Back to Journals » Clinical Ophthalmology » Volume 18
Comparative Analysis of the Osmoprotective Effects of Daily Disposable Contact Lens Packaging Solutions on Human Corneal Epithelial Cells
Authors VanDerMeid KR, Byrnes MG, Millard K, Scheuer CA, Phatak NR ![]() , Reindel W
, Reindel W
Received 22 September 2023
Accepted for publication 12 December 2023
Published 25 January 2024 Volume 2024:18 Pages 247—258
DOI https://doi.org/10.2147/OPTH.S437841
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Karl R VanDerMeid, Mirzi Grace Byrnes, Kimberly Millard, Catherine A Scheuer, Nitasha R Phatak, William Reindel
Vision Care, Bausch & Lomb Incorporated, Rochester, NY, USA
Correspondence: Nitasha R Phatak, Vision Care, Bausch & Lomb Incorporated, Rochester, NY, USA, Tel +1 585-413-6397, Email [email protected]
Purpose: Contact lens (CL) wear challenges the balance of the ocular surface environment by increasing water evaporation and tear osmolarity. Maintaining ocular surface homeostasis during CL wear remains a goal of lens manufacturers and an important consideration for eye care professionals. The purpose of this study was to measure the metabolic activity and inflammatory responses of a transformed human corneal epithelial cell (THCEpiC) line under hyperosmotic conditions in the presence of CL packaging solutions.
Methods: CL packaging solutions sampled from seven daily disposable silicone hydrogel CL blister packages were prepared at 25% and made hyperosmolar (400 mOsm/kg) with NaCl. THCEpiCs were incubated with each solution for 24 hr, after which cell culture supernatants were collected. THCEpiC metabolic activity was determined by an alamarBlue assay. Concentrations in cell culture supernatants of inflammatory cytokine (interleukin [IL]-6) and chemokine (IL-8), as well as monocyte chemoattractant protein-1 (MCP-1), were quantitated by specific enzyme-linked immunosorbent assays.
Results: THCEpiC metabolic activity under hyperosmolar conditions decreased in the presence of somofilcon A and senofilcon A solutions (p=0.04 and 0.004, respectively), but no other solution (all p≥ 0.09). Concentrations of IL-6 increased in the presence of delefilcon A, somofilcon A, narafilcon A, and senofilcon A solutions (all p≤ 0.001), but no other solution (all p≥ 0.08), while those of IL-8 increased in the presence of all solutions (all p≤ 0.03) but kalifilcon A (p> 0.99), and those of MCP-1 increased in the presence of delefilcon A, verofilcon A, somofilcon A, and stenfilcon A solutions (all p< 0.0001), but no other solution (all p> 0.99).
Conclusion: CL packaging solutions differ in their capacity to inhibit epithelial inflammation. THCEpiC inflammatory response was less in the presence of a CL packaging solution containing osmoprotectants than in solutions lacking osmoprotectants under moderately hyperosmolar conditions in vitro. Clinical studies are warranted to further substantiate the benefit of osmoprotectants.
Keywords: contact lens, cornea, TFOS, hyperosmolarity, osmoprotection, homeostasis
Introduction
Contact lens (CL) is one of the most widespread and successfully used medical devices available today. The Centers for Disease Control and Prevention (CDC, Atlanta, GA) estimated that about 45 million people older than 17 wore CLs in the United States,1 and the Tear Film and Ocular Surface Society (TFOS) International Workshop on Contact Lens Discomfort estimated that over 140 million people wore CLs worldwide.2 Recent advances in lens design and manufacturing with the goal of maintaining ocular surface homeostasis have led to newer CLs with the potential to better maintain eye health and comfort during CL wear. This includes more benign interactions between the lens material, the tear film, and the ocular surface with which it makes intimate contact.
A 2017 report of the TFOS International Dry Eye Workshop II (TFOS DEWS II) defined dry eye disease (DED) as
a multifactorial disease of the ocular surface characterized by a loss of homeostasis of the tear film, and accompanied by ocular symptoms, in which tear film instability and hyperosmolarity, ocular surface inflammation and damage, and neurosensory abnormalities play etiological roles.3
The report attributes DED to reduced tear secretion leading to inflammation and peripheral nerve alteration, the former activating nociceptor nerve endings responsible for the sensation of dryness and pain.4 While the exact relationship between dryness-mediated cellular and molecular inflammatory mechanisms and peripheral nociceptor terminals is not completely understood, such receptors might respond to both the mechanical stress of tear breakup and the hyperosmotic stress of tears following tear film evaporation.4
DED symptoms can occur both in the presence or absence of CLs, the former including CL-induced dry eye (CLIDE, characterized by DED signs and symptoms that did not exist prior to CL wear) and CL-associated dry eye (CLADE, characterized by DED signs and symptoms during CL wear).5 The TFOS DEWS II report summarizes the consequences of CL wear that lead to CLIDE and CLADE, including a thinner, patchy lipid layer, poor wettability with impaired spreading, tear film instability, increased tear evaporation rate, lower basal tear turnover rate, increased tear osmolarity, and reduced tear film meniscus volume, as well as biochemical changes within the tear film.5 CL wear further challenges ocular surface homeostasis by disrupting the tear film, splitting it into distinct pre-lens and post-lens films,6,7 which can lead to undesirable physical and chemical interactions between the lens, the tear film, and the ocular surface. This manifests as evaporation from the pre-lens tear film and the deleterious consequences of tear film thinning.8 The TFOS DEWS II report additionally cites tear hyperosmolarity and inflammatory mediators as causes of DED symptoms and ocular cell damage and dysfunction.9 McMonnies proposed an amplifying evaporative dryness cascade that occurs during CL wear, culminating in hyperosmolar tears, CL dryness, and ocular surface inflammation;10 the latter occurs in response to hyperosmolar tears,10 but proteins sorbed on and denatured at the CL surface,11 as well as mechanical irritation by a dehydrated and dewetted lens, can also play a role. CLs that best maintain water at the surface and throughout the lens to ameliorate hyperosmolarity if it does occur might help prevent or reduce ocular surface inflammation, as this may prevent the dryness cycle leading to loss of homeostasis.12
Tear hyperosmolarity was recognized as a core mechanism of DED prior to DEWS II,13,14 but DEWS II recognized loss of tear film homeostasis as the unifying element.3 Hyperosmolar tears are reported to disturb ocular homeostasis primarily by affecting ocular inflammation via corneal epithelial cell expression of inflammatory cytokines, chemokines, and matrix metalloproteinases (eg MMP-9).15–19 This occurs through activation of mitogen-activated protein kinase p38, c-Jun N-terminal kinase, nuclear factor-kB, and activator protein-1.20 Hyperosmolarity also leads to loss of barrier function,21,22 increases corneal epithelial transient receptor potential vanilloid type-1 channel activity,23 affects cellular apoptosis,24 and disrupts normal cellular metabolism.25 Additionally, hyperosmolar stress is reported to disrupt neuroimmune homeostasis of the ocular surface by reducing the density of corneal intraepithelial nerves and terminals and sensitizing the ocular surface to hypertonicity,26 as well as induce functional and structural alterations of corneal nerves.27 Hyperosmolar stress can also inhibit neutrophil activity, reducing protection against corneal infection.28
Cytokine interleukin (IL)-6 and chemokines IL-8 and monocyte chemoattractant protein-1 (MCP-1) are significant pro-inflammatory mediators whose concentrations are frequently reported to increase significantly in the tears of DED patients.29–31 However, clinical testing is not always feasible for evaluating novel ocular formulations, and cellular models have proven to be more efficient.
