")
Back to Journals » Risk Management and Healthcare Policy » Volume 16
Comparative Assessment of Oral Health Attitudes and Behaviors of First-Time and Previous Dental Patients Undergoing Exodontia Treatment During the COVID-19 Pandemic in Private Dental Clinics in Riyadh City, Saudi Arabia
Authors AlHaj MAK, Baseer MA , AlSaffan AD , Ingle NA
Received 10 May 2023
Accepted for publication 16 August 2023
Published 30 August 2023 Volume 2023:16 Pages 1679—1691
DOI https://doi.org/10.2147/RMHP.S420859
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jongwha Chang
Muhanad Abdul Kareem AlHaj, Mohammad Abdul Baseer, Abdulrahman Dahham AlSaffan, Navin Anand Ingle
Preventive Dentistry Department, College of Dentistry, Riyadh Elm University, Riyadh, Saudi Arabia
Correspondence: Mohammad Abdul Baseer, Preventive Dentistry Department, College of Dentistry, Riyadh Elm University, Namuthajiya Campus, PO Box No 84891, Riyadh, 11681, Saudi Arabia, Email [email protected]
Background: The COVID-19 lockdown affected oral health behaviors. This study aims to assess and compare the oral health attitudes and behaviors of first-time and previous patients undergoing dental extractions during the COVID-19 pandemic at private dental clinics in Riyadh City, Saudi Arabia.
Methods: This cross-sectional study was conducted among patients aged 18– 65 years undergoing dental extractions at private dental clinics in Riyadh City, Saudi Arabia. Four hundred and eighty patients were selected using a convenient sampling methodology. A structured, close-ended questionnaire investigated demographic information, tooth extraction attendance, and oral health attitudes and behaviors using 20 items Hiroshima University Dental Behavioral Inventory (HUDBI).
Results: A total of 480 exodontia patients [282 (58.8%) males and 198 (41.2%) females] participated in this study. All patients used a stiff-bristled toothbrush and were concerned about their teeth’ color and bad breath. Similarly, all the participants did not feel brushed unless they used strong strokes, and the dentist told them to brush very well. An overall mean HUDBI score of 6.34± 1.12 was observed. Patients with a primary education (5.61± 0.79), income ≤ 5000 SAR (6.00± 0.92), residing in rural areas (5.84± 0.93), and government employees (5.62± 0.96) exhibited lower HU-DBI scores compared to their counterparts. The study revealed a significant variation in HUDBI scores across different demographic factors, including education, income, residence, occupation, and reason for extraction (p< 0.001). The HUDBI score of first-time attendees to dental extraction (5.88± 1.03) was found to be significantly poorer than to those of previous attendees (6.63± 1.09), (p< 0.001).
Conclusion: Patients who underwent dental extractions at private dental clinics in Riyadh City, Saudi Arabia, during the post-lockdown COVID-19 pandemic exhibited average oral health attitudes and behaviors. Oral health attitudes and behaviors differed by socioeconomic status. Patients undergoing dental extractions for reasons other than dental caries and periodontal diseases and first-time attendees demonstrated poor oral health attitudes and behaviors.
Keywords: attitude, behavior, tooth extraction, oral health, private dental clinics, pandemic
Introduction
The sudden emergence of Corona Virus Disease −19 (COVID-19) created a worldwide public health emergency, resulting in over a million deaths.1,2 Saudi Arabia reported the first case of COVID-19 on 2nd March 2020. The Saudi Ministry of Health (MOH) immediately launched public awareness initiatives to increase understanding about COVID-19 transmission channels and preventive actions. This was followed by the imposition of a nationwide lockdown to prevent the spread of COVID-19. Until 20th June 2020, high-risk transmission locations such as shopping malls, restaurants, coffee shops, and saloons were also closed. The health ministry enabled telemedicine and teleconsultation. In addition, the Ministry of Health3 recommended that dental clinics be closed except for dental emergencies. Also, patients were urged to postpone nonurgent dental treatments and contact their dental practices through teleconsultation to prioritize cases according to their urgency and plan management appropriately.4,5
Higher levels of fear, anxiety, and depression were associated with the COVID-19 pandemic among adults in Saudi Arabia.6,7 According to Alkhamees et al (2020), 23.6% of the general population of Saudi Arabia had a moderate or severe psychological impact.7 These psychological problems, such as fear, might impact health and healthcare-seeking behavior. It has been reported that fear of COVID-19 adversely affected the desire to seek dental care in Saudi Arabia. Age, the perceived risk of COVID-19 infection at dental clinics, and untreated dental problems were associated with dental anxiety.8 Previously published studies on dental patients’ attitudes and behaviors during Ebola outbreaks and MERS indicated avoidance of treatments due to the risk of contracting the infections.9,10
Previous research from Saudi Arabia indicates dental caries is the leading cause of tooth extractions, followed by residual roots, periodontal disease, and impactions.11 Over 1.5 million Saudi population is projected to receive regular dental care in 2013, and over 6.5 million require dental services.12 According to studies, these numbers have climbed in recent years, reflecting the rising need for dental treatments in Saudi Arabia.13,14
The Hiroshima University-Dental Behavioral Inventory (HU-DBI), founded by Kawamura, was beneficial for assessing oral health attitudes and behavior and demonstrated better cross-cultural adaptations.15,16 Moreover, it has been utilized to assess oral health attitudes and behaviors of patients, professional groups, and students.15,17–19 Furthermore, the questionnaire has been successfully translated into English and other languages, demonstrating high test–retest reliability.15,20
