Back to Journals » Clinical Ophthalmology » Volume 20
Comparative Analysis of Corneal Endothelial Cell Loss After Phacoemulsification in Microcornea versus Normal-Sized Corneas
Authors Zheng T, Lin P, Miao A, Tang Y, Jiang Y, Xu J
Received 6 May 2026
Accepted for publication 26 June 2026
Published 8 July 2026 Volume 2026:20 616945
DOI https://doi.org/10.2147/OPTH.S616945
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sotiria Palioura
Tianyu Zheng,1,* Peimin Lin,2– 4,* Ao Miao,2– 4,* Yating Tang,2– 4 Yongxiang Jiang,2– 4 Jie Xu2– 4
1Department of Ophthalmology, Shanghai Tenth People’s Hospital, Tongji University School of Medicine, Shanghai, People’s Republic of China; 2Department of Ophthalmology, Eye & ENT Hospital, Fudan University, Shanghai, People’s Republic of China; 3NHC Key Laboratory of Myopia and Related Eye Diseases, Shanghai, People’s Republic of China; 4Shanghai Key Laboratory of Visual Impairment and Restoration, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jie Xu; Yongxiang Jiang, Department of Ophthalmology, Eye & ENT Hospital, Fudan University, 83 Fenyang Road, Shanhai, 200031, People’s Republic of China, Email [email protected]; [email protected]
Background: Phacoemulsification is inevitably accompanied by loss of corneal endothelial cells, and microcornea eyes with crowded anterior segments may be more susceptible to this damage.
Purpose: This study aimed to compare endothelial cell loss (ECL) after cataract phacoemulsification surgery between eyes with microcornea and those with normal-sized corneas.
Methods: This retrospective study included 50 eyes from 50 patients with microcornea and 120 eyes from 120 patients with normal-sized corneas who underwent phacoemulsification. Demographic data and biometric parameters were evaluated preoperatively. Postoperative corneal endothelial cell parameters were measured 3 months after surgery.
Results: Compared with the normal controls, the microcornea group had a shallower anterior chamber, thicker lens and shorter white-to-white distance (WTW) (P < 0.01). Additionally, at 3 months postoperatively, the microcornea group had significantly greater ECL (662.20 ± 496.79 cells/mm2) than the control group did (360.53 ± 364.29 cells/mm2) (P < 0.001). The increase in the mean cell area in the microcornea group (185.38 ± 144.04 μm2) was significantly greater than that in the control group (75.56 ± 92.48 μm2) (P < 0.001). Multiple regression analysis revealed that WTW (Beta=− 0.330, P< 0.001) and average phaco energy (Beta=0.288, P=0.030) were significant determinants of postoperative ECL in patients with normal-sized corneas. WTW was also a statistically significant risk factor for ECL in all patients (Beta=− 0.331, P< 0.001).
Conclusion: Compared with normal-sized corneas, microcorneas were more prone to endothelial cell loss after phacoemulsification. WTW was a significant risk factor for postoperative ECL. Preoperative measurement of WTW may serve as a useful risk stratification tool to identify patients who may require additional endothelial protective measures during cataract surgery.
Keywords: microcorneas, phacoemulsification, corneal endothelial cell loss
Introduction
Corneal endothelial cell loss (ECL), a major complication that occurs after cataract surgery, can lead to corneal edema and decompensation if the cell density decreases to 450–800 cells/mm2.1,2 Previous studies have revealed that several clinical parameters may influence the risk of ECL after phacoemulsification surgery. An increased risk of ECL is associated with significant lens nucleus hardness, advanced age, a long phacoemulsification time (Phaco time), the use of high-energy ultrasound, diabetes mellitus and a short axial length.3–8
Additionally, phacoemulsification surgery is performed in a limited and confined space. Narrow space can aggravate the damage induced by the phacoemulsification procedure. Although ophthalmic viscosurgical devices (OVDs) and the soft-shell technique are routinely used to protect the endothelium in crowded spaces, the risk of ECL may still be elevated in eyes with pre-existing anatomical constraints. Microcornea is a rare congenital anomaly, with an estimated prevalence of approximately 1 in 100,000 births, in which the horizontal diameter of the cornea is less than or equal to 11 mm; hence, cataract surgery in eyes with microcornea is challenging because of the narrow space for phacoemulsification.9–11 However, to our knowledge, no published studies have specifically reported ECL following routine phacoemulsification in microcornea eyes. Existing reports have mainly focused on postoperative visual outcomes and complication rates, rather than quantitative ECL.12–14 Given the rarity of this condition and the lack of robust evidence, characterizing ECL and its risk factors in microcornea eyes is of considerable clinical importance.
Therefore, this comparative study was designed to assess ECL after cataract phacoemulsification surgery in eyes with microcornea versus those with normal-sized corneas. We hypothesized that microcornea eyes would experience greater postoperative ECL. We also examined the effects of several clinical parameters on postoperative ECL to identify potential risk factors. Understanding these risk factors may better inform approaches for reducing the risk of intraoperative corneal endothelial injuries in patients with microcornea.
Methods
Patients
This retrospective study included patients who underwent phacoemulsification at the Eye and ENT Hospital of Fudan University between January 2023 and December 2023. The exclusion criteria were as follows: a history of ocular surgery, any serious intraoperative or postoperative complications, corneal disease (eg., dystrophy, scarring), and other severe ocular comorbidities (eg., trauma, glaucoma, uveitis, coloboma, and nanophthalmos (axial length < 20.5 mm)). In addition, patients who were unable to attend the 3-month postoperative follow-up visit were also excluded. Ultimately, 50 eyes from 50 patients with microcornea and 120 eyes from 120 patients with normal-sized cornea were enrolled. Microcornea was defined as a horizontal corneal diameter ≤11 mm, while normal controls had a horizontal corneal diameter >11 mm. All enrolled patients had grade III–IV nuclear cataracts. The severity of cataracts was graded according to the Lens Opacities Classification System III (LOCS III) by a single observer physician trained in the use of LOCS. The primary outcome was absolute ECL, defined as preoperative corneal endothelial cell density (CECD) minus postoperative CECD. Percentage ECL was calculated as (absolute ECL/preoperative CECD) × 100%. The study was approved by the ethics committee of the Eye and ENT Hospital of Fudan University and was conducted in accordance with the tenets of the Declaration of Helsinki. Informed consent was obtained from all patients.
