Back to Journals » Infection and Drug Resistance » Volume 19
Comparative Analysis of Pathogen-Specific IgM Antibody and Nucleic Acid Detection in Patients with Respiratory Tract Infectionsin Northern Anhui, China: An Epidemiological Study
Authors Wei X, Liu Z, Xu L, Wu N, Wang Z
Received 24 August 2025
Accepted for publication 11 January 2026
Published 6 February 2026 Volume 2026:19 562867
DOI https://doi.org/10.2147/IDR.S562867
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Oliver Planz
Xueting Wei,1,2 Zheng Liu,3 Liang Xu,4 Nan Wu,4 Zhongxin Wang1
1Department of Clinical Laboratory Science, The First Affiliated Hospital of Anhui Medical University, Hefei, Anhui, 230022, People’s Republic of China; 2Department of Pulmonary and Critical Care Medicine, The First Affiliated Hospital of Bengbu Medical University, Anhui Province Key Laboratory of Clinical and Preclinical Research in Respiratory Disease, Bengbu, Anhui, 233004, People’s Republic of China; 3Department of Emergency Surgery, The Third People’s Hospital of Bengbu, Bengbu, Anhui, 233000, People’s Republic of China; 4Molecular Diagnostics Center, The First Affiliated Hospital of Bengbu Medical University, Bengbu, Anhui, 233004, People’s Republic of China
Correspondence: Zhongxin Wang, Department of Clinical Laboratory Science, The First Affiliated Hospital of Anhui Medical University, No. 120, Wanshui Road, Shushan District, Hefei, Anhui, 230022, People’s Republic of China, Email [email protected]
Background: Respiratory tract infections are among the most common causes of acute illnesses, with viruses accounting for the majority of cases, particularly in outpatient settings. Regression-based study designs have been commonly employed to estimate the burden of influenza; however, these estimates frequently suffer from a lack of timeliness, and numerous countries face limitations due to insufficient virological data. Specifically for the northern region of Anhui Province, the local profile and infection patterns of respiratory pathogens remain not well-documented. This study seeks to contribute to bridging these knowledge gaps.
Methods: A total of 15,774 patients with acute respiratory tract infections treated at the First Affiliated Hospital of Bengbu Medical University from January 1, 2020, to December 31, 2022 were included. Associations between pathogen detection and demographic variables were analyzed. IgM antibodies against multiple respiratory pathogens were detected using serological methods. Paired serum and throat swab samples from 374 non-COVID-19 patients were tested using both IgM antibody assays and multiplex nucleic acid amplification to compare diagnostic efficacy.
Results: The overall IgM antibody positivity rate was 24.45%, with annual rates of 17.58% in 2020, 28.66% in 2021, and 25.83% in 2022. The highest detection rate was for Mycoplasma pneumoniae (MP; 15.22%), followed by Influenza B virus (IFBV; 3.75%) and Legionella (LP; 2.15%). Seasonal detection rates were 21.62% in spring, 26.31% in summer, 29.83% in autumn, and 20.40% in winter. Females had a higher detection rate (26.06%) than males (23.05%). Detection rates by age group were 33.83% in children, 13.81% in adolescents, 3.39% in young adults, 14.61% in middle-aged individuals, and 19.39% in the elderly. Nucleic acid testing demonstrated a higher positivity rate compared with IgM antibody testing.
Conclusion: The detection rate of pathogen-specific IgM antibodies in respiratory tract infections varies by year, season, sex, and age. Nucleic acid testing provides superior diagnostic sensitivity compared with IgM antibody detection and should be prioritized in clinical practice.
Keywords: respiratory tract infections, immunoglobulin M antibody, nucleic acid tests, Mycoplasma pneumoniae, influenza virus
Introduction
Respiratory tract infections represent the most prevalent cause of acute illness in developed nations, with an estimated annual incidence of 500 million non-influenza viral respiratory infections in the United States.1,2 In China, acute respiratory tract infections are the leading cause of mortality among children under five years of age, imposing a significant burden on both families and the healthcare system.3 These infections are characterized by a range of clinical manifestations, including fever, sore throat, cough, expectoration, and wheezing, and can be attributed to various pathogens. Notably, over 80% of these infections are viral in origin, with atypical pathogens such as severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), Mycoplasma pneumoniae (MP), and Chlamydia pneumoniae also posing substantial risks to public health.4
The early identification of the causative agents is crucial for the effective treatment and prevention of acute respiratory tract infections. Current diagnostic methods include immunological assays, pathogen isolation and culture, and nucleic acid detection techniques.5 Accurate and timely pathogen identification enables targeted clinical interventions, thereby improving patient outcomes. Nucleic acid detection methods are particularly advantageous due to their high sensitivity and specificity, enabling detailed pathogen identification and the early diagnosis of latent infections.6 Clinicians must select the appropriate diagnostic approach based on the individual patient’s condition. Despite the availability of these techniques, there remains a notable gap in the detailed epidemiological data, including a head-to-head comparison of IgM serology and nucleic acid testing, specifically for the Northern Anhui region. Filling this gap is essential for optimizing local diagnostic protocols and clinical management.Therefore, this study aimed to compare the diagnostic results for common respiratory pathogens obtained from serum IgM antibody testing and nucleic acid testing.
Materials and Methods
Ethical and Safety Issues
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of The First Affiliated Hospital of Bengbu Medical University (Approval No. 2022208). Written informed consent was obtained from all participants or their legal guardians. All data were anonymized to ensure confidentiality. Laboratory procedures followed BSL-2 safety protocols. The publication of this manuscript was approved by the Institutional Ethics Committee of Bengbu Medical College (Approval No. [2023] 389).
Study Design and Participant Inclusion
This was a cross-sectional study. Patients diagnosed with respiratory tract infections at the First Affiliated Hospital of Bengbu Medical University between January 1, 2020, and December 31, 2022, were considered for inclusion. The primary inclusion criterion was the availability of a serum sample for immunoglobulin M (IgM) antibody testing. For the comparative diagnostic analysis, an additional criterion was the availability of a paired throat swab sample for nucleic acid testing. Patients with confirmed COVID-19 were excluded from the comparative analysis subgroup.