A United Kingdom-based study revealed that the most common treatment administered during the first 6 weeks of the COVID-19 epidemic was extraction (63%), followed by antibiotic prescription (13%).21 After the announcement of the COVID-19 pandemic, a Chinese study observed a 38% decline in dental emergencies and a 13% decline in non-emergencies.22 Nonetheless, during the COVID-19 pandemic in Saudi Arabia, there were social disparities in emergency dental care-seeking decisions.23 It has been regularly emphasized that the individual’s attitudes and behaviors are crucial in improving oral health.24
Negative oral health-seeking attitudes and behaviors have been documented during the COVID-19 lockdown. However, after the resumption of dental services with precautionary measures during the pandemic, there is a need for a greater understanding of oral health self-care among dental patients. In this context, factors influencing self-care oral health-related attitudes and behaviors of patients undergoing dental extractions must be investigated to provide appropriate oral health promotion and disease prevention measures. Moreover, the difference in self-care oral health attitudes and behaviors between the first-time attendees undergoing tooth extraction for the first time during the pandemic after the lockdown period and the previous attendees with a history of dental extraction before the pandemic and seeking teeth extraction during the pandemic has not been reported. Hence, this study aims to assess and compare the self-care oral health attitudes, and behaviors of first-time and previous patients undergoing dental extractions during the COVID-19 pandemic at private dental clinics in Riyadh City, Saudi Arabia.
Subjects and Methods
Ethical Approval and Informed Consent
The current study was conceived and carried out in accordance with the Helsinki Declaration for human subject research. The study proposal was reviewed and approved by the research and innovation center of Riyadh Elm University, Riyadh, under reference number (IRB #: FPGRP/2022/702/806/780). The respective clinical directors were permitted to conduct the study in private dental clinics. The patients provided written informed consent to participate in the study after receiving the information on the purpose of the study. No monetary incentives or other inducements were used in this study. All patient identifiers were coded, and data was collected anonymously.
Study Design
This cross-sectional study was conducted in four private dental clinics in Riyadh City. Three university-affiliated large private dental clinics (An Namuthajiyah, Olaya, and Munesiyah) and one privately run dental clinic were considered in this study.
Study Sample
A convenient sample of adult cohort patients aged between 18 and 65 years undergoing tooth extractions for various reasons was included in the study. This study sample was calculated using G*Power 3.1.9.7 sample size and power calculator. Since no previous study was reported comparing HUDBI scores of first-time and previous attendees undergoing dental extraction, a pilot study was conducted that resulted in an effect size of 0.340. Thus, a final sample of 480 patients was calculated based on small effect size (0.34), alpha error of probability (0.05), power (1-Beta) (0.95), and allocation ratio (1.65) needed to compare the mean HUDBI-score between first-time attendees and previous attendees of exodontia services. The study’s power and allocation ratio were adjusted based on the advice of a statistician, taking into account the available time of 5 months and available resources.
Inclusion and Exclusion Criteria
All patients aged ≥18 years, undergoing extraction in selected private dental clinics and willing to participate were included in this study. Those dental patients under 18 years who were undergoing extraction, unwilling to participate in the study, and seeking other treatments were excluded. Moreover, patients receiving exodontia treatment in government dental clinics and public university facilities were excluded from the study.
Study Instrument
The study participants’ oral health attitudes and behaviors were assessed using an English version of the HUDBI25,26 (Table 1). The HU-DBI developed by Kawamura is a validated tool with apparently strong psychometric qualities for measuring self-care oral health-related attitudes and behaviors.15,17 A structured, close-ended questionnaire comprised demographic data, information on dental care, and 20 HU-DBI items evaluated patients’ self-care oral health attitudes and behaviors. The demographic components included age, gender, education, occupation, income, and residence information. Each patient’s dental care utilization was documented, including first-time or previous attendees, the reason for extraction, and the extraction pattern (single vs multiple extractions).
 |
Table 1 HU-DBI Questionnaire Items with Agree/Disagree Responses |
Before dental extraction, a trained and calibrated bilingual (English and Arabic) investigator interviewed each patient using the paper-based questionnaire and recorded the responses. All original HU-DBI items have responses in either “Agree” or “Disagree” format, and 12 were used to determine the overall HU-DBI score. For items 4, 9, 11, 12, 16, and 19, each “agree” answer was given a one point score. For items 2, 6, 8, 10, 14, and 15, each “disagree” answer was given one point. Therefore, the entire HU-DBI score ranges from 0 (the worst score) to 12 (the best score). A total score of 12 includes the components of attitudes and behaviors, with a higher score indicating better oral health. Eight dummy items of the HUDBI questionnaire were excluded from the final scoring17 although they are useful to verify the reproducibility of the inventory and used for other investigations (Table 2).
 |
Table 2 Relation Between Patient’s Characteristics and Dental Extraction Visiting Pattern |
The data were collected from August to December-2022. All the collected responses were coded and entered into the Excel sheet. The coded sheet was then imported into the statistical program for analysis.
