Back to Journals » Clinical Ophthalmology » Volume 20
Comparative Clinical Outcomes of Radiofrequency, Intense Pulsed Light, and Combined Therapy for Meibomian Gland Dysfunction-Related Dry Eye
Authors Tsai J
Received 5 November 2025
Accepted for publication 28 May 2026
Published 10 June 2026 Volume 2026:20 577318
DOI https://doi.org/10.2147/OPTH.S577318
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sotiria Palioura
Jennifer Tsai
Dry Eye and Ocular Surface Center, LINE of SIGHT, New York, NY, USA
Correspondence: Jennifer Tsai, Dry Eye and Ocular Surface Center, LINE of SIGHT, New York, NY, USA, Email [email protected]
Purpose: To evaluate and compare the clinical effectiveness of radiofrequency (RF), intense pulsed light (IPL), and combined RF+IPL therapy in patients with dry eye disease (DED) associated with Meibomian Gland Dysfunction (MGD), using real-world data from a high-volume ophthalmic clinic.
Patients and Methods: This retrospective cohort study included 286 adult patients diagnosed with MGD-related DED who received treatment between August 2022 and August 2024. Patients were divided into three groups based on the treatment modality administered: RF alone, IPL alone, or combined RF+IPL. Clinical outcomes were assessed using the Ocular Surface Disease Index (OSDI), the Standard Patient Evaluation of Eye Dryness (SPEED) questionnaire, tear break-up time (TBUT), and Meibomian gland score (MGS), measured before intervention (baseline), 1 month and 3 months post-treatment. Statistical comparisons were performed within and between groups to assess treatment efficacy.
Results: All treatment groups showed statistically significant improvements from baseline to 4 weeks in OSDI, SPEED, TBUT, and MGS scores (p < 0.001). MGS improved within all groups, although the group-by-time interaction did not reach statistical significance. In the combined RF+IPL group, OSDI decreased from 22.70 to 3.61, SPEED from 18.17 to 5.25, TBUT increased from 7.29 to 11.54 seconds, and MGS from 25.00 to 29.63. Improvements were greatest in the combined group across most outcome domains. No serious adverse events occurred.
Conclusion: Energy-based therapies represent an effective, non-invasive approach for managing MGD-related DED. The combined RF+IPL treatment demonstrated superior outcomes across most clinical domains compared to monotherapies, including the greatest improvement in gland function. These findings support its integration into routine clinical dry eye care and underscore the value of personalized, technology‑driven treatment approaches in modern ophthalmology.
Keywords: dry eye disease, DED, Meibomian gland dysfunction, MGD, radiofrequency, RF, intense pulsed light, IPL, combination therapy, non-invasive treatment
Introduction
Dry Eye Disease (DED) is a common, multifactorial disorder of the ocular surface that affects an estimated 5% to 33% of adults worldwide,1 with prevalence increasing with age and screen exposure.2,3 Characterized by a loss of tear film homeostasis and associated ocular symptoms, DED can lead to visual disturbances, chronic discomfort, and a significant decline in quality of life.4 In addition to the personal burden, DED contributes to an estimated $2 billion annually in direct healthcare costs in the United States alone.5
Among the various etiologies of DED, Meibomian Gland Dysfunction (MGD) accounts for approximately 65% of cases, making it the leading cause of evaporative dry eye.6,7 The meibomian glands secrete lipids that form the outermost layer of the tear film, which serves to retard tear evaporation and stabilize the ocular surface.8 Dysfunction of these glands—due to obstruction, inflammation, or altered lipid composition—results in insufficient lipid secretion, increased tear evaporation, and downstream inflammatory cascades.9
A hallmark of MGD is the alteration of the physical properties of the meibum, the oily secretion produced by the glands. In healthy individuals, meibum transitions to a fluid state below eyelid temperature (~33°C), allowing efficient spread across the ocular surface.10 However, in MGD, changes in lipid composition raise the phase-transition temperature, rendering the meibum abnormally viscous and gel-like, prone to gland obstruction.11,12 This contributes to gland obstruction and reduced lipid delivery. Heating the eyelids to above the pathological phase-transition temperature can liquefy the meibum, improve gland expressibility, and enhance tear film stability.13
Conventional treatments such as warm compresses and thermal pulsation devices are often recommended as first-line therapies, but they are limited by poor patient adherence, variability in temperature delivery, and often transient or clinically insignificant improvement.13–15 Automated thermal therapies like radiofrequency (RF) and intense pulsed light (IPL) have emerged as alternative approaches that provide controlled, targeted energy delivery, though their comparative effectiveness to other modalities has not been established.
