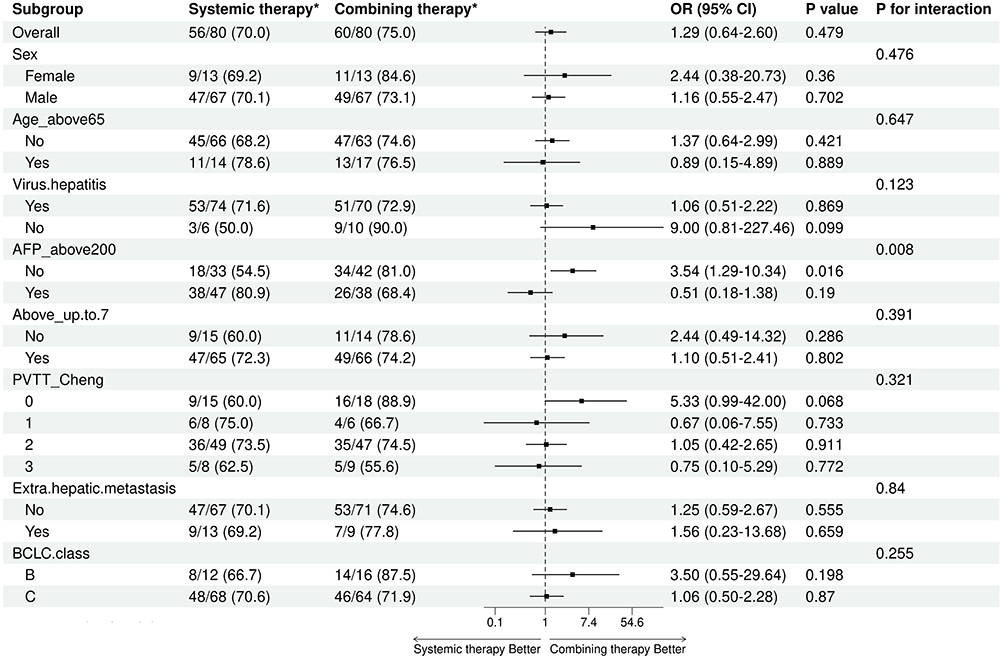 |
Figure 1 Forest plot of subgroup analysis of ORR: *no. of events/total no.(%). |
Of the 80 patients who received systemic therapy, 56 (70.0%) achieved ORR. In the combining therapy group, 60 out of 80 patients (75.0%) achieved ORR. Overall, the crude odds ratio (OR) for the ORR in the combining therapy group compared to the systemic therapy group was 1.29 (95% CI: 0.64–2.60; p-value: 0.479) without statistically significant.
However, the analysis revealed a significant interaction with alpha-fetoprotein (AFP) levels above 200 (P for interaction = 0.008), suggesting that the effect of the treatment might be different for patients with different AFP levels. In the subgroup of patients with AFP levels≤200, the combining therapy group had a notably higher response rate of 81.0% compared to 54.5% in the systemic therapy group. This difference translated into a statistically significant crude OR of 3.54 (95% CI: 1.29–10.34, P = 0.016), indicating that patients with lower AFP levels might respond significantly better to combining therapy relative to systemic therapy.
In the subgroup of patients without PVTT (PVTT-0), patients receiving combining therapy had a response rate of 88.9%, remarkably higher than the 60.0% response rate in the systemic therapy group. The crude OR was 5.33 with marginal significance (95% CI: 0.99–42.00, P=0.068).
Progression-Free Survival
In PFS analysis including comprising 109 cases in the systemic therapy group and 113 cases in the TACE combination therapy group, 121 events were recorded, with 64 events in the systemic therapy group and 57 in the combination therapy group. The median PFS was 15.4 months in the systemic therapy group and 13.1 months in the combination therapy group.
In the systemic therapy group, the PFS rates were 58.49% (95% CI: 49.14–69.63), 22.46% (95% CI: 13.61–37.07), and 10.11% (95% CI: 3.87–26.42) at 12, 24, and 36 months, respectively. In the combination therapy group, the PFS rates were 55.39% (95% CI: 46.05–66.61), 25.16% (95% CI: 15.03–42.11), and 18.87% (95% CI: 8.78–40.55) at 12, 24, and 36 months, respectively.