Statistical Analysis
The statistical package for Social Sciences version 25.0 (IBM-SPSS, Armonk, NY: USA) was utilized to execute all the statistical analyses. Descriptive statistics were performed to describe the characteristics of the study participants and HUDBI responses using frequency distributions, percentages, mean, and standard deviation scores. Normality examination showed the non-normal distribution of the data. The chi-square test was applied to evaluate the association between sociodemographic factors and dental extraction attendance pattern (first-time vs previous attendee). Kruskal–Wallis’s test was applied to compare mean HUDBI ranks across education, income, occupation, and reasons for tooth extraction. The Mann–Whitney U-test was applied to compare mean HUDBI ranks of gender, residence, number of extractions, and extraction attendance pattern. A value of p<0.05 was considered significant for all the statistical tests.
Results
Four hundred and eighty patients undergoing dental extractions in various private dental clinics in Riyadh City participated in this study. Of the 480 participants, 282 (58.8%) were males and 198 (41.2%) were females. The age of the study participants ranged between 18 and 65 years, with a mean age of 48 years. The dental extraction attendance in first-time attendees vs previous attendees between males (38.7% vs 61.3%) and females (36.4% vs 63.6%) did not differ significantly (p=0.611). The highest proportion of the participants had a college education 169 (35.2%), followed by secondary 123 (25.6%), intermediate 103 (21.5%), and primary 85 (17.7%). The dental extraction attendance (first-time attendees vs previous attendees) of primary (29.4% vs 70.6%), intermediate (79.6% vs 20.4%), secondary (22% vs 78%), and college education (27.8% vs 72.2%) showed a statistically significant difference (p<0.001).
A large percentage, 213 (44.4%) of the participants, had their income <5000 SAR, followed by 5001–10,000 SAR 183 (38.1%) and 10,001–15,000 SAR 84 (17.5%). Dental extraction attendance of first-time attendees vs previous attendees across income categories showed a <5000 SAR (47.4% vs 52.6%), 5001–10,000 SAR (26.8% vs 73.2%), and 10,000–15,000 SAR (36.9% vs 63.1%), a statistically significant difference was observed (p<0.001). When the dental extraction attendance of first-time attendees vs previous attendees was compared between the rural (56.6% vs 43.4%) and urban (21.6% vs 78.4%) residents, a statistically significant difference was observed (p<0.001). The dental extraction attendance of first-time attendees vs previous attendees of government employees (61.6% vs.38.4%), private (24.6% vs 75.4%), and unemployed/student/homemaker (37.9% vs.62.1%) differed significantly (p<0.001). The occupational status revealed that more than half of the study participants worked in the private sector 268 (55.8%), while 146 (30.4%) were government employees.
Nearly 259 (54%) of the study participants underwent tooth extraction due to dental caries and its sequelae, while 147 (30.6%) needed tooth extraction due to periodontal diseases. Almost 74 (15.4%) had their teeth extracted for other reasons (orthodontic treatment, trauma, and prosthodontic treatment). When the dental extraction attendance of first-time attendees vs the previous attendees was compared due to dental caries and its sequelae (21.6% vs 78.4%), periodontal disease (34.7% vs 65.3%) and other reasons (100% vs 0%), a statistically significant difference was observed (p<0.001).
Over three-fourths, 365 (76%) of the patients required single tooth extractions, and less than a quarter, 115 (24%), needed multiple extractions. The dental extraction attendance did not differ significantly between patients undergoing single (37.5% vs 62.5%) versus multiple (38.3% vs 61.7%) extractions (p=0.889). The sociodemographic factors and patient’s dental extraction attendance pattern are shown in (Table 2).
Figure 1 presents study participants’ agreed responses to the HUDBI items. All the patients were worried about their teeth' color (item 3) and bad breath (item 13) and used a toothbrush with stiff bristles (item 17). In addition, all the participants did not feel brushed unless they used strong strokes (item 18), and the dentist told them to brush very well (item 20). All participants disagreed with using child-sized toothbrushes (item 5). Only 2.1% did not worry much about visiting the dentist (item 1), and 3.8% brushed each of their teeth carefully (item 9). Nearly 5.4% suffered bleeding gums when brushing their teeth (item 2). Almost 18.1% used a dye to see the cleanliness of their teeth (item 16). Approximately 21.5% had never been taught by professionals how to brush their teeth (item 10). Less than half (44.6%) of participants agreed to have false teeth in old age (item 6). Almost (46.9%) agreed to clean their teeth well without using toothpaste (item 11), and (48.3%) participants put off going to the dentist until toothache (item 15). More than half (59.8%) of the participants opined that their teeth are getting worse despite daily brushing (item 8). Almost 71.5% of the patients often checked their teeth in the mirror after brushing (item 12), and 71.9% felt it sometimes took too much time to brush their teeth (item 19). Over three-fourths of participants felt it is impossible to prevent gum disease by brushing alone (item 14). Many participants (80.2%) noticed some white sticky deposits on their teeth (item 4), and 97.9% were bothered by their gum color (item 7).
