Back to Journals » Neuropsychiatric Disease and Treatment » Volume 18
Comorbidity Between Recent Diagnosis of Type 2 Diabetes and Non-Psychotic Psychiatric Disorders: Metabolic Characteristics and Clinical Correlates
Authors Alcántara-Garcés MT ![]() , Rodríguez-Ramírez AM
, Rodríguez-Ramírez AM ![]() , García-Ulloa AC
, García-Ulloa AC ![]() , Hernández-Jiménez S
, Hernández-Jiménez S ![]()
Received 4 March 2022
Accepted for publication 27 May 2022
Published 12 June 2022 Volume 2022:18 Pages 1151—1163
DOI https://doi.org/10.2147/NDT.S364556
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Roger Pinder
María Teresa Alcántara-Garcés, Alejandra Monserrat Rodríguez-Ramírez, Ana Cristina García-Ulloa, Sergio Hernández-Jiménez On behalf of the Group of Study CAIPaDi
Centro de Atención Integral del Paciente con Diabetes (CAIPaDi), Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán, Mexico City, Mexico
Correspondence: Alejandra Monserrat Rodríguez-Ramírez, Centro de Atención Integral del Paciente con Diabetes (CAIPaDi), Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán, Vasco de Quiroga No. 15, Colonia Sección XVI, Tlalpan, Mexico City, 14080, Mexico, Tel +1 52 55 54870900 5045 ; +1 52 55 55737378, Email [email protected]
Purpose: To describe the metabolic status and clinical characteristics associated with NPPD in patients with less than five years of T2D diagnosis and explore the role of age in the presentation of psychiatric comorbidities.
Patients and Methods: This was a cross-sectional study of subjects who attended a comprehensive care program. Patients were assessed using the Mini-International Neuropsychiatric Interview, and clinical and metabolic characteristics were registered. Multivariate logistic regression analyses were conducted to identify risk and protective factors for psychiatric disorders. We performed an analysis to further explore age’s influence on our results.
Results: We included 1953 patients, and 40.1% had any psychiatric disorder. Younger age, female sex, and personal psychiatric history were associated with NPPD. The use of insulin was reported as a protective factor for eating disorders. Body mass index was associated with any psychiatric disorders and eating disorders. The analysis of age reported that patients younger than 45 years had the worst metabolic parameters and increased odds for NPPD, while patients older than 65 years had the best metabolic measures and decreased odds for psychiatric comorbidity.
Conclusion: NPPD were frequent comorbidities in our sample; younger age, female sex, and personal psychiatric history were the most important factors associated with psychiatric comorbidities. Younger subjects experience a higher risk for psychiatric disorders and worst metabolic control.
Keywords: diabetic care, psychiatric comorbidity, psychopathology
Introduction
Non-psychotic psychiatric disorders (NPPD) are frequent comorbidities of type 2 diabetes (T2D) with an estimated prevalence of 42.5%.1,2 Among the most frequent conditions are depressive and anxiety disorders2–4 which have been associated with poor outcomes and complications in diabetes.5–8 There is a complex interrelation between NPPD and diabetes that implicates genetic factors, adverse early environment, neuroendocrine dysfunction, changes in lifestyle, and psychotropic side effects.1,9–11 Nonetheless, the interaction between these conditions in patients with T2D of recent diagnosis has not been fully elucidated.
TD2 is a global public health problem principally in low- and middle-income countries.12 According to a Mexican National Health and Nutrition Survey (2018), 10.3% of the Mexican population over 20 years old has diabetes.13 The Institute for Health Metrics and Evaluation in 2019 reported diabetes as the cause of 5.14% of total disability-adjusted life years for the Mexican population between 50 and 69 years old, and 4.31% in patients over 70 years old.14
Previous studies reported variable frequencies of psychiatric disorders in T2D patients, with anxiety prevalence reports from 19% to 55%,15,16 whereas the prevalence of depression goes from 10.8% to 63%.3,15–17 Whitworth et al6 reported an association of depression and anxiety with higher HbA1c, body mass index (BMI), greater likelihood of current smoking, and reduced self-monitoring of blood glucose. Other studies related NPPD with increased mortality risk in patients with type 2 diabetes5 compared to controls without psychiatric comorbidities.
Nonetheless, most of the studies used different tools to assess depression and anxiety, including patients with different clinical courses and variable times of evolution of the endocrinologic disease. The time elapsed since the diagnosis of diabetes can influence the process of illness, adaptation to the disease, modifications of self-care behavior, and lifestyle changes to achieve glycemic control.18 Magnetic resonance imaging studies reported brain structural and functional alterations in T2D patients which are believed to be originated from vascular changes over time.19 Since psychiatric symptoms are an expression of brain function, these time-related alterations might also contribute to changes in the presentation of NPPD throughout a lifetime. Therefore, the prevalence and correlates of non-psychotic psychiatric comorbidities could be different along with the evolution of the disease. NPPD which is present during the first years of diabetes diagnosis and remains untreated might interfere with metabolic control, the prevention or delay of complications, and the optimization of the quality of life. Early screening and treatment of NPPD are clinically relevant for the comprehensive care of these patients and the limitation of potential risks.6 Hence, this study aims to describe the metabolic status and clinical characteristics associated with NPPD in patients with less than five years of T2D diagnosis and to explore the role of age in the presentation of psychiatric comorbidities.
Materials and Methods
Cross-sectional study, from a multidisciplinary care model for patients with diabetes in Mexico City, the Center of Comprehensive Care for the Patient with Diabetes (CAIPaDi, an acronym for its name in Spanish).20,21
Participants
We included patients over 18 years old, with less than 5 years of T2D diagnosis, BMI <45 kg/m2, without disabling diabetes complications, non-smokers, and without a psychotic psychiatric disorder. Pregnant women and drug users were excluded from the study. The Institutional Ethics and Research Committees from the National Institute of Medical Sciences and Nutrition Salvador Zubirán approved this study (Ref 1198). Written consent was obtained from subjects who participated in the study and the research was conducted according to the Declaration of Helsinki standards. All participants were informed about the purpose of the study.
Procedure
Our sample was collected from patients who attended the CAIPaDi. T2D was confirmed by blood test according to ADA diagnostic criteria (hemoglobin A1c ≥6.5% or fasting plasma glucose ≥ 126mg/dL or random plasma glucose ≥200mg/dL).22 A consultation-liaison psychiatrist made an initial face-to-face psychiatric evaluation, which included a clinical interview, and the application of the Mini International Neuropsychiatric Interview (M.I.N.I.) Spanish version 5.0.0,24 and an evaluation of eating behavior alterations.
The M.I.N.I. Spanish version,23,24 is a short diagnostic structured interview to identify 16 psychiatric disorders according to the Diagnostic and Statistical Manual IV-TR edition (DSM-IV-TR) classification (major depressive disorder, dysthymic disorder, manic or hypomanic episode, suicide risk, panic disorder, agoraphobia, social phobia, obsessive-compulsive disorder, post-traumatic stress disorder, alcohol dependence, drugs dependence, psychotic disorders, anorexia, bulimia, generalized anxiety disorder, and antisocial personality disorder).
The evaluation of eating behavior alterations included binge eating disorder (BED), other specified feeding or eating disorders like BED of low and limited duration, and eating disorders not otherwise specified like emotional eating according to the Diagnostic and Statistical Manual 5th edition (DSM-5) criteria.25
We obtained blood tests to measure fasting glucose, creatinine, lipid profile (using colorimetric methods, SYNCHRON CX System), and HbA1c (using HPLC method, Bio-Rad Variant II Turbo HbA1c Kit 2). Body composition was assessed by bioimpedance (body composition analyzer JAWON medical ioi353).