Further, while physical and chemical characterizations of many contact lens packaging and care solutions (eg, pH, osmolarity, surface tension, and viscosity) have been reported in literature,32,33 neither the clinical significance of each individual property nor the combination of all properties is completely understood. As such, in vitro cell line models are frequently employed for multi-purpose solution (MPS) cytotoxicity studies and for evaluating the potential effects of ocular formulation ingredients due to their availability and reproducibility. Numerous studies have demonstrated that human corneal epithelial cells exposed to hyperosmolar and desiccation stresses induced significant IL-6, IL-8, and MCP-1 responses;34,35 as such, these pro-inflammatory mediators were selected for measurement in this study.
Fortunately, several osmolytes have been found to be effective in osmoregulation and mitigation of the deleterious effects of tear hyperosmolarity;36,37 these include amino acids and their derivatives such as proline, betaine, and L-carnitine, as well as polyols such as erythritol and glycerol, and sugars and their derivatives such as trehalose.16,23,24,36–51 Including these osmotic management agents in ocular solutions like artificial tears, CL MPSs, and CL rewetting drops may help ameliorate the effects of tear film evaporation and maintain ocular surface homeostasis. Studies in literature report decreased symptoms of eye dryness and improved comfort in CL wearers using rewetting drops containing osmoprotectants.50,51
In many CL packaging solutions, buffering agents like sodium chloride and sodium salts, such as sodium borates and sodium phosphates, contribute the most to the total solution osmolarity. Substituting potassium for sodium reduces the concentration of sodium, which is the electrolyte whose concentration becomes elevated in lacrimal gland disease.52 Additionally, including organic osmolytes in the solution allows for further reduction in sodium concentration.
Lens manufacturers incorporate ingredients into their CLs, including daily disposable (DD) silicone hydrogel lenses,53 through their respective solutions to support the lens,54 including one that contains osmoprotectants. The delefilcon A and verofilcon A (both Alcon Laboratories, Inc., Ft. Worth, TX) solutions contain copolymers of polyamidoamine and poly(acrylamide-acrylic) acid;55,56 the kalifilcon A (Bausch & Lomb Incorporated, Rochester, NY) solution contains poloxamer 181, poloxamine 1107, glycerin, and erythritol;57 the somofilcon A and stenfilcon A (both CooperVision Inc., Pleasanton, CA) solutions contain poloxamer 407 and polysorbate, respectively;58,59 and the narafilcon A and senofilcon A (both Johnson & Johnson Inc., Jacksonville, FL) solutions contain methyl ether cellulose60,61 (Table 1). The objectives of this study were as follows: 1. To determine if ingredients for managing osmolarity affect metabolic activity and cytokine/chemokine levels of human corneal epithelial cells under hyperosmotic stress and 2. To measure and compare metabolic activity and cytokine/chemokine levels of the same cell line exposed to DD silicone hydrogel CL packaging solutions with and without osmoprotectants under hyperosmotic conditions.
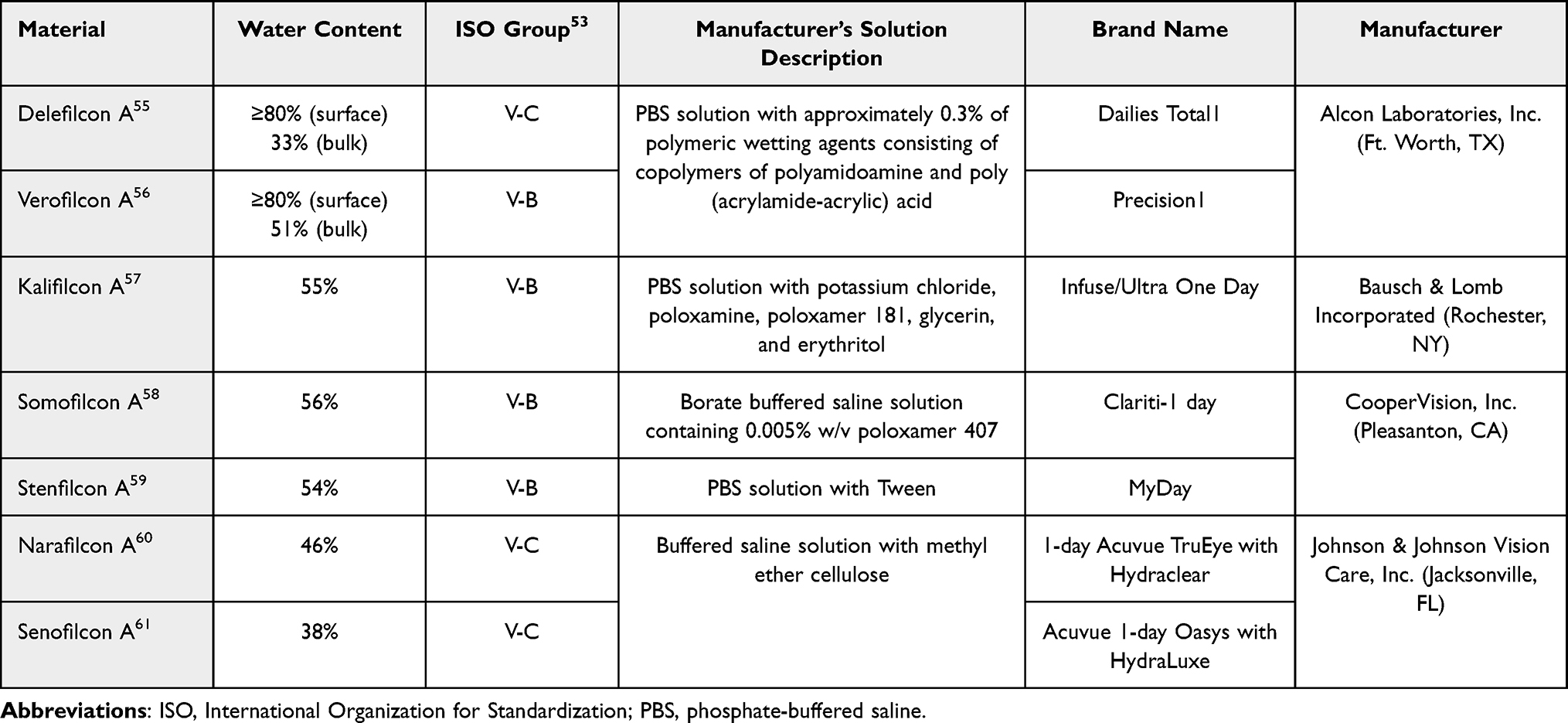 |
Table 1 Contact Lenses Evaluated |
Materials and Methods
Cell Line
A human corneal epithelial cell transformed with simian virus 40 to corneal epithelial cell line 2.040 pRSV-T (ATCC® CRL-11516™) (THCEpiC) was obtained from the American Type Culture Collection (ATCC, Manassas, VA). Such cell lines are commonly used in studies of corneal epithelium,62,63 as they do not vary phenotypically compared with primary cells. THCEpiCs were received at passage 22 and used between passages 25 and 40 for these experiments. Cells were grown in Gibco™ EpiLife™ Medium (Catalog number MEPI500CA, Thermo Fisher Scientific, Waltham, MA) with human corneal growth supplement (Catalog number S0095, Thermo Fisher Scientific) and 50 IU/mL penicillin/50 μg/mL streptomycin (Catalog number 15-140-122, Thermo Fisher Scientific).
Cell Culture
Cells were cultured in a supplemented EpiLife medium in a 5% CO2/95% humidity incubator at 37°C for 72 hr for all experiments. The medium was then replaced with a fresh medium, and the cells were incubated for additional 24 hours under the same conditions prior to incubation with test solutions.