Preoperative Examinations
Preoperatively, all patients underwent comprehensive ophthalmologic examinations, including slit‒lamp microscopy, intraocular pressure (IOP) measurement and B-mode ultrasound. The white-to-white distance (WTW, defined as the horizontal corneal diameter by the limbal position), anterior chamber depth (ACD), axial length (AL) and lens thickness (LT) were measured using an IOL Master 700 optical biometer (Carl Zeiss Meditec AG). The lens position (LP) was calculated using the following formula: ACD + 1/2 LT.15 Corneal endothelial cell analysis, including CECD, coefficient of variation (CV) of the cell area, mean cell area (MCA), percentage of hexagonal cells (HEX) and central corneal thickness (CCT), was performed with a specular microscopy device (EM-3000; Tomey Corporation).
Phacoemulsification Surgery
All eyes were subjected to uncomplicated phacoemulsification with IOL implantation by an experienced surgeon (TYZ, with over 10 years of experience and approximately 8,000 cataract surgeries performed). First, a 2.3-mm self-sealing temporal cornea incision was made, and the same cohesive viscoelastic (sodium hyaluronate 1.5%, Qisheng Biological Preparation Co. Ltd. Shanghai, China) was injected into the anterior chamber. A capsulorhexis approximately 5.5 mm in diameter was created, and then lens–nucleus hydrodissection was performed. All phacoemulsifications were conducted using the phaco-and-chop technique with torsional phacoemulsification on a Centurion system (Alcon Surgical, Texas, USA). The machine settings were: vacuum 320 mmHg, aspiration rate 28 cc/min, and bottle height 90 cm. After phacoemulsification, an acrylic IOL (PCB00, Abbott Medical Optics, Santa Ana, CA, USA) was implanted, and then the corneal incision was hydrated. The following variables were recorded at the end of the surgery: average phaco energy (%) and total phaco time (seconds). Since conventional cumulative dissipated energy (CDE) was developed for longitudinal ultrasound and does not directly apply to torsional mode, total phaco energy was defined as average phaco energy (%) × phaco time (seconds), expressed in %·
Postoperative Follow-Up