With Log rank test, the TACE combination therapy group exhibited an HR of 1.07 (95% CI: 0.75–1.54; p-value: 0.712) compared to the systemic therapy group. However, in the multivariate Cox regression model including age, sex, AFP, virus hepatitis, extrahepatic metastasis, “Up-to-7”, BCLC-stage, PVTT classification, and surgical resection as covariates, the combination therapy group demonstrated an HR of 0.68 (95% CI: 0.44–1.11; p-value: 0.131) compared to the systemic therapy group (Figure 2). Holding other covariates constant, patients with baseline AFP>200 ng/mL had a significantly increased HR of PFS compared to patients with AFP≤200 ng/mL (HR=1.68, 95% CI: 1.12–2.51; p-value: 0.012). Additionally, patients undergoing surgical resections had a significantly decreased HR of PFS compared to those who did not (HR=0.42, 95% CI: 0.26–0.68; p-value<0.001).
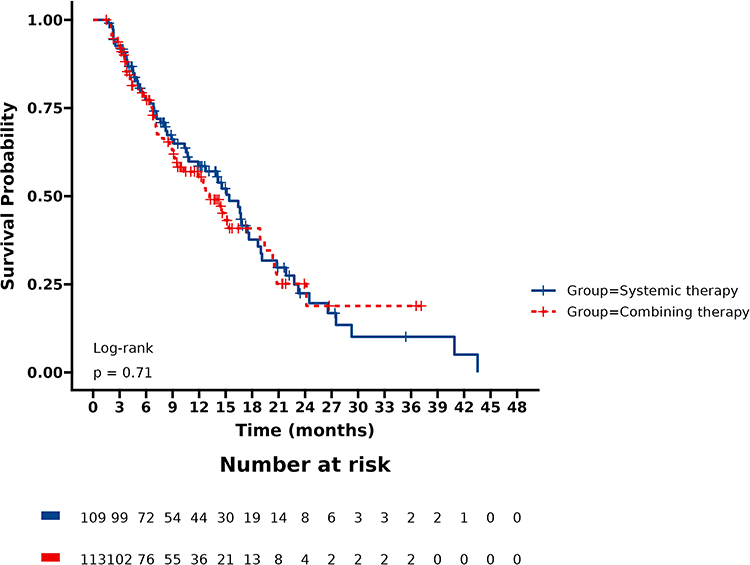 |
Figure 2 Kaplan–Meier analysis of progression-free survival. |
Overall Survival
A total of 43 deaths were recorded, comprising 23 deaths in the systemic therapy group and 20 deaths in the combination therapy group. The primary causes of death were liver failure, gastrointestinal bleeding, and infection.
In the systemic therapy group, the survival rates were 87.27% (CI: 80.76~94.30), 77.28% (CI: 68.49~87.21), and 63.57% (CI: 49.00~82.48) at 12, 24, and 36 months, respectively. In the combination therapy group, the survival rates were 87.19% (CI: 80.64~94.28), 73.22% (CI: 61.26~87.52), and 55.47% (CI: 35.68~86.25) at 12, 24, and 36 months, respectively. The median survival could not be calculated as less than half of the patients had experienced the event.
With Log rank test, the HR of OS for the TACE combination therapy group compared to the systemic therapy group was 1.19 (95% (CI): 0.64–2.20; p-value: 0.582). In the multivariate Cox regression model with age, sex, AFP, virus hepatitis, extrahepatic metastasis, “Up-to-7”, BCLC-stage, PVTT classification, and surgical resection as covariates, the HR decreased to 0.86 (95% CI: 0.42~1.76, p-value: 0.674) for the TACE combination therapy group compared to the systemic therapy group (Figure 3). Similar to the PFS analysis result, patients with baseline AFP>200 ng/mL had a significantly increased HR of OS compared to patients with AFP≤200 ng/mL (HR=2.33, 95% CI: 1.13–4.78; p-value: 0.021). Additionally, patients receiving surgical resection had a significantly decreased HR of OS compared to those not receiving surgical resections (HR=0.31, 95% CI: 0.14–0.68; p-value: 0.004).
