Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Community Pharmacists’ Role in Palliative Care: Evaluating Knowledge, Attitudes, Practices, and Perceived Barriers in the UAE
Authors Jarab AS ![]() , Al-Qerem W
, Al-Qerem W ![]() , Elsherif R
, Elsherif R ![]() , Al Meslamani AZ, Al Hamarneh YN, Khdour M
, Al Meslamani AZ, Al Hamarneh YN, Khdour M ![]() , Beiram R, Aburuz S
, Beiram R, Aburuz S
Received 11 November 2025
Accepted for publication 5 February 2026
Published 24 February 2026 Volume 2026:19 580863
DOI https://doi.org/10.2147/JMDH.S580863
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Tilakavati Karupaiah
Anan S Jarab,1 Walid Al-Qerem,2 Rahma Elsherif,3 Ahmad Z Al Meslamani,3 Yazid N Al Hamarneh,4 Maher Khdour,5 Rami Beiram,6 Salahdein Aburuz6
1Department of Clinical Pharmacy, Faculty of Pharmacy, Jordan University of Science and Technology, Irbid, 22110, Jordan; 2Department of Pharmacy, Faculty of Pharmacy, Al-Zaytoonah University of Jordan, Amman, 11733, Jordan; 3College of Pharmacy, Al Ain University, Abu Dhabi, United Arab Emirates; 4Department of Pharmacology, Faculty of Medicine and Dentistry, University of Alberta, Edmonton, Canada; 5College of Pharmacy, Al-Quds University, Jerusalem, Palestine; 6Department of Pharmacology and Therapeutics, College of Medicine and Health Sciences, United Arab Emirates University, Al Ain, United Arab Emirates
Correspondence: Salahdein Aburuz, Department of Pharmacology and Therapeutics, College of Medicine and Health Sciences, United Arab Emirates University, Al Ain, United Arab Emirates, Email [email protected]
Background: Pharmacists are well-positioned to enhance medication management and support patients; however, their participation in palliative care in the UAE remains limited due to insufficient training, unclear professional roles, and organizational constraints. Addressing these issues is vital to enable pharmacists to contribute to comprehensive, patient-centred care and improved health outcomes.
Aim: To assess the knowledge, attitudes, and practices of community pharmacists in the UAE toward palliative care, and to identify perceived barriers and factors associated with suboptimal practice.
Methods: A cross-sectional online survey was conducted among 431 pharmacists using convenience sampling. A validated, self-administered questionnaire assessed demographics, knowledge (true/false/I do not know), attitudes and practices (5-point Likert scales), and perceived barriers. Content validity was confirmed through expert review, and reliability was assessed using Cronbach’s alpha. Quantile regression identified factors influencing palliative care practices.
Results: Among 431 respondents, the median (IQR) knowledge score was 4 (3– 5) out of 13, with fewer than half answering any knowledge item correctly. Attitude and practice scores showed scope for improvement, with median (IQR) values of 45 (41– 48) out of 60 and 41 (37– 44) out of 55, respectively. Only 10% conducted home visits, while 16% offered pain management advice. Common activities included medication monitoring (38.3%) and ensuring access to essential medicines (36%). Higher attitude scores (β = 0.375; 95% CI: 0.283– 0.467) and older age (β = 0.122; 95% CI: 0.009– 0.235) were associated with better practices. The main barriers were lack of training (53.4%) and limited public awareness (50.1%).
Conclusion: Despite positive attitudes, pharmacists demonstrate limited knowledge and engagement in palliative care. Targeted education, integration of palliative care into pharmacy curricula, and enhanced institutional and public support are essential to strengthen pharmacists’ roles in patient-centred care in the UAE.
Keywords: palliative care, community pharmacists, multidisciplinary care, knowledge, attitudes, practices, barriers, UAE
Introduction
Palliative care has increasingly become an integral component of modern health care, focusing on improving the quality of life of patients with serious and life-limiting diseases through comprehensive management of symptoms, psychosocial support and interprofessional working.1 This dimension of care goes beyond the traditional concern for curing disease to one of holistic care that attends to the physical, psychological, social, and spiritual needs of patients and their families.2,3 The core purpose is the alleviation of the suffering and promoting comfort regardless of disease stage or prognosis, therefore supplementing curative or life-sustaining treatment but not substituting.2 Globally, an estimated 40 million people require palliative care each year, however, fewer than 14% receive it, reflecting significant gaps in both service provision and professional knowledge.1 The greatest need for palliative care exists in low - and middle-income countries, which account for 80% of the global demand but often lack adequate resources and trained professionals.4
Palliative care is provided across various settings, from patients’ homes to hospices and specialized hospital units, which expands the scope of responsibilities for pharmacists.5 As essential members of multidisciplinary teams, pharmacists contribute to quality assurance, direct patient care, and comprehensive medication management.5 They play a central role in tailoring medication regimens to alleviate symptoms such as pain, nausea, and dyspnea, while minimizing the risks associated with polypharmacy, including adverse effects and drug interactions.5 Pharmacists can take on a preventive role by conducting medication reviews, reconciling prescriptions during care transitions, and identifying potential risks such as allergies, contraindications, and dosing errors.6
Evidence from international data suggests that including pharmacists into palliative care teams improves symptom management, promotes safer opioid use, reduces medication-related difficulties, and improves healthcare coordination.5 Global comparisons highlight pharmacists as critical members of interdisciplinary palliative care teams, especially given the heavy dependence on tailored and frequently high-risk pharmaceutical regimens in end-of-life treatment.5 These criteria demonstrate the necessity of extending pharmacist-led services to improve palliative care outcomes.
In the United Arab Emirates (UAE), national data highlight a growing demand for palliative care, driven by aging, multicultural population, and rising burden of cancer and chronic diseases,7 with palliative care services legally recognized since 2007. Nonetheless, palliative care remains largely hospital-based in major cities, with limited integration into primary care and community settings. The role of community pharmacists in palliative care is still emerging and inconsistently implemented across healthcare settings.