Postoperative follow-up at 3 months was chosen because corneal endothelial cell loss stabilizes by this timepoint after uncomplicated phacoemulsification, and earlier measurements may be confounded by transient postoperative inflammation and corneal edema. At this visit, IOP and corneal endothelial cell parameters, including the CECD, CV, MCA, HEX and CCT, were recorded.
Statistical Analysis
All statistical analyses were performed using SPSS 19.0 (IBM Corp., Armonk, NY, USA). Continuous variables were compared using an independent t test. A paired t test was used to compare the corneal endothelial cell parameters before surgery with those after surgery. Categorical variables were compared using the chi-square test. The associations of risk factors with postoperative ECL were examined via univariate and multivariate regression analyses. Contributing factors with a P value<0.2 in the univariate analysis were subsequently included in the multivariate regression model. Given the rarity of microcornea, a formal power analysis was not performed prior to data collection. However, our microcornea sample size (n = 50) is the largest reported to date for postoperative endothelial analysis in this condition, and the control group (n = 120) was selected to provide adequate statistical power for detecting clinically meaningful differences in ECL between groups. A P value <0.05 was considered to indicate statistical significance.
Results
Participants’ Clinical Data
One hundred seventy eyes of 170 patients were included in this study. The microcornea group included 50 eyes, and the normal control group included 120 eyes. Table 1 shows the preoperative, intraoperative and postoperative clinical data of these patients and the potential risk factors for postoperative ECL. Compared with the normal controls, the microcornea group had a shallower anterior chamber, thicker lens, and shorter WTW (P < 0.01). In the microcornea group, the mean WTW was 10.76 ± 0.24 mm, the mean ACD was 2.78 ± 0.50 mm, the mean LT was 4.62 ± 0.49 mm, and the mean LP was 5.09 ± 0.38 mm. In the control group, the mean WTW was 11.73 ± 0.36 mm, the mean ACD was 3.16 ± 0.34 mm, the mean LT was 4.39±0.39, and the mean LP was 5.36 ± 0.26 mm.
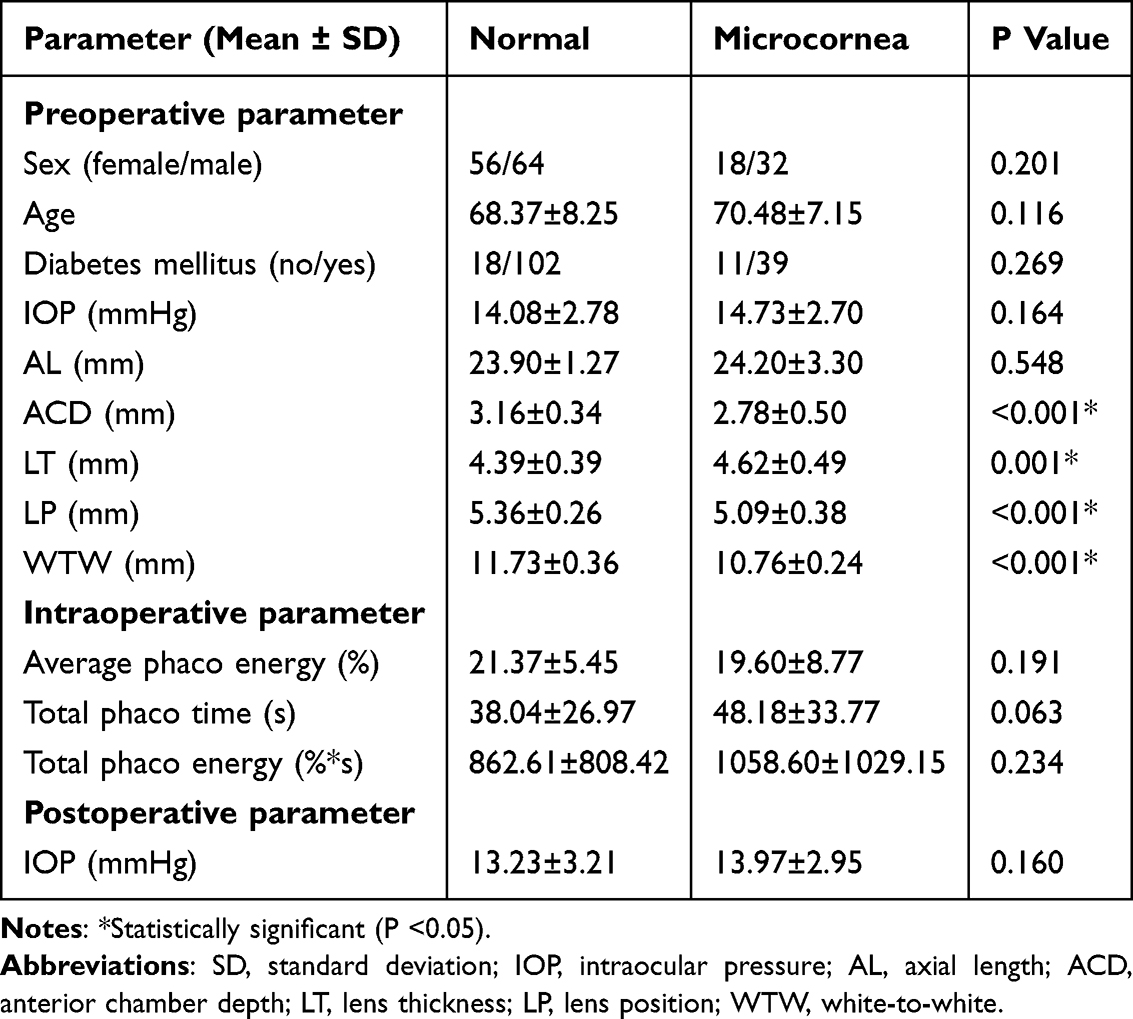 |
Table 1 Preoperative, Intraoperative and Postoperative Clinical Data |
Changes in Corneal Endothelial Cells After Phacoemulsification