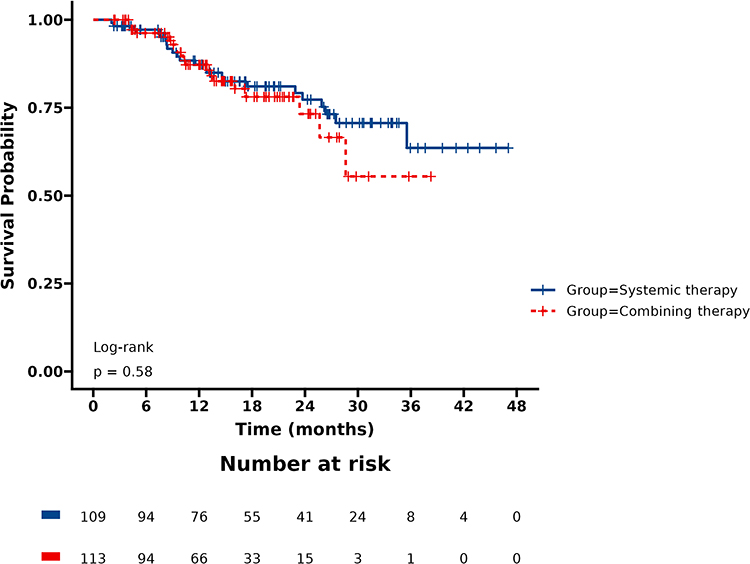 |
Figure 3 Kaplan–Meier analysis of overall survival. |
Adverse Events
During the follow-up period, 75 cases (33.8%) of grade 3 or higher adverse events (AEs) were observed, including 16 cases in the systemic therapy group and 59 cases in the combination therapy group. The incidence of grade 3 or higher AEs was significantly higher in the TACE combining group than the systemic group (52% vs 15%, p-value<0.0001). In the systemic therapy group, the three most common adverse events were rash, peeling of hands/feet, and hypertension. In the combination therapy group, the three most common adverse events were elevated ALT /AST, rash, and peeling of hands/feet. No adverse events leading to death were observed in either group during follow-up.
Discussion
This study reveals that patients treated with TACE combined with MTT plus PD-(L)1 exhibit a similar overall response rate (ORR) to those treated with MTT plus PD-(L)1 alone during the first follow-up. Few studies have directly compared the objective response between these two treatment modalities. A previous report suggested that TACE combined with apatinib plus camrelizumab significantly improved ORR and disease control rate (DCR) compared to apatinib plus camrelizumab alone in patients with unresectable HCC.36 However, the present study did not align with this report.
Tissue and serum VEGF levels have been significantly associated with overall survival in HCC.37,38 TACE-induced hypoxic environments stimulate the VEGF pathway, promoting neovascularization.38 When TACE is less effective, especially in cases with heavy tumor burden or advanced HCC, it may induce significant neoangiogenic reactions, vascular remodeling, and overgrowth of residual tumors, indicated by an increase in VEGF levels following treatment.39–41 A significant rise in serum VEGF shortly after TACE correlates with extrahepatic metastasis and poor outcomes.36 Furthermore, TACE has demonstrated limited efficacy in patients with intermediate-stage HCC exceeding the “Up-to-7” criteria.42
A recent multicenter retrospective cohort study demonstrated that TACE combined with systemic therapy for unresectable HCC achieved superior clinical outcomes compared to TACE alone.43 However, this result only confirmed the added value of systemic therapy in combination with TACE, which is not the standard treatment for advanced HCC. In advanced cases, the embolization effect may not be as effective as theoretically anticipated, as supported by a meta-analysis showing that hepatic arterial infusion chemotherapy (HAIC) outperforms TACE in advanced HCC patients.44 Even for intermediate-stage HCC, recent findings from a phase III trial revealed that FOLFOX-HAIC significantly improved overall survival, response rate, progression-free survival, and symptomatic progression-free survival compared to TACE.44
Although the TACE combination group did not demonstrate a significant overall advantage compared to systemic therapy, subgroup analyses provide critical insights. Patients with AFP ≤ 200 ng/mL exhibited higher odds of achieving an ORR with TACE combination therapy, as did patients without PVTT. The efficacy of TACE in intermediate-stage HCC without PVTT is well-recognized and widely recommended. In such cases, TACE is more likely to achieve complete embolic necrosis, resulting in higher ORR, which systemic therapy alone may struggle to achieve. Although there are no direct comparative studies of MTT combined with PD-(L)1 for intermediate-stage HCC, our subgroup results suggest that TACE remains an important component of treatment in cases without portal invasion.32
While few studies have compared the survival outcomes of TACE combined with MTT plus PD-(L)1 versus MTT plus PD-(L)1 alone, previous research has demonstrated that the combination improves median overall survival (mOS) and median progression-free survival (mPFS) in patients with advanced HCC.31,32 However, our study reveals similar PFS and OS between the two groups, challenging previous findings.
