Back to Journals » ClinicoEconomics and Outcomes Research » Volume 18
Comparative Cost Analysis of Ambulance Utilization: Advanced Life Support (ALS) vs Basic Life Support (BLS) at King Abdulaziz Medical City, Riyadh
Authors Alabdali A ![]() , Alharkan M
, Alharkan M
Received 16 October 2025
Accepted for publication 15 January 2026
Published 20 January 2026 Volume 2026:18 570790
DOI https://doi.org/10.2147/CEOR.S570790
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Giorgio Colombo
Abdullah Alabdali,1– 3 Mohammed Alharkan3
1Emergency Medical Services Department, College of Applied Medical Sciences, King Saud bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia; 2King Abdullah International Medical Research Center, Riyadh, Saudi Arabia; 3Department of Emergency Medicine, Emergency Medical Services, King Abdulaziz Medical City, Ministry of National Guard-Health Affairs, Riyadh, Saudi Arabia
Correspondence: Abdullah Alabdali, College of Applied Medical Sciences, King Saud bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia, Tel +966114295252, Email [email protected]
Purpose: Unit-hour utilization (UHU) is the most common metric for evaluating the productivity of ambulances and crews for ambulance services. Calculating UHU is essential for maximizing profitability and evaluating the number of hours of ambulance utilization during a shift. This has not been examined previously at King Abdulaziz Medical City (KAMC). KAMC is a major tertiary-care medical center in Riyadh, Saudi Arabia, with dedicated ALS (Advanced Life Support) and BLS (Basic Life Support) ambulance units. This study aimed to determine the cost of operating the emergency calls (advanced life support [ALS]) unit and non-emergency calls (basic life support [BLS]) unit and compare the costs of emergency calls (ALS) and non-emergency calls (BLS). The study used a standardized institutional checklist that itemizes expenditures across logistics, equipment, maintenance, salary, pharmacy, and fuel cost components.
Methods: This was a retrospective cross-sectional study. Institutional Review Board approval was obtained from King Abdullah International Medical Research Center. The study examined emergency and non-emergency calls for a period of 12 months. This study was based on a checklist assessing various expenditures to calculate the cost of ambulance utilization at KAMC in 2022.
Results: The total average ambulance utilization cost per year for ALS was 4,806,245.7 SR, and the average ambulance utilization cost per hour was 548.65 SR; these costs were to operate the ALS crew for 24 hours, seven days a week. Conversely, the total average ambulance utilization cost per year for BLS was 3,934,156.92 SR, and the average ambulance utilization cost per hour was 449.10 SR. The main expenses concerned salaries and overhead costs for ALS and BLS.
Conclusion: This study provides insights into the cost of ambulance utilization between ALS and BLS. The higher cost of ALS calls may be attributed to the higher level of training, equipment, and staffing required.
Keywords: ambulance, economics, ambulance utilization and healthcare cost
Introduction
Emergency Medical Services (EMS) is the system that offers emergency medical care. Its primary objective is to provide care to patients in response to significant illness or injury. EMS is most visibly identified through emergency vehicles but encompasses a broader, coordinated system involving many people and organizations. A complete EMS system operates daily, prepared for all emergencies.