The endothelial cell density and morphometry values as well as the CCT measurements assessed preoperatively and at 3 months after surgery and their preoperative-postoperative changes are summarized in Table 2. No significant difference was observed preoperatively between the microcornea group and the normal control group in any of the endothelial cell parameters or in the CCT, except the CV (Table 2). Patients with microcornea had a significantly lower CV than patients with normal-sized corneas did (P=0.035). Postoperatively, patients with microcornea had a significantly lower CECD and a significantly larger MCA than the normal controls did (both P < 0.001, Table 2). Both groups experienced a significant decrease in the CECD, a significant increase in the MCA and a significant decrease in the HEX (P < 0.01, Figure 1). The mean ECL was 662.20 ± 496.79 cells/mm2 (24.67 ± 18.49%) in the microcornea group and 360.53 ± 364.29 cells/mm2 (13.75 ± 14.18%) in the control group. Compared with the control group, the microcornea group had significantly greater ECL (Table 2, P < 0.001; Cohen’s d = 0.741, indicating a moderate-to-large effect size). Additionally, the enlargement of the MCA in the microcornea group (185.38 ± 144.04 μm2, 48.56 ± 37.39%) was significantly greater than that in the control group (75.56 ± 92.48 μm2, 19.57 ± 23.32%) (Table 2, P < 0.001; Cohen’s d = 0.998, indicating a large effect size). Outlier analysis using the IQR method did not reveal any extreme values that disproportionately influenced the group comparisons.
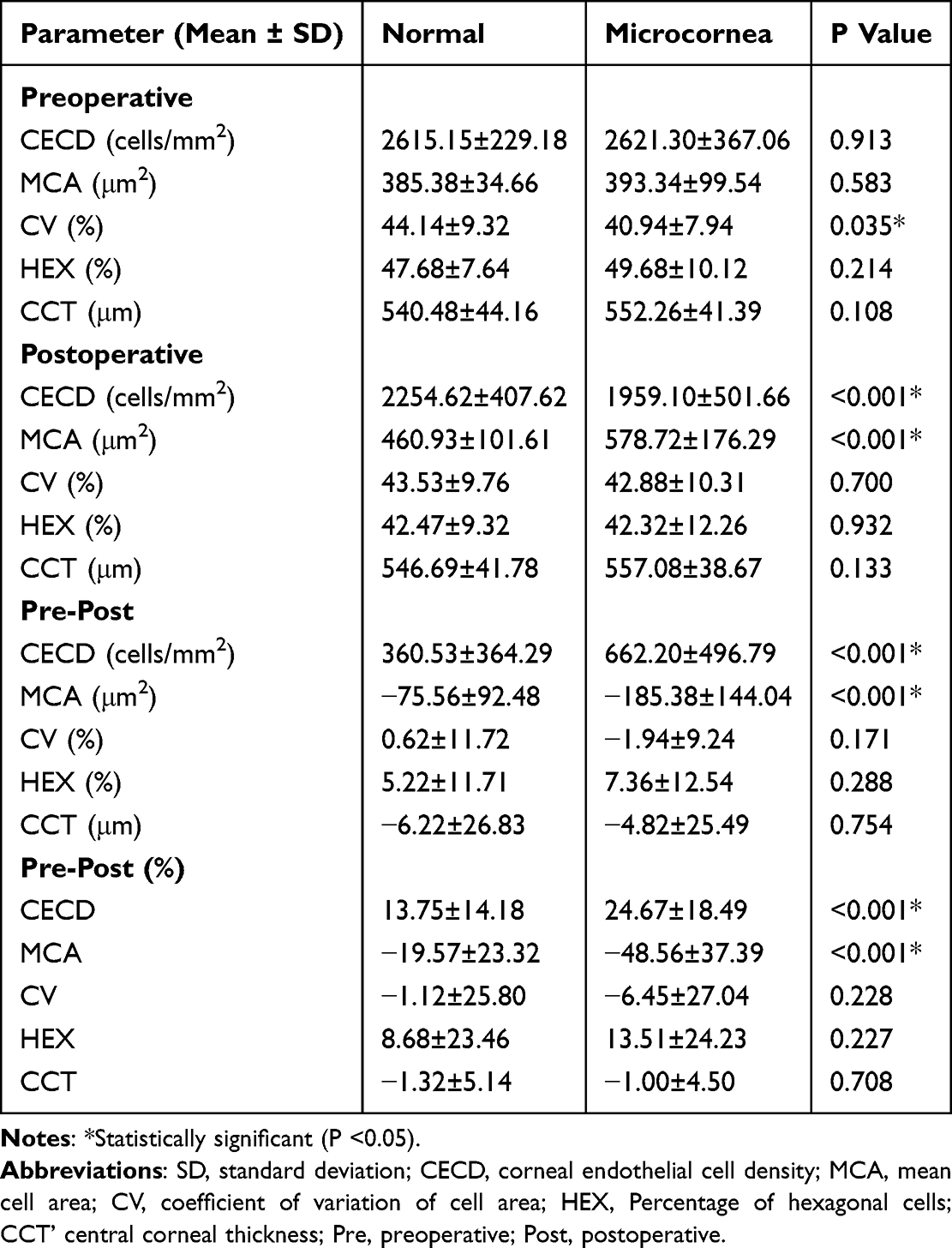 |
Table 2 Changes in Corneal Endothelial Cell After Phacoemulsification |
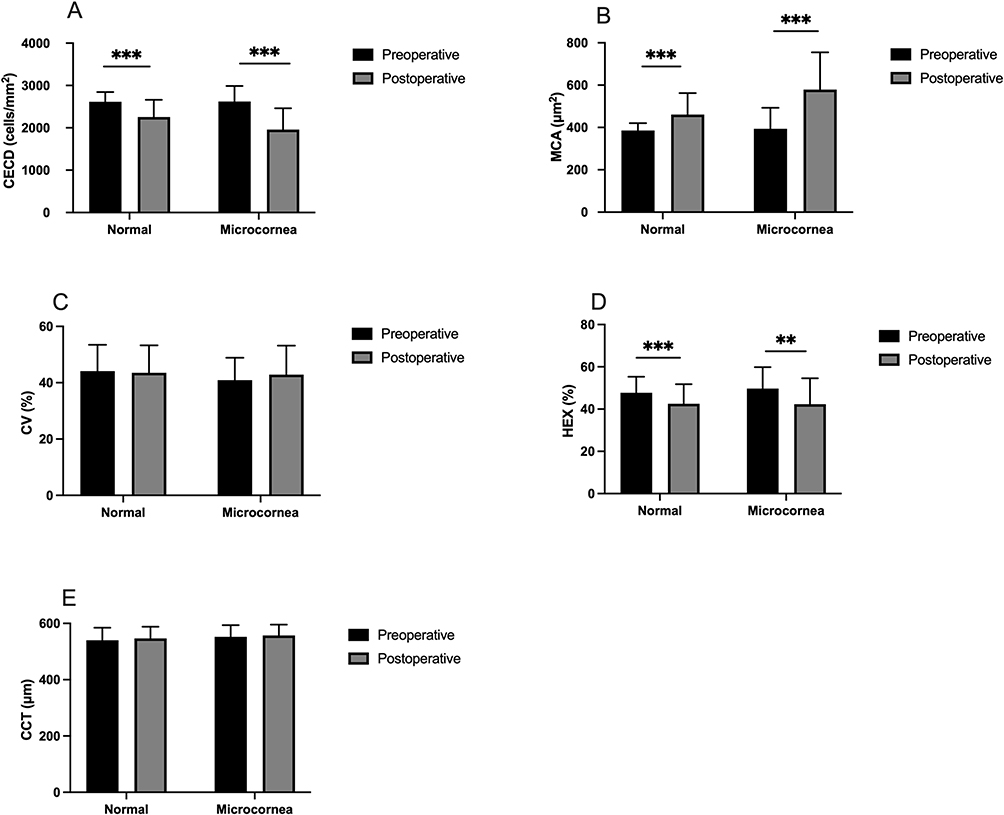 |
Figure 1 Changes in corneal endothelial cells after phacoemulsification surgery. (A) Corneal endothelial cell density (CECD). (B) Mean cell area (MCA) of corneal endothelial cells. (C) Coefficient of variation (CV) of the cell area. (D) Percentage of hexagonal cells (HEX). (E) Central corneal thickness (CCT). **P<0.01, ***P<0.001. |
Risk Factors for ECL in Normal Patients
Table 3 shows the correlations of the 17 variables from the univariate analysis with the ECL at postoperative month 3. In the normal control group, we selected age, preoperative CV, preoperative HEX, preoperative CCT, AL, ACD, LP, WTW, average phaco energy, total phaco time and total phaco energy (all P<0.2) for further multivariate linear regression analyses.