The effectiveness of TACE is particularly pronounced in patients with lower tumor burden or without PVTT. However, for patients with higher tumor burdens, TACE requires a more aggressive approach, including higher dosages of embolic agents. This can cause significant liver damage, reducing the opportunity for patients to receive alternative therapies and diminishing overall survival. Notably, a higher tumor burden is associated with a decrease in overall survival from 25.1 to 8.4 months following TACE treatment.45 Although liver function generally recovers post-TACE, its long-term impact on hepatic reserve remains uncertain. For HCC patients, most of whom have underlying cirrhosis, preserving liver function is crucial to survival.
The ORR and survival results in our study exceeded those reported in earlier studies. Previous single-arm observational studies reported an ORR of 46.7–68.2% for TACE combined with MTT plus PD-(L)1, with mPFS ranging from 8.5–13.3 months and mOS from 14.0–24.0 months.26–31 In our study, the overall ORR was 71.6%, with 75.2% in the TACE combination group and 67.9% in the MTT plus PD-(L)1 antibodies group. Comparative cohort studies on survival data revealed that the TACE combination group exhibited a median OS and PFS of 20.3 to 24.8 months and 7.4 to 12.1 months, respectively, compared to 10.5 to 13.1 months and 3.7 to 7.8 months in the MTT plus PD-(L)1 antibodies group.31,32 The mPFS was reported as 6.9 months in the IMbrave150 trial,17 6.8 months in the KEYNOTE-524 trial,18 and 4.6 months in the ORIENT-32 trial.14 In our study, the median PFS was 15.4 months in the systemic therapy group and 13.1 months in the combination therapy group. The mOS could not be calculated as fewer than half of the patients experienced the event during the median follow-up of 15.1 months, suggesting potential longer survival times in both groups.
On one hand, despite the “T+A” regimen being a guideline recommendation, actual clinical practice reveals various combination regimens with significant discrepancies among studies.46 In our study, the sindilizumab and lenvatinib combination was the most commonly used in both groups. Therefore, the variations in PFS and OS might be linked to the study cohorts’ characteristics or the selected targeted immune drugs. Reports indicate a median PFS of 11.3 months for lenvatinib plus sintilimab therapy in real-world practice.47 A multicenter retrospective study focusing on TACE combined with lenvatinib plus sintilimab in unresectable HCC reported a mPFS of 13.3 months, closely aligning with our findings.28 Another study investigating the efficacy and safety of TACE combining lenvatinib plus PD-(L)1 in advanced HCC achieved an objective response rate (ORR) of 69.3%.26 On the other hand, our study, like the previously mentioned studies, has a retrospective nature, carrying potential selection bias. It is conceivable that patients with accessible follow-up information or those who received follow-up were those with better treatment outcomes, potentially leading to an overestimation of the treatment effect, while those with poor outcomes may have been overlooked or missed.