Preparation of Hyperosmolar Test Media
Hyperosmolar media (400, 450, 500, and 530 mOsm/kg) with or without 0.9% erythritol + 0.9% glycerin osmoprotectants added were prepared from basal medium by addition of NaCl.
Preparation of Hyperosmolar Contact Lens Solutions
Preliminary experiments indicated that 50% CL packaging solutions significantly affected cell metabolic activity in 450 and 500 mOsm/kg hyperosmolar media. Therefore, CL packaging solutions were sampled from delefilcon A, verofilcon A, kalifilcon A, somofilcon A, stenfilcon A, narafilcon A, and senofilcon A blister packages (Table 1); for each lens, three to four packages of solution from same lot number were pooled, diluted to 25%, and made hyperosmolar [400 mOsm/kg] by addition of NaCl. Hanks’ Balanced Salt Solution (HBSS) diluted to 25% was prepared as the control.
Experimental Procedure
THCEpiCs cultured to confluency in 96 well plates were incubated for 24 hr with 0.25 mL of normal osmolar (315 mOsm/kg) and hyperosmolar media (450, 500, and 530 mOsm/kg), with or without osmoprotectants to determine the effect of osmolarity and osmoprotection on metabolic activity. Note that 315 mOsm/kg tonicity of normal medium is slightly hypertonic relative to normal tears, in which a value of 316 mOsm/L was the threshold proposed as the “osmolarity referent” in the diagnosis of keratoconjunctivitis sicca, compared with an average value of 302 ± 9.7 mOsm/L for normal tears across 16 published studies;64 subsequently, the TFOS DEWS report proposed 308 mOsm/L as a sensitive threshold for early-stage DED.28 More recently, 316 mOsm/L in either eye, 308 mOsm/L in both eyes, or >8 mOsm/L inter-eye difference was proposed as a pathological cut-off.65,66 It should be noted that these values refer to osmolarity of tears sampled from the meniscus and that local, transient osmolarity in areas of high evaporation rate and tear break-up can be as high as 600–900 mOsm/L.67,68 In this study, isotonic refers to normal media rather than normal tears, regardless of the definition of “normal” tear osmolarity.
After determining the osmolarity at which cell metabolism decreases relative to normal medium (500 mOsm/kg), as well as the osmolarity at which osmoprotectants lessen the decrease in cell metabolism relative to unprotected media (530 mOsm/kg), the experiment was repeated using media ranging from normal (315 mOsm/kg) to hypertonic (400, 450, 500 mOsm/kg), ie, concentrations at which respective solutions with and without osmoprotectants do not affect cell metabolism differently. Cell culture supernatants were collected for assessment of cytokine/chemokine activation.
To evaluate the interactions between THCEpiCs and CL solutions, the experiment was repeated using moderately hypertonic (400 mOsm/kg) solutions to increase the likelihood that no CL solution would decrease metabolic activity.
Cell Metabolism and Cytokine/Chemokine Activity Assays
An alamarBlue assay was performed to evaluate THCEpiC metabolic activity incubation with the respective solutions.69 Cell culture supernatants were quantitated with specific enzyme-linked immunosorbent assays (ELISAs) for the detection of inflammatory cytokine (IL-6) and chemokines (IL-8, MCP-1) (Quantikine ELISA, R&D Systems, Inc., Minneapolis, MN). IL-6, IL-8, and MCP-1 were chosen as biomarkers of corneal inflammation due to their respective roles in the pathogenesis of DED.70 IL-6 affects differentiation of B cells into antibody producing cells,71 IL-8 affects neutrophil activation in response to inflammatory stimuli,72 and MCP-1 acts as a monocyte chemoattractant.73 Hyperosmolar stress has been reported to increase corneal epithelial production of IL-6 and IL-8,25,34 as well as MCP-1.34 While evidence that reducing these inflammatory markers improves clinical outcomes is lacking in literature, recent studies demonstrate that anti–IL-6 antibodies reduce inflammatory responses, both in vitro and in a murine model of fungal keratitis,74 and alkali burn.75
In this study, metabolic activity data were collected from four replicates per test group (n=4). Pro-inflammatory cellular response markers were collected from these same test groups.
Statistical Analysis
All test group data sets were first analyzed using descriptive statistics and calculated as the mean values and standard errors. Additional statistical analysis was evaluated for any statistical significance by two-way analysis of variance (ANOVA) followed by Tukey’s or Dunnett’s multiple comparisons.76 Results were considered statistically significant at an alpha level of 5.0% and a p-value ≤0.05. All test group data sets were analyzed using GraphPad Prism version 8.0 for Windows (GraphPad Software, San Diego, CA; www.graphpad.com).
Results
Metabolic activity of THCEpiCs incubated with hyperosmolar media with and without added osmoprotectants is shown in Figure 1. Activity decreased with increased solution osmolarity, the difference from isotonic being significant at 500 and 530 mOsm/kg (both p≤0.0001). Activity is greater in the presence of osmoprotectants only in the higher osmolar medium (530 mOsm/kg; p≤0.0001).
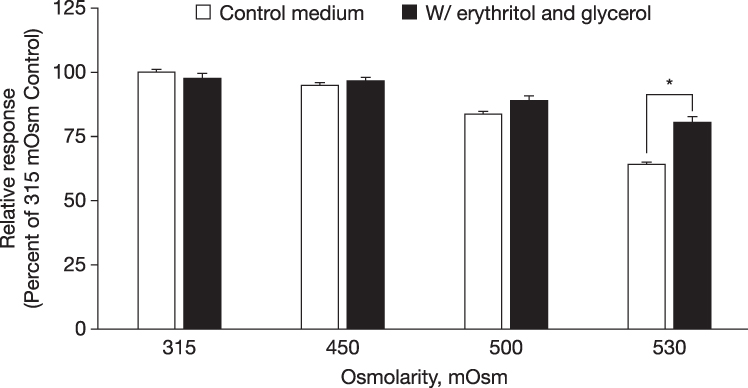 |
Figure 1 Metabolic activity relative to control medium of THCEpiC cultured in baseline EpiLife control medium until confluent, then incubated with hyperosmolar EpiLife medium in the absence (□ bars) or presence (■ bars) of 0.9% erythritol + 0.9% glycerol (mean ± standard error). Two-way ANOVA versus equivalent hyperosmolarity without osmoprotectants using Tukey’s multiple comparisons (*p≤0.05). Abbreviations: ANOVA, analysis of variance; THCEpiC, transformed human corneal epithelial cell. |
Cytokine/chemokine concentrations measured in the supernatants of isotonic and hypertonic media are shown in Figure 2A–D. The addition of glycerol and erythritol osmoprotectants significantly reduced pro-inflammatory cytokine/chemokine response at solution osmolarities of 400 mOsm/kg (MCP-1, p=0.04; Figure 2D) and 450–500 mOsm/kg (IL-6, both p=0.02, and IL-8, both p<0.0001; Figure 2B and C, respectively).