Importantly, RF therapy is uniquely suited for treating eyelid anatomy because of its ability to deliver bipolar electrical energy to the dermis and subcutaneous tissues of the periocular region, including the meibomian glands. This heating mechanism not only melts viscous meibum but may also induce tissue remodeling and glandular rejuvenation.15 IPL, though originally developed for dermatologic use, has demonstrated anti-inflammatory and vascular-modulating effects in the treatment of MGD.16,17
Despite increasing clinical interest, there remains a gap in the literature: while small prospective studies and case series suggest both RF and IPL can improve dry eye parameters, there is limited evidence from large-scale, well-controlled studies using multimodal clinical endpoints. No prior study has directly compared RF, IPL, and combination therapy using validated symptom scores, gland imaging, and ocular surface measures in a single design.
To our knowledge, this is the largest, age-adjusted, three-arm real-world cohort study evaluating the comparative effectiveness of RF, IPL, and combination RF+IPL therapy for MGD-associated DED. The objective of this retrospective cohort study was to assess both subjective and objective clinical outcomes using multimodal endpoints and determine whether combination energy-based therapy provides a measurable advantage over monotherapy.
Materials and Methods
Study Design and Setting
This retrospective, observational cohort study was conducted at LINE OF SIGHT, a specialty ophthalmology clinic, and evaluated the outcomes of three energy-based treatment modalities—radiofrequency (RF), intense pulsed light (IPL), and their combination—for dry eye disease (DED) associated with Meibomian Gland Dysfunction (MGD). The analysis was based on real-world clinical data collected between August 1, 2022, and August 1, 2024. The study complies with the Declaration of Helsinki and the protocol received approval from a centralized Institutional Review Board (IRB), SterlingIRB, [IRB #: 12222-JTsai, protocol: DO613929A]. A waiver of informed consent was obtained in accordance with regulatory guidelines for retrospective minimal-risk studies. Patients were not randomized; treatment modality was determined by routine clinical decision-making and patient preference. These treatments were generally paid for out‑of‑pocket as elective procedures.
Study Population
Medical records of approximately 300 adult patients aged 18 years and older were screened for eligibility. After applying the exclusion criteria, 286 patients were enrolled in the study. Inclusion criteria required patients to have undergone at least one treatment with RF (Forma / Forma-I) and/or IPL (Lumecca / Lumecca-I) within the study period and to have at least two documented pre- and post-treatment clinical evaluations relevant to dry eye assessment. These evaluations included validated symptom questionnaires (SPEED and OSDI), tear break-up time (TBUT), corneal fluorescein staining, and meibomian gland imaging or grading.
Patients were excluded if they had active ocular or systemic infections, autoimmune or collagen vascular diseases, immunosuppressive conditions, or were using systemic or topical medications known to modulate inflammation. Vulnerable populations, including minors and pregnant women, were also excluded.
Intervention Groups and Devices
Based on the treatments received, patients were categorized into three groups: those treated with RF alone, IPL alone, or a combination of RF and IPL. RF treatments were administered using Forma / Forma-I (InMode Ltd., Israel), which deliver bipolar RF energy at controlled skin surface temperatures of approximately 41–42°C. Forma / Forma-I is specifically adapted for the periorbital area, with integrated temperature sensors to ensure uniform thermal delivery and safety. IPL treatments were performed using the Lumecca / Lumecca-I device (InMode Ltd., Israel), which emits high-intensity pulses of broad-spectrum light (515–1200 nm) targeting periocular vasculature and inflammation. Both treatments were conducted as part of routine clinical care, and their frequency and protocol were individualized at the discretion of the treating physician.
Treatment and Follow-Up Schedule
Participants received either RF monotherapy (4 sessions), IPL monotherapy (4 sessions), or combined RF+IPL therapy (4 sessions), based on clinical indication. All participants included in the analysis completed all four treatment sessions. For patients receiving combined RF+IPL therapy, both treatments were typically performed within the same treatment session, following standard clinic protocols. Only those with complete retrospective data for all clinical evaluations were included. The average interval between treatment sessions was approximately 12 ± 5 days across all three treatment modalities.
Clinical outcomes were assessed at three timepoints: baseline (prior to treatment), first follow-up (approximately 1-month post-treatment), and second follow-up (approximately 3 months post-treatment). Given the treatment course duration of approximately 6–8 weeks (4 sessions spaced ~12 days apart), these post-treatment follow-up timepoints correspond to approximately 3 months and 6 months from baseline, respectively, consistent with the figure labels (3M FU, 6M FU).