Statistical Analysis
For the statistical analysis, we employed the software STATA 13.0 (StataCorp. 2013. Stata Statistical Software: Release 13. College Station, TX: StataCorp LP). Normal distribution was assessed with the Kolmogorov–Smirnov test and all the quantitative variables were non-parametric distribution (p<0.000). We present our data with median with interquartile range according to distribution, and categorical variables are reported in frequency and percentage. Comparative analyses were conducted between groups with and without NPPD, affective, anxiety, and eating disorders. Continuous variables were compared with the Mann–Whitney U-test. The association between categorical variables was assessed using the χ2 test.
Multiple logistic regression analyses identified variables associated with NPPD, anxiety disorders (AXD), affective disorders (AFD), and eating disorders (ED). Each model was constructed by the forward method and the presence of the psychiatric condition (NPPD, AXD, AFD, ED) was the dependent variable. The p-value <0.05 was considered statistically significant.
For the analysis of age influence in our results, we divided patients into three groups: less than 45 years, 45 to 65, and more than 65 years of age. We compared the three groups using the χ2 test and Kruskal–Wallis test. Finally, we performed a multivariate logistic regression analysis for each of the age groups using as dependent variables the presence of any NPPD, AXD, AFD, and ED. Covariates were the significant variables obtained in the previous multivariate logistic regression.
Results
NPPD Prevalence and Descriptive Data
Patients were recruited from January 2016 to December 2020, our sample included 1953 patients, 54.8% were women, and the median years of TD2 diagnosis was 1 (0–3). Non-psychotic psychiatric disorder was present in 40.1%. The most frequent conditions were anxiety disorders (n=416, 21.3%), affective disorders (n=383, 19.6%), and eating disorders (n=483, 24.7%). Among affective disorders we included patients with major depressive disorder (n=299, 15.3%) dysthymic disorder (n=63, 3.2%), suicide risk (n=80, 4.1%) and manic or hypomanic episode (n=39, 3.3%). The anxiety disorders group was composed by panic disorder (n=49, 2.5%), agoraphobia (n=47, 2.4%), social phobia (n=17, 0.9%), obsessive-compulsive disorder (n=29, 1.5%), posttraumatic stress disorder (n=33, 1.7%) and general anxiety disorder (n=275, 14.1%). Eating disorders included emotional eating in 23.7% (n=463) and BED and other specified feeding or eating disorders like BED of low and limited duration in 7.0% (n=137).
A comparative analysis was conducted between groups with and without, any non-psychotic psychiatric comorbidity, anxiety disorders (AXD), affective disorders (AFD), and eating disorders (ED) (Tables 1 and 2). The group of patients with any NPPD reported lower median age, a higher proportion of female subjects, a higher presence of personal psychiatric history (PPH), and higher levels of total cholesterol, LDL-cholesterol, and non-HDL cholesterol, triglycerides, and BMI compared to the group without psychiatric conditions. AXD group reported lower median age, a higher proportion of female sex subjects, a higher proportion