 |
Figure 2 (A) Baseline metabolic activity of THCEpiC cultured in baseline EpiLife control medium until confluent, then incubated with hyperosmolar EpiLife medium in the absence (□ bars) or presence (■ bars) of 0.9% erythritol + 0.9% glycerol relative to 25% HBSS control (mean ± standard error); (B) Relative IL-6 response; (C) Relative IL-8 response; (D) Relative MCP-1 response. For (A), two-way ANOVA followed by Dunnett’s multiple comparisons finds no significant differences in metabolic activity with or without osmoprotection at equivalent osmolarity (p≥0.05). For (B–D), two-way ANOVA versus equivalent hyperosmolarity without osmoprotectants followed by Dunnett’s multiple comparisons (*p≤0.05). Abbreviations: ANOVA, analysis of variance; HBSS, Hanks’ Balanced Salt Solution; IL, interleukin; MCP-1, monocyte chemoattractant protein-1; THCEpiC, transformed human corneal epithelial cell. |
THCEpiC metabolic activity in all isotonic CL solutions was comparable to that in the HBSS control (all p>0.05, data not shown). Metabolic activity in moderately hypertonic (400 mOsm/kg) diluted CL solutions, as well as supernatant cytokine/chemokine responses relative to control, are shown in Figure 3. Activity was lower in hypertonic somofilcon A and senofilcon A CL solutions (p=0.04 and 0.004, respectively), but not kalifilcon A (p=0.84), delefilcon A (p=0.65), verofilcon A (p=0.97), narafilcon A (p=0.09), or stenfilcon A (p=0.45; Figure 3A). IL-6 responses were greater in hypertonic solutions of delefilcon A (p=0.001), somofilcon A, narafilcon A, and senofilcon A (all p<0.0001), but not kalifilcon A (p=0.67), verofilcon A (p=0.26), or stenfilcon A (p=0.08; Figure 3B). IL-8 responses were greater in hypertonic solutions of all CLs (delefilcon A, senofilcon A, narafilcon A, and somofilcon A (all p<0.0001), verofilcon A (p=0.0001), and stenfilcon A (p=0.03) but kalifilcon A (p>0.99; Figure 3C)). MCP-1 responses were greater in hypertonic solutions of delefilcon A, verofilcon A, somofilcon A, and stenfilcon A (all p<0.0001), but not kalifilcon A, narafilcon A, or senofilcon A (all p>0.99, Figure 3D).
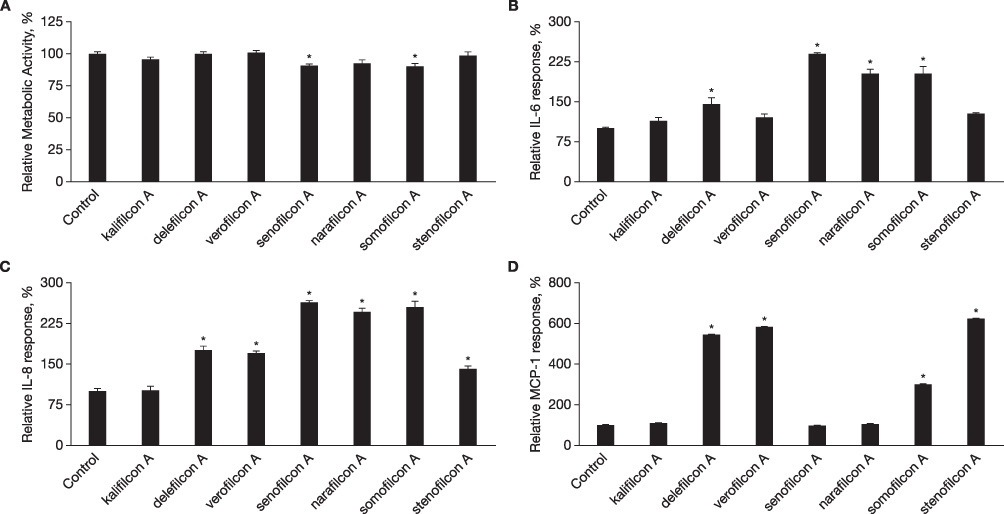 |
Figure 3 (A) Metabolic activity of THCEpiC cultured in baseline EpiLife control medium until confluent, then exposed to 400 mOsm/kg hyperosmolar CL solutions relative to 25% HBSS control (mean ± standard error); (B) Relative IL-6 response; (C) Relative IL-8 response; (D) Relative MCP-1 response. Two-way ANOVA followed by Dunnett’s multiple comparisons (* indicates greater than control; all p≤0.05). Abbreviations: ANOVA, analysis of variance; CL, contact lens; HBSS, Hanks’ Balanced Salt Solution; IL, interleukin; MCP-1, monocyte chemoattractant protein-1; THCEpiC, transformed human corneal epithelial cell. |
Discussion
Tear concentrations of certain inflammatory markers, notably IL-1β, IL-6, IL-8, IL-17, LTB4, and MMP-9, are reported to increase over the daily course of CL wear, more so with planned replacement compared with DD lenses.77 A study of CL wearers found that in a controlled adverse desiccating environment (5% relative humidity, 23°C, and 0.43 m/s [mean velocity] localized airflow), those subjects whose tears contained the highest levels of inflammatory cytokines IL-4 and IL-6 were associated with increased CL wear symptoms including dryness and discomfort,78 which is significant as these are the primary reasons for CL discontinuation.79 A similar study found the increase in tear concentrations of some inflammatory mediators to differ between CL models,80 possibly reflecting differences in lens polymers and components of their respective packaging solutions. In most CL wearers, ocular surface inflammation is not a major complication of lens wear and is often asymptomatic if it does occur.81 Nonetheless, it can contribute to discomfort at the end of the day.10 Most CL-mediated inflammation is reported to be subclinical with DD lens wear.82
With the recognition that maintaining ocular homeostasis during CL wear has the potential to improve lens comfort and vision,83 manufacturers have adopted technologies that support homeostasis. While improving lens water retention during wear represents one approach,84,85 infusion of beneficial ingredients into the lens is another.86 All lenses evaluated in this study include humectant and/or surfactant wetting agents in the solution; the kalifilcon A lens additionally includes osmoprotectants also used in other ocular solutions,36,37 as well as potassium electrolyte.57 While physical and chemical characterization of CL packaging solutions is beyond the scope of this study, published literature demonstrates broad ranges in pH, osmolarity, and surface tension of commercial CL blister package solutions, as well as variation in contact angle between different lens/solution combinations, reflective of the surfactants in the solutions and the specific lenses.87,88
THCEpiCs were used in this study to determine the effects of glycerol and erythritol osmoprotectants, as well as CL packaging solutions, upon epithelial stress in hyperosmotic cell culture media. Experiments with isotonic and hyperosmolar cell culture media with and without osmoprotectants highlight two important phenomena. First, THCEpiC metabolic activity in isotonic medium was comparable to that in 450 mOsm/kg medium, while activity in 500 and 530 mOsm/kg media was significantly less; further, the osmoprotectants minimized loss of metabolic activity only in high osmolarity medium (530 mOsm/kg). Second, when cell culture supernatants were analyzed under conditions of equivalent metabolic activity and the same osmolarity, significantly lower cytokine/chemokine responses were observed with osmoprotectants at thresholds of 450 mOsm/kg (IL-6 and IL-8; Figure 2B and C) and 400 mOsm/kg (MCP-1; Figure 2D). These results are similar to those of Corrales et al, who reported that osmoprotectants L-carnitine and erythritol, alone or in combination, protected against hyperosmolar stress activation of primary corneal epithelial cells cultured in 400 mOsm/kg media;38 and Hua et al, who reported that L-carnitine, erythritol, and betaine reduced expression of pro-inflammatory cytokines and chemokines by primary corneal epithelial cells cultured in 450 mOsm/kg media,40 suggesting that osmoprotectants could play a role in reducing hyperosmotic stress in CL dryness.