Outcome Measures and Scoring
Symptom-based and objective outcome measures were collected at three time points: baseline, first follow-up, and second follow-up.
Subjective symptom assessments included the Standard Patient Evaluation of Eye Dryness (SPEED) and Ocular Surface Disease Index (OSDI). The SPEED questionnaire includes eight items measuring frequency and severity of dry eye symptoms, with scores ranging from 0 to 28, where higher scores indicate more severe symptoms.18 The OSDI is a 12-item validated instrument that assesses ocular symptoms and their functional impact over the prior week; total scores range from 0 to 100, with stratifications for normal (0–12), mild (13–22), moderate (23–32), and severe (≥33) dry eye.19 Both questionnaires were included because they capture complementary aspects of symptom severity and are widely used in dry eye clinical research.17–19
Tear film stability and ocular surface parameters were evaluated using several tools. Tear break-up time (TBUT) was assessed with fluorescein dye under cobalt blue illumination, recording the interval between the last blink and appearance of the first dry spot. A TBUT less than 10 seconds was considered abnormal.
Meibomian gland function was assessed both structurally and functionally. The Meibomian Gland Score (MGS) evaluated gland expressibility and secretion quality, with scores ranging from 0 to 45; higher scores indicated better gland function. Meibography imaging was performed using infrared illumination to visualize gland dropout, graded on a scale from 1 to 4, where higher scores represented more significant gland loss.
Ocular surface damage was evaluated through corneal fluorescein staining, scored from 0 (no staining) to 4 (severe punctate epithelial erosions), using standardized slit-lamp examination protocols. External images of eyelid and ocular inflammation, when available, were also reviewed qualitatively as part of the record.
Data Collection and Confidentiality
All data were abstracted manually from paper and electronic records by trained study personnel using a standardized data collection tool. Each patient record was assigned a unique study identification number. All personal identifiers were removed, and de-identified data were stored on secure, password-protected computers accessible only to authorized members of the research team.
Statistical Analysis
Statistical analyses were performed using IBM SPSS Statistics version 31.0 (IBM Corp., Armonk, NY, USA). All statistical analyses were performed at the patient level rather than the eye level to avoid inter-eye correlation and ensure independence of observations. Continuous variables were summarized as means with standard deviations, while categorical variables were presented as frequencies and percentages. One-way analysis of variance (ANOVA) was used to assess baseline differences in continuous variables, including age and baseline scores, across the three treatment groups: RF only, IPL only, and combined RF+IPL. The Chi-square test was used to evaluate differences in gender distribution. To evaluate longitudinal changes over time, linear mixed-effects models (LMM) were applied for all continuous outcomes (SPEED, OSDI, TBUT, MGS, and corneal staining). The models included fixed effects for treatment group, time, and the group-by-time interaction, with age included as a covariate due to baseline differences between groups. Patient ID was specified as a random effect to account for within-subject correlation across repeated measurements. A variance-components covariance structure and an unstructured repeated variance were used to allow flexible modeling of within-subject variability. Estimated marginal means (EMMs) were calculated to describe adjusted changes over time, and line graphs were generated to illustrate temporal patterns across groups.
For ordinal outcomes such as corneal staining and meibography, LMM were also applied, treating these measures as continuous variables in accordance with common practice in ophthalmic research. All hypothesis tests were two-sided, and a p-value less than 0.05 was considered statistically significant.
Results
Demographics
A total of 286 patients with Meibomian Gland Dysfunction (MGD)-associated dry eye disease were included and stratified into three treatment groups: radiofrequency (RF, n=82), intense pulsed light (IPL, n=106), and combined RF+IPL therapy (n=98) (Table 1). There was no significant difference in gender distribution between groups (p=0.249), although the RF group was significantly younger (mean age: 33.6 ± 8.3 years) compared to the IPL (39.1 ± 11.6) and combined (39.8 ± 11.1) groups (p < 0.001). All subsequent analyses were adjusted for age.