of PPH, and higher levels of HDL cholesterol compared with subjects without anxiety disorders. For AFD, differences in clinical correlates were age (younger), female sex, school years, and PPH. We found no differences in metabolic characteristics. The group with ED presented younger age, a higher proportion of females, a higher median of school years, a higher proportion of PPH, and higher levels of non-HDL cholesterol, triglycerides, and BMI. Patients without ED reported a higher frequency of insulin use.
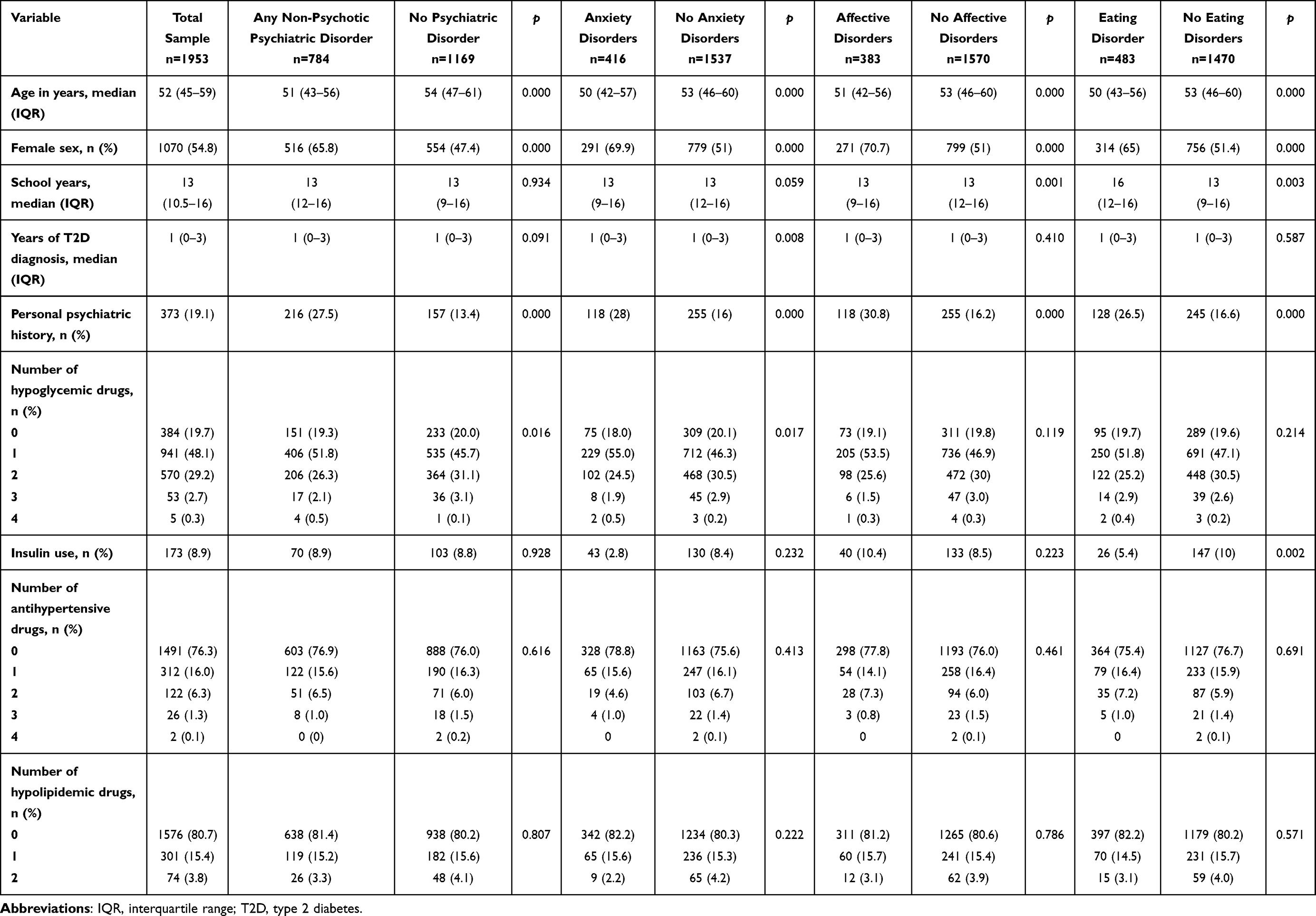 |
Table 1 Sociodemographic Characteristics and Clinical Features. Comparative Analysis of Patients with and without Any Non-Psychotic Psychiatric Disorder, Anxiety, Affective and Eating Disorders |
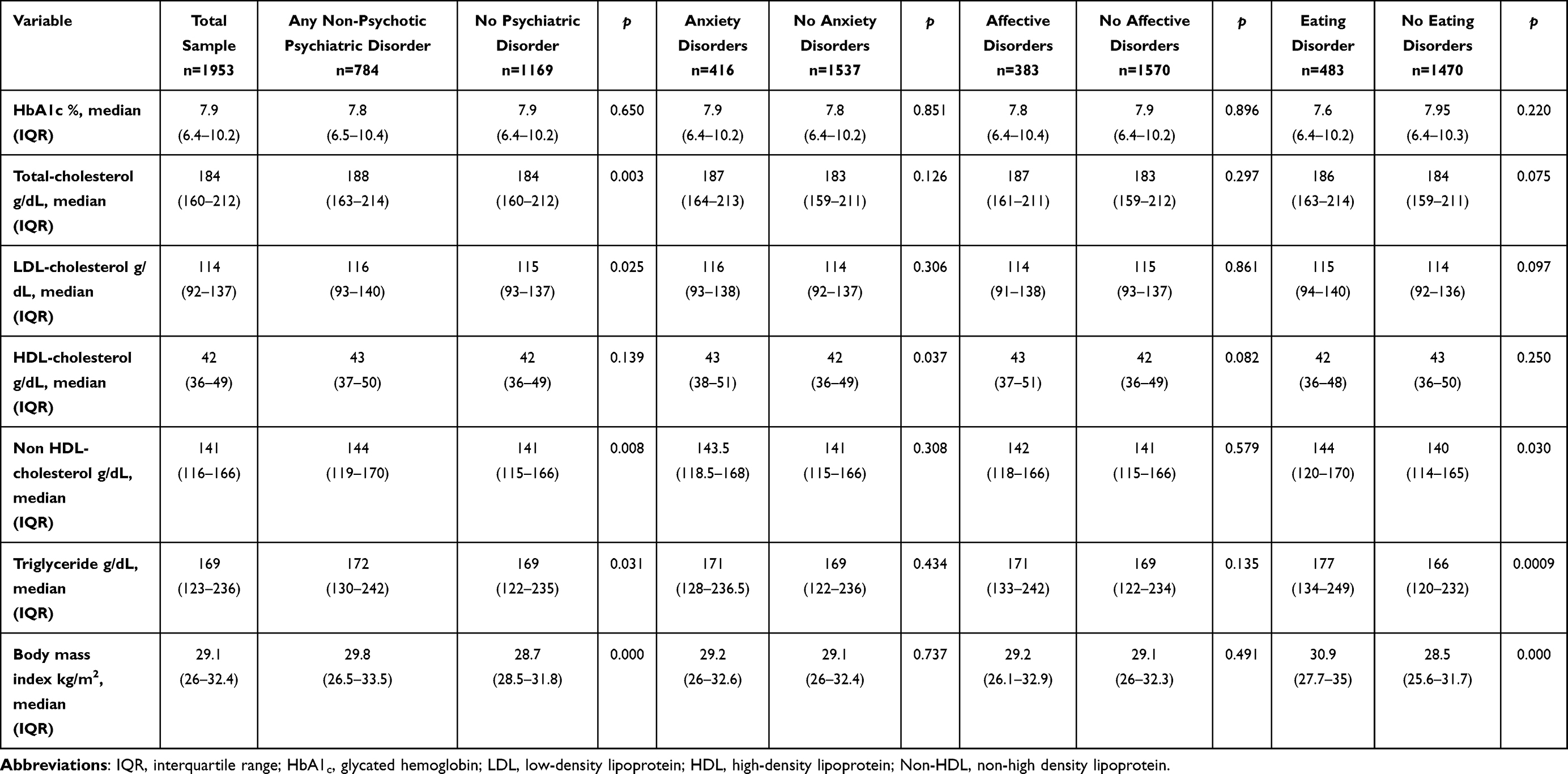 |
Table 2 Metabolic Parameters. Comparative Analysis of Patients with and without Any Non-Psychotic Psychiatric Disorder, Anxiety, Affective and Eating Disorders |
Risk Factors Associated with NPPD
The results of the multivariate analyses are shown in Table 3. A first logistic regression analysis reported an association of NPPD with female sex, PPH, and BMI. Age was also associated with NPPD as a protective factor. Total cholesterol, LDL-cholesterol, non-HDL cholesterol, triglycerides, and hypoglycemic drugs had no association with NPPD. Female sex, younger age, years of diagnosis, and personal psychiatric history were associated with AXD, whereas HDL-cholesterol and oral hypoglycemic medications were not significant. The logistic regression for the presence of AFD reported an association of age, female sex, school years, and PPH with those conditions. Age was also a protective factor for AFD. Last, we found associations between female sex, age, school years, PPH, no-HDL cholesterol, BMI, and insulin use with ED, whereas triglycerides were not significant. Again, age was a protective factor for eating disorders.
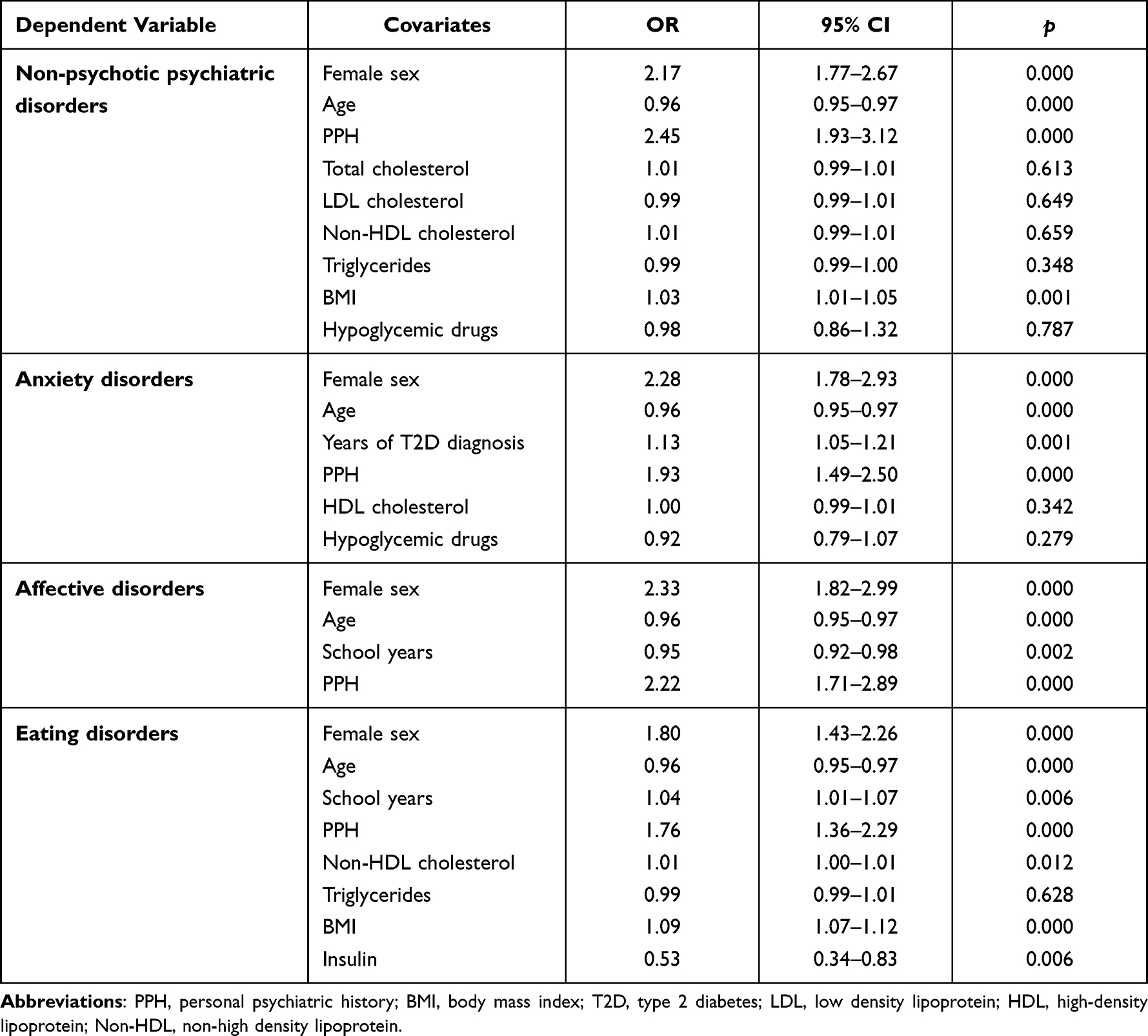 |
Table 3 Multivariate Logistic Regression Analyses for the Presence of Any Non-Psychotic Psychiatric Disorder, Anxiety, Affective and Eating Disorders |
Age-Related Findings
The comparative analysis of age groups is depicted in Table 4. The younger group (<45 years) reported a higher percentage of male subjects, a greater number of school years and insulin use, and fewer years of T2D diagnosis. Their metabolic status presented higher levels of HbA1c, triglycerides, and BMI compared to other groups. Young subjects also reported a higher prevalence of any NPPD, AXD, AFD, and ED than older patients. The group of age between 45 and 65 years was 68% of the sample and had a higher presence of female subjects. This group presented higher levels of total cholesterol and LDL-cholesterol compared to the other groups. The prevalence of NPPD for this group was greater than the younger ones but higher than the oldest. The >65 years old group presented a female majority, with fewer years of formal education, and longer time elapsed since T2D diagnosis. Nonetheless, they showed lower levels of HbA1c, triglycerides, and BMI than the other groups. Lower prevalence of any NPPD, anxiety, affective, and eating disorders were reported in this group compared with younger subjects.