Recent health system reforms and workforce development initiatives in the Gulf region have expanded pharmacists’ clinical and patient-facing responsibilities, particularly in chronic disease management, medication review, and collaborative care.5 However, their involvement in palliative care remains limited due to gaps in standardized training, regulatory constraints, cultural perceptions, and minimal exposure to international palliative care guidelines.7,8 Studies have identified deficiencies in pharmacists’ competencies, especially in opioid management, including dosing, titration, and side effect monitoring, as well as challenges in managing complex non-pain symptoms and communicating effectively with patients and families about end-of-life care and treatment goals.6,9 These limitations can reduce pharmacists’ confidence and hinder their participation in multidisciplinary palliative care teams.8,10
Evaluating pharmacists’ knowledge, attitudes, practices, and perceived barriers is therefore essential, as these factors directly influence clinical judgment, professional competence, and the ability to deliver safe, patient-centered palliative care. This study aims to assess pharmacists’ knowledge and attitudes toward palliative care, examine the frequency with which they perform palliative care–related practices, explore factors influencing their engagement, and identify barriers to providing optimal care. Findings from this research are intended to guide strategies that strengthen the role of community pharmacists in palliative care within the UAE and inform best practices in similar healthcare settings.
Materials and Methods
Study Design and Participants
This study followed a cross-sectional design and was conducted between March and September 2024. It involved licensed community pharmacists working in different regions across the UAE. Data was gathered using a structured, self-administered questionnaire that had undergone prior validation. The survey was distributed through Google Forms, and research pharmacists, who are licensed pharmacists with training and experience in academic or clinical research, circulated the link within their residential areas using a convenience sampling method. Each research pharmacist was based in a different geographic region, allowing for wider coverage across both urban and rural settings. They were instructed to approach a diverse mix of pharmacy types, including independent and chain pharmacies, to ensure representation across various practice environments. To be included in the study, participants had to be graduates of universities accredited by the UAE Ministry of Higher Education and registered as community pharmacists with the UAE Ministry of Health. Anonymity was maintained throughout the survey to encourage honest responses and minimize bias. The survey began with an introductory section outlining the study’s purpose and assuring participants of the confidentiality and voluntary nature of their participation. Before proceeding with the questionnaire, participants were required to provide informed consent by selecting a confirmation statement: “I have read the study information, and I agree to participate.” The questionnaire took approximately 10 minutes to complete.
Study Instrument
The questionnaire was developed based on a review of relevant, previously published studies.9,11,12 The first section of the survey collected sociodemographic and job-related data, including age, gender, workplace location, highest academic qualification, pharmacy type, job role, years of experience, average number of prescriptions dispensed daily, number of patients served per day, average consultation time per patient, and sources of drug information. The second section assessed pharmacists’ knowledge of palliative care using a three-point scale: true, false, or “I do not know.” The third section evaluated attitudes toward palliative care and pharmacists’ roles in its management using a 5-point Likert scale ranging from strongly disagree (1) to strongly agree (5). The fourth section examined the frequency of pharmacists’ engagement in palliative care practices using another 5-point Likert scale, from never (1) to always (5). In the final section, respondents were asked to identify perceived barriers to providing palliative care in the community pharmacy setting.
To ensure content validity, a panel of experts, including two clinical pharmacists with experience in palliative care, a physician and a nurse specialist in palliative care, and two professors of pharmacy practice, reviewed the questionnaire for relevance and comprehensiveness. A pilot test was then conducted with ten community pharmacists to assess the clarity and applicability of the questions; their responses were excluded from the final analysis. Prior to final implementation, face validity and comprehensibility were evaluated through cognitive debriefing during a pilot test with ten community pharmacists, focusing on clarity, interpretability of response options, and overall questionnaire flow; pilot responses were excluded from the final analysis. In addition, basic item analysis used to identify poorly performing items for review. The internal consistency of the scales was confirmed, with Cronbach’s alpha values of 0.84 and 0.72 for the attitudes and practice scales, respectively, indicating acceptable reliability.
Sample Size Calculation
The required sample size was determined using Green’s rule of thumb for regression analysis: n = 50 + 8 × number of predictors.13 This method ensures sufficient statistical power and accounts for the complexity added by each additional variable. The largest regression model in this study included 11 predictors, yielding a minimum required sample size of 138 participants (50 + 8×11 = 138).
Ethical Approval
The study was approved by the Research Ethics Committee at Al Ain University – Abu Dhabi Campus (Reference #: COP/AREC/AD/28), dated February 8, 2024.
Statistical Analysis
Data were analyzed using SPSS version 28, Illinois, New York, USA. Considering the non-normal distribution of continuous data, as verified by Q-Q plots, continuous variables were presented using medians and interquartile ranges (IQR), while categorical variables were summarized as percentages and frequencies. A quantile regression was conducted to explore the factors influencing the dependent variable, which was pharmacists’ practices of palliative care. The independent variables included in the model were age, gender, educational level, type of pharmacy, years of experience working as a community pharmacist, average number of prescriptions dispensed daily, and knowledge and attitude scores. Statistical significance was set at a threshold of p < 0.05. Variables were chosen based on their theoretical relevance and previous research linking these factors with pharmacists’ involvement in palliative care. Sociodemographic and professional variables were used to account for potential differences in practice patterns, whereas knowledge and attitude scores were included due to their anticipated impact on palliative care practices. All factors were entered simultaneously in the regression model to evaluate their independent associations with pharmacists’ practice scores.
Results
A total of 431 community pharmacists participated in the study. The majority were female (56.8%) with a median (IQR) age of 33 (27–38) years. Most pharmacists had a bachelor’s in pharmacy (73.8%), worked in Abu Dhabi (95.4%), worked in chain community pharmacies (71.0%), were pharmacists in charge or employee pharmacists (93.0%), and had between 1 and 10 years of experience (65%). The majority dispensed 10–29 prescriptions daily (60.1%), served 30 or more patients daily (48.7%) and spent 2 to 5 minutes in patient consultation (60.8%). Sociodemographic and job-related characteristics are shown in Table 1.