Patients and Sample Collection
Between January 1, 2020, and December 31, 022, a total of 15,774 patients diagnosed with respiratory tract infections were admitted to the First Affiliated Hospital of Bengbu Medical University, the largest comprehensive hospital in northern Anhui Province, with over 3,800 beds and an annual patient volume exceeding 2.2 million visits. Among the patients included in this study, 8,430 were male and 7,344 were female. Participants were stratified into five age groups: children (3–14 years), adolescents (15–18 years), young adults (19–40 years), middle-aged adults (41–65 years), and elderly adults (66–85 years).
Additionally, 374 adult patients with acute respiratory infections (excluding COVID-19) who were treated in the Department of Respiratory Medicine at the First Affiliated Hospital of Bengbu Medical University between January 2022 and May 2022 were enrolled for comparative diagnostic analysis. These patients underwent both serum IgM antibody testing and nucleic acid testing for respiratory pathogens.
To detect IgM antibody, serum or plasma anticoagulated with EDTA, heparin, or citrate was collected and promptly transported to the Immunology Division of the Key Laboratory of the Respiratory Department. Samples were stored at 4°C until analysis. For the detection of respiratory viruses, nasopharyngeal and oropharyngeal swabs were obtained from each patient, combined, and placed in viral transport medium. These samples were immediately transported to the Molecular Diagnostics Division of the same laboratory and stored at −80°C until testing.
Detection of IgM Antibodies Against Respiratory Pathogens
IgM antibodies were detected using a respiratory pathogen detection kit (Oon Medical Experimental Diagnosis Company, Germany) based on an indirect Immunofluorescence (IF) assay. Briefly, diluted patient serum was incubated with antigen-coated slides. If specific IgM antibodies were present, they bound to their corresponding antigens. After washing, fluorescein isothiocyanate (FITC)-labeled anti-human IgM antibodies were added, and specific fluorescence patterns were observed under a fluorescence microscope.
Prior to testing, immunoglobulin G (IgG) antibodies were removed from patient samples using immunoabsorption to prevent false-positive results caused by rheumatoid factors (RF) or false-negative results due to competitive binding with specific IgG. RF adsorbents were also used to remove RF from the samples. For qualitative testing, the initial dilution of the sample was 1:10 (and 1:100 for Legionella pneumophila). When using IgG absorbents, 16.6 µL of the sample was mixed with 150 µL of the adsorbent, vortexed for 4 seconds, incubated at room temperature for 15 minutes, and centrifuged for 5 minutes at 2000 rpm at room temperature. For dilution of 1:100, the supernatant was further diluted 1:10 with phosphate buffer saline (PBS).