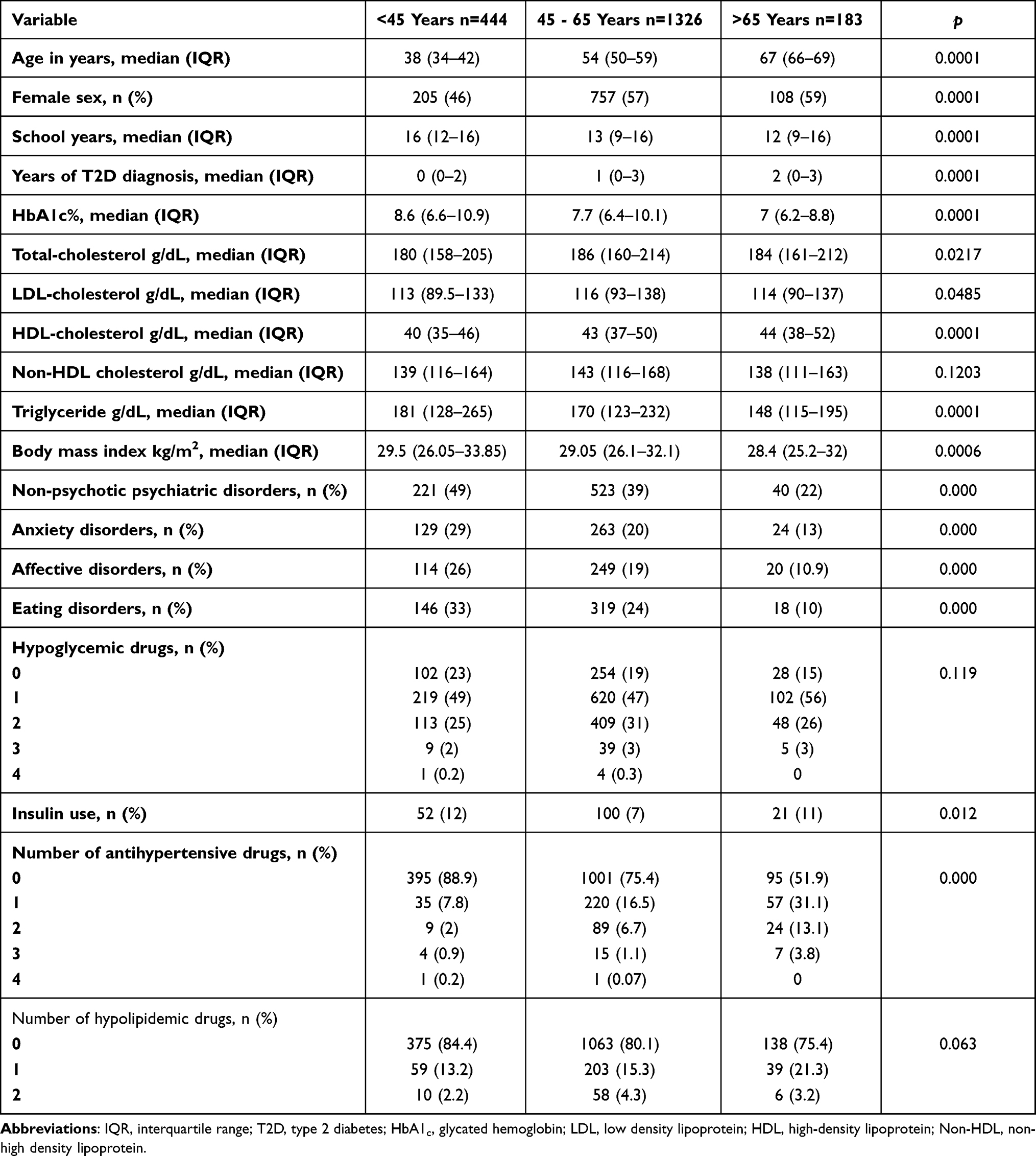 |
Table 4 Comparative Analysis of Sociodemographic, Clinical Features, Metabolic Status, and Psychiatric Disorders of Patients with Less Than 45, 45 to 65, and More Than 65 Years |
The multivariate logistic regression analysis reported differences in the odds of presenting psychiatric disorders for each age group as shown in Table 5. For the younger group, the results reported an association of NPPD with age, female sex, PPH, and BMI. Age was reported as a risk factor.
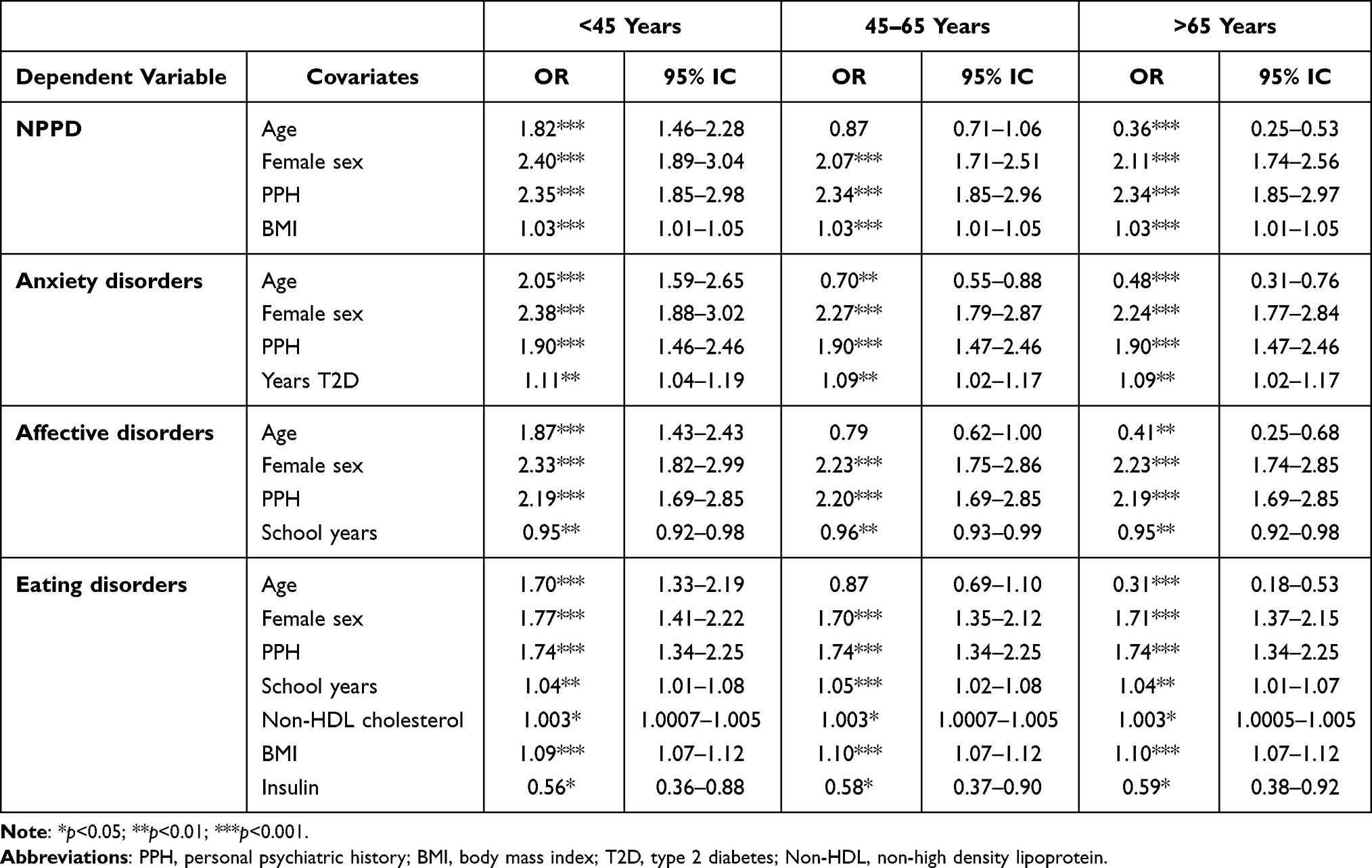 |
Table 5 Multivariate Logistic Regression Analyses for the Presence of Any Non-Psychotic Psychiatric Disorders, Anxiety, Affective and Eating Disorders of Patients with Less Than 45, 45 to 65, and More Than 65 Years |
The analysis for the second group showed no association of age with the presence of any NPPD (p=0.177), whereas the rest of the covariates remained significant. The model for the older group also reported an association of all the analyzed covariates with NPPD, but age was a protective factor in this group.