Multivariate analysis identified AFP <200 ng/mL and surgical resection as independent positive factors associated with PFS and OS. Although AFP is not an ideal prognostic marker for HCC, it is the most frequently used biomarker in clinical management. AFP levels (with cut-off values of 200 ng/mL or 400 ng/mL) have repeatedly proven predictive or prognostic in various clinical scenarios, including transplantation.48
It has been reported that subsequent surgery can be feasible and safe for selected patients after downgrading through the combination of MTT and PD-(L)1. In a study by Zhang et al, 44 patients with unresectable recurrent HCC received MTT plus PD-(L)1 combination therapy, resulting in a median OS of 27.0 months and median PFS of 15.0 months.49 In another study by Zhu et al, 24 patients who underwent R0 resection were independently associated with a favorable overall survival in multivariate analysis.50 The median OS post-surgery was not reached in the median follow-up time of 23.4 months, compared to a median of 16 months in the non-surgery group. The overall survival rates observed in these two studies were numerically greater than those reported in the IMbrave150 trial (19.2 months) and the KEYNOTE-524 trial (22.4 months).17,18
Treatment-related side effects are important indicators for evaluating HCC treatment regimens. In this study, the incidence of grade 3 or higher adverse events was significantly higher in the TACE combination group compared to the systemic group. This elevation was attributed to the relatively high incidence of hepatocellular damage resulting from decreased artery infusion and local chemotherapy, evident in elevated ALT/AST levels, which constituted the most common adverse events in the TACE combination therapy group. Therefore, considering adverse events and potential liver damage is essential before contemplating the addition of TACE to the systemic therapy in the treatment regimen for unresectable HCC.
There were several limitations in this study. Firstly, being retrospective, it inherently includes biases of various origins, particularly selection bias, and confounders. Although regression analysis aids in mitigating the effects of covariates on primary results, it cannot eliminate unknown factors that may contribute to the endpoints. Another factor that needs to be addressed is the variety of MTT plus PD-(L)1 combinations. The uneven distribution of combinations between the two study arms might diminish the power of the study results. The follow up was relatively short.
Conclusion
Based on the study results and its retrospective nature, we conservatively conclude that no significant benefits were evident for unresectable HCC patients with simultaneous TACE combined with MTT plus PD-(L)1 compared to MTT plus PD-(L)1 alone. TACE might augment treatment value for a subgroup of patients with AFP≤200 ng/mL or without PVTT. A prospective randomized controlled trial is imperative before drawing a definitive conclusion.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Yang C, Zhang H, Zhang L, et al. Evolving therapeutic landscape of advanced hepatocellular carcinoma. Nat Rev Gastroenterol Hepatol. 2023;20(4):203–222. doi:10.1038/s41575-022-00704-9
2. Sahin TK, Rizzo A, Aksoy S, Guven DC. Prognostic significance of the Royal Marsden Hospital (RMH) score in patients with cancer: a systematic review and meta-analysis. Cancers. 2024;16(10):1835. doi:10.3390/cancers16101835
3. Villanueva A. Hepatocellular carcinoma. N Engl J Med. 2019;380(15):1450–1462. doi:10.1056/NEJMra1713263