The IF protocol was as follows: 30 µL of diluted serum was added to each designated reaction area of the sample plate. Antigen-coated slides were placed face-down in the grooves and incubated at 18–25 °C for 30 minutes. After washing with PBS, 25 μL of FITC-labeled anti-human IgM antibody was added, followed by a second incubation for 30 minutes protected from light. Slides were washed again, mounted with glycerol/PBS, and examined under a fluorescence microscope. Representative images are shown in Figures 1 and 2 presents a positive Mycoplasma pneumoniae IgM fluorescence pattern.
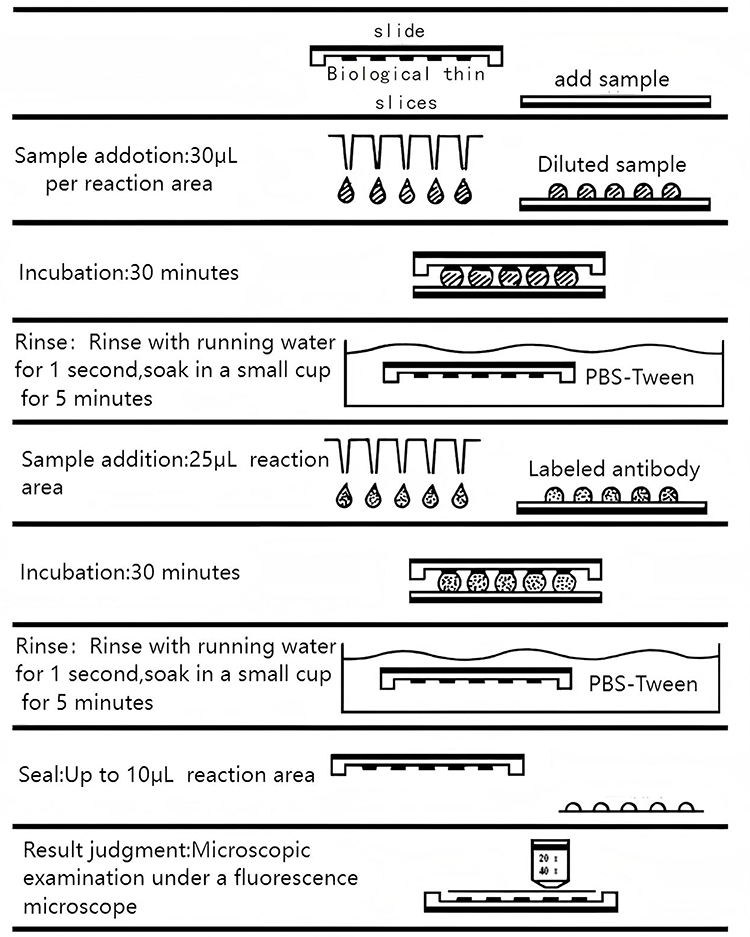 |
Figure 1 Experimental operation of titration plate technology.The overarching process of indirect IF assay operations. |
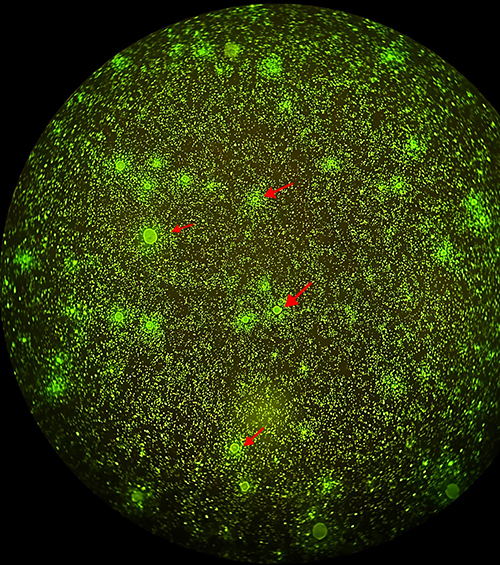 |
Figure 2 Under the 20 × fluorescence microscope, scattered inclusions are observable within the cell envelope of the infected MP. These inclusions exhibit fine to coarse granular fluorescence, resembling large stars surrounded by numerous smaller stars in a night sky. The inclusions are indicated by the red arrow in the accompanying image. |
Detection of Nucleic Acids of Respiratory Pathogens
The nucleic acid testing for respiratory pathogens was performed utilizing the SureX 13 Respiratory Pathogen Multiplex Detection Kit (Ningbo Heath Gene Technologies, China) and the SLAN-96S real-time PCR instrument (Shanghai Hongshi Medical Technology Co., Ltd., China). This assay utilizes multiplex fluorescent probe reverse transcription polymerase chain reaction (RT-PCR) with four detection channels (FAM, VIC, ROX, CY5) and melt curve analysis to simultaneously detect 13 respiratory pathogens. The FAM, VIC, and ROX channels designated for the amplification detection of target pathogens. Identification of these pathogens is based on the cycle threshold (Ct) values of the amplification signals recorded in each channel, as well as the rate of change in peak height within the specific melting temperature range associated with the target pathogens. The CY5 channel monitors endogenous internal control to ensure sample quality.