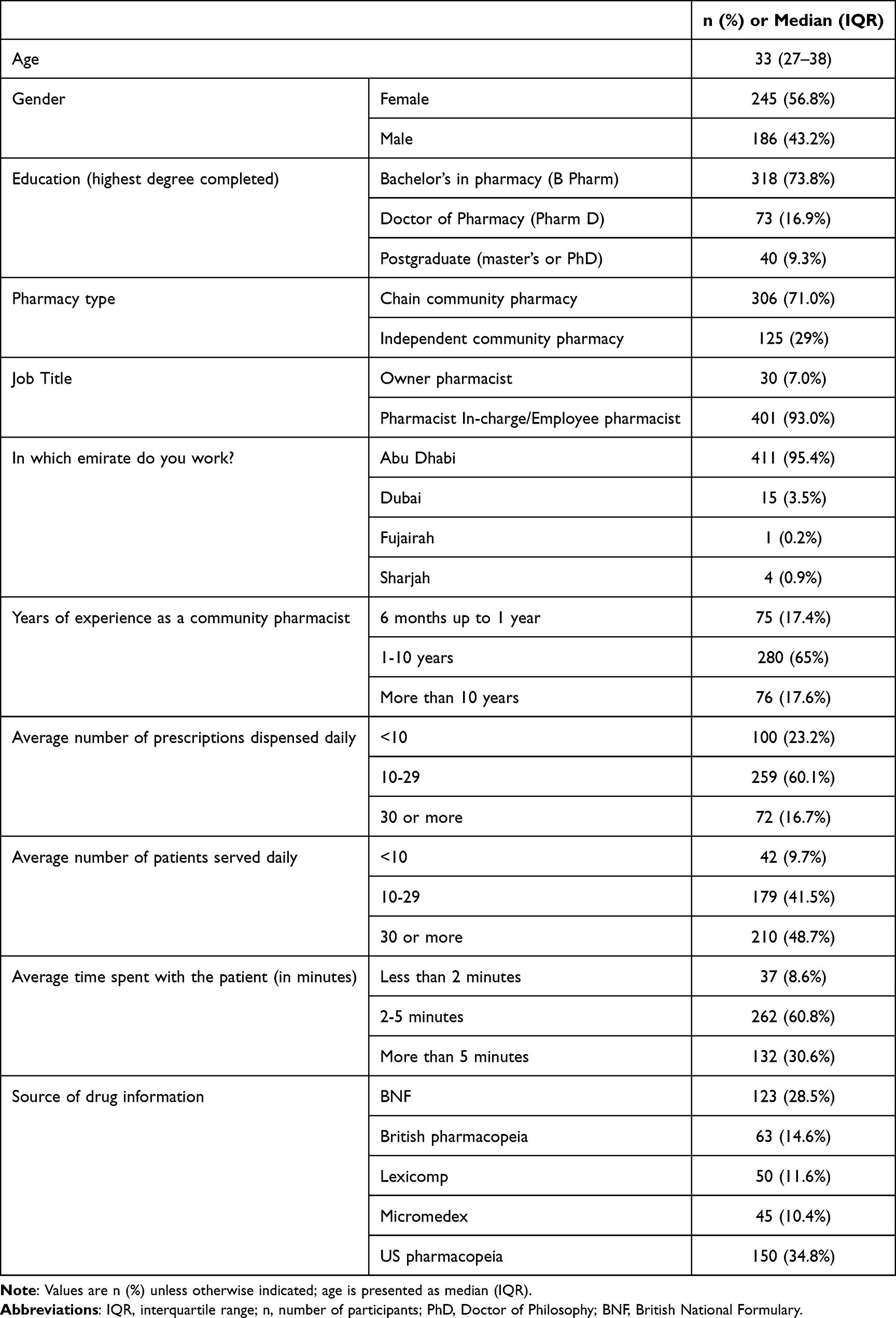 |
Table 1 Sociodemographic and Job-Related Characteristics for the Study Pharmacists (n = 431) |
Table 2 summarizes the responses of community pharmacists to a series of statements assessing their knowledge of palliative care. The median (IQR) knowledge score was 4 (3–5) out of a maximum of 13, with fewer than 50% of the pharmacists answering any of the knowledge items correctly. The most frequently correct answer was for the statement “Long-term use of opioids for palliative care patients does not often induce addiction” (46.9%), followed by “Benzodiazepines should be effective for controlling delirium in palliative care patients” (44.1%). The least correctly answered item was “Palliative care should focus on both physical and psychological needs of the affected patient” (16.7%).
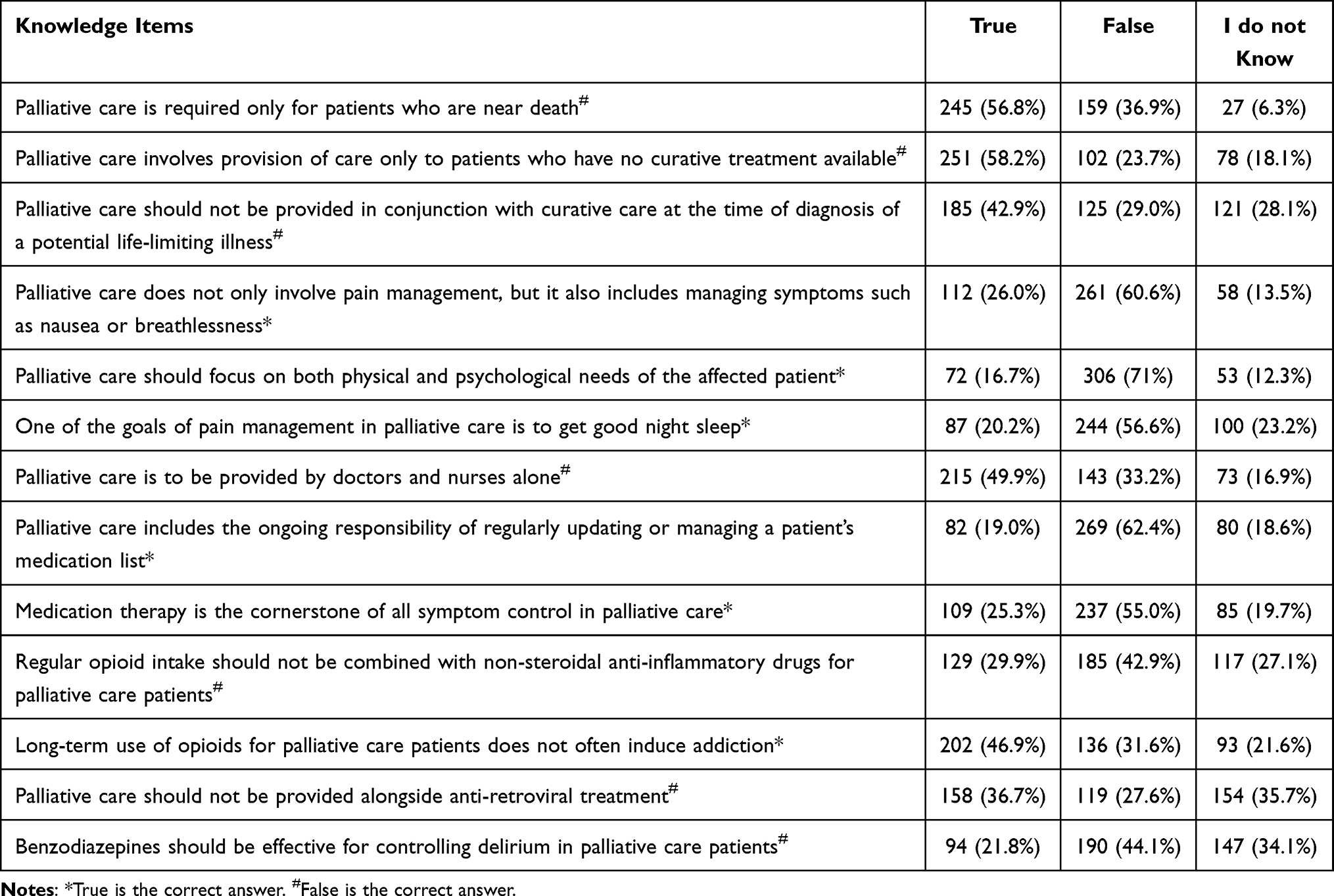 |
Table 2 Community Pharmacists’ Knowledge of Palliative Care and Its Management n (%) |
The median (IQR) attitude score was 45 (41–48) out of a maximum possible score of 60, demonstrating room for improvement, particularly in the perceived ability to provide palliative care (51.7%) and the perceived confidence in managing pain and symptoms (53.2%). In contrast, the most favourable attitudes were reflected in agreement with statements such as “Palliative care offers hope and comfort to patients” (71.5%) and “The pharmacist has a key role to play as a member of the palliative care team” (66.8%; Table 3).