4. Vogel A, Meyer T, Sapisochin G, et al. Hepatocellular carcinoma. Lancet. 2022;400(10360):1345–1362. doi:10.1016/S0140-6736(22)01200-4
5. Cheng AL, Kang Y-K, Chen Z, et al. Efficacy and safety of sorafenib in patients in the Asia-Pacific region with advanced hepatocellular carcinoma: a phase III randomised, double-blind, placebo-controlled trial. Lancet Oncol. 2009;10(1):25–34. doi:10.1016/S1470-2045(08)70285-7
6. Llovet JM, Ricci S, Mazzaferro V, et al. Sorafenib in advanced hepatocellular carcinoma. N Engl J Med. 2008;359(4):378–390. doi:10.1056/NEJMoa0708857
7. Kudo M, Finn RS, Qin S, et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: a randomised Phase 3 non-inferiority trial. Lancet. 2018;391(10126):1163–1173. doi:10.1016/S0140-6736(18)30207-1
8. El-Khoueiry AB, Sangro B, Yau T, et al. Nivolumab in patients with advanced hepatocellular carcinoma (CheckMate 040): an open-label, non-comparative, Phase 1/2 dose escalation and expansion trial. Lancet. 2017;389(10088):2492–2502. doi:10.1016/S0140-6736(17)31046-2
9. Zhu AX, Finn RS, Edeline J, et al. Pembrolizumab in patients with advanced hepatocellular carcinoma previously treated with sorafenib (KEYNOTE-224): a non-randomised, open-label Phase 2 trial. Lancet Oncol. 2018;19(7):940–952. doi:10.1016/S1470-2045(18)30351-6
10. Guven DC, Erul E, Kaygusuz Y. Immune checkpoint inhibitor-related hearing loss: a systematic review and analysis of individual patient data. Support Care Cancer. 2023;31(12):624. doi:10.1007/s00520-023-08083-w
11. Rizzo A, Ricci AD. Challenges and future trends of hepatocellular carcinoma immunotherapy. Int J Mol Sci. 2022;23(19):11363. doi:10.3390/ijms231911363
12. Yau T, Park J-W, Finn RS, et al. Nivolumab versus sorafenib in advanced hepatocellular carcinoma (CheckMate 459): a randomised, multicentre, open-label, phase 3 trial. Lancet Oncol. 2022;23(1):77–90. doi:10.1016/S1470-2045(21)00604-5
13. Finn RS, Ryoo B-Y, Merle P, et al. Pembrolizumab as second-line therapy in patients with advanced hepatocellular carcinoma in KEYNOTE-240: a randomized, double-blind, phase III trial. J Clin Oncol. 2020;38(3):193–202. doi:10.1200/JCO.19.01307
14. Ren Z, Xu J, Bai Y, et al. Sintilimab plus a bevacizumab biosimilar (IBI305) versus sorafenib in unresectable hepatocellular carcinoma (ORIENT-32): a randomised, open-label, phase 2-3 study. Lancet Oncol. 2021;22(7):977–990. doi:10.1016/S1470-2045(21)00252-7
15. Xu J, Shen J, Gu S, et al. Camrelizumab in combination with apatinib in patients with advanced hepatocellular carcinoma (RESCUE): a nonrandomized, open-label, phase II trial. Clin Cancer Res. 2021;27(4):1003–1011. doi:10.1158/1078-0432.CCR-20-2571
16. Rizzo A, Santoni M, Mollica V. Peripheral neuropathy and headache in cancer patients treated with immunotherapy and immuno-oncology combinations: the MOUSEION-02 study. Expert Opin Drug Metab Toxicol. 2021;17(12):1455–1466. doi:10.1080/17425255.2021.2029405
17. Cheng AL, Qin S, Ikeda M, et al. Updated efficacy and safety data from IMbrave150: atezolizumab plus bevacizumab vs. sorafenib for unresectable hepatocellular carcinoma. J Hepatol. 2022;76(4):862–873. doi:10.1016/j.jhep.2021.11.030
18. Finn RS, Qin S, Ikeda M, et al. Atezolizumab plus bevacizumab in unresectable hepatocellular carcinoma. N Engl J Med. 2020;382(20):1894–1905. doi:10.1056/NEJMoa1915745
19. Bruix J, Chan SL, Galle PR, et al. Systemic treatment of hepatocellular carcinoma: an EASL position paper. J Hepatol. 2021;75(4):960–974. doi:10.1016/j.jhep.2021.07.004
20. Reig M, Forner A, Rimola J, et al. BCLC strategy for prognosis prediction and treatment recommendation: the 2022 update. J Hepatol. 2022;76(3):681–693. doi:10.1016/j.jhep.2021.11.018