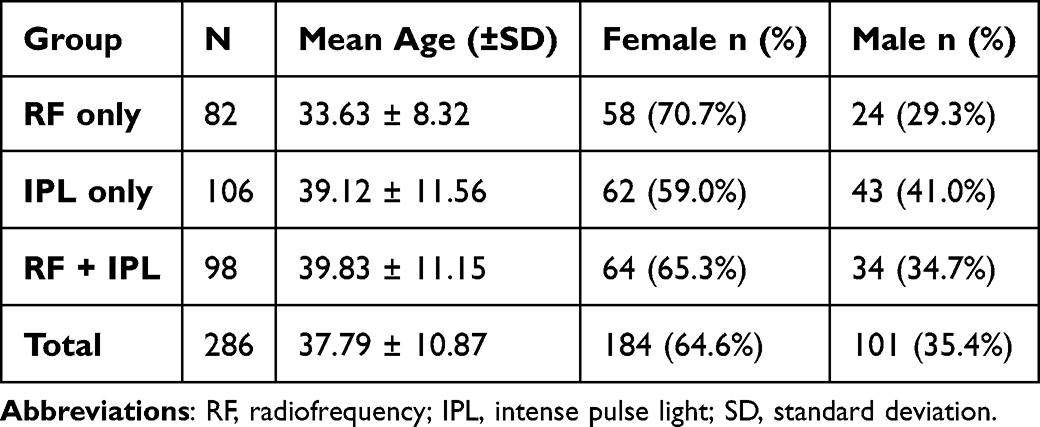 |
Table 1 Baseline Age and Gender Distribution Across Treatment Groups |
Clinical Outcomes
Baseline symptom severity was similar across groups. During the period from baseline to 3 month follow up, all groups demonstrated significant improvements in SPEED scores, with the greatest reduction observed in the combined group (from 11.74 to 6.82), followed by RF (11.23 to 7.46) and IPL (9.71 to 7.68). Linear mixed‑model analysis demonstrated a significant group‑by‑time interaction (F(4, 281)=3.545, p=0.008), indicating differential improvement among the groups. Estimated marginal means were used to describe adjusted changes over time, and line graphs were added to illustrate temporal patterns across groups. Post-hoc comparisons revealed that the combined group’s improvement was significantly greater than IPL alone at both follow-up points (p = 0.013, p = 0.002).
The OSDI scores also significantly improved across all groups, with the combined group again demonstrating the most substantial reduction—from 22.70 at baseline to 3.61 at final follow-up. The RF and IPL groups improved from their respective baseline OSDI scores of 22.27 and 18.09 to 8.29 and 6.20, respectively. The group‑by‑time interaction was highly significant (F(4, 281.005)=96.985, p<0.001). Post-hoc testing confirmed that the combined group’s improvement was significantly greater than both RF and IPL groups at every time point (p < 0.001) (Figure 1).
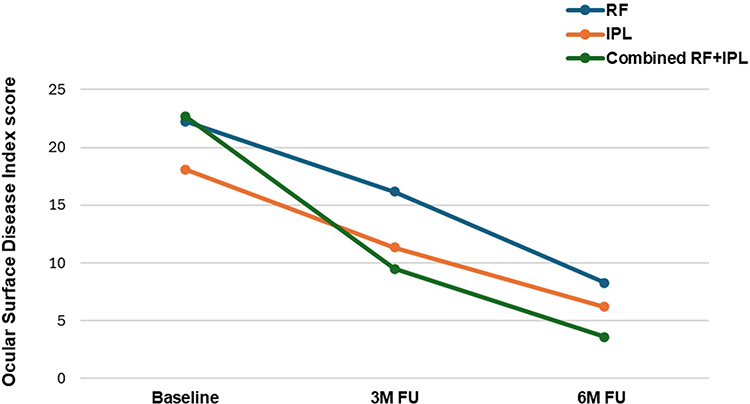 |
Figure 1 Improvement in OSDI Scores Following RF, IPL, and Combined RF+IPL Treatment in MGD-Associated DED. Abbreviations: RF, radiofrequency; IPL, intense pulse light; MGD, meibomian gland dysfunction; DED, dry eye disease. |
All groups showed significant within-group improvement in TBUT values. The RF group improved from 6.60 to 11.27 seconds, IPL from 6.76 to 10.86, and combined from 7.29 to 11.54. Although these gains were statistically significant over time (p < 0.001), the group‑by‑time interaction was not significant (F(4, 281.017)=1.795, p=0.130),suggesting similar efficacy across modalities in restoring tear film stability (Figure 2).