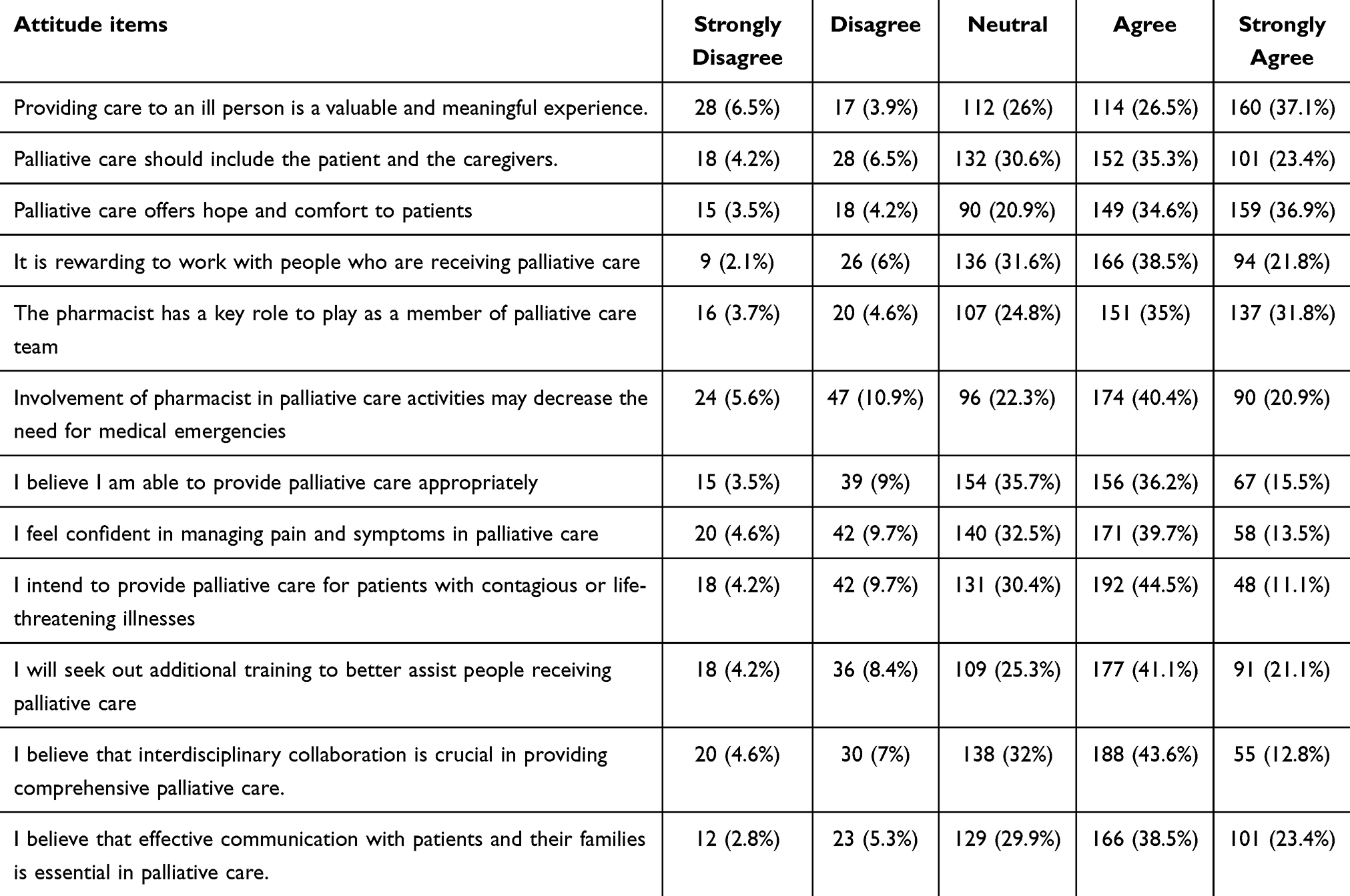 |
Table 3 Community Pharmacists’ Attitudes Toward Palliative Care and Their Role in Palliative Care Management n (%) |
The median (IQR) practice score was 41 (37–44) out of a maximum possible score of 55. As shown in Table 4, pharmacists demonstrated poor practices, as less than half of them performed the essential palliative care practices across all measured items. Specifically, poor performance was evident in practices such as visiting patients’ homes to communicate directly with patients and their caregivers and to make necessary assessments (10.0%) and providing medication-related pain management recommendations to other healthcare providers (16.0%). In contrast, the most performed practices included monitoring prescription and non-prescription medications for safety and effectiveness (38.3%) and providing patients with essential medications to ensure continuous symptom control (36%). Nevertheless, less than 50% of the participants performed either of these practices.