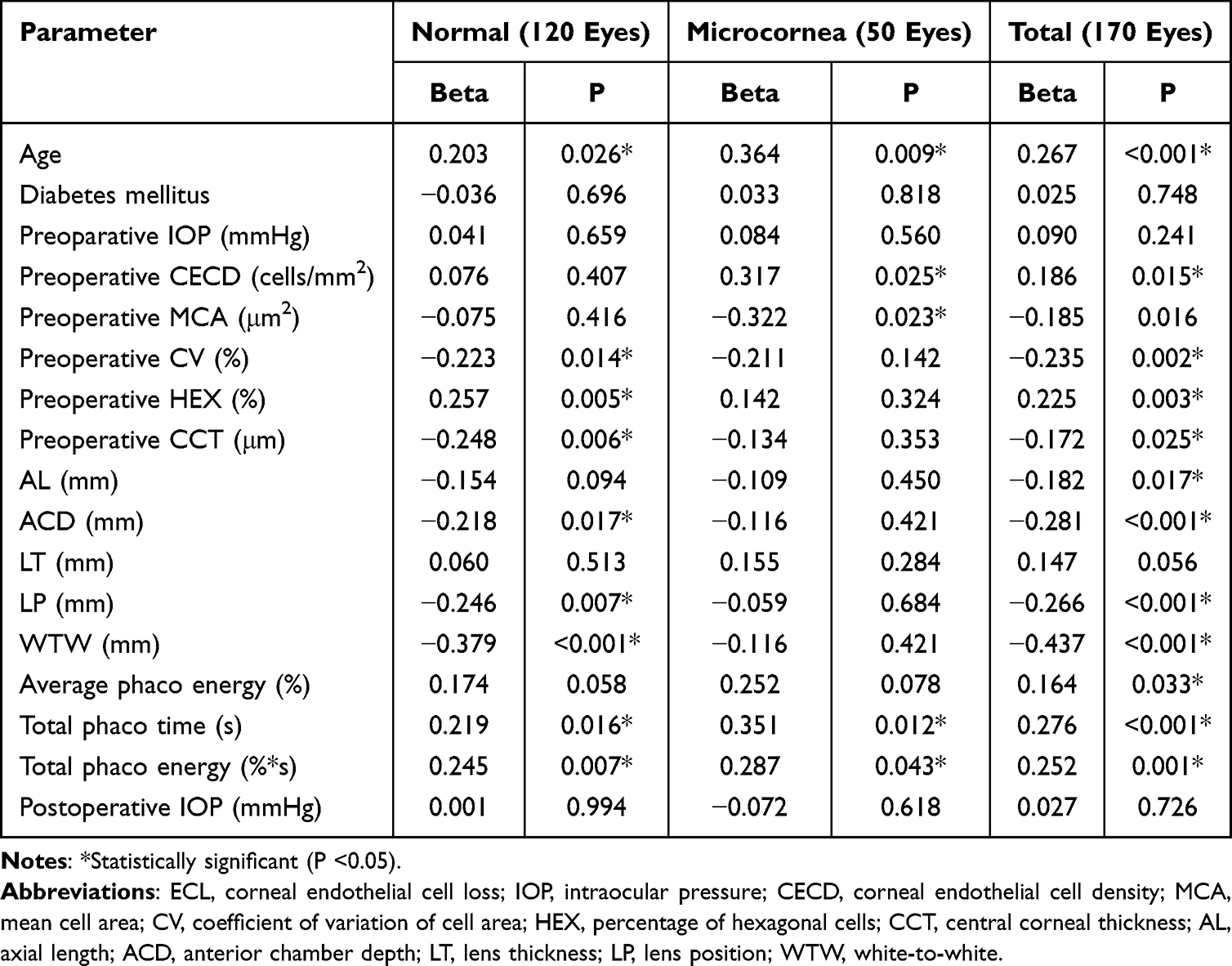 |
Table 3 Univariate Analyses of the Associations Between the ECL and the Clinical Parameters |
Ultimately, we obtained a model comprising WTW (Beta=−0.330, P<0.001) and average phaco energy (Beta=0.288, P=0.030) that predicted ECL in the normal control group (P<0.001, adj. R2=0.313 (Table 4). A smaller WTW and higher average phaco energy were the best set of independent predictors of greater postoperative ECL.
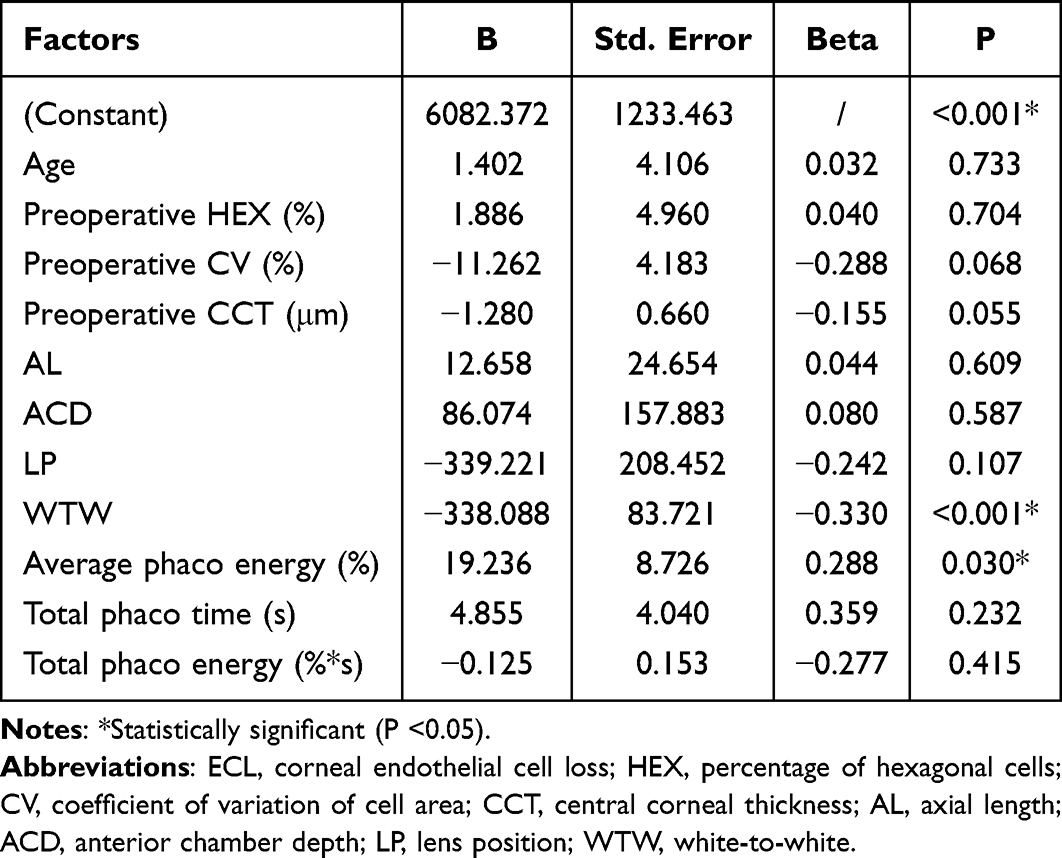 |
Table 4 Multivariable Model Predicting the ECL at Eyes with Normal-Sized Corneas, P<0.001, Adj. R2 = 0.313 |
Risk Factors for ECL in Patients with Microcornea
By univariate analysis, the factors that correlated with a lower postoperative CECD in patients with microcornea were patient age, preoperative CECD, preoperative MCA, preoperative CV, average phaco energy, total phaco time and total phaco energy (all P<0.2, Table 3). However, after stepwise multiple linear regression analysis, no significant multiple regression model was identified in the microcornea group (data not shown).