For amplification, the 20 μL reaction mixture contained 1 μL reverse transcriptase mix (reverse transcriptase and RNase inhibitor), 4 μL enzyme mix (hot-start DNA polymerase, dNTPs, MgCl2), 3 μL primer/probe working solution, 7 μL DEPC-treated water, and 5 μL extracted nucleic acid. Reverse transcription was performed at 55 °C for 10 min. After adding samples, tubes were sealed, briefly centrifuged, placed on ice, and loaded into the PCR instrument. Fluorescence channels FAM, VIC, ROX, and CY5 were selected for amplification and detection.
Statistical Analysis
Statistical analysis was conducted using SPSS version 25.0 (IBM Corp., Armonk, NY, USA). Categorical variables were expressed as frequencies and percentages, and group comparisons were performed using the chi-square (χ2) test. Statistical significance was set at p-value of less than 0.05. The agreement between serum IgM antibody detection and nucleic acid testing was evaluated using the Kappa consistency test.
Results
Prevalence of Respiratory Viruses in Patient Groups
Among the 15,774 specimens analyzed, respiratory pathogen–specific IgM antibodies were detected in 3,857 cases, yielding an overall positivity rate of 24.45%. Annual detection rates were 17.58% in 2020, 28.66% in 2021, and 25.83% in 2022, with significant interannual variation (χ2 = 167.699, P < 0.001). The highest detection rate of respiratory pathogen IgM antibodies was recorded for MP at 2,401 cases (15.22%), followed by IFVB at 591 cases (3.75%), and then by LP at 339 cases (2.15%). Detection rates for adenovirus (ADV) did not differ significantly across the three years (χ2 = 1.455, P = 0.483), whereas detection rates for other pathogens showed significant year-to-year variation (P < 0.05; Table 1).
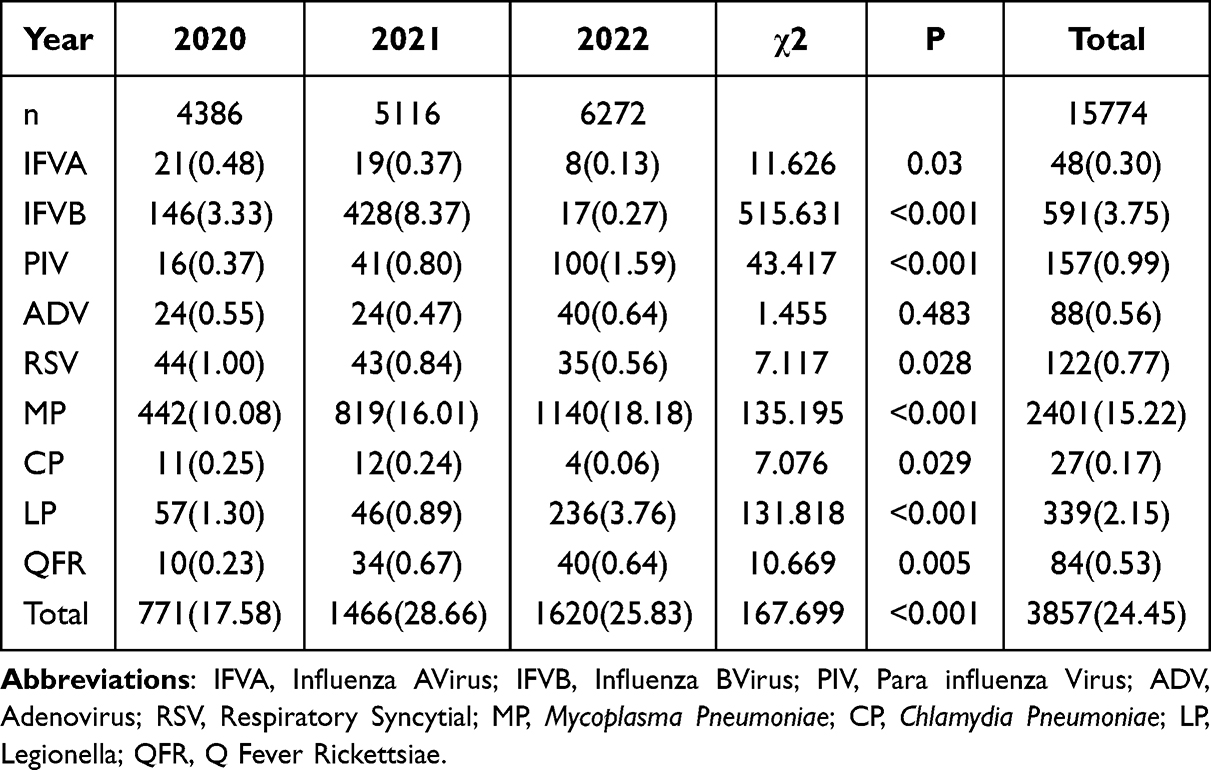 |
Table 1 A Comparative Analysis of IgM Antibody Detection for Respiratory Pathogens in Specimens Collected from 2020 to 2022 [n (%)] |
Respiratory Viruses According to the Season of Infection
A comparative analysis of IgM antibody detection rates for respiratory pathogens among patients across different seasons revealed statistically significant differences (χ2 = 123.351, P < 0.001). The detection rate was highest in autumn (29.86%) and lowest in winter (20.49%). Additionally, the peak infection periods for various pathogens differed. Infections caused by IFVB and Respiratory Syncytial Virus (RSV) peaked in winter, whereas MP and LP infections peaked in autumn. Furthermore, the comparison of IgM antibody detection rates for IFVB, Parainfluenza virus (PIV), RSV, MP, Chlamydia pneumoniae (CP), LP, and Q fever rickettsiae (QFR) across different seasons demonstrated statistically significant differences (all P < 0.05; Figure 3).