21. Rizzo A, Ricci AD, Brandi G. Trans-arterial chemoembolization plus systemic treatments for hepatocellular carcinoma: an update. J Pers Med. 2022;12(11):1788. doi:10.3390/jpm12111788
22. Park JW, Chen M, Colombo M, et al. Global patterns of hepatocellular carcinoma management from diagnosis to death: the BRIDGE study. Liver Int. 2015;35(9):2155–2166. doi:10.1111/liv.12818
23. Raoul JL, Forner A, Bolondi L, et al. Updated use of TACE for hepatocellular carcinoma treatment: how and when to use it based on clinical evidence. Cancer Treat Rev. 2019;72:28–36. doi:10.1016/j.ctrv.2018.11.002
24. Montasser A, Beaufrère A, Cauchy F, et al. Transarterial chemoembolisation enhances programmed death-1 and programmed death-ligand 1 expression in hepatocellular carcinoma. Histopathology. 2021;79(1):36–46. doi:10.1111/his.14317
25. Greten TF, Mauda-Havakuk M, Heinrich B, et al. Combined locoregional-immunotherapy for liver cancer. J Hepatol. 2019;70(5):999–1007. doi:10.1016/j.jhep.2019.01.027
26. Feng JK, Liu Z-H, Fu Z-G, et al. Efficacy and safety of transarterial chemoembolization plus antiangiogenic- targeted therapy and immune checkpoint inhibitors for unresectable hepatocellular carcinoma with portal vein tumor thrombus in the real world. Front Oncol. 2022;12:954203. doi:10.3389/fonc.2022.954203
27. Yang F, Yang J, Xiang W, et al. Safety and efficacy of transarterial chemoembolization combined with immune checkpoint inhibitors and tyrosine kinase inhibitors for hepatocellular carcinoma. Front Oncol. 2021;11:657512. doi:10.3389/fonc.2021.657512
28. Cao F, Yang Y, Si T, et al. The efficacy of TACE combined with lenvatinib plus sintilimab in unresectable hepatocellular carcinoma: a multicenter retrospective study. Front Oncol. 2021;11:783480. doi:10.3389/fonc.2021.783480
29. Liu J, Li Z, Zhang W, et al. Comprehensive treatment of trans-arterial chemoembolization plus lenvatinib followed by camrelizumab for advanced hepatocellular carcinoma patients. Front Pharmacol. 2021;12:709060. doi:10.3389/fphar.2021.709060
30. Teng Y, Ding X, Li W, et al. A retrospective study on therapeutic efficacy of transarterial chemoembolization combined with immune checkpoint inhibitors plus lenvatinib in patients with unresectable hepatocellular carcinoma. Technol Cancer Res Treat. 2022;21:15330338221075174. doi:10.1177/15330338221075174
31. Ju S, Zhou C, Yang C, et al. Apatinib plus camrelizumab with/without chemoembolization for hepatocellular carcinoma: a real-world experience of a single center. Front Oncol. 2021;11:835889. doi:10.3389/fonc.2021.835889
32. Wang J, Zhao M, Han G, et al. Transarterial chemoembolization combined with pd-1 inhibitors plus lenvatinib showed improved efficacy for treatment of unresectable hepatocellular carcinoma compared with PD-1 inhibitors plus lenvatinib. Technol Cancer Res Treat. 2023;22:15330338231166765. doi:10.1177/15330338231166765
33. Li H, Su K, Guo L, et al. PD-1 inhibitors combined with antiangiogenic therapy with or without transarterial chemoembolization in the treatment of hepatocellular carcinoma: a propensity matching analysis. J Hepatocell Carcinoma. 2023;10:1257–1266. doi:10.2147/JHC.S415843
34. Mazzaferro V, Llovet JM, Miceli R, et al. Predicting survival after liver transplantation in patients with hepatocellular carcinoma beyond the Milan criteria: a retrospective, exploratory analysis. Lancet Oncol. 2009;10(1):35–43. doi:10.1016/S1470-2045(08)70284-5
35. Llovet JM, Lencioni R. mRECIST for HCC: performance and novel refinements. J Hepatol. 2020;72(2):288–306. doi:10.1016/j.jhep.2019.09.026