Traditionally, contacting EMS involves calling 911 to transfer patients to larger hospitals for advanced care. EMS manages multiple intravenous drips, medications, ventilators, and other critical interventions. Paramedics also lead educational programs, CPR, stop-the-bleed courses, and provide community paramedic services.1
Both emergency and non-emergency calls are vital to the healthcare system but differ significantly in cost. Emergency calls, involving life-threatening situations, require highly trained responders and immediate action, resulting in higher costs. Non-emergency calls, involving stable patients or minor issues, typically use EMTs and are less costly. Understanding these cost differences helps organizations allocate resources efficiently and manage healthcare services.2
EMS is often the first point of contact in emergencies. Over the past decade, Saudi EMS has seen improvements; however, it still faces ongoing challenges such as limited analysis, community engagement, and professional academic standing. To date, no published study has quantified the operating costs of ALS and BLS ambulances within the Saudi healthcare system. Establishing these baseline values supports evidence-based resource allocation and planning. These challenges lead to inconsistent statistics on response times and patient transfers. In Saudi Arabia, dispatchers cannot reject calls due to a lack of policy, resulting in wasted resources and higher system costs.3
Unit-hour utilization (UHU) is the primary metric to assess ambulance productivity. Focusing on UHU helps optimize profitability and utilization during shifts.4
Ambulance services are crucial for emergency care but can be financially burdensome, especially where socialized healthcare is lacking. Costs vary by location, ambulance type, care level, and distance. ALS is generally costlier than BLS. Cost-reduction strategies include community paramedicine, telemedicine, alternative transport, enhanced triage, and improved data analysis.5
This study analyzed the costs and utilization of ALS and BLS ambulance services at King Abdulaziz Medical City (KAMC), Riyadh. Its objective was to compare operational costs between emergency and non-emergency units.
A Malaysian study (March–December 2019) assessed ambulance costs in MOH facilities, covering 239 ambulances across 144 hospitals and 698 clinics. A cross-sectional design was used. Utilization was measured by trips, distance, and duration. Costs included salaries, maintenance, fuel, overheads, and consumables. Average costs were $2,756.12 for hospitals and $2,312.65 for clinics, with salaries being the largest expense (44% in hospitals, 42% in clinics). Clinics showed higher median trips (31.88) and usage hours (58.58) than hospitals (16.25 trips, 39.35 hours).6 A US study in Maryland examined pediatric emergency transfers from remote EDs to PEDs. It analyzed 352 transfers from July 2009 to June 2010, focusing on cases discharged within 12 hours without intervention. Of these, 108 (30.7%) were admitted, 42 (11.9%) went to ICU, 36 (10.2%) had surgery, and 166 (47.2%) were discharged. The average hospital fee per transfer was $4,843. Most costs (89%) were fixed; 11% were variable. For the 101 patients discharged within 12 hours without assistance, hospital costs totaled $489,143.6
Material and Methods
Study Setting
Data on the costs of ambulance emergency ALS units versus non-emergency BLS units were collected from King Abdulaziz Medical City (KAMC).
Data Collection
The data collected from the dispatcher system can provide valuable information, such as the number of transfers and the type of ambulance used. Data were collected using a checklist comprising six parts—logistics supplies and equipment, maintenance, salary, gas station, pharmacy, and dispatcher system, which contains the number of transfers for both BLS and ALS are detailed in Table 1. Logistics provides information on ambulance prices, equipment, medical supplies, and vehicle (ambulance) depreciation. Overhead expenses, such as electricity and water bills, furniture, and other items, can also be identified through logistics. Maintenance provides information on scheduled maintenance for the ambulances, as well as the cost of maintenance and spare parts. Gas station provides data on fuel consumption, whereas pharmacy provides information on the cost of medications in an EMS box. The fire station provides information on the costs of fire alarms and fire extinguishers in the EMS department, and the IT department provides information on the costs of desktop computers, components, and Internet access. Salary information was obtained from the Unified Healthcare Salary Scale and used to calculate costs.