Female sex, age, PPH, and years of T2D diagnosis were associated with AXD in the three age models. Nonetheless, age was reported as a risk factor for AXD in the group younger than 45 years and as a protective factor for subjects in the two older groups.
We found an association of AFD with female sex, PPH, and years of formal education in all three groups. Age was reported as a risk factor in patients younger than 45 years, whereas for subjects older than 65 years was a protective factor. There was no association of age with AFD in the group of age 45 to 65 (p=0.056).
Finally, ED was associated with female sex, personal psychiatric history, years of formal education, non-HDL cholesterol, BMI, and insulin use in all the groups. Age was found as a risk factor for ED in subjects younger than 45 years, and as a protective factor in patients older than 65 years. We found no association between age and ED in subjects from 45 to 65 years (p=0.264).
Discussion
The present study analyzed the clinical and metabolic characteristics of subjects who suffer any NPPD as well as the description of the groups with AXD, AFD, and ED in patients with less than 5 years of T2D diagnosis. Previous studies reported a high prevalence of NPPD in patients with T2D with a heterogenic duration of time since diagnosis.15,26 There is scarce information about the metabolic status and integrative clinical features of each of the main psychiatric comorbidities in patients with T2D with recent diagnoses. The main findings of this study are the identification of risk factors and metabolic profiles associated with the presence of any NPPD, AXD, AFD, and ED.
In our sample, 40% had some non-psychotic psychiatric disorder, being a similar number of previous reports of psychiatric comorbidity in different populations with diabetes, and higher than the reported in newly diagnosed T2D and populations without diabetes. Weyerer et al27 reported a prevalence of any psychiatric condition of 43% using CIE-8 criteria in patients with diabetes older than 65 years from Munich. De Ornelas et al2 found psychiatric comorbidity in 42.5% of 200 Brazilian patients with type 1 and 2 diabetes included in the study. Nonetheless, compared with data of newly diagnosed patients with type 2 diabetes in a Danish cohort,28 our prevalence of NPPD is almost twice the reported. This disparity might be associated with the methods of measuring since the reports included in the Danish cohort are based on discharge and treatment codes from the system of health, which may not include subjects who are not under treatment or who are not diagnosed. In contrast, our study evaluated intentionally the presence of psychiatric conditions with a structured interview, which allow us to detect psychiatric conditions in all subjects who attended our center. In non-T2D populations, Amruth et al29 reported a prevalence of the psychiatric disorder in 32.5% of subjects with epilepsy, whereas Winkler et al30 recently found a psychiatric condition in 32.94% of otherwise healthy adults during the second wave of COVID-19 pandemic. So far, the reports on Mexican samples with T2D had focused on depressive disorder. This is the first study to report a prevalence of various non-psychotic psychiatric disorders in our population using a structured interview and psychiatric evaluation, which are the gold standard for the diagnosis of psychiatric disorders.
The main conditions that we detected were categorized as anxiety, affective and eating disorders. AXD were present in one-fifth of our patients, and generalized anxiety disorder was the most frequent diagnosis in this group. Other studies reported a higher prevalence of anxiety symptoms in the Mexican population using different tools.15,16 Tovilla et al15 reported that 55.1% of 820 patients had anxiety and identified a high association with complications in diabetes. Martínez-Hernández et al16 reported a prevalence of anxiety symptoms of 48.48%. However, there are no previous reports on the prevalence of other anxiety disorders in the Mexican population with T2D. This paper is the first publication to provide a prevalence of specific anxiety disorders in this population.
In our sample, one of the five patients had an AFD; among those, the most prevalent was major depressive disorder, which was present in 15% of subjects. These results are discordant with other studies in Mexican populations that reported depressive symptoms in 34–63%15,16 using non-diagnostic screening tools. Our numbers agree with the findings of Castro-Aké et al7 who conducted a study on a sample of 186 T2D patients using also the MINI International Neuropsychiatric Interview for the diagnosis of major depressive disorder. They identified a prevalence of major depression of 10.8% in patients with less than 5 years of diabetes diagnosis and 16.6% in patients with more than 5 years. These disparities between the prevalence of depressive symptoms and depressive disorder are a common finding while comparing the use of screening tools with diagnostic structured interviews or psychiatric clinical assessment.
We report a higher proportion of ED in comparison to the general population in Latin America reported at 3.5%.31 Two studies on Brazilian samples,32,33 identified prevalence using Structured Clinical Interview for DM-IV-TR and Binge Eating Scale in patients with more than 5 years of diabetes. They reported 20% of eating behavior alterations, being BED with the highest prevalence (10%) and eating disorders not otherwise specified (5.7%). Other studies focused on BED reported a prevalence from 5% to 25.6%.34 A study on the Mexican population utilized the EFRATA tool (Escala de Factores de Riesgo Asociados a Trastornos Alimentarios, as an acronym in Spanish), and identified higher values of emotional eating in patients with diabetes.35 In our study, the most prevalent ED was eating disorders not otherwise specified (emotional eating). We also found a lower prevalence of BED; nonetheless, it is still higher than the general population of the American continent (4.6%).36
Three factors were significant in all the regression models that we constructed. First, female sex was a risk factor for the presence of any NPPD, AXD, AFD, and ED. This information is consistent with previous data about the higher prevalence of depressive, anxiety, and eating disorders in females compared with males in the general population. Several studies,3,37–39 including a collaborative study in 14 countries reported that among T2D patients, women had increased odds of major depressive disorder than men (OR=1.96).37 Also, a systematic literature review identified a different prevalence of BED according to sex (0–9.8% for women and 0–0.5%for men).36
The second risk factor associated with all NPPD groups was younger age. In contrast with previous psychiatric research,40 our population with psychopathology was younger. The regression models for NPPD, anxiety, affective and eating disorders reported age as a protective factor. This information is discordant with several reports where a higher risk for mental health conditions is associated with age in patients without T2D.5,17 According to our age analysis, patients younger than 45 years presented the worst metabolic parameters and higher prevalence of psychiatric conditions compared with the other two age groups. On the multivariate logistic analysis, it was evident that patients with less than 45 years had higher odds of presenting any NPPD, anxiety, affective, and eating disorders than subjects of other ages. Data for patients between 45 and 65 years was heterogenic since there was no association between this range of age with the presence of NPPD or AFD. This group had decreased odds of anxiety and eating behavior disorders. Subjects older than 65 years reported better metabolic status and lesser odds of presenting any NPPD, anxiety, affective, and eating behavior disorders compared with younger subjects. Our evidence suggests that risk factors for NPPD in patients with a recent diagnosis of T2D differ from what has been reported in other samples. There are different possible explanations for this phenomenon. First, subjects younger than 45 years are likely to be early-onset T2D patients that have been associated with higher rates of diabetes-related complications, increased mortality, and worst metabolic control.41 This is in line with our results where younger patients reported the worst metabolic parameters. Glycemic and metabolic poor control in T2D has been linked with a chronic low inflammatory process that involves the activation of pro-inflammatory molecules, such as interleukins and TNFα.42 These same molecules had been implicated in the pathophysiology of psychiatric disorders with several meta-analyses reporting higher levels of proinflammatory molecules in association with affective, anxiety, and eating disorders.43–45 Therefore, the subjacent inflammatory process in our early-onset T2D patients that exhibit poor metabolic control might link to the increased odds of NPPD in patients younger than 45 years.