Decreased metabolic activity in high osmolarity solutions suggests that investigations of cellular response to hyperosmolar solutions be conducted at osmolarities no greater than 450 mOsm/kg to avoid concomitant responses due to change in cellular metabolism. For this reason, THCEpiC interactions with CL solutions were investigated in a moderately hypertonic medium (400 mOsm/kg). Because the osmolarities of the evaluated CL packaging solutions vary from hypotonic to hypertonic, solutions were first diluted to 25%, then osmolarity was adjusted by the addition of NaCl. THCEpiC metabolic activity was lower in hypertonic (400 mOsm/kg) senofilcon A and somofilcon A CL solutions compared with HBSS control (Figure 3A), complicating interpretation of cytokine/chemokine response to these solutions. IL-6 concentrations were greater in hypertonic solutions of delefilcon A, somofilcon A, narafilcon A, and senofilcon A compared with control (Figure 3B). IL-8 concentrations were greater in hypertonic solutions of all CLs but kalifilcon A (Figure 3C). MCP-1 concentrations were greater in hypertonic solutions of delefilcon A, verofilcon A, somofilcon A, and stenfilcon A (Figure 3D).
All CL solutions except kalifilcon A elicit at least one cytokine/chemokine response under hyperosmotic conditions. Overall, the kalifilcon A solution elicited the least THCEpiC inflammatory response, likely reflecting in part the presence of the osmoprotectants, consistent with the results in cell culture media. Previous in vitro studies similarly report solution-dependent responses to different CL packaging solutions89 and MPSs.90,91 The present study demonstrates the potential for osmoprotectants to reduce corneal epithelial stress under hyperosmotic conditions that occur in some CL wearers, particularly at the end of the day.10
The clinical benefit of osmoprotectants in the packaging solution has not been widely studied. While CLs packaged in solutions lacking osmoprotectants have acceptable performance in asymptomatic wearers and wearers experiencing only minor symptoms while wearing lenses,92–96 a recent clinical study found that subjects who reported experiencing CL dryness symptoms with their habitual lenses noticed increased comfort while wearing the kalifilcon A lens.86 In addition, a different study reported that CL wearers who used hypo-osmotic saline drops, which reduce tear osmolarity by dilution experienced improved end-of-day comfort and reduced dryness and burning.97 We propose that while hyperosmotic stress leading to ocular inflammation in symptomatic patients results in discomfort, inclusion of osmoprotectants in CL packaging solutions can lead to decreased symptoms of discomfort.
While moisturizers and surfactants have previously been used in ophthalmic and CL solutions, the infusion of osmoprotectants into a commercial CL packaging solution is a more recent development. Components included in the kalifilcon A solution were selected based upon recommendations from the TFOS DEWS II report,37 while maintaining ocular surface homeostasis in mind.86 Surfactants promote tear film spreading98 and stabilize protein structure.99 Poloxamine 1107 is reported to be especially effective at suppressing aggregation of heat-denatured lysozyme.100 Osmoprotectants balance osmotic pressure under osmotic stress, inhibiting inflammation. Glycerin boasts protein stabilizing101 and demulcent properties, while both glycerin and erythritol are included as ingredients in numerous ophthalmic solutions.37,102 Potassium electrolyte plays a role in epithelial surface homeostasis.103 Further investigation to identify properties of other kalifilcon A solution ingredients and any synergistic effect between them is warranted.
The primary limitation of this study is the in vitro nature of the experiments, which do not necessarily predict clinical CL wear outcomes. The ocular surface, which includes multiple cell types, is dynamic and resists internal and external assaults more capably than do exposed cells. In addition, the osmolarities of the solutions evaluated in this study are higher than would typically be found in asymptomatic CL wearers, although transient, local osmolarity can exceed these levels up to three-fold.67,68 Moderately high osmolarity is required to elicit cellular inflammatory responses in vitro in order to evaluate the beneficial effects of CL packaging solutions and their respective ingredients. Also, packaging solutions were tested at 25% of their normal concentrations; it is not known if the solutions and their ingredients at full concentration would elicit the same cellular responses, in vitro or clinically.
Conclusion
Including osmoprotectants in CL packaging solution may protect corneal epithelium from inflammation under hyperosmotic conditions that occur in CL-related DEDs and that, in some wearers, worsen at the end of the day. Other components such as surfactants and potassium electrolyte might also contribute to preserving ocular surface homeostasis, and their potential roles remain to be determined. Overall, this study underscores the significance of exploring novel strategies, particularly osmoprotective agents, to enhance the safety and comfort of CL wearers and maintain ocular health.
Data Sharing Statement
All relevant data are within the manuscript. Clarification requests around the manuscript and its data can be made to the corresponding author.
Acknowledgments
The authors thank Vicki Barniak, Deborah McGrath, Thomas Menzel, and Marjorie Rah (all Bausch & Lomb Incorporated) for thoughtful discussions. Medical writing/editorial support was provided by Joseph Chinn (J Chinn LLC, Lafayette CO) and funded by the study sponsor.
The abstracts of this paper were presented at the virtual 2020 Annual Meeting of the American Academy of Ophthalmology (AAO), held November 13–15, 2020, and the virtual 2021 Association for Research in Vision and Ophthalmology (ARVO) Annual Meeting, held May 1–7, 2021.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was funded by Bausch & Lomb Incorporated.
Disclosure
All authors are employees of Bausch & Lomb Incorporated. Ms Catherine Scheuer reports a patent US 17/398,556 pending to Bausch+Lomb, a patent Taiwan 110129328 pending to Bausch+Lomb, a patent PTC/EP2021/072140 pending to Bausch+Lomb. Dr William Reindel has a patent WO2022034010A1 pending to Bausch+Lomb. The authors report no other conflicts of interest in this work.
References
1. Cope JR, Collier SA, Nethercut H, Jones JM, Yates K, Yoder JS. Risk behaviors for contact lens-related eye infections among adults and adolescents - United States, 2016. MMWR Morb Mortal Wkly Rep. 2017;66(32):841–845. doi:10.15585/mmwr.mm6632a2
2. Nichols JJ, Willcox Nichols JJ, Willcox MDP, et al. The TFOS International Workshop on Contact Lens Discomfort: executive summary. Invest Ophthalmol Vis Sci. 2013;54(11):TFOS7–TFOS13. doi:10.1167/iovs.13-13212
3. Craig JP, Nichols KK, Akpek EK, et al. TFOS DEWS II definition and classification report. Ocul Surf. 2017;15(3):276–283. doi:10.1016/j.jtos.2017.05.008
4. Belmonte C, Nichols JJ, Cox SM, et al. TFOS DEWS II pain and sensation report. Ocul Surf. 2017;15(3):404–437. doi:10.1016/j.jtos.2017.05.002
5. Gomes JAP, Azar DT, Baudouin C, et al. TFOS DEWS II iatrogenic report. Ocul Surf. 2017;15(3):511–538. doi:10.1016/j.jtos.2017.05.004
6. Willcox MDP, Argüeso P, Georgiev G, et al. TFOS DEWS II tear film report. Ocul Surf. 2017;15(3):366–403. doi:10.1016/j.jtos.2017.03.006
7. Guillon M, Dumbleton K, Theodoratos P, et al. Pre-contact lens and pre-corneal tear film kinetics. Cont Lens Anterior Eye. 2019;42(3):246–252. doi:10.1016/j.clae.2019.02.001
8. Guillon M, Maissa C. Contact lens wear affects tear film evaporation. Eye Contact Lens. 2008;34(6):326–330. doi:10.1097/ICL.0b013e31818c5d00
9. Nelson JD, Craig JP, Akpek EK, et al. TFOS DEWS II introduction. Ocul Surf. 2017;15(3):269–275. doi:10.1016/j.jtos.2017.05.005
10. McMonnies CW. An amplifying cascade of contact lens-related end-of-day hyperaemia and dryness symptoms. Curr Eye Res. 2018;43(7):839–847. doi:10.1080/02713683.2018.1457163
11. Latour RA. Fundamental principles of the thermodynamics and kinetics of protein adsorption to material surfaces. Colloids Surf B Biointerfaces. 2020;191:110992. doi:10.1016/j.colsurfb.2020.110992
12. Gupta P, Asbell MP, Sheppard MJ. Current and future pharmacological therapies for the management of dry eye. Eye Contact Lens. 2020;46(Suppl 2):S64–S69 doi:10.1097/ICL.0000000000000666.