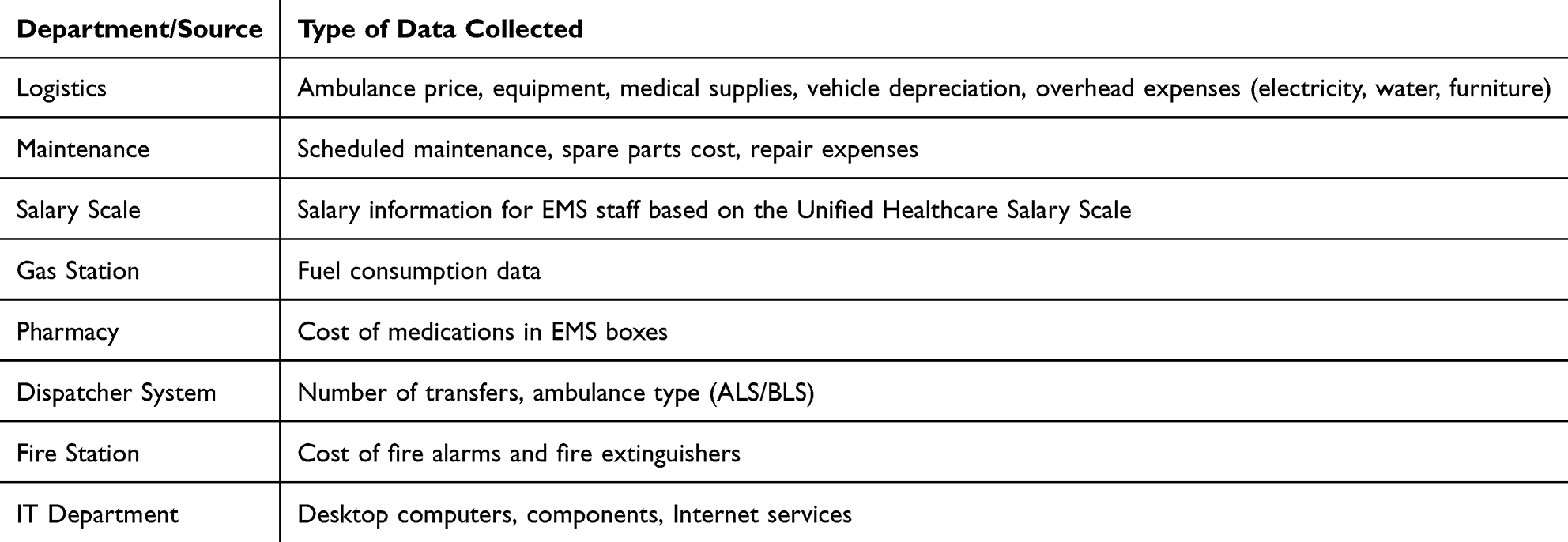 |
Table 1 Summary of Data Collected for ALS and BLS Ambulance Cost Analysis (2022) |
All data reflect actual operational and expenditure records for ALS and BLS units from January to December 2022 and were extracted by authorized EMS administrative personnel. All cost values represent actual documented expenditures from relevant KAMC departments. Currency conversions to USD were based on the average 2022 exchange rate published by the Saudi Central Bank.
Results
The cost of ambulance utilization hours for BLS ambulances in KAMC was estimated to be 449.10 SR per hour (approximately 119.76 US dollars per hour). A comparison of average ambulance utilization cost per hour between ALS and BLS units is illustrated in Figure 1. This cost includes various factors, such as ambulance price, maintenance cost, fuel cost, medical supplies, salary, and overhead expenses. The total operating cost for a BLS ambulance, including all the aforementioned factors and overhead, was calculated to be 3,934,156.92 SR per year (approximately 1,049,108.51 US dollars per year) as summarized in (Table 2).