Also, premature aging in subjects with psychiatric disorders has been described in clinical and biological research.46 Several studies reported a reduction of life expectancy of 8–10 years in patients with psychiatric disorders compared with controls.47–49 This phenomenon had been associated with an increased risk of cardiovascular and metabolic morbidity and telomere shortening.46,49 Meta-analyses data reported shorter telomeres in psychiatric populations compared with controls.50 Different mechanisms have been implicated in this situation including oxidative stress and inflammatory pathways associated with psychiatric conditions. Telomere shortening is linked with dysregulated immune function, cancer, diabetes, and cardiovascular disease.50 Therefore, patients with psychiatric conditions might experience an earlier presentation of comorbidities such as T2D.
Another important subject to address while discussing our results is the alterations in brain metabolism and insulin resistance in the central nervous system (CNS). Younger ages of T2D onset had been associated with severe insulin resistance51,52 which may impact brain activity.53 Several studies had reported changes in neural and glial cell function54–56 in association with insulin resistance, which include changes in dopamine signaling,57 hippocampal synaptic plasticity,58 blood–brain barrier function,59 and mitochondrial function,60 to mention a few findings. These data might translate to clinical practice in the frequently observed cognitive and behavioral alterations in patients with insulin resistance.53,58,61 Researchers had highlighted the disruption of the mesocorticolimbic circuit in subjects with insulin resistance62 since this dopaminergic pathway is involved in the regulation of food intake,60 mood, and behavior,54,61 which might explain the high prevalence of psychiatric disorders in T2D.62,63 We believe this data might also explain part of our findings in young subjects. Nonetheless, more research is needed in the field.
The third risk factor associated with all NPPD groups was personal psychiatric history. We identified two kinds of antecedents: first as a previous episode of a psychiatric disorder, and second as another psychiatric disorder. Other studies included mild anxiety or depressive symptoms as risk factors associated with mental illness in patients without T2D.64 Inversely, association of psychiatric disorders as risk factor for type 2 diabetes has been identified, Lindekilde et al9 conducted an overview review and reported depression (RR = 1.18 [95% IC 1.12–1.24] to RR = 1.60 [95% IC 1.37–1.88]), anxiety (OR = 1.47 [95% IC 1.23–1.75]) and insomnia (RR = 1.55 [95% IC 1.21–1.99] to RR = 1.74 [95% IC 1.30–2.34]) as risk factors for T2D.
For metabolic parameters, we found differences between NPPD vs non NPPD in non-HDL cholesterol, triglycerides, and BMI. On the multivariate analysis, BMI remained significant. Anxiety and affective disorders were not associated with metabolic parameters following multivariate analysis. Eating disorders reported an association with non-HDL cholesterol and BMI. We did not identify a difference in HbA1c, which can be explained by a recent diagnosis and early medical attention, the absence of T2D-related complications, and their impact on glycemic control. Regarding the characteristics of T2D, we report an association of years of T2D with AXD. The use of insulin was a protective factor for eating disorders in our sample, which might be in line with better metabolic control and less diabetes-related hyperphagia; as well as the modulation of food intake exerted by insulin.53
We acknowledge some limitations in our study such as the lack of a control group, the lack of inclusion of drug users, and the exclusion of patients with psychotic disorders; these difficult the extrapolation of our results to the population with these characteristics; finally, we were unable to control recall bias. The strengths of this study are a big sample size which allows a methodological quality through control of selection, measurement, and interview bias.
Conclusion
Younger age, female sex, and previous psychiatric diagnosis are the main risk factors for NPPD. Patients younger than 45 years are a population with increased odds of NPPD and poor metabolic control. The presence of NPPD at early-onset of T2D highlights the necessity of mental health attention to reduce the total disability-adjusted life years, improve quality of life, and decrease complications and mortality.
Acknowledgments
CAIPaDi study group: Denise Arcila-Martínez, Rodrigo Arizmendi-Rodríguez, Michelle Díaz-Pineda, Humberto Del Valle-Ramírez, Arturo Flores García, Fernanda Garnica-Carrillo, Eduardo González-Flores, Mariana Granados-Arcos, Arely Hernández-Jasso, Diana Hernández-Juárez, Héctor Infanzón-Talango, Victoria Landa-Anell, Claudia Lechuga-Fonseca, Marco Antonio Melgarejo-Hernández, Angélica Palacios-Vargas, Liliana Pérez-Peralta, Sofía Ríos-Villavicencio, David Rivera de la Parra, Francis Rojas-Torres, Sandra Sainos-Muñoz, María Luisa Velasco-Pérez, Héctor Velázquez-Jurado, Andrea Villegas-Narvaez, Luz Elena Urbina-Arronte, Verónica Zurita-Cortés, Carlos A. Aguilar-Salinas, Francisco J Gómez-Pérez, and David Kershenobich-Stalnikowitz. Others: Oswaldo Briseño-González, Eder Patiño-Rivera, and Victor Trejo-Terreros.
Disclosure
The CAIPaDi program has received grants from Astra Zeneca, Fundación Conde de Valenciana, Novartis, Consejo Nacional de Ciencia y Tecnología (“Proyectos de Desarrollo Científico para Atender Problemas Nacionales 2013 project 214718”), Nutrición Médica y Tecnología, NovoNordisk, Boehringer Ingelheim, Dirección General de Calidad y Educación en Salud, Eli Lilly, Merck Serono, MSD, Silanes, Chinoin and Carlos Slim Health Institute. There are no other potential conflicts of interest relevant to this article.
References
1. Balhara YP. Diabetes and psychiatric disorders. Indian J Endocrinol Metab. 2011;15(4):274. doi:10.4103/2230-8210.85579
2. Claudia A, de Ornelas Maia C, de Azevedo Braga A, et al. Prevalence of psychiatric disorders in patients with diabetes types 1 and 2. Comprehensive psychiatry.2012. doi:10.1016/j.comppsych.2012.03.011
3. Lloyd CE, Nouwen A, Sartorius N, et al. Prevalence and correlates of depressive disorders in people with type 2 diabetes: results from the International Prevalence and Treatment of Diabetes and Depression (INTERPRET-DD) study, a collaborative study carried out in 14 countries. Diabet Med. 2018;35(6):760–769. doi:10.1111/DME.13611
4. Garduño-Espinosa J, Téllez-Zenteno JF, Hernãndez-Ronquillo L. Frecuencia de depresión en pacientes con diabetes mellitus tipo 2 [Frequency of depression in patients with diabetes mellitus type 2]. Rev Invest Clin. 1998;50(4):287–291. Spanish.