36. Basch E, Reeve BB, Mitchell SA, et al. Development of the National Cancer Institute’s patient-reported outcomes version of the common terminology criteria for adverse events (PRO-CTCAE). J Natl Cancer Inst. 2014;106(9):dju244–dju244. doi:10.1093/jnci/dju244
37. Liu K, Min X-L, Peng J, et al. The changes of HIF-1alpha and VEGF expression after TACE in patients with hepatocellular carcinoma. J Clin Med Res. 2016;8(4):297–302. doi:10.14740/jocmr2496w
38. Schoenleber SJ, Kurtz DM, Talwalkar JA, et al. Prognostic role of vascular endothelial growth factor in hepatocellular carcinoma: systematic review and meta-analysis. Br J Cancer. 2009;100(9):1385–1392. doi:10.1038/sj.bjc.6605017
39. Sergio A, Cristofori C, Cardin R, et al. Transcatheter arterial chemoembolization (TACE) in hepatocellular carcinoma (HCC): the role of angiogenesis and invasiveness. Am J Gastroenterol. 2008;103(4):914–921. doi:10.1111/j.1572-0241.2007.01712.x
40. Shim JH, Park J-W, Kim JH, et al. Association between increment of serum VEGF level and prognosis after transcatheter arterial chemoembolization in hepatocellular carcinoma patients. Cancer Sci. 2008;99(10):2037–2044. doi:10.1111/j.1349-7006.2008.00909.x
41. Hsieh MY, Lin ZY, Chuang WL. Serial serum VEGF-A, angiopoietin-2, and endostatin measurements in cirrhotic patients with hepatocellular carcinoma treated by transcatheter arterial chemoembolization. Kaohsiung J Med Sci. 2011;27(8):314–322. doi:10.1016/j.kjms.2011.03.008
42. Kokudo N, Takemura N, Hasegawa K, et al. Clinical practice guidelines for hepatocellular carcinoma: the Japan Society of Hepatology 2017 (4th JSH-HCC guidelines) 2019 update. Hepatol Res. 2019;49(10):1109–1113. doi:10.1111/hepr.13411
43. Zhu HD, Li H-L, Huang M-S, et al. Transarterial chemoembolization with PD-(L)1 inhibitors plus molecular targeted therapies for hepatocellular carcinoma (CHANCE001). Signal Transduct Target Ther. 2023;8(1):58. doi:10.1038/s41392-022-01235-0
44. Liu J, Zhang J, Wang Y, et al. HAIC versus TACE for patients with unresectable hepatocellular carcinoma: a systematic review and meta-analysis. Medicine. 2022;101(51):e32390. doi:10.1097/MD.0000000000032390
45. Borde T, Nezami N, Laage Gaupp F, et al. Optimization of the BCLC staging system for locoregional therapy for hepatocellular carcinoma by using quantitative tumor burden imaging biomarkers at MRI. Radiology. 2022;304(1):228–237. doi:10.1148/radiol.212426
46. Ciliberto D, Caridà G, Staropoli N, et al. First-line systemic treatment for hepatocellular carcinoma: a systematic review and network meta-analysis. Heliyon. 2023;9(8):e18696. doi:10.1016/j.heliyon.2023.e18696
47. Zhao L, Chang N, Shi L, et al. Lenvatinib plus sintilimab versus lenvatinib monotherapy as first-line treatment for advanced HBV-related hepatocellular carcinoma: a retrospective, real-world study. Heliyon. 2022;8(6):e09538. doi:10.1016/j.heliyon.2022.e09538
48. Ozdemir F, Baskiran A. The Importance of AFP in Liver Transplantation for HCC. J Gastrointest Cancer. 2020;51(4):1127–1132. doi:10.1007/s12029-020-00486-w
49. Zhang Z, Jiao T, Li J, et al. Efficacy of treatment based on TKIs in combination with PD-1 inhibitors for unresectable recurrent hepatocellular carcinoma. World J Surg Oncol. 2023;21(1):53. doi:10.1186/s12957-023-02939-5
50. Zhu XD, Huang C, Shen Y-H, et al. Hepatectomy after conversion therapy using tyrosine kinase inhibitors plus anti-PD-1 antibody therapy for patients with unresectable hepatocellular carcinoma. Ann Surg Oncol. 2023;30(5):2782–2790. doi:10.1245/s10434-022-12530-z
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.