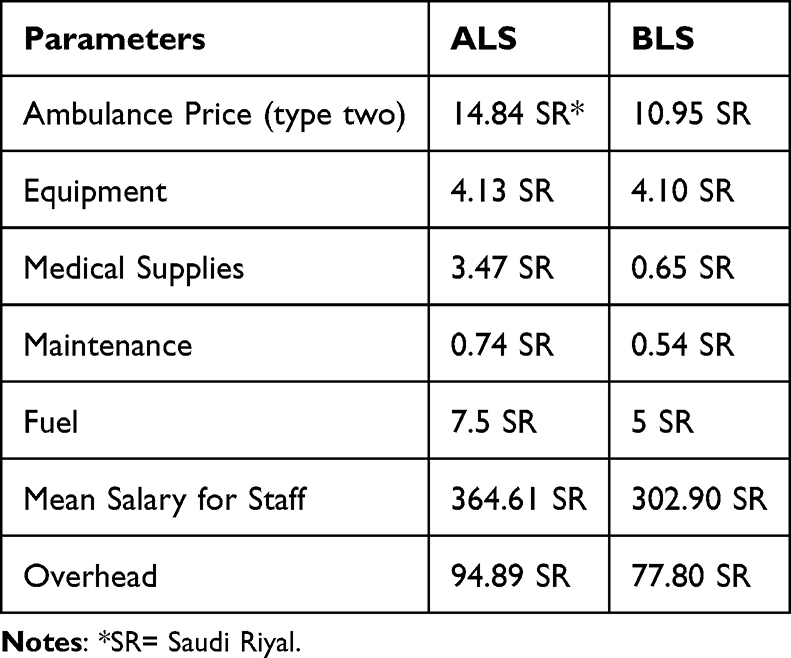 |
Table 2 Average Ambulance Utilization Cost per Hour |
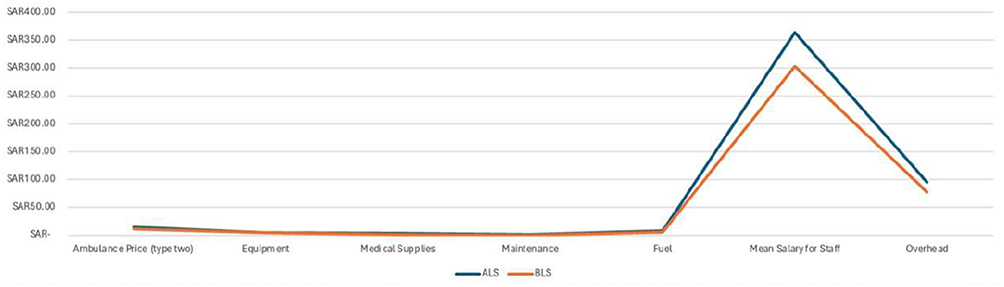 |
Figure 1 Average Ambulance Utilization Cost per Hour. |
The study also found that it would require eight full time employees to operate one ambulance and four staff members to cover holiday and annual vacations, with an average cost of 2,983,982.4 SR per year (approximately 795,728.64 US dollars per year) for BLS ambulance staff. These staff members operate the ambulance 24 hours/7 days.
Regarding ALS, the cost of UHU for ambulances in KAMC was estimated to be 548.65 SR per hour (approximately 146.30 US dollars per hour). This cost includes various factors, such as ambulance price, maintenance cost, fuel cost, medical supplies, salary, and overhead expenses. The total operating cost for an ALS ambulance, including all the aforementioned factors, was calculated to be 4,806,245.7 SR per year (approximately 1,281,665.52 US dollars per year). The comparison of average ambulance utilization cost per year between ALS and BLS units is illustrated in Figure 2. The study also found that operating one ALS ambulance would require 12 full time employees. These findings provide important insights into the cost of ambulance utilization for ALS ambulances in KAMC, which may help inform resource allocation and budgeting decisions for EMS in this region are presented in (Table 3).