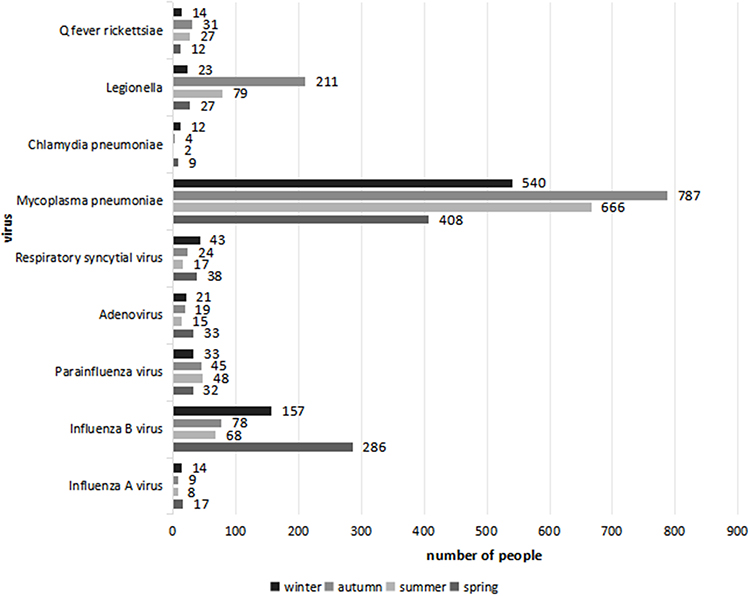 |
Figure 3 A Comparative Analysis of IgM Antibody Detection for Respiratory Pathogens in Specimens Collected Across Different Seasons. |
Respiratory Viruses According to Age of Infection
IgM detection rates varied significantly across age groups, with the highest positivity observed in children (33.83%) and the lowest in young adults (3.39%). MP positivity was greatest among children (1,758 cases), lower in adolescents and young adults, and increased again in middle-aged and elderly individuals. This pattern suggests higher susceptibility to MP infection in populations with less mature or compromised immune systems, such as children and older adults. Statistically significant age-related differences were found for IFVB, PIV, RSV, MP, LP, and QFR (P < 0.05; Table 2).
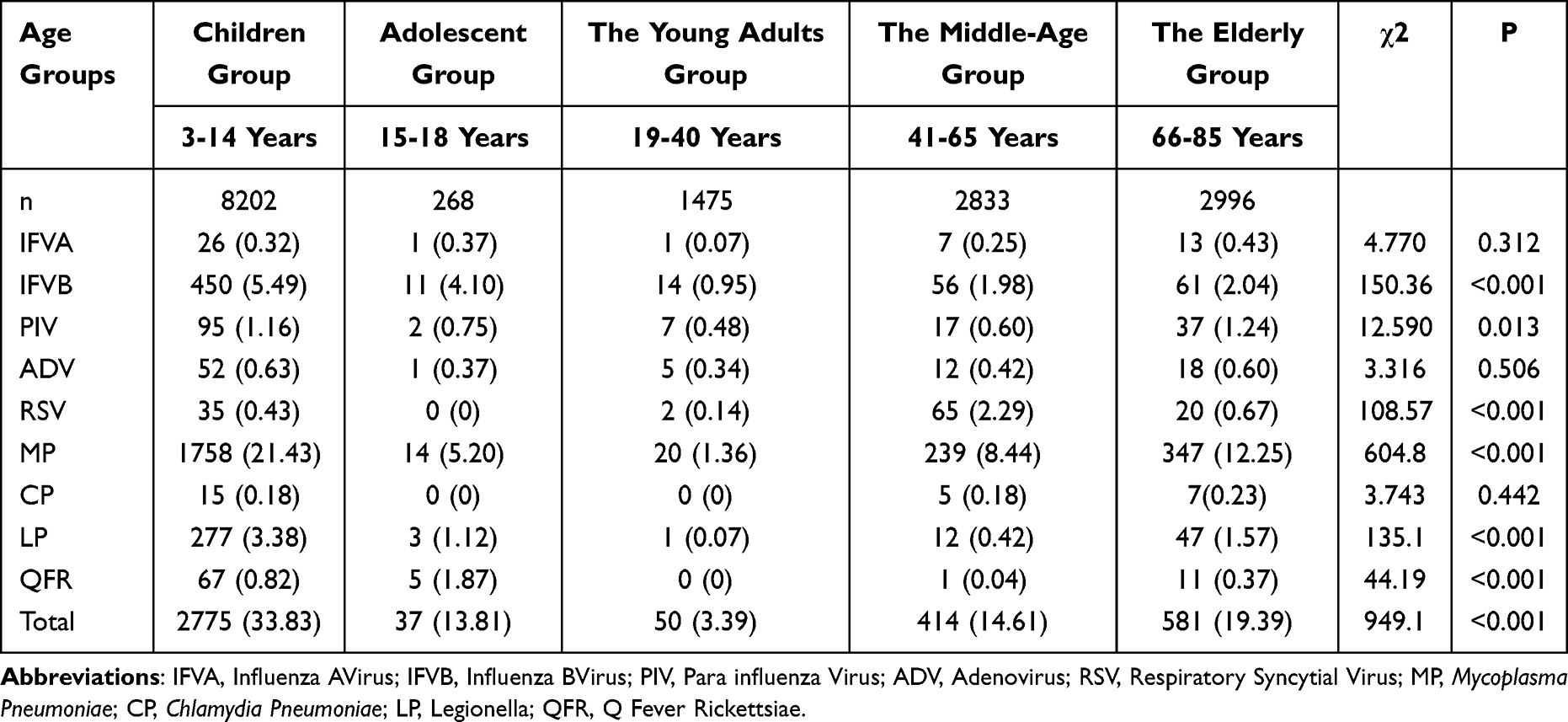 |
Table 2 A Comparative Analysis of IgM Antibody Detection for Respiratory Pathogens in Specimens Collected from Patients Across Various Age Groups [n (%)] |
Respiratory Viruses Based on the Gender of the Infected Individuals
Among 8,430 male patients, the IgM antibody positivity rate was 23.05%, compared with 26.06% among 7,344 female patients (χ2 = 19.341, P < 0.001). Furthermore, comparisons of the detection rates of IgM antibodies to IFVB,MP, and QFR between genders revealed statistically significant differences (χ2 = 6.296, 17.522, 5.938, all P < 0.05). However, the detection rates of IgM antibodies for other pathogens did not show statistically significant differences when compared across genders (P>0.05; Table 3).
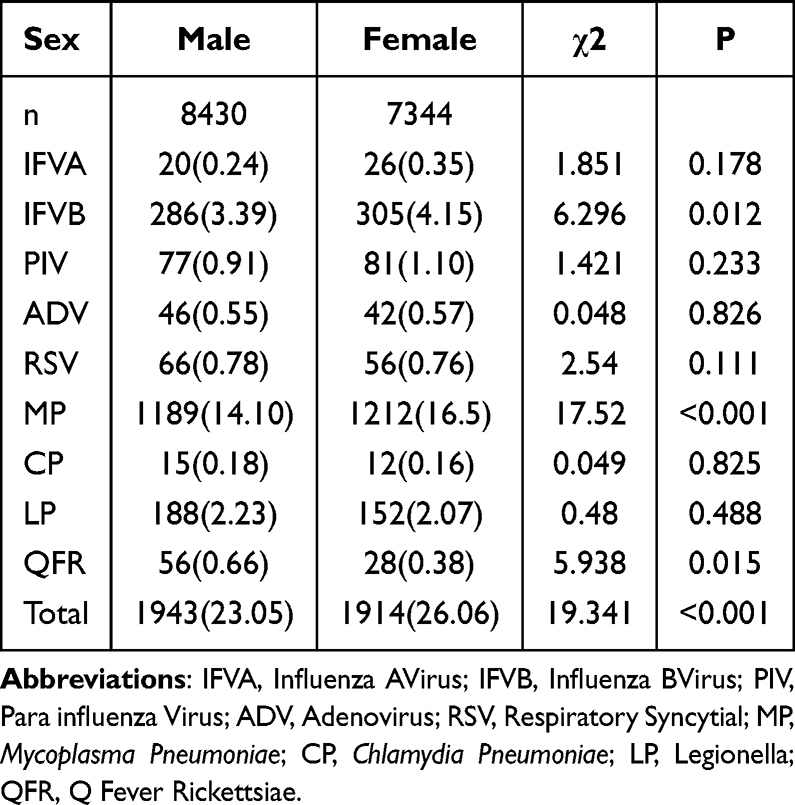 |
Table 3 A Comparative Analysis of IgM Antibody Detection for Respiratory Pathogens in Specimens Collected from Patients of Varying Genders[n (%)] |
Comparison of Serum IgM Antibody Test Results and Nucleic Acid Test Outcomes
Among the 374 comparison samples analyzed, 110 (29.40%) were positive by serum IgM testing, whereas 126 (33.69%) were positive by nucleic acid testing. The positive rate for nucleic acid testing was significantly higher than that for serum IgM antibody testing, with a statistically significant difference observed (P = 0.007). Agreement between the two methods was substantial (Kappa = 0.809, P < 0.001). Serum IgM antibody and nucleic acid detection were employed to assess seven common respiratory pathogens. For seven common respiratory pathogens, agreement was high (Kappa > 0.75, P < 0.001) for influenza A virus (IFVA), IFVB, PIV, RSV, and MP. ADV showed moderate agreement (Kappa = 0.492, P < 0.001) (Figure 4).