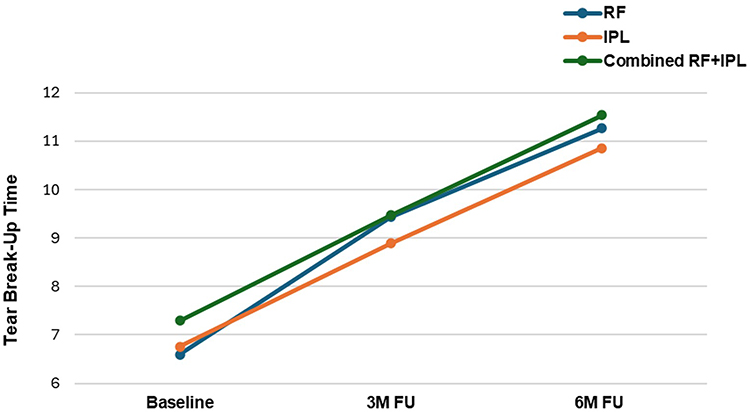 |
Figure 2 TBUT Improvement After RF, IPL, and Combined RF+IPL Therapy in MGD-Associated DED. Abbreviations: TBUT, tear break-up time; RF, radiofrequency; IPL, intense pulse light; MGD, meibomian gland dysfunction; DED, dry eye disease. |
Functional assessment of the meibomian glands showed superior improvement in the combined group (from 25.00 to 29.63), compared to RF (25.10 to 28.90) and IPL (24.62 to 26.24). The group‑by‑time interaction did not reach statistical significance (F(4, 236.945)=2.346, p=0.055), although the combined group showed the largest numerical improvement.(Figure 3).
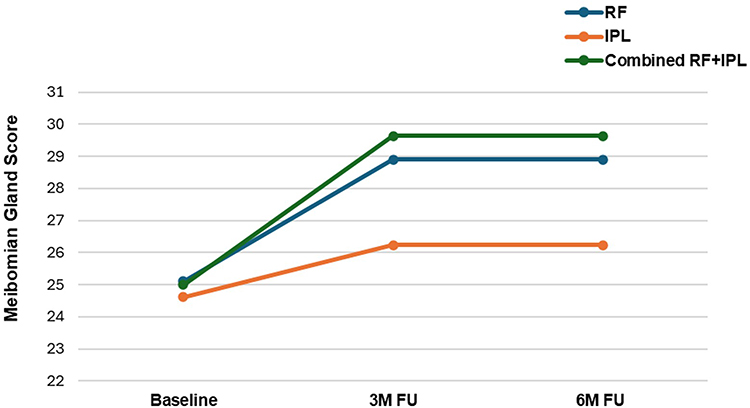 |
Figure 3 Improvement in MGS after RF, IPL, and Combined RF+IPL Therapy in MGD-Associated DED. Abbreviations: MGS, meibomian gland score; RF, radiofrequency; IPL, intense pulse light; MGD, meibomian gland dysfunction; DED, dry eye disease. |
At baseline, mean corneal staining scores were similar across groups (~2.2–2.5). At final follow-up, the combined group had the lowest staining score (0.26), compared to IPL (0.54) and RF (1.00). The group‑by‑time interaction was statistically significant (F(4, 281)=5.777, p<0.001). Improvement over time (baseline to final) was also significantly greater in the combined group compared to RF and IPL (p = 0.007).
Meibography scores, reflecting structural gland dropout, improved in all groups, with the combined group demonstrating the greatest reduction in gland loss score (from 2.34 to 1.08). The RF group improved from their respective baseline scores of 2.27 to 1.43 and IPL group from 2.40 to 2.20. The group‑by‑time interaction was significant (F(4, 645.280)=15.112, p<0.001). Mean changes from baseline were also significantly greater in the combined group compared to both RF and IPL (p < 0.001).
Complications
All treatments were generally well-tolerated across groups. A single minor adverse event was reported: a superficial skin burn following an RF session, which resolved completely within two weeks without the need for medical intervention. This reaction is a known and expected side effect of RF therapy. No serious or long-term complications were observed in any treatment group.
Summary
- Combined RF+IPL therapy resulted in the most consistent and significant improvements across all outcome domains: symptoms (SPEED, OSDI), gland function (MGS), corneal staining, and gland structure (meibography), and showed the largest numerical improvement in gland function (MGS), although this did not reach statistical significance.
- All three modalities significantly improved tear film stability (TBUT), with no clear superiority of one over another.
- The pattern of results, including several statistically significant group‑by‑time interactions, generally favored combination therapy across most outcome domains for MGD‑associated dry eye.