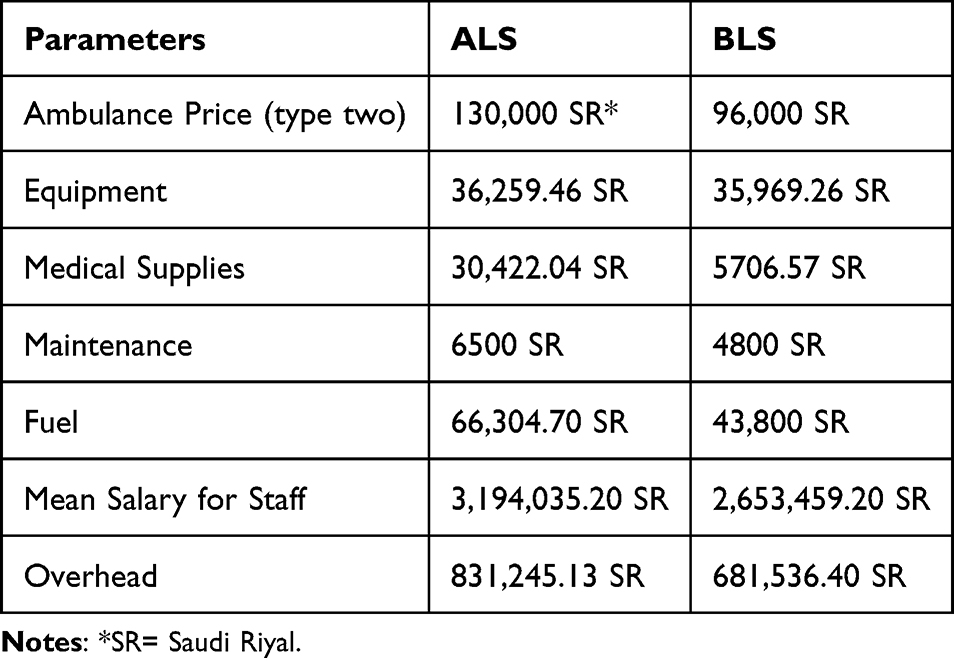 |
Table 3 Average Ambulance Utilization Cost per Year |
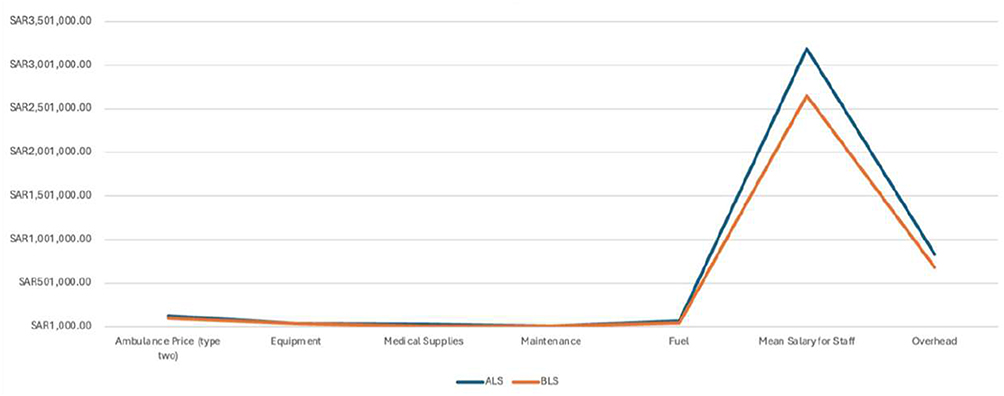 |
Figure 2 Average Ambulance Utilization Cost per Year. |
Discussion
Regarding the cost of UHU of the ambulance services at KAMC, emergency ALS units were found to be costlier than non-emergency BLS units. ALS was more expensive but provided better high-quality care than BLS. The patterns of hospital and pre-hospital healthcare services in Saudi Arabia differ, as reflected in the patterns of ambulance utilization. A study conducted in Malaysia examined the distance and duration of travel in ambulances. The average total cost of ambulance service was MYR 11,410.44 (2,756.14 US dollars) for hospitals.7 In the present study, the average total cost of ambulance utilization for BLS transfer was 3,934,156.92 SR (approximately 1,049,108.51 US dollars) per year, and the UHU was 449.10 SR per hour (119.76 US dollars), including equipment, maintenance, medical supplies, salaries, and other components. Additionally, another study in Maryland state examined the cost of care in pediatric transfers from the ED to the PED or discharge to home. The average hospital charge for these transfers was 489,143 US dollars, and the UHU was 60.83 US dollars.6 In our study, the average cost of ambulance utilization for ALS was 4,806,245.7 SR (approximately 1,281,665.52 US dollars) per year, and the UHU was 548.65 SR (146.30 US dollars). If all units were operated by ALS, it would improve the quality of care provided to patients. However, the cost difference between operating the ambulance fleet with BLS versus ALS is significant, with the total cost being 872,088.78 SR per year (232,557 US dollars) to operate the units with ALS and provide high-quality care. These cost differences can guide decisions on staffing allocation and service configuration to balance resource use with quality of care. These findings may assist EMS administrators in evaluating staffing models and planning budgets for ALS and BLS services. Moreover, a study conducted in Iran found that the total cost of ground ambulance transfer and treatment of patients was 412.88 US dollars.8 Conversely, the cost for ALS in our study was 548.65 SR per hour (146.30 US dollars), and that for BLS was 449.10 SR per hour (119.76 US dollars). This difference is likely due to the healthcare provided to the patients. BLS usually provides basic care, whereas ALS provides many advanced procedures and administers medications that make the cost higher than that of BLS.
There were differences in many studies worldwide; these studies have primarily focused on ambulance utilization in EMS; in China to investigate EMS utilization a study has found the total cost to be 11,190 US dollars.9
In the current study, the annual ALS unit cost at KAMC was estimated to be 4,806,245.7 SR (approximately 1,281,665.52 US dollars). KAMC covers many places and responds to many cases in the MNGHA area to provide high-quality care to their employees and their families and to cover events by EMS. Interestingly, the cost of ambulance services in Saudi Arabia is higher than that in Denmark, which was estimated to be 266 US dollars for two years.10 By contrast, in our study in 2022, BLS utilization costs were estimated to be 449.10 SR per hour (approximately 119.76 US dollars per hour), and ALS utilization costs were estimated at 548.65 SR per hour (approximately 146.30 US dollars per hour).