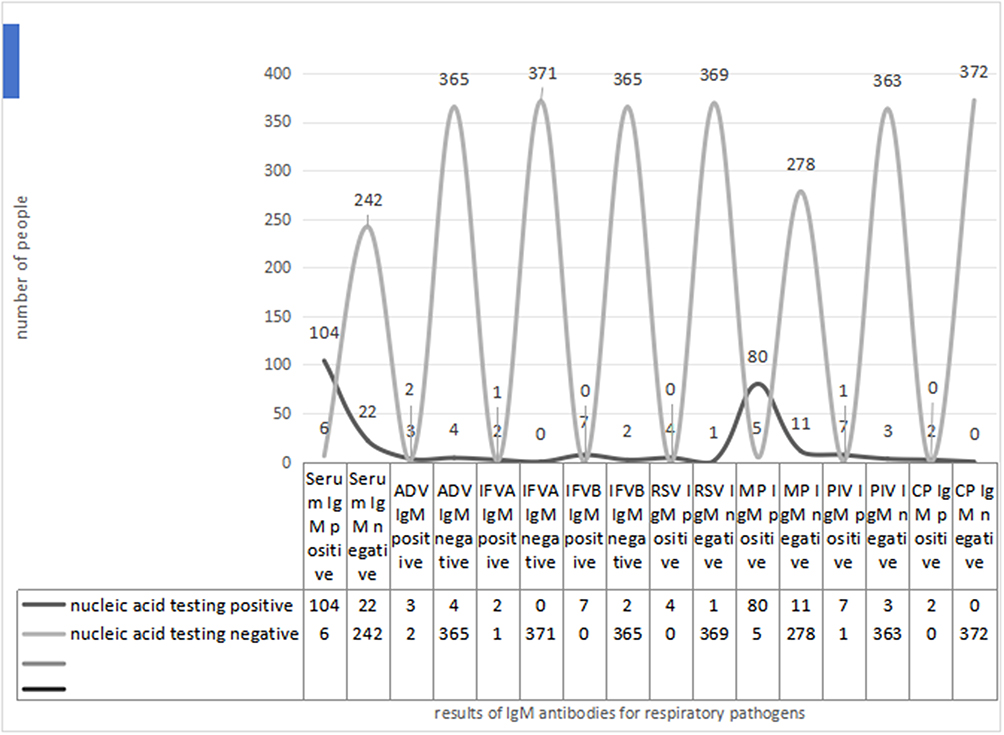 |
Figure 4 Comparison of Serum IgM Antibody Test Results and Nucleic Acid Testing Outcomes. |
Discussion
Acute airway infections represent a prevalent health concern among humans. In recent years, the predominant etiology of acute respiratory tract infections has shifted from bacterial to viral and atypical respiratory pathogen infections, largely due to the widespread use of antimicrobial agents.7 Clinical management varies depending on the causative agent; therefore, accurate pathogen identification is critical for guiding practice, ensuring the rational use of antibiotics, and mitigating antimicrobial resistance.8
In this study, we assessed the prevalence of common respiratory viruses in hospitalized and outpatient cases with acute respiratory infection symptoms and analyzed virus distribution over a two-year period. Our results are consistent with previously published studies that investigated the etiology of acute respiratory infection, especially those focused on people with lower respiratory tract infections.9,10 Since the emergence of the COVID-19 pandemic, which is attributed to the SARS-CoV-2, a series of non-pharmaceutical interventions were rapidly implemented to mitigate the virus’s transmission.11 In addition to efforts aimed at controlling the spread of COVID-19, the epidemiology of atypical pathogens, including MP, has experienced notable changes as a result of these interventions. Our results show a decline in acute respiratory infection cases in 2020 compared to 2021, with the MP detection rate falling from 16.01% to 10.08%. These findings align with previous research outcomes.12 Furthermore, the number of positive cases of MP in other regions of China significantly decreased in 2020 due to the public health response to COVID-19.13 As pandemic restrictions eased in 2022, increased gatherings and reduced adherence to preventive measures led to a resurgence of viral infections, particularly MP, PIV, and LP.
This rate is largely consistent with those reported in existing literature both domestically and internationally.14 Notably, the detection rate of IgM antibodies for MP was 15.22%, followed by IFVB and LP, while the detection rate for mixed infections was relatively low. Consequently, MP emerges as the predominant pathogen responsible for acute respiratory tract infections in adults within this region. These findings corroborate previous conclusions that MP infection is the typical respiratory pathogen with the highest daily detection rate reported in domestic pneumonia cases.15
Among MP-positive cases, children had significantly higher rates than adults,16 likely due to differences in immunity and hygiene practices. Children aged 3–14 years were most affected from 2020 to 2022, with MP rates higher in younger children than adolescents, consistent with earlier studies.17–19 Recent studies indicate that the infection rate of LP in pediatric populations increases with age.20 While culture remains the gold standard for the diagnosis of Legionella, serological antibody testing is the most frequently employed laboratory method for diagnosing Legionella pneumonia.21 Our study found higher LP IgM positivity in children aged 3–14 years, particularly in preschoolers. LP can also cause extrapulmonary symptoms, and co-infection with MP may result in more severe illness,22 highlighting the need for early diagnosis and treatment.23
Seasonal variations in the infection rates of different pathogens were also observed. The study demonstrated that infection rates during the summer and autumn months were significantly higher than those in spring and winter. However, distinct patterns emerged among different pathogen categories; for instance, the peak incidence of IFVB infections occurred in winter and spring, while MP infections were most prevalent in summer and autumn.24,25 The methodologies employed for the detection of respiratory pathogens include microbial culture, serological testing, and molecular biology techniques.26 While microbial culture is a traditional method, it is often time-consuming and exhibits a low detection rate. Serological testing is frequently favored for its speed and convenience; however, it has the potential for false positive and false negative results.27 In the present study, we employed indirect immunofluorescence to identify IgM antibodies in serum samples, while atypical pathogen RNA was detected in nasopharyngeal specimens using PCR. Conversely, several other studies have utilized passive agglutination methods to identify MP antibodies.13,28 Molecular approach offers rapid and precise identification of pathogens, thereby enhancing diagnostic accuracy.29 Molecular diagnostics allow rapid and precise identification, though limitations remain, including low sensitivity and predictive value.30–32 Consequently, both serological testing and PCR methods possess distinct advantages and disadvantages. An accurate diagnosis necessitates the integration of laboratory test results with clinical manifestations.33 Understanding regional epidemiology and promptly selecting appropriate diagnostic methods enables individualized treatment, prudent antibiotic use, and better public health interventions.