13. Lemp MA. Report of the National Eye Institute/Industry workshop on clinical trials in dry eyes. CLAO J. 1995;21(4):221–232.
14. Lemp MA, Foulks GN. The definition and classification of dry eye disease: report of the Definition and Classification Subcommittee of the International Dry Eye Workshop (2007). Ocul Surf. 2007;5(2):75–92. doi:10.1016/S1542-0124(12)70081-2
15. Li DQ, Luo L, Chen Z, Kim HS, Song XJ, Pflugfelder SC. JNK and ERK MAP kinases mediate induction of IL-1beta, TNF-alpha and IL-8 following hyperosmolar stress in human limbal epithelial cells. Exp Eye Res. 2006;82(4):588–596. doi:10.1016/j.exer.2005.08.019
16. Panigrahi T, Shivakumar S, Shetty R, et al. Trehalose augments autophagy to mitigate stress induced inflammation in human corneal cells. Ocul Surf. 2019;17(4):699–713. doi:10.1016/j.jtos.2019.08.004
17. Pflugfelder SC, de Paiva CS, Li DQ, Stern ME. Epithelial-immune cell interaction in dry eye. Cornea. 2008;27 Suppl 1(0 1):S9–S11. doi:10.1097/ICO.0b013e31817f4075
18. Igarashi T, Fujimoto C, Suzuki H, et al. Short-time exposure of hyperosmolarity triggers interleukin-6 expression in corneal epithelial cells. Cornea. 2014;33(12):1342–1347. doi:10.1097/ICO.0000000000000256
19. Liu Z, Chen D, Chen X, et al. Autophagy activation protects ocular surface from inflammation in a dry eye model in vitro. Int J Mol Sci. 2020;21(23):8966. doi:10.3390/ijms21238966
20. Favero G, Moretti E, Krajčíková K, Tomečková V, Rezzani R. Evidence of polyphenols efficacy against dry eye disease. Antioxidants (Basel). 2021;10(2):190. doi:10.3390/antiox10020190
21. Ubels JL, Williams KK, Lopez Bernal D, Edelhauser HF. Evaluation of effects of a physiologic artificial tear on the corneal epithelial barrier: electrical resistance and carboxy fluorescein permeability. Adv Exp Med Biol. 1994;350:441–452.
22. Pflugfelder SC, Bian F, De Paiv C. Matrix metalloproteinase-9 in the pathophysiology and diagnosis of dry eye syndrome. Metalloproteinases Med. 2017;4:37–46. doi:10.2147/MNM.S107246
23. Khajavi N, Reinach PS, Skrzypski M, Lude A, Mergler S. L-carnitine reduces in human conjunctival epithelial cells hypertonic-induced shrinkage through interacting with TRPV1 channels. Cell Physiol Biochem. 2014;34(3):790–803. doi:10.1159/000363043
24. Khandekar N, Willcox MD, Shih S, Simmons P, Vehige J, Garrett Q. Decrease in hyperosmotic stress-induced corneal epithelial cell apoptosis by L-carnitine. Mol Vis. 2013;19:1945–1956.
25. Bogdan ED, Stuard WL, Titone R, Robertson DM. IGFBP-3 mediates metabolic homeostasis during hyperosmolar stress in the corneal epithelium. Invest Ophthalmol Vis Sci. 2021;62(7):11. doi:10.1167/iovs.62.7.11
26. Guzmán M, Miglio M, Keitelman I, et al. Transient tear hyperosmolarity disrupts the neuroimmune homeostasis of the ocular surface and facilitates dry eye onset. Immunology. 2020;161(2):148–161. doi:10.1111/imm.13243
27. Hirata H, Mizerska K, Marfurt CF, Rosenblatt MI. Hyperosmolar tears induce functional and structural alterations of corneal nerves: electrophysiological and anatomical evidence toward neurotoxicity. Invest Ophthalmol Vis Sci. 2015;56:8125e40. doi:10.1167/iovs.15-18383
28. Bron AJ, de Paiva CS, Chauhan SK, et al. TFOS DEWS II pathophysiology report. Ocul Surf. 2017;15(3):438–510. doi:10.1016/j.jtos.2017.05.011
29. Massingale ML, Li X, Vallabhajosyula M, Chen D, Wei Y, Asbell PA. Analysis of inflammatory cytokines in the tears of dry eye patients. Cornea. 2009;28(9):1023–1027. doi:10.1097/ICO.0b013e3181a16578
30. Zhao H, Li Q, Ye M, Yu J. Tear Luminex analysis in dry eye patients. Med Sci Monit. 2018;24:7595–7602. doi:10.12659/MSM.912010
31. Wu X, Chen X, Ma Y, et al. Analysis of tear inflammatory molecules and clinical correlations in evaporative dry eye disease caused by meibomian gland dysfunction. Int Ophthalmol. 2020;40(11):3049–3058. doi:10.1007/s10792-020-01489-z
32. Pena-Verdeal H, Garcia-Queiruga J, García-Resúa C, Yebra-Pimentel E, Giráldez MJ. Osmolality and pH of commercially available contact lens care solutions and eye drops. Cont Lens Anterior Eye. 2021;44(4):101379. doi:10.1016/j.clae.2020.10.009
33. Dalton K, Subbaraman LN, Rogers R, Jones L. Physical properties of soft contact lens solutions. Optom Vis Sci. 2008;85(2):122–128. doi:10.1097/OPX.0b013e318162261e
34. Cavet ME, Harrington KL, Ward KW, Zhang JZ. Mapracorat, a novel selective glucocorticoid receptor agonist, inhibits hyperosmolar-induced cytokine release and MAPK pathways in human corneal epithelial cells. Mol Vis. 2010;16:1791–1800.
35. Higuchi A, Kawakita T, Tsubota K. IL-6 induction in desiccated corneal epithelium in vitro and in vivo. Mol Vis. 2011;17:2400–2406.
36. Baudouin C, Aragona P, Messmer EM, et al. Role of hyperosmolarity in the pathogenesis and management of dry eye disease: proceedings of the OCEAN group meeting. Ocul Surf. 2013;11(4):246–258. doi:10.1016/j.jtos.2013.07.003
37. Jones L, Downie LE, Korb D, et al. TFOS DEWS II management and therapy report. Ocul Surf. 2017;15(3):575–628. doi:10.1016/j.jtos.2017.05.006
38. Corrales RM, Luo L, Chang EY, Pflugfelder SC. Effects of osmoprotectants on hyperosmolar stress in cultured human corneal epithelial cells. Cornea. 2008;27(5):574–579. doi:10.1097/ICO.0b013e318165b19e
39. Deng R, Su Z, Hua X, Zhang Z, Li DQ, Pflugfelder SC. Osmoprotectants suppress the production and activity of matrix metalloproteinases induced by hyperosmolarity in primary human corneal epithelial cells. Mol Vis. 2014;20:1243–1252.