5. Naicker K, Johnson JA, Skogen JC, et al. Type 2 diabetes and comorbid symptoms of depression and anxiety: longitudinal associations with mortality risk. Diabetes Care. 2017;40(3):352–358. doi:10.2337/dc16-2018
6. Whitworth SR, Bruce DG, Starkstein SE, Davis WA, Davis TME, Bucks RS. Lifetime depression and anxiety increase prevalent psychological symptoms and worsen glycemic control in type 2 diabetes: the Fremantle diabetes study phase II. Diabetes Res Clin Pract. 2016;122:190–197. doi:10.1016/j.diabres.2016.10.023
7. Castro-Aké GA, Tovar-Espinosa JA, Mendoza-Cruz U. Trastorno depresivo y control glucémico en el paciente con diabetes mellitus 2 [Depressive disorder and glycemic control in the patient with diabetes mellitus 2]. Rev Med Inst Mex Seguro Soc. 2009;47(4):377–382. Spanish.
8. Ciechanowski PS, Katon WJ, Russo JE Depression and diabetes impact of depressive symptoms on adherence, function, and costs. Available from: http://archinte.jamanetwork.com/.
9. Lindekilde N, Rutters F, Erik Henriksen J, et al. Psychiatric disorders as risk factors for type 2 diabetes: an umbrella review of systematic reviews with and without meta-analyses. Diabetes Res Clin Pract. 2021;176:108855. doi:10.1016/j.diabres.2021.108855
10. Sevilla-González M, Del R, Quintana-Mendoza BM, Aguilar-Salinas CA. Interaction between depression, obesity, and type 2 diabetes: a complex picture. Arch Med Res. 2017;48(7):582–591. doi:10.1016/j.arcmed.2018.02.004
11. Calkin CV, Gardner DM, Ransom T, Alda M. The relationship between bipolar disorder and type 2 diabetes: more than just co-morbid disorders. Ann Med. 2013;45(2):171–181. doi:10.3109/07853890.2012.687835
12. Sun H, Saeedi P, Karuranga S, et al. IDF diabetes atlas: global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res Clin Pract. 2021;183:109119. doi:10.1016/j.diabres.2021.109119
13. Shamah-Levy T, Vielma-Orozco E, Heredia-Hernández O, et al. Encuesta Nacional de Salud y Nutrición 2018–19: Resultados Nacionales [National survey of health and nutrition 2018-19: National results]. Francisco R, Ana TV, Jessica GS, eds.. Instituto Nacional de Salud Pública; 2020. Spanish.
14. Institute for Health Metrics and Evaluation. Global burden of disease compare. GBD 2019 Cause and Risk Summaries; 2019. Available from: https://vizhub.healthdata.org/gbd-compare/.
15. Tovilla-Zárate C, Juárez-Rojop I, Jimenez Y, et al. Prevalence of anxiety and depression among outpatients with type 2 diabetes in the Mexican population. PLoS One. 2012;7(5):e36887. doi:10.1371/JOURNAL.PONE.0036887
16. Martínez Hernández F, Tovilla Zárate CA, López Narváez L, et al. Prevalencia y gravedad de la depresión y la ansiedad en pacientes con obesidad y diabetes de tipo 2: estudio en población de Tabasco, México [Prevalence and gravity of depression and anxiety in patients with obesity and type 2 diabetes: a study in the population of Tabasco, Mexico]. Gac Med Mex. 2014;150(Suppl 1):101–106. Spanish.
17. Mendenhall E, Norris SA, Shidhaye R, Prabhakaran D. Depression and type 2 diabetes in low- and middle-income countries: a systematic review. Diabetes Res Clin Pract. 2014;103(2):276–285. doi:10.1016/j.diabres.2014.01.001
18. Laiteerapong N, Ham SA, Gao Y, et al. The legacy effect in type 2 diabetes: impact of early glycemic control on future complications (the diabetes & aging study). Diabetes Care. 2019;42(3):416–426. doi:10.2337/dc17-1144
19. Brundel M, Kappelle LJ, Biessels GJ. Brain imaging in type 2 diabetes. Eur Neuropsychopharmacol. 2014;24(12):1967–1981. doi:10.1016/J.EURONEURO.2014.01.023
20. Hernández-Jiménez S, García-Ulloa AC, Bello-Chavolla OY, Aguilar-Salinas CA, Kershenobich-Stalnikowitz D. Long-term effectiveness of a type 2 diabetes comprehensive care program. The CAIPaDi model. Diabetes Res Clin Pract. 2019;151:128–137. doi:10.1016/j.diabres.2019.04.009
21. Hernandez-Jimenez S, Garcia-Ulloa C, Mehta R, Aguilar-Salinas C, Kershenobich-Stalnikowitz D. Innovative models for the empowerment of patients with type 2 diabetes: the CAIPaDi program. Recent Pat Endocr Metab Immune Drug Discov. 2014;8(3):202–209. doi:10.2174/1872214808999141110155515
22. American Diabetes Association. 2. Classification and diagnosis of diabetes: standards of medical care in diabetes-2021. Diabetes Care. 2021;44:S15–S33. doi:10.2337/dc21-S002
23. Ferrando L, Bobes J, Gibert J, Soto M, Soto O. MINI Entrevista Neuropsiquiátrica Internacional [MINI International Neuropsychiatric Interview, MINI]. Detección Orientación Diagnóstica. 2000;1–25. Spanish.
24. Lecrubier Y, Sheehan DV, Weiller E, et al. The Mini International Neuropsychiatric Interview (MINI). A short diagnostic structured interview: reliability and validity according to the CIDI. Eur Psychiatry. 1997;12(5):224–231. doi:10.1016/S0924-9338(97)83296-8
25. American Psychiatric Association. Diagnostic and statistical manual of mental disorders. Am Psychiatric Associ. 2013. doi:10.1176/appi.books.9780890425596
26. Gómez-Peralta TG, González-Castro TB, Fresan A, et al. Risk factors and prevalence of suicide attempt in patients with type 2 diabetes in the Mexican population. Int J Environ Res Public Health. 2018;15(6):1198. doi:10.3390/ijerph15061198
27. Weyerer S, Hewer W, Pfeifer-Kurda M, Dilling H. Psychiatric disorders and diabetes-results from a community study. J Psychosom Res. 1989;33(S):633–640. doi:10.1016/0022-3999(89)90070-6
28. Christensen DH, Nicolaisen SK, Berencsi K, et al. Danish Centre for Strategic Research in type 2 diabetes (DD2) project cohort of newly diagnosed patients with type 2 diabetes: a cohort profile. BMJ Open. 2018;8:17273. doi:10.1136/bmjopen-2017-017273
29. Amruth G, Praveen-kumar S, Nataraju B, Kasturi P. Study of psychiatric comorbidities in epilepsy by using the mini international neuropsychiatric interview. Epilepsy Behav. 2014;33:94–100. doi:10.1016/J.YEBEH.2014.02.001
30. Winkler P, Mohrova Z, Mlada K, et al. Prevalence of current mental disorders before and during the second wave of COVID-19 pandemic: an analysis of repeated nationwide cross-sectional surveys. J Psychiatr Res. 2021;139:167. doi:10.1016/J.JPSYCHIRES.2021.05.032
31. Kolar DR, Rodriguez DLM, Chams MM, Hoek HW. Epidemiology of eating disorders in Latin America: a systematic review and meta-analysis. Curr Opin Psychiatry. 2016;29(6):363–371. doi:10.1097/YCO.0000000000000279
32. Papelbaum M, Appolinário JC, Moreira R, et al. Prevalence of eating disorders and psychiatric comorbidity in a clinical sample of type 2 diabetes mellitus patients. Revista Brasileira de Psiquiatria. 2005;27(2):135–138. doi:10.1590/S1516-44462005000200012
33. Papelbaum M, de Oliveira Moreira R, Coutinho WF, et al. Does binge-eating matter for glycemic control in type 2 diabetes patients? J Eat Disord. 2019;7(1). doi:10.1186/s40337-019-0260-4
34. Winston AP. Eating Disorders and Diabetes. Curr Diab Rep. 2020;20(8). doi:10.1007/s11892-020-01320-0
35. Saucedo-Molina TDJ, Villalon L, Zaragoza-Cortes J, León Hernández R, Calderón Ramos Z. Disordered eating behaviors in Mexican patients with and without type 2 diabetes mellitus. Rev Mex de Trastor Aliment. 2015;6(1):13–21. doi:10.1016/j.rmta.2015.05.001
36. Galmiche M, Déchelotte P, Lambert G, Tavolacci MP. Prevalence of eating disorders over the 2000–2018 period: a systematic literature review. Am J Clin Nutr. 2019;109(5):1402–1413. doi:10.1093/ajcn/nqy342
37. Lloyd CE, Sartorius N, Ahmed HU, et al. Factors associated with the onset of major depressive disorder in adults with type 2 diabetes living in 12 different countries: results from the INTERPRET-DD prospective study. Epidemiol Psychiatr Sci. 2020;29. doi:10.1017/S2045796020000438
38. Goldney RD, Phillips PJ, Laura MA, Fisher J, Hons BA, Wilson DH Diabetes, depression, and quality of life a population study; 2004.