Nevertheless, our study faced several limitations. Firstly, this research is a single-center study, despite the fact that this hospital is the largest in Northern Anhui Province, China. The prevalence of atypical pathogens may vary in other provinces of China due to differences in climate, economic conditions, and lifestyles.34 Diagnostic results must be interpreted with clinical context and should not be the sole criterion for diagnosis. Influenza vaccination can cause IgM positivity, requiring vaccination history consideration.35,36 In nucleic acid testing, sequence variation, poor sample handling, or suboptimal laboratory conditions can cause false negatives or positives.37
Conclusion
This study clarifies the local epidemiology of respiratory infections and provides a critical evaluation of diagnostic methods. We identified Mycoplasma pneumoniae and Influenza B virus as the predominant pathogens, a finding consistent with broader national trends yet now specifically documented for Northern Anhui. Infections exhibited a distinct seasonal pattern, with a notably higher burden observed in school-aged children (3–14 years) – a group defined according to common clinical and public health reporting categories, as discussed in the study limitations. A key finding is the confirmed superior sensitivity of nucleic acid testing over IgM serology for early detection. This methodological comparison, supported by a high overall agreement (Kappa > 0.8) yet clear disparity in positivity rates, directly informs clinical laboratory strategy. It underscores that while both methods are reliable for surveillance, molecular diagnostics should be prioritized when clinical demands require maximal sensitivity. The observed epidemiological and diagnostic insights collectively argue for integrating sensitive molecular methods into season- and risk-aware diagnostic pathways. Future work should aim to translate these findings into cost-effective testing algorithms and employ finer age stratifications to further delineate within-group risk, as noted in our limitations.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Statement
The study protocol was approved by the Ethics Committee of The First Affiliated Hospital of Bengbu Medical University (Approval No. 2022208). The publication of this manuscript was additionally approved by the Institutional Ethics Committee of Bengbu Medical College (Approval No. [2023] 389). Written informed consent was obtained from all participants or their legal guardians.
Acknowledgments
The authors thank Dr. Zheng Liu from The Third The People’s Hospital of Bengbu for his valuable contribution to data collection.
Author Contributions
Xueting Wei and Zheng Liu are regarded as co-first authors. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Key Project of Natural Science Research in Anhui Universities (grant number KJ2015A337).
Disclosure
The authors declare no conflict of interest.
References
1. Kirkpatrick GL. The common cold. Prim Care. 1996;23:657–11. doi:10.1016/s0095-4543(05)70355-9
2. Fendrick AM, Monto AS, Nightengale B, Sarnes M. The economic burden of non-influenza-related viral respiratory tract infection in the United States. Arch Intern Med. 2003;163:487–494. doi:10.1001/archinte.163.4.487
3. Williams BG, Gouws E, Boschi-Pinto C, Bryce J, Dye C. Estimates of world-wide distribution of child deaths from acute respiratory infections. Lancet Infect Dis. 2002;2:25–32. doi:10.1016/s1473-3099(01)00170-0
4. Kuang L, Liang Z, Wang C, et al. Serum 25-Hydroxy vitamin D levels in children with acute respiratory infections caused by respiratory virus or atypical pathogen infection. Nutrients. 2023;15. doi:10.3390/nu15061486
5. Chen Z, Ji W, Wang Y, et al. Epidemiology and associations with climatic conditions of Mycoplasma pneumoniae and Chlamydophila pneumoniae infections among Chinese children hospitalized with acute respiratory infections. Ital J Pediatr. 2013;39:34. doi:10.1186/1824-7288-39-34
6. Huang XN, Jia N, Xiao F, et al. Application of dual amplification method for nucleic acids of respiratory pathogens in the diagnosis of pathogens in pediatric upper respiratory infections. Chin J Experi Clin Virol. 2020;34:57–60. doi:10.3760/cma.j.issn.1003-9279.2020.01.012
7. Li Y, Wang X, Blau DM, et al. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in children younger than 5 years in 2019: a systematic analysis. Lancet. 2022;399:2047–2064. doi:10.1016/S0140-6736(22)00478-0
8. Hawke K, van Driel ML, Buffington BJ, McGuire TM, King D. Homeopathic medicinal products for preventing and treating acute respiratory tract infections in children. Cochrane Database Syst Rev. 2018;9:CD005974. doi:10.1002/14651858.CD005974.pub5
9. Chen WJ, Arnold JC, Fairchok MP, et al. Epidemiologic, clinical, and virologic characteristics of human rhinovirus infection among otherwise healthy children and adults: rhinovirus among adults and children. J Clin Virol. 2015;64:74–82. doi:10.1016/j.jcv.2015.01.007
10. Ning G, Wang X, Wu D, et al. The etiology of community-acquired pneumonia among children under 5 years of age in mainland China, 2001-2015: a systematic review. Hum Vaccin Immunother. 2017;13:2742–2750. doi:10.1080/21645515.2017.1371381
11. Zhang Y, Quigley A, Wang Q, MacIntyre CR. Non-pharmaceutical interventions during the roll out of covid-19 vaccines. BMJ. 2021;375:n2314. doi:10.1136/bmj.n2314