40. Hua X, Su Z, Deng R, Lin J, Li DQ, Pflugfelder SC. Effects of L-carnitine, erythritol and betaine on pro-inflammatory markers in primary human corneal epithelial cells exposed to hyperosmotic stress. Curr Eye Res. 2015;40(7):657–667. doi:10.3109/02713683.2014.957776
41. Turan E, Valtink M, Reinach PS, et al. L-carnitine suppresses transient receptor potential vanilloid type 1 activity and myofibroblast transdifferentiation in human corneal keratocytes. Lab Invest. 2021;101(6):680–689. doi:10.1038/s41374-021-00538-0
42. López-Cano JJ, González-Cela-Casamayor MA, Andrés-Guerrero V, Herrero-Vanrell R, Benítez-Del-Castillo JM, Molina-Martínez IT. Combined hyperosmolarity and inflammatory conditions in stressed human corneal epithelial cells and macrophages to evaluate osmoprotective agents as potential DED treatments. Exp Eye Res. 2021;211:108723. doi:10.1016/j.exer.2021.108723
43. Iturriaga G, Suárez R, Nova-Franco B. Trehalose metabolism: from osmoprotection to signaling. Int J Mol Sci. 2009;10:3793–3810. doi:10.3390/ijms10093793
44. Aragona P, Colosi P, Rania L, et al. Protective effects of trehalose on the corneal epithelial cells. ScientificWorldJournal. 2014;2014:717835. doi:10.1155/2014/717835
45. Matsuo T. Trehalose protects corneal epithelial cells from death by drying. Br J Ophthalmol. 2001;85(5):610–612. doi:10.1136/bjo.85.5.610
46. Hovakimyan M, Ramoth T, Löbler M, et al. Evaluation of protective effects of trehalose on desiccation of epithelial cells in three dimensional reconstructed human corneal epithelium. Curr Eye Res. 2012;37(11):982–989. doi:10.3109/02713683.2012.700754
47. Hill-Bator A, Misiuk-Hojło M, Marycz K, Grzesiak J. Trehalose-based eye drops preserve viability and functionality of cultured human corneal epithelial cells during desiccation. Biomed Res Int. 2014;2014:292139. doi:10.1155/2014/292139
48. Liu Z, Chen D, Chen X, et al. Trehalose induces autophagy against inflammation by activating TFEB signaling pathway in human corneal epithelial cells exposed to hyperosmotic stress. Invest Ophthalmol Vis Sci. 2020;61(10):26. doi:10.1167/iovs.61.10.26
49. Garrett Q, Khandekar N, Shih S, et al. Betaine stabilizes cell volume and protects against apoptosis in human corneal epithelial cells under hyperosmotic stress. Exp Eye Res. 2013;108:33–41. doi:10.1016/j.exer.2012.12.001
50. Aslan Bayhan S, Bayhan HA, Muhafız E, Bekdemir Ş, Gürdal C. Effects of osmoprotective eye drops on tear osmolarity in contact lens wearers. Can J Ophthalmol. 2015;50(4):283–289. doi:10.1016/j.jcjo.2015.03.008
51. Fernández-Jimenez E, Diz-Arias E, Peral A. Improving ocular surface comfort in contact lens wearers. Cont Lens Anterior Eye. 2022;45(3):101544. doi:10.1016/j.clae.2021.101544
52. Pflugfelder SC. Tear dysfunction and the cornea: LXVIII Edward Jackson memorial lecture. Am J Ophthalmol. 2011;152(6):900–909.e1. doi:10.1016/j.ajo.2011.08.023
53. ISO 18369-1:2017. Ophthalmic optics. Contact lenses. Part 1: Vocabulary, classification system and recommendations for labelling specifications. International Organization for Standardization. 2017.
54. Pence N. Thinking inside the blister. Cont Lens Spectrum. 2009;24(5):25.
55. DAILIES TOTAL1® and DAILIES TOTAL1® Multifocal (delefilcon A) soft contact lenses for Daily Disposable Wear [package insert]. Fort Worth, TX: Alcon Laboratories, Inc.; 2019.
56. Package Insert for Alcon Precision1™ (verofilcon A) Soft Contact Lenses [package insert]. Fort Worth, TX: Alcon Laboratories, Inc.; 2019.
57. BAUSCH + LOMB INFUSE® (kalifilcon A) One-Day Soft (Hydrophilic) Contact Lenses [package insert]. Rochester, NY: Bausch & Lomb Incorporated; 2020.
58. CLARITI 1 DAY CONTACT LENS [package insert]. Scottsville, NY: CooperVision; 2019.
59. U.S. Food and Drug Administration. FDA 510(k) Summary K191763. MyDay (stenfilcon A) Soft (Hydrophilic) Daily Disposable Contact Lens; 2019. Available from: https://www.accessdata.fda.gov/cdrh_docs/pdf19/K190965.pdf.
60. 1-DAY ACUVUE® TruEye® Brand Contact Lenses with HYDRACLEAR® 1 Technology (narafilcon A). Visibility Tinted with UV Blocker for Daily Wear Single Use Only [package insert]. Jacksonville, FL: Johnson & Johnson Vision Care, Inc.; 2013.
61. Johnson & Johnson Vision Care, Inc. (Jacksonville, FL). ACUVUE® oasys BRAND CONTACT LENS 1-Day with HydraLuxe™ [package insert]. Jacksonville, FL: Johnson & Johnson Vision Care, Inc.; 2016.
62. Cavet ME, Harrington KL, Vollmer TR, Ward KW, Zhang JZ. Anti-inflammatory and anti-oxidative effects of the green tea polyphenol epigallocatechin gallate in human corneal epithelial cells. Mol Vis. 2011;17:533–542.
63. Tsai TY, Chen TC, Wang IJ, et al. The effect of resveratrol on protecting corneal epithelial cells from cytotoxicity caused by moxifloxacin and benzalkonium chloride. Invest Ophthalmol Vis Sci. 2015;56(3):1575–1584. doi:10.1167/iovs.14-15708
64. Tomlinson A, Khanal S, Ramaesh K, Diaper C, McFadyen A. Tear film osmolarity: determination of a referent for dry eye diagnosis. Invest Ophthalmol Vis Sci. 2006;47(10):4309–4315. doi:10.1167/iovs.05-1504
65. Gjerdrum B, Gundersen KG, Lundmark PO, Aakre BM. Repeatability of OCT-based versus scheimpflug- and reflection-based keratometry in patients with hyperosmolar and normal tear film. Clin Ophthalmol. 2020;14:3991–4003. doi:10.2147/OPTH.S280868
66. Tashbayev B, Utheim TP, Utheim ØA, et al. Utility of tear osmolarity measurement in diagnosis of dry eye disease. Sci Rep. 2020;10(1):5542. doi:10.1038/s41598-020-62583-x
67. McMonnies CW. Conjunctival tear layer temperature, evaporation, hyperosmolarity, inflammation, hyperemia, tissue damage, and symptoms: a review of an amplifying cascade. Curr Eye Res. 2017;42(12):1574–1584. doi:10.1080/02713683.2017.1377261
68. Liu H, Begley C, Chen M, et al. A link between tear instability and hyperosmolarity in dry eye. Invest Ophthalmol Vis Sci. 2009;50(8):3671–3679. doi:10.1167/iovs.08-2689
69. Kumar P, Nagarajan A, Uchil PD. Analysis of cell viability by the alamarBlue assay. Cold Spring Harb Protoc. 2018;2018(6). doi:10.1101/pdb.prot095489
70. Fong PY, Shih KC, Lam PY, Chan TCY, Jhanji V, Tong L. Role of tear film biomarkers in the diagnosis and management of dry eye disease. Taiwan J Ophthalmol. 2019;9(3):150–159. doi:10.4103/tjo.tjo_56_19
71. Kishimoto T. The biology of Interleukin-6. Blood. 1989;74(1):1–10. doi:10.1182/blood.V74.1.1.1
72. Baggiolini M, Clark-Lewis I. Interleukin-8, a chemotactic and inflammatory cytokine. FEBS Lett. 1992;307(1):97–101. doi:10.1016/0014-5793(92)80909-Z