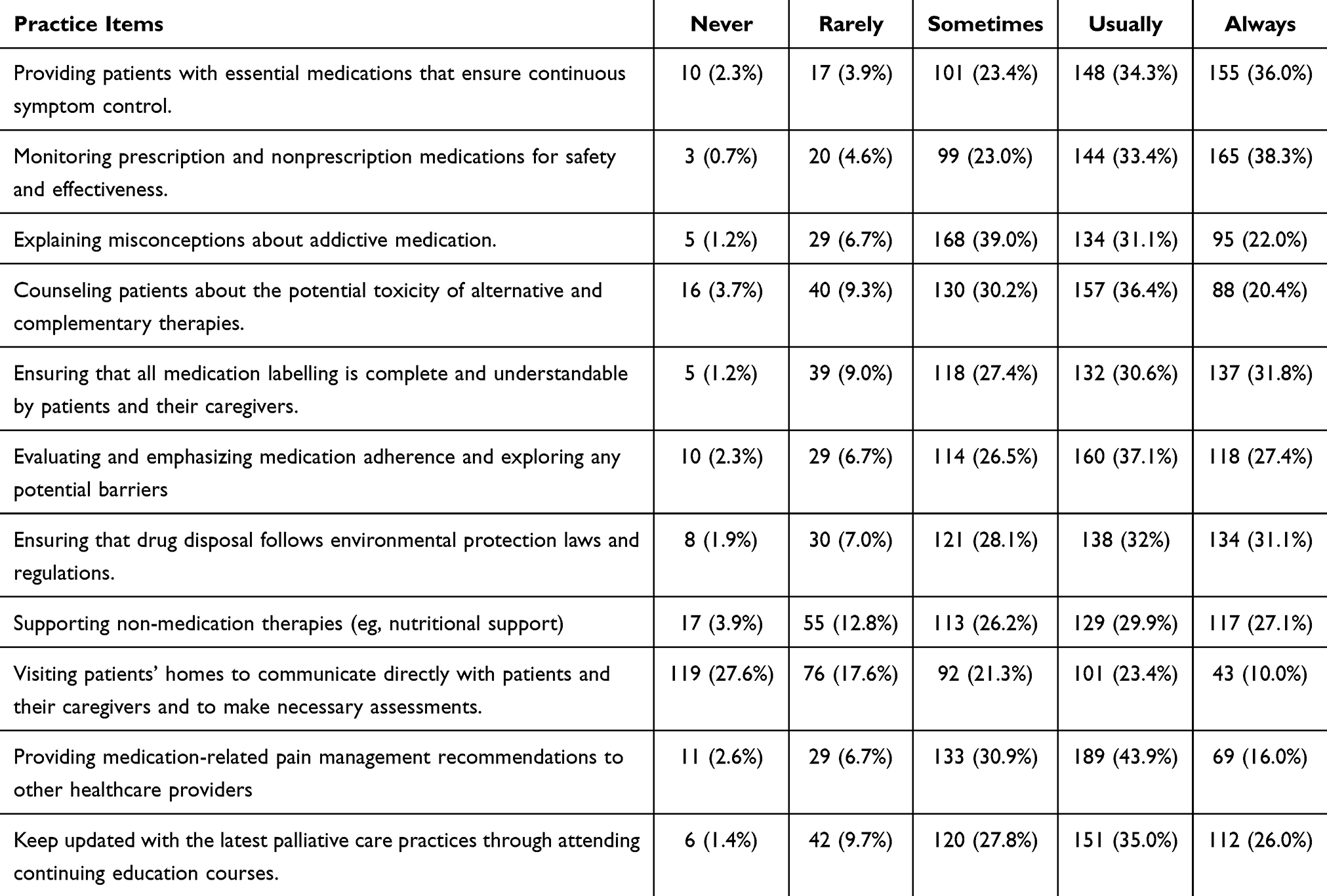 |
Table 4 Community Pharmacists’ Practices Regarding Palliative Care n (%) |
The results of the quantile regression (Table 5) revealed that pharmacists with higher attitude scores had significantly higher practice scores (coefficient = 0.375; 95% CI: 0.283–0.467; p < 0.001). Additionally, increased age was associated with higher practice scores (coefficient = 0.122, 95% CI: 0.009–0.235; p = 0.034).
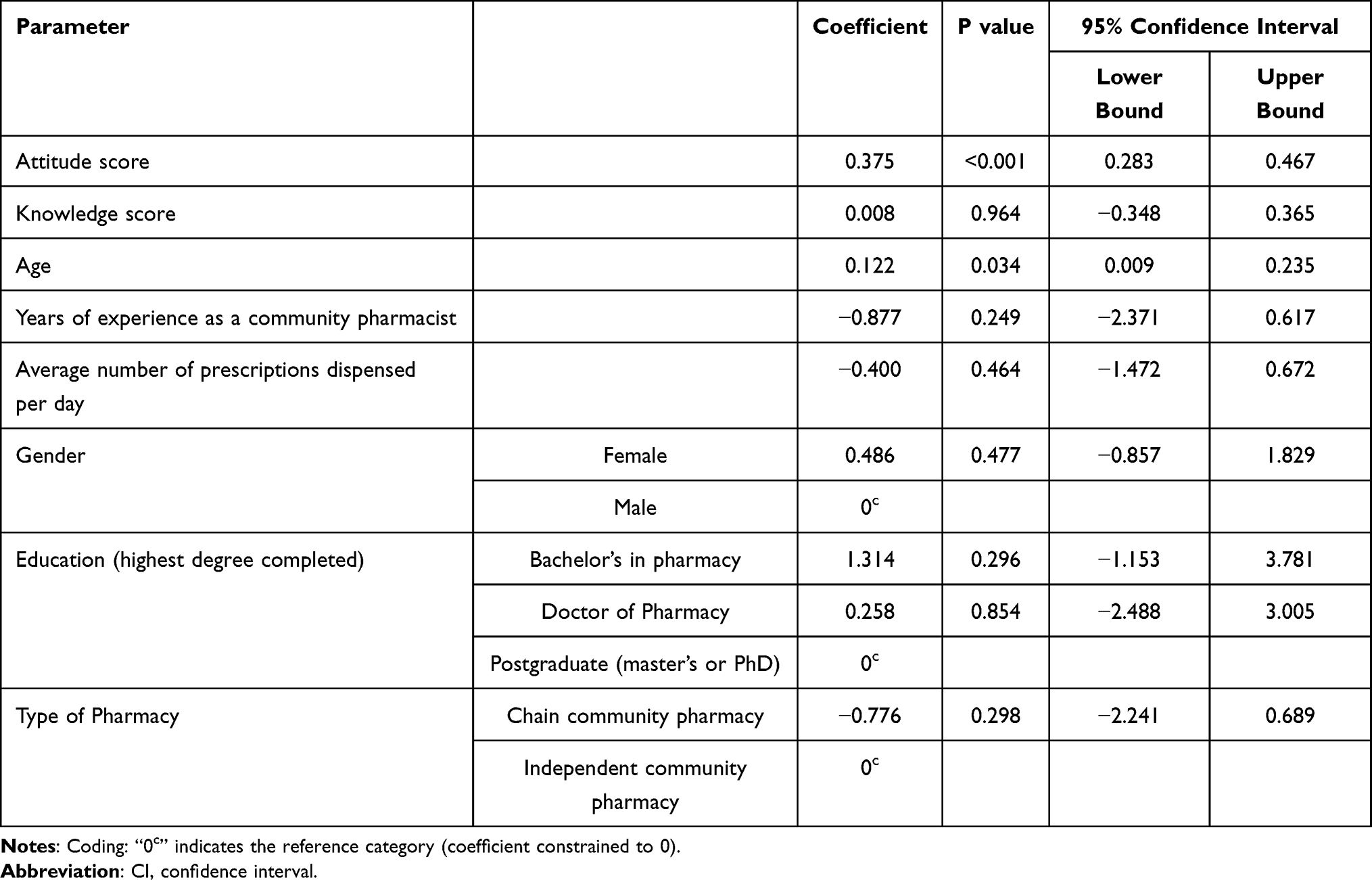 |
Table 5 Quantile Regression Analysis of Variables Associated with Pharmacists’ Practices Toward Palliative Care |
Figure 1 displays the obstacles pharmacists face in providing palliative care. The most reported barrier was a lack of training (53.4%), followed by a lack of patient awareness regarding the pharmacist’s role in palliative care (50.1%). In contrast, inadequate knowledge of the concept of palliative care (27.8%) and a lack of reimbursement (28.5%) were the least reported barriers.