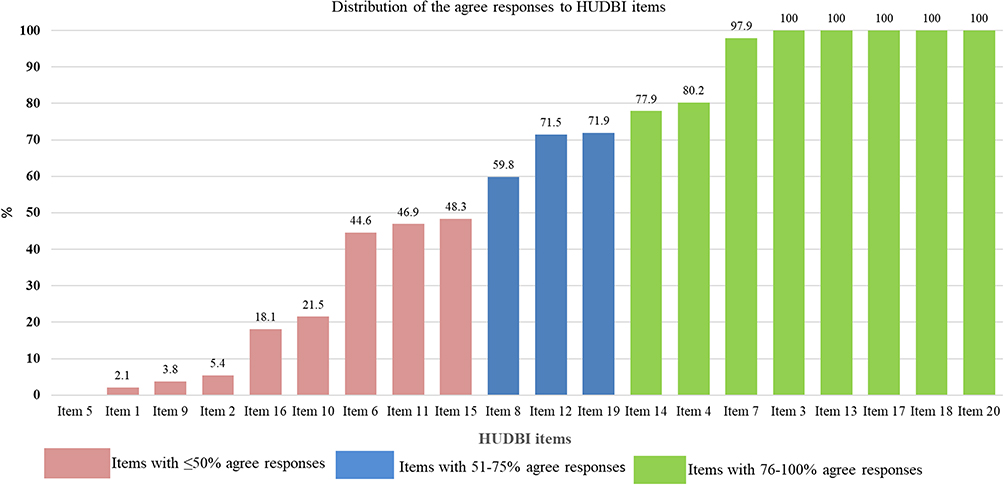 |
Figure 1 Distribution of the study participant’s “agree” responses to the HUDBI items. |
The percentage of agreement and disagreement for different HUDBI items between first-time and previous attendees are shown in (Table 3). All the first-time attendees and previous attendees agreed with item 3 (I worry about the color of my teeth), item 13 (I worry about having bad breath), item 17 (I use a toothbrush with hard bristles), item 18 (I do not feel I have brushed well unless I brush with strong strokes) and item 20 (I have had my dentist tell me that I brush very well). A significantly higher percentage of first-time attendees than previous attendees suffered bleeding gums (9.9% vs 2.7%, p=0.001), worsening of the teeth despite daily brushing (77.3% vs 49.2%, p<0.001), careful brushing of each tooth (7.2% vs 1.7%, p=0.002), never been taught professionally how to brush (43.6% vs 8%, p<0.001). Similarly, a high percentage of first-time attendees than previous attendees put off going to the dentist until they had a toothache (59.1% vs 41.8%, p<0.001) and used dye to see the cleanliness of their teeth (42.5% vs 3.3%, p<0.001). In contrast, a significantly higher percentage of previous attendees than first-time attendees agreed for not helping to have false teeth during old age (54.8% vs 27.6%, p<0.001), cleaning teeth well without using toothpaste (57.2% vs 29.8%, p<0.001), and often checked their teeth in the mirror after brushing (87% vs 45.9%, p<0.001).
 |
Table 3 HUDBI Items and Extraction Attendance Patterns of Patients |
The oral health attitudes and behaviors of patients undergoing dental extractions are displayed in (Table 4 and Figure 2). An overall mean HUDBI score of 6.34±1.12 and minimum and maximum scores of 4 and 8 were observed in this study. The comparison of mean HUDBI ranks between males (234.51) and females (249.03) did not reveal any statistically significant differences in oral health attitudes and behaviors of the study participants (p=0.241).
 |
Table 4 Comparison of Mean HUDBI Score in Different Groups |
 |
Figure 2 Comparison of mean HUDBI score across the extraction related variables indicating *potential outlier position and probable outlier position. |
A statistically significant difference was observed in mean ranks across various educational categories (p<0.001). The study participants with a college level of education demonstrated higher HUDBI ranks (303.33), followed by secondary (267.83), intermediate (176.22), and primary (153.92) education. Patients with primary and intermediate levels of education demonstrated significantly lower mean HUDBI ranks than those with secondary and college levels of education. Further comparison showed a significantly higher mean HUDBI rank in college-level educated patients than the secondary educated ones. Similarly, a statistically significant difference was observed when mean ranks were compared across different income categories (p<0.001). The mean HUDBI ranks across different income groups indicated a higher mean rank in 10,001–15,000 SAR (274.90), followed by 5001–10,000 SAR (273.90) and <5000 SAR (198.50). The study participants with <5000 SAR income showed significantly lower mean HUDBI ranks than the other two income groups. However, comparing mean HUDBI ranks between 5001–10,000 SAR and 10,001–15,000 SAR did not yield any significant difference. Patients from urban residences (292.06) showed significantly higher mean HUDBI ranks compared to their rural counterparts (180.08) (p<0.001).