Discussion
In this retrospective cohort study, we evaluated and compared the clinical effectiveness of RF, IPL, and their combination for the treatment of MGD-related dry eye disease (DED). All three treatment strategies led to significant improvements in both subjective symptoms and objective clinical outcomes. Notably, the group receiving combined RF and IPL therapy experienced the most substantial and consistent benefit across all measured parameters, including symptom severity (SPEED, OSDI), tear break-up time (TBUT), corneal staining, gland morphology (meibography), and numerical—but not statistically significant—improvement in gland function (MGS).
MGD is well established as the leading cause of evaporative DED and is characterized by terminal duct obstruction, altered lipid composition, and inflammatory changes that lead to tear film instability and ocular surface damage.6–9,20 The lipid layer secreted by the meibomian glands is essential for preventing excessive tear evaporation and maintaining ocular surface homeostasis. In MGD, meibum becomes more viscous due to elevated phase-transition temperature, leading to gland blockage and inadequate tear film protection.10–12
Thermal-based therapies aim to liquefy the meibum and improve gland expressibility. However, traditional warm compresses often fail to reach or sustain therapeutic temperatures, limiting their effectiveness.14,15 Automated, energy-based devices such as RF and IPL provide controlled, reproducible thermal stimulation, and have been increasingly used in clinical practice with promising outcomes.16,17,21 In our study, we used the Forma / Forma-I and Lumecca / Lumecca-I applicators (InMode Ltd., Israel), which deliver bipolar RF and broad-spectrum IPL, respectively. Both systems were well tolerated, and no serious adverse events were recorded across any treatment group, in line with prior safety profiles reported in the literature.16,17,22
RF therapy works by delivering controlled heat to the dermis and eyelids, effectively melting obstructed meibum and promoting gland clearance.21,23 IPL, originally used in dermatology, has demonstrated additional benefits in dry eye management through its ability to reduce inflammation, ablate abnormal periocular vasculature, and modulate cytokine expression.16,17,24,25 Previous studies by Toyos et al and Dell et al have reported significant improvements in tear film quality, meibomian gland function, and ocular comfort using Lumenis IPL.16,17 Similarly, Forma RF systems have been described in aesthetic and now ophthalmic literature as safe and effective tools for enhancing gland expressibility and periocular tissue health in patients with MGD.21,23
Our findings extend this prior research by showing that combination therapy is associated with superior outcomes across multiple domains. The reduction in OSDI scores observed in the combined group was particularly notable, decreasing from a baseline of 22.7 to 3.6, indicating a shift from moderate to nearly asymptomatic levels. Improvements in SPEED scores also supported this trend. Moreover, while all groups experienced gains in TBUT, the group-by-time interaction was not statistically significant, suggesting that RF, IPL, and combination therapy are comparably effective in restoring tear film stability—consistent with previous findings that any form of sustained thermal application can improve tear film dynamics.13,17
Interestingly, the most pronounced differences in favor of combination therapy emerged in structural and functional gland assessments. The meibography scores in the combined group showed a significant reduction in gland dropout scores, an outcome that is rarely reported outside of prospective interventions.14 However, given the retrospective nature of this study, these structural findings should be interpreted cautiously, and they do not establish evidence of true glandular regeneration. Meibomian gland scores (MGS) also improved most in the combined group, although the group-by-time interaction did not reach statistical significance (p = 0.055), indicating a numerical but not statistically confirmed advantage. These associations may also be influenced by unmeasured confounders or selection bias, but they remain consistent with the model proposed by Baudouin et al and Craig et al, which emphasize the importance of targeting multiple pathogenic pathways in MGD-related DED.7,24
The clinical significance of these findings lies in their real-world applicability. InMode’s platforms were found to be safe, efficient, and suitable for use in a busy ophthalmic setting, offering an effective alternative or complement to pharmacologic therapies, particularly for patients with contraindications to long-term anti-inflammatory drops. The user-friendly interface, treatment consistency, and absence of serious adverse effects make these technologies attractive additions to the therapeutic armamentarium for evaporative DED.21,22
Nevertheless, this study has several limitations. Its retrospective design and reliance on available clinical documentation limit control over treatment schedules and follow-up timing. Because this was a retrospective study, reasons for loss to follow‑up were not systematically documented, and travel‑related dropouts could not be assessed. Lipid layer thickness could not be analyzed because these measurements were not consistently available in the retrospective dataset. Automated area‑based quantification of meibography images was not possible because the imaging system used did not support area estimation. Baseline severity may have differed across groups despite statistical adjustment, and additional unmeasured confounders (eg., compliance with home care regimens) cannot be ruled out. Furthermore, as noted above, the relatively short follow-up period limits the ability to draw firm conclusions regarding structural gland changes observed on meibography, as improvement for this endpoint is known to occur slowly. Despite these limitations, the study has notable strengths. To our knowledge, this is the first real-world comparative evaluation of RF, IPL, and combined RF+IPL treatment modalities in a single study population. The relatively large sample size (N=286), derived from routine clinical practice, enhances the generalizability of findings. In addition, the comprehensive assessment of both subjective symptom scores and objective functional parameters provides a well-rounded evaluation of treatment efficacy.