Risk Factors for ECL in All Patients
We also conducted univariate and multiple regression analyses for ECL in all patients. Table 3 shows the results of the univariate analysis for ECL. We selected age, preoperative CECD, preoperative MCA, preoperative CV, preoperative HEX, preoperative CCT, AL, ACD, LT, LP, WTW, average phaco energy, total phaco time and total phaco energy (P<0.2, Table 3) for further multiple regression analysis. Multiple regression analysis revealed that the WTW was the only statistically significant risk factor for ECL (Beta=−0.331, P<0.001, adj. R2=0.341, Table 5). A shorter WTW was significantly associated with greater ECL (Table 5).
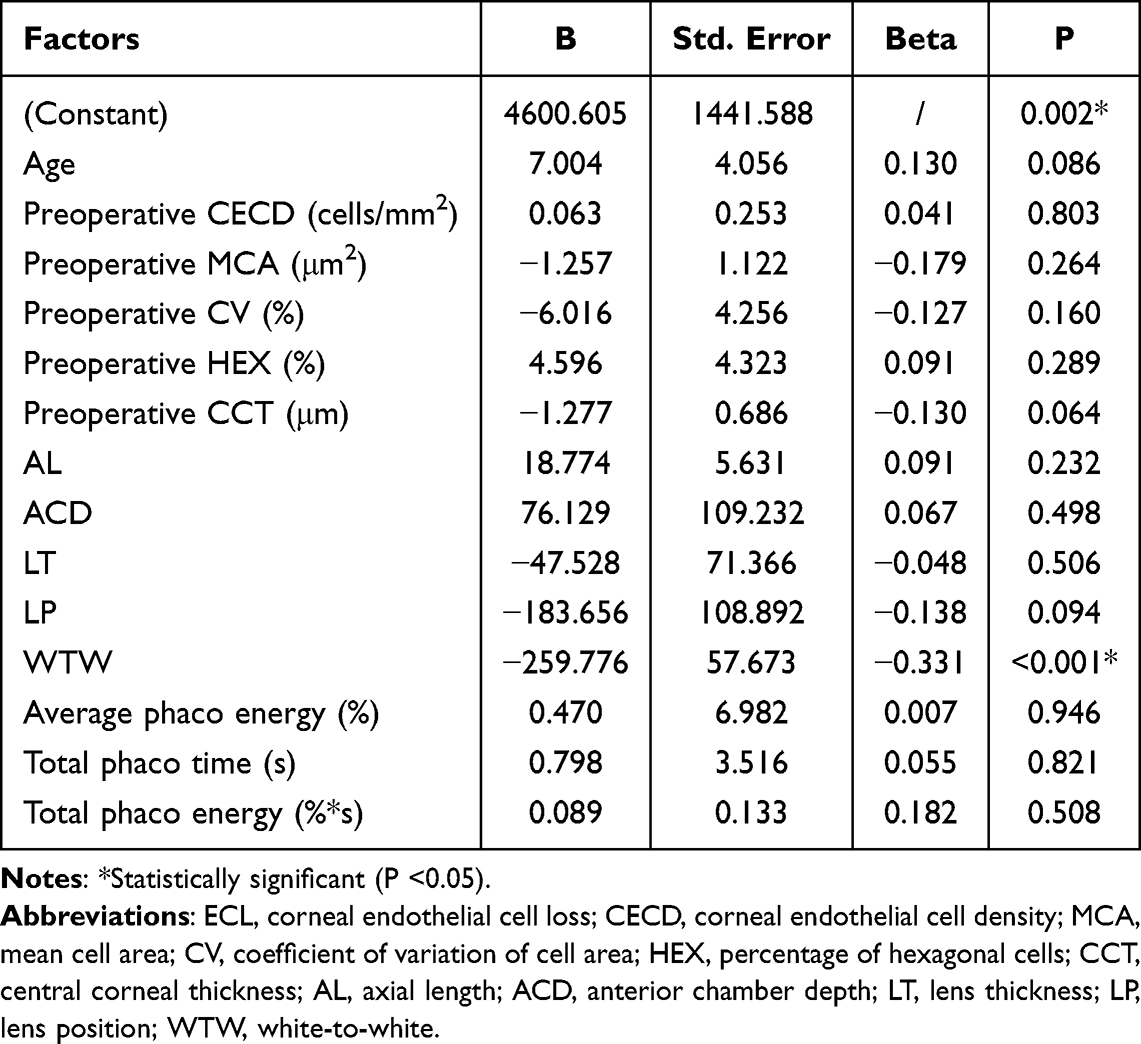 |
Table 5 Multivariable Model Predicting the ECL in Total Eyes, P<0.001, Adj. R2 = 0.341 |
Discussion
Lens extraction with phacoemulsification is inevitably accompanied by loss of corneal endothelial cells, and microcornea eyes with crowded anterior segments may be more susceptible to this damage.16,17 However, microcornea is a rare disease, and knowledge on postoperative ECL in this population remains limited. To our knowledge, no prior study has specifically quantified ECL following routine phacoemulsification in microcornea eyes. This is the first to demonstrate significantly greater ECL compared to normal-sized corneas, and to identify WTW as a strong risk factor. Understanding these results may better inform approaches to minimize corneal endothelial injury intraoperatively and assist in the identification of patients at greater risk of future complications.
Not surprisingly, patients with microcornea had significantly smaller corneal diameters than patients with normal-sized corneas did. In this study, the horizontal corneal diameters were 10.76 ± 0.24 mm and 11.73 ± 0.36 mm in the microcornea group and control group, respectively. Additionally, some characteristic features of microcornea include a significantly shallower anterior chamber, thicker lens, and shorter lens position. Wei et al reported a positive correlation between the WTW and ACD.18
Endothelial cell parameters were also explored. The preoperative CECD was not significantly different between the microcornea and control groups. The CECD was 2621.30 ± 367.06 cells/mm2 and 2615.15 ± 229.18 cells/mm2 in the microcornea group and control group (P = 0.913), respectively. Compared with the control group, the microcornea group tended to have a significantly greater CV of endothelial cells. This may be because a smaller surface area in the microcornea, leading to a compact cell arrangement and less pleomorphism.19 However, as there are few studies that can help us understand these exact correlations better, further exploration of the etiology of these relationships is needed.