A comparison of HUDBI rankings of patients employed in the private sector (288.21), unemployed/students/homemakers (234.36), and those engaged in the government sector (155.70) showed a statistically significant (p<0.001) difference. Patients engaged in the government sector (155.70) had significantly lower mean HUDBI rankings than those of unemployed (234.36) or employed in the private sector (288.21). Similarly, patients employed in the private sector had a significantly better HUDBI ranking than those of unemployed/students/homemakers.
A statistically significant difference was observed when the mean HUDBI ranks were compared across various reasons for tooth extraction (p<0.001). Patients undergoing tooth extractions owing to dental caries and its sequelae had the highest mean HUDBI rank (292.06), followed by those with periodontal disease (222.87) and other causes of tooth extractions (95.07). Patients undergoing dental extraction for other reasons showed a significantly lower mean HUDBI rank than those undergoing extractions due to dental caries and its sequelae and periodontal diseases. Similarly, patients undergoing extraction due to dental caries and its sequelae showed significantly higher mean HUDBI ranks than those with periodontal diseases. In contrast, the mean HUDBI ranks did not differ significantly between patients undergoing single-tooth extraction (246.74) and multiple teeth extractions (220.70) (p=0.068). Patients who have had a previous dental extraction showed a significantly higher mean HUDBI rank (273.97) compared to first-time attendees undergoing tooth extraction (185.20) (p<0.001) (Table 4).
Discussion
Dental care utilization in Saudi Arabia has indicated that most patients visit dental clinics to treat their dental problems and for emergency dental services.12,27–29 Patients undergoing dental extractions in private dental clinics and university hospitals were contacted to determine their oral health attitudes and behaviors in this study. This study demonstrated average oral health attitudes and behaviors of patients undergoing dental extraction in private dental clinics in Riyadh City, Saudi Arabia. However, comparing HUDBI ranks across different socioeconomic and dental variables demonstrated statistically significant differences except for the gender and the number of extractions at the time of visit. Irrespective of the visiting pattern, this finding corroborates with previously published work that reported negative attitudes towards dental care resulting in an increased rate of extraction visits among patients.30
In the present study, 37.6% of the patients were first-time-attenders seeking dental extraction, while the remaining had previously undergone dental extraction for various reasons. Additionally, more males than females were first-time attendees for dental extraction. In contrast, most of the females had undergone extraction previously, suggesting an insignificantly higher rate of dental services utilization among females than male patients. Despite this, oral health attitudes and behaviors did not differ significantly between male and female patients. This finding aligns with a previous study in which non-attenders and in-trouble attendees constituted most patients attending mainly exodontia clinics without significant differences between males and females.31
Education is intended to promote health-seeking behavior, assuming increased access to information will improve health knowledge, motivating individuals to change.31 The visiting pattern indicated that patients with an intermediate level of education were more likely to be first-time attendees for tooth extraction compared to other educational levels, where most of the patients previously received treatment for extraction. As educational levels increased, the utilization of services for exodontia increased, corroborating previous study findings that utilization of dental services was greater among people with a high level of education.12,32 A comparison of oral health attitudes and behaviors across educational levels revealed a significant variation, with primary and intermediate education participants demonstrating poor attitudes and behaviors and patients with secondary and college education demonstrating better oral health attitudes and behaviors. This finding is similar to a previous report in which higher education relates to better health-seeking behavior.33 Gbolahan et al found no significant association between educational level and oral health-seeking behavior.31
Income is considered a predictor of dental service utilization. Patients with higher incomes tend to utilize more dental care than those with lower incomes.12,14 In this study, most patients had a <5000 SAR monthly income, which differed significantly between first-time and previous attendees of tooth extraction. Lower income levels were associated with poor oral health attitudes and behaviors due to greater cigarette use and sugar intake rates, infrequent and symptomatic dental visits, and poor oral hygiene. Lower-income individuals were probably less likely to have routine dental examinations because they could not afford the treatments. In contrast, high incomes are associated with essential resources, such as the capacity to buy food of higher quality and preventative and routine dental treatment. Alternatively, low earnings are related to poor oral health behaviors.34,35
Despite the improved dentist population ratio (5.3 per 10,000 people) in Saudi Arabia, most licensed dentists practice in urban and suburban areas, and only 13% of the dentists serve in rural areas.36 Hence, patients residing in rural areas tend to travel to urban areas for their dental needs. In this study, more than half of urban residents and 46% of rural residents attended for the extraction of their teeth. Most first-time attendees were from rural areas, while previous attendees for extraction were mainly from urban areas. A significant variation was observed in obtaining exodontia services between first-time and previous attendees. Moreover, oral health attitudes and behaviors were poorer among rural patients, highlighting access and availability concerns for dental care in rural areas. This finding is in line with the study reported by Qi et al in China, where place of residence was found to be associated with dental services utilization.37 However, it should be noted that the distance traveled by the patients to reach the dental clinics was not documented in this study.