In summary, this study demonstrates that both RF and IPL therapies are effective in managing MGD-related DED, with combination therapy yielding the most substantial improvements in symptoms, ocular surface health, and structural gland outcomes, and the largest numerical (but not statistically significant) improvement in gland function (MGS). These findings reinforce the value of energy-based, non-pharmacologic interventions in treating chronic evaporative dry eye and highlight the potential role of multimodal therapy in achieving better outcomes. Future prospective, randomized studies should focus on optimizing treatment parameters, understanding molecular mechanisms, and evaluating long-term effects on gland preservation and visual quality.
Conclusion
This retrospective study demonstrates that radiofrequency (RF), intense pulsed light (IPL), and especially their combination are effective and safe treatment modalities for managing Meibomian Gland Dysfunction-related dry eye disease. Combination therapy resulted in the greatest improvements in symptom severity, gland function, and ocular surface health, and showed the largest numerical, but not statistically significant, improvement in gland function (MGS). These findings support the use of multimodal, energy-based treatments, such as those delivered by the InMode platforms, as valuable tools in the comprehensive management of evaporative dry eye.
Ethics Approval and Informed Consent
This study was reviewed and approved by Sterling IRB (Protocol No. DO613929A). The study was conducted as a retrospective chart review at LINE OF SIGHT Eyecare, New York, NY, under the supervision of Principal Investigator Jennifer Tsai, OD. All procedures were conducted in accordance with the ethical standards of the Declaration of Helsinki. Informed consent was waived by the approving IRB given the retrospective nature of the study.
Acknowledgments
Dr. Jennifer Tsai was supported in part by InMode Ltd. The author would like to thank the clinical staff at LINE OF SIGHT for their valuable assistance with data collection. The contribution of medical writers from HaMaDa Clinical Consulting in the preparation of this manuscript is gratefully acknowledged. Finally, the author expresses her sincere gratitude to all the participants whose retrospective clinical data made this study possible.
Disclosure
The author reports no conflicts of interest related to this work. Partial support from InMode Ltd. is disclosed in the Acknowledgments section. The author maintained full independence in all aspects of the study.
References
1. Jones L, Craig JP, Markoulli M, et al. TFOS DEWS III: management and therapy. Am J Ophthalmol. 2025;279:
2. Stapleton F, Alves M, Bunya VY, et al. TFOS DEWS II epidemiology report. Ocul Surf. 2017;15(3):334–9. doi:10.1016/j.jtos.2017.05.003
3. Farrand KF, Fridman M, Stillman IÖ, Schaumberg DA. Prevalence of diagnosed dry eye disease in the United States among adults aged 18 years and older. Am J Ophthalmol. 2017;182:90–98. doi:10.1016/j.ajo.2017.06.033
4. Craig JP, Nichols KK, Akpek EK, et al. TFOS DEWS II definition and classification report. Ocul Surf. 2017;15(3):276–283. doi:10.1016/j.jtos.2017.05.008
5. Yu J, Asche CV, Fairchild CJ. The economic burden of dry eye disease in the United States: a decision tree analysis. Cornea. 2011;30(4):379–387. doi:10.1097/ICO.0b013e3181f7f363
6. Nelson JD, Shimazaki J, Benitez-del-Castillo JM, et al. The international workshop on Meibomian Gland Dysfunction: report of the definition and classification subcommittee. Invest Ophthalmol Vis Sci. 2011;52(4):1930–1937. doi:10.1167/iovs.10-6997b
7. Baudouin C, Messmer EM, Aragona P, et al. Revisiting the vicious circle of dry eye disease: a focus on the pathophysiology of Meibomian Gland Dysfunction. Br J Ophthalmol. 2016;100(3):300–306. doi:10.1136/bjophthalmol-2015-307415