After cataract surgery, we found that the CECD was significantly lower than that before surgery in both the microcornea and control groups. Additionally, the eyes with microcornea had significantly greater ECL (662.20±496.79 cells/mm2, 24.67±18.49%) than the eyes with normal-sized corneas did (360.53±364.29 cells/mm2, 13.75±14.18%). The reasons for these differences may be attributed to the narrower operating space in the eyes with microcornea, which have shallower anterior chambers and smaller WTWs. The shallower anterior chamber and smaller WTW reduce the working distance and bring the phaco tip closer to the endothelium, limiting the surgeon’s ability to maintain a safe margin.17 Moreover, these anatomical features reduce aqueous volume, which may diminish heat dissipation and result in a greater temperature rise for the same ultrasonic energy. In addition, mechanical shockwaves may have less distance to dissipate before reaching the endothelium, potentially leading to more concentrated mechanical stress. Consequently, even standard phaco energy levels could become more hazardous in microcornea eyes, contributing to disproportionately greater endothelial damage. Accordingly, postoperative enlargement of the MCA in the microcornea group was significantly greater than that in the control group. The increase in corneal cell area could be perceived as a possible compensatory mechanism in response to corneal endothelial cell loss.20
Furthermore, we performed univariate and multiple regression analyses of ECL to identify the significant risk factors for ECL in both the microcornea group and the control group.
Our results revealed that a smaller WTW and higher average phaco energy were the best set of independent predictors of greater ECL in eyes with normal-sized corneas. These findings further corroborate our abovementioned conclusion that eyes with normal-sized corneas have significantly less ECL than eyes with microcornea do. However, no significant correlation was found between ACD and postoperative ECL in our current study. A possible explanation is that the ACD was significantly associated with the WTW (Beta=0.441, P < 0.001). After adjusting for confounders through multiple regression analysis, ACD, which was a significant determinant of postoperative ECL in the univariate analyses (P=0.017, Table 3), was excluded from the final prediction model.
In addition, consistent with the findings of previous studies, average phaco energy was also proven to have a significant influence on ECL in the normal group in our current study.7,21,22 Nevertheless, we did not observe a significant correlation between the total phaco time and postoperative ECL, despite previous studies revealing that patients with longer phaco times could be at greater risk of corneal endothelial cell loss.4,23,24 We attributed this discrepancy to the different inclusion criteria. All the patients included in our study had Grade III–IV nuclei. Therefore, for patients with normal-sized corneas and middle-grade nuclei, we recommend that surgeons use low phaco energy, even at the cost of a longer total phaco time.
However, we obtained no statistically significant multivariate linear regression models that predicted postoperative ECL for eyes with microcornea, possibly because of the insufficient sample sizes of microcornea group.
We also performed univariate and multivariate regression analyses of ECL in all the patients and found that the WTW was positively correlated with postoperative ECL, further confirming the results in patients with normal-sized corneas.
Since microcornea can correlate with short AL, we considered whether AL might have confounded the association between microcornea and ECL. In our study, patients with nanophthalmos were excluded, AL did not differ significantly between groups (P = 0.548, Table 1), and AL was not significant in any regression model. These findings suggest that the observed ECL in microcornea eyes is unlikely to be attributable to AL-related factors, reinforcing WTW as the key anatomical predictor.
Therefore, phacoemulsification should be performed more carefully in patients with smaller WTW, and we recommend higher-viscosity OVDs or soft-shell technique, minimized phaco energy, lower aspiration flow rates, and a chop technique.
Limitations
The current study has several limitations. Only 50 eyes with microcornea were enrolled, so future studies with larger sample sizes are warranted to validate our initial findings. Second, eyes with extreme microcornea, defined as a WTW < 10 mm, were not enrolled; further studies involving patients with extremely small corneas are necessary to verify our results. Third, our inclusion of only Grade III–IV nuclear cataracts enhances the homogeneity of the study population but also limits the generalizability of our findings to patients with softer or denser cataracts. This design choice was intentional to minimize confounding by varying nucleus hardness, but caution is warranted when extrapolating our results to all cataract grades.
Conclusions
In conclusion, our current study revealed that eyes with microcornea were more prone to endothelial cell loss after phacoemulsification compared to eyes with normal-sized corneas. We also noted that ECL was significantly related to the WTW and average phaco energy used during the surgical procedure in eyes with normal-sized corneas, and the WTW was further confirmed as a significant risk factor for ECL in all patients. Phacoemulsification in microcornea requires meticulous surgical technique, with careful attention to energy control and endothelial protection. Preoperative WTW measurement may serve as a simple and valuable tool for risk stratification, identifying patients who may benefit from enhanced endothelial protective strategies.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding authors (Dr. Jie Xu) upon reasonable request.
Ethics Approval and Patient Consent to Participate
This study was approved by the Ethics Committee of the Eye & Ear, Nose, and Throat Hospital of Fudan University (Shanghai, China). The ethical approval number is 2013021. All procedures adhered to the tenets of the Declaration of Helsinki. Participants gave informed consent to participate in the study before taking part.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. In detail: concept and design: JX and YXJ; data acquisition and research execution: TYZ, PML, AM, YTT; analysis and interpretation: JX, YXJ, TYZ, PML and AM; manuscript preparation and final approval: JX, YXJ, TYZ, PML, AM and YTT; guarantor: JX and YXJ.
Funding
This study was supported by grants from the National Natural Science Foundation of China (NSFC 82101103 and 81300747), Young Clinical Scientist Training Program of Shanghai Medical College of Fudan University (2023, DGF828019-2/038); Natural Science Foundation of Shanghai (Research Project of Science and Technology Commission of Shanghai Municipality; 22ZR1410400 and 19ZR1408600), the Scientific Research Program of Shanghai Pudong New Area Health Commission (the Joint Research and Development Program), the “Medicine + X” Interdisciplinary Research Project of Tongji University (2025) and the Excellent Young Doctor Training Program of Shanghai (2015).
Disclosure
The authors declare that they have no conflicts of interest to disclose for this work.
References
1. Daus W, Völcker HE. Corneal endothelium. Anatomy, physiology, biomicroscopy, clinical aspects and pathology. Ophthalmologe. 1992;89(2):15–10.
2. Reuschel A, Bogatsch H, Oertel N, Wiedemann R. Influence of anterior chamber depth, anterior chamber volume, axial length, and lens density on postoperative endothelial cell loss. Graefes Arch Clin Exp Ophthalmol. 2015;253(5):745–752. doi:10.1007/s00417-015-2934-1
3. Orski M, Synder A, Pałenga-Pydyn D, Omulecki W, Wilczyński M. The effect of the selected factors on corneal endothelial cell loss following phacoemulsification. Klin Oczna. 2014;116(2):94–99.