Regarding occupation and oral health behaviors, differences in oral cleanliness and dental visiting behaviors were evident across various occupations. A high percentage of skilled workers did not brush their teeth before going to bed, and salespersons received lower regular dental checkups.38 In this study, occupational status of the participants was broadly categorized into government services, private, and unemployed/student/homemaker. Most of the study participants were in private services, with first-time and previous attendees demonstrating a significant difference in utilization of exodontia services. When oral health attitudes and behaviors were compared across various occupational groups, participants working in government services showed significantly poor oral health attitudes and behaviors.
In this study, dental caries and periodontal diseases are the primary reasons for teeth extraction among the study participants. This finding agrees with past studies conducted in Saudi Arabia.39,40 Caries and periodontal disease are mostly avoidable causes of tooth loss if detected early during routine dental visits. However, first-time and previous attendees visited dental clinics at a late stage of the disease that required teeth extraction either due to the high cost of the treatment or because there was no other treatment option left.41
Hence, it is evident that most patients with dental pain opted for extraction in private dental clinics. When oral health attitudes and behaviors were compared across various reasons for tooth extraction, patients requiring tooth extraction for other reasons demonstrated significantly poor oral health attitudes and behaviors. Patients requiring extractions for reasons other than the consequences of dental caries and periodontal diseases may visit clinics less often, which may have affected their attitudes and behaviors, resulting in poor oral health attitudes and behaviors. In contrast, patients undergoing extraction due to dental caries and periodontal diseases will likely visit clinics more frequently, resulting in better oral health attitudes and behaviors. Moreover, patients undergoing single or multiple tooth extractions at a time did not vary significantly in their oral health attitudes and behaviors.
In this study, patients who attended previous dental extractions showed significantly better oral health attitudes and behaviors than first-time attendees for dental extractions. It may be explained by the fact that despite the history of poor oral attitudes and behaviors, consistent reinforcement of oral health information at each visit may lead to better oral health attitudes and behaviors.31
The global outbreak of the coronavirus pandemic has resulted in widespread uncertainty and perplexity across nations. The variation in guidelines adopted by different countries also contributes to this confusion. The scientific literature on the process of coronavirus diffusion and its characteristics remains scant. Temperature, humidity, and surface material have been observed to be useful in establishing guidelines for preventing the spread of the coronavirus.42 Consequently, reducing fear and anxiety of viral transmission in dental clinics and enhancing the quality of dental care for the patients.
Limitations of the Study
This study did not investigate oral health knowledge; nonetheless, based on the findings of the oral health habit, it is reasonable to presume that most of our participants had poor oral health knowledge. Owing to the cross-sectional character of the research, the cause-and-effect connection between the variables could not be investigated. Only patients seeking extraction treatments at private dental clinics in Riyadh City were considered in this research. Therefore, the study’s findings cannot be extrapolated to patients in the public sector. Further studies involving larger representative samples from different cities and government dental clinics are required.
Conclusion
Patients who underwent dental extractions at private dental clinics in Riyadh City, Saudi Arabia, during the post-lockdown COVID-19 pandemic exhibited average oral health attitudes and behaviors. Patients undergoing dental extractions for reasons other than dental caries and periodontal diseases and first-time attendees demonstrated poor oral health attitudes and behaviors. On the other hand, patients with lower levels of education, rural residents, and government employees showed poor oral health attitudes and behaviors, suggesting socioeconomic disparities in oral health.
Data Sharing Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Research and Innovation Center of Riyadh Elm University (IRB No: FPGRP/2022/702/806/780).
Acknowledgments
Authors would like to thank the research and innovation center of Riyadh Elm University for supporting and granting this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research has not received any funding from external sources.
Disclosure
All authors declare no conflicts of interest in this work.
References
1. World Health Organization. Novel Coronavirus (2019-NCoV): situation Report, 11. World Health Organization; 2020. Available from: https://apps.who.int/iris/handle/10665/330776.
2. CDC. COVID data tracker. centers for disease control and prevention. Available from: https://covid.cdc.gov/covid-data-tracker.
3. Ministry Of Health Saudi Arabia. Ministry Of Health Saudi Arabia. Available from: https://www.moh.gov.sa/en/Pages/Default.aspx.
4. Ministry of Health. Dental Emergency Protocol During COVID-19 Pandemic; 2020. Available from: https://www.moh.gov.sa/Ministry/MediaCenter/Publications/Documents/MOH-Dental-emergency-guideline.
5. COVID Statement | oral Health | CDC; 2022. Available from: https://www.cdc.gov/oralhealth/infectioncontrol/statement-COVID.html.