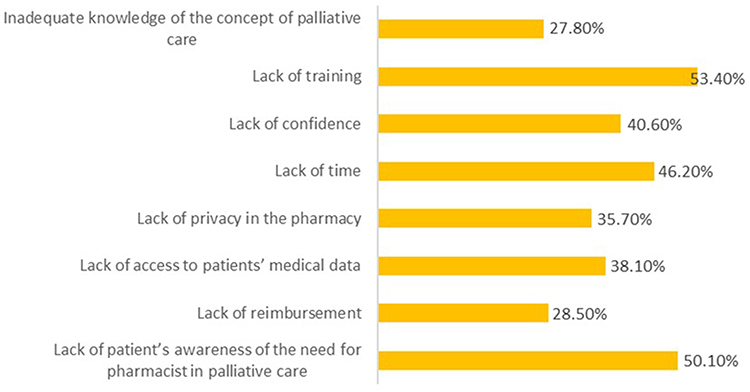 |
Figure 1 Barriers to providing palliative care. |
Discussion
This study highlighted critical gaps in pharmacists’ knowledge regarding palliative care and its effective management, shed light on their perception towards their roles and responsibilities, evaluated how frequently they are involved in palliative care, identified the key factors influencing their involvement, and uncovered the barriers affecting the delivery of care to patients. These findings are crucial for developing strategies to enhance pharmacists’ roles in palliative care, particularly within the UAE and similar healthcare settings.
In line with earlier findings,9,11 the present study revealed significant gaps in pharmacists’ understanding of fundamental aspects of palliative care, indicating a widespread lack of knowledge across several critical themes. Similar to earlier research findings,9,14 many pharmacists in the present study believed that palliative care is only necessary for patients who are imminently dying or for whom curative treatment is no longer needed. This overlooks the important concept that palliative care should be introduced early alongside curative efforts to address the complex and ongoing needs of patients with life-limiting illnesses Previous studies have emphasized the multifaceted scope of palliative care9,11 nevertheless, pharmacists in the current study revealed insufficient awareness that, in addition to pain management, palliative care extends to include the relief of distressing symptoms such as nausea and breathlessness, as well as addressing the psychological and emotional needs of patients.
Consistent with previous findings,9,15 the present study revealed misunderstandings about the multidisciplinary approach to palliative care. Pharmacists in our study incorrectly assumed that doctors and nurses solely deliver palliative care, thereby underestimating the pharmacist’s vital role in medication management and symptom control in palliative care. Additionally, the study identified that pharmacists showed uncertainty regarding key pharmacological principles, such as the safe use of opioids, the importance of combining different types of analgesics appropriately and the misconception that long-term opioid use necessarily leads to addiction in palliative patients, which is consistent with previous research findings.6,9,11
These knowledge gaps likely contribute to reduced pharmacist engagement in palliative care, limiting both confidence and effective participation within multidisciplinary teams. Overall, these results indicate an urgent need to strengthen pharmacists’ education and training on palliative care. Addressing these gaps through targeted interventions will be essential to empower pharmacists to participate fully in delivering comprehensive, patient-centered care that improves quality of life for individuals facing serious illnesses.14
Despite demonstrating generally positive attitudes toward palliative care, many pharmacists reported limited confidence in their practical competencies, indicating that positive professional values do not necessarily translate into clinical readiness. The findings align with research from Australia, where pharmacists consistently valued palliative care principles but reported certain emotional challenges in its implementation.16 In the present study, pharmacists understood the importance of involving both patients and their caregivers and saw palliative care as a source of hope and comfort. They also acknowledged the crucial role pharmacists play within the palliative care team and stressed the need for good communication and teamwork among healthcare providers. However, despite these encouraging attitudes, two key areas stood out where pharmacists expressed uncertainty. Only about half felt confident in their ability to provide palliative care and manage pain and symptoms effectively aligning with research from Nigeria where pharmacists showed limited confidence in core palliative care competencies.9 This pattern is consistent across diverse contexts, with studies from Australia and Saudi Arabia reporting that although pharmacists demonstrate positive attitudes towards palliative care, they felt unprepared and showed concerns about their practical involvement and clinical competencies in providing palliative care.11,16 Without confidence in these skills, pharmacists may hesitate to fully engage in patient care, which could limit the quality of services provided. Bridging this gap requires more focused support and targeted educational interventions that go beyond knowledge enhancement to boost pharmacists’ confidence and improve pharmacists’ self-assurance in managing symptoms and providing care. Additionally, integrating palliative care modules into pharmacy curricula and fostering collaborative practice models can further strengthen pharmacists’ essential contributions to palliative care delivery.