4. Lee NSY, Ong K. Risk factors for corneal endothelial cell loss after phacoemulsification. Taiwan J Ophthalmol. 2024;14(1):83–87. doi:10.4103/tjo.TJO-D-23-00146
5. Ko YC, Liu CJL, Lau LI, Wu CW, Chou JC, Hsu WM. Factors related to corneal endothelial damage after phacoemulsification in eyes with occludable angles. J Cataract Refract Surg. 2008;34(1):46–51. doi:10.1016/j.jcrs.2007.07.057
6. Goldstein AS, Janson BJ, Skeie JM, Ling JJ, Greiner MA. The effects of diabetes mellitus on the corneal endothelium: a review. Surv Ophthalmol. 2020;65(4):438–450. doi:10.1016/j.survophthal.2019.12.009
7. Mahdy MAS, Eid MZ, Mohammed MAB, Hafez A, Bhatia J. Relationship between endothelial cell loss and microcoaxial phacoemulsification parameters in noncomplicated cataract surgery. Clin Ophthalmol. 2012;6:503–510. doi:10.2147/OPTH.S29865
8. Joo JH, Kim TG. Comparison of corneal endothelial cell changes after phacoemulsification between type 2 diabetic and nondiabetic patients. Medicine. 2021;100(35):e27141. doi:10.1097/MD.0000000000027141
9. Chang TC, Tran KD, Cernichiaro-Espinosa LA, et al. Microcornea and Thickened Lens in Angle Closure following Nonsurgical Treatment of Retinopathy of Prematurity. J Ophthalmol. 2020;2020:7510903. doi:10.1155/2020/7510903
10. Abouzeid H, Meire FM, Osman I, et al. A New Locus for Congenital Cataract, Microcornea, Microphthalmia, and Atypical Iris Coloboma Maps to Chromosome 2. Ophthalmology. 2009;116(1):154–162. doi:10.1016/j.ophtha.2008.08.044
11. Nirmalan PK, Krishnaiah S, Nutheti R, et al. Consanguinity and eye diseases with a potential genetic etiology. Data from a prevalence study in Andhra Pradesh, India. Ophthalmic Epidemiol. 2006;13(1):7–13. doi:10.1080/09286580500473795
12. Kesimal B, Kocamış Sİ. Approach to Cataract Surgery in a Case with Microcornea and Coloboma. Rom J Ophthalmol. 2025;69(3):436–439. doi:10.22336/rjo.2025.68
13. Zhang F, Li ZL, Wu JY, Zhao YE. Comparison of outcomes after early congenital cataract surgery in eyes with/without microcornea. Int J Ophthalmol. 2025;18(10):1875–1879. doi:10.18240/ijo.2025.10.08
14. Oshika T, Matsuki N, Endo T, et al. Long-term outcomes of congenital cataract surgery in eyes with microcornea operated within the first year of life. Sci Rep. 2026;16(1):11138. doi:10.1038/s41598-026-51101-0
15. Hwang HS, Ahn YS, Cho YK. Preoperative Mannitolization Can Decrease Corneal Endothelial Cell Damage After Cataract Surgery. Curr Eye Res. 2016;41(9):1161–1165. doi:10.3109/02713683.2015.1101138
16. Ganesh S, Brar S, Wadhokar S. Changes in endothelial cell density after conventional phacoemulsification and FLACS in eyes with dense cataracts. J Cataract Refract Surg. 2024;50(6):572–577. doi:10.1097/j.jcrs.0000000000001408
17. Cho YK, Chang HS, Kim MS. Risk Factors for Endothelial Cell Loss after Phacoemulsification: comparison in Different Anterior Chamber Depth Groups. Korean J Ophthalmol. 2010;24(1):10. doi:10.3341/kjo.2010.24.1.10
18. Wei L, He W, Meng J, Qian D, Lu Y, Zhu X. Evaluation of the White-to-White Distance in 39,986 Chinese Cataractous Eyes. Invest Ophthalmol Vis Sci. 2021;62(1):7. doi:10.1167/iovs.62.1.7
19. Dhakal R, Mohamed A, Chaurasia S, Ramappa M, Jalali S. Corneal Endothelial Cell Density in Uveal Coloboma Associated With Microcornea. Cornea. 2019;38(1):74–77. doi:10.1097/ICO.0000000000001755
20. Kim DH, Wee WR, Hyon JY. The pattern of early corneal endothelial cell recovery following cataract surgery: cellular migration or enlargement? Graefes Arch Clin Exp Ophthalmol. 2015;253(12):2211–2216. doi:10.1007/s00417-015-3100-5
21. Baradaran-Rafii A, Rahmati-Kamel M, Eslani M, Kiavash V, Karimian F. Effect of hydrodynamic parameters on corneal endothelial cell loss after phacoemulsification. J Cataract Refract Surg. 2009;35(4):732–737. doi:10.1016/j.jcrs.2008.12.017
22. Sorrentino FS. Qualitative Alterations on Corneal Endothelial Cell Morphometry and Hexagonality After Cataract Surgery. Clin Ophthalmol. 2021;15:4847–4853. doi:10.2147/OPTH.S338001
23. O’Brien PD, Fitzpatrick P, Kilmartin DJ, Beatty S. Risk factors for endothelial cell loss after phacoemulsification surgery by a junior resident. J Cataract Refract Surg. 2004;30(4):839–843. doi:10.1016/S0886-3350(03)00648-5
24. Perone JM, Luc MS, Zevering Y, Vermion JC, Gan G, Goetz C. Narrative review after post-hoc trial analysis of factors that predict corneal endothelial cell loss after phacoemulsification: tips for improving cataract surgery research. PLoS One. 2024;19(3):e0298795. doi:10.1371/journal.pone.0298795
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Relationship Between Postoperative Oxidative Stress Levels and Corneal Endothelial Cell Loss After Phacoemulsification in Diabetic Patients with Cataract
Gao Y, Yang N, Wei L, Yan Y, Li L
Clinical Ophthalmology 2024, 18:3957-3965
Published Date: 25 December 2024