6. Alyami M, de Albuquerque JV, Krägeloh CU, Alyami H, Henning MA. Effects of Fear of COVID-19 on Mental Well-Being and Quality of Life among Saudi Adults: a Path Analysis. Saudi J Med Med Sci. 2021;9(1):24–30. doi:10.4103/sjmms.sjmms_630_20
7. Alkhamees AA, Aljohani MS, Alghesen MA, Alhabib AT. Psychological Distress in Quarantine Designated Facility During COVID-19 Pandemic in Saudi Arabia. Risk Manag Healthc Policy. 2020;13:3103–3120. doi:10.2147/RMHP.S284102
8. Ibrahim MS, Alibrahim H, Al Madani A, Alamri A, Bamashmous M, Tounsi A. Fear Factor in Seeking Dental Care among Saudis during COVID-19 Pandemic. Int J Environ Res Public Health. 2021;18(20):10589. doi:10.3390/ijerph182010589
9. Ashok N, Rodrigues JC, Azouni K, et al. Knowledge and Apprehension of Dental Patients about MERS-A Questionnaire Survey. J Clin Diagn Res JCDR. 2016;10(5):ZC58–62. doi:10.7860/JCDR/2016/17519.7790
10. Sun J, Xu Y, Qu Q, Luo W. Knowledge of and attitudes toward COVID-19 among parents of child dental patients during the outbreak. Braz Oral Res. 2020;34:e066. doi:10.1590/1807-3107BOR-2020.vol34.0066
11. Aljafar A, Alibrahim H, Alahmed A, et al. Reasons for Permanent Teeth Extractions and Related Factors among Adult Patients in the Eastern Province of Saudi Arabia. Sci World J. 2021;2021:e5534455. doi:10.1155/2021/5534455
12. El Bcheraoui C, Tuffaha M, Daoud F, et al. Use of dental clinics and oral hygiene practices in the Kingdom of Saudi Arabia, 2013. Int Dent J. 2016;66(2):99–104. doi:10.1111/idj.12210
13. Al-Jaber A, Da’ar OB. Primary health care centers, extent of challenges and demand for oral health care in Riyadh, Saudi Arabia. BMC Health Serv Res. 2016;16(1):628. doi:10.1186/s12913-016-1876-6
14. Quadri FA, Jafari FA, Albeshri AT, Zailai AM. Factors influencing Patients’ Utilization of Dental Health Services in Jazan, Kingdom of Saudi Arabia. Int J Clin Pediatr Dent. 2018;11(1):29–33. doi:10.5005/jp-journals-10005-1479
15. Kawamura M. Dental behavioral science. The relationship between perceptions of oral health and oral status in adults. Hiroshima Daigaku Shigaku Zasshi. 1988;20(2):273–286.
16. Dagli RJ, Tadakamadla S, Dhanni C, Duraiswamy P, Kulkarni S. Self reported dental health attitude and behavior of dental students in India. J Oral Sci. 2008;50(3):267–272. doi:10.2334/josnusd.50.267
17. Uppin RB, Aldawsari AF, Alsulaiman SA, Alotaibi IA, Almutairi FS. Self reported oral health behavior and dental attendance pattern between smokers and non-smokers in Saudi Arabia: a cross-sectional study. Med Sci. 2022;26:ms516e2624. doi:10.54905/disssi/v26i130/ms516e2624
18. Riad A, Al-Khanati NM, Issa J, et al. Oral Health-Related Knowledge, Attitudes and Behaviours of Arab Dental Students: multi-National Cross-Sectional Study and Literature Analysis 2000-2020. Int J Environ Res Public Health. 2022;19(3):1658. doi:10.3390/ijerph19031658
19. AlMugeiren OM, Baseer MA, AlSenani YA, et al. Comparative evaluation of oral health attitudes and behaviors among dental and medical students during COVID-19 pandemic in Saudi Arabia. Eur Rev Med Pharmacol Sci. 2022;26(9):3351–3360. doi:10.26355/eurrev_202205_28755
20. Komabayashi T, Kawamura M, Kim KJ, et al. The hierarchical cluster analysis of oral health attitudes and behaviour using the Hiroshima University - Dental Behavioural Inventory (HU-DBI) among final year dental students in 17 countries. Int Dent J. 2006;56(5):310–316. doi:10.1111/j.1875-595X.2006.tb00106.x
21. Carter E, Currie CC, Asuni A, et al. The first six weeks - setting up a UK urgent dental care centre during the COVID-19 pandemic. Br Dent J. 2020;228(11):842–848. doi:10.1038/s41415-020-1708-2
22. Guo H, Zhou Y, Liu X, Tan J. The impact of the COVID-19 epidemic on the utilization of emergency dental services. J Dent Sci. 2020;15(4):564–567. doi:10.1016/j.jds.2020.02.002
23. Meisha DE, Alsolami AM, Alharbi GM. Social determinants of seeking emergency and routine dental care in Saudi Arabia during the COVID-19 pandemic. BMC Oral Health. 2021;21(1):212. doi:10.1186/s12903-021-01577-1
24. Opeodu OI, Dosumu EB, Arowojolu MO. Dental health service utilisation by resident doctors/medical officers in the University College Hospital, Ibadan, Oyo State, Nigeria. Afr J Med Med Sci. 2012;41(3):277–282.