39. Téllez-Zenteno JF, Cardiel MH. Risk factors associated with depression in patients with type 2 diabetes mellitus. Arch Med Res. 2002;33(1):53–60. doi:10.1016/S0188-4409(01
40. Kessler RC, Bromet EJ. The epidemiology of depression across cultures. Annu Rev Public Health. 2013;34:119. doi:10.1146/ANNUREV-PUBLHEALTH-031912-114409
41. García-García E, Aguilar-Salinas CA, Tusié-Luna T, Rull-Rodrigo JA. Early-onset type 2 diabetes in Mexico. IMAJ. 2002;4:444–448.
42. Furman D, Campisi J, Verdin E, et al. Chronic inflammation in the etiology of disease across the life span. Nat Med. 2019;25(12):1822–1832. doi:10.1038/s41591-019-0675-0
43. Iwata M, Ota KT, Duman RS. The inflammasome: pathways linking psychological stress, depression, and systemic illnesses. Brain Behav Immun. 2013;31:105–114. doi:10.1016/j.bbi.2012.12.008
44. Abelaira HM, Réus GZ, Petronilho F, Barichello T, Quevedo J. Neuroimmunomodulation in depression: a review of inflammatory cytokines involved in this process. Neurochem Res. 2014;39(9):1634–1639. doi:10.1007/s11064-014-1372-5
45. Réus GZ, Fries GR, Stertz L, et al. The role of inflammation and microglial activation in the pathophysiology of psychiatric disorders. Neuroscience. 2015;300:141–154. doi:10.1016/j.neuroscience.2015.05.018
46. Kiecolt-Glaser JK, Wilson SJ. Psychiatric disorders, morbidity, and mortality: tracing mechanistic pathways to accelerated aging HHS public access author manuscript. Psychosom Med. 2016;78(7):772–775. doi:10.1097/PSY.0000000000000373
47. Jf H, Miles J, Walters K, King M. A systematic review and meta-analysis of premature mortality in bipolar affective disorder. Acta Psychiatr Scand. 2015:417–425. doi:10.1111/acps.12408
48. Keinänen J, Mantere O, Markkula N, et al. Mortality in people with psychotic disorders in Finland: a population-based 13-year follow-up study. Schizophr Res. 2018;192:113–118. doi:10.1016/j.schres.2017.04.048
49. Correll CU, Solmi M, Veronese N, et al. Prevalence, incidence and mortality from cardiovascular disease in patients with pooled and specific severe mental illness: a large-scale meta-analysis of 3,211,768 patients and 113,383,368 controls. World Psychiatry. 2017;16(2):163–180. doi:10.1002/wps.20420
50. Monroy-Jaramillo N, Dyukova E, Walss-Bass C. Psychiatry Telomere length in psychiatric disorders: is it more than an ageing marker? Telomere length in psychiatric disorders: is it more than an ageing marker? World J Biol Psychiatry. 2018;19(S2):S2–S20. doi:10.1080/15622975.2016.1273550
51. Burns N, Finucane FM, Hatunic M, et al. Early-onset type 2 diabetes in obese white subjects is characterised by a marked defect in beta cell insulin secretion, severe insulin resistance and a lack of response to aerobic exercise training. Diabetologia. 2007;50:1500–1508. doi:10.1007/s00125-007-0655-7
52. Lyssenko V, Jonsson A, Almgren P, et al. Clinical risk factors, DNA variants, and the development of type 2 diabetes. N Engl J Med. 2008;359(21):2220–2232. doi:10.1056/NEJMoa0801869
53. Kleinridders A, Ferris HA, Cai W, Kahn CR. Insulin action in brain regulates systemic metabolism and brain function. Diabetes. 2014;63(7):2232–2243. doi:10.2337/DB14-0568
54. Cai W, Xue C, Sakaguchi M, et al. Insulin regulates astrocyte gliotransmission and modulates behavior. J Clin Invest. 2018;128(7):2914–2926. doi:10.1172/JCI99366
55. Evans MC, Rizwan MZ, Anderson GM. Insulin action on GABA neurons is a critical regulator of energy balance but not fertility in mice. Endocrinology. 2014;155(11):4368–4379. doi:10.1210/EN.2014-1412
56. García-Cáceres C, Quarta C, Varela L, et al. Astrocytic insulin signaling couples brain glucose uptake with nutrient availability. Cell. 2016;166(4):867–880. doi:10.1016/J.CELL.2016.07.028
57. Zhang X, van den Pol AN. Dopamine/Tyrosine Hydroxylase neurons of the hypothalamic arcuate nucleus release GABA, communicate with dopaminergic and other arcuate neurons, and respond to dynorphin, met-enkephalin, and oxytocin. J Neurosci. 2015;35(45):14966–14982. doi:10.1523/JNEUROSCI.0293-15.2015
58. Biessels GJ, Reagan LP. Hippocampal insulin resistance and cognitive dysfunction. Nat Rev Neurosci. 2015;16(11):660–671. doi:10.1038/NRN4019
59. Rhea EM, Banks WA. Role of the blood-brain barrier in central nervous system insulin resistance. Front Neurosci. 2019;13(JUN). doi:10.3389/FNINS.2019.00521
60. Wardelmann K, Blümel S, Rath M, et al. Insulin action in the brain regulates mitochondrial stress responses and reduces diet-induced weight gain. Mol Metab. 2019;21:68–81. doi:10.1016/J.MOLMET.2019.01.001
61. Kleinridders A, Cai W, Cappellucci L, et al. Insulin resistance in brain alters dopamine turnover and causes behavioral disorders. Proc Natl Acad Sci USA. 2015;112(11):3463–3468. doi:10.1073/PNAS.1500877112
62. Kullmann S, Kleinridders A, Small DM, et al. Central nervous pathways of insulin action in the control of metabolism and food intake. Lancet Diabetes Endocrinol. 2020;8:524–534. doi:10.1016/S2213-8587(20)30113-3
63. Milstein JL, Ferris HA. The brain as an insulin-sensitive metabolic organ. Mol Metab. 2021;52:101234. doi:10.1016/J.MOLMET.2021.101234
64. Markkula N, Suvisaari J. Prevalence, risk factors and prognosis of depressive disorders. Duodecim. 2017. 133(3):275–282.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.