12. Li ZJ, Zhang HY, Ren LL, et al. Etiological and epidemiological features of acute respiratory infections in China. Nat Commun. 2021;12:5026. doi:10.1038/s41467-021-25120-6
13. Gao LW, Yin J, Hu YH, et al. The epidemiology of paediatric Mycoplasma pneumoniae pneumonia in North China: 2006 to 2016. Epidemiol Infect. 2019;147:e192. doi:10.1017/S0950268819000839
14. Kehl SC, Kumar S. Utilization of nucleic acid amplification assays for the detection of respiratory viruses. Clin Lab Med. 2009;29:661–671. doi:10.1016/j.cll.2009.07.008
15. Zhang Y, Huang Y, Ai T, Luo J, Liu H. Effect of COVID-19 on childhood Mycoplasma pneumoniae infection in Chengdu, China. BMC Pediatr. 2021;21:202. doi:10.1186/s12887-021-02679-z
16. Chen J, Li X, Wang W, et al. The prevalence of respiratory pathogens in adults with community-acquired pneumonia in an outpatient cohort. Infect Drug Resist. 2019;12:2335–2341. doi:10.2147/IDR.S213296
17. Jain S, Williams DJ, Arnold SR, et al. Community-acquired pneumonia requiring hospitalization among U.S. children. N Engl J Med. 2015;372:835–845. doi:10.1056/NEJMoa1405870
18. Sondergaard MJ, Friis MB, Hansen DS, Jorgensen IM. Clinical manifestations in infants and children with Mycoplasma pneumoniae infection. PLoS One. 2018;13:e0195288. doi:10.1371/journal.pone.0195288
19. Liu J, Wang M, Zhao Z, et al. Viral and bacterial coinfection among hospitalized children with respiratory tract infections. Am J Infect Control. 2020;48:1231–1236. doi:10.1016/j.ajic.2020.01.013
20. von Baum H, Luck C. Community-acquired legionella pneumonia: data from the CAPNETZ study. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2011;54:688–692. doi:10.1007/s00103-011-1287-0
21. Eidy H, Senger B, Steele J, Kathawa J. An atypical presentation of legionnaires’ disease. Cureus. 2024;16:e60856. doi:10.7759/cureus.60856
22. Heine S, Fuchs A, Von Muller L, et al. Legionellosis must be kept in mind in case of pneumonia with lung abscesses in children receiving therapeutic steroids. Infection. 2011;39:481–484. doi:10.1007/s15010-011-0131-7
23. Beersma MF, Dirven K, van Dam AP, et al. Evaluation of 12 commercial tests and the complement fixation test for Mycoplasma pneumoniae-specific immunoglobulin G (IgG) and IgM antibodies, with PCR used as the “gold standard”. J Clin Microbiol. 2005;43:2277–2285. doi:10.1128/JCM.43.5.2277-2285.2005
24. Ma JE, Ma QF, Wang W, et al. Analysis of common respiratory infected pathogens in 3100 children after the coronavirus disease 2019 pandemic. Curr Med Sci. 2022;42:1094–1098. doi:10.1007/s11596-022-2635-z
25. Liang W, Guang SH, Zhou Q, et al. Epidemiological analysis of community-acquired M. pneumoniae infection in children. Int J Lab Med. 2018;39:2708–2711. doi:10.3969/j.issn.1673-4130.2018.21.030
26. Chen SY, Yu FY. Detection technology and development trends of respiratory tract infection pathogens. New Clin Med China. 2022;15:894–899. doi:10.3969/j.issn.1674-3806.2022.10.02
27. Pancer KW. Problem of immunoglobulin M co-detection in serological response to bacterial and viral respiratory pathogens among children suspected of legionellosis. Cent Eur J Immunol. 2015;40:174–179. doi:10.5114/ceji.2015.52831
28. Gao CH, Ji BJ, Han C, Wang MS. Comparison of enzyme-linked immunosorbent assay with indirect immunofluorescence assay for the diagnosis of Mycoplasma pneumoniae infection. J Clin Lab Anal. 2019;33:e22677. doi:10.1002/jcla.22677
29. Nilsson AC, Bjorkman P, Persson K. Polymerase chain reaction is superior to serology for the diagnosis of acute Mycoplasma pneumoniae infection and reveals a high rate of persistent infection. BMC Microbiol. 2008;8:93. doi:10.1186/1471-2180-8-93
30. Kurkela S, Puolakkainen M, Hokynar K, et al. Mycoplasma pneumoniae outbreak, Southeastern Finland, 2017-2018: molecular epidemiology and laboratory diagnostic lessons. Eur J Clin Microbiol Infect Dis. 2019;38:1867–1871. doi:10.1007/s10096-019-03619-7
31. Chang HY, Chang LY, Shao PL, et al. Comparison of real-time polymerase chain reaction and serological tests for the confirmation of Mycoplasma pneumoniae infection in children with clinical diagnosis of atypical pneumonia. J Microbiol Immunol Infect. 2014;47:137–144. doi:10.1016/j.jmii.2013.03.015
32. Meyer Sauteur PM, Unger WW, Nadal D, et al. Infection with and carriage of Mycoplasma pneumoniae in children. Front Microbiol. 2016;7:329. doi:10.3389/fmicb.2016.00329
33. Kutty PK, Jain S, Taylor TH, et al. Mycoplasma pneumoniae among children hospitalized with community-acquired pneumonia. Clin Infect Dis. 2019;68:5–12. doi:10.1093/cid/ciy419
34. Yu XF, Kou Y, Zhou YY, et al. Analysis of pathogen characteristics in children with acute respiratory tract infection. Chin J Experi Clin Virol. 2018;32:160–165. doi:10.3760/cma.j.issn.1003-9279.2018.02.011
35. Chen J, Zhang J, Lu Z, et al. Mycoplasma pneumoniae among Chinese outpatient children with mild respiratory tract infections during the coronavirus disease 2019 pandemic. Microbiol Spectr. 2022;10:e0155021. doi:10.1128/spectrum.01550-21
36. Wang YN, Xu SM. Clinical characteristics of influenza virus antigen-positive patients in a Tertiary Hospital in Tianjin from 2017 to 2019. J Med Informat. 2021;34:155–158. doi:10.3969/j.issn.1006-1959.2021.16.044
37. He WW, Zhou HX, Wang WJ, et al. Multicenter analysis of false positive results of novel coronavirus specific antibody detection. Guangdong Med J. 2022;43:133–137. doi:10.13820/j.cnki.gdyx.20212637
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.