This could be due to various factors such as differences in healthcare systems, technology, staffing, and equipment costs. Notably, the cost of ambulance services can vary widely depending on the level of care needed, location, and type of service provided. This study aimed to investigate the costs of EMS transport in different regions. A study published in 2016 analyzed ambulance service costs in the United States between 2007 and 2011 and found that the average cost of ambulance utilization hours was approximately 667 US dollars. The study identified staffing, fuel, and maintenance as factors contributing to the cost.10
Comparing that with the current study, we observe that the cost of EMS UHU is significantly higher in the United States than in Saudi Arabia. However, it is important to note that the two studies were conducted during different time periods, and other factors may have contributed to the difference in cost. Additionally, the differences in healthcare systems and infrastructure between the two regions should be considered, which may also affect the cost of EMS transport.
A study conducted in France found that the average cost of an ambulance utilization hour ranged from €150 to €600 (164.27–657.06 US dollars), depending on the level of EMS response required.10 The study identified factors such as the level of training and equipment required and the salaries of medical personnel as contributing to the cost. Compared with the UHU results in our study, the cost of EMS response and patient transport in Saudi Arabia is higher than that in France. Several factors may contribute to the difference in costs between these two countries, such as differences in healthcare systems, quality of care, equipment availability, and personnel salaries.
Furthermore, the cost of the EMS response and patient transport in Saudi Arabia may have increased since the data were collected. Overall, these results highlight the importance of investigating the cost of EMS response and patient transport in different countries to better understand the factors that contribute to the cost and identify opportunities to improve efficiency and reduce costs.
Limitation
This study encountered several limitations. The foremost limitation was the issue of data availability. The acquisition of accurate and comprehensive data pertaining to ambulance utilization proved to be a challenging task. Moreover, the cost components associated with ambulances and utilization services can be multifaceted, encompassing personnel, equipment, maintenance, and fuel costs, among others. Ascertaining the precise cost allocation for each component can be a formidable undertaking. Additionally, the study faced a dearth of time due to the considerable amount of data that needed to be collected, posing further limitations. This study was descriptive in nature and did not involve inferential statistical testing.