Fewer than half of the pharmacists in this study reported engaging in most of the assessed practices that covered several key themes, including symptom control through appropriate medication provision, drug safety monitoring, patient and caregiver education, interprofessional collaboration, support for non-drug therapies, and ongoing professional development. Consistent with previous research finding,9 pharmacists in this study were less involved in proactive, patient-centered palliative treatments, such as conducting direct home visits to patients and caregivers, and providing medication-related pain management advice to other healthcare professionals. These gaps significantly limit pharmacists’ ability to support patients with terminal illnesses in managing their symptoms and improving their quality of life. To address these challenges, educational interventions must focus not only on knowledge but also on practical application of palliative care skills. Additionally, interprofessional care models to better integrate pharmacists into clinical teams are deemed necessary. Furthermore, there is a need for a policy-level support to formally recognize and facilitate the pharmacist’s role in home-based care and shared decision-making. An emphasis on continuous professional development in palliative care and creating pathways for pharmacists to lead on medication management and symptom control can greatly enhance practice standards and help pharmacists contribute to comprehensive, compassionate care for patients at the end of life.
When viewed regionally and globally, the findings of this study are consistent with reports from other countries, including Saudi Arabia, Nigeria, Australia, and several European settings, where pharmacists have expressed positive attitudes toward palliative care but have limited knowledge and practical experience.5,9,11,16 Similar disparities in confidence, training, and role clarity have been reported worldwide,5 implying that the difficulties identified in the UAE are part of a larger global trend rather than isolated local inadequacies.
The positive correlation between higher attitude scores and improved practices in palliative care emphasizes the critical role that positive attitudes play in improving the quality and scope of care provided. Recent research confirms that pharmacists’ positive perceptions of their professional role significantly increase their engagement in palliative care, as positive attitudes foster the motivation and assurance required for effective practice.11 Current research further supports this connection by showing that pharmacists with positive attitudes are more likely to actively participate in comprehensive care interventions and use patient-centered approaches, highlighting the idea that attitude essentially influences clinical practices and behavioral intentions.17 Similar findings emerge in chronic diseases18 and mental health19 management, where pharmacists’ positive perceptions of their role correlate with increased engagement in medication therapy reviews and collaborative care planning.
Recent regional evidence strengthens and contextualizes these findings. A recent Saudi Arabian study found that community pharmacists had positive attitudes and a willingness to participate in palliative care, but only moderate readiness due to training gaps, emotional preparedness challenges, and a lack of role clarity.20 While these findings are similar to the current study in terms of attitudes and perceived barriers, we extend the regional literature by demonstrating a direct link between positive attitudes and higher levels of palliative care practice. This suggests that, in similar healthcare systems, attitudes may play a more important role in translating willingness into action when combined with appropriate training and system-level integration.
The study’s significant link between higher palliative care practice scores and increased age implies that senior pharmacists utilize extensive clinical experience to develop greater confidence and a deeper comprehension of palliative care difficulties.5,21 These observations highlight the urgent need for focused educational programs, and reflective professional development courses aimed at improving pharmacists’ perspectives on palliative care, particularly among those with fewer years of experience. Furthermore, leveraging the experience and mentoring skills of more seasoned pharmacists to support early-career colleagues offers a crucial approach to bridge knowledge and confidence gaps, which promotes a culture of continuous improvement and elevates overall standards of care. To maximize patient-centered outcomes in this specialized field and advance pharmacists’ role within palliative care teams, intentional strategies that cultivate positive attitudes and utilize experiential wisdom are essential.11
The predominance of training-related and awareness-based barriers indicates that limited pharmacist involvement in palliative care is driven more by system-level constraints than by individual willingness. Previous studies in Western Europe and Australia reported that insufficient specialized palliative care education and training remain key barriers, severely restricting pharmacists’ confidence, competence, and integration within multidisciplinary teams, while limited patient awareness curtails their practical engagement and recognition as integral care providers.16,22,23 A trend that is strikingly consistent with global and cross-specialty findings highlights education and awareness gaps as significant challenges in maximizing pharmacists’ contributions to complex care domains such as palliative care, chronic diseases, and mental health management.8,17
The inadequate public awareness of pharmacists’ roles reported in this study has also been reported in earlier studies targeting chronic conditions24 and pandemics.25 Enhancing public engagement and raising awareness are crucial steps toward clearly defining and promoting the pharmacist’s role in palliative care teams.26 These efforts can facilitate better integration of pharmacists into multidisciplinary care settings, ultimately contributing to improved patient outcomes.
The study’s findings have significant implications for pharmacy education and national palliative care planning in the UAE. Integrating structured palliative care content into undergraduate pharmacy curricula, with a focus on symptom management, communication skills, and interdisciplinary collaboration, could help to close the identified knowledge and confidence gaps. On a nationwide scale, explicitly acknowledging community pharmacists within palliative care frameworks and extending their participation in drug administration, patient education, and home-based care could improve service delivery and patient outcomes. Such techniques would help pharmacists integrate into multidisciplinary palliative care teams while also aligning with the UAE’s overall healthcare development goals.
This study has several limitations. The findings are based on self-reported data from community pharmacists and therefore reflect respondents’ perceived knowledge, attitudes, and practices about palliative care. Although this approach is appropriate for capturing professional perspectives and experiences, self-reported measures may be subject to social desirability or recall bias, potentially leading to an overestimation of engagement or confidence. Nonetheless, the observed associations, particularly the relationship between positive attitudes and improved practices, are consistent with data reported in regional and international studies, supporting credibility and relevance of the findings.
Conclusions
This study is the first to conduct a comprehensive assessment of community pharmacists’ knowledge, attitudes, practices, and perceived barriers to palliative care in the United Arab Emirates, providing evidence that is directly relevant to national workforce development and palliative care planning. Although pharmacists expressed generally positive attitudes, notable knowledge gaps and limited practical engagement highlight a persistent disconnect between professional willingness and clinical readiness.
Importantly, professional attitudes emerged as a significant predictor of palliative care practice, implying that effective workforce development in the UAE must go beyond knowledge acquisition and include strategies to boost confidence, role clarity, and clinical readiness. Integrating competency-based training and structured continuing professional development into national frameworks could aid in translating positive attitudes into meaningful practice.
The limited involvement of community pharmacists appears to be primarily due to system-level barriers, such as insufficient training, a lack of formal role recognition, and low public awareness. Addressing these challenges is consistent with the UAE’s ongoing health system transformation goals of integrated, patient-centered care and optimal use of healthcare professionals. Formal inclusion of community pharmacists in national palliative care strategies, backed up by regulatory recognition and interdisciplinary collaboration, could improve service delivery and continuity of care.
Despite the use of self-reported data, the findings’ consistency with regional and international evidence supports their relevance for informing policy and practice. Strengthening community pharmacists’ roles in palliative care pathways represents a feasible and scalable opportunity to improve medication management, team-based care, and quality of life for patients with life-limiting illnesses in the UAE.
Data Sharing Statement
The data that supports the findings of this study are available from the corresponding author, upon reasonable request.