73. Stepp MA, Menko AS. Immune responses to injury and their links to eye disease. Transl Res. 2021;236:52–71. doi:10.1016/j.trsl.2021.05.005
74. Peng L, Zhong J, Xiao Y, et al. Therapeutic effects of an anti-IL-6 antibody in fungal keratitis: macrophage inhibition and T cell subset regulation. Int Immunopharmacol. 2020;85:106649. doi:10.1016/j.intimp.2020.106649
75. Sakimoto T, Sugaya S, Ishimori A, Sawa M. Anti-inflammatory effect of IL-6 receptor blockade in corneal alkali burn. Exp Eye Res. 2012;97(1):98–104. doi:10.1016/j.exer.2012.02.015
76. Armstrong RA, Davies LN, Dunne MC, Gilmartin B. Statistical guidelines for clinical studies of human vision. Ophthalmic Physiol Opt. 2011;31(2):123–136. doi:10.1111/j.1475-1313.2010.00815.x
77. Insua Pereira E, Sampaio AP, Lira M. Effects of contact lens wear on tear inflammatory biomarkers. Cont Lens Anterior Eye. 2022;45(5):101600. doi:10.1016/j.clae.2022.101600
78. Fernández I, López-Miguel A, Martín-Montañez V, et al. Inflammatory status predicts contact lens discomfort under adverse environmental conditions. Ocul Surf. 2020;18(4):829–840. doi:10.1016/j.jtos.2020.07.015
79. Dumbleton K, Woods CA, Jones LW, Fonn D. The impact of contemporary contact lenses on contact lens discontinuation. Eye Contact Lens. 2013;39(1):93–99. doi:10.1097/ICL.0b013e318271caf4
80. Martín-Montañez V, Enríquez-de-Salamanca A, López-de la Rosa A, et al. Effect of environmental conditions on the concentration of tear inflammatory mediators during contact lens wear. Cornea. 2016;35(9):1192–1198. doi:10.1097/ICO.0000000000000960
81. Efron N. Contact lens wear is intrinsically inflammatory. Clin Exp Optom. 2017;100(1):3–19. doi:10.1111/cxo.12487
82. Saliman NH, Morgan PB, MacDonald AS, Maldonado-Codina C. Subclinical inflammation of the ocular surface in soft contact lens wear. Cornea. 2020;39(2):146–154. doi:10.1097/ICO.0000000000002192
83. Efron N, Brennan NA, Bright FV, et al. 2. Contact lens care and ocular surface homeostasis. Cont Lens Anterior Eye. 2013;36(Suppl 1):S9–S13. doi:10.1016/S1367-0484(13)60004-1
84. Schafer J, Reindel W, Steffen R, Mosehauer G, Chinn J. Use of a novel extended blink test to evaluate the performance of two polyvinylpyrrolidone-containing, silicone hydrogel contact lenses. Clin Ophthalmol. 2018;12:819–825. doi:10.2147/OPTH.S162233
85. Schafer J, Steffen R, Mosehauer G, Reindel W, Wygladacz K, Seyboth S Evaluation of the stability of surface water characteristics of contact lenses using refractive index shifts after wear of daily disposable lenses.
86. Reindel W, Steffen R, Mosehauer G, et al. Performance of a silicone hydrogel daily disposable contact lens among wearers with lens-related dryness. Open J Ophthalmol. 2023;17:e187436412303021. doi:10.2174/18743641-v17-230316-2022-57
87. Menzies KL, Rogers R, Jones L. In vitro contact angle analysis and physical properties of blister pack solutions of daily disposable contact lenses. Eye Contact Lens. 2010;36(1):10–18. doi:10.1097/ICL.0b013e3181c5b385
88. Menzies KL, Jones L. In vitro analysis of the physical properties of contact lens blister pack solutions. Optom Vis Sci. 2011;88(4):493–501. doi:10.1097/OPX.0b013e3181ff9d39
89. Gorbet MB, Tanti NC, Jones L, Sheardown H. Corneal epithelial cell biocompatibility to silicone hydrogel and conventional hydrogel contact lens packaging solutions. Mol Vis. 2010;16:272–282.
90. Choy CK, Cho P, Boost MV. Cytotoxicity and effects on metabolism of contact lens care solutions on human corneal epithelium cells. Clin Exp Optom. 2012;95(2):198–206. doi:10.1111/j.1444-0938.2011.00687.x
91. Cavet ME, VanDerMeid KR, Harrington KL, Tchao R, Ward KW, Zhang JZ. Effect of a novel multipurpose contact lens solution on human corneal epithelial barrier function. Cont Lens Anterior Eye. 2010;33(Suppl 1):S18–S23. doi:10.1016/j.clae.2010.06.012
92. Montani G, Martino M. Tear film characteristics during wear of daily disposable contact lenses. Clin Ophthalmol. 2020;14:1521–1531. doi:10.2147/OPTH.S242422
93. Lorente-Velázquez A, García-Montero M, Gómez-Sanz FJ, Rico Del Viejo L, Hernández-Verdejo JL, Madrid-Costa D. Comparison of the impact of nesofilcon A hydrogel contact lens on the ocular surface and the comfort of presbyopic and non-presbyopic wearers. Int J Ophthalmol. 2019;12(4):640–646. doi:10.18240/ijo.2019.04.19
94. Pena-Verdeal H, Noya-Padin V, Losada-Oubiña M, Saborido-Rey M, Vilas-Alonso M, Giraldez MJ. Changes of symptomatology, tear film and ocular surface integrity one week during somofilcon-A and omafilcon-A lens wear. Eur J Ophthalmol. 2023;33(2):890–899. doi:10.1177/11206721221131131
95. Sapkota K, Franco S, Lira M. Daily versus monthly disposable contact lens: which is better for ocular surface physiology and comfort? Cont Lens Anterior Eye. 2018;41(3):252–257. doi:10.1016/j.clae.2017.12.005
96. Diec J, Papas E, Naduvilath T, Xu P, Holden BA, Lazon de la Jara P. Combined effect of comfort and adverse events on contact lens performance. Optom Vis Sci. 2013;90(7):674–681. doi:10.1097/OPX.0000000000000008
97. Stahl U, Willcox M, Stapleton F. Role of hypo-osmotic saline drops in ocular comfort during contact lens wear. Cont Lens Anterior Eye. 2010;33(2):68–75. doi:10.1016/j.clae.2010.01.001
98. Tonge S, Jones L, Goodall S, Tighe B. The ex vivo wettability of soft contact lenses. Curr Eye Res. 2001;23(1):51–59. doi:10.1076/ceyr.23.1.51.5418
99. Lee HJ, McAuley A, Schilke KF, McGuire J. Molecular origins of surfactant-mediated stabilization of protein drugs. Adv Drug Deliv Rev. 2011;63(13):1160–1171. doi:10.1016/j.addr.2011.06.015
100. Chin J, Mustafi D, Poellmann MJ, Lee RC. Amphiphilic copolymers reduce aggregation of unfolded lysozyme more effectively than polyethylene glycol. Phys Biol. 2017;14(1):016003. doi:10.1088/1478-3975/aa5788
101. Singh S, Singh J. Effect of polyols on the conformational stability and biological activity of a model protein lysozyme. AAPS PharmSciTech. 2003;4(3):E42. doi:10.1208/pt040342
102. Kathuria A, Shamloo K, Jhanji V, Sharma A. Categorization of marketed artificial tear formulations based on their ingredients: a rational approach for their use. J Clin Med. 2021;10(6):1289. doi:10.3390/jcm10061289
103. Bachman WG, Wilson G. Essential ions for maintenance of the corneal epithelial surface. Invest Ophthalmol Vis Sci. 1985;26(11):1484–1488.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.