25. Kawamura K, Kawabata K, Sasahara H, Fakuda S, Iwamoto Y. Dental behavioral science: part IX. Bilinguals’ responses to the dental behavioral inventory (HU-DBI) written in English and in Japanese. J Hiroshima Univ Dent Soc. 1992;22:198–204.
26. Karem hassan B, Jabbar Ali B, Mahmood Alwan A, Badeia R. Self-Reported Oral Health Attitudes and Behaviors, and Gingival Status of Dental Students. Clin Cosmet Investig Dent. 2020;12:225–232. doi:10.2147/CCIDE.S249708
27. Al-Hussyeen AJA. Factors affecting utilization of dental health services and satisfaction among adolescent females in Riyadh City. Saudi Dent J. 2010;22(1):19–25. doi:10.1016/j.sdentj.2009.12.004
28. Farsi JMA. Dental visit patterns and periodontal treatment needs among Saudi students. East Mediterr Health J Rev Sante Mediterr Orient Al-Majallah Al-Sihhiyah Li-Sharq Al-Mutawassit. 2010;16(7):801–806.
29. Almutlaqah MA, Baseer MA, Ingle NA, Assery MK, Al Khadhari MA. Factors Affecting Access to Oral Health Care among Adults in Abha City, Saudi Arabia. J Int Soc Prev Community Dent. 2018;8(5):431–438. doi:10.4103/jispcd.JISPCD_205_18
30. Riley JL, Gilbert GH, Heft MW. Dental attitudes: proximal basis for oral health disparities in adults. Community Dent Oral Epidemiol. 2006;34(4):289–298. doi:10.1111/j.1600-0528.2006.00280.x
31. Gbolahan OO, Fasola AO, Aladelusi TO. Attitude and Behavior to Oral Health of 456 Patients Who Presented for Tooth Extraction at 2 Health Facilities in Southwestern Nigeria. J Patient Exp. 2019;6(2):157–163. doi:10.1177/2374373518788851
32. Alshahrani AM, Raheel SA. Health-care System and Accessibility of Dental Services in Kingdom of Saudi Arabia: an Update. J Int Oral Health. 2016;8(8):54.
33. Johnson R, Horne B, Feltbower RG, Butler GE, Glaser AW. Hospital attendance patterns in long term survivors of cancer. Arch Dis Child. 2004;89(4):374–377. doi:10.1136/adc.2002.021816
34. Kawachi I, Adler NE, Dow WH. Money, schooling, and health: mechanisms and causal evidence. Ann N Y Acad Sci. 2010;1186:56–68. doi:10.1111/j.1749-6632.2009.05340.x
35. Singh A, Peres MA, Watt RG. The Relationship between Income and Oral Health: a Critical Review. J Dent Res. 2019;98(8):853–860. doi:10.1177/0022034519849557
36. AlBaker AA, Al-Ruthia YSH, AlShehri M, Alshuwairikh S. The characteristics and distribution of dentist workforce in Saudi Arabia: a descriptive cross-sectional study. Saudi Pharm J SPJ off Publ Saudi Pharm Soc. 2017;25(8):1208–1216. doi:10.1016/j.jsps.2017.09.005
37. Qi X, Qu X, Wu B. Urban-Rural Disparities in Dental Services Utilization Among Adults in China’s Megacities. Front Oral Health. 2021;2. doi:10.3389/froh.2021.673296
38. Suzuki S, Sugiyama S, Okamoto M, et al. Working Environment Factors Associated with Regular Dental Attendance. Bull Tokyo Dent Coll. 2017;58(3):193–197. doi:10.2209/tdcpublication.2016-0030
39. Aljafar A, Alibrahim H, Alahmed A, et al. Reasons for Permanent Teeth Extractions and Related Factors among Adult Patients in the Eastern Province of Saudi Arabia. ScientificWorldJournal. 2021;2021:5534455. doi:10.1155/2021/5534455
40. Almahdi HM, Alabdrabulridha Z, AlAbbas J, et al. Permanent First Mandibular Molar: loss Prevalence and Pattern among Saudis in Al-Ahsa. Eur J Dent. 2022. doi:10.1055/s-0042-1757904
41. Oginni FO. Tooth loss in a sub-urban Nigerian population: causes and pattern of mortality revisited. Int Dent J. 2005;55(1):17–23. doi:10.1111/j.1875-595x.2005.tb00027.x
42. Cervino G, Fiorillo L, Surace G, et al. SARS-CoV-2 Persistence: data Summary up to Q2. Data. 2020;5:81. doi:10.3390/data5030081
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.