Ethics Approval and Informed Consent
The study was approved by the Research Ethics Committee at Al Ain University – Abu Dhabi Campus (Reference #: COP/AREC/AD/28), dated February 8, 2024.
Acknowledgments
The authors would like to thank all the pharmacists who completed the study questionnaire.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
1. Sharkey L, Loring B, Cowan M, Riley L, Krakauer EL. National palliative care capacities around the world: results from the World Health Organization Noncommunicable Disease Country Capacity Survey. Palliat Med. 2018;32(1):106–12. doi:10.1177/0269216317716060
2. NICE U. End of life care for adults: service delivery. NICE Guidel. 2019;(November 2011):1–17.
3. The Lancet Healthy Longevity. Universal palliative care for healthy longevity. Lancet Heal Longev. 2024;5(5):e303. doi:10.1016/S2666-7568(24)00070-9
4. Etkind SN, Bone AE, Gomes B, et al. How many people will need palliative care in 2040? Past trends, future projections and implications for services. BMC Med. 2017;15(1):1–10. doi:10.1186/s12916-017-0860-2
5. Krzyzaniak N, Pawłowska I, Bajorek B. An overview of pharmacist roles in palliative care: a worldwide comparison. Med Paliatywna w Prakt. 2016;10(4):160–173.
6. Moody JJ, Poon IO, Braun UK. The role of an inpatient hospice and palliative clinical pharmacist in the interdisciplinary team. Am J Hosp Palliat Med. 2022;39(7):856–864. doi:10.1177/10499091211049401
7. Blair I, Sharif AA. Population structure and the burden of disease in the United Arab Emirates. J Epidemiol Glob Health. 2012;2(2):61–71. doi:10.1016/j.jegh.2012.04.002
8. ElMokhallalati Y, Bradley SH, Chapman E, et al. Identification of patients with potential palliative care needs: a systematic review of screening tools in primary care. Palliat Med. 2020;34(8):989–1005. doi:10.1177/0269216320929552
9. Adisa R, Anifowose AT. Pharmacists’ knowledge, attitude and involvement in palliative care in selected tertiary hospitals in southwestern Nigeria. BMC Palliat Care. 2019;18(1):107. doi:10.1186/S12904-019-0492-8
10. Harhara T, Ibrahim H. Undergraduate palliative care education in the United Arab Emirates: a nationwide assessment of medical school deans. BMC Med Educ. 2021;21(1):1–8. doi:10.1186/s12909-021-02966-4
11. Alshehri AM, Almogbel YS, Alonazi RE, et al. Pharmacists’ knowledge and intention to provide palliative care services in Saudi Arabia: using the theory of planned behaviour. Healthcare. 2023;11(15):2173. doi:10.3390/HEALTHCARE11152173
12. Getie A, Wondmieneh A, Mengesha A, Fitwi A, Gedefaw G, Demis A. Assessment of knowledge and attitude towards palliative care and associated factors among nurses working in North Wollo Hospitals. Ethiop J Health Sci. 2021;31(2):393–400. doi:10.4314/ejhs.v31i2.22
13. Green SB. How many subjects does it take to do a regression analysis? Multivariate Behav Res. 1991;26(3):499–510. doi:10.1207/S15327906MBR2603_7
14. Alsolami FN, Alharbi IM, Alsulami JN, et al. Assessment of knowledge and attitudes toward palliative care and end-of-life decision-making in Saudi Arabia: a cross-sectional study. Cureus. 2023;15(9). doi:10.7759/CUREUS.45781
15. Bryant LJM, Coster G, Gamble GD, McCormick RN. General practitioners’ and pharmacists’ perceptions of the role of community pharmacists in delivering clinical services. Res Soc Adm Pharm. 2009;5(4):347–362. doi:10.1016/J.SAPHARM.2009.01.002
16. O’Connor M, Hewitt LY, Tuffin PHR. Community pharmacists’ attitudes toward palliative care: an australian nationwide survey. J Palliat Med. 2013;16(12):1575. doi:10.1089/JPM.2013.0171
17. Yamada M, Uchida M, Hada M, et al. Pharmacists’ behavioral changes after attending a multi-prefectural palliative care education program. Pharm. 2024;12(3):87. doi:10.3390/PHARMACY12030087
18. Dawsar A, Khathami A, Ziad Aldaajani M, et al. The role of clinical pharmacists in chronic disease management: review. Int J Health Sci (Qassim). 2024;8(S1):1766–1776. doi:10.53730/IJHS.V8NS1.15389
19. Soubolsky A, Halpape K, Jorgenson D, Remillard AJ, Necyk C. Between what is and what could be: a survey of pharmacists’ practices, attitudes, and beliefs in the provision of mental health care. Int J Clin Pharm. 2023;45(5):1192–1202. doi:10.1007/S11096-023-01633-6/METRICS
20. Alshahrani SM. Perception and readiness of community pharmacists in delivering palliative care services in Saudi Arabia: a new role in the game. Front Pharmacol. 2025;16:1646531. doi:10.3389/fphar.2025.1646531
21. L MC-W, A MB, Hattingh L. Cross-sectional study to evaluate patients’ medication management with a new model of care: incorporating a pharmacist into a community specialist palliative care telehealth service. BMC Palliat Care. 2024;23(1).
22. Carey ML, Zucca AC, Freund MAG, Bryant J, Herrmann A, Roberts BJ. Systematic review of barriers and enablers to the delivery of palliative care by primary care practitioners. Palliat Med. 2019;33(9):1131–1145. doi:10.1177/0269216319865414
23. Tait P, Chakraborty A, Tieman J. The roles and responsibilities of community pharmacists supporting older people with palliative care needs: a rapid review of the literature. Pharm. 2020;8(3):143. doi:10.3390/PHARMACY8030143
24. Eades CE, Ferguson JS, O’Carroll RE. Public health in community pharmacy: a systematic review of pharmacist and consumer views. BMC Public Health. 2011;11(1):1–13. doi:10.1186/1471-2458-11-582/TABLES/2
25. Jarab AS, Al-Qerem W, Mukattash TL, et al. Public perception of pharmacist’s role during COVID-19 outbreak in Jordan. Jordan J Pharm Sci. 2022;15(3):365–377. doi:10.35516/JJPS.V15I3.410
26. Alnajar M, Darawad M, Khater W, et al. Exploring palliative care needs among patients with cancer and non-cancer serious chronic diseases: a comparison study. American Journal of Hospice and Palliative Medicine. 2025;42(1):20–31. doi:10.1177/10499091241235920
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.