Conclusion
In conclusion, this study’s findings indicate that ambulance utilization with ALS is more expensive than with BLS due to the higher levels of training, equipment, and staffing required for ALS services. These insights can help healthcare providers and policymakers develop strategies to manage and reduce ambulance utilization costs while maintaining high-quality emergency medical care. Additionally, further research is essential to explore the cost-effectiveness of various EMS models and identify methods to optimize ambulance services, ultimately improving patient outcomes and reducing costs. Future studies may employ analytical or cost-effectiveness models to evaluate system-level optimization.
Abbreviations
ALS, Advanced Life Support; BLS, Basic Life Support; CPR, Cardiopulmonary Resuscitation; ED, Emergency Department; EMS, Emergency Medical Services; EUR, Euro; ICU, Intensive Care Unit; IRB, Institutional Review Board; KAMC, King Abdulaziz Medical City; KAIMRC, King Abdullah International Medical Research Center; KSAU-HS, King Saud bin Abdulaziz University for Health Sciences; MNGHA, Ministry of National Guard, Health Affairs; MOH, Ministry of Health; MYR, Malaysian Ringgit; PED, Pediatric Emergency Department; SR, Saudi Riyal; UHU, Unit-Hour Utilization; US, United States; USD, United States Dollar.
Acknowledgments
The authors wish to acknowledge the invaluable support provided by King Saud University, King Abdulaziz Medical City, and King Abdullah International Medical Research Center for facilitating this study. The authors would like to acknowledge Mr. Shujaa Almutairi, Mr. Nawaf Alanazi, Mr. Hatim Alotaibi and Dr. Zainab Alhussaini for their support during data collection.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Cheung V. How to unlock EMS profitability by using utilization rate. Available from: https://traumasoft.com/ems-best-practices/how-to-use-utilization-rate-to-unlock-ems-profitability/.
2. Brown LHBL. Paramedic determinations of medical necessity: a meta-analysis. Prehospital Emergency Care. 2015;2015:1.
3. CSG Justice Center. Conducting emergency and non-emergency call triage. 2022, Available from: https://csgjusticecenter.org/publications/expanding-first-response/the-toolkit/call-triage/.
4. Maine. What is EMS? Maine Emergency Medical Services. Available from: https://www.maine.gov/ems/whatisems.
5. Qawwas L-A-A, Algaribi SA, Haliq SAA, Almufareh B, Almakhalas KM. An analysis of cost and time for non-emergency calls: a retrospective study on the Emergency Medical Services Resources Management. J Emergency Med Trauma Acute Care. 2023;2023:3.
6. Gattu RK, De Fee AS, Lichenstein R, Teshome G. Consideration of cost of care in pediatric emergency trans-fer-an opportunity for improvement. Pediatric Emergency Care. 2023;2023:2.
7. Bahari MS, Aminuddin F, Raman S, et al. Analysis of costs and utilization of ambulance services in the Ministry of Health Facilities, Malaysia. PLoS One. 2022;17(11):e0276632. doi:10.1371/journal.pone.0276632
8. Is LKM. Non-urgent emergency callers: characteristics and Prognosis. Prehospital Emergency Care. 2020;2020:1
9. Solberg R, Edwards BL, Chidester JP, Perina DG, Brady WJ, Williams MD. The prehospital and hospital costs of emergency care for frequent Ed patients. Am J Emergency Med. 2015;34(3):459–7. doi:10.1016/j.ajem.2015.11.066
10. Association of EMS Physici N, National Association of EMS Physicians. Reimbursement for EMS response, medical care, and transport. Prehosp Emerg Care. 2011;15(4):545–548. doi:10.3109/10903127.2011.598624
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.