8. Knop E, Knop N, Millar T, Obata H, Sullivan DA. The International workshop on Meibomian Gland Dysfunction: report of the subcommittee on anatomy, physiology, and pathophysiology of the meibomian gland. Invest Ophthalmol Vis Sci. 2011;52(4):1938–1978. doi:10.1167/iovs.10-6997c
9. Geerling G, Tauber J, Baudouin C, et al. The international workshop on Meibomian Gland Dysfunction: report of the subcommittee on management and treatment of Meibomian Gland Dysfunction. Invest Ophthalmol Vis Sci. 2011;52(4):2050–2064. doi:10.1167/iovs.10-6997g
10. Nagymihályi A, Dikstein S, Tiffany JM. The influence of eyelid temperature on the delivery of meibomian oil. Exp Eye Res. 2004;78(3):367–370. doi:10.1016/s0014-4835(03)00197-0
11. Borchman D, Foulks GN, Yappert MC, et al. Human meibum lipid conformation and thermodynamic changes with Meibomian-Gland Dysfunction. Invest Ophthalmol Vis Sci. 2011;52(6):3805–3817. doi:10.1167/iovs.10-6514
12. Butovich IA, Millar TJ, Ham BM. Understanding and analyzing Meibomian lipids—a review. Curr Eye Res. 2008;33(5–6):405–420. doi:10.1080/02713680802018419
13. Blackie CA, Carlson AN, Korb DR. Treatment for Meibomian Gland Dysfunction and dry eye symptoms with a single-dose vectored thermal pulsation: a review. Curr Opin Ophthalmol. 2015;26(4):306–313. doi:10.1097/ICU.0000000000000165
14. Finis D, Hayajneh J, König C, et al. Evaluation of an automated thermodynamic treatment (LipiFlow®) system for Meibomian Gland Dysfunction: a prospective, randomized, observer-masked trial. Ocul Surf. 2014;12(2):146–154. doi:10.1016/j.jtos.2013.12.001
15. Lee G. Evidence-based strategies for warm compress therapy in meibomian gland dysfunction. Ophthalmology and Therapy. 2024;13(9):2481–2493. doi:10.1007/s40123-024-00988-x
16. Liu R, Rong B, Tu P, et al. Analysis of cytokine levels in tears and clinical correlations after intense pulsed light treating Meibomian Gland Dysfunction. Am J Ophthalmol. 2017;183:81–90. doi:10.1016/j.ajo.2017.08.021
17. Dell SJ. Intense pulsed light for evaporative dry eye disease. Clin Ophthalmol. 2017;11:1167–1173. doi:10.2147/OPTH.S139894
18. Ngo W, Situ P, Keir N, Korb D, Blackie C, Simpson T. Psychometric properties and validation of the standard patient evaluation of eye dryness questionnaire. Cornea. 2013;32(9):1204–1210. doi:10.1097/ICO.0b013e318294b0c0
19. Schiffman RM. Reliability and validity of the ocular surface disease index. Arch Ophthalmol. 2000;118(5):615–621. doi:10.1001/archopht.118.5.615
20. Bron AJ, de Paiva CS, Chauhan SK, et al. TFOS DEWS II pathophysiology report. Ocul Surf. 2017;15(3):438–510. doi:10.1016/j.jtos.2017.05.011
21. Lam PY, Shih KC, Fong PY, et al. A review on evidence-based treatments for Meibomian Gland Dysfunction. Eye Contact Lens. 2020;46(1):3–16. doi:10.1097/ICL.0000000000000680
22. Chelnis J, Garcia CN, Hamza H. Multi-frequency RF combined with intense pulsed light improves signs and symptoms of dry eye disease due to Meibomian Gland Dysfunction. Clin Ophthalmol. 2023;Volume 17:3089–3102. doi:10.2147/OPTH.S426564
23. Toyos R, McGill W, Briscoe D. Intense pulsed light treatment for dry eye disease due to meibomian gland dysfunction; a 3-year retrospective study. Photomed Laser Surg. 2015;33(1):41–46. doi:10.1089/pho.2014.3819
24. Craig JP, Chen Y-H, Turnbull PRK. Prospective trial of intense pulsed light for the treatment of Meibomian Gland Dysfunction. Invest Ophthalmol Vis Sci. 2015;56(3):1965–1970. doi:10.1167/iovs.14-15764
25. Leng X, Shi M, Liu X, Cui J, Sun H, Lu X. Intense pulsed light for meibomian gland dysfunction: a systematic review and meta-analysis. Graefes Arch Clin Exp Ophthalmol. 2021;259(1):1–10. doi:10.1007/s00417-020-04834-1
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.